Case presentation. Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD
|
|
|
- Augusta Patrick
- 6 years ago
- Views:
Transcription
1 Case presentation Dr Connie Haley, MD, MPH Dr Gautam Kalyatanda, MD
2 History of presenting illness 20 Year old woman from Nigeria who came to study at Montgomery in August 2013 About 2 weeks after arriving, she presented to student health, complaining of a cough for a week. Cough was productive with white colored sputum. She was initially given amoxcillin with very little improvement
3 History of presenting illness Her cough got worse and she found it hard to sleep at night Episodes of vomiting associated with bouts of cough Had an episode of hemoptysis about 4-5 weeks after these episodes began Low grade fevers more at night Occasional night sweats Weight loss
4 She had been having some shortness of breath for about 3 years prior to the start of these symptoms. Shortness of breath was progressively getting worse She would be Short of breath with minimal exertion Positive for pleurophasic pain
5 Social history Lived in Lagos 8 siblings No known exposure to anyone with active tuberculosis Worked as a primary school teacher Father passed away in 2008.
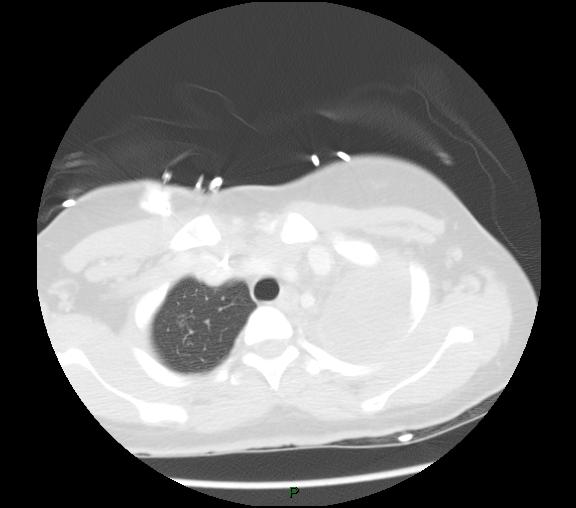
6 Had a chest x-ray after about 6 weeks due to persistence of these symptoms

7 Oct 7, 2013
8 Sputum AFB obtained: positive.
9 Would we start her on therapy
10 Begun on standard 4 drug antituberculous therapy: Isoniazid Rifampin Pyrazinamide Ethambutol

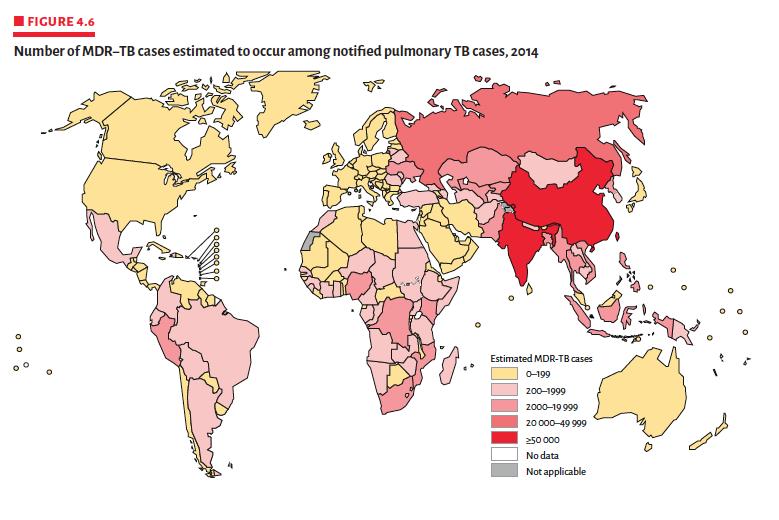
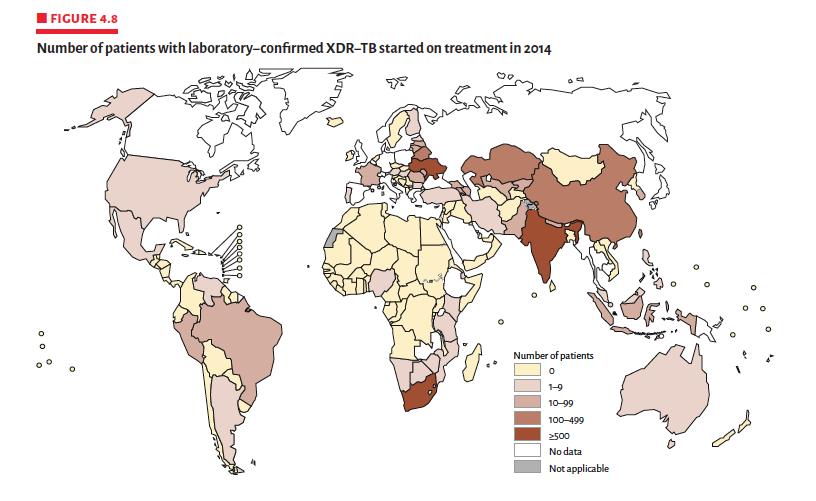
11 Nigeria WHO. Global TB Report,

12 Tuberculosis in Nigeria 2014 WHO Global TB Report Nigeria 4 th highest TB burden country WHO. Global TB Report,
13 WHO. Global TB Report,
14 WHO. Global TB Report,
15 GeneXpert result: M. tuberculosis complex with rifampin resistance (rpob mutation) Sample sent to CDC for molecular susceptibilities Patient removed from dorm, placed in hotel under isolation (quarantine) awaiting transfer to UAB for admission
16 What would we do now
17 CDC Molecular Detection of Drug Resistance (MDDR): INH: katg (Ser315Thr: complete INH resist) RIF: 2 rpob mutations not previously seen in CDC database (Asp516Glu, Ser522Leu) Oflox: gyra D94G (Asp94Gly)??? EMB: embb (Pro404Ser) 79% EMB resistant isolates have a mutation other than this one but cannot rule out if this mutation causes resistance (ie true mutation vs. polymorphism) No mutations seen in AG s (rrs, eis, tlya loci) PZA (pnca) loci examined no mutations found
18 Date : 10/07/13 PZA 100mcg/ml Streptomycin 20mcg/ml Streptomycin 10mcg/ml INH 2 mcg/ml INH 10mcg/ml Rif 10mcg/ml Ethambutol 50mcg/ml Kanamycin 50mcg/ml Ofloxacin 20mcg/ml Susceptibility S Possible R S Possible R Possible R Possible R Possible R S Possible R
19 Locus Result Interpretation Rpo B InhA( promoter) No mutation Likely rifampin resistance KatG AGC>ACC INH resistance EmbB CCG>TCG Can not rule out resistance pnca GGC>GAC Effect of this mutation on PZA unknown gyra Rrs No mutation Ofloxacin resistant Els No mutation Can not rule out resistance tya No mutation
