Identification and Treatment of the Patient with Sleep Related Hypoventilation
|
|
|
- Henry Shepherd
- 6 years ago
- Views:
Transcription
1 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center
2 X Conflict of Interest Disclosures for Speakers 1. I do not have any relationships with any entities producing, marketing, reselling, or distributing health care goods or services consumed by, or used on, patients, OR 2. I have the following relationships with entities producing, marketing, reselling, or distributing health care goods or services consumed by, or used on, patients. Type of Potential Conflict Details of Potential Conflict Grant/Research Support Consultant Speakers Bureaus Financial support Other 3. The material presented in this lecture has no relationship with any of these potential conflicts, OR 4. This talk presents material that is related to one or more of these potential conflicts, and the following objective references are provided as support for this lecture:
3 Objectives 1- Understand basic pulmonary physiology and the mechanisms through which hypoxia and hypoventilation occur. 2- Establish patient populations in which hypoventilation needs to be considered. 3- Know diagnostic criteria for sleep-related hypoventilation syndromes. 4- Understand treatment options and qualifying criteria for patients with clinical hypoventilation.
4 PHYSIOLOGY OF VENTILATION
5 V E = V T x f Minute Ventilation: closely linked with blood CO 2 values.
6 Alveolar Anatomy

")
7 Alveolar Ventilation Normal PaCO 2 = κ x (VCO 2 /VA) where VA = VE VE (VD/VT) Emphysema

8 Alveolar Ventilation V D = dead space Fixed dead space Alveolar dead space VQ mismatch Atelectasis, pulmonary embolism, pulmonary vascular disease, pneumonia R to L shunt Impaired Diffusion Interstitial lung disease
9 Hypoxemia in Hypoventilation PAO 2 = (Patm PH 2 O)FIO 2 (PACO 2 /RQ) *Contribution of FIO 2 in this equation shows why hypoxemia can be overcome By addition of supplemental oxygen.
10 Renal Compensation Respiratory acidosis is buffered by renal compensation CO 2 + HOH H 2 CO 3 H + + HCO 3 -


11 Pulmonary Function Testing
12 POPULATIONS TO CONSIDER HYPOVENTILATION
13 Known Gas Abnormalities Sustained hypoxia on baseline study Supplemental oxygen requirement in wakefulness Prior ABG with pco 2 > 45 mmhg PAO 2 = (Patm PH 2 O)FIO 2 (PACO 2 /RQ)
14 Lung disease Other Populations Neuromuscular disease Chest wall disease Morbid obesity Elevated serum bicarbonate Polycythemia
15 Other Populations Lung disease Increased dead space Neuromuscular disease Decreased V T Chest wall disease Decreased V T Morbid obesity Decreased V T, atelectasis and VQ mismatch Elevated serum bicarbonate Polycythemia
16 ESTABLISHING THE DIAGNOSIS OF HYPOVENTILATION
17 AASM Scoring Manual: Scoring Hypoventilation If electing to score hypoventilation, score hypoventilation during sleep if EITHER of the below occur: a. There is an increase in the arterial PCO 2 (or surrogate) to a value >55 mmhg for 10 minutes. b. There is 10 mmhg increase in arterial PCO 2 (or surrogate) during sleep (in comparison to an awake supine value) to a value exceeding 50 mmhg for 10 minutes.
18 Methodologies for Measuring CO 2 Arterial Blood Gas End Tidal CO 2 - non-invasive measurement of partial pressure of CO2 exhaled TCO2- CO2 is still measured potentiometrically by determining the ph of an electrolyte layer
19 ICSD-3: Sleep Related Hypoventilation Categories Disorders Obesity Hypoventilation Syndrome Congenital Central Alveolar Hypoventilation Syndrome Late-Onset Central Hypoventilation with Hypothalamic Dysfunction Idiopathic Central Alveolar Hypoventilation Sleep Related Hypoventilation Dues to a Medication or Substance Sleep Related Hypoventilation Does to a Medical Disorder
20 ICSD-3: Obesity Hypoventilation Syndrome Criteria A-C must be met A. Presence of hypoventilation during wakefulness (PaCO 2 > 45 mmhg) as measured by arterial PCO 2, end-tidal CO 2, or transcutaneous CO 2 B. Presence of obesity (BMI > 30 kg/m 2 ) C. Hypoventilation is not primarily due to lung parenchymal or airway disease, pulmonary vascular pathology, chest wall disorder, medication use, neurologic disorder, muscle weakness, or a known congenital or idiopathic central alveolar hypoventilation syndrome
21 ICSD-3: Congenital Central Alveolar Hypoventilation Syndrome Criteria A & B must be met A. Sleep related hypoventilation is present B. Mutation of the PHOX2B gene is present
22 ICSD-3: Late-Onset Central Hypoventilation with Hypothalamic Dysfunction Criteria A-E must be met A. Sleep related hypoventilation is present B. Symptoms are absent during the first few years of life C. The patient has at least two of the following: 1. Obesity 2. Endocrine abnormalities of hypothalamic origin 3. Severe emotional or behavioral disturbances 4. Tumor of neural origin D. Mutation of the PHOX2B gene is not present. E. The disorder is not better explained by another sleep disorder, medical or neurological disorder, medication use, or substance use disorder.
