14. Percent
|
|
|
- Berenice Burke
- 5 years ago
- Views:
Transcription

 of drugs or devices during the course of their presentations. What is Insomnia?")


 10% Trouble falling asleep Frequent awakening or trouble returning to sleep after awakening Waking earlier than desired")
1 4:30 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau for Merck & Co., Inc. and XenoPort, Inc. SPEAKER Alon Y. Avidan, MD, MPH, FAAN, FAASM Off-Label/Investigational Discussion In accordance with pmicme policy, faculty have been asked to disclose discussion of unlabeled or unapproved use(s) of drugs or devices during the course of their presentations. What is Insomnia? Prevalence of Insomnia by Age Group Difficulties Falling Asleep Difficulties Maintaining Early Morning Awakenings Next Day Consequences: Fatigue Attention, concentration, or memory impairment Social/vocational dysfunction Mood disturbance/irritability Proneness for errors/accident at work or while driving Tension headaches, and/or GI symptoms in response to sleep loss Concerns or worries about sleep Despite adequate opportunity for sleep. Percent Age Group ICSD III Mellinger GD et al. Arch Gen Psychiatry. 1985;42: DSM-5 INSOMNIA Causes of Insomnia 3 nights/wk 3 months Primary / psychophysiologic 20% Periodic limb movement 10% Initiation Maintaining Waking early Circadian rhythm ( DSPS / shift ) 10% Trouble falling asleep Frequent awakening or trouble returning to sleep after awakening Waking earlier than desired Breathing related 5% Substances 5% Psychiatric 40% Other 10% APA Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition: DSM-5 Ohayon MM. Med Rev. 2002;6:

 1 1.")
2 Insomnia According to Timing at Night Difficulties Initiating RLS Anxiety Drugs Difficulties Maintaining Primary Disorder: OSA, Nocturia Poor sleep environment Early morning awakening ASPS Depression Drugs Approach to the Management of Insomnia What Do People Take to Try to Improve Their? Diagnosis 1,2 Education, including good sleep practices 1,2 Nonpharmacologic and/or pharmacologic therapy 1,2 Alcohol 1,2,3 Herbals 3,4 Dietary supplements 1,4 Homeopathic preparations 4 Melatonin 1,3,4 OTC sleep aids 2 Sedating antidepressants 1 Sedative-hypnotics 1,5 Melatonin receptor agonist Hypocretin Receptor Antagonist Referral to sleep specialist (in cases of treatment failure) 1 1. Kupfer DJ, Reynolds CF III. N Engl J Med. 1997;336: [Evidence Level C]; 2. Consensus Conference. Drugs and insomnia. JAMA ;251: [Evidence Level C] 1. Neubauer DN. Clinical Cornerstone. 2003;5: Ancoli-Israel S, Roth T ;22(suppl 2):S347-S Wagner J et al. Neuropsychiatry. 1998;32: Larzelere MM, Wiseman P.Prim Care Clin Office Pract. 2002;29: Mitler MM ;23(suppl 1):S39-S47. What Do People Take to Try to Improve Their? Diary 28% use alcohol

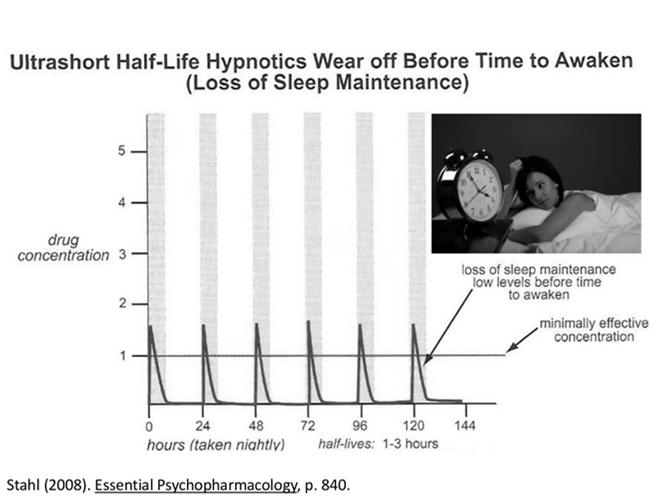
3 Characteristics of the Ideal Hypnotic No memory deficits Rapid absorption Address underlying pathophysiology Drug classes No respiratory depression No interaction with ethanol Ideal Hypnotic Rapid sleep induction Minimal adverse effect on sleep physiology Histamine Receptor Antagonist BZA Receptor Agonists Melatonin Receptor Agonist Hypocretin Receptor Antagonist No tolerance No physical dependence No rebound insomnia No residual effects Optimal duration of action No formation of active metabolites Doxepin Zolpidem Eszopiclone Zaleplon Triazolam Ramelteon Suvorexant Adapted from Mendelson et al. Med Rev 2004;8: Hypnotics: Mechanism of Action & Labeling Class 1 Drugs 1,2 Acts on:1 Controlled Substance Schedule 2 Barbiturates Antipsychotics Phenobarbital, mephobarbital, amobarbital, secobarbital Quetiapine, risperidone, aripiprazole Non-selective CNS depressants Dopamine, serotonin II, III, IV Not scheduled Antidepressants Tradozone, amitriptyline Serotonin/histamine Not scheduled Benzodiazepines Temazepam, estazolam, flurazepam, quazepam, triazolam GABA Antihistamines Diphenhydramine 5 Histamine Not scheduled Nonbenzodiazepines Zolpidem, eszopiclone, zaleplon GABA IV Melatonin receptor agonist Ramelteon Melatonin Not scheduled Selective H 1 receptor antagonist 3 Doxepin Histamine H 1 Not scheduled Orexin receptor antagonist 4 Suvorexant Orexin IV IV DRUGS INDICATED FOR INSOMNIA Generic Brand T 1/2 (Hours) Dose (mg) Drug Class Flurazepam Dalmane BZD Temazepam Restoril BZD Triazolam Halcion BZD Estazolam Prosom BZD Quazepam Doral BZD Zolpidem Ambien non-bzd Zaleplon Sonata non-bzd Eszopiclone Lunesta non-bzd Zolpidem Ex Rel Ambien CR * non-bzd Ramelteon Rozerem MT agonist Silenor Doxepin , 6 H 1 Antagnonist Suvorexant Belsomra 12 5, 10, 15, 20 Hcrt Antagonist 1. Roth T, Culpepper L. Clinical Symposia. 2008;58:1-32; 2. Controlled Substances Act. Accessed June 9, 2015; 3. SILENOR (doxepin) [package insert]. Morristown, NJ: Pernix Therapeutics; 2014; 4. Belsomra (suvorexant) [package insert]. Whitehouse Station, NJ; Merck and Co. 2014; 5. Richardson GS et al. J Clin Psychopharmacol. 2002;22: * Modified formulation. No short-term use limitation. BZRA Hypnotics: Possible Adverse Effects Agent Initiates Maintains with limited opportunity Required Inactivity (hr) Dose (mg) Eszopiclone 8+ 1,2,3 Zaleplon 4 5,10 Zolpidem 7-8 5,10 Extended release , 12.5 Intermezzo (Sublingual) (4 hrs) , , 10 Zolpimist (oral spray) Elduar (Sublingual) 4 5, 10 Silenor 7-8 3, 6 Ramelteon - 8 Suvorexant 7 5, 10, 15, 20


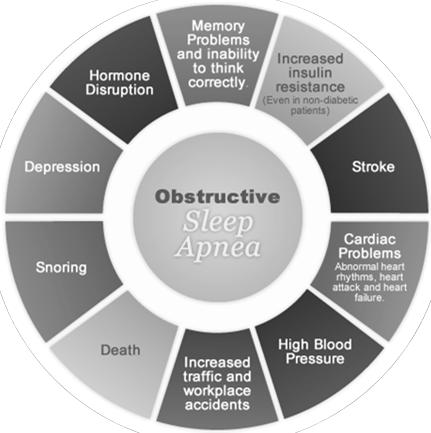
