Sleep. Anil Rama, MD Medical Director, Division of Sleep Medicine The Permanente Medical Group
|
|
|
- Lucy Thompson
- 6 years ago
- Views:
Transcription
1 Sleep Anil Rama, MD Medical Director, Division of Sleep Medicine The Permanente Medical Group Assistant Adjunct Clinical Faculty Stanford School of Medicine
2 Circadian Rhythm of Sleep Body temperature 7 AM Wake Sleep 7 AM Courtesy of R. Bogan, MD. Time
3 Sleep Stages and Function (NREM) (REM) States Stage 1 Stage 2 Stage 3 Stage 4 Phasic eye movements Loss of muscle tone EEG neutral Function Body s rest and metabolic restoration Active state of brain functions in learning and memory Vander et al. Consciousness and behavior. In: Human Physiology

4
 Hobson. Sleep and Dreaming. In: Fundamental Neuroscience. 1999. Roffwarg et al. Science. 1996;152:604.")
5 Sleep and Age 24 Hours in day 16 8 REM sleep Awake NREM sleep Conception Birth Death Age (y) Hobson. Sleep and Dreaming. In: Fundamental Neuroscience Roffwarg et al. Science. 1996;152:604.
6 Sleepy cabbie.wmv
7 Epworth Sleepiness Scale (ESS) How likely are you to doze off or fall asleep in the following s ituations, in contrast to feeling just tired? This refers to your way of life in recent times. Eve n if you have not done some of these things recently, try to work out how they would have affec ted you. Use the following scale to choose the most appropriate number for each situation. 0 = would never doze 2 = moderate chance of dozing Situation 1 = slight chance of dozing 3 = high chance of dozing Chance of Dozing Sitting and reading Watching TV Sitting, inactive in a public place (eg, a theater or a meeting) As a passenger in a car for an hour without a break Lying down to rest in the afternoon when circumstances permit Sitting and talking to someone Sitting quietly after a lunch without alcohol In a car, while stopped for a few minutes in traffic Johns. Sleep. 1991;14:540.
8 Sleepiness: Clinical Presentation Pervasive drowsiness Sleep attacks Fatigue Microsleep episodes Visual disturbances Apathy Mood changes Automatic activity Impaired alertness Lethargy Impaired memory and concentration Poor performance in work/school Accident prone Overeem et al. J Clin Neurophysiol. 2001;18:78. Bassetti and Aldrich. Neurol Clin. 1996;14:545. J. Black, MD. Personal communications. October 2002.
9
10
11 The Two-process Model of Sleep Regulation Process S (Homeostatic Process) Increases during waking and decreases during sleep Process C (Circadian Process) Clock-like process that is independent of sleep and waking
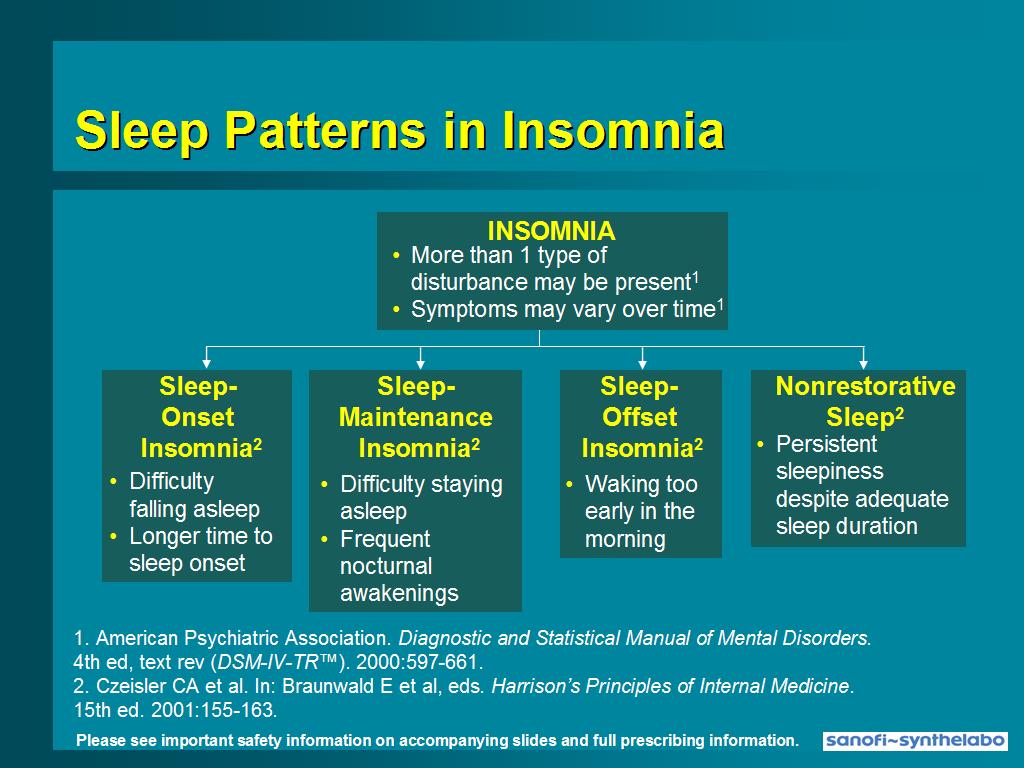
12 Insomnia: Differential Diagnosis Environmental Behavioral Psychiatric Disorders Neurological Disorders Sleep-Wake Pattern Timing Disorders Movement Disorders Respiratory Disorders Miscellaneous Medical Conditions Sleep State Misperception Idiopathic
13 Behavioral Insomnia Adjustment Sleep Disorder Psychophysiological Insomnia Inadequate Sleep Hygiene Limit-setting Sleep Disorder Sleep-onset Association Disorder
14 Psychiatric Disorders Causing Insomnia Mood Disorders Anxiety Disorders Panic Disorder Alcohol and Drug Dependency Psychoses

15 Neurological Disorders Causing Insomnia Parkinson Disease Nocturnal Epilepsy Degenerative Brain Disorders Fatal Familial Insomnia
16 Sleep-Wake Pattern Timing Disorders Causing Insomnia Time Zone Change Shift Work Delayed Sleep Phase Syndrome Advanced Sleep Phase Syndrome Non-24 Hour Sleep-Wake Syndrome Irregular Sleep-Wake Pattern Short Sleeper
