Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
|
|
|
- Gilbert Carroll
- 5 years ago
- Views:
Transcription
1 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim
2 Content Definition Classification Weaning criteria Weaning methods Criteria for extubation
3 Introduction Weaning comprises 40% of the duration of mechanical ventilation 20% to 30% of patients are difficult to wean from invasive mechanical ventilation. Undue delay leads to excess stay, iatrogenic lung injury, unnecessary sedation, and even higher mortality
4 Stages of Mechanical Ventilation 2 EUROPEAN RESPIRATORY JOURNAL
5 Definition Weaning can be considered once the underlying process necessitating mechanical ventilation is resolving Weaning is the process of liberation from, or discontinuation of mechanical ventilatory support ( weaning per se is not always required, liberation may be a better term!) American Journal of respiratory and Critical care
6
7 Classification Simple Weaning ventilator discontinued after the first assessment Difficult Weaning ventilator discontinued from 2 7d after initial assessment Prolonged Weaning ventilator discontinued in >7d after initial assessment RESPIRATORY CARE OCTOBER 2012 VOL 57 NO 10

8 CAUSE OF DIFFICULT WEANING ICU Protocol 2012

9 ICU Protocol 2012

10 ICU Protocol 2012





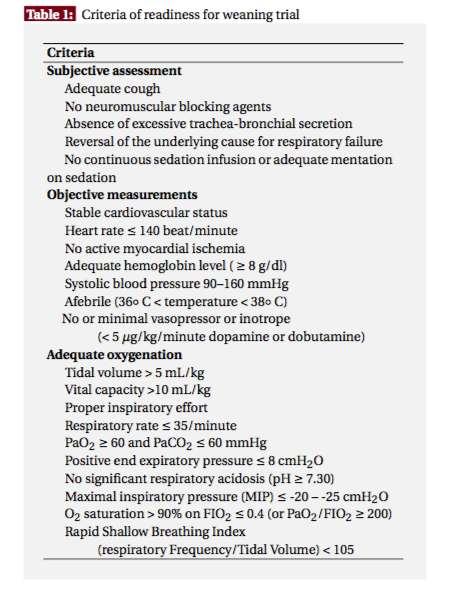
11 CLINICAL CRITERIA PULMONARY CRITERIA WEANING CRITERIA VENTILATORY CRITERIA PULMONARY RESERVE OXYGENATION CRITERIA
12 Assessment for weaning Clinical Criteria Evidence for some reversal of the underlying cause for respiratory failure Adequate oxygenation and ph Hemodynamic stability The capability to initiate an inspiratory effort 12
13 VENTILATORY CRITERIA PaCO2 Spontaneous Tidal Volume Spontaneous Frequency Minute Ventilation
14 PaCO2 PaCO2 is a reliable indicator for weaning Weaning can be attempted when PaCO2 is less than 50mmhg Patients with COAD, the acceptable PaCO2 may be slightly higher and the ph slightly lower, depending on the patient s baseline normal values prior to mechanical ventilation
15 Spontaneous Frequency The spontaneous frequency should be less than 35/min while the corresponding PaCO2 should be less than 50 mm Hg. A frequency of greater than 35/min is associated with rapid shallow breathing. This breathing pattern increases dead space ventilation and is highly ineffective for gas exchange during spontaneous breathing.
16 Oxygenation Criteria PaO2 and SaO2 PaO2/FIO2
17 Accepted oxygenation weaning criteria include a PaO2 of greater than 60 mm Hg (or SaO2. 90%) on an FIO2 of 0.40 or less.. A PaO2/FIO2 of > mm Hg suggests acceptable physiologic shunt and compatible to successful weaning trial.

18 Pulmonary Reserve Vital Capacity Maximum Inspiratory Pressure P100

19 PULMONARY RESERVE VC measures the maximum amount of lung volume that the patient can exhale following maximal inspiration.