20 What type of drug resistance is this?
21 By definition, she has multidrug resistant (MDR) TB Resistance to at least INH and Rifampin Extensively drug resistant (XDR)-TB is defined as MDR-TB plus additional resistance to a fluoroquinolone and a 2 nd line injectable (amikacin or capreomycin) Since she has one of the two XDR-TB criteria, she would be classified as pre-xdr-tb
22 What drugs would we use now
23 Began MDR-TB regimen (7 drugs): Amikacin 750mg (IV) 5 days/week Ethambutol 1200mg/daily PZA 1500mg/daily Rifabutin 300mg/daily Moxifloxacin 400mg/daily Ethionamide 750mg/daily (after ramp up) Cycloserine 250mg/daily (awaiting shipment) Vitamin B6 200mg/daily
24 10/21/13: AL state lab reports phenotypic high level ethambutol resistance and low level streptomycin resistance 11/14/13: CDC lab reports resistance to rifabutin Ethambutol and rifabutin discontinued and regimen modified:
25 Adjusted Regimen (7 Drugs) Capreomycin 750mg 5 days/wk Moxifloxacin 400mg/daily PZA 1500mg/daily Ethionamide 750mg/daily (after ramp up) Cycloserine 250mg/daily PAS 8 grams daily (after ramp up) Linezolid 600mg daily Vit B6 200mg/daily
26 Progress AFB smears went from numerous to 1+ in 2 weeks on MDR regimen AFB smear negative x 4 into 3rd week with (ultimately) negative cultures (initial cultures time to growth 7-10 days) Patient discharged from hospital after 1 month, placed in long term hotel Therapeutic drug monitoring (TDM): serum drug levels checked and found in range Weight increased from 112 to 125 pounds
27 Drug levels Drug levels in 12/13 are as follows Ethionamide 0.26 and 0.89mcg/ml Cycloserine 20 and 18. 5mcg/ml Moxifloxacin 2.63 and 3.08 mcg/ml Capreomycin 3.53 and 2.38mcg/ml Linezolid and 9.81 mcg/ml PZA mcg/ml PAS and mcg/ml Ethionamide 1.58 and 0.89 mcg/ml
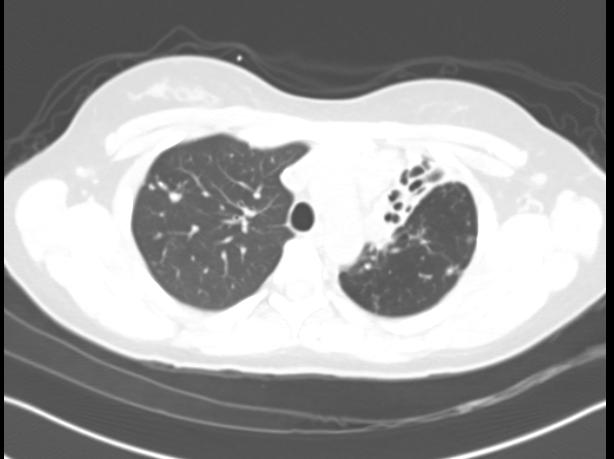
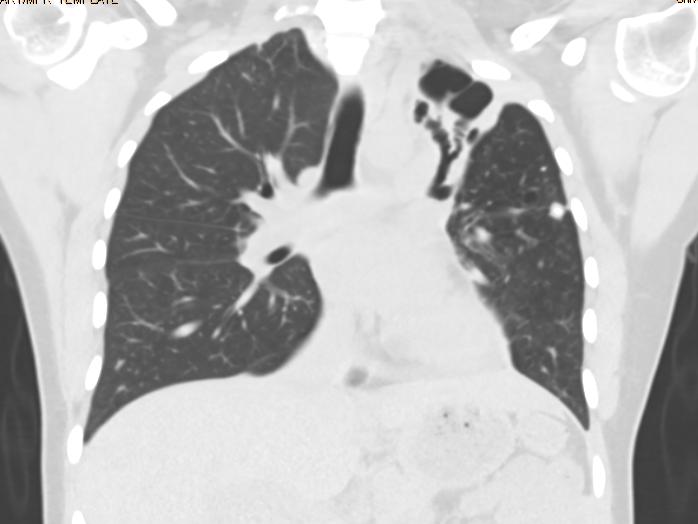
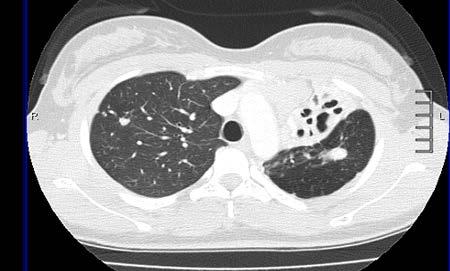
28 CXR after 2 months of MDR-TB therapy


29 Initial 2 months therapy
30 Patient completed 5 and ½ months of capreomycin, had challenges with PICC line related to severe tape/adhesive allergy and line coming out Continuation phase 5 drugs: Moxifloxacin PZA Ethionamide Cycloserine Linezolid Completed 16 months total therapy, having 15 months of negative cultures

31 Closing CXR Jan 21, 2015
32 One month later she began to complain of a cough for which she was treated with azithromycin with immediate resolution of her symptoms