17 Movement Disorders Causing Insomnia Restless Legs Syndrome Periodic Limb Movement Disorder Sleep Starts Nocturnal Seizures
18 Respiratory Disorders Causing Insomnia Obstructive Sleep Apnea Central Sleep Apnea Obesity-Hypoventilation Syndrome Nocturnal Asthma Chronic Lung Diseases High Altitude
19 Miscellaneous Medical Conditions Causing Insomnia Gastroesphageal Reflux Hyperthyroidism Fibromyalgia Pregnancy Menopause

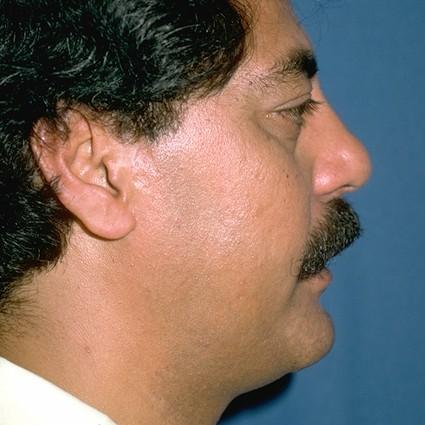
20 Craniofacial Abnormality OSA Identification

21
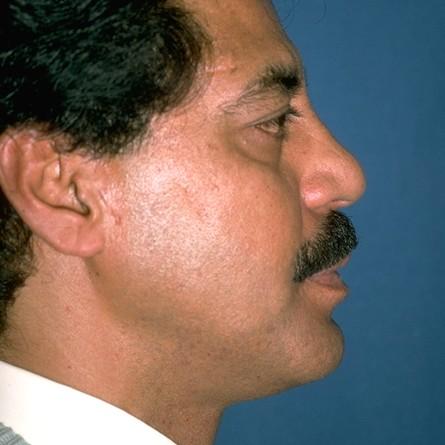
22 Maxillary/Mandibular Mandibular Advancement OSA Intervention - Surgical

23 Mandibular Repositioners OSA Intervention - Mechanical Courtesy of Sleep Disorders Dental Society
The following questions are about your sleep. Please consider both what others have told you about your sleep and what you know yourself.
 Sleep History Form FORM CODE: SLE VERSION A 1/29/2009 PARTICIPANT ID NUMBER: CONTACT YEAR: 0 9 LAST NAME: INITIALS: INSTRUCTIONS: This form should be completed during the participant's clinic visit. ID
Sleep History Form FORM CODE: SLE VERSION A 1/29/2009 PARTICIPANT ID NUMBER: CONTACT YEAR: 0 9 LAST NAME: INITIALS: INSTRUCTIONS: This form should be completed during the participant's clinic visit. ID
130 Preston Executive Drive Cary, NC Ph(919) Fax(919) Page 1 of 6. Patient History
 Fax(919) Page 1 of 6. Patient History") 130 Preston Executive Drive Cary, NC 27513 Ph(919)462-8081 Fax(919)462-8082 www.parkwaysleep.com Page 1 of 6 Patient History *Please fill out in dark BLACK INK only. General Information Name Sex: Male
130 Preston Executive Drive Cary, NC 27513 Ph(919)462-8081 Fax(919)462-8082 www.parkwaysleep.com Page 1 of 6 Patient History *Please fill out in dark BLACK INK only. General Information Name Sex: Male
Assessment of Sleep Disorders DR HUGH SELSICK
 Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Assessment of Sleep Disorders DR HUGH SELSICK Goals Understand the importance of history taking Be able to take a basic sleep history Be aware the technology used to assess sleep disorders. Understand
Sleep & Wakefulness Disorders in Parkinson s Disease: The Challenge of Getting a Good Night s Sleep
 Sleep & Wakefulness Disorders in Parkinson s Disease: The Challenge of Getting a Good Night s Sleep Helene A. Emsellem, MD March 25, 2017 The Center for Sleep & Wake Disorders PFNCA Symposium Sleep is
Sleep & Wakefulness Disorders in Parkinson s Disease: The Challenge of Getting a Good Night s Sleep Helene A. Emsellem, MD March 25, 2017 The Center for Sleep & Wake Disorders PFNCA Symposium Sleep is
PULMONARY & CRITICAL CARE CONSULTANTS OF AUSTIN 1305 West 34 th Street, Suite 400, Austin, TX Phone: Fax:
 Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
Sleep Center. Have you had a previous sleep study? Yes No If so, when and where? Name of facility Address
 Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Balboa Island Dentistry (949)
") Do You Snore? Are you always tired? Snoring is no laughing matter! It may be more than an annoying habit. It may be a sign of. How well do you sleep? Just about everyone snores occasionally. Even a baby
Do You Snore? Are you always tired? Snoring is no laughing matter! It may be more than an annoying habit. It may be a sign of. How well do you sleep? Just about everyone snores occasionally. Even a baby
Help I Have Problems with My Sleep!