20 Maximum Inspiratory Pressure The maximum inspiratory pressure (also called negative inspiratory force) is the amount of negative pressure that the patient can generate when inspiring against an occluded measuring device The MIP is considered a measure of ventilatory muscle strength, and weaning will likely be successful if the patient can generate an MIP of at least -20 cmh2o
21 P100 or P0.1 The P100 is the most negative pressure that the patient can generate against a closed system during the first one hundred miliseconds of a spontaneous effort. P100 can be used as an indicator of the level of central respiratory drive. Value of less than 2 cm h2o in normal subjects.
22 Pulmonary Measurements Static Compliance Airway Resistance
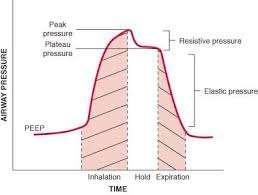
23 Static Compliance The static lung compliance is measured by dividing the patient s tidal volume by the difference in the plateau pressure and the PEEP. The lower the compliance, the greater the work of breathing. The minimal compliance value consistent with successful weaning is 30 ml/cm H2O or greater.
24
25 Airway Resistance The airway resistance can be estimated by dividing the difference in the peak inspiratory pressure and the plateau pressure (H2O) by the constant inspiratory flow (L/sec). The normal range for airway resistance is cm H2O/L/sec and higher for ventilated patients because of the associated pathological conditions (e.g., bronchospasm) and tubing resistance
26
27
28 Therapeutic measures to enhance weaning progress
29 Weaning Methods
30 Spontaneous Breathing Trial SBT can be conducted while the patient connected to a ventilator circuit or Allow breathing through an independent source of oxygen via a T piece. 1. SBT through Ventilator: Use PSV. PS 5-7 cm h20 plus low PEEP(5cmh20) 2. SBT through T-piece- deliver oxygen enriched gas at high flow rates. RESPIRATORY CARE OCTOBER 2012 VOL 57 NO 10
31 Frequency of Tolerating an SBT in Selected Patients and Rate of Permanent Ventilator Discontinuation Following a Successful SBT*
32 ICU Protocol 2012
33 Anaesthesia, Critical Care & Pain Volume 5 Number

34 ICU Protocol 2012
35 Rapid Shallow Breathing Index (RSBI) Failure of weaning may be related to the development of a spontaneous breathing pattern that is rapid (high frequency) and shallow (low tidal volume). Rapid shallow breathing is quantified as the f (number of breaths per minute) divided by the VT in liters. When the RSBI or f/vt index is greater than 100 breaths/min/l, it correlates with weaning failure. RESPIRATORY CARE OCTOBER 2012 VOL 57 NO 10
36 Mechanical Ventilation Rest 24 hrs PaO2/FiO2 200 mm Hg PEEP 5 cm H2O Intact airway reflexes No need for continuous infusions of vasopressors or inotrops RSBI > 100 Stable Support Strategy Assisted/PSV 24 hours <100 Daily SBT min Low level CPAP (5 cm H2O), Low levels of pressure support (5 to 7 cm H2O) T-piece breathing Yes RR > 35/min Spo2 < 90% HR > 140/min Sustained 20% increase in HR SBP > 180 mm Hg, DBP > 90 mm Hg Anxiety Diaphoresis No Extubation
37 Weaning Failure Weaning failure is defined as the failure to pass a spontaneousbreathing trial or the need for reintubation within 48 hours following extubation. Predicting success is important to reduce rates of reintubation. RESPIRATORY CARE OCTOBER 2012 VOL 57 NO 10

38 Anaesthesia, Critical Care & Pain Volume 5 Number
39 Weaning failure Reintubation is associated with a 7-11x increase in hospital mortality. Reintubation rates of 5% to 20% are acceptable for most well-run ICUs (a target of 0% is unrealistic and would lead to prolonged ventilation) RESPIRATORY CARE OCTOBER 2012 VOL 57 NO

40 A-Airway/Lung compliance B- Brain Dysfunction C- Cardiovascular D-Drugs/diaphragm E-Electrolytes/endocrine
41 SBT Failure Correct reversible causes for failure adequacy of pain control the appropriateness of sedation fluid status bronchodilator needs the control of myocardial ischemia, and the presence of other disease processes Subsequent SBTs should be performed every 24 H RESPIRATORY CARE OCTOBER 2012 VOL 57 NO
