AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK. Michael Smolensky, Ph.D. The University of Texas Austin & Houston
|
|
|
- Gabriel Wiggins
- 6 years ago
- Views:
Transcription
1 AGING, BLOOD PRESSURE & CARDIOVASCULAR DISEASE EVENT RISK Michael Smolensky, Ph.D. The University of Texas Austin & Houston
2 Disclosures Partner: Circadian Ambulatory Diagnostics Consultant: Spot On Sciences (Austin, Texas) Consultant: National Toxicology Program, US Dept. Health & Human Services
3 Outline Accuracy of daytime office blood pressure (BP) measurement (OBPM) vs. 24-hour ambulatory BP monitoring (ABPM) to diagnose hypertension Accuracy of cardiovascular disease (CVD) event prediction by daytime OBPM vs. ABPM-derived awake or asleep BP means Trend in awake & asleep SBP & DBP with aging Male/female difference in BP diagnostic thresholds & relevance to CVD risk reduction of women Differential reduction of CVD events by treatment that targets normalization of daytime OBPM vs. asleep BP vs. awake BP
4 Part I: Merit of 24-hour ABPM vs. Daytime OBPM to Diagnose Hypertension & Assess CVD Risk Significance: Accurate diagnosis of normal vs. elevated BP Accurate prognostication of future CVD events State of art knowledge: ABPM more consistent and accurate than OBPM & better predictor of future CVD events

5 Each 20/10 mm Hg Increase in BP Doubles CV Mortality Risk
6 Continued US Prevention Services Task Forces 2015 report: Confirmation of daytime OBPM-diagnosed hypertension by out-of-office measurement poor - as low as 35% & generally no better than 75% 1 ABPM predicts long-term CVD events independently of OBPM: Hazard ratio = 1.28 to ABC-H Investigators 2015 report: ABPM, especially nighttime SBP, significantly better predictor of future CVD events than daytime OBPM 2 1 Piper et al., Ann Intern Med. 2015;162: ABC-Investigators et al., J. Hypertens. 2015;32:
7 Merit of OBPM vs. ABPM-Derived Awake vs. Asleep BP to Predict Future CVD Events 2005 Dublin 8.4 yr median duration trial (5292 pts): ABPM superior to daytime OBPM as predictor of CVD & all-cause mortality, nighttime SBP strongest predictor European CVD events trial (3468 pts): ABPM-derived daytime & nighttime SBP means predicted CVD & all-cause, coronary heart disease & stroke mortality independently from daytime OBPM. When the SBPs simultaneously entered into statistical model, nighttime SBP predicted all outcomes, whereas daytime SBP did not add prognostic precision 2 1 Dolan et al., Hypertension. 2005;46: Fagard et al., Hypertension 2008;51:55-61
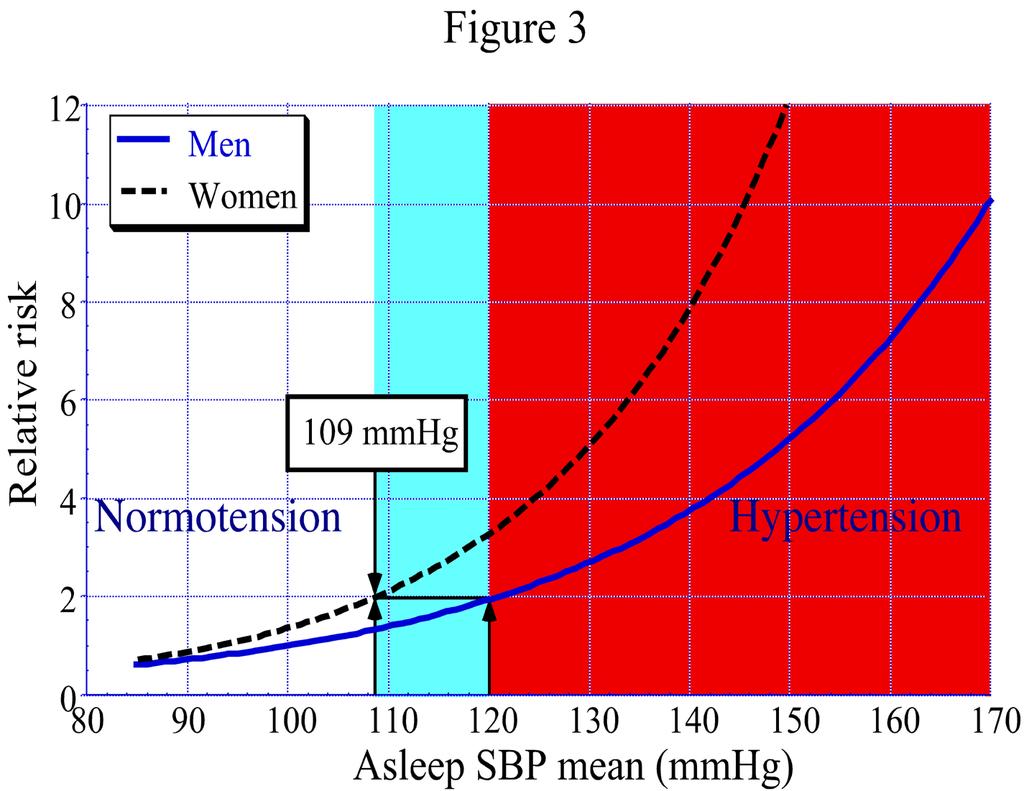
