Common Pulmonary Problems. Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine
|
|
|
- Anne Woods
- 6 years ago
- Views:
Transcription
1 Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine


2 Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive Sleep Apnea
3 Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Asthma COPD
4 Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Cancer, Nodules
5 Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive Sleep Apnea
6 Mr. Nap 56 year old obese man complaining of daytime somnolence. Difficulty concentrating at work, falls asleep during meetings. Wife notes loud snoring at night and episodes of interrupted breathing.
7 Obstructive Sleep Apnea Repeated episodes of apnea and hypopnea during sleep Defined as >5 episodes per hour Artist: Habib M'henni
8 Obstructive Sleep Apnea Present in 20-30% of men and 10-15% of women 63% of obese men, 22% obese women Artist: Habib M'henni
9 Other Risk Factors Craniofacial abnormalities Smoking Nasal congestion Age Menopause Family History

10 Neurocognitive Sequelae Excessive daytime sleepiness Decreased cognitive performance Increased automobile accidents Decreased quality of life Mood disturbance Morning headache Basner, R. Continuous Positive Airway Pressure for Obstructive Sleep Apnea N Engl J Med 2007

11 Sequelae Cardiac and metabolic Pulmonary hypertension Coronary artery disease Cerebrovascular disease Arrhythmias Systemic hypertension Heart failure Insulin resistance Basner, R. Cardiovascular Morbidity and Obstructive Sleep Apnea. N Engl J Med 2014

12 Physical Exam Obesity Crowded pharynx (Friedman Tongue Position) Systemic hypertension Nasal obstruction Neck circumference > 17 Lower extremity edema
13 Diagnosis Apnea-Hypopnea Index: Number of apneas, hypopneas/hour AHI >5 + symptoms Sleepiness, insomnia Waking with breath holding, gasping, or choking Habitual snoring, breathing interruptions Hypertension, mood disorder, cognitive dysfunction, coronary artery disease, stroke, congestive heart failure, atrial fibrillation, or type 2 diabetes mellitus AHI >15 <5 Normal 5-15 Mild Moderate >30 Severe
14 Split night polysomnography Gold standard test Measures AHI, Sleep stage, arousals, limb movement Diagnostic study for 2-3hr, then apply CPAP, titrate and monitor effects
15 Home Sleep Apnea Testing (HSAT) Measures respiration, heart rate, and O2 sat Appropriate for patients without CHF, lung disease
16 Treatment Behavior Modification: Weight loss Also ameliorates cardiovascular risk Tobacco cessation Avoid sedative hypnotics, alcohol Positioning Sleep position trainer
17 Continuous Positive Airway Pressure Most effective treatment Reduces apneic events Reduces sleepiness Reduces systolic BP Should be offered to anyone with AHI>15 or AHI>5 and symptoms or signs Efficacy directly correlates with hours/night used


18 Oral Appliances Reduce night-time awakenings, hypoxia Improve neurocognitive function, reduce sleepiness, improve QOL Less effective than CPAP Can be offered to patients with mild-moderate OSA who do not want or tolerate CPAP
19 Surgery Effective if an obstructing lesion is present Tonsilar hypertrophy Uvulopalatopharyngoplasty (UPPP) for other patients Scant evidence of efficacy Cure achieved in a minority of patients
20 Upper Airway Stimulation Therapy Approved by FDA in 2014 Senses inspiration and provides mild stimulation to upper airway muscles to maintain airway patency Reduces apneic events by 68% Improves quality of life measures Small RCTs so far Not yet recommended by any national guidelines
21 Mr. Nap Polysomnography showed an AHI of 21. During the test, CPAP was administered and improved the AHI to normal at a pressure of 5 mm Hg You prescribe CPAP and on follow up, the patient s daytime sleepiness has resolved
22 Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Asthma COPD
23 Ms. Wheeze 34 year old woman complains of episodic shortness of breath and wheezing, particularly severe when she visits her neighbor, who has a dog. Has episodes of dyspnea 3-4 times a week, and wakes at night coughing twice a week. She was hospitalized on multiple occasions for respiratory issues as a child. No smoking history.