42 SBT failure Left Heart Failure: Increased metabolic demands Increases in venous return and pulmonary edema Appropriate management of cardiovascular status is necessary before weaning will be successful RESPIRATORY CARE OCTOBER 2012 VOL 57 NO
43 Extubation Criteria Ability to protect upper airway Effective cough Alertness
44 Improving clinical condition Adequate lumen of trachea and larynx Leak test to identify patients who are at risk for postextubation stridor RESPIRATORY CARE OCTOBER 2012 VOL 57 NO
45 Cuff Leak Test in MV Set a tidal Volume ml/kg Measure the expired tidal volume Deflated the cuff Remeasure expired tidal volume (average of 4-6 breaths) RESPIRATORY CARE OCTOBER 2012 VOL 57 NO
46 The difference in the tidal volumes with the cuff inflated and deflated is the leak A value of 130ml 85% sensitivity 95% specificity RESPIRATORY CARE OCTOBER 2012 VOL 57 NO
47 Cough / Leak test in spontaneous breathing Tracheal cuff is deflated and monitored for the first 30 seconds for cough. Only cough associated with respiratory gurgling (heard without a stethoscope and related to secretions) is taken into account. RESPIRATORY CARE OCTOBER 2012 VOL 57 NO
48 The risk of post extubation upper airway obstruction increases with the duration of mechanical ventilation female gender trauma repeated or traumatic intubation RESPIRATORY CARE OCTOBER 2012 VOL 57 NO
49 Weaning a tracheostomised patient ICU Protocol 2012
50 Conclusion Weaning is an essential component in mechanical ventilation. Patients receiving ventilatory support should be assessed on a daily basis for their suitability for weaning. Consider weaning if, the gas exchange is adequate with low PEEP/FIO2 requirements,hemodynamics are stable without a need for pressors, and capable to initiate spontaneous breaths Resolve causes of weaning failure to avoid prolonged ventilation.
51
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Weaning: The key questions
 Weaning from mechanical ventilation Weaning / Extubation failure: Is it a real problem in the PICU? Reported extubation failure rates in PICUs range from 4.1% to 19% Baisch SD, Wheeler WB, Kurachek SC,
Weaning from mechanical ventilation Weaning / Extubation failure: Is it a real problem in the PICU? Reported extubation failure rates in PICUs range from 4.1% to 19% Baisch SD, Wheeler WB, Kurachek SC,
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Difficult weaning from mechanical ventilation
 Difficult weaning from mechanical ventilation Paolo Biban, MD Director, Neonatal and Paediatric Intensive Care Unit Division of Paediatrics, Major City Hospital Azienda Ospedaliera Universitaria Integrata
Difficult weaning from mechanical ventilation Paolo Biban, MD Director, Neonatal and Paediatric Intensive Care Unit Division of Paediatrics, Major City Hospital Azienda Ospedaliera Universitaria Integrata
17400 Medina Road, Suite 100 Phone: Minneapolis, MN Fax:
 17400 Medina Road, Suite 100 Phone: 763-398-8300 Minneapolis, MN 55447-1341 Fax: 763-398-8400 www.pulmonetic.com Clinical Bulletin To: Cc: From: Domestic Sales Representatives and International Distributors
17400 Medina Road, Suite 100 Phone: 763-398-8300 Minneapolis, MN 55447-1341 Fax: 763-398-8400 www.pulmonetic.com Clinical Bulletin To: Cc: From: Domestic Sales Representatives and International Distributors
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Spontaneous Breathing Trial and Mechanical Ventilation Weaning Process
 Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Although the literature reports that approximately. off a ventilator
 Taking your patient off a ventilator Although the literature reports that approximately 33% of patients in the ICU require mechanical ventilation (MV),! the figure is closer to 90% for the critically SONIA
Taking your patient off a ventilator Although the literature reports that approximately 33% of patients in the ICU require mechanical ventilation (MV),! the figure is closer to 90% for the critically SONIA
MECHANICAL VENTILATION PROTOCOLS
 GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Recovery from ICU-acquired weakness; do not forget the respiratory muscles!