8 Part II: ABPM-Derived Asleep BP Parameters Significance: Asleep systolic BP (SBP) mean more strongly correlated with CVD events than awake or 24-hour SBP means Incidence of elevated asleep SBP increases steadily after 45 yrs of age Studies suggest diagnostic hypertension thresholds for women should be lower than current ones State of art knowledge: ABPM plus pt diary/wrist actigraphy to denote actual sleep & awake spans is the only way to assess sleep SBP & DBP means
9 . 130 SBP IN NORMOTENSIVE SUBJECTS PHASE (360 = 24 HOURS) M M M M M M M M M M M M M SYSTOLIC BLOOD PRESSURE (mmhg) M F M F F F F F F F F F F F F F F M F M F M MESOR= MESOR= M M M M M M M M MALES F F FEMALES * p<0.05 AMONG GROUPS F F 95 F F F F F 0 * * * * * * * * * * * * * * * * * * * * * * * * 00:00 04:00 08:00 12:00 16:00 20:00 00:00 TIME (HOURS AFTER AWAKENING) Hermida et al. Chronobiol Int. 2002;19:
10 PATTERNS OF BLOOD PRESSURE VARIABILITY 180 SYSTOLIC BLOOD PRESSURE (mm Hg) NORMOTENSIVE - DIPPER HYPERTENSIVE - DIPPER HYPERTENSIVE - SUPER-DIPPER HYPERTENSIVE - NONDIPPER MEAN = 125 mm Hg TIME (HOURS AFTER AWAKENING)
11 Change in awake and asleep SBP means with age in hypertensive individuals. 140 Awake SBP mean Asleep SBP mean 135 SBP (mmhg) < Age (years) Hermida et al., Chronobiol Int. 2013;30:176-91
12 Change in sleep-time relative SBP decline with age in hypertensive individuals. 14 Sleep-time relative SBP decline (%) < Age (years) Hermida et al. Chronobiol Int. 2013;30:176-91
13 Elevated Asleep BP & Non-Dipping & BP Patterning Is Common Aging ( 60% in elderly >age 65 yrs) Resistant hypertension (~80%) Type 2 diabetes (>75%) Chronic renal disease (~70%) Sleep disorders: insomnia, obstructive sleep apnea, etc. (??) Chronic pain syndromes that disturb sleep (??) Chronic nocturnal COPD that disturbs sleep (??) Chronic nocturia that disturbs sleep (??) Neurological conditions that disturb sleep (??) Metabolic syndrome (??) Previous CVD events (??)
14 MAPEC Outcomes Trial (1626 Female/1728 Male Day-Active Pts)* Prospective clinical trial to compare differential merit of: Daytime OBPM vs. ABPM-derived awake & asleep BP parameters to predict future CVD events Targeting control of awake vs. asleep BP by bedtime therapy (full dose of 1 conventional hypertension medications) vs. typical morning therapy for BP control & CVD event reduction. *Hermida et al., Chronobiol Int. 2010;27:
15 MAPEC Trial Methods At inclusion & annually, pts assessed for 48 consecutive hours by ABPM: Δt=20 min 07:00 to 23:00 & Δt=30 min overnight Physical activity monitored by wrist actigraphy (Δt=1 min) to accurately derive per pt awake & asleep SBP & DBP means ABPM integrated into primary pt care medicine & done at least annually to enable detection of relationship between BP parameters & 24-hour patterning that immediately preceded a CVD event.