 Help I Have Problems with My Sleep! Over An 85 Year Lifespan Sleep 31% Work 21% Exercise 1% Food and Drink 11% Sleep Is Important! You can survive without food for up to 2 months Without water 3-5 days
Help I Have Problems with My Sleep! Over An 85 Year Lifespan Sleep 31% Work 21% Exercise 1% Food and Drink 11% Sleep Is Important! You can survive without food for up to 2 months Without water 3-5 days
Associated Neurological Specialties and Sleep Disorder Center
 Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Sleep Disorders Diagnostic Center 9733 Healthway Drive, Berlin, MD , ext. 5118
 Sleep Questionnaire *Please complete the following as accurate as possible. Please bring your completed questionnaire, insurance card, photo ID, Pre-Authorization and/or Insurance referral form, and all
Sleep Questionnaire *Please complete the following as accurate as possible. Please bring your completed questionnaire, insurance card, photo ID, Pre-Authorization and/or Insurance referral form, and all
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS
 WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
PATIENT DEMOGRAPHICS
 PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
Patient Information. Name: Date of Birth: Address: Number & Street City State Zip Code. Home Number: ( ) Cell Number: ( )
 Cell Number: ( )") Patient Information Name: Date of Birth: Age: Address: Number & Street City State Zip Code Home Number: ( ) Cell Number: ( ) Social Security Number: Marital Status: Religion: Race: Height: Weight: Sex:
Patient Information Name: Date of Birth: Age: Address: Number & Street City State Zip Code Home Number: ( ) Cell Number: ( ) Social Security Number: Marital Status: Religion: Race: Height: Weight: Sex:
Sleep History Questionnaire
 Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
New Patient Sleep Intake
 New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
Sleep Medicine Questionnaire
 Please bring this completed questionnaire with you to your sleep medicine appointment. Our sleep medicine staff strives to understand your sleep symptoms, which may be complex in nature. Thank you for
Please bring this completed questionnaire with you to your sleep medicine appointment. Our sleep medicine staff strives to understand your sleep symptoms, which may be complex in nature. Thank you for
Sleep Questionnaire Name: Sex: Age: Da te: Da te of birth: Height: Weight: Neck siz e: Ref erring Physician: Primary Car e MD:
 www.myvcmf.com 1133 E. Stanley Blvd., Suite 101 Livermore, CA 94550 925 454-4280 5725 W. Las Positas Blvd., Suite 110 Pleasanton, CA 94588 925-416-6767 Sleep Questionnaire Name: Sex: Age: Da te: Da te
www.myvcmf.com 1133 E. Stanley Blvd., Suite 101 Livermore, CA 94550 925 454-4280 5725 W. Las Positas Blvd., Suite 110 Pleasanton, CA 94588 925-416-6767 Sleep Questionnaire Name: Sex: Age: Da te: Da te
PATIENT QUESTIONNAIRE Boise Location 7272 W. Potomac Drive Boise, ID (208)
") PATIENT QUESTIONNAIRE Boise Location 7272 W. Potomac Drive Boise, ID 83704 (208)884-2922 ***Questionnaire MUST be completed PRIOR to arrival for appointment*** Today s Date / / / / Last First MI DOB Referring
PATIENT QUESTIONNAIRE Boise Location 7272 W. Potomac Drive Boise, ID 83704 (208)884-2922 ***Questionnaire MUST be completed PRIOR to arrival for appointment*** Today s Date / / / / Last First MI DOB Referring
Sleep Center New Patient Questionnaire
 For office use only Appt date: Sleep Center Clinician: Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 #1 respiratory hospital
For office use only Appt date: Sleep Center Clinician: Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 #1 respiratory hospital
Intake Questionnaire
 Intake Questionnaire In order to make the best use of your appointment time, please complete this form prior to your initial appointment. What is your name? (Who filled in this form?) (Y= yes N=no DK=
Intake Questionnaire In order to make the best use of your appointment time, please complete this form prior to your initial appointment. What is your name? (Who filled in this form?) (Y= yes N=no DK=
1960 FP CENTER FOR SLEEP DISORDERS
 1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
Sleep Symptoms & History
 Sleep Symptoms & History In your own words, please tell us what brings you to the sleep clinic today? How long have you been experiencing your sleep problems? yrs. mos. To give us a precise understanding
Sleep Symptoms & History In your own words, please tell us what brings you to the sleep clinic today? How long have you been experiencing your sleep problems? yrs. mos. To give us a precise understanding
Emergency Contact Information Name: Phone: Address: Employer Information Employer Name: Address/Street: City: Zip: Phone: Fax:
 SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SLEEP DISORDERS CENTER QUESTIONNAIRE
 Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
Treating Insomnia in Primary Care. Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team
 Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
What s the name of your position?
 What s the name of your position? What are some basic work responsibilities (e.g primarily front desk/administration, light lifting or heavy liftingplease indicate pounds)? CONSENT FORM FOR USE AND DISCLOSURE
What s the name of your position? What are some basic work responsibilities (e.g primarily front desk/administration, light lifting or heavy liftingplease indicate pounds)? CONSENT FORM FOR USE AND DISCLOSURE
Sleep History Questionnaire. Sleep Disorders Center Duke University Medical Center. General Information. Age: Sex: F M (select one)
") Sleep History Questionnaire Sleep Disorders Center Duke University Medical Center Part I: General Information Name: Address: Date: Phone: Age: Sex: F M (select one) Education (years of school): Occupation:
Sleep History Questionnaire Sleep Disorders Center Duke University Medical Center Part I: General Information Name: Address: Date: Phone: Age: Sex: F M (select one) Education (years of school): Occupation:
Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine
 Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine PATIENT DEMOGRAPHICS Who is the Physician that referred you to us? Who is the primary care Physician? Date: Do you want this report
Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine PATIENT DEMOGRAPHICS Who is the Physician that referred you to us? Who is the primary care Physician? Date: Do you want this report
Littleton, CO Welcome Packet 8151 Southpark Lane, Suite 200 Littleton, CO 80120
 Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk PATIENT QUESTIONNAIRE
 THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk 55 Frid Street, Unit 7, Hamilton, Ontario L8P 4M3 Phone:905-529-2259 Fax: 905-529-2262 282 Linwell Road, Suite 118, St. Catharines, Ontario
THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk 55 Frid Street, Unit 7, Hamilton, Ontario L8P 4M3 Phone:905-529-2259 Fax: 905-529-2262 282 Linwell Road, Suite 118, St. Catharines, Ontario
Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy
![Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy](/thumbs/96/127246551.jpg "Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy") Health Benefits Employee Services HBE Preventive Health - Sleep Assessment Form Please bring your completed assessment form to your appointment. To schedule an appointment please call 505 844-HBES (4237).