 Recovery from ICU-acquired weakness; do not forget the respiratory muscles! Beatrix Clerckx Department of Rehabilitation Sciences, Department of Intensive Care Medicine, University Hospitals Leuven, Catholic
Recovery from ICU-acquired weakness; do not forget the respiratory muscles! Beatrix Clerckx Department of Rehabilitation Sciences, Department of Intensive Care Medicine, University Hospitals Leuven, Catholic
You are caring for a patient who is intubated and. pressure control ventilation. The ventilator. up to see these scalars
 Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Test yourself Test yourself #1 You are caring for a patient who is intubated and ventilated on pressure control ventilation. The ventilator alarms and you look up to see these scalars What is the most
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
Weaning from Mechanical Ventilation
 CHAPTER 47 Victor Kim and Gerard J. Criner Weaning from Mechanical Ventilation CHAPTER OUTLINE Learning Objectives Case Study Determining the Cause of Respiratory Failure When is the Patient Ready to Wean?
CHAPTER 47 Victor Kim and Gerard J. Criner Weaning from Mechanical Ventilation CHAPTER OUTLINE Learning Objectives Case Study Determining the Cause of Respiratory Failure When is the Patient Ready to Wean?
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Definitions. Definitions. Weaning. Weaning. Disconnection (Discontinuation) Weaning
 Weaning") Definitions 2 Disconnection (Discontinuation) Implies patient no longer needs that form of therapy 80% of patients requiring temporary MVS do not require weaning Definitions 3 Implies some need for MVS
Definitions 2 Disconnection (Discontinuation) Implies patient no longer needs that form of therapy 80% of patients requiring temporary MVS do not require weaning Definitions 3 Implies some need for MVS
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
RESPIRATORY COMPLICATIONS AFTER SCI
 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA 30309-1465 404-352-2020 DISCLOSURE STATEMENT I have no
Home Mechanical Ventilation. Anthony Bateman
 Home Mechanical Ventilation Anthony Bateman What is Long Term Ventilation? LTV is the provision of respiratory support to individuals with non-acute respiratory failure Progression of expected disease
Home Mechanical Ventilation Anthony Bateman What is Long Term Ventilation? LTV is the provision of respiratory support to individuals with non-acute respiratory failure Progression of expected disease
Basics of NIV. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Potential Conflicts of Interest
 Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
WEANING FROM MECHANICAL VENTILATION. Dr MEGHA JAIN. University College of Medical Sciences & GTB Hospital, Delhi
 WEANING FROM MECHANICAL VENTILATION Dr MEGHA JAIN University College of Medical Sciences & GTB Hospital, Delhi HEADINGS Purpose of weaning and extubation. Rationale of predictive indices in weaning. Application
WEANING FROM MECHANICAL VENTILATION Dr MEGHA JAIN University College of Medical Sciences & GTB Hospital, Delhi HEADINGS Purpose of weaning and extubation. Rationale of predictive indices in weaning. Application
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
STATE OF OKLAHOMA 2014 EMERGENCY MEDICAL SERVICES PROTOCOLS
 3K NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ADULT EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC Indications: 1. Dyspnea Uncertain Etiology Adult. 2. Dyspnea Asthma Adult. 3. Dyspnea Chronic
3K NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ADULT EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC Indications: 1. Dyspnea Uncertain Etiology Adult. 2. Dyspnea Asthma Adult. 3. Dyspnea Chronic
Caring Practice: Evidence-based Terminal Ventilator Withdrawal
 1 Caring Practice: Evidence-based Terminal Ventilator Withdrawal Margaret L Campbell PhD, RN, FPCN 2 Webinar Goals Describe the processes for ensuring patient comfort during terminal ventilator withdrawal