16 MAPEC Trial Outcomes (Blue=Major; Blue + Black=Total CVD events) CVD event outcomes: Myocardial infarction Hemorrhagic stroke Ischemic stroke CVD death Coronary revascularization Heart failure Additional registered events: Angina pectoris Transient ischemic attacks Acute arterial occlusion of lower extremities Thrombotic occlusion of retinal artery Non-CVD death

17 What Is the Best Predictor of CVD Events: ABPM-Derived Asleep vs. Awake BP? Patients of MAPEC Trial divided into 4 groups according to ABPM-derived awake & asleep SBP & DBP means at final evaluation before CVD event: Normal awake SBP/DBP means: <135/85 mmhg Normal asleep SBP/DBP means: <120/70 mmhg *Hermida et al., J Am Coll Cardiol. 2011;58:
18 Adjusted HR Adjusted hazard ratio of total CVD events Classification by awake and asleep BP means 1.00 Normal awake BP High awake BP P<0.001 P=0.39 P<0.001 P=0.002 P= ( ) 1.84 ( ) 2.31 ( ) Normal asleep BP High asleep BP Hermida et al. J Am Coll Cardiol. 2011;58:
19 Adjusted hazard ratio of major CVD events Classification by awake and asleep BP means 5 4 P<0.001 P=0.10 P<0.001 Adjusted HR P=0.98 Normal awake BP High awake BP 0.98 ( ) Normal asleep BP P= ( ) High asleep BP 4.36 ( ) Hermida et al., J Am Coll Cardiol. 2011;58: Hermida et al., Chronobiol Int. 2013;30(3):
20 Simultaneous Evaluation of OBPM & Awake & Asleep BP for Best Predictor of Future CVD Events MAPEC Trial Pts of the same 4 groups categorized according to awake & asleep BP now additionally classified by normal vs. elevated daytime OBPM Normal daytime OBPM: <140/90 mmhg Elevated daytime OBPM: 140/90 mmhg
21 Adjusted HR of total CVD events in the MAPEC Study. Classification by clinic, awake, and asleep BP means Normal asleep BP Elevated asleep BP Adjusted HR Normal awake BP Elevated awake BP Normal awake BP Elevated awake BP Normal clinic BP Elevated clinic BP Hermida et al., J Am Coll Cardiol. 2011;58:
22
23 Diagnostic ABPM Thresholds (mmhg) ABPM-Derived Men 18 yrs Women 18 yrs Awake mean SBP DBP Asleep mean SBP DBP 70 65
24 Part III: Bedtime Hypertension Therapy to Optimize BP Control & Reduce CVD Risk Significance: Asleep SBP mean more strongly correlated with CVD event risk than awake SBP or daytime OBPM values State of art knowledge: Conventional long-acting BP-lowering medications when ingested at bedtime vs. morning are more effective in normalizing entire BP 24-hour pattern Conventional hypertension therapy ingested at bedtime substantially reduces CVD event risk
25 Ingestion-Time Differences in Effect of 6 Classes of Hypertension Therapies on Asleep BP Class Medication Dose mg No. Pts Reduction: asleep SBP/DBP mean Sleep-time relative SBP/DBP decline Awakening R x Bedtime R x Awakening R x Bedtime R x ACEIs Ramipril / /-11.5* -3.3/ /4.9* Spirapril / /-8.6* -2.5/ /4.5* ARBs Valsartan / /-13.9* 0.4/ /7.1* Telmisartan / /-9.7* -1.6/ /3.9* CCB Nifedipine GITS / /-7.8* -0.7/ /1.5 α-blocker Doxazosin GITS / / / /1.9 β-blocker Nebivolol / / / /-1.4 Diuretic Torasemide / /-8.0* -1.6/ /-0.2
26 Age, diabetes and sex-adjusted hazard ratio as a function of treatment-time (1 medication at bedtime compared to all medication upon awakening) in hypertensive subjects (MAPEC study) Primary endpoints Total events Major events* Secondary endpoints Total death Bedtime better Hazard ratio Awakening better Cardiovascular death Cerebrovascular events Cardiovascular events Heart failure Myocardial infarction Angina pectoris Occlusion retinal artery * Includes cardiovascular death, myocardial infarction, and stroke. Hermida et al. Chronobiol Int. 2010;27:
27 Conclusions Hypertension in adults should be established by 24- hour ABPM ABPM-derived asleep SBP mean -- not awake SBP mean or daytime OBPM -- most significant & independent predictor of future CVD events Elevated asleep BP & nocturnal non-dipping BP patterning increase steadily after age >45 yrs Diagnostic thresholds that differentiate elevated from normal BP appear to be lower for women than men Targeting asleep SBP by bedtime vs. upon wakening ingestion of conventional BP medications reduces CVD events substantially