23 ICSD-3: Idiopathic Central Alveolar Hypoventilation Criteria A & B must be met A. Sleep related hypoventilation is present B. Hypoventilation is not primarily due to lung parenchymal or airway disease, pulmonary vascular pathology, chest wall disorder, medication use, neurologic disorder, muscle weakness, or obesity or congenital hypoventilation syndromes.
24 ICSD-3: Sleep Related Hypoventilation Dues to a Medication or Substance Criteria A-C must be met A. Sleep related hypoventilation is present. B. A medication or substance known to inhibit respiration and/or ventilatory drive is believed to be the primary cause of sleep related hypoventilation. C. Hypoventilation is not primarily due to lung parenchymal or airway disease, pulmonary vascular pathology, chest wall disorder, neurologic disorder, muscle weakness, obesity hypoventilation syndrome, or known congenital central alveolar hypoventilation syndrome.
25 ICSD-3: Sleep Related Hypoventilation Dues to a Medical Disorder Criteria A-C must be met A. Sleep related hypoventilation is present B. A lung parenchymal or airway disease, pulmonary vascular pathology, chest wall disorder, neurologic disorder, or muscle weakness is believed to be the primary cause of hypoventilation C. Hypoventilation is not primary due to obesity hypoventilation syndrome, medication use, or a known congenital central alveolar hypoventilation syndrome
26 TREATMENT OPTIONS
27 E0470: Bi-level PAP No back up rate, most algorithms require that a patient fail this prior to covering more advanced device.
28 E0471: Bi-level PAP with back-up rate Bi-level PAP with back up rate Compared with traditional bi-level PAP, guarantees a minimal number of breaths per minute Does not guarantee goal minute ventilation
29 E0471: AVAPS Average Volume Assured Pressure Support Settings Target V T IPAP min & IPAP max EPAP (some devices now have adjusting EPAP) Breath rate Inspiratory time (T i ) Rise time
30 QUALIFYING CRITERIA
31 Restrictive Thoracic Disorders

 No sooner than 61")

32 COPD For COPD to qualify for E0471 device: 1) After initial period of use of E0470, ABG with PaCO 2 7 mmhg higher than original ABG result or facility based PSG with O 2 saturation < 88% for > cumulative 5 minutes on E0470 2) No sooner than 61 days after initiation of E0470, ABG shows PaCO 2 52 mmhg or sleep oximetry on E0470 demonstrates O 2 saturation, 88% for a cumulative > 5 minutes.
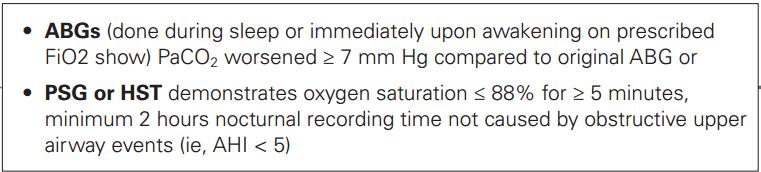

33 Hypoventilation
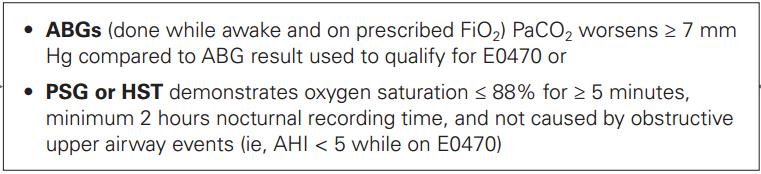
34 Hypoventilation, continued
35 Case- OHS June yo female with morbid obesity presents with subacute dyspnea and 30lb weight gain. ABG on 5L supplemental oxygen: ph 7.37, pco 2 74, po 2 46, SpO 2 76% Measured HCO 3- : >40
36 PFT- OHS (7/2011)

37 PFT- OHS (7/2011) DLCO 36% DL/VA 97%
38 Mechanisms of Impairment in OHS PaCO 2 = κ x (VCO 2 /VA) Increased work of breathing Decreased mechanical efficiency of ventilation Heart failure Atelectasis with VQ mismatch OSA
 Nadir O2: 71% 49 minutes with sat")
39 Baseline PSG (9/2011) AHI 7.2 events/hr (NREM 2.2, REM 51) Nadir O2: 71% 49 minutes with sat <88%
40 OHS Case Treated with diuresis and BPAP 18/8 with 4L O2 in CCMU with improvement in pco2 to low 60s. Ultimately discharged home on BPAP 18/8. Has had 2 f/u titrations in interim, most recent recommendation is BPAP 25/20 with 1L O2, but only observed in REM for 3 min. Most recent ABG: 7.36/48/68 on RA; HCO 3- : 28
41 References The AASM Manual for the Scoring of Sleep and Associated Events, Version 2.0. The AASM International Classification of Sleep Disorders, Third Edition. Eberhard, P. The design, use, and results of transcutaneous carbon dioxide analysis: current and future directions. Anesth Analg Dec;105(6 Suppl):S Theerakittikul T, et al. Noninvasive positive pressure ventilation for stable outpatients: CPAP and beyond. CCJM 2010 Oct;77(10):
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT
, RPSGT") BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
2/13/2018 OBESITY HYPOVENTILATION SYNDROME
 OBESITY HYPOVENTILATION SYNDROME David Claman, MD UCSF Professor of Medicine Director, UCSF Sleep Disorders Center Disclosures: None. 1 COMPLICATIONS OF OSA Cardiovascular HTN, CHF, CVA, arrhythmia, Pulm
OBESITY HYPOVENTILATION SYNDROME David Claman, MD UCSF Professor of Medicine Director, UCSF Sleep Disorders Center Disclosures: None. 1 COMPLICATIONS OF OSA Cardiovascular HTN, CHF, CVA, arrhythmia, Pulm
CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center
 FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
Challenging Cases in Pediatric Polysomnography. Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep
 Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
Average volume-assured pressure support