4 MELATONIN OREXIN HISTAMIN OBSTRUCTIVE SLEEP APNEA SYNDROME




5 Obesity Trends in the US: CDC Dataset Phenotypic Features Consistent with OSA EKG Airflow Exhale Airway obstructs Airway opens Thoracic effort Inhale Effort gradually increases Abd. effort Paradoxing SAO2 Paradoxing Ends Blood oxygen levels reduce to < 3% of baseline value Obstructive Apnea A complete blockage of the airway despite efforts to breath. Notice the effort gradually increasing ending in airway opening. Kryger: Principles and Practice of Medicine, 5th ed. Nuchton, TJ et al Jul;29(7): Treatment of OSA SLEEP HYPNOGRAM Weight loss CPAP/BiPAP Positional Tx Oral Appliances UPPP LAUP Bimax Advancement Trach Drugs Avoidance of Rx/Etoh OXYGEN SATURATION

 Study Group in collaboration with the National Institutes of Health (NIH). Allen et al. Med. 2003;4:101-119.")
6 Willis-Ekbom Disease Essential Criteria* Supportive Features* disturbances Urge to move the legs usually accompanied or caused by uncomfortable leg Periodic leg movements sensations Positive family history for RLS Getting up: Temporary relief with movement partial or total relief from discomfort by walking or stretching Positive response to dopaminergic therapy Differential Diagnosis of RLS Rest: Onset or worsening of symptoms at rest or inactivity, such as when lying or sitting Evening: Worsening or onset of symptoms in the evening or at night * Diagnostic criteria developed by the International RLS (IRLS) Study Group in collaboration with the National Institutes of Health (NIH). Allen et al. Med. 2003;4: RLS RLS is a symptom based Dx PLMS PLMS are an EMG finding Management of RLS Conservative Tx Pharmacotehrapy RLS is Dx in the physician s office PLM s are Dx in the sleep lab Alerting activities Iron state Ferritin <45 ug/l 80% of people who have RLS will have PLM s 30% of individuals who have PLM s have RLS symptoms Avoid Etoh, Caffeine Nicotine Review Medications 1. Ropinirole, 2. Pramipexole, 3. Rotigotine 4. Gabapentin Enacarbil FDA-approved medication for the treatment of moderate-tosevere primary RLS. Hypnotics Levodopa, Opioids Silber, M, et al September 2013;88(9): Narcolepsy Disorder of unknown etiology Consists of: Excessive sleepiness REM sleep phenomena (i.e cataplexy) PARASOMNIAS Undesirable motor, or verbal phenomena that arise from sleep or sleep - wake transition











 Not")
7 Case WAKE A 64 y/o man presented to the ER with a broken wrist experienced during a fighting dream. For the last 6m, he has been sleeping in a separate room than his wife after he had punched her during one of these dreams. What is the most likely diagnosis? REM NREM NREM REM Behavior Disorder RBD is most commonly associated with neurodegenerative disease, particularly ɑ-synucleinopathies: Parkinson s disease Dementia with Lewy Bodies Multiple System Atrophy Pharmacologic treatment of RBD Drug (*) Dose Level of Recommendation mg Clonazepam QHS Suggested ( ) Special considerations Environmental Safety Use with caution in patient s with dementia, gait disorders, or concomitant OSA. Side effect include sedation, impotence, motor incoordination, confusion and memory dysfunction. Melatonin 3 mg to 12 mg before bedtime. Suggested( ) Effective in patients with alphasynucleinopathies, memory problems, and sleep-disordered breathing. Side effects include headaches, sleepiness and delusions/hallucinations. Summary: Treatments of Disorders Condition Nonpharmacologic Pharmacologic Insufficient Syndrome Obstructive Apnea Increase total sleep time, e.g., naps Positive Pressure Therapy Airway surgery (CPAP) Not recommended Modafinil* (for residual sleepiness with CPAP compliance) Insomnia Behavioral Tx BZA *, non-bza agonists*, H1 antidepressants*, melatonin agonist, Hcrt antagonist* Narcolepsy Prophylactic power naps Modafinil,* dexamphetamine,* methylphenidate* RLS Hot bath, massage Dopaminergic agents, Dopamine agonist*, α2 delta ligand. Parasomnias Safety, Avoid exacerbating factors BZA
14. Percent Mellinger GD et al. Arch Gen Psychiatry. 1985;42: ICSD III
 4:45 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
4:45 5:45 pm Management of Insomnia and Other Disorders Presenter Disclosure Information The following relationships exist related to this presentation: Alon Y. Avidan, MD, MPH, FAAN, FAASM: Speakers Bureau
Sleep Disorders and Insomnia
 7:45 8:45 am Management of Insomnia and Other Disorders SPEAKER Alon Y. Avidan, MD, MPH, FAAN, FAASM Presenter Disclosure Information The following relationships exist related to this presentation: Alon
7:45 8:45 am Management of Insomnia and Other Disorders SPEAKER Alon Y. Avidan, MD, MPH, FAAN, FAASM Presenter Disclosure Information The following relationships exist related to this presentation: Alon
DSM-5 INSOMNIA. Maintaining. Maintaining Sleep. Difficulty Falling Asleep: Difficulty. Early AM awakenings: (> 30 minutes before desired wake time)
") DSM-5 INSOMNIA 3 nights/wk 3 months Difficulty Falling Asleep: > 30 minutes Difficulty Maintaining Sleep Next Day Consequences Early AM awakenings: (> 30 minutes before desired wake time) Initiation Trouble
DSM-5 INSOMNIA 3 nights/wk 3 months Difficulty Falling Asleep: > 30 minutes Difficulty Maintaining Sleep Next Day Consequences Early AM awakenings: (> 30 minutes before desired wake time) Initiation Trouble
Insomnia: Updates in Medical Management. Michael Newnam M.D.
 Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Insomnia. Arturo Meade MD
 Insomnia Arturo Meade MD Goals Definition Prevalence Pathophysiology The role of Orexin Orexin receptor blockers Consequences: Daily Functioning Insomnia: Consequences Decreased quality of life
Insomnia Arturo Meade MD Goals Definition Prevalence Pathophysiology The role of Orexin Orexin receptor blockers Consequences: Daily Functioning Insomnia: Consequences Decreased quality of life
Definitions. Prevalence. Chronic Insomnia DSM-5 INSOMNIA. Insomnia Is a Distinct Disorder That Should Be Treated ~10% 3 nights/wk 3 months
 Chronic Definitions Alon Y. Avidan, M.D., M.P.H UCLA Sleep Disorders Center Is a Distinct Disorder That Should Be Treated NIH (1983) 1 NIH (2005) 2 is a symptom, is a disorder not a disorder DSM-5 INSOMNIA
Chronic Definitions Alon Y. Avidan, M.D., M.P.H UCLA Sleep Disorders Center Is a Distinct Disorder That Should Be Treated NIH (1983) 1 NIH (2005) 2 is a symptom, is a disorder not a disorder DSM-5 INSOMNIA
The Medical Letter. on Drugs and Therapeutics. Usual Adult Hypnotic Dose 1,2 Some Adverse Effects Comments Cost 3
 The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call:
Insomnia treatment. Sleep hygiene education sleep hygiene teaches good sleeping habits. This includes:
 Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Pharmacological Help for a Good Night s s Sleep. Thomas Owens, MD
 Pharmacological Help for a Good Night s s Sleep Thomas Owens, MD Objectives 1. Define insomnia and characterize the symptoms and array of causes. 2. Describe traditional and new pharmacologic approaches
Pharmacological Help for a Good Night s s Sleep Thomas Owens, MD Objectives 1. Define insomnia and characterize the symptoms and array of causes. 2. Describe traditional and new pharmacologic approaches
Available Strengths Limits. 200 mg tablets PA. 50 mg, 150 mg, 200 mg, 250 mg tablets. 500 mg/ml solution PA
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY Sleeping Disorders P&T DATE: 12/14/2016 THERAPEUTIC CLASS Psychiatric Disorders REVIEW HISTORY: 2/16, 5/15, 2/12 LOB AFFECTED
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY Sleeping Disorders P&T DATE: 12/14/2016 THERAPEUTIC CLASS Psychiatric Disorders REVIEW HISTORY: 2/16, 5/15, 2/12 LOB AFFECTED
Insomnia Agents (Sherwood Employer Group)
") Insomnia Agents (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf Link to
Insomnia Agents (Sherwood Employer Group) BCBSKS will review Prior Authorization requests Prior Authorization Form: https://www.bcbsks.com/customerservice/forms/pdf/priorauth-6058ks-st-ippi.pdf Link to
Addressing Pharmacologic Issues in. DSM-5 Sleep-Wake. Insomnia. Disorders. DSM-5 Insomnia Disorder. Insomnia. Disorder
 Addressing Pharmacologic Issues in David N. Neubauer, MD Associate Professor of Psychiatry and Behavioral Sciences Johns Hopkins School of Medicine Baltimore, Maryland Restless Legs Syndrome Substance/
Addressing Pharmacologic Issues in David N. Neubauer, MD Associate Professor of Psychiatry and Behavioral Sciences Johns Hopkins School of Medicine Baltimore, Maryland Restless Legs Syndrome Substance/
Question #1. Disclosures. CAPA 2015 Annual Conference. All of the following occur as we get older EXCEPT: Evaluating Patients with Insomnia
 Evaluating Patients with Roger D. Seheult, M.D. Pulmonary Critical Care Physician - Beaver Medical Group, Redlands California Assistant Clinical Professor of Medicine - Loma Linda University School of
Evaluating Patients with Roger D. Seheult, M.D. Pulmonary Critical Care Physician - Beaver Medical Group, Redlands California Assistant Clinical Professor of Medicine - Loma Linda University School of
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Sleep Disorders: Assessment and Therapeutic Options
 Sleep Disorders: Assessment and Therapeutic Options John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Professor
Sleep Disorders: Assessment and Therapeutic Options John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Professor
Insomnia treatment in primary care
 Insomnia treatment in primary care Daniel J. Buysse, MD UPMC Professor of Sleep Medicine Professor of Psychiatry and Clinical and Translational Science University of Pittsburgh School of Medicine buyssedj@upmc.edu
Insomnia treatment in primary care Daniel J. Buysse, MD UPMC Professor of Sleep Medicine Professor of Psychiatry and Clinical and Translational Science University of Pittsburgh School of Medicine buyssedj@upmc.edu
INSOMNIA IN THE GERIATRIC POPULATION. Shannon Bush, MS4
 INSOMNIA IN THE GERIATRIC POPULATION Shannon Bush, MS4 CHANGES IN SLEEP ARCHITECTURE 2 Reduction in slow wave sleep (stage 3 and 4) Increase in lighter stages of sleep (stage 1 and 2) Decrease in REM sleep
INSOMNIA IN THE GERIATRIC POPULATION Shannon Bush, MS4 CHANGES IN SLEEP ARCHITECTURE 2 Reduction in slow wave sleep (stage 3 and 4) Increase in lighter stages of sleep (stage 1 and 2) Decrease in REM sleep
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Non-Benzodiazepine Insomnia Reference Number: CP.PMA_10.11.23 Effective Date: 07.16 Last Review Date: 04.18 Line of Business: Medicaid- Arizona (AHCS, CIC) Revision Log See Important Reminder
Clinical Policy: Non-Benzodiazepine Insomnia Reference Number: CP.PMA_10.11.23 Effective Date: 07.16 Last Review Date: 04.18 Line of Business: Medicaid- Arizona (AHCS, CIC) Revision Log See Important Reminder