24 Asthma Caused by bronchial inflammation Increased secretions Bronchial constriction
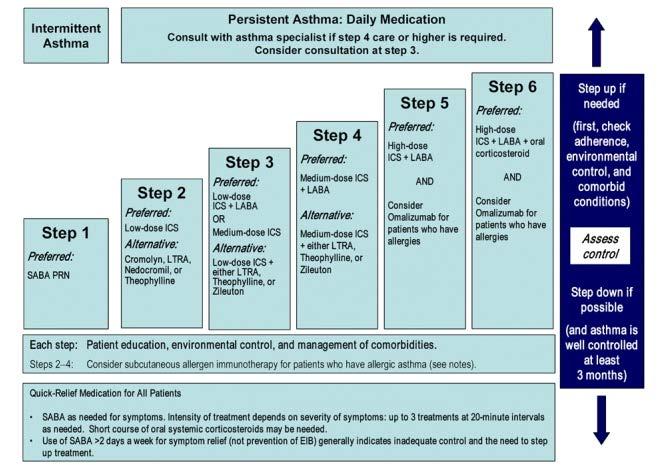
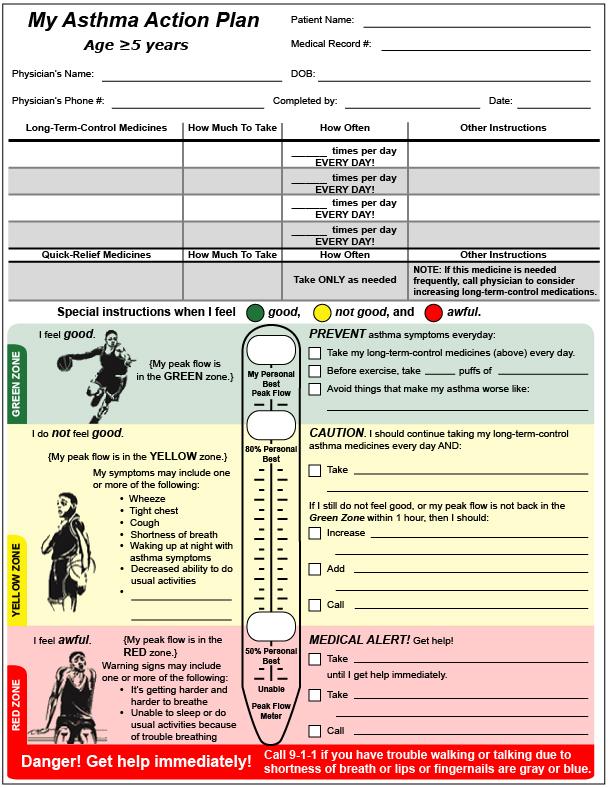
25 Recent guidelines emphasize Assess asthma severity Assess and monitor asthma control Use inhaled corticosteroids early Use written asthma action plans Control environmental exposures
26 Assessing Asthma Severity Mild Intermittent Mild Persistent Moderate Persistent Severe Persistent Symptoms 2 per week > 2 per week daily continual Nighttime symptoms Lung function 2 per month > 2 per month> 1 per week FEV 1 >80 % predicted FEV 1 /FVC normal FEV 1 80 %predicted FEV 1 /FVC normal FEV 1 >60 but <80 % predicted FEV 1 /FVC reduced 5 % frequent FEV 1 <60 % predicted FEV 1 /FVC reduced >5 % Oral steroid 0-1 per year >1 per year Albuterol PRN Low dose inhaled steroid Add LABA or steroid LABA + mod dose steroid
27 Assess Control
28
29
30 Ms. Wheeze You diagnose mild persistent asthma and prescribe Albuterol PRN Low dose inhaled steroid Avoidance of dogs and other triggers On follow up, the patient reports dyspneic episodes once or twice a month, no nighttime awakening
31 Mr. Hack 72 year old man complaining of 2 years of progressively worsening dyspnea and cough productive of white sputum. Needs to rest every 2 blocks when walking. 50 pack year smoking history. On exam, diffuse expiratory wheeze is heard.

32 Chronic Obstructive Pulmonary 4 th leading cause of death in United States Disease Progressive development of airflow limitation that is not fully reversible
33 Risk Factors Smoked tobacco Particulate air pollutants Indoor wood burning stoves or open fires Occupational chemicals α1 antitrypsin deficiency (<1%)
34 Diagnosis and Severity Spirometric Grade FEV1/FVC FEV1 1 <70% 60% 2 <70% 30% FEV1<60% 3 <70% <30% With emphysema, will see a greater in DLCO COPD Foundation
35 Risk Post- Bronchodilator FEV-1 >50% predicted <50% predicted and and/or Symptoms Exacerbations <2 per year 2 per year Low* 0-1 on mmrc High** 2 on mmrc Low 0-1 on mmrc High 2 on mmrc Group A B C D * Low= breathless only with strenuous exercise, while hurrying on level ground, or climbing stairs ** High= need to walk slowly or stop on level ground
36 First Line Second Line A B C and D SA anticholinergic PRN or SA β-agonist PRN LA anticholinergic or LABA LABA + ICS or LA anticholinergic Continue Short Acting Anticholinergic or β-agonist PRN LA anticholinergic or LABA or SABA +SA anticholinergic LA anticholinergic and LABA LAAC +LABA Combine LABA, LAAC, and ICS or Add PDE- 4 inhibitor
37 A B C D Smoking cessation Reduce occupational and environmental exposures Exercise/physical therapy Good nutrition Influenza and pneumococcal vaccines Pulmonary rehabilitation Pulmonologist referral Address end of life decisions Consider surgery
38 Theophylline Other considerations Third line therapy but can be used as adjunct Use lowest possible dose Macrolides Reduce exacerbation rates in severe COPD Oral steroids Should not be used to predict response to inhaled steroids Late stage patients may become steroid dependent Albert R et al. Azithromycin for Prevention of Exacerbations of COPD. N Engl J Med Aug 25; 365(8):
39 Mr. Hack PFTs: FEV1/FVC = 64%, FEV1 = 53%. Needs to stop on flat surface, no exacerbations, Class B You discuss smoking cessation with the patient, who enrolls in a smoking cessation group. You discuss an exercise plan to maintain exercise tolerance. You initiate albuterol PRN and tiotropium daily. You provide a pneumococcal and flu vaccine. On his return visit, the patient notes much improved dyspnea and the ability to walk to the grocery store without difficulty.
40 Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Cancer, Nodules
41 Mr. Spot 49 yo man requires chest x-ray for a physical exam for work. No cough, dyspnea, or chest pain. Chest radiograph shows 1 cm nodule in right upper lobe with central calcification ppd negative No prior films for comparison
42 Solitary pulmonary nodules Solitary mass <3cm surrounded by normal lung tissue Low Risk High Risk Age Size Appearance Interval change <35 <6mm Non-solid, popcorn appearance Diffuse, laminar or central calcification >35 OR by 0.1 per mm Spiculated No calcium Solid nodule No growth over 2 years Growth on serial imaging Smoking No smoking history Smoking history Other Male Female, Upper lobe, Prior history or FH of cancer
43 Management Nodule type <6mm 6-8mm >8mm Single Solid Low Risk No follow up CT at 6-12 mo, then 18-24mo High Risk Multiple Solid Consider CT at 12 mo CT at 6-12 mo and mo Low Risk No follow up CT at 3-6 mo then mo High Risk Consider CT at 12 mo CT at 3-6 mo then mo CT at 3 mo, PET, or biopsy CT at 3 mo, PET, or biopsy CT at 3-6 mo then mo CT at 3-6 mo then mo Fleischner Society Guidelines
44 Management Nodule type <6 mm 6 mm Single non-solid Ground Glass No follow up CT at 6-12 mo, then q 2 years for 5 years Part solid No follow up CT at 3-6 mo then annually if solid component <6mm for 5 years Multiple non-solid CT at 3-6 mo then 2 and 4 years CT at 3-6 mo then follow most suspicious nodule
45 Mr. Spot Continued Has a history of smoking and, because he is 49 years old, has 2 high risk features. Moderate risk. You order a CT scan, but the patient does not follow up and is lost to care. Two years later, he returns complaining of fatigue, weight loss and occasional hemoptysis
46 Lung Cancer
47 Risk Factors Tobacco 2 nd hand smoke Dose response Radon Asbestos COPD, pulmonary fibrosis, TB Family history
48 Screening Mortality benefit found for Low dose CT Annually In high risk cohort 30 pack year history If quit, <15 years ago Age Aberle DR et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. NEJM 2011, 365(5): ]
49 Diagnosis Biopsy Four types: Small-cell carcinoma Adenocarcinoma Squamous cell carcinoma Large-cell carcinoma Non-small cell lung cancer (NSCLC)
50 Small Cell Lung Cancer SCLC is considered systemic from the outset TNM staging not used Surgery not an option
51 Limited SCLC Confined to one half of the chest and ipsilateral supraclavicular nodes Treatment: Combination Radiation and Chemotherapy 80-90% Response 50-60% Remission 30-40% 2-yr Survival 10-15% 5-yr Survival Median Survival months
52 Extensive SCLC Disease spreading beyond one hemithorax Treatment: Chemotherapy only 60-80% Response 20-30% Remission <10% 2-yr Survival Rare 5-yr Survival Median survival 9-10 months
53 Non small cell lung cancers Adenocarcinoma Squamous cell carcinoma Large cell carcinoma Treatment similar for all three
54 Non small cell lung cancers Determine TNM stage Chest and liver CT and, if resectable, PET scan to look for metastases Brain MRI Bone scan If no metastases, and resectable, surgical cure may be possible
55 Mr. Spot A CT shows that the nodule has grown to 3cm. Percutaneous biopsy shows NSCLC, and TNM staging shows that the tumor is stage 2. The patient has the tumor resected and begins chemotherapy.
56 Thank You
Common Pulmonary Problems. Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine
 Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
Common Pulmonary Problems Diana Coffa, MD Residency Program Director UCSF Department of Family and Community Medicine Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist Obstructive
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Triennial Pulmonary Workshop 2012
 Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2012 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Sleep Apnea: Diagnosis & Treatment
 Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
Disclosure Sleep Apnea: Diagnosis & Treatment Lawrence J. Epstein, MD Sleep HealthCenters Harvard Medical School Chief Medical Officer for Sleep HealthCenters Sleep medicine specialty practice group Consultant
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA
 ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA A Person is physically qualified to drive a motor vehicle if that person; -(5) has no established medical history or clinical diagnosis
ROBERT C. PRITCHARD DIRECTOR MICHAEL O. FOSTER ASSISTANT DIR. SLEEP APNEA A Person is physically qualified to drive a motor vehicle if that person; -(5) has no established medical history or clinical diagnosis
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Questions: What tests are available to diagnose sleep disordered breathing? How do you calculate overall AHI vs obstructive AHI?
 Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
COPD, Lung Cancer, OSA, Sarcoidosis
 COPD, Lung Cancer, OSA, Sarcoidosis Shawn K. Conner, MD Assistant Clinical Professor Wayne State University School of Medicine Detroit, Michigan Disclosure Statement It is the policy of the AAFP that all
COPD, Lung Cancer, OSA, Sarcoidosis Shawn K. Conner, MD Assistant Clinical Professor Wayne State University School of Medicine Detroit, Michigan Disclosure Statement It is the policy of the AAFP that all
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
Pre-op Clinical Triad - Pulmonary. Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018
 Pre-op Clinical Triad - Pulmonary Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018 Disclosures none Case Mr. G is a 64 year-old man who presents to
Pre-op Clinical Triad - Pulmonary Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018 Disclosures none Case Mr. G is a 64 year-old man who presents to
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Update on Sleep Apnea Diagnosis and Treatment
 Update on Sleep Apnea Diagnosis and Treatment Damien Stevens MD Pulmonary/Critical Care/Sleep Medicine Medical Director KU Medical Center Sleep Laboratory Objectives Discuss physiology of sleep and obstructive
Update on Sleep Apnea Diagnosis and Treatment Damien Stevens MD Pulmonary/Critical Care/Sleep Medicine Medical Director KU Medical Center Sleep Laboratory Objectives Discuss physiology of sleep and obstructive
Sleep and the Heart. Physiologic Changes in Cardiovascular Parameters during Sleep
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart. Rami N. Khayat, MD
 Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Sleep and the Heart Rami N. Khayat, MD Professor of Internal Medicine Medical Director, Department of Respiratory Therapy Division of Pulmonary, Critical Care and Sleep Medicine The Ohio State University
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX
 MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
Is CPAP helpful in severe Asthma?
 Is CPAP helpful in severe Asthma? P RAP UN KI TTIVORAVITKUL, M.D. PULMONARY AND CRITICAL CARE DIVISION DEPARTMENT OF MEDICINE, PHRAMONGKUTKLAO HOSPITAL Outlines o Obstructive sleep apnea syndrome (OSAS)
Is CPAP helpful in severe Asthma? P RAP UN KI TTIVORAVITKUL, M.D. PULMONARY AND CRITICAL CARE DIVISION DEPARTMENT OF MEDICINE, PHRAMONGKUTKLAO HOSPITAL Outlines o Obstructive sleep apnea syndrome (OSAS)
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Alaska Sleep Education Center
 Alaska Sleep Education Center The 3 Types of Sleep Apnea Explained: Obstructive, Central, & Mixed Posted by Kevin Phillips on Jan 28, 2015 6:53:00 PM Sleep apnea is a very common sleep disorder, affecting
Alaska Sleep Education Center The 3 Types of Sleep Apnea Explained: Obstructive, Central, & Mixed Posted by Kevin Phillips on Jan 28, 2015 6:53:00 PM Sleep apnea is a very common sleep disorder, affecting
Pulmonary hypertension
 Common Pulmonary Problems In Adults Todd A. May, M.D. Chief of the Medical Staff San Francisco General Hospital Clinical Professor Family & Community Medicine University of California, San Francisco Pulmonary
Common Pulmonary Problems In Adults Todd A. May, M.D. Chief of the Medical Staff San Francisco General Hospital Clinical Professor Family & Community Medicine University of California, San Francisco Pulmonary
Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease
 1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
1 Sleep and the Heart Reversing the Effects of Sleep Apnea to Better Manage Heart Disease Rami Khayat, MD Professor of Internal Medicine Director, OSU Sleep Heart Program Medical Director, Department of
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome
 The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Pulmonary Predicaments in Primary Care Peter F. Bidey, DO
 Pulmonary Predicaments in Primary Care Peter F. Bidey, DO Pulmonary Predicaments in Primary Care Peter F. Bidey, D.O. Clinical Instructor -Family Medicine Philadelphia College of Osteopathic Medicine
Pulmonary Predicaments in Primary Care Peter F. Bidey, DO Pulmonary Predicaments in Primary Care Peter F. Bidey, D.O. Clinical Instructor -Family Medicine Philadelphia College of Osteopathic Medicine
Sleep Disordered Breathing
 Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
Sleep Disordered Breathing SDB SDB Is an Umbrella Term for Many Disorders characterized by a lack of drive to breathe Results n repetitive pauses in breathing with no effort Occurs for a minimum of 10
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Obstructive Sleep Apnea and COPD overlap syndrome. Financial Disclosures. Outline 11/1/2016
 Obstructive Sleep Apnea and COPD overlap syndrome Chitra Lal, MD, FCCP, FAASM Associate Professor of Medicine, Pulmonary, Critical Care, and Sleep, Medical University of South Carolina Financial Disclosures
Obstructive Sleep Apnea and COPD overlap syndrome Chitra Lal, MD, FCCP, FAASM Associate Professor of Medicine, Pulmonary, Critical Care, and Sleep, Medical University of South Carolina Financial Disclosures
Polysomnography (PSG) (Sleep Studies), Sleep Center
 (Sleep Studies), Sleep Center") Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Policy Number: 1036 Policy History Approve Date: 07/09/2015 Effective Date: 07/09/2015 Preauthorization All Plans Benefit plans vary in coverage and some plans may not provide coverage for certain service(s)
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene
 Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
IEHP considers the treatment of obstructive sleep apnea (OSA) medically necessary according to the criteria outlined below:
 medically necessary according to the criteria outlined below:") : Positive Airway Pressure, Oral Appliances, and Surgical Interventions Policy: Obstructive sleep apnea (OSA) is characterized by an interruption of breathing during sleep most commonly due to extra or
: Positive Airway Pressure, Oral Appliances, and Surgical Interventions Policy: Obstructive sleep apnea (OSA) is characterized by an interruption of breathing during sleep most commonly due to extra or
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
Mario Kinsella MD FAASM 10/5/2016
 Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Mario Kinsella MD FAASM 10/5/2016 Repetitive episodes of apnea or reduced airflow Due to upper airway obstruction during sleep Patients often obese Often have hypertension or DM 1 Obstructive apneas, hypopneas,
Circadian Variations Influential in Circulatory & Vascular Phenomena
 SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
SLEEP & STROKE 1 Circadian Variations Influential in Circulatory & Vascular Phenomena Endocrine secretions Thermo regulations Renal Functions Respiratory control Heart Rhythm Hematologic parameters Immune
NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C.
 NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C. Past Medical History AIDS/HIV disease Anemia Asthma Bronchitis Cancer Date of last Chest X-ray Diabetes Mellitus, Type I Diabetes Mellitus,
NORTHERN VIRGINIA PULMONARY AND CRITICAL CARE ASSOCIATES, P.C. Past Medical History AIDS/HIV disease Anemia Asthma Bronchitis Cancer Date of last Chest X-ray Diabetes Mellitus, Type I Diabetes Mellitus,
Evaluation, Management and Long-Term Care of OSA in Adults
 Evaluation, Management and Long-Term Care of OSA in Adults AUGUST 2015 Providing diagnostic tools and therapies that are evidence-based is a key part of a successful sleep practice. This resource outlines
Evaluation, Management and Long-Term Care of OSA in Adults AUGUST 2015 Providing diagnostic tools and therapies that are evidence-based is a key part of a successful sleep practice. This resource outlines
UNDERSTANDING COPD MEDIA BACKGROUNDER
 UNDERSTANDING COPD MEDIA BACKGROUNDER What is COPD? Chronic Obstructive Pulmonary Disease (COPD) also called emphysema and/or chronic obstructive bronchitis* is a preventable lung disease caused by the
UNDERSTANDING COPD MEDIA BACKGROUNDER What is COPD? Chronic Obstructive Pulmonary Disease (COPD) also called emphysema and/or chronic obstructive bronchitis* is a preventable lung disease caused by the
11/19/2012. The spectrum of pulmonary diseases in HIV-infected persons is broad.
 The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
The spectrum of pulmonary diseases in HIV-infected persons is broad. HIV-associated Opportunistic infections Neoplasms Miscellaneous conditions Non HIV-associated Antiretroviral therapy (ART)-associated
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Sleep Apnea: Vascular and Metabolic Complications
 Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Disclosures. Chronic Obstructive Pulmonary Disease. Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
Chronic Obstructive Pulmonary Disease May 14, 2016 Orlando, FL COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United States. Alarmingly, COPD recently became
SLEEP HISTORY QUESTIONNAIRE
 Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Diabetes & Obstructive Sleep Apnoea risk. Jaynie Pateraki MSc RGN
 Diabetes & Obstructive Sleep Apnoea risk Jaynie Pateraki MSc RGN Non-REM - REM - Both - Unrelated - Common disorders of Sleep Sleep Walking Night terrors Periodic leg movements Sleep automatism Nightmares
Diabetes & Obstructive Sleep Apnoea risk Jaynie Pateraki MSc RGN Non-REM - REM - Both - Unrelated - Common disorders of Sleep Sleep Walking Night terrors Periodic leg movements Sleep automatism Nightmares
What is this patient s diagnosis?
 Asthma and COPD KANTA VELAMURI, MD ASSOCIATE PROFESSOR OF MEDICINE PULMONARY, CRITICAL CARE AND SLEEP MEDICINE SECTION MICHAEL E. DEBAKEY VA MEDICAL CENTER BAYLOR COLLEGE OF MEDICINE Disclosures None Case
Asthma and COPD KANTA VELAMURI, MD ASSOCIATE PROFESSOR OF MEDICINE PULMONARY, CRITICAL CARE AND SLEEP MEDICINE SECTION MICHAEL E. DEBAKEY VA MEDICAL CENTER BAYLOR COLLEGE OF MEDICINE Disclosures None Case
Dr Rob Young. General Physician Auckland City Hospital
 Dr Rob Young General Physician Auckland City Hospital Managing COPD case studies. Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP Department of Medicine, Auckland City Hospital
Dr Rob Young General Physician Auckland City Hospital Managing COPD case studies. Associate Professor Robert Young BMedSc, MBChB, DPhil (Oxon), FRACP, FRCP Department of Medicine, Auckland City Hospital
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update
 OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
UPDATES IN SLEEP APNEA:
 UPDATES IN SLEEP APNEA: CPAP,CPAP COMPLIANCE, & ALTERNATIVES MICHELLE ZETOONY, DO, FCCP, FACOI BOARD CERTIFIED PULMONARY, CRITICAL CARE, SLEEP & INTERNAL MEDICINE CLEARWATER, FL DISCLOSURE I have no conflicts
UPDATES IN SLEEP APNEA: CPAP,CPAP COMPLIANCE, & ALTERNATIVES MICHELLE ZETOONY, DO, FCCP, FACOI BOARD CERTIFIED PULMONARY, CRITICAL CARE, SLEEP & INTERNAL MEDICINE CLEARWATER, FL DISCLOSURE I have no conflicts
New Pulmonary Patient Questionnaire. Name Age Date. General Medical History
 New Pulmonary Patient Questionnaire Name Age Date General Medical History 1 John S. Kim, M.D., Diplomate ABSM Lawrence A. Lynn, D.O., FCCP 1. Please list any surgeries you have had and their approximate
New Pulmonary Patient Questionnaire Name Age Date General Medical History 1 John S. Kim, M.D., Diplomate ABSM Lawrence A. Lynn, D.O., FCCP 1. Please list any surgeries you have had and their approximate
Presented by UIC College of Nursing
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long-acting inhalers and emergency use inhalers.
Chronic Obstructive Pulmonary Disease 1/18/2018
 Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Presented by UIC College of Nursing Describe COPD. Identify red flags for a COPD exacerbation. Identify COPD triggers or risk factors. Differentiate between long acting inhalers and emergency use inhalers.
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Outline. Major variables contributing to airway patency/collapse. OSA- Definition
 Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
Current Approaches to Asthma & COPD
 10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
PEARLS IN PULMONARY MEDICINE. Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center
 PEARLS IN PULMONARY MEDICINE Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center Case 1 While moonlighting in the ER, you are asked to evaluate a lady for shortness of
PEARLS IN PULMONARY MEDICINE Kellie R. Jones, MD Associate Professor University of Oklahoma Health Sciences Center Case 1 While moonlighting in the ER, you are asked to evaluate a lady for shortness of
AHA Sleep Apnea and Cardiovascular Disease. Slide Set
 AHA 2008 Sleep Apnea and Cardiovascular Disease Slide Set Based on the AHA 2008 Scientific Statement Sleep Apnea and Cardiovascular Disease Virend K. Somers, MD, DPhil, FAHA, FACC Mayo Clinic and Mayo
AHA 2008 Sleep Apnea and Cardiovascular Disease Slide Set Based on the AHA 2008 Scientific Statement Sleep Apnea and Cardiovascular Disease Virend K. Somers, MD, DPhil, FAHA, FACC Mayo Clinic and Mayo
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC
 KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC") Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) KAREN ALLEN MD PULMONARY & CRITICAL CARE MEDICINE VA HOSPITAL OKC / OUHSC I have no financial disclosures Definition COPD is a preventable and treatable disease
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD)
 Instructions for the Pulmonary Diagnosis Form (PLD)") Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
Challenging Cases in Pediatric Polysomnography. Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep
 Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
Challenging Cases in Pediatric Polysomnography Fauziya Hassan, MBBS, MS Assistant Professor Pediatric Pulmonary and Sleep Conflict of Interest None pertaining to this topic Will be using some slides from
An update on childhood sleep-disordered breathing
 An update on childhood sleep-disordered breathing แพทย หญ งวนพร อน นตเสร ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร มหาว ทยาล ยสงขลานคร นทร Sleep-disordered breathing Primary snoring Upper airway resistance syndrome
An update on childhood sleep-disordered breathing แพทย หญ งวนพร อน นตเสร ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร มหาว ทยาล ยสงขลานคร นทร Sleep-disordered breathing Primary snoring Upper airway resistance syndrome
COPD or not COPD, that is the question.
 COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Referring for specialist respiratory input. Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL
 Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Referring for specialist respiratory input Dr Melissa Heightman Consultant respiratory physician, UCLH,WH, CNWL Respiratory Specialist- who? GPSI Community Team Secondary Care Respiratory physician and
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Triennial Pulmonary Workshop 2015
 Triennial Pulmonary Workshop 2015 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Triennial Pulmonary Workshop 2015 Rod Richie, M.D., DBIM Medical Director Texas Life Insurance Company, Waco, TX EMSI, Waco, TX Lisa Papazian, M.D., DBIM Assistant Vice President and Medical Director Sun
Advances in Chronic Obstructive Pulmonary Disease
 Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Level 3 Sleep Study Utilization and Interpretation. CSIM October 14, 2015 Dr. Nicole Drost
 Level 3 Sleep Study Utilization and Interpretation CSIM October 14, 2015 Dr. Nicole Drost Disclosures I have no financial disclosures that would present a conflict of interest with this presentation Objectives
Level 3 Sleep Study Utilization and Interpretation CSIM October 14, 2015 Dr. Nicole Drost Disclosures I have no financial disclosures that would present a conflict of interest with this presentation Objectives
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea
 Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
What is COPD? COPD Pharmacotherapy. COPD Mortality Is Increasing
 COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
SCREENING AND PREVENTION
 These protocols are designed to implement standard guidelines, based on the best evidence, that provide a consistent clinical experience for AHC II Integrated Clinical Delivery Network patients and allow
These protocols are designed to implement standard guidelines, based on the best evidence, that provide a consistent clinical experience for AHC II Integrated Clinical Delivery Network patients and allow