 Focused review Average volume-assured pressure support Abdurahim Aloud MD Abstract Average volume-assured pressure support (AVAPS) is a relatively new mode of noninvasive positive pressure ventilation
Focused review Average volume-assured pressure support Abdurahim Aloud MD Abstract Average volume-assured pressure support (AVAPS) is a relatively new mode of noninvasive positive pressure ventilation
NIPPV FOR THE HYPERCAPNIC COPD AND OBSESITY HYPOVENTILATION PATIENT
 NIPPV FOR THE HYPERCAPNIC COPD AND OBSESITY HYPOVENTILATION PATIENT Gaurav Singh, MD Stanford University Associate Professor Saturday, January 19, 2019 3:20 p.m. 4:00 p.m. Gaurav Singh, MD, completed all
NIPPV FOR THE HYPERCAPNIC COPD AND OBSESITY HYPOVENTILATION PATIENT Gaurav Singh, MD Stanford University Associate Professor Saturday, January 19, 2019 3:20 p.m. 4:00 p.m. Gaurav Singh, MD, completed all
Policy Specific Section: October 1, 2010 January 21, 2013
 Medical Policy Bi-level Positive Airway Pressure (BPAP/NPPV) Type: Medical Necessity/Not Medical Necessity Policy Specific Section: Durable Medical Equipment Original Policy Date: Effective Date: October
Medical Policy Bi-level Positive Airway Pressure (BPAP/NPPV) Type: Medical Necessity/Not Medical Necessity Policy Specific Section: Durable Medical Equipment Original Policy Date: Effective Date: October
A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation
 1 A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation The following 3 minute polysomnogram (PSG) tracing was recorded in a 74-year-old man with severe ischemic cardiomyopathy
1 A 74-year-old man with severe ischemic cardiomyopathy and atrial fibrillation The following 3 minute polysomnogram (PSG) tracing was recorded in a 74-year-old man with severe ischemic cardiomyopathy
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Interpretation of Arterial Blood Gases. Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB)
") Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
OSA and COPD: What happens when the two OVERLAP?
 2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
2011 ISRC Seminar 1 COPD OSA OSA and COPD: What happens when the two OVERLAP? Overlap Syndrome 1 OSA and COPD: What happens when the two OVERLAP? ResMed 10 JAN Global leaders in sleep and respiratory medicine
Causes and Consequences of Respiratory Centre Depression and Hypoventilation
 Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
3. Which of the following would be inconsistent with respiratory alkalosis? A. ph = 7.57 B. PaCO = 30 mm Hg C. ph = 7.63 D.
 Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Respiratory Failure how the respiratory physicians deal with airway emergencies
 Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Respiratory Failure how the respiratory physicians deal with airway emergencies Dr Michael Davies MD FRCP Consultant Respiratory Physician Respiratory Support and Sleep Centre Papworth Hospital NHS Foundation
Physiological Causes of Abnormal ABG s
 Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
PEDIATRIC PAP TITRATION PROTOCOL
 PURPOSE In order to provide the highest quality care for our patients, our sleep disorders facility adheres to the AASM Standards of Accreditation. The accompanying policy and procedure on pediatric titrations
PURPOSE In order to provide the highest quality care for our patients, our sleep disorders facility adheres to the AASM Standards of Accreditation. The accompanying policy and procedure on pediatric titrations
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
11/20/2015. Beyond CPAP. No relevant financial conflicts of interest. Kristie R Ross, M.D. November 12, Describe advanced ventilation options
 Beyond CPAP Kristie R Ross, M.D. November 12, 2015 No relevant financial conflicts of interest Sponsored by The Warren Alpert Medical School of Brown University Describe advanced ventilation options Compare
Beyond CPAP Kristie R Ross, M.D. November 12, 2015 No relevant financial conflicts of interest Sponsored by The Warren Alpert Medical School of Brown University Describe advanced ventilation options Compare
Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine
 Management of pediatric OSA Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine Chulalongkorn University Treatment modalities Surgery Medications NIV during
Management of pediatric OSA Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine Chulalongkorn University Treatment modalities Surgery Medications NIV during
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
Arterial Blood Gas Analysis
 Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Arterial Blood Gases. Dr Mark Young Mater Health Services
 Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