33 She had a chest xray done which showed consolidation of the left lung apex.
34 Would you start her on therapy now? TB vs Pneumonia?
35 Sputum was smear negative but culture positive for MTb
36 Repeat MDDR results (3/12/2015) Received 4/3/2015, reported 4/6/2015. Identical to initial (primary) isolate except with addition of pnca promoter mutation of uncertain significance: Effect of this mutation on PZA resistance is not known. Cannot rule out PZA resistance
37 Course at Shands Admitted to the hospital on 4/9/2015 Airborne isolation in negative pressure room. On admission she had no shortness of breath, cough or fever Was clinically stable on admission
38 GPE General examination: No cyanosis, clubbing, pallor or icterus HEENT: No posterior pharyngeal wall congestion, Sinus tenderness or lymphadenopathy CVS: Normal with no murmurs or gallops RS: PA: NAD. No hepatospleenomegaly Musculoskeletal: No joint effusions or pain Skin: No rashes or ulcers Neurological: NAD
39 Labs performed prior to therapy Audiology consult- Normal Ekg: Normal with no Qtc prolongation
40 Medications Medications started on 4/10/2015 Linezolid Capremomycin Cycloserine Pyrazinamide Vitamin B6 Imipenem
41 Ethionamide was started on 4/20 and sequentially increased to full dose( 500mg at night and 250mg in the morning on 4/27)
42 Port placed on 4/13. Had a rash at the Port site secondary to the dressing which resolved with the use of a steroid cream local application
43 Pyrazinamide discontinued on 4/27 after strain showed resistance
44 Course With an increase in her creatinine, the dose of Capreomycin was held on 5/8 and then changed to thrice weekly after 5/11.
45 Side effects Diziness associated with Capreomycin infusion Improved with 500ml NS infusion soon after Capreomycin infusion Intractable nausea and vomiting associated with PAS and Ethionamide( missed a few doses of her medication) Ativan was given with minimal improvement Zofran and Reglan with minimal improvement Olanzapine given but discontinued after a day with significant side effects like dry mouth and diziness
46 What would you do to relieve the nausea in this patient?
47 Marked improvement after Gtube was placed on 5/11
48 Was depressed, lonely and anxious Was followed by clinical psychology at Shands( felt this was acute stress reaction) Would take walks outside the hospital with Social service Daily meeting with social service Pastoral care Had problems with appetite especially since she was used to a different diet Improved and patient had a weight gain of about 4 Lbs at the end of her hospitalization
49 Bedaquiline started after G tube was placed on 5/12 at 400mg po daily After G tube was placed all her medications were crushed and given through her G tube except for Bedaquiline
50 Course complicated by Hypomagnesia and Hypokalemia for which she required K and Mag replacement Mag replaced on 4/21, 4/28, 4/29, 4/30, 5/15, 5/17, 5/18 and 5/19
51 Date 4/9/15 4/20/15 4/24/15 4/28/15 5/5/2015 5/8/2015 5/12/15 5/15/15 Na K Cl Creat Glu Ca TP Alb AST ALT T bili Alk Phos Mag
52 Date 4/9/15 4/20/15 5/5/15 5/14/15 5/18/15 Wbc Hb Hct Platelet Mcv Neutr Lympho Monocytes eosinophils
53 Date 5/15/2015 Free T TSH 2.00
54 Drug levels Drug Date Dose / time given Concentration Concentration normal Linezolid 4/22/ mg po daily given at 10:00 AM 32.28mcg/ml at 1200 hrs 12.37mcg/ml at 1600 hrs 12-26mcg 2 hours after oral dose/ trough 3-9mcg/ml Linezolid 5/1/ mg po daily given at 11:00 AM 14.35mcg/ml at 13: 15 hrs 13.20mcg/ml at 17: 15hrs
55 Drug levels Drug Date Dose /time given Capreomycin 4/16/ gm IV daily/ Concentration Concentration Normal 22.14mcg/ml at 04:30am 5.73mcg/ml at 08:46 am 35-45mcg/ml
56 Drug levels Drug Date Dose/ time given Conentration Concentration Normal Cycloserine 4/22/ mg po daily/ 23.0mcg/ml at 12:00hrs 15.1mcg/ml at 1600 hrs 20-35mcg/ml after 2 hrs PAS 5/1/2015 4gms po BID/ ETA 5/1/ mg po daily (PM) 3.50mcg/ml 7.38mcg/ml 20-60mcg/ml 6 hrs after dose 1.21mcg/ml 0.57mcg/ml Peak level 1-5mcg/ml PZA 4/22/ mg po daily given at mcg/ml at 1200 hrs 38.98mcg/ml at 1600 hrs 29-60mcg/ml 2 hours after oral dose
57 Discharge medications Imipenem 1gm IV BID Capreomycin 1gm three times a week Mon, Wed and Friday. Cycloserine 250mg through G tube daily Linezolid 600mg through G tube daily Bedaquiline 400mg po daily until 5/26/2015 and then 200mg po three times a week( patient needs to swallow this medicine) Ethionamide 250mg through G tube in the morning and 500mg through the G tube at night PAS 4 gms twice a day through the G tube Vit B6 200mg po daily through G tube Give 500ml NS over 60 minutes