Health Benefits Employee Services HBE Preventive Health - Sleep Assessment Form Please bring your completed assessment form to your appointment. To schedule an appointment please call 505 844-HBES (4237).
Denver, CO Welcome Packet
 Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Sleep History Questionnaire B/P / Pulse: Neck Circum Wgt: Pulse Ox
 2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
Pre-Test Questionnaire. Name: Sex: Age: Date of Birth: Height: ft. in. Weight: lbs Gain? Loss? of lbs over
 Pre-Test Questionnaire Date: Hospital # (Please Print) Name: Sex: Age: Date of Birth: Height: ft. in. Weight: lbs Gain? Loss? of lbs over Chief Complaints What problem(s) brings you to sleep disorders
Pre-Test Questionnaire Date: Hospital # (Please Print) Name: Sex: Age: Date of Birth: Height: ft. in. Weight: lbs Gain? Loss? of lbs over Chief Complaints What problem(s) brings you to sleep disorders
PEDIATRIC SLEEP EVALUATION
 PEDIATRIC SLEEP EVALUATION Directions: Please answer each of the following questions by writing in or choosing the best answer. This will help us know more about your family and your child. CHILD S INFORMATION
PEDIATRIC SLEEP EVALUATION Directions: Please answer each of the following questions by writing in or choosing the best answer. This will help us know more about your family and your child. CHILD S INFORMATION
Baptist Health Floyd 1850 State Street New Albany, IN Sleep Disorders Center Lung & Sleep Specialists. Date of Birth: Age:
 Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Robert E. McMichael, M.D. Medical Director Patient Instructions for a Diagnostic Sleep Study
 NORTH TEXAS SLEEP DISORDERS CENTER Neurology Associates of Arlington, P.A 811 West Interstate 20, Suite G12 Arlington, Texas 76017 (817) 419-6375 Fax (817) 419-6371 Robert E. McMichael, M.D. Medical Director
NORTH TEXAS SLEEP DISORDERS CENTER Neurology Associates of Arlington, P.A 811 West Interstate 20, Suite G12 Arlington, Texas 76017 (817) 419-6375 Fax (817) 419-6371 Robert E. McMichael, M.D. Medical Director
Home Sleep Testing Questionnaire
 Home Sleep Testing Questionnaire Patient Name: DOB: / / Gender: Male Female Study Date: / / Marital Status: Married Cohabitate Single Divorced Widow/Widower Email: Phone: Height: Weight: Neck Size: What
Home Sleep Testing Questionnaire Patient Name: DOB: / / Gender: Male Female Study Date: / / Marital Status: Married Cohabitate Single Divorced Widow/Widower Email: Phone: Height: Weight: Neck Size: What
Huron Medical Sleep Center Saad S. Ahmad, MD
 Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
Patient Adult Information History
 Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Sleep History Questionnaire
 Location South Loop Katy Steeplechase Fort Bend NAME ADDRESS PHONE SEX DOB AGE HEIGHT WEIGHT NECK COLLAR SIZE (inches) Do you have difficulty falling asleep? Is your sleep restless or disturbed? Do you
Location South Loop Katy Steeplechase Fort Bend NAME ADDRESS PHONE SEX DOB AGE HEIGHT WEIGHT NECK COLLAR SIZE (inches) Do you have difficulty falling asleep? Is your sleep restless or disturbed? Do you
604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA SLEEP HISTORY QUESTIONNAIRE
 604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA 70301 985-493-4759 SLEEP HISTORY QUESTIONNAIRE DATE: / / NAME: AGE (First) (Middle) (Last) ADDRESS: (Street) (City) (State) (Zip) PHONE: Home( ) Work:( )
604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA 70301 985-493-4759 SLEEP HISTORY QUESTIONNAIRE DATE: / / NAME: AGE (First) (Middle) (Last) ADDRESS: (Street) (City) (State) (Zip) PHONE: Home( ) Work:( )
SLEEP HISTORY QUESTIONNAIRE
 Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
I would like for my patient to be seen in Sleep Medicine consultation and managed by the sleep physician. Yes No
 701 E. COUNTY LINE ROAD, SUITE 207. GREENWOOD, IN. 46143 OFFICE317-887-6400 FAX 317-887-6500 indianasleepcenter.com REFERRAL FOR SLEEP EVALUATION Patient Name:_ Phone: I would like for my patient to be
701 E. COUNTY LINE ROAD, SUITE 207. GREENWOOD, IN. 46143 OFFICE317-887-6400 FAX 317-887-6500 indianasleepcenter.com REFERRAL FOR SLEEP EVALUATION Patient Name:_ Phone: I would like for my patient to be
General Information. Name Age Date of Birth. Address Apt. # City State Zip. Home Phone Work Phone. Social Security Number Marital Status
 Accredited Member Center of The American Academy of Sleep Medicine 400 Riverside Drive, Suite 1500, Bourbonnais, IL 60914 Phone (815) 933-2874 Fax (815) 939-9413 www.riversidemc.net/sleep General Information
Accredited Member Center of The American Academy of Sleep Medicine 400 Riverside Drive, Suite 1500, Bourbonnais, IL 60914 Phone (815) 933-2874 Fax (815) 939-9413 www.riversidemc.net/sleep General Information
PATIENT SLEEP QUESTIONNAIRE
 PATIENT SLEEP QUESTIONNAIRE Name: Date of Birth: Today s Date Primary Care Physician Telephone # Physician ordering test (Other than PCP): Physician s Tel. #: _ Age: Years Height: Feet Inches Weight: Lb