Managing Insomnia Disorder A Review of the Research for Adults
 Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
Managing Insomnia Disorder A Review of the Research for Adults e Is This Information Right for Me? This information is right for you if: Your health care professional said you have insomnia disorder (said
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Non-Benzodiazepine Insomnia Medications Reference Number: CP.HNMC.265 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder
Clinical Policy: Non-Benzodiazepine Insomnia Medications Reference Number: CP.HNMC.265 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Non-Benzodiazepine Insomnia Medications Reference Number: CP.CPA.265 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at
Clinical Policy: Non-Benzodiazepine Insomnia Medications Reference Number: CP.CPA.265 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at
OBJECTIVES. The psychiatric, medical, and neurologic causes of sleep problems. Office-based and objective methods of evaluating sleep
 SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
SLEEP ISSUES 1 OBJECTIVES 2 Know and understand: Age-related changes in sleep The psychiatric, medical, and neurologic causes of sleep problems Office-based and objective methods of evaluating sleep Appropriate
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
SLEEP UPDATE 2008 SLEEP HYPNOGRAM. David Claman, MD UCSF Sleep Disorders Center
 SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
SLEEP UPDATE 2008 SLEEP HYPNOGRAM David Claman, MD UCSF Sleep Disorders Center Insomnia Case A 40 year old man c/o insomnia at sleep onset. He worries about sleep at night, and takes 2-3 hrs to fall asleep.
Sleep and Parkinson's Disease
 Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
Parkinson s Disease Clinic and Research Center University of California, San Francisco 505 Parnassus Ave., Rm. 795-M, Box 0114 San Francisco, CA 94143-0114 (415) 476-9276 http://pdcenter.neurology.ucsf.edu
AGING CHANGES IN SLEEP
 OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
OBJECTIVES: Understand the common age-related changes in sleep Discuss the evaluation of the older person with sleep complaints Identify sleep apnea, PLMS, RLS, and REM sleep disorders and their treatments
Modern Management of Sleep Disorders. If Only I Could Sleep Like I Did Before
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures If Only I Could Sleep Like I Did Before Sleep Case 52 yr. old WF with >4 yr. of poor sleep
Modern Management of Sleep Disorders
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Diagnosis and treatment of sleep disorders
 Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Diagnosis and treatment of sleep disorders Normal human sleep Sleep cycle occurs about every 90 minutes, approximately 4-6 cycles occur per major sleep episode NREM (70-80%) slow wave sleep heart rate,
Learning Objectives. Management of Insomnia. Impact of Chronic Insomnia. Insomnia: Definitions. Measurement of Goals. Goals of Therapy 9/29/2017
 Learning Objectives Characterize insomnia and its negative effects Management of Insomnia Discuss the goals of treatment Summarize guidelines of management of insomnia including non-pharmacologic and pharmacologic
Learning Objectives Characterize insomnia and its negative effects Management of Insomnia Discuss the goals of treatment Summarize guidelines of management of insomnia including non-pharmacologic and pharmacologic
Psychopharmacology of Sleep Disorders
 Psychopharmacology of Sleep Disorders John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Professor of Psychiatry
Psychopharmacology of Sleep Disorders John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Professor of Psychiatry
SEDATIVE-HYPNOTIC AGENTS
 SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
OUTLINE SLEEP UPDATE 2011 DISCLOSURES. David Claman, MD. Formerly on Lunesta Speakers Bureau Resigned 2011
 SLEEP UPDATE 2011 David Claman, MD Professor of Medicine UCSF Sleep Disorders Center DISCLOSURES Formerly on Lunesta Speakers Bureau Resigned 2011 Former Consultant for Provent Consulting activity was
SLEEP UPDATE 2011 David Claman, MD Professor of Medicine UCSF Sleep Disorders Center DISCLOSURES Formerly on Lunesta Speakers Bureau Resigned 2011 Former Consultant for Provent Consulting activity was
Insomnia Treatment in Brief
 Insomnia Treatment in Brief Project ECHO May 7, 2015 Jonathan Emens, M.D. Associate Professor, Departments of Psychiatry and Internal Medicine Oregon Health & Science University Staff Physician and Sleep
Insomnia Treatment in Brief Project ECHO May 7, 2015 Jonathan Emens, M.D. Associate Professor, Departments of Psychiatry and Internal Medicine Oregon Health & Science University Staff Physician and Sleep
SLEEP-WAKE DISORDERS: INSOMNIA. Prof. Paz Gía-Portilla
 SLEEP-WAKE DISORDERS: INSOMNIA Prof. Paz Gía-Portilla SLEEP-WAKE DISORDERS AND ICD-10 Chapter V: Mental and Behavioural Disorders F51. Non-organic sleep disorders Chapter VI: Nervous System Illnesses G47.
SLEEP-WAKE DISORDERS: INSOMNIA Prof. Paz Gía-Portilla SLEEP-WAKE DISORDERS AND ICD-10 Chapter V: Mental and Behavioural Disorders F51. Non-organic sleep disorders Chapter VI: Nervous System Illnesses G47.