Arterial Blood Gases Interpretation Definition Values respiratory metabolic
 Arterial Blood Gases Interpretation Definition A blood gas test measures the amount of oxygen and carbon dioxide in the blood. It is also useful in determining the ph level of the blood. The test is commonly
Arterial Blood Gases Interpretation Definition A blood gas test measures the amount of oxygen and carbon dioxide in the blood. It is also useful in determining the ph level of the blood. The test is commonly
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
SIMPLY Arterial Blood Gases Interpretation. Week 4 Dr William Dooley
 SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment
 Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment Judith R. Fischer, MSLS, Editor, Ventilator-Assisted Living (fischer.judith@sbcglobal.net) Thanks to Josh Benditt, MD, University
Hypoventilation? Obstructive Sleep Apnea? Different Tests, Different Treatment Judith R. Fischer, MSLS, Editor, Ventilator-Assisted Living (fischer.judith@sbcglobal.net) Thanks to Josh Benditt, MD, University
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Transcutaneous Monitoring and Case Studies
 Transcutaneous Monitoring and Case Studies Objectives General concept, applications and principles of operation Role of TCM in clinical settings Role of TCM in home care settings Need for continuous TCM
Transcutaneous Monitoring and Case Studies Objectives General concept, applications and principles of operation Role of TCM in clinical settings Role of TCM in home care settings Need for continuous TCM
Control of Ventilation [2]
![Control of Ventilation [2]](/thumbs/83/87644191.jpg "Control of Ventilation [2]") Control of Ventilation [2] สรช ย ศร ส มะ พบ., Ph.D. ภาคว ชาสร รว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล มหาว ทยาล ยมห ดล Describe the effects of alterations in chemical stimuli, their mechanisms and response to
Control of Ventilation [2] สรช ย ศร ส มะ พบ., Ph.D. ภาคว ชาสร รว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล มหาว ทยาล ยมห ดล Describe the effects of alterations in chemical stimuli, their mechanisms and response to
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist. This program has been approved for 1 hour of continuing education credit.
 Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Titration protocol reference guide
 PN 1079754_Cover:22037_Cov_Canada 11/22/10 Philips Healthcare is part of Royal Philips Electronics How to reach us www.philips.com/healthcare healthcare@philips.com Asia +49 7031 463 2254 Europe, Middle
PN 1079754_Cover:22037_Cov_Canada 11/22/10 Philips Healthcare is part of Royal Philips Electronics How to reach us www.philips.com/healthcare healthcare@philips.com Asia +49 7031 463 2254 Europe, Middle
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
New Government O2 Criteria and Expert Panel. Jennifer Despain, RPSGT, RST, AS
 New Government O2 Criteria and Expert Panel Jennifer Despain, RPSGT, RST, AS Lead Sleep Technologist, Central Utah Clinic Sleep Disorders Center; Provo, Utah Objectives: Review new government O2 criteria
New Government O2 Criteria and Expert Panel Jennifer Despain, RPSGT, RST, AS Lead Sleep Technologist, Central Utah Clinic Sleep Disorders Center; Provo, Utah Objectives: Review new government O2 criteria
Obrigada por ver esta apresentação. Lembramos que esta apresentação é propriedade do autor
 Obrigada por ver esta apresentação Lembramos que esta apresentação é propriedade do autor É-lhe proporcionada pela Associação Portuguesa de Sono no contexto da Lufada 2016, para seu uso pessoal, tal como
Obrigada por ver esta apresentação Lembramos que esta apresentação é propriedade do autor É-lhe proporcionada pela Associação Portuguesa de Sono no contexto da Lufada 2016, para seu uso pessoal, tal como
For more information about how to cite these materials visit
 Author(s): John G. Younger, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author(s): John G. Younger, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Carbon Dioxide Transport. Carbon Dioxide. Carbon Dioxide Transport. Carbon Dioxide Transport - Plasma. Hydrolysis of Water
 Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
Respiratory Complications of Obesity. Diana Wilson, M.D. ACP Educational Session September 16, 2017
 Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting
 Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting Lisa F. Wolfe MD Northwestern University Chicago, Illinois Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting
Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting Lisa F. Wolfe MD Northwestern University Chicago, Illinois Choosing the Appropriate Mode of PAP Therapy in the Perioperative Setting
Monitoring: gas exchange, poly(somno)graphy or device in-built software?