PATIENT SLEEP QUESTIONNAIRE Name: Date of Birth: Today s Date Primary Care Physician Telephone # Physician ordering test (Other than PCP): Physician s Tel. #: _ Age: Years Height: Feet Inches Weight: Lb
Occupation: Usual Work Hours/Days: Referring Physician: Family Physician (PCP): Marital status: Single Married Divorced Widowed
: Marital status: Single Married Divorced Widowed") Name Social Security No. Last First MI Address Phone No. ( ) City State Zip Secondary No. ( ) Date of Birth Sex (M/F) Race Email County Primary Care Marital Status Single Divorced Married Widowed Employer
Name Social Security No. Last First MI Address Phone No. ( ) City State Zip Secondary No. ( ) Date of Birth Sex (M/F) Race Email County Primary Care Marital Status Single Divorced Married Widowed Employer
Huron Medical Sleep Center Saad S. Ahmad, MD
 Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
PATIENT REGISTRATION PERSON TO NOTIFY IN CASE OF EMERGENCY. Name: Relationship: Phone:
 PATIENT REGISTRATION Patient's Name (Last, First, MI): Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: Employment Status:
PATIENT REGISTRATION Patient's Name (Last, First, MI): Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: Employment Status:
493 Blackwell Road, Suite 317-A, Warrenton, VA
 493 Blackwell Road, Suite 317-A, Warrenton, VA. 20186 Dear Sleep Study Patient, Attached is the patient questionnaire for your sleep study. Please complete and mail or fax the enclosed forms as soon as
493 Blackwell Road, Suite 317-A, Warrenton, VA. 20186 Dear Sleep Study Patient, Attached is the patient questionnaire for your sleep study. Please complete and mail or fax the enclosed forms as soon as
Patient Medical History
 Date: The PMA Metabolic and Bariatric Weight Management Center 410 West Linfield-Trappe Road, Suite 100 Limerick, PA 19468 (610) 495-2338 Patient Medical History Name: Date of Birth: Age: Female Male ALLERGIES:
Date: The PMA Metabolic and Bariatric Weight Management Center 410 West Linfield-Trappe Road, Suite 100 Limerick, PA 19468 (610) 495-2338 Patient Medical History Name: Date of Birth: Age: Female Male ALLERGIES:
PATIENT NAME: M.R. #: ACCT #: HOME TEL: WORK TEL: AGE: D.O.B.: OCCUPATION: HEIGHT: WEIGHT: NECK SIZE: GENDER EMERGENCY CONTACT: RELATIONSHIP: TEL:
 SLEEP DISORDERS INSTITUTE HOSPITAL: DePaul Building Street Address City, State Zip Tel: (202) 555-1212 Fax: (202) 555-1212 SLEEP QUESTIONNAIRE PATIENT NAME: M.R. #: ACCT #: STREET ADDRESS: CITY: STATE:
SLEEP DISORDERS INSTITUTE HOSPITAL: DePaul Building Street Address City, State Zip Tel: (202) 555-1212 Fax: (202) 555-1212 SLEEP QUESTIONNAIRE PATIENT NAME: M.R. #: ACCT #: STREET ADDRESS: CITY: STATE:
Sleep Medicine. Maintenance of Certification Examination Blueprint. Purpose of the exam
 Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
The Implications of a Hospital Break Policy: A Comparison of Two Regional Hospitals Using Survey Data
 The Implications of a Hospital Break Policy: A Comparison of Two Regional Hospitals Using Survey Data Samantha M. Riedy, BS, RPSGT Experimental Psychology Doctoral Program Sleep and Performance Research
The Implications of a Hospital Break Policy: A Comparison of Two Regional Hospitals Using Survey Data Samantha M. Riedy, BS, RPSGT Experimental Psychology Doctoral Program Sleep and Performance Research
PATIENT REGISTRATION PERSON TO NOTIFY IN CASE OF EMERGENCY. Name: Relationship: Phone:
 PATIENT REGISTRATION Patient's Name (Last, First, MI): Date Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: PERSON TO NOTIFY
PATIENT REGISTRATION Patient's Name (Last, First, MI): Date Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: PERSON TO NOTIFY
Room # Critical Care & Pulmonary Consultants, P.C.
 Room # Critical Care & Pulmonary Consultants, P.C. Health History You have been scheduled for an appointment with Critical Care and Pulmonary Consultants, P.C. This health history will help us facilitate
Room # Critical Care & Pulmonary Consultants, P.C. Health History You have been scheduled for an appointment with Critical Care and Pulmonary Consultants, P.C. This health history will help us facilitate
MESA EXAM 5 ANCILLARY STUDY 113 SLEEP QUESTIONNAIRE DATA SET VARIABLE GUIDE
 MESA EXAM 5 ANCILLARY STUDY 113 SLEEP QUESTIONNAIRE DATA SET VARIABLE GUIDE Data Set name : Principal Investigator : Contact Information : MESAe5_SleepQ_20140617 Susan Redline sredline1@rics.bwh.harvard.edu
MESA EXAM 5 ANCILLARY STUDY 113 SLEEP QUESTIONNAIRE DATA SET VARIABLE GUIDE Data Set name : Principal Investigator : Contact Information : MESAe5_SleepQ_20140617 Susan Redline sredline1@rics.bwh.harvard.edu
Sleep apnea. What is sleep apnea? What are the symptoms of sleep apnea? Symptoms during the day. Symptoms during sleep
 Sleep apnea Your doctor thinks you may have sleep apnea. The purpose of this fact sheet is to inform you about this disease. It also gives you details about the tests done to diagnose it and possible treatments.
Sleep apnea Your doctor thinks you may have sleep apnea. The purpose of this fact sheet is to inform you about this disease. It also gives you details about the tests done to diagnose it and possible treatments.