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
How to Manage Insomnia with and without medications
 How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
How to Manage Insomnia with and without medications Tatyana Gurvich, Pharm.D. USC School of Pharmacy UC Irvine SeniorHealth Center Insomnia: How common is it? 26-50% of adult population complain of insomnia
Sleep Disorders in the Psychiatric Context
 Sleep Disorders in the Psychiatric Context John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Associate Professor
Sleep Disorders in the Psychiatric Context John W. Winkelman MD, PhD Chief, Sleep Disorders Clinical Research Program Departments of Psychiatry and Neurology Massachusetts General Hospital Associate Professor
Modern Management of Sleep Disorders. Case. Introduction. Topics Covered. Douglas C. Bauer, MD University of California, San Francisco
 Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Modern Management of Sleep Disorders Douglas C. Bauer, MD University of California, San Francisco No Disclosures Case 68 yr. old WF with >15 yr. of poor sleep Difficulty with both initiation and maintenance
Sedative Hypnotics. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.11 Subject: Sedative Hypnotics Page: 1 of 8 Last Review Date: September 15, 2016 Sedative Hypnotics
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.11 Subject: Sedative Hypnotics Page: 1 of 8 Last Review Date: September 15, 2016 Sedative Hypnotics
Sedative Hypnotics. Description
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.11 Subject: Sedative Hypnotics Page: 1 of 7 Last Review Date: December 8, 2017 Sedative Hypnotics
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.60.11 Subject: Sedative Hypnotics Page: 1 of 7 Last Review Date: December 8, 2017 Sedative Hypnotics
Treating sleep disorders
 Treating sleep disorders Sue Wilson Centre for Neuropsychopharmacology Imperial College London sue.wilson@imperial.ac.uk Suggested algorithm for treatment of insomnia Diagnosis of insomnia Associated with
Treating sleep disorders Sue Wilson Centre for Neuropsychopharmacology Imperial College London sue.wilson@imperial.ac.uk Suggested algorithm for treatment of insomnia Diagnosis of insomnia Associated with
Anxiolytic and Hypnotic drugs
 Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
Anxiolytic and Hypnotic drugs Anxiolytic and Hypnotic drugs Anxiety is unpleasant state of tension and fear that seems to arise from unknown source. The symptoms of severe anxiety are similar to those
Managing Sleep Disorders in Primary Care. Objectives. Disclosures. Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center
 Managing Sleep Disorders in Primary Care Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center www.sleeplessinidaho.com 1 Objectives 1) Identify stages and behaviors for normal
Managing Sleep Disorders in Primary Care Nancy Nadolski, FNP, MSN, M.Ed Insomnia Medicine of Idaho Boise Counseling Center www.sleeplessinidaho.com 1 Objectives 1) Identify stages and behaviors for normal
Sleep disorders. Norbert Kozak
 Sleep disorders Norbert Kozak About the sleep Each of us will spend about 1/3 of our lifetime sleeping....and 1/3 part of the population has sleep complain Sleep is an essential biological function, but
Sleep disorders Norbert Kozak About the sleep Each of us will spend about 1/3 of our lifetime sleeping....and 1/3 part of the population has sleep complain Sleep is an essential biological function, but
Index 265. Feeding bottle, 37 methods, 37
 Index 263 Index A Actigraphy delayed sleep phase syndrome, 66f Activity, 19 Adenoidectomy OSAHS, 121 Adolescents insomnia, 71 81 assessment and treatment, 76 78 etiology, 75, 76 female, 74, 75 sleep need
Index 263 Index A Actigraphy delayed sleep phase syndrome, 66f Activity, 19 Adenoidectomy OSAHS, 121 Adolescents insomnia, 71 81 assessment and treatment, 76 78 etiology, 75, 76 female, 74, 75 sleep need
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
continuing education for pharmacists
 continuing education for pharmacists General Insomnia Disorder in Adults and Treatment Guidelines Amanda R. Kriesen, R.Ph., PharmD Volume XXXV, No. 9 Dr. Amanda Kriesen has no relevant financial relationships
continuing education for pharmacists General Insomnia Disorder in Adults and Treatment Guidelines Amanda R. Kriesen, R.Ph., PharmD Volume XXXV, No. 9 Dr. Amanda Kriesen has no relevant financial relationships
INSOMNIA IN GERIATRICS. Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow
 INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER
 Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER Disclosure: Financial - none Non-Financial - none Selected Topics Sleep epidemiology Sleep
Sleep Science: better sleep for you and your patients CHUNBAI ZHANG, MD MPH UW MEDICINE VALLEY MEDICAL CENTER Disclosure: Financial - none Non-Financial - none Selected Topics Sleep epidemiology Sleep
노인병원에서 Light Therapy 의 활용 박 기 형 진주삼성병원 송도병원 신경과
 Light Therapy 1 : 15 / 63 (23.8%) 1 : 7 2 : 8 : 6 / 86 (7%) 1, : 48 / 205 (23.4%) 1 : 43 2 : 5 Sleep in Geriatrics Prevalence NIH survey of 9000 american senior above age 65 ; 88% had sleep disturbances
Light Therapy 1 : 15 / 63 (23.8%) 1 : 7 2 : 8 : 6 / 86 (7%) 1, : 48 / 205 (23.4%) 1 : 43 2 : 5 Sleep in Geriatrics Prevalence NIH survey of 9000 american senior above age 65 ; 88% had sleep disturbances
Restless Legs Syndrome: Is This a Pain Issue?