graphy or device in-built software?") Monitoring: gas exchange, poly(somno)graphy or device in-built software? Alessandro Amaddeo Noninvasive ventilation and Sleep Unit & Inserm U 955 Necker Hospital, Paris, France Inserm Institut national
Monitoring: gas exchange, poly(somno)graphy or device in-built software? Alessandro Amaddeo Noninvasive ventilation and Sleep Unit & Inserm U 955 Necker Hospital, Paris, France Inserm Institut national
PAP Therapy Devices: Delivering the Right Therapy To The Right Patient. Ryan Schmidt, BS, RRT Clinical Specialist Philips Respironics
 PAP Therapy Devices: Delivering the Right Therapy To The Right Patient Ryan Schmidt, BS, RRT Clinical Specialist Philips Respironics Conflict of Interest Disclosure(s) I do not have any potential conflicts
PAP Therapy Devices: Delivering the Right Therapy To The Right Patient Ryan Schmidt, BS, RRT Clinical Specialist Philips Respironics Conflict of Interest Disclosure(s) I do not have any potential conflicts
Complex Sleep Apnea. Can we do better? David Weed D.O.,FCCP,FAASM. September 8, 2016
 Complex Sleep Apnea Can we do better? David Weed D.O.,FCCP,FAASM September 8, 2016 If you don t know where you are going, you ll end up somewhere else. Yogi Berra Objectives Discuss what syndromes comprise
Complex Sleep Apnea Can we do better? David Weed D.O.,FCCP,FAASM September 8, 2016 If you don t know where you are going, you ll end up somewhere else. Yogi Berra Objectives Discuss what syndromes comprise
High Flow Nasal Cannula in Children During Sleep. Brian McGinley M.D. Associate Professor of Pediatrics University of Utah
 High Flow Nasal Cannula in Children During Sleep Brian McGinley M.D. Associate Professor of Pediatrics University of Utah Disclosures Conflicts of Interest: None Will discuss a product that is commercially
High Flow Nasal Cannula in Children During Sleep Brian McGinley M.D. Associate Professor of Pediatrics University of Utah Disclosures Conflicts of Interest: None Will discuss a product that is commercially
CASE REPORT. Miyuki Okuda 1*, Makoto Kashio 1, Nobuya Tanaka 1, Takashi Fujii 1 and Yoshinari Okuda 2
 Okuda et al. Journal of Medical Case Reports 2012, 6:284 JOURNAL OF MEDICAL CASE REPORTS CASE REPORT Positive outcome of average volume-assured pressure support mode of a Respironics V60 Ventilator in
Okuda et al. Journal of Medical Case Reports 2012, 6:284 JOURNAL OF MEDICAL CASE REPORTS CASE REPORT Positive outcome of average volume-assured pressure support mode of a Respironics V60 Ventilator in
RESPIRATION AND SLEEP AT HIGH ALTITUDE
 MANO Pulmonologist-Intensivis Director of ICU and Sleep Dis Evangelism Ath RESPIRATION AND SLEEP AT HIGH ALTITUDE 2 nd Advanced Course in Mountain Medicine MAY 25-27 OLYMPUS MOUNTAIN Respiration Breathing
MANO Pulmonologist-Intensivis Director of ICU and Sleep Dis Evangelism Ath RESPIRATION AND SLEEP AT HIGH ALTITUDE 2 nd Advanced Course in Mountain Medicine MAY 25-27 OLYMPUS MOUNTAIN Respiration Breathing
Κλινικό Φροντιστήριο Αναγνώριση και καταγραφή αναπνευστικών επεισοδίων Λυκούργος Κολιλέκας Επιμελητής A ΕΣΥ 7η Πνευμονολογική Κλινική ΝΝΘΑ Η ΣΩΤΗΡΙΑ
 Κλινικό Φροντιστήριο Αναγνώριση και καταγραφή αναπνευστικών επεισοδίων Λυκούργος Κολιλέκας Επιμελητής A ΕΣΥ 7 η Πνευμονολογική Κλινική ΝΝΘΑ Η ΣΩΤΗΡΙΑ SCORING SLEEP -Rechtschaffen and Kales (1968) - AASM
Κλινικό Φροντιστήριο Αναγνώριση και καταγραφή αναπνευστικών επεισοδίων Λυκούργος Κολιλέκας Επιμελητής A ΕΣΥ 7 η Πνευμονολογική Κλινική ΝΝΘΑ Η ΣΩΤΗΡΙΑ SCORING SLEEP -Rechtschaffen and Kales (1968) - AASM
OXYGEN USE IN PHYSICAL THERAPY PRACTICE. Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR
 OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
Pain patient with sleep-disordered breathing
 Pain patient with sleep-disordered breathing Clinical scenario: A 50-year old female with a history of acid reflux, fibromyalgia, spinal stenosis and degenerative disk disease s/p C3/C4 disk fusion, depression
Pain patient with sleep-disordered breathing Clinical scenario: A 50-year old female with a history of acid reflux, fibromyalgia, spinal stenosis and degenerative disk disease s/p C3/C4 disk fusion, depression
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Sleep and Neuromuscular Disease. Sharon De Cruz, MD Tisha Wang, MD
 Sleep and Neuromuscular Disease Sharon De Cruz, MD Tisha Wang, MD Case Presentation Part I GR is a 21-year old male with Becker muscular dystrophy who comes to your office complaining of progressively
Sleep and Neuromuscular Disease Sharon De Cruz, MD Tisha Wang, MD Case Presentation Part I GR is a 21-year old male with Becker muscular dystrophy who comes to your office complaining of progressively
RESPIRATORY ASSIST DEVICE E0471
 JURISDICTIONS B &C Bi-Level Pressure Capacity WITH Backup Rate REQUIRED DOCUMENTATION All Claims for E0471 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the E0470
JURISDICTIONS B &C Bi-Level Pressure Capacity WITH Backup Rate REQUIRED DOCUMENTATION All Claims for E0471 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the E0470