Original Sleep Hygiene Rules*
 Original Sleep Hygiene Rules* 1. Sleep as much as needed to feel refreshed and healthy during the following day, but not more. Curtailing time in bed a bit seems to solidify sleep; excessively long times
Original Sleep Hygiene Rules* 1. Sleep as much as needed to feel refreshed and healthy during the following day, but not more. Curtailing time in bed a bit seems to solidify sleep; excessively long times
Tallahassee Memorial Sleep Center Patient Questionnaire
 Tallahassee Memorial Sleep Center Patient Questionnaire Name _ Age Date Date of Birth Sex Height ft in Weight lbs Neck size inches (If known) Body Mass Index (BMI) (If known) Phone(s) (home) (work) (cell)
Tallahassee Memorial Sleep Center Patient Questionnaire Name _ Age Date Date of Birth Sex Height ft in Weight lbs Neck size inches (If known) Body Mass Index (BMI) (If known) Phone(s) (home) (work) (cell)
SLEEP STUDY - PATIENT QUESTIONNAIRE
 NOTE: You cannot fill out this form on Mozilla Firefox, please try another browser. You have two options for completing a questionnaire: - Enter the information on the fillable PDF and click Print at the
NOTE: You cannot fill out this form on Mozilla Firefox, please try another browser. You have two options for completing a questionnaire: - Enter the information on the fillable PDF and click Print at the
EPWORTH SLEEPINESS SCALE
 EPWORTH SLEEPINESS SCALE Name: Sponsors last 4 of SSN#: DOB: Today s Date: Age (years): Gender (circle): MALE FEMALE How likely are you to doze off or fall asleep in the following situation, in contrast
EPWORTH SLEEPINESS SCALE Name: Sponsors last 4 of SSN#: DOB: Today s Date: Age (years): Gender (circle): MALE FEMALE How likely are you to doze off or fall asleep in the following situation, in contrast
Sleep Disorders The Effect on our Lives Every Day
 Sleep Disorders The Effect on our Lives Every Day Julie Hatleli, RN Sheri Krenz, RN Regional Sleep Disorders Center-Mankato, MN 2016 MFMER slide-1 Agenda Sleep Stages Sleep Apnea Sleep Disorders DOT requirements
Sleep Disorders The Effect on our Lives Every Day Julie Hatleli, RN Sheri Krenz, RN Regional Sleep Disorders Center-Mankato, MN 2016 MFMER slide-1 Agenda Sleep Stages Sleep Apnea Sleep Disorders DOT requirements
Please complete the following questionnaire by filling in the blanks and placing a check in appropriate areas. For how many months/years?
 St. Louis Heart and Vascular - McKelvey Office May 28, 2018 (Page 1) Please complete the following questionnaire by filling in the blanks and placing a check in appropriate areas. Today s Date: My Main
St. Louis Heart and Vascular - McKelvey Office May 28, 2018 (Page 1) Please complete the following questionnaire by filling in the blanks and placing a check in appropriate areas. Today s Date: My Main
Telephone: Fax:
 PATIENT AUTHORIZATION TO RELEASE MEDICAL RECORDS AND DEMOGRAPHIC INFORMATION DATE: SS #: PATIENT NAME: BIRTHDATE: / / PATIENT ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE #: CELL PHONE #: REFERRING PHYSICIAN
PATIENT AUTHORIZATION TO RELEASE MEDICAL RECORDS AND DEMOGRAPHIC INFORMATION DATE: SS #: PATIENT NAME: BIRTHDATE: / / PATIENT ADDRESS: CITY: STATE: ZIP CODE: HOME PHONE #: CELL PHONE #: REFERRING PHYSICIAN
Maintenance for Wakefulness Testing (MWT)
") Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness Testing (MWT) will begin on the morning of at 7 a.m. and will end at 5 p.m. ARRIVAL TIME: If you are not able to arrive
Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness Testing (MWT) will begin on the morning of at 7 a.m. and will end at 5 p.m. ARRIVAL TIME: If you are not able to arrive
Sleep Medicine Maintenance of Certification Examination Blueprint
 Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Sleep Medicine Maintenance of Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
*521634* Sleep History Questionnaire. Name of primary care doctor:
 *521634* Today s Date: Sleep History Questionnaire Appointment Date: Please answer the following questions before coming to your appointment. Please arrive 15 minutes early with this packet filled out.
*521634* Today s Date: Sleep History Questionnaire Appointment Date: Please answer the following questions before coming to your appointment. Please arrive 15 minutes early with this packet filled out.
Maintenance for Wakefulness Testing (MWT)
") SLEEP DISORDERS CENTER St. Joseph Mercy Ann Arbor 5305 Elliott Drive, Ypsilanti, MI 48197 734-712-2276 / Fax 734-712-2967 Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness
SLEEP DISORDERS CENTER St. Joseph Mercy Ann Arbor 5305 Elliott Drive, Ypsilanti, MI 48197 734-712-2276 / Fax 734-712-2967 Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness
Psychological Sleep Services Sleep Assessment
 Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Management of OSA in the Acute Care Environment. Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018
 Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
Management of OSA in the Acute Care Environment Robert S. Campbell, RRT FAARC HRC, Philips Healthcare May, 2018 1 Learning Objectives Upon completion, the participant should be able to: Understand pathology
SLEEP SCREENING QUESTIONNAIRE
 SLEEP SCREENING QUESTIONNAIRE Please answer each question accurately and to the best of your knowledge, to help us obtain an accurate picture of your health and sleep issues, only this way will we be able
SLEEP SCREENING QUESTIONNAIRE Please answer each question accurately and to the best of your knowledge, to help us obtain an accurate picture of your health and sleep issues, only this way will we be able
DESERT CENTER FOR ALLERGY AND CHEST DISEASES HEALTH QUESTIONAIRE NAME. PAST MEDICAL PROBLEMS- Check mark if you have any of the following
 DESERT CENTER FOR ALLERGY AND CHEST DISEASES Pulmonary Medicine, Allergy/Immunology, Sleep Disorders Pulmonary Rehabilitation, Pulmonary Function Laboratory HEALTH QUESTIONAIRE NAME What is your presenting
DESERT CENTER FOR ALLERGY AND CHEST DISEASES Pulmonary Medicine, Allergy/Immunology, Sleep Disorders Pulmonary Rehabilitation, Pulmonary Function Laboratory HEALTH QUESTIONAIRE NAME What is your presenting
Please answer as many ques ons as you can before your ini al visit to EvergreenHealth Sleep Services.
 Please answer as many ques ons as you can before your ini al visit to EvergreenHealth Sleep Services. Pa ent Iden fica on: Pa ent name: Date: Age: Date of birth: Who is filling out this ques onnaire? Please
Please answer as many ques ons as you can before your ini al visit to EvergreenHealth Sleep Services. Pa ent Iden fica on: Pa ent name: Date: Age: Date of birth: Who is filling out this ques onnaire? Please
MLA HASS LUNG. SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA Phone: Fax:
 MLA HASS LUNG SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA 01453 Phone: 978-728-4641 Fax: 978-978-1382 MEICAL IRECTOR: Payam Aghassi, M, FCCP Thank you for your sleep study order! Attached
MLA HASS LUNG SLEEP CENTER, Leominster Campus 100 Erdman Way, Leomjnster, MA 01453 Phone: 978-728-4641 Fax: 978-978-1382 MEICAL IRECTOR: Payam Aghassi, M, FCCP Thank you for your sleep study order! Attached
Medical History Questionnaire
 Medical History Questionnaire OFFICE USE Patient ID: FORM DATE: / / NAME: DATE OF BIRTH: / / Allergens No known allergens Iodine Plastic Antibiotics Latex Sedatives Aspirin Local anesthetics Sleeping pills
Medical History Questionnaire OFFICE USE Patient ID: FORM DATE: / / NAME: DATE OF BIRTH: / / Allergens No known allergens Iodine Plastic Antibiotics Latex Sedatives Aspirin Local anesthetics Sleeping pills
Patient History & Sleep Questionnaire
 Patient History & Sleep Questionnaire Patient Full Name: Nick Name: Birth date: Age: Sex: Height: Current Weight: Weight Five Years Ago: Peak Lifetime Weight: Marital Status: Single Married Divorced Widowed
Patient History & Sleep Questionnaire Patient Full Name: Nick Name: Birth date: Age: Sex: Height: Current Weight: Weight Five Years Ago: Peak Lifetime Weight: Marital Status: Single Married Divorced Widowed
ANNUAL FOLLOW-UP QUESTIONNAIRE
 SLEEP HEART HEALTH STUDY - TUCSON ANNUAL FOLLOW-UP QUESTIONNAIRE - 2003 Dear Sleep Heart Health Study participant: Today s Date: / / Month Day Year Please take the time to complete and return this short
SLEEP HEART HEALTH STUDY - TUCSON ANNUAL FOLLOW-UP QUESTIONNAIRE - 2003 Dear Sleep Heart Health Study participant: Today s Date: / / Month Day Year Please take the time to complete and return this short
Sleep Diordered Breathing (Part 1)
") Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Questionnaire. 2. How long has this problem bothered you? My Main Sleep Complaints: - Trouble sleeping at night For how many months/ years?
 Onslow Medical Specialties Clinic Lung Diseases & Sleep Disorders Clinic Pulmonary Function Test/ CardioPulmonary Exercise Test/ Thoracic Ultrasound Methacholine Challenge Test/ Video-Flexible Laryngoscopy/
Onslow Medical Specialties Clinic Lung Diseases & Sleep Disorders Clinic Pulmonary Function Test/ CardioPulmonary Exercise Test/ Thoracic Ultrasound Methacholine Challenge Test/ Video-Flexible Laryngoscopy/
Sweet Dreams. Guide to Getting a Good Night s Sleep
 Sweet Dreams Guide to Getting a Good Night s Sleep Objectives Learn sleep facts, common myths about sleep, and the consequences of sleep deprivation Discover how sleep works and what interferes with sleeping
Sweet Dreams Guide to Getting a Good Night s Sleep Objectives Learn sleep facts, common myths about sleep, and the consequences of sleep deprivation Discover how sleep works and what interferes with sleeping
PEDIATRIC HISTORY FORM
 Lehigh Valley Health Network Pediatric Sleep Center PEDIATRIC HISTORY FORM Please answer the following questions frankly and accurately by filling in the blank or checking/circling the appropriate answer.
Lehigh Valley Health Network Pediatric Sleep Center PEDIATRIC HISTORY FORM Please answer the following questions frankly and accurately by filling in the blank or checking/circling the appropriate answer.
Instructions. If you make a mistake, put an "X" over the checkmark. Then put a checkmark in the correct box and draw a circle around that box.
 SLEEP HEART HEALTH STUDY SLEEP HABITS AND LIFESTYLE QUESTIONNAIRE Instructions Thank you for taking time to fill out the enclosed Sleep Habits Questionnaire. Please fill out the form completely. You may
SLEEP HEART HEALTH STUDY SLEEP HABITS AND LIFESTYLE QUESTIONNAIRE Instructions Thank you for taking time to fill out the enclosed Sleep Habits Questionnaire. Please fill out the form completely. You may
WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA
 WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA Wayne Driscoll Clinical Education Specialist 2 SLEEP APNEA IN THE NEWS Carrie Fisher died from sleep apnea, other factors, coroner says USA Today NJ Transit engineer
WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA Wayne Driscoll Clinical Education Specialist 2 SLEEP APNEA IN THE NEWS Carrie Fisher died from sleep apnea, other factors, coroner says USA Today NJ Transit engineer
Huron Medical Sleep Center Saad S. Ahmad, MD
 Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE
 VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE Name:_ DOB: MR#: Date: Sex: Age: Height: Referring physician: Primary care physician: What is your primary sleep problem? Please explain any strange
VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE Name:_ DOB: MR#: Date: Sex: Age: Height: Referring physician: Primary care physician: What is your primary sleep problem? Please explain any strange
Sleep Disorders and their management
 Clinical Stream Sleep Disorders and their management Dr Alex Bartle Programme. What happens in sleep, and why bother? The effects of sleep loss. Common sleep disorders Brief (but important ) questions.
Clinical Stream Sleep Disorders and their management Dr Alex Bartle Programme. What happens in sleep, and why bother? The effects of sleep loss. Common sleep disorders Brief (but important ) questions.
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS
 SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
Sleep Screening Questionnaire
 Version: SLPQV1 Sleep Screening Questionnaire OFFICE USE Patient ID: NAME: CURRENT DATE: / / DATE OF BIRTH: / / MALE FEMALE Referring Physician: Contact ID: Number Number #1 = the most severe symptom #1
Version: SLPQV1 Sleep Screening Questionnaire OFFICE USE Patient ID: NAME: CURRENT DATE: / / DATE OF BIRTH: / / MALE FEMALE Referring Physician: Contact ID: Number Number #1 = the most severe symptom #1
Rex Surgical Specialist (Bariatric Office)
") Rex Surgical Specialist (Bariatric Office) Medical History Information Today s Date Name DOB Referring Physician phone_ Primary Care Physician phone_ Office Office Medical History (Please Mark all that
Rex Surgical Specialist (Bariatric Office) Medical History Information Today s Date Name DOB Referring Physician phone_ Primary Care Physician phone_ Office Office Medical History (Please Mark all that
Types of Sleep Studies 8/28/2018. Ronald S. Prehn, ThM, DDS. Type 1 Attended in-lab polysomnography (PSG) 18 leads
 18 leads") Ronald S. Prehn, ThM, DDS rprehn@tmjtexas.com Board Certified in Dental Sleep Medicine Board Certified in Orofacial Pain Types of Sleep Studies Type 1 Attended in-lab polysomnography (PSG) 18 leads Type
Ronald S. Prehn, ThM, DDS rprehn@tmjtexas.com Board Certified in Dental Sleep Medicine Board Certified in Orofacial Pain Types of Sleep Studies Type 1 Attended in-lab polysomnography (PSG) 18 leads Type
Sweet Dreams: The Relationship between Sleep Health and Your Weight
 Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
HYPERSOMNIA NEW PATIENT QUESTIONNAIRE please fax back to us at : Current Medications:
 HYPERSOMNIA NEW PATIENT QUESTIONNAIRE please fax back to us at 404-712-8145: Name: Date: Date of Birth: Sex: M F (circle) Height: Weight: Current Medications: At what age did your sleepiness begin? years
HYPERSOMNIA NEW PATIENT QUESTIONNAIRE please fax back to us at 404-712-8145: Name: Date: Date of Birth: Sex: M F (circle) Height: Weight: Current Medications: At what age did your sleepiness begin? years
Your physician has ordered a sleep study for you on. Your arrival time is scheduled for.
 Dear Patient: Your physician has ordered a sleep study for you on. Your arrival time is scheduled for. The Texas State Sleep Lab is located in the Health Professions Building on the Texas State University
Dear Patient: Your physician has ordered a sleep study for you on. Your arrival time is scheduled for. The Texas State Sleep Lab is located in the Health Professions Building on the Texas State University
MICHIGAN INSTITUTE FOR SLEEP MEDICINE NEW PATIENT SLEEP QUESTIONNAIRE. Name: Date of Birth: / / Age: Sex: Address: City: Zip:
 MICHIGAN INSTITUTE FOR SLEEP MEDICINE NEW PATIENT SLEEP QUESTIONNAIRE *Please bring copies of any recent Blood Work and Physician Sleep Referral Order* Please answer every question to the best of your
MICHIGAN INSTITUTE FOR SLEEP MEDICINE NEW PATIENT SLEEP QUESTIONNAIRE *Please bring copies of any recent Blood Work and Physician Sleep Referral Order* Please answer every question to the best of your
A Medical Approach to Sleep Disorders in School-Aged Children and Adolescents.
 A Medical Approach to Sleep Disorders in School-Aged Children and Adolescents. Akinyemi Ajayi, MD, FAAP, FCCP, D,ABSM, FAASM. Children s Lung, Asthma and Sleep Specialists Children s Sleep Laboratory Sleep
A Medical Approach to Sleep Disorders in School-Aged Children and Adolescents. Akinyemi Ajayi, MD, FAAP, FCCP, D,ABSM, FAASM. Children s Lung, Asthma and Sleep Specialists Children s Sleep Laboratory Sleep
Nash Sleep Disorders Center 250 Medical Arts Mall Suite C Rocky Mount NC Phone: Fax:
 Appointment Date: Arrival Time: *Please give at least 24 hour notice if you are unable to keep your appointment or need to reschedule. 1. Patients will need to bring pictured identification, insurance
Appointment Date: Arrival Time: *Please give at least 24 hour notice if you are unable to keep your appointment or need to reschedule. 1. Patients will need to bring pictured identification, insurance
BMI: Family physician : Neck circumference (cm) Hypertension + 4 cm Snoring + 3 cm Witnessed apnea + 3cm Total
 Hypertension + 4 cm Snoring + 3 cm Witnessed apnea + 3cm Total") Last and first names: F M Date: Date of birth: / / YYYY MM DD Weight: kg /lbs Profession/job: Height: _ cm /ft.in. BMI:_ Family physician : ANC (adjusted neck circumference) : Neck circumference (cm) Hypertension
Last and first names: F M Date: Date of birth: / / YYYY MM DD Weight: kg /lbs Profession/job: Height: _ cm /ft.in. BMI:_ Family physician : ANC (adjusted neck circumference) : Neck circumference (cm) Hypertension