 Restless Legs Syndrome: Is This a Pain Issue? Kathy Lattavo, RN, MSN, ACNS- BC, RN-BC Objectives Describe the pathophysiology of RLS. Evaluate treatment for RLS. Compare & contrast RLS & pain. Definitions
Restless Legs Syndrome: Is This a Pain Issue? Kathy Lattavo, RN, MSN, ACNS- BC, RN-BC Objectives Describe the pathophysiology of RLS. Evaluate treatment for RLS. Compare & contrast RLS & pain. Definitions
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
Dr Alex Bartle. Medical Director Sleep Well Clinic Christchurch
 Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 8:30-9:25 WS #191: Sleep Disorders in The Elderly 9:35-10:30 WS #203: Sleep Disorders in The Elderly (Repeated) REM - Rapid Eye Movement
Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 8:30-9:25 WS #191: Sleep Disorders in The Elderly 9:35-10:30 WS #203: Sleep Disorders in The Elderly (Repeated) REM - Rapid Eye Movement
CPT David Shaha, MC US Army
 CPT David Shaha, MC US Army None Thoughts and comments are my own and do not represent the official policy of the Department of the Army, Department of Defense, or United States Government. Clinical Case
CPT David Shaha, MC US Army None Thoughts and comments are my own and do not represent the official policy of the Department of the Army, Department of Defense, or United States Government. Clinical Case
ACTIVITY DESCRIPTION Target Audience Learning Objectives
 ACTIVITY DESCRIPTION Target Audience This activity is designed to meet the needs of primary care providers, including primary care physicians, doctors of osteopathy, physician assistants, nurse practitioners,
ACTIVITY DESCRIPTION Target Audience This activity is designed to meet the needs of primary care providers, including primary care physicians, doctors of osteopathy, physician assistants, nurse practitioners,
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
Facts about Sleep. Circadian rhythms are important in determining human sleep patterns/ sleep-waking cycle
 Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Sleep Sleep is described as a state of unconsciousness or partial consciousness from which a person can be roused by stimulation Period of rest and recovery People spend about a third of their lives sleeping
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Accidents, risk of, with insufficient sleep, 318 Acquired immunodeficiency syndrome (AIDS), comorbid with narcolepsy, 298 299 Actigraphy, in
Note: Page numbers of article titles are in boldface type. A Accidents, risk of, with insufficient sleep, 318 Acquired immunodeficiency syndrome (AIDS), comorbid with narcolepsy, 298 299 Actigraphy, in
The Use of Sleep Aids in Our Society Today
 The Use of Sleep Aids in Our Society Today Kathryn Hansen, BS, CPC, CPMA, REEGT Integration Consultants, LLC Sleep Education Partners Executive Director Kentucky Sleep Society Executive Director Society
The Use of Sleep Aids in Our Society Today Kathryn Hansen, BS, CPC, CPMA, REEGT Integration Consultants, LLC Sleep Education Partners Executive Director Kentucky Sleep Society Executive Director Society
Disclosure. Sleep Medications in Primary Care: How to choose, what to avoid
 Sleep Medications in Primary Care: How to choose, what to avoid Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC, FNAP President, Fitzgerald Health Education Associates, North Andover,
Sleep Medications in Primary Care: How to choose, what to avoid Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC, FNAP President, Fitzgerald Health Education Associates, North Andover,
Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine Common Sleep Disorders
 Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine 2018 Common Sleep Disorders Objectives: Understand Understand how Sleep Disorders affects health. Describe Describe some Common Sleep Disorders.
Diana Corzine, MD ABMS Sleep Chief MT VA Sleep Medicine 2018 Common Sleep Disorders Objectives: Understand Understand how Sleep Disorders affects health. Describe Describe some Common Sleep Disorders.
Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM
 Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM Categories of Disturbance Sleep Breathing Disorders Parasomnias Sleepiness Insomnia Breathing?
Sleep Dysfunction in Multiple System Atrophy DR CALLUM DUPRE NEUROLOGY/SLEEP MEDICINE CAPITAL HEALTH SYSTEM Categories of Disturbance Sleep Breathing Disorders Parasomnias Sleepiness Insomnia Breathing?
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling
 Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling Educational Objectives: At the completion of this knowledge-based activity, participants will be able to:
Addressing the Multiple Causes and Lifestyle Impacts of Insomnia: A Guide for Patient Counseling Educational Objectives: At the completion of this knowledge-based activity, participants will be able to:
Sleep Clinic Case: History. Insomnia in Patients with Comorbid Psychiatric Disorders: Shared Neurobiology and Clinical Solutions
 Sleep Clinic Case: History Insomnia in Patients with Comorbid Psychiatric Disorders: Shared Neurobiology and Clinical Solutions David N. Neubauer, MD Associate Professor Johns Hopkins University School
Sleep Clinic Case: History Insomnia in Patients with Comorbid Psychiatric Disorders: Shared Neurobiology and Clinical Solutions David N. Neubauer, MD Associate Professor Johns Hopkins University School
Depression & Anxiety. What can I do? What are other possible treatments? What is this? Why does this happen? KEY POINTS
 Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS
 RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS Tracy Carbone, MD Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL OVERVIEW Although the
RESTLESS LEGS SYNDROME IN CHILDREN AND ADOLESCENTS Tracy Carbone, MD Medical Director of Sleep Medicine Lee Health Golisano Children s Hospital of Southwest Florida Fort Myers, FL OVERVIEW Although the
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES. SEDATIVE HYPNOTIC AGENTS Generic Brand HICL GCN Exception/Other ZOLPIDEM
 Generic Brand HICL GCN Exception/Other ZOLPIDEM AMBIEN 07842 GENERIC IS UNRESTRICTED TARTRATE AMBIEN CR EDLUAR INTERMEZZO ZOLPIMIST ESZOPICLONE LUNESTA 26791 GENERIC IS UNRESTRICTED RAMELTEON ROZEREM 33126