28 Gaps in Knowledge It is unknown if chronic co-morbidities that disrupt sleep elevate asleep (& awake) BP & future CVD event risk It is unknown how sleep length affects asleep BP and future CVD event risk It is unknown to what extent increase of CVD events with age in women is due to misdiagnosis throughout life of elevated BP because of reliance on population & male-based SBP & DBP thresholds It is unknown if a bedtime treatment strategy entailing conventional medications is appropriate for all forms of hypertension
29 Research Questions Does asleep SBP best predict future CVD events across all races & women & men? Is incidence of elevated asleep BP & CVD risk greater in short vs. long sleepers & does it vary by race, age, & sex? Do chronic medical conditions that disrupt sleep result in elevated asleep SBP & higher CVD event risk? Do all obstructive sleep apnea & other sleepdisordered pts have elevated asleep BP & CVD risk? Do awake & asleep hypertension states entail different mechanisms, CVD event risk & is bedtime (chrono)therapy with conventional BP-lowering medications best for all types of hypertension?
30 Acknowledgements Most materials of this presentation were derived from the MAPEC outcomes trial (Ambulatory Blood Pressure Monitoring to Predict Cardiovascular Events); appreciation is extended to the primary investigators, particularly Drs. Ramon Hermida & Diana Ayala, & the many dedicated participating doctors, nursing & patients.
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION*
 Progress in Clinical Medicine 1 ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION* Keishi ABE** Asian Med. J. 44(2): 83 90, 2001 Abstract: J-MUBA was a large-scale clinical
Progress in Clinical Medicine 1 ANTIHYPERTENSIVE DRUG THERAPY IN CONSIDERATION OF CIRCADIAN BLOOD PRESSURE VARIATION* Keishi ABE** Asian Med. J. 44(2): 83 90, 2001 Abstract: J-MUBA was a large-scale clinical
Asleep blood pressure: significant prognostic marker of vascular risk and therapeutic target for prevention
 European Heart Journal (2018) 0, 1 14 doi:101093/eurheartj/ehy475 CLINICAL RESEARCH Hypertension Asleep blood pressure: significant prognostic marker of vascular risk and therapeutic target for prevention
European Heart Journal (2018) 0, 1 14 doi:101093/eurheartj/ehy475 CLINICAL RESEARCH Hypertension Asleep blood pressure: significant prognostic marker of vascular risk and therapeutic target for prevention
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Abnormalities in chronic kidney disease of ambulatory blood pressure 24 h patterning and normalization by bedtime hypertension chronotherapy
 Nephrol Dial Transplant (2014) 29: 1160 1167 doi: 10.1093/ndt/gft285 Advance Access publication 5 September 2013 Abnormalities in chronic kidney disease of ambulatory blood pressure 24 h patterning and
Nephrol Dial Transplant (2014) 29: 1160 1167 doi: 10.1093/ndt/gft285 Advance Access publication 5 September 2013 Abnormalities in chronic kidney disease of ambulatory blood pressure 24 h patterning and
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Bedtime ingestion of hypertension medications reduces the risk of new-onset type 2 diabetes: a randomised controlled trial
 DOI 10.1007/s00125-015-3749-7 ARTICLE Bedtime ingestion of hypertension medications reduces the risk of new-onset type 2 diabetes: a randomised controlled trial Ramón C. Hermida 1 & Diana E. Ayala 1 &
DOI 10.1007/s00125-015-3749-7 ARTICLE Bedtime ingestion of hypertension medications reduces the risk of new-onset type 2 diabetes: a randomised controlled trial Ramón C. Hermida 1 & Diana E. Ayala 1 &
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right. Anthony J. Viera, MD, MPH, FAHA Professor and Chair
 Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Ambulatory BP Monitoring: Getting the Diagnosis of Hypertension Right Anthony J. Viera, MD, MPH, FAHA Professor and Chair Objectives Review limitations of office BP in making a correct diagnosis of hypertension
Optimal timing for antihypertensive dosing: focus on valsartan
 REVIEW Optimal timing for antihypertensive dosing: focus on valsartan Ramón C Hermida Diana E Ayala Carlos Calvo Bioengineering & Chronobiology Laboratories, University of Vigo, Campus Universitario, Vigo,
REVIEW Optimal timing for antihypertensive dosing: focus on valsartan Ramón C Hermida Diana E Ayala Carlos Calvo Bioengineering & Chronobiology Laboratories, University of Vigo, Campus Universitario, Vigo,
The incidence of transient myocardial ischemia,
 AJH 1999;12:50S 55S Heart Rate and the Rate-Pressure Product as Determinants of Cardiovascular Risk in Patients With Hypertension William B. White Inability to supply oxygen to the myocardium when demand
AJH 1999;12:50S 55S Heart Rate and the Rate-Pressure Product as Determinants of Cardiovascular Risk in Patients With Hypertension William B. White Inability to supply oxygen to the myocardium when demand
Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations
 Acta Medica Marisiensis 2016;62(3):350-355 DOI: 10.1515/amma-2016-0038 UPDATE Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations Mako Katalin *, Ureche Corina, Jeremias Zsuzsanna University
Acta Medica Marisiensis 2016;62(3):350-355 DOI: 10.1515/amma-2016-0038 UPDATE Ambulatory Blood Pressure Monitoring Clinical Practice Recommendations Mako Katalin *, Ureche Corina, Jeremias Zsuzsanna University
Bedtime Dosing of Antihypertensive Medications Reduces Cardiovascular Risk in CKD
 Bedtime Dosing of Antihypertensive Medications Reduces Cardiovascular Risk in CKD Ramón C. Hermida, Diana E. Ayala, Artemio Mojón, and José R. Fernández Bioengineering and Chronobiology Laboratories, University
Bedtime Dosing of Antihypertensive Medications Reduces Cardiovascular Risk in CKD Ramón C. Hermida, Diana E. Ayala, Artemio Mojón, and José R. Fernández Bioengineering and Chronobiology Laboratories, University
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Blood Pressure Variability and Its Management in Hypertensive Patients
 Korean J Fam Med. 2012;33:330-335 http://dx.doi.org/10.4082/kjfm.2012.33.6.330 Blood Pressure Variability and Its Management in Hypertensive Patients Review Hee-Jeong Choi* Department of Family Medicine,
Korean J Fam Med. 2012;33:330-335 http://dx.doi.org/10.4082/kjfm.2012.33.6.330 Blood Pressure Variability and Its Management in Hypertensive Patients Review Hee-Jeong Choi* Department of Family Medicine,
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
RISE, FALL AND RESURRECTION OF RENAL DENERVATION. Michael A. Weber, MD State University of New York Downstate College of Medicine
 RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
RISE, FALL AND RESURRECTION OF RENAL DENERVATION Michael A. Weber, MD State University of New York Downstate College of Medicine Michael Weber, Disclosures Research/Trial Commitments and Consulting: Boston
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Chapter-V. Summary, Conclusions and Recommendations
 Summary, Conclusions and Recommendations INTRODUCTION The work included in this thesis entitled, Circadian heart rate and blood pressure variability in apparently healthy subjects using ABPM has been divided
Summary, Conclusions and Recommendations INTRODUCTION The work included in this thesis entitled, Circadian heart rate and blood pressure variability in apparently healthy subjects using ABPM has been divided
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls
 Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls Anthony J. Viera, MD, MPH, FAHA Department of Family Medicine Hypertension Research Program UNC School of Medicine Objectives Review limitations