RESPIRATORY ASSIST DEVICE E0470
 JURISDICTIONS B &C Bi-Level Pressure Capacity WITHOUT Backup Rate REQUIRED DOCUMENTATION All Claims for E0470 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the
JURISDICTIONS B &C Bi-Level Pressure Capacity WITHOUT Backup Rate REQUIRED DOCUMENTATION All Claims for E0470 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Respiratory Assist Device E0470:
 Respiratory Assist Device E0470: Bi-Level Pressure Capacity WITHOUT Backup Rate REQUIRED DOCUMENTATION IN SUPPLIER S FILE All Claims for E0470 Initial Coverage (1st Three Months) 5 Element Order obtained
Respiratory Assist Device E0470: Bi-Level Pressure Capacity WITHOUT Backup Rate REQUIRED DOCUMENTATION IN SUPPLIER S FILE All Claims for E0470 Initial Coverage (1st Three Months) 5 Element Order obtained
Interpretation of Arterial Blood Gases (ABG)
") Interpretation of Arterial Blood Gases (ABG) Prof. Dr. W. Vincken Head Respiratory Division Universitair Ziekenhuis Brussel (UZ Brussel) Vrije Universiteit Brussel (VUB) 29-3-2015 W Vincken - UZ Brussel
Interpretation of Arterial Blood Gases (ABG) Prof. Dr. W. Vincken Head Respiratory Division Universitair Ziekenhuis Brussel (UZ Brussel) Vrije Universiteit Brussel (VUB) 29-3-2015 W Vincken - UZ Brussel
Outline. ABG Interpretation: A Respirologist s approach. Acid-Base Disturbances. What use is an ABG? Acid-Base Disturbances. Alveolar Ventilation
 Outline ABG Interpretation: A Respirologist s approach Dr. Shane Shapera Division of Respirology University Health Network October 2014 A quick review of acidbase physiology The 8 steps to ABG interpretation
Outline ABG Interpretation: A Respirologist s approach Dr. Shane Shapera Division of Respirology University Health Network October 2014 A quick review of acidbase physiology The 8 steps to ABG interpretation
TSANZ meeting 01 Apr Physiology of respiratory failure in COPD & OHS. Bhajan Singh MBBS FRACP PhD
 TSANZ meeting 01 Apr 2015 Physiology of respiratory failure in & OHS Bhajan Singh MBBS FRACP PhD Head of Department, Pulmonary Physiology & Sleep Medicine, Sir Charles Gairdner Hospital Director, West
TSANZ meeting 01 Apr 2015 Physiology of respiratory failure in & OHS Bhajan Singh MBBS FRACP PhD Head of Department, Pulmonary Physiology & Sleep Medicine, Sir Charles Gairdner Hospital Director, West
POLICY. Number: Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE. Authorization
 POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery
 Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
All About Positive Airway Pressure (PAP) Therapy
 Therapy") All About Positive Airway Pressure (PAP) Therapy Nitipatana Chierakul Division of Respiratory Disease and Tuberculosis, Department of Medicine, Siriraj Medical School Siriraj Sleep Center: Fiscal-year
All About Positive Airway Pressure (PAP) Therapy Nitipatana Chierakul Division of Respiratory Disease and Tuberculosis, Department of Medicine, Siriraj Medical School Siriraj Sleep Center: Fiscal-year
Helpful hints for filing
 Helpful hints for filing Respiratory Assist Devices HCPCS Code E0470 E0471 Overview The following information describes the Durable Medical Equipment Medicare Administrative Contractors' (DME MACs) medical
Helpful hints for filing Respiratory Assist Devices HCPCS Code E0470 E0471 Overview The following information describes the Durable Medical Equipment Medicare Administrative Contractors' (DME MACs) medical
RESPIRATORY ASSIST DEVICE E0471
 JURISDICTIONS B &C Bi-Level Pressure Capacity WITH Backup Rate REQUIRED DOCUMENTATION All Claims for E0471 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the E0470
JURISDICTIONS B &C Bi-Level Pressure Capacity WITH Backup Rate REQUIRED DOCUMENTATION All Claims for E0471 Initial Coverage (1st Three Months) 5 Element Order (5EO) obtained prior to delivery for the E0470
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acquired central hypoventilation syndrome, NPPV in children with, 475 Acute cardiogenic pulmonary edema, PAP therapy in, 394 395 Adaptive
Index Note: Page numbers of article titles are in boldface type. A Acquired central hypoventilation syndrome, NPPV in children with, 475 Acute cardiogenic pulmonary edema, PAP therapy in, 394 395 Adaptive
In-Patient Sleep Testing/Management Boaz Markewitz, MD
 In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
In-Patient Sleep Testing/Management Boaz Markewitz, MD Objectives: Discuss inpatient sleep programs and if they provide a benefit to patients and sleep centers Identify things needed to be considered when
CMS Reimbursement of CPAP, Oxygen, BPAP, HMV for Sleep Disordered Breathing Peter C Gay Professor of Medicine Mayo Clinic Rochester, MN
 45th Annual New Mexico Thoracic Society Lung Disease Symposium CMS Reimbursement of CPAP, Oxygen, BPAP, HMV for Sleep Disordered Breathing Peter C Gay Professor of Medicine Mayo Clinic Rochester, MN Conflicts?