Generic Brand HICL GCN Exception/Other ZOLPIDEM AMBIEN 07842 GENERIC IS UNRESTRICTED TARTRATE AMBIEN CR EDLUAR INTERMEZZO ZOLPIMIST ESZOPICLONE LUNESTA 26791 GENERIC IS UNRESTRICTED RAMELTEON ROZEREM 33126
Basics of Restless Legs Syndrome (Willis-Ekbom Disease)
") Basics of Restless Legs Syndrome (Willis-Ekbom Disease) Michael H. Silber, M.B.Ch.B. Professor of Neurology Mayo Clinic College of Medicine Objectives Understand how RLS is diagnosed Understand what we
Basics of Restless Legs Syndrome (Willis-Ekbom Disease) Michael H. Silber, M.B.Ch.B. Professor of Neurology Mayo Clinic College of Medicine Objectives Understand how RLS is diagnosed Understand what we
3/24/2016 DISCLOSURE STATEMENT PHARMACIST OBJECTIVES OVERVIEW TECHNICIAN OBJECTIVES PREVALENCE OF INSOMNIA THE WRONG SIDE OF THE BED: CHRONIC INSOMNIA
 DISCLOSURE STATEMENT I do not have any actual or potential conflict of interest in relation to this presentation THE WRONG SIDE OF THE BED: CHRONIC INSOMNIA DANIELLE ROWAN, PHARMD, MBA PGY1 PHARMACY PRACTICE
DISCLOSURE STATEMENT I do not have any actual or potential conflict of interest in relation to this presentation THE WRONG SIDE OF THE BED: CHRONIC INSOMNIA DANIELLE ROWAN, PHARMD, MBA PGY1 PHARMACY PRACTICE
Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles
 Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles Sleep Disorders Restless Legs Syndrome (RLS) and Periodic Limb Movement Disorder (PLMD) Sleep
Earl J. Soileau, MD, FSAHM Asst Professor, Family Medicine LSU HSC Medical School New Orleans at Lake Charles Sleep Disorders Restless Legs Syndrome (RLS) and Periodic Limb Movement Disorder (PLMD) Sleep
Disclosure. Sleep Medications in Primary Care: How to choose, what to avoid
 Sleep Medications in Primary Care: How to choose, what to avoid Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC, FNAP President, Fitzgerald Health Education Associates, North Andover,
Sleep Medications in Primary Care: How to choose, what to avoid Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC, FNAP President, Fitzgerald Health Education Associates, North Andover,
Insomnia Pearls in the Geriatric Population
 Insomnia Pearls in the Geriatric Population September 9, 2016 Stephanie Loegering, PharmD, CGP Clinical Pharmacist VA Medical Center Thank You MPhA Wi-fi Information: NETWORK: EC-CTR PASSWORD: westgate252
Insomnia Pearls in the Geriatric Population September 9, 2016 Stephanie Loegering, PharmD, CGP Clinical Pharmacist VA Medical Center Thank You MPhA Wi-fi Information: NETWORK: EC-CTR PASSWORD: westgate252
Sleep in the Patient with Diabetes
 Sleep in the Patient with Diabetes ANDREA RINN, DO SEPTEMBER, 2017 Learning Objectives 1. Recognize the correlation between sleep apnea and diabetes 2. Review potential relationships between sleep and
Sleep in the Patient with Diabetes ANDREA RINN, DO SEPTEMBER, 2017 Learning Objectives 1. Recognize the correlation between sleep apnea and diabetes 2. Review potential relationships between sleep and
Treatment of sleep disorders in
 Treatment of sleep disorders in Parkinson s s disease (PD) K. Ray Chaudhuri London, UK GPSRC CNS 176 0709 RTG 1 Managing insomnia in PD Onset/initiation Adjustment of anti-pd treatment Sleep hygiene Hypnotics
Treatment of sleep disorders in Parkinson s s disease (PD) K. Ray Chaudhuri London, UK GPSRC CNS 176 0709 RTG 1 Managing insomnia in PD Onset/initiation Adjustment of anti-pd treatment Sleep hygiene Hypnotics
Insomnia. St. Joseph s Annual Family Practice Refresher March 1, Robert J. Ostrander, M.D
 St. Joseph s Annual Family Practice Refresher March 1, 2018 Robert J. Ostrander, M.D If in bed I say, When shall I arise? then the night drags on; I am filled with restlessness until the dawn. Job 7:4
St. Joseph s Annual Family Practice Refresher March 1, 2018 Robert J. Ostrander, M.D If in bed I say, When shall I arise? then the night drags on; I am filled with restlessness until the dawn. Job 7:4
What is sleep? o Sleep is a body s rest cycle.
 What is sleep? o Sleep is a state when our senses and motor actvity are relatively suspended; there is a total or partial unconsciousness and all voluntary muscles are inactive. o Sleep is a body s rest
What is sleep? o Sleep is a state when our senses and motor actvity are relatively suspended; there is a total or partial unconsciousness and all voluntary muscles are inactive. o Sleep is a body s rest
Disclosure. Sleep Medications in Primary Care
 Sleep Medications in Primary Care Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC, FNAP President, Fitzgerald Health Education Associates, North Andover, MA Family Nurse Practitioner,
Sleep Medications in Primary Care Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC, FNAP President, Fitzgerald Health Education Associates, North Andover, MA Family Nurse Practitioner,
Ambien vs Rozerem There are people out there who have trouble falling asleep at night. Â Often, this would be considered as a disease that
 22-10-2013 Ambien vs Rozerem There are people out there who have trouble falling asleep at night. Â Often, this would be considered as a disease that can be treated with Ambien vs Rozerem. Ambien:. Ramelteon
22-10-2013 Ambien vs Rozerem There are people out there who have trouble falling asleep at night. Â Often, this would be considered as a disease that can be treated with Ambien vs Rozerem. Ambien:. Ramelteon
Overview of Sleep Medicine
 Overview of Sleep Medicine Rodney Smith. New York Times 11-18-2007 James E. Mojica, MD, FAASM Pulmonary, Sleep, Critical Care Massachusetts General Hospital Sleep Reversible state Perceptual disengagement
Overview of Sleep Medicine Rodney Smith. New York Times 11-18-2007 James E. Mojica, MD, FAASM Pulmonary, Sleep, Critical Care Massachusetts General Hospital Sleep Reversible state Perceptual disengagement
Anjali Ahn, MD Beth Israel Deaconess Medical Center May 1, 2015
 Anjali Ahn, MD Beth Israel Deaconess Medical Center aahn1@bidmc.harvard.edu May 1, 2015 Ms G. is a 50yo female Boston police officer presents with chief complaint: I ve never been a good sleeper! Where
Anjali Ahn, MD Beth Israel Deaconess Medical Center aahn1@bidmc.harvard.edu May 1, 2015 Ms G. is a 50yo female Boston police officer presents with chief complaint: I ve never been a good sleeper! Where
You May Be at Risk. You are taking one of the following sedative-hypnotic medications: Diazepam (Valium ) Estazolam. Flurazepam.