Assessing Blood Pressure for Clinical Research: Pearls & Pitfalls Anthony J. Viera, MD, MPH, FAHA Department of Family Medicine Hypertension Research Program UNC School of Medicine Objectives Review limitations
Sleep-time BP: prognostic marker of type 2 diabetes and therapeutic target for prevention
 Diabetologia (2016) 59:244 254 DOI 10.1007/s00125-015-3748-8 ARTICLE Sleep-time BP: prognostic marker of type 2 diabetes and therapeutic target for prevention Ramón C. Hermida 1 & Diana E. Ayala 1 & Artemio
Diabetologia (2016) 59:244 254 DOI 10.1007/s00125-015-3748-8 ARTICLE Sleep-time BP: prognostic marker of type 2 diabetes and therapeutic target for prevention Ramón C. Hermida 1 & Diana E. Ayala 1 & Artemio
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Hypertension Guidelines 2017
 Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
State of the art treatment of hypertension: established and new drugs. Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland
 State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
State of the art treatment of hypertension: established and new drugs Prof. M. Burnier Service of Nephrology and Hypertension Lausanne, Switzerland First line therapies in hypertension ACE inhibitors AT
The hypertensive effects of the renin-angiotensin
 Comparison of Telmisartan vs. Valsartan in the Treatment of Mild to Moderate Hypertension Using Ambulatory Blood Pressure Monitoring George Bakris, MD A prospective, randomized, open-label, blinded end-point
Comparison of Telmisartan vs. Valsartan in the Treatment of Mild to Moderate Hypertension Using Ambulatory Blood Pressure Monitoring George Bakris, MD A prospective, randomized, open-label, blinded end-point
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Update on HTN and ABPM. Raj Padwal Division of General Internal Medicine University of Alberta
 Update on HTN and ABPM Raj Padwal Division of General Internal Medicine University of Alberta Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic
Update on HTN and ABPM Raj Padwal Division of General Internal Medicine University of Alberta Disclosures Funding: CIHR, AIHS, HSF, UHF Research Collaboration: Novo Nordisk, CVRx Consulting: Vivus, Medtronic
Hypertension has been defined as resistant to treatment, or
 Chronotherapy in Resistant Hypertension Chronotherapy Improves Blood Pressure Control and Reverts the Nondipper Pattern in Patients With Resistant Hypertension Ramón C. Hermida, Diana E. Ayala, José R.
Chronotherapy in Resistant Hypertension Chronotherapy Improves Blood Pressure Control and Reverts the Nondipper Pattern in Patients With Resistant Hypertension Ramón C. Hermida, Diana E. Ayala, José R.
Comparison of arbitrary definitions of circadian time periods with those determined by wrist actigraphy in analysis of ABPM data
 Journal of Human Hypertension (1999) 13, 449 453 1999 Stockton Press. All rights reserved 0950-9240/99 $12.00 http://www.stockton-press.co.uk/jhh ORIGINAL ARTICLE Comparison of arbitrary definitions of
Journal of Human Hypertension (1999) 13, 449 453 1999 Stockton Press. All rights reserved 0950-9240/99 $12.00 http://www.stockton-press.co.uk/jhh ORIGINAL ARTICLE Comparison of arbitrary definitions of
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
STATE OF THE ART BP ASSESSMENT
 STATE OF THE ART BP ASSESSMENT PROFESSOR MOLECULAR PHARMACOLOGY CONWAY INSTITUE UNIVERSITY COLLEGE DUBLIN CO-CHAIRMAN BLOOD PRESCSURE MANAGEMENT IN LOW RESOURCE SETTINGS CENTRE FOR INTERNATIONAL HUMANITARIAN
STATE OF THE ART BP ASSESSMENT PROFESSOR MOLECULAR PHARMACOLOGY CONWAY INSTITUE UNIVERSITY COLLEGE DUBLIN CO-CHAIRMAN BLOOD PRESCSURE MANAGEMENT IN LOW RESOURCE SETTINGS CENTRE FOR INTERNATIONAL HUMANITARIAN
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Is Traditional Clinic Blood Pressure Dead?