58 Any role for surgery?
59
60
61 Denver Discussions between SNTC, Denver and Alabama Department of Health Travelled to NJH and University of Colorado saw Drs. Gwen Huitt and John Mitchell Underwent left upper lobectomy 7/29 (3 months of negative cx s) Ultimately cultures of resected lung were negative for AFB

62 8/24/15
63 8/24/15
64 Drug levels Although initial TDM revealed adequate serum drug levels, repeat levels are low for several drugs: Ethionamide 0.49 (1-5) Cycloserine (20-35) PAS trace (20-60) Linezolid 6.85 (12-26) Cycloserine was increased but she was unable to tolerate increasing ethionamide dose Repeat levels are pending

65 /24/15
66 Port infection- pseudomonas- required removal of port, with placement of PICC Remains in school, continues to excel academically
67 The biggest disease today is not leprosy or tuberculosis, but rather the feeling of being unwanted. - Mother Teresa
Managing Complex TB Cases Diana M. Nilsen, MD, RN
 Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
Managing Complex TB Cases Diana M. Nilsen, MD, RN Director of Medical Affairs NYC Department of Health & Mental Hygiene Bureau of TB Control Case #1 You are managing a patient who was seen at a private
CDC s Approach to Fast Track Laboratory Diagnosis for Persons at Risk of Drug Resistant TB: Molecular Detection of Drug Resistance (MDDR) Service
 Service") CDC s Approach to Fast Track Laboratory Diagnosis for Persons at Risk of Drug Resistant TB: Molecular Detection of Drug Resistance (MDDR) Service Beverly Metchock, DrPH, D(ABMM) Team Lead, Reference Laboratory
CDC s Approach to Fast Track Laboratory Diagnosis for Persons at Risk of Drug Resistant TB: Molecular Detection of Drug Resistance (MDDR) Service Beverly Metchock, DrPH, D(ABMM) Team Lead, Reference Laboratory
Analysis. Answers. Action. Saturday Night Fever. Shaka Brown Capital Congress
 Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Saturday Night Fever Shaka Brown Capital Congress Shaka Zulu October 31, 2012 SICK SUCKS How my illness started October 2013 August to October 2013 Symptoms: Severe fatigue Night sweats Low grade fever
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
Patient History 1. Patient History 2. Social History. The Role of Surgery in the Management of TB. Reynard McDonald, MD & Paul Bolanowski, MD
 Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Patient History 1 The Role of Surgery in the Management of TB Reynard McDonald, MD & Paul Bolanowski, MD September 16, 2010 42 y/o AA male was initially diagnosed with pansensitive pulmonary TB in 1986
Recognizing MDR-TB in Children. Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention February 2016
 Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Recognizing MDR-TB in Children Ma. Cecilia G. Ama, MD 23 rd PIDSP Annual Convention 17-18 February 2016 Objectives Review the definitions and categorization of drugresistant tuberculosis Understand the
Mycobacteria Diagnostic Testing in Manitoba. Dr. Michelle Alfa Medical Director, DSM Clin Micro Discipline
 Mycobacteria Diagnostic Testing in Manitoba Dr. Michelle Alfa Medical Director, DSM Clin Micro Discipline Acknowlegements: Assunta Rendina: Charge Tech HSC Lab Joyce Wolf & Dr. Meenu Sharma: NML Dr. Kanchana
Mycobacteria Diagnostic Testing in Manitoba Dr. Michelle Alfa Medical Director, DSM Clin Micro Discipline Acknowlegements: Assunta Rendina: Charge Tech HSC Lab Joyce Wolf & Dr. Meenu Sharma: NML Dr. Kanchana
Anti Tuberculosis Medications: Side Effects & adverse Events
 Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Anti Tuberculosis Medications: Side Effects & adverse Events Diana Fortune, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Diana Fortune, RN,
Laboratory Diagnosis for MDR TB
 Laboratory Diagnosis for MDR TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination California Department of Public Health Guam March 07 Objectives Describe
Laboratory Diagnosis for MDR TB Neha Shah MD MPH Centers for Disease Control and Prevention Division of Tuberculosis Elimination California Department of Public Health Guam March 07 Objectives Describe
Management of MDR TB. Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore
 Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
Management of MDR TB Dr Priscilla Rupali MD; DTM&H Professor and Head Department of Infectious Diseases Christian Medical College Vellore Outline Global epidemiology of Tuberculosis Epidemiology of Tuberculosis
Treatment of Active Tuberculosis
 Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Treatment of Active Tuberculosis Jeremy Clain, MD Pulmonary & Critical Care Medicine Mayo Clinic October 16, 2017 2014 MFMER slide-1 Disclosures No relevant financial relationships No conflicts of interest
Surgery for MDR/XDR Tuberculosis
 Surgery for MDR/XDR Tuberculosis John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief, General Thoracic Surgery Department of Surgery University of Colorado School of Medicine
Surgery for MDR/XDR Tuberculosis John D. Mitchell, M.D. Davis Endowed Chair in Thoracic Surgery Professor and Chief, General Thoracic Surgery Department of Surgery University of Colorado School of Medicine
Diagnosis of drug resistant TB
 Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Diagnosis of drug resistant TB Megan Murray, MD, ScD Harvard School of Public Health Brigham and Women s Hospital Harvard Medical School Broad Institute Global burden of TB 9 million new cases year 2 million
Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist, NH GEISELMED.DARTMOUTH.EDU GEISELMED.DARTMOUTH.