45th Annual New Mexico Thoracic Society Lung Disease Symposium CMS Reimbursement of CPAP, Oxygen, BPAP, HMV for Sleep Disordered Breathing Peter C Gay Professor of Medicine Mayo Clinic Rochester, MN Conflicts?
Pap Settings. A review of fine tuning settings For patient comfort and compliance Wendy Cook BSRT Judy Salisbury RPGST
 Pap Settings A review of fine tuning settings For patient comfort and compliance Wendy Cook BSRT Judy Salisbury RPGST Conflict of Interest Disclosure x 1. I do not have any relationships with any entities
Pap Settings A review of fine tuning settings For patient comfort and compliance Wendy Cook BSRT Judy Salisbury RPGST Conflict of Interest Disclosure x 1. I do not have any relationships with any entities
Non-Invasive Assessment of Respiratory Function. Chapter 11
 Non-Invasive Assessment of Respiratory Function Chapter 11 Pulse Oximetry Laboratory measurements of ABG s are the gold standard for measuring levels of hypoxemia, however since these are performed intermittently
Non-Invasive Assessment of Respiratory Function Chapter 11 Pulse Oximetry Laboratory measurements of ABG s are the gold standard for measuring levels of hypoxemia, however since these are performed intermittently
Reasons Providers Use Bilevel
 Reasons Providers Use Bilevel More comfort, improve therapy compliance Noncompliant OSA (NCOSA) 1 Scripts from lab referrals Central/Complex Sleep Apnea 2 For ventilations needs Restrictive Thoracic Disorders/Neuromuscular
Reasons Providers Use Bilevel More comfort, improve therapy compliance Noncompliant OSA (NCOSA) 1 Scripts from lab referrals Central/Complex Sleep Apnea 2 For ventilations needs Restrictive Thoracic Disorders/Neuromuscular
Medicare C/D Medical Coverage Policy. Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders
 Medicare C/D Medical Coverage Policy Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January,
Medicare C/D Medical Coverage Policy Respiratory Assist Devices for Obstructive Sleep Apnea and Breathing Related Sleep Disorders Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January,
Auto Servo Ventilation Indications, Basics of Algorithm, and Titration
 Auto Servo Ventilation Indications, Basics of Algorithm, and Titration 1 ASV Learning Objectives Understand the indications for Auto Servo Ventilation Differentiate obstructive versus central hypopneas
Auto Servo Ventilation Indications, Basics of Algorithm, and Titration 1 ASV Learning Objectives Understand the indications for Auto Servo Ventilation Differentiate obstructive versus central hypopneas
Understanding Complex Pulmonary Hypertension through Advanced Hemodynamics
 Understanding Complex Pulmonary Hypertension through Advanced Hemodynamics Franz Rischard, DO, MS Director, Pulmonary Hypertension Program Assistant Professor of Medicine University of Arizona Lillian
Understanding Complex Pulmonary Hypertension through Advanced Hemodynamics Franz Rischard, DO, MS Director, Pulmonary Hypertension Program Assistant Professor of Medicine University of Arizona Lillian
Dr. Sinan Butrus F.I.C.M.S. Clinical Standards & Guidelines. Kurdistan Board For Medical Specialties
 Guidelines For the Management of Respiratory Acidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Respiratory acidosis is an acid-base balance
Guidelines For the Management of Respiratory Acidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Kurdistan Board For Medical Specialties Respiratory acidosis is an acid-base balance
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Case 1. Level of difficulty: 2/5
 Case 1 Level of difficulty: 2/5 Summary Settings in the ventilator BULBAR ALS Ventilation 24h/24, Good tolerance PaO2 82; PaCO2 : 42, ph=7,42 (under ventilation) Mode: S/T Main parameters : Pressure Support
Case 1 Level of difficulty: 2/5 Summary Settings in the ventilator BULBAR ALS Ventilation 24h/24, Good tolerance PaO2 82; PaCO2 : 42, ph=7,42 (under ventilation) Mode: S/T Main parameters : Pressure Support
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
How to suspect hypoven/la/on?
