LVADs, Supraglottic Airways and CPAP
|
|
|
- Sybil Williamson
- 5 years ago
- Views:
Transcription

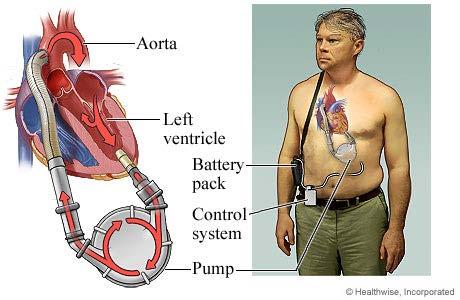
1 LVADs, Supraglottic Airways and CPAP David M. Landsberg, MD, FF/EMT-P, FACP, FCCP Chief of Medicine Crouse Hospital Associate Professor of Medicine and Emergency Medicine Upstate 38MD-1, 83MD-1, 98MD-4
2 I have no relevant conflicts to disclose
3 LVADs in CNY URMC has 160 LVADs in the community Approximately 40 in CNY 3 Artificial Hearts at URMC No Total Artificial Hearts in the community
4
5

6

7

8

9 Jarvik Post-Auricular Cable White Pump Blue Internal Cable Green Connector Yellow Controller Grey Battery Black External Cables

10 Jarvik Post-Auricular Cable

11

12

13

14

15
16

17

18 LOOK Connections intact? Green light?

19 LISTEN Hum? If no hum, back to Look If Look not helpful then forward to Feel

20 FEEL Control Box Temperature Thrombosis of pump or outflow cannula Dislodgement outflow cannula Distal Obstruction
21 Complications Major VAD Complications Bleeding Thrombosis Infection sepsis is leading cause of death in long-term VAD support RV dysfunction/failure Suckdown (low preload causes a nonpulsatle VAD to collapse the ventricle) Device failure/malfunction (highly variable by device type) Hemolysis (the VAD destroys blood cells)
22 Complications Other Common Issues Hypertension High afterload can limit VAD flow/ output Do not administer antihypertensive medications or nitrates unless instructed by a physician or VAD Coordinator Hypotension/ loss of Preload All VADs are preload dependent. A loss or reduction in preload will compromise VAD function and limit flow/ output
23 Complications Other Common Issues Depression/ Adjustment Disorders Living with a VAD is difficult to management for a lot of patients. A large percentage of patients experience symptoms of depression Portability/ Ergonomics The external VAD equipment is heavy and cumbersome limiting a patient s mobility and greatly impacting their quality of life.
24 Complications Bleeding & Thrombosis Careful control of anticoagulation is imperative Patients are often on both anticoagulants and platelet inhibitors Device thrombosis rare in pulsatile devices typically revealed by increased power and signs and symptoms of hemolysis
25 Complications Bleeding & Thrombosis Tx Assess for signs and symptoms of bleeding Neuro Assessment to rule out CVA Initiate IV therapy and administer fluid slowly to maintain preload Device Thrombus is treated with low dose lytics and/ or increasing anticoagulation therapy
26 Complications Infection The leading cause of mortality in VAD patients Higher incidence in pulsatile VADs Direct access into the body and into the blood stream Often recurrent and difficult to treat
27 Complications Treating Suckdown Initiate a peripheral IV and slowly give volume to increase preload If able and instructed by the VAD Coordinator, reduce the speed of the VAD Assess for signs and symptoms of bleeding and sepsis
28 Complications Hemolysis Blood cells are destroyed as they travel through the VAD More common in non pulsatile devices
29 Complications Treating Hemolysis Initiate a peripheral IV and slowly give volume If able and instructed by the VAD Coordinator, reduce the speed of the VAD If thrombus is suspected to be causing hemolysis, administer lytics and anticoagulants as able/ ordered
30 Alarms All VAD devices typically have two distinct alarms to indicate a problem and severity Advisory Alarms Critical/ Hazardous Alarms
31 Alarms Advisory Alarms are intermittent beeping sounds that have a corresponding YELLOW light that illuminates on the system controller Not critical but the device requires attention Likely due to low battery, cable disconnected, or device not functioning properly.
32 Alarms Hazardous or Critical alarms are a loud, continuous, shrill sound that have a corresponding RED light that illuminates on the system controller Indicating the device needs immediate attention Often because the pump has stopped or a problem is detected with the system controller Most likely intervention required is to change out the system controller
33 Field Management All VADs are dependent on adequate preload in order to maintain proper functioning Volume resuscitation in an unstable VAD patient is the first line of therapy before vasopressors but be cautious with fluid as to not over load the right ventricle in L VADs only.
34 Field Management Nitrates can be detrimental to a VAD patient because of the reduction in preload Results in decreased pump efficiency Consult with medical control before administering nitrates per protocol
35 Field Management Initiate IV therapy with all VAD patients if possible Use especially careful aseptic technique due to the patient s increased risks of infection
36 Field Management VAD patients are susceptible to other injuries unrelated to the VAD Contact the VAD Coordinator, they are your most valuable resource when encountering these patients Consult with medical control about transport
37
38 Patient Transport This is emergency, resource and protocol driven decision making VAD patients require unique care that not all medical centers are equipped to handle. Transport to the implanting center when able or the closest VAD center Make sure when transporting to bring all VAD related equipment Secure VAD batteries and the controller to prevent dropping or damage Make sure to keep all cables tangle and kink free
39 LVAD Key Facts Let patient and/or caregiver lead. They will be your experts. Remember not to perform chest compressions because they could dislodge the pump, making the patient bleed to death. (Unless the patient is in obvious cardiac arrest and the pump isn t working. Use the assistance of the VAD coordinator to figure this out before starting any compressions). Perform all other BLS/ACLS protocols as written. Defibrillate/cardiovert as normal. Don t place pads over the device under the patient s skin.
40 LVAD Key Facts Remember that these patients typically have an extremely reduced pulse rate or none at all. A Doppler device and manual blood pressure cuff are the most accurate way to obtain blood pressure. The first sound heard is approximately equivalent to the mean arterial pressure, and mmhg is the acceptable range.
41 LVAD Key Facts Keep in mind that it may be difficult to obtain accurate O2 saturation because of little or no pulse. Be careful when removing/cutting off clothes to ensure you don t cut through the driveline, which is the power cord of the pump. Avoid kinking or twisting driveline when strapping the patient onto the stretcher. Keep batteries and controller in reach and secured to the patient during transport. Keep them dry.
42 LVAD Key Facts Take the patient s emergency travel bag when leaving the scene. It has an extra controller, batteries and the VAD coordinator s emergency contact number. Keep in mind that the most common complications are bleeding (nasal, gastrointestinal or intracranial), thromboemboli (pulmonary embolism, myocardial infarction or cerebrovascular accident), rightsided heart failure, pump malfunction and infection.

43 Supraglottic Airways

44 Supraglottic Airways

45 King Airway
46 King Airway

47 King Airway

48 Laryngeal Mask Airway

49 Laryngeal Mask Airway

50 Laryngeal Mask Airway

51 Fast Trach LMA

52 CPAP
53 CPAP and Obstructive Lung Disease
54 CPAP and Recruitment

55 CPAP and Ventilation

56 Oxygenation versus Ventilation Now hold your breath Note what happens to the two waveforms SpO 2 EtCO 2 How long did it take the EtCO 2 waveform to go flat line? How long did it take the SpO 2 to drop below 90%?
57 Numeric reading: HR 100 Waveform:
58 Numeric reading: HR 100 Waveform:
59 End-tidal CO 2 (EtCO 2 ) Pulmonary Blood Flow Ventilation Right Ventricle Artery Oxygen Vein Left Atrium CO2 O 2 O 2 Perfusion
60 End-tidal CO 2 (EtCO 2 ) Reflects changes in Ventilation - movement of air in and out of the lungs Diffusion - exchange of gases between the air-filled alveoli and the pulmonary circulation Perfusion - circulation of blood
61 End-tidal CO 2 (EtCO 2 ) Monitors changes in Ventilation - asthma, COPD, airway edema, foreign body, stroke Diffusion - pulmonary edema, alveolar damage, CO poisoning, smoke inhalation Perfusion - shock, pulmonary embolus, cardiac arrest, severe dysrhythmias
62 Capnographic Waveform Waveforms on screen and printout may differ in duration On-screen capnography waveform is condensed to provide adequate information the in 4- second view Printouts are in real-time Observe RR on device
63 Capnographic Waveform Capnograph detects only CO 2 from ventilation No CO 2 present during inspiration Baseline is normally zero C D A B E Baseline
64 Capnogram Phase I Dead Space Ventilation Beginning of exhalation No CO 2 present Air from trachea, posterior pharynx, mouth and nose No gas exchange occurs there Called dead space
65 Capnogram Phase I Baseline A B I Baseline Beginning of exhalation
66 Capnogram Phase II Ascending Phase CO 2 from the alveoli begins to reach the upper airway and mix with the dead space air Causes a rapid rise in the amount of CO 2 CO 2 now present and detected in exhaled air Alveoli
67 Capnogram Phase II Ascending Phase C Ascending Phase Early Exhalation II A B CO 2 present and increasing in exhaled air
68 Capnogram Phase III Alveolar Plateau CO 2 rich alveolar gas now constitutes the majority of the exhaled air Uniform concentration of CO 2 from alveoli to nose/mouth
69 Capnogram Phase III Alveolar Plateau Alveolar Plateau C III D A B CO 2 exhalation wave plateaus
70 Capnogram Phase III End-Tidal End of exhalation contains the highest concentration of CO 2 The end-tidal CO 2 The number seen on your monitor Normal EtCO 2 is 35-45mmHg
71 Capnogram Phase III End-Tidal C D End-tidal A B End of the the wave of exhalation
72 Capnogram Phase IV Descending Phase Inhalation begins Oxygen fills airway CO 2 level quickly drops to zero Alveoli
73 Capnogram Phase IV Descending Phase C D A B IV Descending Phase Inhalation E Inspiratory downstroke returns to baseline
74 Normal

75 Intubated with lost patency

76 Leak or Obstruction

77 CPR

78 Return of Spontaneous Circulation

79 COPD/Asthma
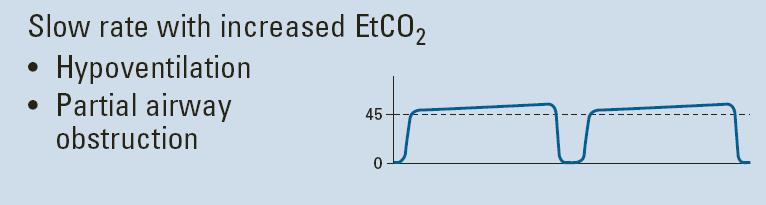
80 Hypoventilation

81 Hyperventilation
82 Resumption of Spontaneous Respiration
83 Rebreathing of Exhaled CO2
84 Esophageal Intubation
85 Incomplete ETT Seal

86 Esophageal Intubation or Apnea

87 Disadvantages Sampling tube obstruction Loose connection Suctioning through ETT
88 Rarely ET tube correct placement but EtCO2 = Zero IF. Equal clear lung sounds No resistance with the esophageal detection device (EDD) No epigastric sounds Direct visualization of the tube passing through the cords THEN = Cardiac Output Problem
89 Summary Where there is metabolism and ventilation there is CO 2 If the ET tube is correctly placed there should be a capnography reading Capnography is more than just ET tube confirmation Ventilation status Prediction of ventilatory failure Real time respiratory rate ph and cardiac output correlation
90 65 y/o cachectic female O2 dependent COPD Active smoker SOB 80% SaO2 on 5L, RR 35
91
92 25 y/o male asthmatic 6 4, 240 lbs Severely dyspneic SaO2 90% on NRB, RR 32
93
94 50 y/o morbidly obese male Lethargic 88 % SaO2 on RA 92% on 4L

95
96 Progressively lethargic, becomes unresponsive.

97

98
99
100 20 y/o male unrestrained driver, ejected BLS in progress by Fire on your arrival Unconscious, unresponsive Unequal pupils
101

102

103
104 50 y/o male COPD Failed CPAP with progressive lethargy and hypoxia Intubated en route to ED VCV, BLEBS, EtCO2 40
105

106

107
108

109

110

111
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
OWN THE AIRWAY. Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP. Paramedic Program
 OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
Capnography (ILS/ALS)
") Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
June 2011 Bill Streett-Training Section Chief
 Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
They aren t the same thing. Daniel Dunham
 They aren t the same thing Daniel Dunham Capnometry Displays the value (as a number) of the partial pressure of CO2 Capnography Waveform capnography shows (as a wave) the change in CO2 over time Both are
They aren t the same thing Daniel Dunham Capnometry Displays the value (as a number) of the partial pressure of CO2 Capnography Waveform capnography shows (as a wave) the change in CO2 over time Both are
EMS System for Metropolitan Oklahoma City and Tulsa 2017 Medical Control Board Treatment Protocols
 S O EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 3H WAVEFORM CAPNOGRAPHY ADULT & PEDIATRIC Indications: 1. Medical General Assessment/General Supportive Care. 2. Trauma General Assessment/Trauma & Hypovolemic
S O EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 3H WAVEFORM CAPNOGRAPHY ADULT & PEDIATRIC Indications: 1. Medical General Assessment/General Supportive Care. 2. Trauma General Assessment/Trauma & Hypovolemic
Left Ventricular Assist Devices LVAD. North Country EMS Program Agency 3/21/12
 Left Ventricular Assist Devices LVAD North Country EMS Program Agency 3/21/12 Objectives Describe indications for and functions of ventricular assist devices (LVAD) Differentiate assessment findings of
Left Ventricular Assist Devices LVAD North Country EMS Program Agency 3/21/12 Objectives Describe indications for and functions of ventricular assist devices (LVAD) Differentiate assessment findings of
How it Works. CO 2 is the smoke from the flames of metabolism 10/21/18. -Ray Fowler, MD. Metabolism creates ETC0 2 for excretion
 CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
FAILURE. Matt Beecroft, MD
 FAILURE Matt Beecroft, MD 64 yo male with no real PMH Sitting on couch when sudden onset SOB Says he s been sweaty FIRST PATIENT OF THE WEEKEND HR 131, RR 28, 132/96, 93% RE-EXAM BP 229/130, HR 180s
FAILURE Matt Beecroft, MD 64 yo male with no real PMH Sitting on couch when sudden onset SOB Says he s been sweaty FIRST PATIENT OF THE WEEKEND HR 131, RR 28, 132/96, 93% RE-EXAM BP 229/130, HR 180s
STATE OF OKLAHOMA 2014 EMERGENCY MEDICAL SERVICES PROTOCOLS
 5M VENTRICULAR ASSIST DEVICE (VAD) MANAGEMENT ADULT EMERGENCY MEDICAL DISPATCHER EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC A Ventricular Assist Device, or VAD, is a mechanical
5M VENTRICULAR ASSIST DEVICE (VAD) MANAGEMENT ADULT EMERGENCY MEDICAL DISPATCHER EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC A Ventricular Assist Device, or VAD, is a mechanical
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist
 Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
3/30/12. Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS
 Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
Don t let your patients turn blue! Isn t it about time you used etco 2?
 Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Interesting Capnography Cases
 Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Interesting Capnography Cases Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com Outline
Airway Management Essentials Self-Study Guide
 Airway Management Essentials Self-Study Guide Fourth Quarter 2010 Self-Study Guide Learning Objectives Cognitive Domain 1. Describe the various conditions that cause concern during treatment in the field
Airway Management Essentials Self-Study Guide Fourth Quarter 2010 Self-Study Guide Learning Objectives Cognitive Domain 1. Describe the various conditions that cause concern during treatment in the field
Capnography: Not just for confirmation
 Capnography: Not just for confirmation Pennsylvania DOH ALS Protocol 2032-ALS Ernest Yeh, M.D. Division of EMS Department of Emergency Medicine Temple University Hospital and School of Medicine Medical
Capnography: Not just for confirmation Pennsylvania DOH ALS Protocol 2032-ALS Ernest Yeh, M.D. Division of EMS Department of Emergency Medicine Temple University Hospital and School of Medicine Medical
Capnography- A Review and Renewed Perspective of its Uses and Limitations
 Capnography- A Review and Renewed Perspective of its Uses and Limitations Prepared and Presented by: Christine Hardie and Dr. Matt Davis December 2014 Learning Objectives Upon completion of this webinar
Capnography- A Review and Renewed Perspective of its Uses and Limitations Prepared and Presented by: Christine Hardie and Dr. Matt Davis December 2014 Learning Objectives Upon completion of this webinar
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
1/21/2016. HeartMate II Indications for Use. Ventricular Assist Device Overview. Jon G. Echterling MSN, CCRN, FNP-BC. Learning Objectives
 Ventricular Assist Device Overview Jon G. Echterling MSN, CCRN, FNP-BC February 5, 2016 Learning Objectives Identify the components and operation of the HeartMate II LVAD Describe the path blood follows
Ventricular Assist Device Overview Jon G. Echterling MSN, CCRN, FNP-BC February 5, 2016 Learning Objectives Identify the components and operation of the HeartMate II LVAD Describe the path blood follows
ETCO2 MONITORING NON-INTUBATED PATIENTS
 Although the standard of care in ETC02 is well established for intubated patients, there has been little emphasis on the use of capnography in nonintubated patients till now. In addition to confirming
Although the standard of care in ETC02 is well established for intubated patients, there has been little emphasis on the use of capnography in nonintubated patients till now. In addition to confirming
Nihon Kohden America. Capnography Monitoring with the CapONE CO2 Sensor For use with the BSM 2300/4100/5100 and the BSM 6000 Series Bedside Monitors
 Nihon Kohden America Capnography Monitoring with the CapONE CO2 Sensor For use with the BSM 2300/4100/5100 and the BSM 6000 Series Bedside Monitors Self Study Training Packet August 2011 Table of Contents
Nihon Kohden America Capnography Monitoring with the CapONE CO2 Sensor For use with the BSM 2300/4100/5100 and the BSM 6000 Series Bedside Monitors Self Study Training Packet August 2011 Table of Contents
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Non-Invasive Assessment of Respiratory Function. Chapter 11
 Non-Invasive Assessment of Respiratory Function Chapter 11 Pulse Oximetry Laboratory measurements of ABG s are the gold standard for measuring levels of hypoxemia, however since these are performed intermittently
Non-Invasive Assessment of Respiratory Function Chapter 11 Pulse Oximetry Laboratory measurements of ABG s are the gold standard for measuring levels of hypoxemia, however since these are performed intermittently
CAPNOGRAPHY. 1.1 To set forth the policy and procedure for performing continuous end-tidal waveform capnography.
 OFFICE OF MEDICAL AFFAIRS DIRECTIVE 2009-02 CAPNOGRAPHY 1. PURPOSE 1.1 To set forth the policy and procedure for performing continuous end-tidal waveform capnography. 2. SCOPE 2.1 This procedure applies
OFFICE OF MEDICAL AFFAIRS DIRECTIVE 2009-02 CAPNOGRAPHY 1. PURPOSE 1.1 To set forth the policy and procedure for performing continuous end-tidal waveform capnography. 2. SCOPE 2.1 This procedure applies
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Continuing Education Packet January-Feb 2018 Ventricular Assist Devices
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Continuing Education Packet January-Feb 2018 Ventricular Assist Devices Simply a ventricular assist device (VAD) is an implantable mechanical
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Continuing Education Packet January-Feb 2018 Ventricular Assist Devices Simply a ventricular assist device (VAD) is an implantable mechanical
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
The Role of Capnography in EMS. By Bob Page, AAS, NREMT-P, CCEMT-P, I/C
 The Role of Capnography in EMS By Bob Page, AAS, NREMT-P, CCEMT-P, I/C Riding the Waves The Role of Capnography in EMS By Bob Page, AAS, NREMT-P, CCEMT-P, I/C Table of Contents Page(s) Introduction and
The Role of Capnography in EMS By Bob Page, AAS, NREMT-P, CCEMT-P, I/C Riding the Waves The Role of Capnography in EMS By Bob Page, AAS, NREMT-P, CCEMT-P, I/C Table of Contents Page(s) Introduction and
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Waitin In The Wings. Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider
 Indications and Use for the Pre-Hospital Provider") Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Waitin In The Wings Esophageal/Tracheal Double Lumen Airway (Combitube ) Indications and Use for the Pre-Hospital Provider 1 CombiTube Kit General Description The CombiTube is A double-lumen tube with
Health Tech Symposium Fall, Dan Sommers P.E. EMT-P
 Health Tech Symposium Fall, 2009 Dan Sommers P.E. EMT-P Human Physiological Signals Simple Explanations for Complicated Systems Ref: Atlas of Human Anatomy, 4 th Edition Simple Schematic RA LA RV LV PCR
Health Tech Symposium Fall, 2009 Dan Sommers P.E. EMT-P Human Physiological Signals Simple Explanations for Complicated Systems Ref: Atlas of Human Anatomy, 4 th Edition Simple Schematic RA LA RV LV PCR
Equipment: NRP algorithm, MRSOPA table, medication chart, SpO 2 table Warm
 NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
NRP Skills Stations Performance Skills Station OR Integrated Skills Station STATION: Assisting with and insertion of endotracheal tube (ETT) Equipment: NRP algorithm, MRSOPA table, medication chart, SpO
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT AVOIDING THE CRASH 1: DON T INTUBATE, OPTIMIZE PRE-AIRWAY MANAGEMENT
 AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
AVOIDING THE CRASH: OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT Robert J. Vissers MD Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Portland,
Facts. STRONG Risk Factors for HF* LVAD, BiVAD, RVAD, HVAD 10/21/ million adults in the US have heart failure.
 10/21/18 1 Facts 5.8 million adults in the US have heart failure. About ½ of those who have HF have a 5 year life expectancy. STRONG Risk Factors for HF* Coronary Heart Disease/MI/Afib COPD Renal Failure
10/21/18 1 Facts 5.8 million adults in the US have heart failure. About ½ of those who have HF have a 5 year life expectancy. STRONG Risk Factors for HF* Coronary Heart Disease/MI/Afib COPD Renal Failure
Airway and Ventilation. Emergency Medical Response
 Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Airway and Ventilation Lesson 14: Airway and Ventilation You Are the Emergency Medical Responder Your medical emergency response team has been called to the fitness center by building security on a report
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
UNIVERSITY OF UTAH HEALTH CARE HOSPITALS AND CLINICS
 UNIVERSITY OF UTAH HEALTH CARE HOSPITALS AND CLINICS CARDIAC MECHANICAL SUPPORT PROGRAM GUIDELINES CARDIAC MECHANICAL SUPPORT: LVAD BASICS FREQUENT SCENARIOS AND TROUBLESHOOTING Review Date: July 2011
UNIVERSITY OF UTAH HEALTH CARE HOSPITALS AND CLINICS CARDIAC MECHANICAL SUPPORT PROGRAM GUIDELINES CARDIAC MECHANICAL SUPPORT: LVAD BASICS FREQUENT SCENARIOS AND TROUBLESHOOTING Review Date: July 2011
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Hemodynamic Monitoring and Circulatory Assist Devices
 Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Hemodynamic Monitoring and Circulatory Assist Devices Speaker: Jana Ogden Learning Unit 2: Hemodynamic Monitoring and Circulatory Assist Devices Hemodynamic monitoring refers to the measurement of pressure,
Northwest Community EMS System Continuing Education Class Credit Questions Respiratory Assessment January 2012
 Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Reminder: You must schedule to take the class post-test with your assigned hospital EMS Coordinator/educator or their designee
Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Reminder: You must schedule to take the class post-test with your assigned hospital EMS Coordinator/educator or their designee
Capnography Could Make You a Rock Star!
 Capnography Could Make You a Rock Star! Mike McEvoy, PhD, RN, CCRN, NRP Staff RN CTICU and Resuscitation Committee Chair Albany Medical Center, New York EMS Coordinator Saratoga County, New York EMS Editor
Capnography Could Make You a Rock Star! Mike McEvoy, PhD, RN, CCRN, NRP Staff RN CTICU and Resuscitation Committee Chair Albany Medical Center, New York EMS Coordinator Saratoga County, New York EMS Editor
Competency Log Professional Responder Courses
 Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Competency Log Professional Responder Courses Check off each competency once successfully demonstrated. This log may be used as a support tool when teaching a Professional Responder course. Refer to the
Guidelines Administrative Practice X Clinical Practice Professional Practice
 Guidelines Administrative Practice X Clinical Practice Professional Practice End Tidal CO 2 (EtCO2) Monitoring Using the Zoll Monitor/Defibrillator Page 1 of 4 Scope: Outcome: Respiratory Therapists (RT),
Guidelines Administrative Practice X Clinical Practice Professional Practice End Tidal CO 2 (EtCO2) Monitoring Using the Zoll Monitor/Defibrillator Page 1 of 4 Scope: Outcome: Respiratory Therapists (RT),
Oxygenation. Chapter 45. Re'eda Almashagba 1
 Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Module 2: Facilitator instructions for Airway & Breathing Skills Station
 Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
FEATURE. 58 EMERGENCY MEDICINE I FEBRUARY
 FEATURE 58 EMERGENCY MEDICINE I FEBRUARY 2016 www.emed-journal.com Troubleshooting the Left Ventricular Assist Device Alicia S. Devine, JD, MD In an update and complement to a previously published article,
FEATURE 58 EMERGENCY MEDICINE I FEBRUARY 2016 www.emed-journal.com Troubleshooting the Left Ventricular Assist Device Alicia S. Devine, JD, MD In an update and complement to a previously published article,
IFT1 Interfacility Transfer of STEMI Patients. IFT2 Interfacility Transfer of Intubated Patients. IFT3 Interfacility Transfer of Stroke Patients
 IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
IFT1 Interfacility Transfer of STEMI Patients IFT2 Interfacility Transfer of Intubated Patients IFT3 Interfacility Transfer of Stroke Patients Interfacility Transfer Guidelines IFT 1 TRANSFER INTERFACILITY
Training. Continuous Positive Airway Pressure (CPAP)
") Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed.
 Chapter 5 Monitoring the Emergency Patient NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1. Monitoring
Chapter 5 Monitoring the Emergency Patient NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1. Monitoring
Chapter 11: Respiratory Emergencies
 29698_CH11_ANS_p001_005 4/12/05 2:02 PM Page 1 Answer Key Chapter 11 1 Chapter 11: Respiratory Emergencies Matching 1. B (page 373) 8. E (page 370) 2. D (page 369) 9. M(page 389) 3. H (page 370) 10. A
29698_CH11_ANS_p001_005 4/12/05 2:02 PM Page 1 Answer Key Chapter 11 1 Chapter 11: Respiratory Emergencies Matching 1. B (page 373) 8. E (page 370) 2. D (page 369) 9. M(page 389) 3. H (page 370) 10. A
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Emergency Care Progress Log
 Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Emergency Care Progress Log For further details on the National Occupational Competencies for EMRs, please visit www.paramedic.ca. Check off each skill once successfully demonstrated the Instructor. All
Cardiac Emergencies. Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington
 Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Cardiac Emergencies Jim Bennett Paramedic and Clinical Education Coordinator American Medical Response Spokane, Washington The Heart -------Aorta Pulmonary Veins---- Superior Vena Cava------ Right Atrium-----
Bronchoconstriction is also treated with medications that inhibit bronchiolar constriction such as: Ipratropium (Atrovent)
") Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
HOSPITAL PROCEDURE Collaborative Practice Committee
 Title: Capnography (ETC0 2 ) Monitoring Code: CPC-2012AUG-1.C.35 HOSPITAL PROCEDURE Collaborative Practice Committee Title of Responsible Party: Director of Medical-Surgical Services Origination Date:
Title: Capnography (ETC0 2 ) Monitoring Code: CPC-2012AUG-1.C.35 HOSPITAL PROCEDURE Collaborative Practice Committee Title of Responsible Party: Director of Medical-Surgical Services Origination Date:
Adult Advanced Cardiovascular Life Support. Emergency Procedures in PT
 Adult Advanced Cardiovascular Life Support Emergency Procedures in PT BLS Can be learned & practiced by the general public Includes: CPR First Aid (e.g. choking relief) Use of AED ACLS Used by healthcare
Adult Advanced Cardiovascular Life Support Emergency Procedures in PT BLS Can be learned & practiced by the general public Includes: CPR First Aid (e.g. choking relief) Use of AED ACLS Used by healthcare
Association for Radiologic & Imaging Nursing
 Overview: Radiology and Imaging Nurses provide procedural sedation to a variety of patients. The administration of procedural sedation in the interventional radiology and diagnostic imaging suites presents
Overview: Radiology and Imaging Nurses provide procedural sedation to a variety of patients. The administration of procedural sedation in the interventional radiology and diagnostic imaging suites presents
Capnography: Creating a Culture of Safety! An Interview With Peggy Lange, RT!
 Capnography: Creating a Culture of Safety An Interview With Peggy Lange, RT Pat Iyer Hi, this is a podcast from the Physician-Patient Alliance for Health & Safety. The podcast that we're presenting today
Capnography: Creating a Culture of Safety An Interview With Peggy Lange, RT Pat Iyer Hi, this is a podcast from the Physician-Patient Alliance for Health & Safety. The podcast that we're presenting today
LESSON ASSIGNMENT. LESSON 2 Heart Attack and Cardiopulmonary Resuscitation. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 2 Heart Attack and Cardiopulmonary Resuscitation. TEXT ASSIGNMENT Paragraphs 2-1 through 2-9. LESSON OBJECTIVES After completing this lesson, you should be able to: 2-1. Define
LESSON ASSIGNMENT LESSON 2 Heart Attack and Cardiopulmonary Resuscitation. TEXT ASSIGNMENT Paragraphs 2-1 through 2-9. LESSON OBJECTIVES After completing this lesson, you should be able to: 2-1. Define
current practices: education series CAPNOGRAPHY IN RESUSCITATION: PEAKS, VALLEYS, AND TRENDS DO THEY SIGNAL THE END?
 current practices: education series CAPNOGRAPHY IN RESUSCITATION: PEAKS, VALLEYS, AND TRENDS DO THEY SIGNAL THE END? Introduction Ninety-six minutes and 12 shocks. Those are the stats from a record-setting
current practices: education series CAPNOGRAPHY IN RESUSCITATION: PEAKS, VALLEYS, AND TRENDS DO THEY SIGNAL THE END? Introduction Ninety-six minutes and 12 shocks. Those are the stats from a record-setting
SEMINOLE COUNTY EMS PROVISIONAL EMT SKILLS VERIFICATION
 The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway.
 PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
PURPOSE This interdisciplinary clinical support document provides guidelines for the safe establishment of an artificial airway. POLICY STATEMENTS Endotracheal intubation will be performed by the Most
CARDIOVASCULAR AND RESPIRATORY SYSTEMS
 CARDIOVASCULAR AND RESPIRATORY SYSTEMS KEY TERMS: Cardiovascular System, cardio, vascular, blood vessels, valves, arteries, capillaries, veins, systemic circulation, pulmonary circulation Your Cardiovascular
CARDIOVASCULAR AND RESPIRATORY SYSTEMS KEY TERMS: Cardiovascular System, cardio, vascular, blood vessels, valves, arteries, capillaries, veins, systemic circulation, pulmonary circulation Your Cardiovascular
Tuesday, December 13, 16. Respiratory System
 Respiratory System Trivia Time... What is the fastest sneeze speed? What is the surface area of the lungs? (hint... think of how large the small intestine was) How many breaths does the average person
Respiratory System Trivia Time... What is the fastest sneeze speed? What is the surface area of the lungs? (hint... think of how large the small intestine was) How many breaths does the average person
PALS Review 2015 Guidelines
 PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
PALS Review 2015 Guidelines BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. 1. Scene Safety 2. Establish Unresponsiveness 3. Check for breathing if absent or agonal (No
AUTOLOGS TM ATLAS ON DEMAND DATA WITH EVERY PATIENT VISIT
 AUTOLOGS TM ATLAS ON DEMAND DATA WITH EVERY PATIENT VISIT Introduction The Autologs Atlas will guide your introduction to our new Autologs service and the information recorded by the HeartWare HVAD TM
AUTOLOGS TM ATLAS ON DEMAND DATA WITH EVERY PATIENT VISIT Introduction The Autologs Atlas will guide your introduction to our new Autologs service and the information recorded by the HeartWare HVAD TM
Disclosures. Learning Objectives. Coeditor/author. Associate Science Editor, American Heart Association
 Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Tracheotomy Challenges for airway specialists Elizabeth H. Sinz, MD Professor of Anesthesiology & Neurosurgery Associate Dean for Clinical Simulation Disclosures Coeditor/author Associate Science Editor,
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies
 : An Intro, Complications, and Emergencies") Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies ERIC T. ROME D.O. HEART FAILURE, MECHANICAL ASSISTANCE AND TRANSPLANTATION CVI Left Ventricular Assist Device An
Modern Left Ventricular Assist Devices (LVAD) : An Intro, Complications, and Emergencies ERIC T. ROME D.O. HEART FAILURE, MECHANICAL ASSISTANCE AND TRANSPLANTATION CVI Left Ventricular Assist Device An
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Interfacility Protocol Protocol Title:
 Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Clearing the air.. How to assist and rescue neck breathing patients. Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA
 Clearing the air.. How to assist and rescue neck breathing patients Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA Learning Objectives Define common terms identified with total (laryngectomy)
Clearing the air.. How to assist and rescue neck breathing patients Presented by: Don Hall MCD, CCC/SLP Sarah Markel RRT, MHA Learning Objectives Define common terms identified with total (laryngectomy)
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. SUBJECT: END TIDAL CARBON DIOXIDE MONITORING (CAPNOGRAPHY)
") Passion for excellence. Compassion for people. P&P REF : NEW 7-2011 ONBASE POLICY ID: 13363 REPLACES: POLICY STATUS : FINAL DOCUMENT TYPE: Policy EFFECTIVE DATE: 4/15/2014 PROPOSED BY: Respiratory Therapy
Passion for excellence. Compassion for people. P&P REF : NEW 7-2011 ONBASE POLICY ID: 13363 REPLACES: POLICY STATUS : FINAL DOCUMENT TYPE: Policy EFFECTIVE DATE: 4/15/2014 PROPOSED BY: Respiratory Therapy
EMS: Care of the VAD Patient. Brittany Butzler BSN RN VAD Coordinator Froedtert and the Medical College of WI
 EMS: Care of the VAD Patient Brittany Butzler BSN RN VAD Coordinator Froedtert and the Medical College of WI Disclosure No relevant financial relationships by planners or presenters Left Ventricular Assist
EMS: Care of the VAD Patient Brittany Butzler BSN RN VAD Coordinator Froedtert and the Medical College of WI Disclosure No relevant financial relationships by planners or presenters Left Ventricular Assist
San Benito County EMS Agency Section 700: Patient Care Procedures
 Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
Purpose: To outline the steps EMTs & paramedics will take to manage possible life threats in any child or adult patient they encounter. This policy is in effect for all treatment protocols & is to be referred
CAE Healthcare Human Patient Simulator (HPS)
") CAE Healthcare Human Patient Simulator (HPS) The Human Patient Simulator, HPS, is a tethered simulator that is capable of patient assessment and treatment including mechanical ventilation and anesthesia.
CAE Healthcare Human Patient Simulator (HPS) The Human Patient Simulator, HPS, is a tethered simulator that is capable of patient assessment and treatment including mechanical ventilation and anesthesia.
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
New and Future Trends in EMS. Ron Brown, MD, FACEP Paramedic Lecture Series 2018
 New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
Pediatric Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
Date: November 15, 2012 Page 1 of 5 Pediatric Cardiac Arrest General This protocol should be followed for all pediatric cardiac arrests. If an arrest is of a known traumatic origin refer to the Dead on
CAPNOGRAPHY DR JOHN ROOS
 CAPNOGRAPHY DR JOHN ROOS Abraham Lincoln If you want me to speak for an hour give me a moment s notice if you want me to speak for five minutes give me a week. Missed oesophageal intubation Many studies
CAPNOGRAPHY DR JOHN ROOS Abraham Lincoln If you want me to speak for an hour give me a moment s notice if you want me to speak for five minutes give me a week. Missed oesophageal intubation Many studies
Airway Anatomy. Soft palate. Hard palate. Nasopharynx. Tongue. Oropharynx. Hypopharynx. Thyroid cartilage
 Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy
Airway Anatomy Hard palate Soft palate Tongue Nasopharynx Oropharynx Hypopharynx Thyroid cartilage Airway Anatomy Hyoid bone Thyroid cartilage Cricoid cartilage Trachea Cricothyroid membrane Airway Anatomy