 The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
The image part with relationship ID rid2 was not found in the file. MDR TB Management Review of the Evolution (or Revolution?) Elizabeth A. Talbot MD Assoc Professor, ID and Int l Health Deputy State Epidemiologist,
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2014
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2014 The Critical First Step Consider TB in the Differential 1. Risks
Case Presentations Part 2
 Case Presentations Part 2 Connie A. Haley, MD MPH University of Florida, Infectious Diseases and Global Medicine Megan Ninneman, PA Jackson Memorial Hospital, Miami FL Objectives Demonstrate the ability
Case Presentations Part 2 Connie A. Haley, MD MPH University of Florida, Infectious Diseases and Global Medicine Megan Ninneman, PA Jackson Memorial Hospital, Miami FL Objectives Demonstrate the ability
TB Grand Rounds. Reynard McDonald, MD & Henry Fraimow, MD January 30, Outline
 TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
TB Grand Rounds Reynard McDonald, MD & Henry Fraimow, MD January 30, 2007 Outline Overview of 2006 ATS statement regarding hepatotoxicity of anti-tb therapy Case examples highlighting management of patients
Debbie Onofre, RN, BSN March 18, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Managing and Monitoring Side Effects and Toxicities of Anti TB Therapy Debbie Onofre, RN, BSN March 18, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Mitnick CD, Shin SS, Seung KJ, et al. Comprehensive treatment
Treatment of Tuberculosis
 TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
TB Clinical i l Intensive Seattle Treatment of Tuberculosis June 16, 2016 Masa Narita, MD Public Health Seattle & King County; Firland Northwest TB Center, University of Washington Outline Unique features
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Drug Side Effects and Toxicity
 Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
Drug Side Effects and Toxicity Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Toxicity Nausea and vomiting Any Drug Can Cause
TB Clinical Guidelines: Revision Highlights March 2014
 TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
TB Clinical Guidelines: Revision Highlights March 2014 AIR TRAVEL & TB CONTROL With respect to non-ambulance air travel of patients diagnosed with or suspected as having active Mycobacterium tuberculosis,
Rapid Diagnosis and Detection of Drug Resistance in Tuberculosis
 Rapid Diagnosis and Detection of Drug Resistance in Tuberculosis YAM Wing-Cheong 任永昌 Department of Microbiology The University of Hong Kong Tuberculosis Re-emerging problem in industrialized countries
Rapid Diagnosis and Detection of Drug Resistance in Tuberculosis YAM Wing-Cheong 任永昌 Department of Microbiology The University of Hong Kong Tuberculosis Re-emerging problem in industrialized countries
Drug susceptibility testing for tuberculosis KRISTEN DICKS, MD, MPH DUKE UNIVERSITY MEDICAL CENTER
 Drug susceptibility testing for tuberculosis KRISTEN DICKS, MD, MPH DUKE UNIVERSITY MEDICAL CENTER Outline Drug resistant TB: definitions and epidemiology How does TB become resistant? Current drug susceptibility
Drug susceptibility testing for tuberculosis KRISTEN DICKS, MD, MPH DUKE UNIVERSITY MEDICAL CENTER Outline Drug resistant TB: definitions and epidemiology How does TB become resistant? Current drug susceptibility
WELCOME. Lab Talk: What a Nurse Hears. April 18, NTNC Annual Meeting Lab Talk: What a Nurse Hears
 Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
Lab Talk: What a Lab Talk: What a Max Salfinger, MD, FIDSA, FAAM Executive Director, Advanced Diagnostic Laboratories Laboratory Director, Mycobacteriology & Pharmacokinetics National Jewish Health Lisa
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
Advanced Concepts in Pediatric TB: Treatment of Tuberculosis Disease Jeffrey R. Starke, M.D. Professor of Pediatrics Baylor College of Medicine [with help from Andrea Cruz, M.D.] Objectives At the end
TB Nurse Case Management. March 7-9, Diagnosis of TB: Ken Jost Wednesday March 7, 2012
 TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7-9, 2012 Diagnosis of TB: Laboratory Ken Jost Wednesday March 7, 2012 Ken Jost has the following disclosures to make: No conflict of interests No relevant
Tuberculosis: update 2013
 Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
Tuberculosis: update 2013 William R. Bishai, MD, PhD Center for TB Research Division of Infectious Diseases Department of Medicine Johns Hopkins School of Medicine Question 1 A TB speaker at a major conference
DRUG SIDE EFFECTS AND TOXICITY
 DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
DRUG SIDE EFFECTS AND TOXICITY Gwen A. Huitt, MD MS Professor, Division of Mycobacterial and Respiratory Infections National Jewish Health Disclosures None Objectives After participating in this lecture,
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
MULTIDRUG- RESISTANT TUBERCULOSIS. Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic
 MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
MULTIDRUG- RESISTANT TUBERCULOSIS Dean Tsukayama Hennepin County Medical Center Hennepin County Public Health Clinic I have no relevant financial relationships. Discussion includes off label use of: amikacin
Pediatric TB Intensive San Antonio, Texas October 14, 2013
 Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Pediatric TB Intensive San Antonio, Texas October 14, 2013 Treatment of Tuberculosis in Children Jeffrey R. Starke, M.D. Professor of Pediatrics October 14, 2013 Jeffrey R. Starke, M.D. has the following
Laboratory s Role in the Battle Against Drug Resistant Tuberculosis
 Laboratory s Role in the Battle Against Drug Resistant Tuberculosis Angela M. Starks, Ph.D. Chief, Laboratory Branch Division of Tuberculosis Elimination June 6, 2016 National Center for HIV/AIDS, Viral
Laboratory s Role in the Battle Against Drug Resistant Tuberculosis Angela M. Starks, Ph.D. Chief, Laboratory Branch Division of Tuberculosis Elimination June 6, 2016 National Center for HIV/AIDS, Viral
Role of Surgery in the Management of TB. Lee Reichman, MD & Paul Bolanowski, MD
 Role of Surgery in the Management of TB Lee Reichman, MD & Paul Bolanowski, MD Patient Background Patient is a 19 year old Bolivian female who immigrated to the US in February 2002 On 3/20/02, she presenting