 Royal College of Physicans May 16 th 2017 Is Traditional Clinic Blood Pressure Dead? Professor Bryan Williams MD FRCP FAHA FESC Chair of Medicine UCL Director National Institute for Health Research Biomedical
Royal College of Physicans May 16 th 2017 Is Traditional Clinic Blood Pressure Dead? Professor Bryan Williams MD FRCP FAHA FESC Chair of Medicine UCL Director National Institute for Health Research Biomedical
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Chapter-IV. Blood pressure and heart rate variability as function of ovarian cycle in young women
 Blood pressure and heart rate variability as function of ovarian cycle in young women INTRODUCTION In human females, the menstrual cycle begins with the onset of menstrual flow on day 1. The menstrual
Blood pressure and heart rate variability as function of ovarian cycle in young women INTRODUCTION In human females, the menstrual cycle begins with the onset of menstrual flow on day 1. The menstrual
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Chronotherapy. Ramón C. Hermida, Diana E. Ayala
 Chronotherapy Chronotherapy With the Angiotensin-Converting Enzyme Inhibitor Ramipril in Essential Hypertension Improved Blood Pressure Control With Bedtime Dosing Ramón C. Hermida, Diana E. Ayala Abstract
Chronotherapy Chronotherapy With the Angiotensin-Converting Enzyme Inhibitor Ramipril in Essential Hypertension Improved Blood Pressure Control With Bedtime Dosing Ramón C. Hermida, Diana E. Ayala Abstract
The Association of Daytime and Nighttime Ambulatory Blood Pressure with Carotid IMT When Controlling for Daytime Physical Activity.
 The Association of Daytime and Nighttime Ambulatory Blood Pressure with Carotid IMT When Controlling for Daytime Physical Activity by Jeanette Garcia BS, University of Pittsburgh, 2004 MS, University of
The Association of Daytime and Nighttime Ambulatory Blood Pressure with Carotid IMT When Controlling for Daytime Physical Activity by Jeanette Garcia BS, University of Pittsburgh, 2004 MS, University of
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Morning Hypertension: A Pitfall of Current Hypertensive Management
 Review Article Hypertension: A Pitfall of Current Hypertensive Management JMAJ 48(5): 234 240, 2005 Kazuomi Kario* 1 Abstract has recently attracted more attention because of the close relation between
Review Article Hypertension: A Pitfall of Current Hypertensive Management JMAJ 48(5): 234 240, 2005 Kazuomi Kario* 1 Abstract has recently attracted more attention because of the close relation between
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
Dr Diana R Holdright. MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION.
 Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Dr Diana R Holdright MD, FRCP, FESC, FACC, MBBS, DA, BSc. Consultant Cardiologist HYPERTENSION www.drholdright.co.uk Blood pressure is the pressure exerted on the walls of the arteries when the heart pumps;
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Blood Pressure Targets in Diabetes
 Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Evaluation of the Extent and Duration of the ABPM Effect in Hypertensive Patients
 Journal of the American College of Cardiology Vol. 40, No. 4, 2002 2002 by the American College of Cardiology Foundation ISSN 0735-1097/02/$22.00 Published by Elsevier Science Inc. PII S0735-1097(02)02011-9
Journal of the American College of Cardiology Vol. 40, No. 4, 2002 2002 by the American College of Cardiology Foundation ISSN 0735-1097/02/$22.00 Published by Elsevier Science Inc. PII S0735-1097(02)02011-9
Prognostic significance of blood pressure measured in the office, at home and during ambulatory monitoring in older patients in general practice
 (2005) 19, 801 807 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE Prognostic significance of blood pressure measured in the office, at home and
(2005) 19, 801 807 & 2005 Nature Publishing Group All rights reserved 0950-9240/05 $30.00 www.nature.com/jhh ORIGINAL ARTICLE Prognostic significance of blood pressure measured in the office, at home and
a Hypertension and Cardiovascular Rehabilitation Unit, Faculty of Medicine, Received 2 June 2008 Revised 1 July 2008 Accepted 9 July 2008
 Original article 325 Prognostic significance of ambulatory blood pressure in hypertensive patients with history of cardiovascular disease Robert H. Fagard a, Lutgarde Thijs a, Jan A. Staessen a, Denis
Original article 325 Prognostic significance of ambulatory blood pressure in hypertensive patients with history of cardiovascular disease Robert H. Fagard a, Lutgarde Thijs a, Jan A. Staessen a, Denis
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN?
 BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN? DECLARATION OF INTEREST Medical Director and Chairman, Advisory Board dabl Ltd., Dublin, Ireland. BLOOD PRESSURE MEASUREMENT
BLOOD PRESSURE MEASUREMENT HOME BASED OR OFFICE BP MONITORING WHICH, HOW AND WHEN? DECLARATION OF INTEREST Medical Director and Chairman, Advisory Board dabl Ltd., Dublin, Ireland. BLOOD PRESSURE MEASUREMENT
Ethics/Regulatory Call with Dr. Rosenthal s Demonstration Project BPMedTime Date: May 31, 2013 MINUTES
 BPMedTime Minutes Ethics/Regulatory Call with Dr. Rosenthal s Demonstration Project BPMedTime Date: May 31, 2013 MINUTES Participants: Jeremy Sugarman (Johns Brian Gryzlak (Univ Iowa ) Barbara Wells (NIH)
BPMedTime Minutes Ethics/Regulatory Call with Dr. Rosenthal s Demonstration Project BPMedTime Date: May 31, 2013 MINUTES Participants: Jeremy Sugarman (Johns Brian Gryzlak (Univ Iowa ) Barbara Wells (NIH)
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION
 EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION Khemchandani D. 1 and * Arif A. Faruqui 2 1 Bairagarh,
EFFICACY & SAFETY OF ORAL TRIPLE DRUG COMBINATION OF TELMISARTAN, AMLODIPINE AND HYDROCHLOROTHIAZIDE IN THE MANAGEMENT OF NON-DIABETIC HYPERTENSION Khemchandani D. 1 and * Arif A. Faruqui 2 1 Bairagarh,
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Don t let the pressure get to you:
 Balanced information for better care Don t let the pressure get to you: An update on the changing recommendations for treating hypertension New trial data and guidelines have made hypertension care more
Balanced information for better care Don t let the pressure get to you: An update on the changing recommendations for treating hypertension New trial data and guidelines have made hypertension care more
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Supplement materials:
 Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
Supplement materials: Table S1: ICD-9 codes used to define prevalent comorbid conditions and incident conditions Comorbid condition ICD-9 code Hypertension 401-405 Diabetes mellitus 250.x Myocardial infarction
TIP. Documentation and coding guide. Disease definitions* Prevalence and statistics associated with HTN**
 Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Documentation and coding guide Disease definitions* HTN is diagnosed when the average of two or more (systolic of diastolic) blood pressure readings are found to be elevated on two or more office visits
Non-dipping morning blood pressure and isolated systolic hypertension in elderly
 DOI: 10.4149/BLL_2013_033 Bratisl Lek Listy 2013; 114 (3) CLINICAL STUDY Non-dipping morning blood pressure and isolated systolic hypertension in elderly Zain-El Abdin MH, Snincak M, Pahuli K, Solarova
DOI: 10.4149/BLL_2013_033 Bratisl Lek Listy 2013; 114 (3) CLINICAL STUDY Non-dipping morning blood pressure and isolated systolic hypertension in elderly Zain-El Abdin MH, Snincak M, Pahuli K, Solarova
apneabp card(x)plore ABPM-04 Ambulatory Blood Pressure Monitors & Combinations
plore ABPM-04 Ambulatory Blood Pressure Monitors & Combinations") apneabp card(x)plore ABPM-04 Ambulatory Blood Pressure Monitors & Combinations Meditech Cardiovascular Monitoring Solutions Meditech is one of the worldwide technology leaders in the area of manufacturing
apneabp card(x)plore ABPM-04 Ambulatory Blood Pressure Monitors & Combinations Meditech Cardiovascular Monitoring Solutions Meditech is one of the worldwide technology leaders in the area of manufacturing
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Patrick Kay, General and Interventional Cardiologist Auckland or healthpoint.co.nz
 Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
University of Padova, Padua, Italy, and HARVEST Study Group, Italy
 University of Padova, Padua, Italy, and HARVEST Study Group, Italy ISOLATED SYSTOLIC HYPERTENSION IN THE YOUNG DOES NOT IMPLY AN INCREASED RISK OF FUTURE HYPERTENSION NEEDING TREATMENT Mos L, Saladini
University of Padova, Padua, Italy, and HARVEST Study Group, Italy ISOLATED SYSTOLIC HYPERTENSION IN THE YOUNG DOES NOT IMPLY AN INCREASED RISK OF FUTURE HYPERTENSION NEEDING TREATMENT Mos L, Saladini