1 Caring Practice: Evidence-based Terminal Ventilator Withdrawal Margaret L Campbell PhD, RN, FPCN 2 Webinar Goals Describe the processes for ensuring patient comfort during terminal ventilator withdrawal
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Weaning: Neuro Ventilatory Efficiency
 Weaning: Neuro Ventilatory Efficiency Christer Sinderby Department of Critical Care Keenan Research Center at the Li Ka Shing Knowledge Institute of St. Michael's Hospital Faculty of Medicine, University
Weaning: Neuro Ventilatory Efficiency Christer Sinderby Department of Critical Care Keenan Research Center at the Li Ka Shing Knowledge Institute of St. Michael's Hospital Faculty of Medicine, University
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
New Modes and New Concepts In Mechanical Ventilation
 New Modes and New Concepts In Mechanical Ventilation Prof Department of Anesthesia and Surgical Intensive Care Cairo University 1 2 New Ventilation Modes Dual Control Within-a-breath switches from PC to
New Modes and New Concepts In Mechanical Ventilation Prof Department of Anesthesia and Surgical Intensive Care Cairo University 1 2 New Ventilation Modes Dual Control Within-a-breath switches from PC to
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders
![Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders](/thumbs/83/87321224.jpg "Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders") Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล
 Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning
 CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
SESSION 3 OXYGEN THERAPY
 SESSION 3 OXYGEN THERAPY Harith Eranga Yapa Department of Nursing Faculty of Health Sciences The Open University of Sri Lanka 1 Outline Methods of delivery Complications of oxygen therapy Artificial airways
SESSION 3 OXYGEN THERAPY Harith Eranga Yapa Department of Nursing Faculty of Health Sciences The Open University of Sri Lanka 1 Outline Methods of delivery Complications of oxygen therapy Artificial airways
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE
 European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section ESICM Trial Group WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE Data Collection
European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section ESICM Trial Group WorldwidE AssessmeNt of Separation of patients From ventilatory assistance WEAN SAFE Data Collection
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Weaning from mechanical ventilation
 Weaning from mechanical ventilation Jeremy Lermitte BM FRCA Mark J Garfield MB ChB FRCA Mechanical ventilation has gone through a dramatic evolution over a relatively short space of time. After the Copenhagen
Weaning from mechanical ventilation Jeremy Lermitte BM FRCA Mark J Garfield MB ChB FRCA Mechanical ventilation has gone through a dramatic evolution over a relatively short space of time. After the Copenhagen
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
An introduction to mechanical ventilation. Fran O Higgins, Adrian Clarke Correspondence
 Update in Anaesthesia An introduction to mechanical ventilation Respiratory Summary Mechanical ventilation is the major invasive intervention offered in the ICU. In low income countries, where the facilities
Update in Anaesthesia An introduction to mechanical ventilation Respiratory Summary Mechanical ventilation is the major invasive intervention offered in the ICU. In low income countries, where the facilities
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section WEAN SAFE. Data Collection Forms
 Acute Respiratory Failure Section WEAN SAFE. Data Collection Forms") European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section WEAN SAFE Data Collection Forms Study ID: Date of Data collection: FORM 0: - ORGANIZATIONAL DATA OF THE PARTICIPATING
European Society of Intensive Care Medicine (ESICM) Acute Respiratory Failure Section WEAN SAFE Data Collection Forms Study ID: Date of Data collection: FORM 0: - ORGANIZATIONAL DATA OF THE PARTICIPATING
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
UCH WEANING FROM MECHANICAL VENTILATION PATHWAY
 UCH WEANING FROM MECHANICAL VENTILATION PATHWAY WAKE WARM AND WEAN. POST OPERATIVE PATIENTS WHO HAVE BEEN VENTILATED < 24 HOURS DAILY EXTUBATION SCREEN A DAILY SCREEN TO BE CARRIED OUT ON ALL PATIENTS
UCH WEANING FROM MECHANICAL VENTILATION PATHWAY WAKE WARM AND WEAN. POST OPERATIVE PATIENTS WHO HAVE BEEN VENTILATED < 24 HOURS DAILY EXTUBATION SCREEN A DAILY SCREEN TO BE CARRIED OUT ON ALL PATIENTS
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
IMPLEMENTATION AT THE BEDSIDE
 CLINICAL EVIDENCE GUIDE IMPLEMENTATION AT THE BEDSIDE Puritan Bennett PAV+ Software Utilization of the PAV+ software has been demonstrated to reduce asynchrony and improve respiratory mechanics. 2 Yet,
CLINICAL EVIDENCE GUIDE IMPLEMENTATION AT THE BEDSIDE Puritan Bennett PAV+ Software Utilization of the PAV+ software has been demonstrated to reduce asynchrony and improve respiratory mechanics. 2 Yet,
Diagnosis and Management of Acute Respiratory Failure
 Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
New York Science Journal 2017;10(5)
") Value of Automatic Tube Compensation during Weaning of Mechanically Ventilated Patient in Medical Intensive Care Unit Mohamed Abouzeid. 1, Ahmed E. Kabil. 2, Ahmed Al-Ashkar 1 and Hafez A. Abdel-Hafeez
Value of Automatic Tube Compensation during Weaning of Mechanically Ventilated Patient in Medical Intensive Care Unit Mohamed Abouzeid. 1, Ahmed E. Kabil. 2, Ahmed Al-Ashkar 1 and Hafez A. Abdel-Hafeez
Slide 1. Slide 2. Slide 3 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Objectives: I have nothing to disclose.
 Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital
 Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital Objectives Upon completion of this module, the learner will be able to: Identify types of airways and indications
Module 4: Understanding MechanicalVentilation Jennifer Zanni, PT, DScPT Johns Hopkins Hospital Objectives Upon completion of this module, the learner will be able to: Identify types of airways and indications
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
How to optimize timing of extubation? Andrew JE Seely MD, PhD, FRCSC
 How to optimize timing of extubation? Andrew JE Seely MD, PhD, FRCSC Disclosure Therapeutic Monitoring Systems (TMS) Founder and Chief Science Officer TMS Aim: improve patient care through innovative variability-derived
How to optimize timing of extubation? Andrew JE Seely MD, PhD, FRCSC Disclosure Therapeutic Monitoring Systems (TMS) Founder and Chief Science Officer TMS Aim: improve patient care through innovative variability-derived
Weaning from mechanical ventilation in 21 st century
 1 Weaning from mechanical ventilation in 21 st century Dr. P.K.Dash. Additional Professor in Anaesthesiology Sree Chitra Tirunal Institute for Medical Sciences ant Technology Trivandrum 695011 Kerala Mechanical
1 Weaning from mechanical ventilation in 21 st century Dr. P.K.Dash. Additional Professor in Anaesthesiology Sree Chitra Tirunal Institute for Medical Sciences ant Technology Trivandrum 695011 Kerala Mechanical
Approach to the Use of the Mechanical Ventilator
 7 MECHANICAL VENTILATION Matthew J. Sena, M.D., and Avery B. Nathens, M.D., Ph.D., M.P.H., F.A.C.S. 7 MECHANICAL VENTILATION 1 Approach to the Use of the Mechanical Ventilator Patients requiring mechanical
7 MECHANICAL VENTILATION Matthew J. Sena, M.D., and Avery B. Nathens, M.D., Ph.D., M.P.H., F.A.C.S. 7 MECHANICAL VENTILATION 1 Approach to the Use of the Mechanical Ventilator Patients requiring mechanical
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Weaning and Extubation in Pediatrics
 68 Current Respiratory Medicine Reviews, 2012, 8, 68-78 Weaning and Extubation in Pediatrics Cíntia Johnston *,1 and Paulo Sérgio Lucas da Silva 2 1 Pediatric Intensive Care Unit, Department of Pediatrics,
68 Current Respiratory Medicine Reviews, 2012, 8, 68-78 Weaning and Extubation in Pediatrics Cíntia Johnston *,1 and Paulo Sérgio Lucas da Silva 2 1 Pediatric Intensive Care Unit, Department of Pediatrics,
High Flow Humidification Therapy, Updates.