Role of Surgery in the Management of TB Lee Reichman, MD & Paul Bolanowski, MD Patient Background Patient is a 19 year old Bolivian female who immigrated to the US in February 2002 On 3/20/02, she presenting
Optimising patient care in MDR TB with existing molecular screening tests in high burden countries
 Optimising patient care in MDR TB with existing molecular screening tests in high burden countries Camilla Rodrigues MD Consultant Microbiologist Hinduja Hospital,India Outline What is the best empiric
Optimising patient care in MDR TB with existing molecular screening tests in high burden countries Camilla Rodrigues MD Consultant Microbiologist Hinduja Hospital,India Outline What is the best empiric
WSLH Testing and Surveillance Updates
 WSLH Testing and Surveillance Updates Wisconsin Mycobacteriology Laboratory Network annual conference November 4, 2015, Madison, WI Updates Outline Collection and Transport Smear and Culture Nucleic Acid
WSLH Testing and Surveillance Updates Wisconsin Mycobacteriology Laboratory Network annual conference November 4, 2015, Madison, WI Updates Outline Collection and Transport Smear and Culture Nucleic Acid
Maha R Farhat, MD MSc Massachusetts General Hospital Harvard Medical School. I have no financial or other potential conflicts of interest to disclose
 Maha R Farhat, MD MSc Massachusetts General Hospital Harvard Medical School I have no financial or other potential conflicts of interest to disclose Update on the epidemiology of TB drug resistance Success
Maha R Farhat, MD MSc Massachusetts General Hospital Harvard Medical School I have no financial or other potential conflicts of interest to disclose Update on the epidemiology of TB drug resistance Success
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Intensive San Antonio, Texas November 11 14, 2014 Diagnosis of TB: Laboratory Ken Jost, BA November 12, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
Etiological Agent: Pulmonary Tuberculosis. Debra Mercer BSN, RN, RRT. Definition
 Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
Pulmonary Tuberculosis Debra Mercer BSN, RN, RRT Definition Tuberculosis is a contagious bacterial infection of the lungs caused by Mycobacterium Tuberculosis (TB) Etiological Agent: Mycobacterium Tuberculosis
The ABC s of AFB s Laboratory Testing for Tuberculosis. Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory
 The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
The ABC s of AFB s Laboratory Testing for Tuberculosis Gary Budnick Connecticut Department of Public Health Mycobacteriology Laboratory Laboratory TAT Goals Case Study Specimen Collection Testing Contact
Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer
 Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Tuberculosis in the 21 st Century Scott Lindquist MD MPH Tuberculosis Medical Consultant Washington State DOH and Kitsap County Health Officer Feedback Poll In my opinion, the recent media coverage of
Laboratory Diagnosis and Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis Complex. Objectives
 Laboratory Diagnosis and Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis Complex Marie-Claire Rowlinson, PhD D(ABMM) Calin Chiribau, PhD, MT(ASCP) Florida Bureau of Public Health Laboratories
Laboratory Diagnosis and Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis Complex Marie-Claire Rowlinson, PhD D(ABMM) Calin Chiribau, PhD, MT(ASCP) Florida Bureau of Public Health Laboratories
Managing the Patients Response to TB Treatment
 Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
Managing the Patients Response to TB Treatment Barbarah Martinez, RN, BSN September 13, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Barbarah Martinez, RN, BSN has
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE NOVEMBER 1-4, 2016 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1.
Management of MDR TB in special situations. Dr Sarabjit Chadha The Union
 Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Management of MDR TB in special situations Dr Sarabjit Chadha The Union MDR TB in special situations Pregnancy Breastfeeding Contraception Renal Insufficiency Diabetes Pregnancy and TB Pregnancy is not
Patient Background. Role of Surgery in the Management of TB. Patient Background CXR 3/20/02
 Patient Background Role of Surgery in the Management of TB Patient is a 19 year old Bolivian female who immigrated to the US in February 2002 On 3/20/02, she presenting to a hospital with complaints of
Patient Background Role of Surgery in the Management of TB Patient is a 19 year old Bolivian female who immigrated to the US in February 2002 On 3/20/02, she presenting to a hospital with complaints of
Treatment of Tuberculosis
 Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Treatment of Tuberculosis, 1940 s Treatment of Tuberculosis ATS/CDC/IDSA Joint Statement 2003 Saskatchewan Lung Association Outline, 2012 Treatment of Tuberculosis Principles of treatment of tuberculosis
Stacy White, PhD May 12, TB for Community Providers. Phoenix, Arizona
 Role of the Laboratory in TB Diagnosis Stacy White, PhD May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Stacy White, PhD has the following disclosures
Role of the Laboratory in TB Diagnosis Stacy White, PhD May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Stacy White, PhD has the following disclosures
DNA FINGERPRINTING. Barry N. Kreiswirth, PhD Director, PHRI TB Center
 DNA FINGERPRINTING Barry N. Kreiswirth, PhD Director, PHRI TB Center Molecular Epidemiology Local Epidemiology Are M. tuberculosis isolates recovered from localized cases of disease the same or different
DNA FINGERPRINTING Barry N. Kreiswirth, PhD Director, PHRI TB Center Molecular Epidemiology Local Epidemiology Are M. tuberculosis isolates recovered from localized cases of disease the same or different
TB for the Intensivist-Update on the Diagnosis and Management of the TB Patient in the ICU
 TB for the Intensivist-Update on the Diagnosis and Management of the TB Patient in the ICU David Ashkin, M.D., F.C.C.P. Medical Director, Southeastern National Tuberculosis Center Florida TB Medical Director,
TB for the Intensivist-Update on the Diagnosis and Management of the TB Patient in the ICU David Ashkin, M.D., F.C.C.P. Medical Director, Southeastern National Tuberculosis Center Florida TB Medical Director,
Property of Presenter. Not for Reproduction DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS
 DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