 Estazolam. Flurazepam.") You May Be at Risk You are taking one of the following sedative-hypnotic medications: Alprazolam (Xanax ) Diazepam (Valium ) Temazepam (Restoril ) Chlorazepate Estazolam Triazolam (Halcion ) Chlordiazepoxide
You May Be at Risk You are taking one of the following sedative-hypnotic medications: Alprazolam (Xanax ) Diazepam (Valium ) Temazepam (Restoril ) Chlorazepate Estazolam Triazolam (Halcion ) Chlordiazepoxide
Treating Insomnia in Primary Care. Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team
 Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
INTRINSIC SLEEP DISORDERS. Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include:
 is a common complaint. Causes of EDS are numerous and include:") INTRINSIC SLEEP DISORDERS Introduction Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include: Intrinsic sleep disorders (e.g. narcolepsy, obstructive sleep apnoea/hypopnea
INTRINSIC SLEEP DISORDERS Introduction Excessive daytime sleepiness (EDS) is a common complaint. Causes of EDS are numerous and include: Intrinsic sleep disorders (e.g. narcolepsy, obstructive sleep apnoea/hypopnea
Sleep Problems in the Elderly
 Emerging Challenges in Primary Care: 2017 Sleep Problems in the Elderly To Sleep, Perchance to Dream Ay There s The Rub MACBETH 1 Faculty Thomas Weiss, MD Researcher and Principle Investigator in Psychiatry
Emerging Challenges in Primary Care: 2017 Sleep Problems in the Elderly To Sleep, Perchance to Dream Ay There s The Rub MACBETH 1 Faculty Thomas Weiss, MD Researcher and Principle Investigator in Psychiatry
Ruby Williams, M.D. Drugs, Alcohol and Sleep February 24, 2018
 Ruby Williams, M.D. Drugs, Alcohol and Sleep February 24, 2018 Objectives Describe pharmacology of commonly prescribed drugs for stimulants and hypnotics Brief review of common drugs that affect sleep
Ruby Williams, M.D. Drugs, Alcohol and Sleep February 24, 2018 Objectives Describe pharmacology of commonly prescribed drugs for stimulants and hypnotics Brief review of common drugs that affect sleep
Sleep and Insomnia 2/8/2018. Presented by. Marie Rataj, MSN, APRN, ANP. Objectives. Everything you wanted to know
 Sleep and Insomnia Everything you wanted to know Presented by Marie Rataj, MSN, APRN, ANP Objectives Develop a basic knowledge of normal sleep and differentiate from abnormal sleep Develop basic understanding
Sleep and Insomnia Everything you wanted to know Presented by Marie Rataj, MSN, APRN, ANP Objectives Develop a basic knowledge of normal sleep and differentiate from abnormal sleep Develop basic understanding
Dr Alex Bartle. Sleep Well Clinic
 Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Insomnia: habits, help, and hazards
 Insomnia: habits, help, and hazards Balanced data about medications www.rxfacts.org Copyright 2010 by The Alosa Foundation www.rxfacts.org November 2010 2 www.rxfacts.org Author: Leslie Jackowski, B.Sc.,
Insomnia: habits, help, and hazards Balanced data about medications www.rxfacts.org Copyright 2010 by The Alosa Foundation www.rxfacts.org November 2010 2 www.rxfacts.org Author: Leslie Jackowski, B.Sc.,
Insomnia. Dr Terri Henderson MBChB FCPsych
 Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
A Review of Sleep Disorders in Cancer Patients: Finding the Dream Treatment
 A Review of Sleep Disorders in Cancer Patients: Finding the Dream Treatment Jordan Pleskow, PharmD Roswell Park Cancer Institute Oncology Symposium 11/11/17 Objectives Evaluate the issues with sleep in
A Review of Sleep Disorders in Cancer Patients: Finding the Dream Treatment Jordan Pleskow, PharmD Roswell Park Cancer Institute Oncology Symposium 11/11/17 Objectives Evaluate the issues with sleep in
Case 1. A. Insomnia B. Restless leg syndrome C. Peripheral neuropathy D. Osteoarthritis of the hip. Disclosures. Diagnosis for trouble falling asleep
 Disclosures I have no disclosures Case 1 Liza Ashbrook, MD Assistant Clinical Professor UCSF Department of Neurology History of Present Illness Diagnosis for trouble falling asleep 70-year-man with obstructive
Disclosures I have no disclosures Case 1 Liza Ashbrook, MD Assistant Clinical Professor UCSF Department of Neurology History of Present Illness Diagnosis for trouble falling asleep 70-year-man with obstructive
9/13/17. Emerging Challenges in Primary Care: Sleep Problems in the Elderly. Faculty. Disclosures
 Emerging Challenges in Primary Care: 2017 Sleep Problems in the Elderly To Sleep, Perchance to Dream Ay There s The Rub MACBETH 1 Faculty Thomas Weiss, MD Researcher and Principle Investigator in Psychiatry
Emerging Challenges in Primary Care: 2017 Sleep Problems in the Elderly To Sleep, Perchance to Dream Ay There s The Rub MACBETH 1 Faculty Thomas Weiss, MD Researcher and Principle Investigator in Psychiatry
Insomnia % of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences)
") 10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
Overview of Sleep Medicine
 Overview of Sleep Medicine Rodney Smith. New York Times 11-18-2007 James E. Mojica, MD, FAASM Pulmonary, Sleep, Critical Care Massachusetts General Hospital What is Sleep? Reversible state Perceptual disengagement
Overview of Sleep Medicine Rodney Smith. New York Times 11-18-2007 James E. Mojica, MD, FAASM Pulmonary, Sleep, Critical Care Massachusetts General Hospital What is Sleep? Reversible state Perceptual disengagement
Pharmacy Benefit Determination Policy
 Policy Subject: CNS Stimulant Medications Policy Number: SHS PBD06 Category: CNS Drugs Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS ASO PPO Individual
Policy Subject: CNS Stimulant Medications Policy Number: SHS PBD06 Category: CNS Drugs Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS ASO PPO Individual
Pharmacy Medical Necessity Guidelines: Insomnia Treatments
 Pharmacy Medical Necessity Guidelines: Effective: January 1, 2019 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED) Benefit
Pharmacy Medical Necessity Guidelines: Effective: January 1, 2019 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical Review Pharmacy (RX) or Medical (MED) Benefit
Comparison of Insomnia Treatments
 PL Detail-Document #280504 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER May 2012 Comparison of Insomnia
PL Detail-Document #280504 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER May 2012 Comparison of Insomnia