 High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP
 with BiPAP Device/Nasal CPAP") I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP II. Policy: PSV with BiPAP device/nasal CPAP will be initiated upon a physician's order by Respiratory Therapy personnel trained
I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP II. Policy: PSV with BiPAP device/nasal CPAP will be initiated upon a physician's order by Respiratory Therapy personnel trained
Response of Mechanically Ventilated Respiratory Failure Patients to Respiratory Muscles Training
 Med. J. Cairo Univ., Vol. 82, No. 1, March: 19-24, 2014 www.medicaljournalofcairouniversity.net Response of Mechanically Ventilated Respiratory Failure Patients to Respiratory Muscles Training AMANY R.
Med. J. Cairo Univ., Vol. 82, No. 1, March: 19-24, 2014 www.medicaljournalofcairouniversity.net Response of Mechanically Ventilated Respiratory Failure Patients to Respiratory Muscles Training AMANY R.
Ventilator Dyssynchrony - Recognition, implications, and management
 Ventilator Dyssynchrony - Recognition, implications, and management Gavin M Joynt Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong Dyssynchrony Uncoupling of mechanical delivered
Ventilator Dyssynchrony - Recognition, implications, and management Gavin M Joynt Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong Dyssynchrony Uncoupling of mechanical delivered
Supplementary Online Content 2
 Supplementary Online Content 2 van Meenen DMP, van der Hoeven SM, Binnekade JM, et al. Effect of on demand vs routine nebulization of acetylcysteine with salbutamol on ventilator-free days in intensive
Supplementary Online Content 2 van Meenen DMP, van der Hoeven SM, Binnekade JM, et al. Effect of on demand vs routine nebulization of acetylcysteine with salbutamol on ventilator-free days in intensive
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
COBIS Management of airway burns and inhalation injury PAEDIATRIC
 COBIS Management of airway burns and inhalation injury PAEDIATRIC 1 A multidisciplinary team should provide the management of the child with inhalation injury. Childhood inhalation injury mandates transfer
COBIS Management of airway burns and inhalation injury PAEDIATRIC 1 A multidisciplinary team should provide the management of the child with inhalation injury. Childhood inhalation injury mandates transfer
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS
 THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
THE USE OF HYPERINFLATION IN THE MANAGEMENT OF INTUBATED AND VENTILATED ADULT PATIENTS RECOMMENDATIONS Recommendation 1 on website Hyperinflation (Ventilator or manual) might be included in the management
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Altered Respiratory Function Lecture 3. Nicole Tinny, RN, MSN Lake Sumter State College
 Altered Respiratory Function Lecture 3 Nicole Tinny, RN, MSN Lake Sumter State College Rhinitis Inflammation of nasal mucosa Due to infection or allergens Allergic rhinitis (hayfever) Rebound rhinitis
Altered Respiratory Function Lecture 3 Nicole Tinny, RN, MSN Lake Sumter State College Rhinitis Inflammation of nasal mucosa Due to infection or allergens Allergic rhinitis (hayfever) Rebound rhinitis