DENVER TB COURSE: CHALLENGING CLINICAL PRESENTATIONS Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES No relevant financial relationships OBJECTIVES
6/8/2018 TB TREATMENT. Bijan Ghassemieh, MD Seattle TB Clinical Intensive Disclosures. None
 TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
TB TREATMENT Bijan Ghassemieh, MD Seattle TB Clinical Intensive 2018 Disclosures None 1 Objectives Understand the following Rationale and goals for standard TB regimen When to initiate TB treatment Standard
The Molecular Epidemiology of Tuberculosis
 The Molecular Epidemiology of Tuberculosis Barry N. Kreiswirth,, PhD Director, PHRI TB Center Airborne pathogen, Mycobacterium tuberculosis Slow grower; doubles 24hrs; 3-4 weeks to culture 3-4 weeks for
The Molecular Epidemiology of Tuberculosis Barry N. Kreiswirth,, PhD Director, PHRI TB Center Airborne pathogen, Mycobacterium tuberculosis Slow grower; doubles 24hrs; 3-4 weeks to culture 3-4 weeks for
Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013 Ken Jost has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 Diagnosis of TB: Laboratory Ken Jost Tuesday April 9, 2013 Ken Jost has the following disclosures to make: No conflict of interests No relevant
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016
 Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
Dose Counting Exercise Elizabeth Foy, RN, BSN September 8, 2016 TB Nurse Case Management September 7-9, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed., has the following disclosures
PROBLEMS IN TX CASE STUDY. JB is a 42 yo BM who was admitted to
 Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE
Why TB Drugs Fail Part 2 Why TB Drugs Fail OR How We Fail TB Drugs (and Tb Patients) 1 PROBLEMS IN TX FAILURE TO RESPOND TB MENINGITIS RENAL FAILURE HEPATITIS CAN T SWALLOW PILLS GI INTOLERANCE ADVERSE
SA TB Guidelines The interface with Advanced Clinical Care
 SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
SA TB Guidelines The interface with Advanced Clinical Care Dr Kogie Naidoo (MBCHB, PHD) Head: CAPRISA Treatment Research Programme Honorary Lecturer - UKZN Department of Public Heath Medicine Annual Workshop
Update on Management of
 Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Update on Management of DR TB Definitions Presumptive MDR-TB A patient suspected of drug-resistant TB, based on RNTCP criteria for submission of specimens for drug-susceptibility testing MDR-TB Case A
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Treatment of Tuberculosis
 Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Treatment of Tuberculosis Marcos Burgos, MD April 5, 2016 TB Intensive April 5 8, 2016 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures to make: No conflict
Research in Tuberculosis: Translation into Practice
 Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Case History Research in Tuberculosis: Translation into Practice This is a 6-year6 year-old Bosnian male, who presented to ER with one-week history of fever and occasional vomiting. No cough, difficulty
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Managing Anti-TB Therapy Side Effects and Complications Lisa Armitige, MD, PhD May 9, 2012 Lisa Armitige, MD, PhD has the following
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Managing Anti-TB Therapy Side Effects and Complications Lisa Armitige, MD, PhD May 9, 2012 Lisa Armitige, MD, PhD has the following
Utilizing All the Tools in the TB Toolbox
 Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Utilizing All the Tools in the TB Toolbox Sandra Morano, B.A., R.N. Public Health Nurse, City of Stamford, CT TB Talk The New England TB Consortium March 18, 2010 Background TB Program, City of Stamford,
Marcos Burgos, MD has the following disclosures to make:
 Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Guidelines for the Treatment of Tuberculosis Marcos Burgos, MD May 13, 2015 TB for Pulmonologist March 13, 2015 Phoenix, AZ EXCELLENCE EXPERTISE INNOVATION Marcos Burgos, MD has the following disclosures
Failure to Implement the Plan to Eliminate TB in the US: Implications in the Era of Declining Resources
 Failure to Implement the Plan to Eliminate TB in the US: Implications in the Era of Declining Resources Sustaining Public Health Capacity in an Age of Austerity Forum on Microbial Threats Board on Global
Failure to Implement the Plan to Eliminate TB in the US: Implications in the Era of Declining Resources Sustaining Public Health Capacity in an Age of Austerity Forum on Microbial Threats Board on Global
Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014
 TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 LTBI and TB Disease Treatment Cara Christ, MD, MS May 8, 2012 Cara Christ, MD, MS has the following disclosures to make: No conflict
TB Nurse Case Management San Antonio, Texas April 9-11, 2013
 TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, Texas April 9-11, 2013 TB / Dose Counting Rachel Munoz, RN. TB Nurse Case Manager/Nurse Consultant Austin/Travis County Health Department April 10, 2013 Rachel Munoz,
TB Nurse Case Management San Antonio, TX. TB Medications and Adverse Effects
 TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
TB Nurse Case Management San Antonio, TX April 1 3, 2014 TB Medications and Adverse Effects Debbie Onofre RN, BSN Nurse Consultant/ Nurse Educator Heartland National TB Center April 1, 2014 Debbie Onofre,
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
PAGE 1 of 7 References Related ACA Standards 4 th Edition Standards for Adult Correctional Institutions 4-4350, 4-4355 These guidelines are based on the recommendations of the American Thoracic Society
Short Course Treatment for MDR TB
 Objectives Short Course Treatment for MDR TB Barbara J Seaworth M.D. Medical Director Heartland National TB Center Professor of Medicine, University of Texas Health Northeast Participants will utilize
Objectives Short Course Treatment for MDR TB Barbara J Seaworth M.D. Medical Director Heartland National TB Center Professor of Medicine, University of Texas Health Northeast Participants will utilize
Treatment of MDR-TB in high HIV- prevalence settings. Hind Satti, M.D. PIH-Lesotho October 20, 2008
 Treatment of MDR-TB in high HIV- prevalence settings Hind Satti, M.D. PIH-Lesotho October 20, 2008 Early outcomes of MDR-TB treatment Retrospective cohort analysis Registered between July 21, 2007 and
Treatment of MDR-TB in high HIV- prevalence settings Hind Satti, M.D. PIH-Lesotho October 20, 2008 Early outcomes of MDR-TB treatment Retrospective cohort analysis Registered between July 21, 2007 and
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
HA Convention 2016 : Special Topic Session 3 May 2016
 HA Convention 2016 : Special Topic Session 3 May 2016 Diagnosis and Management of TB in Adults Dr. Thomas Mok COS(RMD), KH Tuberculosis An airborne infectious disease caused by Mycobacterium tuberculosis
HA Convention 2016 : Special Topic Session 3 May 2016 Diagnosis and Management of TB in Adults Dr. Thomas Mok COS(RMD), KH Tuberculosis An airborne infectious disease caused by Mycobacterium tuberculosis
Pyrosequencing Experience from Mumbai, India. Camilla Rodrigues MD Consultant Microbiologist Hinduja Hospital,Mumbai India
 Pyrosequencing Experience from Mumbai, India Camilla Rodrigues MD Consultant Microbiologist Hinduja Hospital,Mumbai India Mumbai maximum city Slow Fast 1-2 D With increasing drug resistance, DST is vital
Pyrosequencing Experience from Mumbai, India Camilla Rodrigues MD Consultant Microbiologist Hinduja Hospital,Mumbai India Mumbai maximum city Slow Fast 1-2 D With increasing drug resistance, DST is vital
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf
 Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Epidemiology and diagnosis of MDR-TB in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Definitions
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015
 Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 TB Medications and Adverse Drug Events Presented by Evelyn Drzymala, RN, BSN February 11, 2015 Evelyn Drzymala, RN, BSN has
Introduction to TB Nurse Case Management Online February 4, 11, 18 and 25, 2015 TB Medications and Adverse Drug Events Presented by Evelyn Drzymala, RN, BSN February 11, 2015 Evelyn Drzymala, RN, BSN has
TB BASICS: PRIORITIES AND CLASSIFICATIONS
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MAY 8-11, 2018 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. List
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE MAY 8-11, 2018 TB BASICS: PRIORITIES AND CLASSIFICATIONS LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. List
Case Management of the TB/HIV Infected Patient
 TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
TB Nurse Case Management San Antonio, Texas December 8-10, 2009 Case Management of the TB/HIV Infected Patient Sarah Hoffman, MPH, MSN, ACRN December 9, 2009 TB/HIV: Considerations in the Care of the Coinfected
Monica Manandhar. 2 ND YEAR RESEARCH ELECTIVE RESIDENT S JOURNAL Volume V, A. Study Purpose and Rationale
 Randomized Trial of lsoniazid as Secondary Prophylaxis for Prevention of Recurrent Pulmonary Tuberculosis in HIV-positive Patients After One Episode of Tuberculosis Monica Manandhar A. Study Purpose and
Randomized Trial of lsoniazid as Secondary Prophylaxis for Prevention of Recurrent Pulmonary Tuberculosis in HIV-positive Patients After One Episode of Tuberculosis Monica Manandhar A. Study Purpose and
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB Expert Network Conference 9/26/2008
 TB Expert Network Conference 9/26/2008 Case 1-KT1 35 y/o AA male with a history of HIV since 2002. Presented in July 2007 to a hospital in Orlando, FL with 1 month history of productive cough, fevers and
TB Expert Network Conference 9/26/2008 Case 1-KT1 35 y/o AA male with a history of HIV since 2002. Presented in July 2007 to a hospital in Orlando, FL with 1 month history of productive cough, fevers and
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
DRUG RESISTANCE IN TUBERCULOSIS
 DRUG RESISTANCE IN TUBERCULOSIS INTRODUCTION Up to 50 million people may be infected with drug-resistant resistant TB.* Hot zones of MDR-TB such as Russia, Latvia, Estonia, Argentina and the Dominican
DRUG RESISTANCE IN TUBERCULOSIS INTRODUCTION Up to 50 million people may be infected with drug-resistant resistant TB.* Hot zones of MDR-TB such as Russia, Latvia, Estonia, Argentina and the Dominican
Tuberculosis medications: adverse drug reactions
 Tuberculosis medications: adverse drug reactions Rajesh M. Prabhu, M.D. Infectious Diseases Essentia Health, Duluth, MN July 25, 2017 2014 MFMER slide-1 No Finanial Disclosures Learning Objectives 1. Describe
Tuberculosis medications: adverse drug reactions Rajesh M. Prabhu, M.D. Infectious Diseases Essentia Health, Duluth, MN July 25, 2017 2014 MFMER slide-1 No Finanial Disclosures Learning Objectives 1. Describe
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Harmonizing the Use of Molecular & Culture-based DST of Mycobacterium tuberculosis
 Harmonizing the Use of Molecular & Culture-based DST of Mycobacterium tuberculosis Grace Lin, MS. Research Scientist grace.lin@cdph.ca.gov APHL 8 th TB Lab Conference San Diego 8-19-13 Harmonizing? There
Harmonizing the Use of Molecular & Culture-based DST of Mycobacterium tuberculosis Grace Lin, MS. Research Scientist grace.lin@cdph.ca.gov APHL 8 th TB Lab Conference San Diego 8-19-13 Harmonizing? There
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Diagnosis of MDR TB Neha Shah, MD, MPH
 TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis of MDR TB Neha Shah, MD, MPH April 27, 2010 Drug Resistant TB Neha Shah MD MPH Centers for Disease Control and Prevention Division
TB Nurse Case Management Lisle, Illinois April 27-28, 28 2010 Diagnosis of MDR TB Neha Shah, MD, MPH April 27, 2010 Drug Resistant TB Neha Shah MD MPH Centers for Disease Control and Prevention Division
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Mycobacterium tuberculosis
 Mycobacterium tuberculosis Mycobacterium tuberculosis Ø small, aerobic, nonmotile bacteria Ø Gram-positive bacillus Ø can survive in a dry state for weeks Ø grow only within the cells of a host organism
Mycobacterium tuberculosis Mycobacterium tuberculosis Ø small, aerobic, nonmotile bacteria Ø Gram-positive bacillus Ø can survive in a dry state for weeks Ø grow only within the cells of a host organism
MIC = Many Inherent Challenges Sensititre MIC for Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis complex
 MIC = Many Inherent Challenges Sensititre MIC for Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis complex Marie Claire Rowlinson, PhD D(ABMM) Florida Bureau of Public Health Laboratories
MIC = Many Inherent Challenges Sensititre MIC for Antimicrobial Susceptibility Testing of Mycobacterium tuberculosis complex Marie Claire Rowlinson, PhD D(ABMM) Florida Bureau of Public Health Laboratories