 How to suspect hypoven/la/on? David Orlikowski M.D., Ph.D. Clinical investigation center INSERM 1429 Intensive care and home ventilation unit, Reference Centre for Neuromuscular Disease hôpital Raymond
How to suspect hypoven/la/on? David Orlikowski M.D., Ph.D. Clinical investigation center INSERM 1429 Intensive care and home ventilation unit, Reference Centre for Neuromuscular Disease hôpital Raymond
Respiratory Physiology Part II. Bio 219 Napa Valley College Dr. Adam Ross
 Respiratory Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Gas exchange Gas exchange in the lungs (to capillaries) occurs by diffusion across respiratory membrane due to differences in partial
Respiratory Physiology Part II Bio 219 Napa Valley College Dr. Adam Ross Gas exchange Gas exchange in the lungs (to capillaries) occurs by diffusion across respiratory membrane due to differences in partial
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
11/20/2015. Eighth Bi-Annual Pediatric Sleep Medicine Conference. November 12-15, 2015 Omni Amelia Island Plantation Resort Amelia Island, Florida
 Eighth Bi-Annual Pediatric Sleep Medicine Conference November 12-15, 2015 Omni Amelia Island Plantation Resort Amelia Island, Florida Carol L. Rosen, MD Case Western Reserve University School of Medicine
Eighth Bi-Annual Pediatric Sleep Medicine Conference November 12-15, 2015 Omni Amelia Island Plantation Resort Amelia Island, Florida Carol L. Rosen, MD Case Western Reserve University School of Medicine
Testing Clinical Implications
 Cardiopulmonary Exercise Testing Clinical Implications Dr Sahajal Dhooria Outline Basic concepts Case studies Recent advances in clinical applications of CPET Basic Concepts Exercise Any physical activity
Cardiopulmonary Exercise Testing Clinical Implications Dr Sahajal Dhooria Outline Basic concepts Case studies Recent advances in clinical applications of CPET Basic Concepts Exercise Any physical activity
Evaluation of a transcutaneous carbon dioxide monitor in severe obesity
 Intensive Care Med DOI 10.1007/s00134-008-1078-8 PHYSIOLOGICAL AND TECHNICAL NOTES Mauro Maniscalco Anna Zedda Stanislao Faraone Pierluigi Carratù Matteo Sofia Evaluation of a transcutaneous carbon dioxide
Intensive Care Med DOI 10.1007/s00134-008-1078-8 PHYSIOLOGICAL AND TECHNICAL NOTES Mauro Maniscalco Anna Zedda Stanislao Faraone Pierluigi Carratù Matteo Sofia Evaluation of a transcutaneous carbon dioxide
WHAT DO YOU WANT FROM A HOME VENTILATION SYSTEM? 8322_RS_HomeNIV_brochure_v14.ind1 1 4/7/06 12:57:35
 WHAT DO YOU WANT FROM A HOME VENTILATION SYSTEM? 8322_RS_HomeNIV_brochure_v14.ind1 1 4/7/06 12:57:35 D I L E M M A DIFFERENT VENTILATORS DIFFERENT ALGORITHMS TO KNOW YOU VE CHANGED PATIENT LIVES?PATIENT??
WHAT DO YOU WANT FROM A HOME VENTILATION SYSTEM? 8322_RS_HomeNIV_brochure_v14.ind1 1 4/7/06 12:57:35 D I L E M M A DIFFERENT VENTILATORS DIFFERENT ALGORITHMS TO KNOW YOU VE CHANGED PATIENT LIVES?PATIENT??
NON-INVASIVE POSITIVE PRESSURE VENTILATION IN THE EMERGENCY DEPARTMENT
 NON-INVASIVE POSITIVE PRESSURE VENTILATION IN THE EMERGENCY DEPARTMENT Developed by J. Osteraas and K. Fuzzard 2001. Reviewed and by K. Maddern 2010 Contents Introduction Assessment Learning Outcomes Background
NON-INVASIVE POSITIVE PRESSURE VENTILATION IN THE EMERGENCY DEPARTMENT Developed by J. Osteraas and K. Fuzzard 2001. Reviewed and by K. Maddern 2010 Contents Introduction Assessment Learning Outcomes Background
RESPIRATORY SYSTEM and ACID BASE
 RESPIRATORY SYSTEM and ACID BASE Arif HM Marsaban Rudyanto Sedono Department of Anesthesiology and Intensive Therapy Faculty of medicine University of Indonesia Dr Cipto Mangunkusumo General Hospital Jakarta
RESPIRATORY SYSTEM and ACID BASE Arif HM Marsaban Rudyanto Sedono Department of Anesthesiology and Intensive Therapy Faculty of medicine University of Indonesia Dr Cipto Mangunkusumo General Hospital Jakarta
UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1)
") UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1) Textbook of medical physiology, by A.C. Guyton and John E, Hall, Twelfth Edition,
UNIVERSITY OF JORDAN DEPT. OF PHYSIOLOGY & BIOCHEMISTRY RESPIRATORY PHYSIOLOGY MEDICAL STUDENTS FALL 2014/2015 (lecture 1) Textbook of medical physiology, by A.C. Guyton and John E, Hall, Twelfth Edition,
How To Set Up A Ven.lator: Standard Versus High Pressure
 How To Set Up A Ven.lator: Standard Versus High Pressure Dean R. Hess PhD RRT Assistant Director of Respiratory Care MassachuseBs General Hospital Associate Professor of Anesthesia Harvard Medical School
How To Set Up A Ven.lator: Standard Versus High Pressure Dean R. Hess PhD RRT Assistant Director of Respiratory Care MassachuseBs General Hospital Associate Professor of Anesthesia Harvard Medical School
Coding for Sleep Disorders Jennifer Rose V. Molano, MD
 Practice Coding for Sleep Disorders Jennifer Rose V. Molano, MD Accurate coding is an important function of neurologic practice. This section of is part of an ongoing series that presents helpful coding
Practice Coding for Sleep Disorders Jennifer Rose V. Molano, MD Accurate coding is an important function of neurologic practice. This section of is part of an ongoing series that presents helpful coding
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial