New Perspectives on the Pathogenesis of OSA - Anatomic Perspective. New Perspectives on the Pathogenesis of OSA: Anatomic Perspective - Disclosures
|
|
|
- Tabitha Nelson
- 6 years ago
- Views:
Transcription

1 New Perspectives on the Pathogenesis of OSA - Anatomic Perspective Richard J. Schwab, M.D. Professor of Medicine Interim Chief, Division of Sleep Medicine Medical Director, Penn Sleep Centers University of Pennsylvania Perelman School of Medicine New Perspectives on the Pathogenesis of OSA: Anatomic Perspective - Disclosures NIH grants - PPG (phenotyping and OSA) ResMed Grant/Registry to study OSA/CSA and CPAP in hospitalized patients Jazz clinical trial (JZP-110) for daytime sleepiness in OSA Inspire CT study to examine upper airway anatomy with hypoglossal nerve stimulation 1




2 New Insights into the Pathogenesis of Sleep Apnea: Anatomic Perspective Physical examination/anatomic risk factors for OSA Anatomic pathogenesis of OSA Increased size of upper airway soft tissues Importance of tongue fat Dynamic upper airway imaging during respiration Modified Mallampati Classification Class 1 Class 2 Class 3 Class 4 Tsai et al, AJRCCM 167, , 2003 Mallampati et al. (1985). A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaest Soc J, 32(4), ,

/maxilla Narrowed hard palate - overbite/overjet A combination of")
3 Modified Mallampati Classification What is this patient s Modified Mallampati score? Anatomic Risk Factors for Sleep Apnea Obesity and its effects on the upper airway tissues Increased neck circumference Nasal airway restriction: septal deviation, allergic rhinitis, nasal polyps Macroglossia/tongue ridging Adeno-tonsillar hypertrophy (palatine/lingual tonsils) Lateral peritonsillar narrowing Enlargement/elongation of the soft palate Recessed mandible (retrognathia)/maxilla Narrowed hard palate - overbite/overjet A combination of soft tissue and/or craniofacial risk factors is likely most important 3

4 Morphometric Measurements (Schellenberg AJRCCM 162; , 2000) Macroglossia: tongue being above level of mandibular occlusal plane Uvula enlargement: > 1.5 cm in length or > 1.0 cm in width Enlargement of lateral walls: > 25% impingement pharyngeal space by peritonsillar tissues Tonsillar enlargement: > 50% lateral impingement of posterior pharyngeal airspace Normal Upper Airway (Schellenberg et al, AJRCCM 162; , 2000) 4


5 Physical Examination and Sleep Apnea (Schellenberg et al, AJRCCM 162; , 2000) Physical Examination and Sleep Apnea (Schellenberg et al, AJRCCM 162; , 2000) 5

6 Normal Upper Airway (Schellenberg et al, AJRCCM 162; , 2000) Lateral Pharyngeal Grading System Class I = palatopharyngeal arch intersects at the edge of the tongue Class II = palatopharyngeal arch intersects at 25% or more of the tongue diameter Class III = palatopharyngeal arch intersects at 50% or more of the tongue diameter Class IV = palatopharyngeal arch intersects at 75% or more of the tongue diameter Tsai, et al. A Decision Rule for Diagnostic Testing in Obstructive Sleep Apnea. American Journal of Respiratory and Critical Care Medicine, Vol. 167, No. 10 (2003), pp


7 Physical Examination and Sleep Apnea (Schellenberg et al, AJRCCM 162; , 2000) Narrowed Hard Palate and Sleep Apnea 7

8 Physical Examination and Sleep Apnea (Schellenberg et al, AJRCCM 162; , 2000) Physical Examination and Sleep Apnea (Schellenberg AJRCCM 162; , 2000) Adjusted Odds Ratio (OR) for Sleep Apnea Physical Finding OR 95% CI Lateral Narrowing 2.6* Tonsillar hypertrophy 2.1* Macroglossia Enlarged soft palate Retrognathia *Maintained significance after adjusting for BMI/neck size 8
. Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.")

9 Digital Morphometrics: A New Paradigm to Assess Upper Airway Anatomical Risk Factors for Obstructive Sleep Apnea) Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest Quantify Anatomic Risk Factors for OSA with Digital Morphometrics/Laser Ruler Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest


. doi:10.1016/j.chest.")


10 Upper Airway Soft Tissue and Craniofacial Measurements Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest Intraoral Photographs with Indicated Measures Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest
. doi:10.1016/j.chest.2017.05.")

11 Craniofacial Photograph with Laser Ruler The mandibular length is measured from the marked mandibular angle to the most prominent point on the chin Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest Examples of the Four Classes of Modified Mallampati Class I indicates full visibility of the uvula and tonsillar fossa Class II indicates visibility of upper portion of the uvula and partial visibility of the upper airway Class III indicates visibility of the hard palate and base of the uvula Class IV indicates visibility of the hard palate and no visibility of the soft palate Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest
12 Digital Morphometrics: A New Paradigm to Assess Upper Airway Anatomical Risk Factors for Obstructive Sleep Apnea - Demographics Measure All Patients Controls (AHI<10) Apneics (AHI 10) N Estimate N Estimate N Estimate p Age ± ± ± 12.8 < BMI ± ± ± 9.9 < Gender Male % % % Female % % % Race Caucasian % % % African % % % Other % % % AHI ± ± ± 29.4 < ln(ahi+1) ± ± ± 0.67 < Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest Digital Morphometrics: A New Paradigm to Assess Upper Airway Anatomical Risk Factors for Obstructive Sleep Apnea - Results Measure All Patients Controls (AHI<10) Apneics (AHI 10) N Estimate N Estimate N Estimate p Modified Mallampati Class I % % % Class II % % % Class III % % % Class IV % % % Airway Not Visible % % % Mouth Width ± ± ± Mouth Height ± ± ± Mouth Area ± ± ± Tongue Width ± ± ± 0.57 Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest <
13 Digital Morphometrics: A New Paradigm to Assess Upper Airway Anatomical Risk Factors for Obstructive Sleep Apnea - Results Measure All Patients Controls (AHI<10) Apneics (AHI 10) N Estimate N Estimate N Estimate p Mouth Width ± ± ± Tongue Width ± ± ± 0.72 <0.001 Tongue Length ± ± ± Tongue Area ± ± ± Tongue Thickness ± ± ± 0.28 < Tongue Curvature ± ± ± Airway Width ± ± ± Uvula Length (Airway) ± ± ± Uvula Width (Airway) ± ± ± Uvula Area (Airway) ± ± ± Mandibular Length ± ± ± 1.05 <0.001 Mandibular Width ± ± ± 1.04 < Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest, 152, 2017 Associations Between Photography Measurements and OSA and AHI - Conclusions Apneics had higher scores on all measures of Mallampati, less airway visibility, larger mouth width and area, and larger tongue width and thickness Also had more severe pharyngeal narrowing within the subpopulation where this measure was quantifiable Measurements of intraoral crowdedness showed the strongest associations in OSA and AHI status Apneics tended to have more crowded or less visible airways than controls Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi: /j.chest
 (Schwab, Am J Resp Crit Care Med")
14 Different Imaging Modalities to Phenotype the Upper Airway Morphometric examination/digital photography Cephalometrics - craniofacial skeleton Nasopharygnoscopy - awake and sleep induced (Propofol) Acoustic Reflectance - airway Optical Coherence Tomography - airway lumen Computed Tomography Magnetic Resonance Imaging Normal Subject (Mid-Sagittal View) (Schwab, Am J Resp Crit Care Med 152: , 1995) Soft Palate Tongue Airway Mandible Subcutaneous Fat Retropalatal Retroglossal Subcutaneous Fat 14
 Airway Tongue Pharyngeal Wall Mandible Mandible Parapharyngeal Fat Pad")
 Normal Subject")
15 Normal Subject (Axial View) (Schwab, Am J Resp Crit Care Med 152: , 1995) Airway Tongue Pharyngeal Wall Mandible Mandible Parapharyngeal Fat Pad Parotid Pharyngeal Wall Spinal Cord Subcutaneous Fat Sagittal Upper Airway MR Images (Schwab, Am J Resp Crit Care Med 152: , 1995) Normal Subject Apneic Patient 15










16 Axial Upper Airway MR Images (Schwab, Am J Resp Crit Care Med 152: , 1995) Normal Subject Apneic Patient Schwab et al, AJRCCM 168; , 2003 Tongue Mandible Parapharyngeal Fat Pads Airway Normal Subject Soft Palate Pharyngeal Walls Tongue Mandible Parapharyngeal Fat Pads Airway Patient with Sleep Apnea Soft Palate Pharyngeal Walls 16
17 Volumetric Anatomic Risk Factors for Sleep Apnea (Cases/Controls: N = 96) (Schwab et al, AJRCCM 168; , 2003) Adjusted Odds Ratio (OR) for Sleep Apnea: Soft Tissue Volume OR 95% CI Fat pads Lateral Walls 6.01* Soft Palate Tongue 6.55* Total Soft Tissue 6.95* Adjusted for gender, ethnicity, age, craniofacial size and visceral neck fat * = Significant Why are Upper Airway Soft Tissue Structures Enlarged in Apneics? Edema from negative pressure Changes in blood flow/redistribution leg edema Muscle disorder/function/exercise Vibration/snoring/surface tension Weight gain/obesity Gender Ethnicity Genetic factors 17
 In parapharyngeal fat")

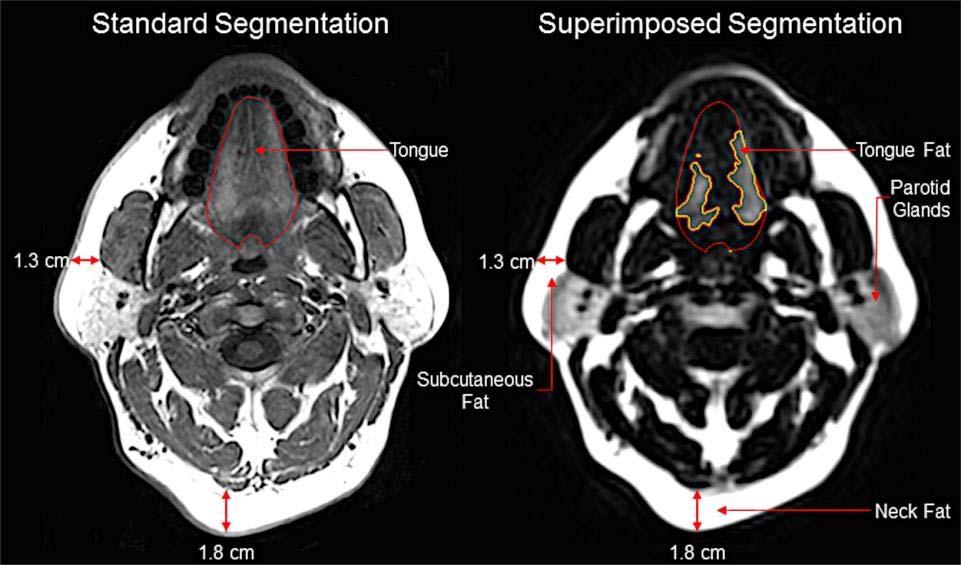
18 Airway Airway Airway Normal Airway Apneic We Still Do Not Understand the Effect of Obesity on Upper Airway Tissues Increased volume of adipose tissue (several studies have demonstrated this) In parapharyngeal fat pads increased tissue pressure?? Within tongue does this size and function? Fat under mandible and subcutaneous Increased muscular tissue with weight gain? Increase in size of lateral walls, tongue, soft palate 18
![Images from the Nashi autopsy study [Laryngoscope 117; 1467-1473, 2007].](/docs-images/80/80484490/images/19-0.jpg "Left panel (A) shows a sagittal image of the tongue demonstrating a")
 is")


 in an obese subject.")
19 Images from the Nashi autopsy study [Laryngoscope 117; , 2007]. Left panel (A) shows a sagittal image of the tongue demonstrating a significant amount of fat in the posterior third of the tongue and in the sublingual region below the intrinsic tongue muscles; bottom (B) is a schematic demonstrating the percent of tongue fat in the anterior, posterior and sublingual regions in 121 tongue autopsy specimens. The right panel demonstrates another autopsy specimen with a significant amount of tongue fat. Psoas muscle Tongue Histomicrographs of psoas muscle (A: top) and tongue (B: bottom) in an obese subject. Note there is greater fat in the tongue than the psoas muscle. Nashi Laryngoscope 117; ,
20 Anterior and posterior percentage tongue fat correlates with increasing body mass index Nashi et al, Laryngoscope 2007; 117: Study Objectives (Kim et al, Sleep 37; , 2014) The primary goal of this study was to identify alterations in fat deposition within the tongue of obese apneics in comparison to obese subjects without sleep apnea using the three-point Dixon method (a method for fat/water discrimination) Compared tongue fat to fat in the masseter muscles Examined tongue fat topography Compared men and women 20

21 Kim et al, (Sleep 37; , 2014) 21

22 Demographics of Case and Control Subjects (Kim et al, Sleep 37; , 2014) Apneics (n=90) Controls (n=31) Factor Mean SD Mean SD t test (p value) Age, years BMI, kg/m < AHI, events/hour < Gender, M:F 42:48 10: Race, C:AA 39:51 18: Definition of abbreviations: AHI=apnea/hypopnea index; BMI=body mass index; C=Caucasian; AA=African American 22
23 Comparison of Muscle Volumes and Intramuscular Fat in Case and Control Subjects (Kim et al, Sleep 37; , 2014) Apneics (n=90) Controls (n=31) Soft Tissue Volume Mean SD Mean SD t Test (p value) 2 p Tongue, mm 3 101,193 17,651 85,542 13,813 < Tongue fat, mm 3 32,791 9,175 23,390 5,511 < Tongue fat, % Left masseter, mm 3 16,204 6,633 14,517 6, Left masseter fat, mm Left masseter fat, % Significant differences (p < 0.05) are presented in bold. 2 p indicates after adjustment for age, BMI, gender, and race Comparison of Muscle Volumes and Intramuscular Fat in Apneics and Controls (Kim et al, Sleep 37; , 2014) Tongue volume and tongue fat increased in apneics compared to controls. No differences in masseter volumes or masseter fat volume 23
24 Kim et al, (Sleep 37; , 2014) Correlations between Muscle Volumes and Intramuscular Fat and AHI in Apneics (Kim et al, Sleep 37; , 2014) Increases in tongue volume and tongue fat increased the AHI 24
25 Main Findings (Kim et al, Sleep 37; , 2014) Obese apneics have enlarged tongue volumes and increased fat within the tongue in comparison to obese normal subjects after adjustment for differences in age, BMI, gender, and race There is a heterogeneous distribution of fat within the tongue Tongue fat distribution in apneics is increased in specific locations of the tongue (greater in the retroglossal region) Tongue size and tongue fat are correlated with AHI No difference in tongue fat between apneic men and women Importance of Tongue Fat (Kim et al, Sleep 37; , 2014) Increased tongue fat increases AHI by increasing the size of the tongue (affects airway collapsibility and size) but may also adversely affect muscle function Increased intramuscular fat may contribute to changes in contractile performance or tongue shape What is the purpose of tongue fat? Why do some individuals have greater tongue fat deposition - genetic/high fat diet? Is this visceral fat? New therapeutic options (upper airway exercises, weight loss, hypoglossal nerve stimulation, dietary 25
 (Schwab et al, in preparation) All patients diagnosed with OSA in Iceland and referred for CPAP treatment at the Landspitali University")
26 Anatomical Imbalance The interaction between upper airway soft tissue structures and craniofacial structures Watanabe, et al. AJCCM 165:260, 2002 Icelandic Sleep Apnea Cohort (ISAC) (Schwab et al, in preparation) All patients diagnosed with OSA in Iceland and referred for CPAP treatment at the Landspitali University Hospital in Reykjavik, Iceland, from September August subjects had MRI (upper airway, neck and abdomen) and PSG (Embletta) All apneics with wide range of severity - AHI/ODI Three BMI categories < 30, 30-35, > 35 kg/m 2 Men and women but mostly men 26
 Total Soft Tissue (mm 3 ) IMV (mm 3 ) AHI 15-30 n = 137 210,241 ± 24,905 259,539 ± 32,518 AHI 30-50 n = 211 213,874 ± 26,316 259,533 ± 32,669 TST/IMV Ratio 1.12 ± 0.")
27 Intra-Mandibular Volume (IMV): the Amount of Tissue within the Box (Schwab et al, in preparation) Severity of AHI: Based on Craniofacial and Soft Tissue Interactions in Men in ISAC (Schwab et al, in preparation) Total Soft Tissue (mm 3 ) IMV (mm 3 ) AHI n = ,241 ± 24, ,539 ± 32,518 AHI n = ,874 ± 26, ,533 ± 32,669 TST/IMV Ratio 1.12 ± ± 0.12 AHI 50 n = ,314 ± 26, ,042 ± 27, ± 0.13 Unadjusted p *Adjusted p *Adjusted for BMI and age The ratio of the total soft tissue (TST) to intramandibular volume (IMV) was significantly greater in the patients with the most severe apnea 27
 Methods: Subjects included 157 obese apneics and 46 obese controls Dynamic")
28 Relationship of Tongue Size, Mandibular Length and AHI in ISAC Schwab et al, in preparation Log AHI was greatest when tongue volume was largest and mandibular length was smallest Dynamic Upper Airway Imaging During Wakefulness in Obese Subjects with and without Sleep Apnea (Feng et al, AJRCCM conditionally accepted) Methods: Subjects included 157 obese apneics and 46 obese controls Dynamic magnetic resonance imaging was performed during wakefulness in the midsagittal and three axial upper airway regions (retropalatal, retroglossal, epiglottal) Differences in measurements were examined using linear regression 28
 B) Mid sagittal image showing the upper boundary set through the top of hard palate and lower boundary through the bottom of C4; the airway between")
 C E are examples of images in the three axial")

29 Dynamic Upper Airway Imaging During Wakefulness in Obese Subjects with and without Sleep Apnea (Feng et al, AJRCCM conditionally accepted) A) Mid sagittal image showing the location of the axial images (RP, RG and Epi) B) Mid sagittal image showing the upper boundary set through the top of hard palate and lower boundary through the bottom of C4; the airway between these two boundaries represents the mid sagittal airway area and the perpendicular distance between two boundaries is the length of airway. Dynamic Upper Airway Imaging During Wakefulness in Obese Subjects with and without Sleep Apnea (Feng et al, AJRCCM conditionally accepted) C E are examples of images in the three axial regions: retopalatal (C),retroglossal (D) and epiglottal (E). F shows an example of the method used to measure airway lateral and anterposterior dimensions. The lateral and anterposterior dimensions are measured in the three axial regions. RP = retropalatal, RG = retroglossal, EPI = epiglottal, AA = airway area, AL = airway length, UB = upper boundary, LB = lower boundary, AP = anterposterior, LAT = lateral 29


30 Mid-Sagittal Dynamic MRI Mid-Retropalatal Dynamic MRI 30

31 Mid-Retroglossal Dynamic MRI Demographic Characteristics of the Study Sample Measure Overall AHI 5 AHI 15 p N Age, years 48.9 ± ± ± 10.5 < Male, % 44.8% 37.0% 47.1% Race, % Caucasian 43.4% 43.5% 43.3% African American 53.2% 52.2% 53.5% Other 3.5% 4.4% 3.2% BMI, kg/m ± ± ± 7.8 < AHI, events/hour 33.4 ± ± ± 27.3 < Significant (p<0.05) differences shown in bold; p-value from T-test or chi-squared test comparing OSA vs. controls for continuous or categorical variables, respectively. Dynamic Upper Airway Imaging During Wakefulness in Obese Subjects with and without Sleep Apnea (Feng et al, AJRCCM conditionally accepted) 31
32 Dynamic Airway Measurements in Apneics and Controls Measurement AHI 5 AHI 15 N Mean ± SD N Mean ± SD p Mid-Sagittal Average airway area, mm ± ± CV of airway area, % ± ± Airway length in slice with maximum area, mm ± ± Airway length in slice with minimum area, mm ± ± Maximum airway area corrected for length, mm ± ± Minimum airway area corrected for length, mm ± ± Middle Soft Palate (Retropalatal) Average airway area, mm ± ± CV of airway area, % ± ± Maximum airway area, mm ± ± Minimum airway area, mm ± ± Lateral distance at maximum area, mm ± ± Lateral distance at minimum area, mm ± ± AP distance at maximum area, mm ± ± AP distance at minimum area, mm ± ± Significant or suggestive (p<0.05) differences shown in bold. p-value from T-test comparing dynamic measure between apneics and controls. CV = coefficient of variation. Dynamic Upper Airway Imaging During Wakefulness in Obese Subjects with and without Sleep Apnea (Feng et al, AJRCCM conditionally accepted) Dynamic Airway Measurements in Apneics and Controls Measurement AHI 5 AHI 15 N Mean ± SD N Mean ± SD Middle Tongue (Retroglossal) Average airway area, mm ± ± CV of airway area, % ± ± Maximum airway area, mm ± ± Minimum airway area, mm ± ± Lateral distance at maximum area, mm ± ± Lateral distance at minimum area, mm ± ± AP distance at maximum area, mm ± ± AP distance at minimum area, mm ± ± Middle Epiglottis (Epiglottal) Average airway area, mm ± ± CV of airway area, % ± ± Maximum airway area, mm ± ± Minimum airway area, mm ± ± Lateral distance at maximum area, mm ± ± Lateral distance at minimum area, mm ± ± AP distance at maximum area, mm ± ± AP distance at minimum area, mm ± ± Significant or suggestive (p<0.05) differences shown in bold. p-value from T-test comparing dynamic measure between apneics and controls. CV = coefficient of variation. Dynamic Upper Airway Imaging During Wakefulness in Obese Subjects with and without Sleep Apnea (Feng et al, AJRCCM conditionally accepted) p 32
33 Dynamic Upper Airway Imaging During Wakefulness in Obese Subjects with and without Sleep Apnea (Feng et al, AJRCCM conditionally accepted) Conclusions: Upper airway caliber during respiration was significantly narrower in obese apneics than obese controls in the retropalatal region There were strong correlations between AHI and dynamic airway caliber in the retropalatal and retroglossal regions These findings provide further evidence that retropalatal airway narrowing plays an important role in the pathogenesis of OSA in obese subjects New Perspectives on the Pathogenesis of OSA: Anatomic Perspective - "Take Home Messages" Increased volume of upper airway soft tissue structures is an important risk factor for sleep apnea Reduction in mandibular size is also an important risk factor for OSA The combination of increased upper airway soft tissue structures and reduced craniofacial skeleton increases OSA risk Tongue fat may explain the relationship between obesity and sleep apnea During respiration upper airway caliber is significantly narrower in obese apneics than obese controls in the retropalatal region 33

34 New Perspectives on the Pathogenesis of OSA - Anatomic Perspective Thank you for your attention! Any Questions? 34
Introduction OPT has been shown to effectively treat sleep apnea in about 40% of patients (Colrain IM et al. Sleep Medicine 14; , 2013)
") Oral Pressure Therapy for OSA Oral Pressure Therapy for OSA - Disclosures Richard J. Schwab, M.D. Professor of Medicine Division of Sleep Medicine Pulmonary, Allergy and Critical Care Division University
Oral Pressure Therapy for OSA Oral Pressure Therapy for OSA - Disclosures Richard J. Schwab, M.D. Professor of Medicine Division of Sleep Medicine Pulmonary, Allergy and Critical Care Division University
Influence of upper airways section area on oxygen blood saturation level in patients with obesity and sleep apnea syndrome
 Influence of upper airways section area on oxygen blood saturation level in patients with obesity and sleep apnea syndrome Poster No.: P-0028 Congress: ESCR 2015 Type: Scientific Poster Authors: E. Butorova,
Influence of upper airways section area on oxygen blood saturation level in patients with obesity and sleep apnea syndrome Poster No.: P-0028 Congress: ESCR 2015 Type: Scientific Poster Authors: E. Butorova,
Examining the Mechanism of Action of a New Device Using Oral Pressure Therapy for the Treatment of Obstructive Sleep Apnea
 MECHANISM OF ACTION OF A NEW DEVICE USING ORAL PRESSURE THERAPY FOR OSA http://dx.doi.org/10.5665/sleep.3846 Examining the Mechanism of Action of a New Device Using Oral Pressure Therapy for the Treatment
MECHANISM OF ACTION OF A NEW DEVICE USING ORAL PRESSURE THERAPY FOR OSA http://dx.doi.org/10.5665/sleep.3846 Examining the Mechanism of Action of a New Device Using Oral Pressure Therapy for the Treatment
Airway and Airflow Characteristics In OSAS
 Airway and Airflow Characteristics In OSAS 16 th Annual Advances in Diagnostics and Treatment of Sleep Apnea and Snoring February 12-13, 2010 San Francisco, CA Nelson B. Powell M.D., D.D.S. Adjunct Clinical
Airway and Airflow Characteristics In OSAS 16 th Annual Advances in Diagnostics and Treatment of Sleep Apnea and Snoring February 12-13, 2010 San Francisco, CA Nelson B. Powell M.D., D.D.S. Adjunct Clinical
Snoring, obstructive sleep apnea (OSA), and upper. impact of basic research on tomorrow. Snoring Imaging* Could Bernoulli Explain It All?
, and upper. impact of basic research on tomorrow. Snoring Imaging* Could Bernoulli Explain It All?") impact of basic research on tomorrow Snoring Imaging* Could Bernoulli Explain It All? Igor Fajdiga, MD, PhD Study objectives: To identify upper airway changes in snoring using CT scanning, to clarify the
impact of basic research on tomorrow Snoring Imaging* Could Bernoulli Explain It All? Igor Fajdiga, MD, PhD Study objectives: To identify upper airway changes in snoring using CT scanning, to clarify the
Sleep Apnea in Women: How Is It Different?
 Sleep Apnea in Women: How Is It Different? Grace Pien, MD, MSCE Division of Pulmonary and Critical Care Department of Medicine Johns Hopkins School of Medicine 16 February 2018 Outline Prevalence Clinical
Sleep Apnea in Women: How Is It Different? Grace Pien, MD, MSCE Division of Pulmonary and Critical Care Department of Medicine Johns Hopkins School of Medicine 16 February 2018 Outline Prevalence Clinical
Alexandria Workshop on
 Alexandria Workshop on 1 Snoring & OSA Surgery Course Director: Yassin Bahgat MD Claudio Vicini MD Course Board: Filippo Montevecchi MD Pietro Canzi MD Snoring & Obstructive ti Sleep Apnea The basic information
Alexandria Workshop on 1 Snoring & OSA Surgery Course Director: Yassin Bahgat MD Claudio Vicini MD Course Board: Filippo Montevecchi MD Pietro Canzi MD Snoring & Obstructive ti Sleep Apnea The basic information
Head and Neck Physical Examination: Comparison Between Nonapneic and Obstructive Sleep Apnea Patients
 The Laryngoscope Lippincott Williams & Wilkins, Inc. 2005 The American Laryngological, Rhinological and Otological Society, Inc. Head and Neck Physical Examination: Comparison Between Nonapneic and Obstructive
The Laryngoscope Lippincott Williams & Wilkins, Inc. 2005 The American Laryngological, Rhinological and Otological Society, Inc. Head and Neck Physical Examination: Comparison Between Nonapneic and Obstructive
Brian Palmer, D.D.S, Kansas City, Missouri, USA. April, 2001
 Brian Palmer, D.D.S, Kansas City, Missouri, USA A1 April, 2001 Disclaimer The information in this presentation is for basic information only and is not to be construed as a diagnosis or treatment for any
Brian Palmer, D.D.S, Kansas City, Missouri, USA A1 April, 2001 Disclaimer The information in this presentation is for basic information only and is not to be construed as a diagnosis or treatment for any
Anesthesia Considerations for Dynamic Upper Airway Evaluation
 Anesthesia Considerations for Dynamic Upper Airway Evaluation Mohamed Mahmoud MD Associate Professor of Anesthesia & Pediatrics Cincinnati Children s Hospital Medical Center Objectives Diagnosis of Sleep
Anesthesia Considerations for Dynamic Upper Airway Evaluation Mohamed Mahmoud MD Associate Professor of Anesthesia & Pediatrics Cincinnati Children s Hospital Medical Center Objectives Diagnosis of Sleep
Identification of Craniofacial Risk Factors for Obstructive Sleep Apnea Using Three-
 Identification of Craniofacial Risk Factors for Obstructive Sleep Apnea Using Three Dimensional MRI Luqi Chi, MD; FrancoisLouis Comyn, DMD; Nandita Mitra, PhD; Muredach P. Reilly, MD; Fei Wan, BS; Greg
Identification of Craniofacial Risk Factors for Obstructive Sleep Apnea Using Three Dimensional MRI Luqi Chi, MD; FrancoisLouis Comyn, DMD; Nandita Mitra, PhD; Muredach P. Reilly, MD; Fei Wan, BS; Greg
11/19/2012 ก! " Varies 5-86% in men 2-57% in women. Thailand 26.4% (Neruntarut et al, Sleep Breath (2011) 15: )
 15: )") Snoring ก Respiratory sound generated in the upper airway during sleep that typically occurs during inspiration but may occur during expiration ICSD-2, 2005..... ก ก! Prevalence of snoring Varies 5-86%
Snoring ก Respiratory sound generated in the upper airway during sleep that typically occurs during inspiration but may occur during expiration ICSD-2, 2005..... ก ก! Prevalence of snoring Varies 5-86%
Sleep Diordered Breathing (Part 1)
") Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Diordered Breathing (Part 1) History (for more topics & presentations, visit ) Obstructive sleep apnea - first described by Charles Dickens in 1836 in Papers of the Pickwick Club, Dickens depicted
Sleep Disorders and the Metabolic Syndrome
 Sleep Disorders and the Metabolic Syndrome Tom V. Cloward, M.D. Intermountain Sleep Disorders Center LDS Hospital Objectives Describe how sleep disorders impact your daily medical practice Don Don t do
Sleep Disorders and the Metabolic Syndrome Tom V. Cloward, M.D. Intermountain Sleep Disorders Center LDS Hospital Objectives Describe how sleep disorders impact your daily medical practice Don Don t do
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update
 OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
OBSTRUCTIVE SLEEP APNEA and WORK Treatment Update David Claman, MD Professor of Medicine Director, UCSF Sleep Disorders Center 415-885-7886 Disclosures: None Chronic Sleep Deprivation (0 v 4 v 6 v 8 hrs)
Comparative Effects of Two Oral Appliances on Upper Airway Structure in Obstructive Sleep Apnea
 COMPARISON OF EFFECTS OF ORAL APPLIANCES ON THE AIRWAY IN OSA Comparative Effects of Two Oral Appliances on Upper Airway Structure in Obstructive Sleep Apnea Kate Sutherland, PhD 1,2 ; Sheryn A. Deane,
COMPARISON OF EFFECTS OF ORAL APPLIANCES ON THE AIRWAY IN OSA Comparative Effects of Two Oral Appliances on Upper Airway Structure in Obstructive Sleep Apnea Kate Sutherland, PhD 1,2 ; Sheryn A. Deane,
Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2
 Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2 CAUSES OF SNORING AND SLEEP APNEA We inhale air through our nose and mouth. From the nostrils, air flows
Snoring and Obstructive Sleep Apnea: Patient s Guide to Minimally Invasive Treatments Chapter 2 CAUSES OF SNORING AND SLEEP APNEA We inhale air through our nose and mouth. From the nostrils, air flows
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea
 Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Surgical Options for the Successful Treatment of Obstructive Sleep Apnea Benjamin J. Teitelbaum, MD, FACS Otolaryngology Head and Neck Surgery Saint Agnes Medical Center Fresno, California Terms Apnea
Morphological variations of soft palate and influence of age on it: A digital cephalometric study
 Original Research Article Morphological variations of soft palate and influence of age on it: A digital cephalometric study C. Vani 1*, T. Vinila Lakshmi 2, V. Dheeraj Roy 3 1 Professor, 2 Post graduate
Original Research Article Morphological variations of soft palate and influence of age on it: A digital cephalometric study C. Vani 1*, T. Vinila Lakshmi 2, V. Dheeraj Roy 3 1 Professor, 2 Post graduate
Identification of Upper Airway Anatomic Risk Factors for Obstructive Sleep Apnea with Volumetric Magnetic Resonance Imaging
 Identification of Upper Airway Anatomic Risk Factors for Obstructive Sleep Apnea with Volumetric Magnetic Resonance Imaging Richard J. Schwab, Michael Pasirstein, Robert Pierson, Adonna Mackley, Robert
Identification of Upper Airway Anatomic Risk Factors for Obstructive Sleep Apnea with Volumetric Magnetic Resonance Imaging Richard J. Schwab, Michael Pasirstein, Robert Pierson, Adonna Mackley, Robert
Neuromuscular Stimulation for Sleep Apnea. Overview 1/24/2013. Disclosures. Midline Glossectomy. Palate + Hypopharyngeal Surgery: BMI
 Neuromuscular Stimulation for Sleep Apnea Disclosures The following personal financial relationships with commercial interests relevant to this presentation: Eric J. Kezirian, MD, MPH Director, Division
Neuromuscular Stimulation for Sleep Apnea Disclosures The following personal financial relationships with commercial interests relevant to this presentation: Eric J. Kezirian, MD, MPH Director, Division
Sleep Medicine. Paul Fredrickson, MD Director. Mayo Sleep Center Jacksonville, Florida.
 Sleep Medicine Paul Fredrickson, MD Director Mayo Sleep Center Jacksonville, Florida Fredrickson.Paul@mayo.edu DISCLOSURES No relevant conflicts to report. Obstructive Sleep Apnea The most common sleep
Sleep Medicine Paul Fredrickson, MD Director Mayo Sleep Center Jacksonville, Florida Fredrickson.Paul@mayo.edu DISCLOSURES No relevant conflicts to report. Obstructive Sleep Apnea The most common sleep
Updated Friedman Staging System for Obstructive Sleep Apnea
 Updated Friedman Staging System for Obstructive Sleep Apnea Michael Friedman a, b Anna M. Salapatas b Lauren B. Bonzelaar c a Section of Sleep Surgery, Rush University Medical Center, and b Section of
Updated Friedman Staging System for Obstructive Sleep Apnea Michael Friedman a, b Anna M. Salapatas b Lauren B. Bonzelaar c a Section of Sleep Surgery, Rush University Medical Center, and b Section of
Management of OSA. saurabh maji
 Management of OSA saurabh maji INTRODUCTION Obstructive sleep apnea is a major public health problem Prevalence of OSAS in INDIA is 2.4% to 4.96% in men and 1% to 2 % in women In the rest of the world
Management of OSA saurabh maji INTRODUCTION Obstructive sleep apnea is a major public health problem Prevalence of OSAS in INDIA is 2.4% to 4.96% in men and 1% to 2 % in women In the rest of the world
SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA
 SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA INTRODUCTION Snoring with or without excessive daytime somnolence, restless sleep and periods of apnoea are all manifestations of sleep disordered
SURGERY FOR SNORING AND MILD OBSTRUCTIVE SLEEP APNOEA INTRODUCTION Snoring with or without excessive daytime somnolence, restless sleep and periods of apnoea are all manifestations of sleep disordered
BTS sleep Course. Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith)
") BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
BTS sleep Course Module 10 Therapies I: Mechanical Intervention Devices (Prepared by Debby Nicoll and Debbie Smith) S1: Overview of OSA Definition History Prevalence Pathophysiology Causes Consequences
Goal of Evaluation. Overview. Characterize disorder to guide effective treatment 1/10/2018. Disclosures
 to Identify Sites of Obstruction in Patients with OSA Eric J. Kezirian, MD, MPH Professor, Otolaryngology Head & Neck Surgery President, International Surgical Sleep Society Sleep-Doctor.com Eric.Kezirian@med.usc.edu
to Identify Sites of Obstruction in Patients with OSA Eric J. Kezirian, MD, MPH Professor, Otolaryngology Head & Neck Surgery President, International Surgical Sleep Society Sleep-Doctor.com Eric.Kezirian@med.usc.edu
Sleep Apnea: Vascular and Metabolic Complications
 Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Sleep Apnea: Vascular and Metabolic Complications Vahid Mohsenin, M.D. Professor of Medicine Yale University School of Medicine Director, Yale Center for Sleep Medicine Definitions Apnea: Cessation of
Outline. Major variables contributing to airway patency/collapse. OSA- Definition
 Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
Outline Alicia Gruber Kalamas, MD Associate Clinical Professor of Anesthesia & Perioperative Care University of California, San Francisco September 2011 Definition Pathophysiology Patient Risk Factors
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Hypoglossal Nerve Stimulation in the Treatment of Obstructive Sleep Apnea MP-079-MD-DE Medical Management Provider Notice
Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Hypoglossal Nerve Stimulation in the Treatment of Obstructive Sleep Apnea MP-079-MD-DE Medical Management Provider Notice
Obstructive Sleep Apnea in Truck Drivers
 Rocky Mountain Academy of Occupational and Environmental Medicine Denver, Colorado February 6, 2010 Obstructive Sleep Apnea in Truck Drivers Philip D. Parks, MD, MPH, MOccH Medical Director, Lifespan Health
Rocky Mountain Academy of Occupational and Environmental Medicine Denver, Colorado February 6, 2010 Obstructive Sleep Apnea in Truck Drivers Philip D. Parks, MD, MPH, MOccH Medical Director, Lifespan Health
Year in Review. Outline of Lecture
 Year in Review Allan I. Pack, M.B.Ch.B., Ph.D. John Miclot Professor of Medicine Director, Center for Sleep and Circadian Neurobiology University of Pennsylvania Perelman School of Medicine Philadelphia,
Year in Review Allan I. Pack, M.B.Ch.B., Ph.D. John Miclot Professor of Medicine Director, Center for Sleep and Circadian Neurobiology University of Pennsylvania Perelman School of Medicine Philadelphia,
Upper Airway Obstruction
 Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Upper Airway Obstruction Adriaan Pentz Division of Otorhinolaryngology University of Stellenbosch and Tygerberg Hospital Stridor/Stertor Auditory manifestations of disordered respiratory function ie noisy
Nasal Mass Presenting as Obstructive Sleep Apnea Syndrome
 ORIGINAL ARTICLE pissn 2093-9175 / eissn 2233-8853 http://dx.doi.org/10.17241/smr.2015.6.2.54 Nasal Mass Presenting as Obstructive Sleep Apnea Syndrome Seung Hoon Lee, MD, PhD, In Sik Song, MD, Jae Woo
ORIGINAL ARTICLE pissn 2093-9175 / eissn 2233-8853 http://dx.doi.org/10.17241/smr.2015.6.2.54 Nasal Mass Presenting as Obstructive Sleep Apnea Syndrome Seung Hoon Lee, MD, PhD, In Sik Song, MD, Jae Woo
Medicare C/D Medical Coverage Policy
 Medicare C/D Medical Coverage Policy Surgical Treatment of Obstructive Sleep Apnea Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January, 2019 DESCRIPTION OF PROCEDURE OR SERVICE
Medicare C/D Medical Coverage Policy Surgical Treatment of Obstructive Sleep Apnea Origination: June 26, 2000 Review Date: January 18, 2017 Next Review January, 2019 DESCRIPTION OF PROCEDURE OR SERVICE
Obstructive sleep apnoea (OSA) has been. Heritability of upper airway dimensions derived using acoustic pharyngometry
 has been. Heritability of upper airway dimensions derived using acoustic pharyngometry") Eur Respir J 2008; 32: 1304 1308 DOI: 10.1183/09031936.00029808 CopyrightßERS Journals Ltd 2008 Heritability of upper airway dimensions derived using acoustic pharyngometry S.R. Patel*,#, J.M. Frame #,
Eur Respir J 2008; 32: 1304 1308 DOI: 10.1183/09031936.00029808 CopyrightßERS Journals Ltd 2008 Heritability of upper airway dimensions derived using acoustic pharyngometry S.R. Patel*,#, J.M. Frame #,
Upper Airway Stimulation for Obstructive Sleep Apnea
 Upper Airway Stimulation for Obstructive Sleep Apnea Background, Mechanism and Clinical Data Overview Seth Hollen RPSGT 21 May 2016 1 Conflicts of Interest Therapy Support Specialist, Inspire Medical Systems
Upper Airway Stimulation for Obstructive Sleep Apnea Background, Mechanism and Clinical Data Overview Seth Hollen RPSGT 21 May 2016 1 Conflicts of Interest Therapy Support Specialist, Inspire Medical Systems
Cause and Prevention of OSA. Principles involved in OSA Hypothesis Prevention
 Cause and Prevention of OSA Principles involved in OSA Hypothesis Prevention D1 Principles involved in airway collapse Vacuum Gravity Venturi principle Bernoulli principle D2 Vacuum D3 A vacuum can create
Cause and Prevention of OSA Principles involved in OSA Hypothesis Prevention D1 Principles involved in airway collapse Vacuum Gravity Venturi principle Bernoulli principle D2 Vacuum D3 A vacuum can create
Pediatric OSA. Pediatric OSA: Treatment Options Beyond AT. Copyright (c) 2012 Boston Children's Hospital 1
 2012 Boston Children's Hospital 1") Pediatric OSA Treatments Options Beyond AT Report of Financial Relationships (past 12 months) with commercial entities producing, marketing, re selling, or distributing health care goods or services consumed
Pediatric OSA Treatments Options Beyond AT Report of Financial Relationships (past 12 months) with commercial entities producing, marketing, re selling, or distributing health care goods or services consumed
Sleep Apnoea : its impact outside the chest. Dr Tom Mackay Consultant Respiratory Physician Royal Infirmary Edinburgh
 Sleep Apnoea : its impact outside the chest Dr Tom Mackay Consultant Respiratory Physician Royal Infirmary Edinburgh Body Mass Index < 20 kg/m 2 20-25 kg/m 2 25-30 kg/m 2 > 30 kg/m 2 underweight normal
Sleep Apnoea : its impact outside the chest Dr Tom Mackay Consultant Respiratory Physician Royal Infirmary Edinburgh Body Mass Index < 20 kg/m 2 20-25 kg/m 2 25-30 kg/m 2 > 30 kg/m 2 underweight normal
ORIGINAL ARTICLE. for mild to moderate obstructive
 ORIGINAL ARTICLE An Investigation of Upper Airway Changes Associated With Mandibular Advancement Device Using Sleep Videofluoroscopy in Patients With Obstructive Sleep Apnea Chul Hee Lee, MD, PhD; Jeong-Whun
ORIGINAL ARTICLE An Investigation of Upper Airway Changes Associated With Mandibular Advancement Device Using Sleep Videofluoroscopy in Patients With Obstructive Sleep Apnea Chul Hee Lee, MD, PhD; Jeong-Whun
Upper Airway Fat Tissue Distribution in Subjects With Obstructive Sleep Apnea and Its Effect on Retropalatal Mechanical Loads
 Upper Airway Fat Tissue Distribution in Subjects With Obstructive Sleep Apnea and Its Effect on Retropalatal Mechanical Loads Yanru Li MD, Na Lin MD, Jingying Ye MD PhD, Qinglin Chang MD, Demin Han MD
Upper Airway Fat Tissue Distribution in Subjects With Obstructive Sleep Apnea and Its Effect on Retropalatal Mechanical Loads Yanru Li MD, Na Lin MD, Jingying Ye MD PhD, Qinglin Chang MD, Demin Han MD
Association of Palatine Tonsil Size and Obstructive Sleep Apnea in Adults
 The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Association of Palatine Tonsil Size and Obstructive Sleep Apnea in Adults Sebastian M. Jara, MD ; Edward
The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Association of Palatine Tonsil Size and Obstructive Sleep Apnea in Adults Sebastian M. Jara, MD ; Edward
The Mandibular Advancement Device and Patient Selection in the Treatment of Obstructive Sleep Apnea
 ORIGINAL ARTICLE The Mandibular Advancement Device and Patient Selection in the Treatment of Obstructive Sleep Apnea Chul Hee Lee, MD; Ji-Hun Mo, MD; Ik-Joon Choi, MD; Hyun Jong Lee, MD; Beom Seok Seo,
ORIGINAL ARTICLE The Mandibular Advancement Device and Patient Selection in the Treatment of Obstructive Sleep Apnea Chul Hee Lee, MD; Ji-Hun Mo, MD; Ik-Joon Choi, MD; Hyun Jong Lee, MD; Beom Seok Seo,
Snoring and Its Outcomes
 Disclosures None Snoring and Its Outcomes Jolie Chang, MD Otolaryngology, Head and Neck Surgery University of California, San Francisco February 14, 2014 Otolaryngology Head Outline Snoring and OSA Acoustics
Disclosures None Snoring and Its Outcomes Jolie Chang, MD Otolaryngology, Head and Neck Surgery University of California, San Francisco February 14, 2014 Otolaryngology Head Outline Snoring and OSA Acoustics
Contemporary Snoring Management
 Contemporary Snoring Management Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu Sleepsurgery.ucsf.edu
Contemporary Snoring Management Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu Sleepsurgery.ucsf.edu
Snoring: What Works?
 Snoring: What Works? Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu Sleepsurgery.ucsf.edu
Snoring: What Works? Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu Sleepsurgery.ucsf.edu
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome
 The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
The most accurate predictors of arterial hypertension in patients with Obstructive Sleep Apnea Syndrome Natsios Georgios University Hospital of Larissa, Greece Definitions Obstructive Sleep Apnea (OSA)
Ped e iat a r t i r c c S lee e p e A p A nea e a Surg r er e y
 Airway Imaging in Pediatric OSA Kasey Li, MD, DDS, FACS Stanford University Sleep Medicine Program The airway is smaller in children with OSA compared to controls The adenoid and tonsils are larger and
Airway Imaging in Pediatric OSA Kasey Li, MD, DDS, FACS Stanford University Sleep Medicine Program The airway is smaller in children with OSA compared to controls The adenoid and tonsils are larger and
Tongue Fat and its Relationship to Obstructive Sleep Apnea
 pii: sp-00806-13 http://dx.doi.org/10.5665/sleep.4072 TONGUE FAT AND ITS RELATIONSHIP TO OBSTRUCTIVE SLEEP APNEA Tongue Fat and its Relationship to Obstructive Sleep Apnea Andrew M. Kim, BS 1 ; Brendan
pii: sp-00806-13 http://dx.doi.org/10.5665/sleep.4072 TONGUE FAT AND ITS RELATIONSHIP TO OBSTRUCTIVE SLEEP APNEA Tongue Fat and its Relationship to Obstructive Sleep Apnea Andrew M. Kim, BS 1 ; Brendan
Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine
 Management of pediatric OSA Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine Chulalongkorn University Treatment modalities Surgery Medications NIV during
Management of pediatric OSA Suchada Sritippayawan, MD Div. Pulmonology & Critical Care Dept. Pediatrics, Faculty of Medicine Chulalongkorn University Treatment modalities Surgery Medications NIV during
Hypoglossal Nerve Stimulator Surgery for treatment of OSA. Disclosures. Hypoglossal Nerve Stimulation 11/9/2016
 Hypoglossal Nerve Stimulator Surgery for treatment of OSA olando Molina MD South Florida ENT Associates A Disclosures I do not have any relevant financial disclosures at this time. Hypoglossal Nerve Stimulation
Hypoglossal Nerve Stimulator Surgery for treatment of OSA olando Molina MD South Florida ENT Associates A Disclosures I do not have any relevant financial disclosures at this time. Hypoglossal Nerve Stimulation
Overview. Goal of Evaluation. DISE: Identifying the Sites of Obstruction in OSA. Characterize disorder to guide effective treatment.
 DISE: Identifying the Sites of Obstruction in OSA Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu
DISE: Identifying the Sites of Obstruction in OSA Eric J. Kezirian, MD, MPH Director, Division of Sleep Surgery Otolaryngology Head and Neck Surgery University of California, San Francisco ekezirian@ohns.ucsf.edu
Sleep Apnea. Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa
 Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Sleep Apnea Herbert A Berger, MD Pulmonary Division Department of Internal Medicine University of Iowa Disclosures No Relevant Financial Interests to Report Objectives Learn the history and physical examination
Obstructive sleep apnea (OSA)
") Obstructive sleep apnea (OSA) In a healthy sleeping child, the mouth is typically closed, the oral cavity is collapsed, and the nasopharynx and hypopharynx are patent with minimal wall motion Obstructive
Obstructive sleep apnea (OSA) In a healthy sleeping child, the mouth is typically closed, the oral cavity is collapsed, and the nasopharynx and hypopharynx are patent with minimal wall motion Obstructive
Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty: A Single University Experience
 771395AORXXX10.1177/0003489418771395Annals of Otology, Rhinology & LaryngologyHuntley et al research-article2018 Original Article Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty:
771395AORXXX10.1177/0003489418771395Annals of Otology, Rhinology & LaryngologyHuntley et al research-article2018 Original Article Comparing Upper Airway Stimulation to Expansion Sphincter Pharyngoplasty:
Snoring And Sleep Apnea in the U.S. Definitions Apnea: Cessation of ventilation for > 10 seconds. Defining Severity of OSA
 Snoring and Obstructive Sleep Apnea: Oral Appliance Therapy Management Midwest Society of Orthodontists October 16-17, 2009 Anthony J DiAngelis DMD, MPH Chief, Department of Dentistry, HCMC Professor,
Snoring and Obstructive Sleep Apnea: Oral Appliance Therapy Management Midwest Society of Orthodontists October 16-17, 2009 Anthony J DiAngelis DMD, MPH Chief, Department of Dentistry, HCMC Professor,
Is CPAP helpful in severe Asthma?
 Is CPAP helpful in severe Asthma? P RAP UN KI TTIVORAVITKUL, M.D. PULMONARY AND CRITICAL CARE DIVISION DEPARTMENT OF MEDICINE, PHRAMONGKUTKLAO HOSPITAL Outlines o Obstructive sleep apnea syndrome (OSAS)
Is CPAP helpful in severe Asthma? P RAP UN KI TTIVORAVITKUL, M.D. PULMONARY AND CRITICAL CARE DIVISION DEPARTMENT OF MEDICINE, PHRAMONGKUTKLAO HOSPITAL Outlines o Obstructive sleep apnea syndrome (OSAS)
Morphometric Analysis of Left & Right Tonsils in Adult Symptomatic Type 1 Chiari Patients and Healthy Controls
 The University of Akron IdeaExchange@UAkron Honors Research Projects The Dr. Gary B. and Pamela S. Williams Honors College Spring 2015 Morphometric Analysis of Left & Right Tonsils in Adult Symptomatic
The University of Akron IdeaExchange@UAkron Honors Research Projects The Dr. Gary B. and Pamela S. Williams Honors College Spring 2015 Morphometric Analysis of Left & Right Tonsils in Adult Symptomatic
Obstructive Sleep Apnea and COPD overlap syndrome. Financial Disclosures. Outline 11/1/2016
 Obstructive Sleep Apnea and COPD overlap syndrome Chitra Lal, MD, FCCP, FAASM Associate Professor of Medicine, Pulmonary, Critical Care, and Sleep, Medical University of South Carolina Financial Disclosures
Obstructive Sleep Apnea and COPD overlap syndrome Chitra Lal, MD, FCCP, FAASM Associate Professor of Medicine, Pulmonary, Critical Care, and Sleep, Medical University of South Carolina Financial Disclosures
Original Article. Chisato Iida-Kondo 1, Norio Yoshino 4, Tohru Kurabayashi 4, Shirou Mataki 2, Makoto Hasegawa 3 and Norimasa Kurosaki 1
 J Med Dent Sci 2006; 53: 119 126 Original Article Comparison of Tongue Volume/Oral Cavity Volume Ratio between Obstructive Sleep Apnea Syndrome Patients and Normal Adults Using Magnetic Resonance Imaging
J Med Dent Sci 2006; 53: 119 126 Original Article Comparison of Tongue Volume/Oral Cavity Volume Ratio between Obstructive Sleep Apnea Syndrome Patients and Normal Adults Using Magnetic Resonance Imaging
Brazilian Journal of OTORHINOLARYNGOLOGY. Obstructive sleep apnea and primary snoring: diagnosis. Objective.
 Braz J Otorhinolaryngol. 2014;80(1 Supl. 1):S1-S16 Brazilian Journal of OTORHINOLARYNGOLOGY www.bjorl.org.br GUIDELINE Obstructive sleep apnea and primary snoring: diagnosis Authors Associação Brasileira
Braz J Otorhinolaryngol. 2014;80(1 Supl. 1):S1-S16 Brazilian Journal of OTORHINOLARYNGOLOGY www.bjorl.org.br GUIDELINE Obstructive sleep apnea and primary snoring: diagnosis Authors Associação Brasileira
Questions: What tests are available to diagnose sleep disordered breathing? How do you calculate overall AHI vs obstructive AHI?
 Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
Pediatric Obstructive Sleep Apnea Case Study : Margaret-Ann Carno PhD, CPNP, D,ABSM for the Sleep Education for Pulmonary Fellows and Practitioners, SRN ATS Committee April 2014. Facilitator s guide Part
IEHP considers the treatment of obstructive sleep apnea (OSA) medically necessary according to the criteria outlined below:
 medically necessary according to the criteria outlined below:") : Positive Airway Pressure, Oral Appliances, and Surgical Interventions Policy: Obstructive sleep apnea (OSA) is characterized by an interruption of breathing during sleep most commonly due to extra or
: Positive Airway Pressure, Oral Appliances, and Surgical Interventions Policy: Obstructive sleep apnea (OSA) is characterized by an interruption of breathing during sleep most commonly due to extra or
Pharyngeal shape and dimensions in healthy
 722 Pulmonary Division D Rodenstein Y Thomas G Liistro D C Stanescu Radiology Department G Dooms Electrophysiology Laboratory C Cuke G Aubert-Tulkens Cliniques Universitaires St Luc, Brussels, Belgium
722 Pulmonary Division D Rodenstein Y Thomas G Liistro D C Stanescu Radiology Department G Dooms Electrophysiology Laboratory C Cuke G Aubert-Tulkens Cliniques Universitaires St Luc, Brussels, Belgium
An update on childhood sleep-disordered breathing
 An update on childhood sleep-disordered breathing แพทย หญ งวนพร อน นตเสร ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร มหาว ทยาล ยสงขลานคร นทร Sleep-disordered breathing Primary snoring Upper airway resistance syndrome
An update on childhood sleep-disordered breathing แพทย หญ งวนพร อน นตเสร ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร มหาว ทยาล ยสงขลานคร นทร Sleep-disordered breathing Primary snoring Upper airway resistance syndrome
Update on Sleep Apnea Diagnosis and Treatment
 Update on Sleep Apnea Diagnosis and Treatment Damien Stevens MD Pulmonary/Critical Care/Sleep Medicine Medical Director KU Medical Center Sleep Laboratory Objectives Discuss physiology of sleep and obstructive
Update on Sleep Apnea Diagnosis and Treatment Damien Stevens MD Pulmonary/Critical Care/Sleep Medicine Medical Director KU Medical Center Sleep Laboratory Objectives Discuss physiology of sleep and obstructive
Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome
 Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome Director, Sleep Laboratory Center for Pediatric Sleep Disorders Boston Children s Hospital Copyright 2014 Boston Children s Hospital
Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome Director, Sleep Laboratory Center for Pediatric Sleep Disorders Boston Children s Hospital Copyright 2014 Boston Children s Hospital
Obesity, Weight Loss and Obstructive Sleep Apnea
 Obesity, Weight Loss and Obstructive Sleep Apnea Gary D. Foster, Ph.D. Center for Obesity Research and Education Temple University School of Medicine Overview Sociocultural context Obesity: Prevalence
Obesity, Weight Loss and Obstructive Sleep Apnea Gary D. Foster, Ph.D. Center for Obesity Research and Education Temple University School of Medicine Overview Sociocultural context Obesity: Prevalence
Sleep Apnea and CardioMetabolic Syndrome in women
 Sleep Apnea and CardioMetabolic Syndrome in women 신원철 강동경희대병원신경과, 수면센터 1 Today s Talks 폐쇄성수면무호흡증의정의와발생기전 수면무호흡증의합병증 : 고혈압, 관상동맥질환, 부정맥, 뇌졸중, 돌연사, 당뇨, 대사증후군 여성에서의폐쇄성수면무호흡증 폐쇄성수면무호흡증 (Obstructive Sleep Apnea:
Sleep Apnea and CardioMetabolic Syndrome in women 신원철 강동경희대병원신경과, 수면센터 1 Today s Talks 폐쇄성수면무호흡증의정의와발생기전 수면무호흡증의합병증 : 고혈압, 관상동맥질환, 부정맥, 뇌졸중, 돌연사, 당뇨, 대사증후군 여성에서의폐쇄성수면무호흡증 폐쇄성수면무호흡증 (Obstructive Sleep Apnea:
Roles of Surgery in OSA MASM Annual Fall Conference 2017 October 14, 2017 Kathleen Yaremchuk, MD, MSA Chair, Department of Otolaryngology/Head and
 Roles of Surgery in OSA MASM Annual Fall Conference 2017 October 14, 2017 Kathleen Yaremchuk, MD, MSA Chair, Department of Otolaryngology/Head and Neck Surgery Senior Staff Sleep Medicine Henry Ford Hospital
Roles of Surgery in OSA MASM Annual Fall Conference 2017 October 14, 2017 Kathleen Yaremchuk, MD, MSA Chair, Department of Otolaryngology/Head and Neck Surgery Senior Staff Sleep Medicine Henry Ford Hospital
Upper Airway Muscle Stimulation for Obstructive Sleep Apnea
 Upper Airway Muscle Stimulation for Obstructive Sleep Apnea M. Safwan Badr, MD, MBA Chair, Department of Medicine, Wayne State University School of Medicine. Staff Physician, John D. Dingell VA Medical
Upper Airway Muscle Stimulation for Obstructive Sleep Apnea M. Safwan Badr, MD, MBA Chair, Department of Medicine, Wayne State University School of Medicine. Staff Physician, John D. Dingell VA Medical
Sleep Apnoea. The Story of a Pause
 Sleep Apnoea The Story of a Pause There is almost zero awareness in India that many amongst us maybe living with Sleep Apnoea, which left untreated could be life threatening tomorrow. This largely undiagnosed
Sleep Apnoea The Story of a Pause There is almost zero awareness in India that many amongst us maybe living with Sleep Apnoea, which left untreated could be life threatening tomorrow. This largely undiagnosed
Modified Uvulopalatopharyngoplasty: The Extended Uvulopalatal Flap
 Modified Uvulopalatopharyngoplasty: The Extended Uvulopalatal Flap Hseuh-Yu Li, MD,* Kasey K. Li, MD, DDS, Ning-Hung Chen, MD, and Pa-Chun Wang, MD Objective: To investigate the surgical outcomes of a
Modified Uvulopalatopharyngoplasty: The Extended Uvulopalatal Flap Hseuh-Yu Li, MD,* Kasey K. Li, MD, DDS, Ning-Hung Chen, MD, and Pa-Chun Wang, MD Objective: To investigate the surgical outcomes of a
Obstructive Sleep Apnea Syndrome
 SMGr up Obstructive Sleep Apnea Syndrome Alper Dilci, Handan Koyuncu and Vural Fidan* Otorhinolaryngology Department, Yunus Emre Government Hospital, Turkey *Corresponding author: Vural Fidan, Otorhinolaryngology
SMGr up Obstructive Sleep Apnea Syndrome Alper Dilci, Handan Koyuncu and Vural Fidan* Otorhinolaryngology Department, Yunus Emre Government Hospital, Turkey *Corresponding author: Vural Fidan, Otorhinolaryngology
Overnight fluid shifts in subjects with and without obstructive sleep apnea
 Original Article Overnight fluid shifts in subjects with and without obstructive sleep apnea Ning Ding 1 *, Wei Lin 2 *, Xi-Long Zhang 1, Wen-Xiao Ding 1, Bing Gu 3, Bu-Qing Ni 4, Wei Zhang 4, Shi-Jiang
Original Article Overnight fluid shifts in subjects with and without obstructive sleep apnea Ning Ding 1 *, Wei Lin 2 *, Xi-Long Zhang 1, Wen-Xiao Ding 1, Bing Gu 3, Bu-Qing Ni 4, Wei Zhang 4, Shi-Jiang
Basic Anatomy and Physiology of the Lips and Oral Cavity. Dr. Faghih
 Basic Anatomy and Physiology of the Lips and Oral Cavity Dr. Faghih It is divided into seven specific subsites : 1. Lips 2. dentoalveolar ridges 3. oral tongue 4. retromolar trigone 5. floor of mouth 6.
Basic Anatomy and Physiology of the Lips and Oral Cavity Dr. Faghih It is divided into seven specific subsites : 1. Lips 2. dentoalveolar ridges 3. oral tongue 4. retromolar trigone 5. floor of mouth 6.
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
UCSD Pulmonary and Critical Care
 Sleep Apnea Phenotyping Atul Malhotra, MD amalhotra@ucsd.edu UCSD Pulmonary and Critical Care Director of Sleep Medicine NAMDRC 2014 Dr. Malhotra has declared no conflicts of interest related to the content
Sleep Apnea Phenotyping Atul Malhotra, MD amalhotra@ucsd.edu UCSD Pulmonary and Critical Care Director of Sleep Medicine NAMDRC 2014 Dr. Malhotra has declared no conflicts of interest related to the content
The future of health is digital
 Dated: XX/XX/XXXX Name: XXXXXXXX XXXXXXXXXXX Birth Date: XX/XX/XXXX Date of scan: XX/XX/XXXX Examination of the anatomical volume: The following structures are reviewed and evaluated for bilateral symmetry,
Dated: XX/XX/XXXX Name: XXXXXXXX XXXXXXXXXXX Birth Date: XX/XX/XXXX Date of scan: XX/XX/XXXX Examination of the anatomical volume: The following structures are reviewed and evaluated for bilateral symmetry,
Surgical Treatment of OSA. Han-Soo Bae, MD Monroe Ear Nose and Throat Associates May 5, 2017
 Surgical Treatment of OSA Han-Soo Bae, MD Monroe Ear Nose and Throat Associates May 5, 2017 Disclosure None Treatment of OSA PAP Oral appliance Surgery OSA and Mortality Surgical Treatment of OSA Surgery
Surgical Treatment of OSA Han-Soo Bae, MD Monroe Ear Nose and Throat Associates May 5, 2017 Disclosure None Treatment of OSA PAP Oral appliance Surgery OSA and Mortality Surgical Treatment of OSA Surgery
JlntSocPlastination, Vol4:16-22,
 JlntSocPlastination, Vol4:16-22, 1990 16 SECTIONAL ANATOMY: STANDARDIZED METHODOLOGY Alexander Lane, Coordinator of Anatomy and Physiology, Triton College, Visiting Associate Professor, University of Illinois
JlntSocPlastination, Vol4:16-22, 1990 16 SECTIONAL ANATOMY: STANDARDIZED METHODOLOGY Alexander Lane, Coordinator of Anatomy and Physiology, Triton College, Visiting Associate Professor, University of Illinois
Precision Sleep Medicine
 Precision Sleep Medicine Picking Winners Improves Outcomes and Avoids Side-Effects North American Dental Sleep Medicine Conference February 17-18, 2017 Clearwater Beach, FL John E. Remmers, MD Conflict
Precision Sleep Medicine Picking Winners Improves Outcomes and Avoids Side-Effects North American Dental Sleep Medicine Conference February 17-18, 2017 Clearwater Beach, FL John E. Remmers, MD Conflict
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Accidents. See Motor vehicle accidents. Acetazolamide, in OSA therapy, 531 Acetylcholinesterase inhibitors, in OSA therapy, 532 533 Acromegaly,
Note: Page numbers of article titles are in boldface type. A Accidents. See Motor vehicle accidents. Acetazolamide, in OSA therapy, 531 Acetylcholinesterase inhibitors, in OSA therapy, 532 533 Acromegaly,
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Obstructive Sleep Apnea Diagnosis and Management TEXAS ACADEMY OF FAMILY PRACTICE NOVEMBER 10, 2018 W. DAVID BROWN, PHD, FAASM, CBSM
 Obstructive Sleep Apnea Diagnosis and Management TEXAS ACADEMY OF FAMILY PRACTICE NOVEMBER 10, 2018 W. DAVID BROWN, PHD, FAASM, CBSM Speaker Disclosure Dr. Brown has disclosed that he has no actual or
Obstructive Sleep Apnea Diagnosis and Management TEXAS ACADEMY OF FAMILY PRACTICE NOVEMBER 10, 2018 W. DAVID BROWN, PHD, FAASM, CBSM Speaker Disclosure Dr. Brown has disclosed that he has no actual or
Cone-beam CT analysis of patients with obstructive sleep apnea compared to normal controls
 Imaging Science in Dentistry 2016; 46: 9-16 http://dx.doi.org/10.5624/isd.2016.46.1.9 Cone-beam CT analysis of patients with obstructive sleep apnea compared to normal controls Allison Buchanan 1, *, Ruben
Imaging Science in Dentistry 2016; 46: 9-16 http://dx.doi.org/10.5624/isd.2016.46.1.9 Cone-beam CT analysis of patients with obstructive sleep apnea compared to normal controls Allison Buchanan 1, *, Ruben
CSS PHYSICAL ASSESSMENT
 CSS PHYSICAL ASSESSMENT Date... IDNumber... Name... Date of Birth... Consent Blood Pressure Urine, shower Blood yes No Cogstate Stanford Pre, Stanford Post Height Weight Skinfolds Neck Circumference Pharyngeal
CSS PHYSICAL ASSESSMENT Date... IDNumber... Name... Date of Birth... Consent Blood Pressure Urine, shower Blood yes No Cogstate Stanford Pre, Stanford Post Height Weight Skinfolds Neck Circumference Pharyngeal
Investigation of positional and non-positional OSA: impact. on outcomes in patients treated with mandibular
 Investigation of positional and non-positional OSA: impact on outcomes in patients treated with mandibular advancement devices Short title: Oral Appliances in positional and non-positional OSA JIN WOO
Investigation of positional and non-positional OSA: impact on outcomes in patients treated with mandibular advancement devices Short title: Oral Appliances in positional and non-positional OSA JIN WOO
If you suspect airway problems, get a second opinion before you anaesthetise, not after!
 Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Obstructive sleep apnoea hypopnoea syndrome (OSAHS)
") Obstructive sleep apnoea hypopnoea syndrome (OSAHS) G C Mbata and J C Chukwuka Introduction Obstructive sleep apnoea hypopnoea syndrome (OSAHS) is an important medical condition that has received increasing
Obstructive sleep apnoea hypopnoea syndrome (OSAHS) G C Mbata and J C Chukwuka Introduction Obstructive sleep apnoea hypopnoea syndrome (OSAHS) is an important medical condition that has received increasing
Impact of tongue size on occlusion.
 Impact of tongue size on occlusion. D1 D2 Macroglossia (large tongue) in patient with severe OSA D3 Massive tongue can impact position of teeth. D4 This massive tongue has contributed to Class III occlusion.
Impact of tongue size on occlusion. D1 D2 Macroglossia (large tongue) in patient with severe OSA D3 Massive tongue can impact position of teeth. D4 This massive tongue has contributed to Class III occlusion.
Does the Oropharyngeal Fat Tissue Influence the Oropharyngeal Airway in Snorers? Dynamic CT Study
 Does the Oropharyngeal Fat Tissue Influence the Oropharyngeal Airway in Snorers? Dynamic CT Study Tolga Aksoz, MD 1 Huseyin Akan, MD 1 Mehmet Celebi, MD 2 Banu Baglan Sakan, MD 1 Index terms: Computed
Does the Oropharyngeal Fat Tissue Influence the Oropharyngeal Airway in Snorers? Dynamic CT Study Tolga Aksoz, MD 1 Huseyin Akan, MD 1 Mehmet Celebi, MD 2 Banu Baglan Sakan, MD 1 Index terms: Computed
Pediatric Obstructive Sleep apnea An update What else is there to know?
 Pediatric Obstructive Sleep apnea An update What else is there to know? Garani S. Nadaraja, MD, FAAP Medical Director BCH-Oakland Clinical Assistant Professor Division of Pediatric Otolaryngology UCSF
Pediatric Obstructive Sleep apnea An update What else is there to know? Garani S. Nadaraja, MD, FAAP Medical Director BCH-Oakland Clinical Assistant Professor Division of Pediatric Otolaryngology UCSF
Obstructive Sleep Apnea In The Perioperative Setting. Christopher Karcher, MD Diplomate, ABPN Medical Director The Neuroscience Sleep Center
 Obstructive Sleep Apnea In The Perioperative Setting Christopher Karcher, MD Diplomate, ABPN Medical Director The Neuroscience Sleep Center Obstructive Sleep Apnea Cyclic collapse of upper airway tissues
Obstructive Sleep Apnea In The Perioperative Setting Christopher Karcher, MD Diplomate, ABPN Medical Director The Neuroscience Sleep Center Obstructive Sleep Apnea Cyclic collapse of upper airway tissues
Diagnosis and Management of Obstructive Sleep Apnea in Primary Care
 Saturday General Session Diagnosis and Management of Obstructive Sleep Apnea in Primary Care W. David Brown, PhD Sleep Psychologist, Department of Psychiatry Children s Medical Center Dallas, Texas Educational
Saturday General Session Diagnosis and Management of Obstructive Sleep Apnea in Primary Care W. David Brown, PhD Sleep Psychologist, Department of Psychiatry Children s Medical Center Dallas, Texas Educational
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA)
") PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
PEDIATRIC OBSTRUCTIVE SLEEP APNEA (OSA) DEFINITION OSA Inspiratory airflow is either partly (hypopnea) or completely (apnea) occluded during sleep. The combination of sleep-disordered breathing with daytime
Tired of being tired?
 Tired of being tired? Narval CC MRD ResMed.com/Narval Sleepiness and snoring are possible symptoms of sleep apnea. Did you know that one in every four adults has some form of sleep disordered-breathing
Tired of being tired? Narval CC MRD ResMed.com/Narval Sleepiness and snoring are possible symptoms of sleep apnea. Did you know that one in every four adults has some form of sleep disordered-breathing