Applied Physiology of One Lung Ventilation
|
|
|
- Derrick Shepherd
- 5 years ago
- Views:
Transcription
1 Applied Physiology of One Lung Ventilation
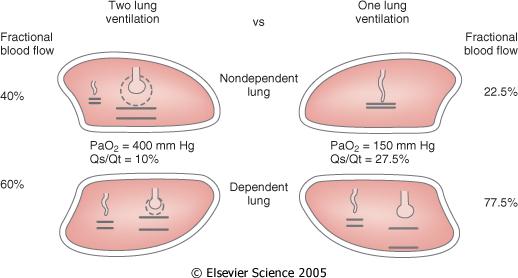
2 One Lung Ventilation Usual situation Thoracic surgery Lateral decubitus position GA, paralysis, PPV Non-dependant lung collapsed and non-ventilated Chest may be open or closed
3 Normal Physiology
4 Lateral Decubitus Spont Vent V/Q maintained Non-dependant lung Q due to gravity V due to position on compliance curve Dependant lung: Q due to gravity V due to Diaphragm advantage Position on compliance curve


5 Lateral Decubitus Ventilated Non-dependant lung further V/Q Q due to gravity V due to position on compliance curve Further V if chest opened Dependant lung further V/Q Q due to gravity V due to Position on compliance curve Loss of diaphragm advantage Greater impact of abdominal contents and mediastinum Sub-optimal positioning
6 OLV Physiology Main problem is obligatory shunt through the nonventilated lung Main compensatory measure is hypoxic pulmonary vasoconstriction
7 OLV Physiology

8 V/Q ratio in OLV Non-dependant lung Zero V Q due to HPV major factor, 50% reduction Gravity Surgical interference Pre-existing disease Dependant lung As previously discussed for later decubitus, GA, PPV
9 Determinants of HPV Decreased by Drugs Volatile anaesthetics, GTN, SNP, NO, some Ca channel antagonists, PDE, α agonists, β agonists Mechanisms: direct vasodilatation, increasing PVR in the ventilated lung, increasing PAP Dopamine extensively studied no significant effect High PAP Poor smooth muscle overcome by pressure Low PAP Creates zone 1 areas in ventilated lung Non-ventilated lung already zone 1 (atelectatic) Some blood diverted non-ventilated lung High PvO2 reverse diffusion of O2 Low PvO2, Low FiO2 induces HPV in ventilated lung Some blood diverted to non-ventilated lung
10 Determinants of HPV Decreased by Hypercapnia causes pulmonary vasoconstriction in ventilated lung Hypocapnia causes pulmonary vasodilatation in non-ventilated lung High AWP Increases PVR in ventilated lung Ventilated lung PEEP Diverts blood to non-ventilated lung by increasing PVR Maximise by Normocapnia, lower AWP, normal PAP Use of FiO2 50% initially
11 Hypoxia under OLV General causes Failure of O2 supply Failure of O2 delivery External: machine, circuit, airway Patient: V/Q mismatch or shunt, including any cause of alveolar hypoventilation or reduced CO diffusion abnormality Increased O2 demands e.g. sympathetic drive, hyperthermia, shivering Causes more common in OLV Malpositioned, blocked or kinked DLT Increased shunt fraction Other Absorption atelectasis of ventilated lung Gradual resorption of residual O2 in non-ventilated lung TRALI preferentially affects ventilated lung
12 Management - General Attempt to rapidly diagnose the problem, while simultaneously providing general management until specific management can be implemented Quickly confirm oximetry probe position and waveform 100% O2 Scan the monitor for any change: BP, ETCO2, AWP, ECG, FiO2 Auscultate chest
13 Management - Specific If DLT problem is suspected, check position with fibreoptic bronchoscope Apply PEEP to the ventilated lung Apply CPAP to the non-ventilated lung Differential PEEP/CPAP Intermittent two-lung ventilation Clamping of the PA to the non-ventilated lung
14 PEEP PaO2 may be increased, decreased or unaffected Diseased lung often responds more favourably Start with no more than 5 cmh2o, to minimise the increase in PVR
15 CPAP External circuit, non-tidal Shunt is reduced O2 uptake is possible from the non-ventilated lung Often results in significant increases in PaO2 Interferes with surgery Must be applied during deflation following a large tidal volume Does not tend to affect technical difficulty
16 Differential PEEP/CPAP Highly efficacious Exact distribution of blood flow becomes less important

17 External CPAP circuit Requirements O2 source Pressure regulating device Manometer


18 Broncho-Cath CPAP system
Thoracic anaesthesia. Simon May
 Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
One-lung anaesthesia
 Jo Eastwood FRCA Ravi Mahajan DM FRCA One-lung anaesthesia (OLA) may be indicated in lung, oesophageal, mediastinal and spinal surgery (Table 1). This review examines preoperative considerations, physiology
Jo Eastwood FRCA Ravi Mahajan DM FRCA One-lung anaesthesia (OLA) may be indicated in lung, oesophageal, mediastinal and spinal surgery (Table 1). This review examines preoperative considerations, physiology
MANAGMENT OF ONE-LUNG VENTILATION
 MANAGMENT OF ONE-LUNG VENTILATION A. NEYRINCK, MD, PhD VERSION MARCH 2013 DOUBLE-LUMEN TUBE (DLT) OR BRONCHIAL BLOCKER (BB) FOR ONE-LUNG VENTILATION (OLV) OLV LUNG ISOLATION LUNG SEPARATION to avoid contamination
MANAGMENT OF ONE-LUNG VENTILATION A. NEYRINCK, MD, PhD VERSION MARCH 2013 DOUBLE-LUMEN TUBE (DLT) OR BRONCHIAL BLOCKER (BB) FOR ONE-LUNG VENTILATION (OLV) OLV LUNG ISOLATION LUNG SEPARATION to avoid contamination
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Anaesthetic considerations for laparoscopic surgery in canines
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
THORACIC ANESTHESIA A. NEYRINCK
 THORACIC ANESTHESIA A. NEYRINCK LUNG ISOLATION DEVICES indications for one-lung ventilation devices for one-lung ventilation bronchial blocker Univent tube fogarty catheter bronchus blocker wire guided
THORACIC ANESTHESIA A. NEYRINCK LUNG ISOLATION DEVICES indications for one-lung ventilation devices for one-lung ventilation bronchial blocker Univent tube fogarty catheter bronchus blocker wire guided
a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure.
 B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
Oxygen Toxicity Walid Habre, MD, PhD
 Oxygen Toxicity Walid Habre, MD, PhD Anaesthesiological Investigations Unit & Paediatric Anaesthesia Unit Geneva University Hospitals and University of Geneva www.walidhabre.org Disclosure I have no conflicts
Oxygen Toxicity Walid Habre, MD, PhD Anaesthesiological Investigations Unit & Paediatric Anaesthesia Unit Geneva University Hospitals and University of Geneva www.walidhabre.org Disclosure I have no conflicts
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
June 2011 Bill Streett-Training Section Chief
 Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
Capnography 102 June 2011 Bill Streett-Training Section Chief Terminology Capnography: the measurement and numerical display of end-tidal CO2 concentration, at the patient s airway, during a respiratory
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Interpretation of Arterial Blood Gases. Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB)
") Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
Lung Injury and Protection in the Perioperative Period
 J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
J. Earl Wynands Lung Injury and Protection in the Perioperative Period Non-injured Lungs: Perioperative Experience (Surgeon) Injured Lungs: Anesthesiologist 78 y.o. Male, Chronic Gallstone Pancreatitis,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Airway pressure release ventilation (APRV) in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital
 in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital") Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Anaesthesia. Fred Roberts*, Ian Kestin *Correspondence
 Update in Anaesthesia Originally published in Update in Anaesthesia, editions 2 (1992) and 12 (2000) Respiratory Physiology Fred Roberts*, Ian Kestin *Correspondence Email: coolfred@btinternet.com Summary
Update in Anaesthesia Originally published in Update in Anaesthesia, editions 2 (1992) and 12 (2000) Respiratory Physiology Fred Roberts*, Ian Kestin *Correspondence Email: coolfred@btinternet.com Summary
For more information about how to cite these materials visit
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Pulmonary circulation. Lung Blood supply : lungs have a unique blood supply system :
 Dr. Ali Naji Pulmonary circulation Lung Blood supply : lungs have a unique blood supply system : 1. Pulmonary circulation 2. Bronchial circulation 1- Pulmonary circulation : receives the whole cardiac
Dr. Ali Naji Pulmonary circulation Lung Blood supply : lungs have a unique blood supply system : 1. Pulmonary circulation 2. Bronchial circulation 1- Pulmonary circulation : receives the whole cardiac
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Anaesthesia and Morbid Obesity
 Anaesthesia and Morbid Obesity Facts 20% adults Obese (1% Morbidly Obese) BMI >35 with comorbidity / BMI >40 without comorbidity = morbidly obese BMI > 55 = super-morbidly obese BMI > 30 rapid increase
Anaesthesia and Morbid Obesity Facts 20% adults Obese (1% Morbidly Obese) BMI >35 with comorbidity / BMI >40 without comorbidity = morbidly obese BMI > 55 = super-morbidly obese BMI > 30 rapid increase
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Perioperative Use of Oxygen: What is the Right Amount?
 Perioperative Use of Oxygen: What is the Right Amount? Walid Habre, MD, PhD Anesthesiological Investigations Unit & Pediatric Anesthesia Unit Geneva University Hospitals and University of Geneva www.walidhabre.org
Perioperative Use of Oxygen: What is the Right Amount? Walid Habre, MD, PhD Anesthesiological Investigations Unit & Pediatric Anesthesia Unit Geneva University Hospitals and University of Geneva www.walidhabre.org
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Northwest Community EMS System Continuing Education Class Credit Questions Respiratory Assessment January 2012
 Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Reminder: You must schedule to take the class post-test with your assigned hospital EMS Coordinator/educator or their designee
Name (PRINT): Date submitted: Affiliation: Rating: [ ] Complete [ ] Incomplete Reminder: You must schedule to take the class post-test with your assigned hospital EMS Coordinator/educator or their designee
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Mechanical Ventilation
 Mechanical Ventilation Effects of Mechanical Ventilation Cardiovascular Effects PPV Q T HR 1. intrathoracic pressure 2. card. tamponade effect 3. loss of +/- press chg in lungs w/spont breathing normal
Mechanical Ventilation Effects of Mechanical Ventilation Cardiovascular Effects PPV Q T HR 1. intrathoracic pressure 2. card. tamponade effect 3. loss of +/- press chg in lungs w/spont breathing normal
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Slide 1. Slide 2. Slide 3 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Objectives: I have nothing to disclose.
 Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Hypoxia during Thoracic Surgery
 Hypoxia during Thoracic Surgery Javier H. Campos, MD Division of Cardiothoracic Anesthesia Department of Anesthesia University of Iowa Carver College of Medicine Iowa City, Iowa Learning Objectives: As
Hypoxia during Thoracic Surgery Javier H. Campos, MD Division of Cardiothoracic Anesthesia Department of Anesthesia University of Iowa Carver College of Medicine Iowa City, Iowa Learning Objectives: As
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Chapter 7 The pulmonary circulation: Bringing blood and gas together
 Chapter 7 The pulmonary circulation: Bringing blood and gas together Department of Pathophysiology, the School of Medicine, Shandong University Zhongrui Yuan, Ph.D. zhongruiyuan@sdu.edu.cn 肺脏有两组血液循环系统,
Chapter 7 The pulmonary circulation: Bringing blood and gas together Department of Pathophysiology, the School of Medicine, Shandong University Zhongrui Yuan, Ph.D. zhongruiyuan@sdu.edu.cn 肺脏有两组血液循环系统,
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia
 End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia Tidal Volume Noninvasive monitoring of ventilation and exhaled carbon dioxide of a patient End Tidal CO2 Produces
End Tidal CO2 Not All Its Cracked Up To Be The Limitations of PETCO2 In Sedation Analgesia Tidal Volume Noninvasive monitoring of ventilation and exhaled carbon dioxide of a patient End Tidal CO2 Produces
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Respiratory Complications of Obesity. Diana Wilson, M.D. ACP Educational Session September 16, 2017
 Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Respiratory Complications of Obesity Diana Wilson, M.D. ACP Educational Session September 16, 2017 1 Prevalence of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2011 Prevalence
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Cardiothoracic Anaesthesia Masterclass
 Cardiothoracic Anaesthesia Masterclass Background Cardiothoracic Anaesthesia is a Mandatory Unit of Training A question on Cardiothoracic Anaesthesia will appear in each SAQ paper The RCOA acknowledges
Cardiothoracic Anaesthesia Masterclass Background Cardiothoracic Anaesthesia is a Mandatory Unit of Training A question on Cardiothoracic Anaesthesia will appear in each SAQ paper The RCOA acknowledges
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
A Comparative Study for the Lung Mechanics during One-Lung Ventilation in Thoracic Surgeries Using Two Different Modes of Mechanical Ventilation
 Med. J. Cairo Univ., Vol. 85, No. 3, June: 967-972, 2017 www.medicaljournalofcairouniversity.net A Comparative Study for the Lung Mechanics during One-Lung Ventilation in Thoracic Surgeries Using Two Different
Med. J. Cairo Univ., Vol. 85, No. 3, June: 967-972, 2017 www.medicaljournalofcairouniversity.net A Comparative Study for the Lung Mechanics during One-Lung Ventilation in Thoracic Surgeries Using Two Different
VENTILATOR GRAPHICS ver.2.0. Charles S. Williams RRT, AE-C
 VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
Essentials of Anaesthetic Monitoring in Veterinary Practice
 Essentials of Anaesthetic Monitoring in Veterinary Practice A refresher and update lecture By Prof Yves Moens, Dipl ECVAA Presented by Dr Alessandra Bergadano, Dipl ECVAA Technical Monitoring human From
Essentials of Anaesthetic Monitoring in Veterinary Practice A refresher and update lecture By Prof Yves Moens, Dipl ECVAA Presented by Dr Alessandra Bergadano, Dipl ECVAA Technical Monitoring human From
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Neonatal/Pediatric Cardiopulmonary Care. Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN. Other. Other Diseases
 PPHN. Other. Other Diseases") Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Tissue Hypoxia and Oxygen Therapy
 Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP
 with BiPAP Device/Nasal CPAP") I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP II. Policy: PSV with BiPAP device/nasal CPAP will be initiated upon a physician's order by Respiratory Therapy personnel trained
I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP II. Policy: PSV with BiPAP device/nasal CPAP will be initiated upon a physician's order by Respiratory Therapy personnel trained
Thoracic Anesthesia Can Be a Pleasure!
 Thoracic Anesthesia Can Be a Pleasure! Tips and Tricks For Maximizing Success Karen Sibert, MD Associate Clinical Professor Department of Anesthesiology & Perioperative Medicine David Geffen School of
Thoracic Anesthesia Can Be a Pleasure! Tips and Tricks For Maximizing Success Karen Sibert, MD Associate Clinical Professor Department of Anesthesiology & Perioperative Medicine David Geffen School of
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up!
 November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up! Bridgett Ronan, MD Department of Pulmonary Medicine Mayo Clinic Arizona Scottsdale, AZ History of Present
November 2012 Critical Care Case of the Month: I Just Can t Do It Captain! I Can t Get the Sats Up! Bridgett Ronan, MD Department of Pulmonary Medicine Mayo Clinic Arizona Scottsdale, AZ History of Present
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
Capnography: Not just for confirmation
 Capnography: Not just for confirmation Pennsylvania DOH ALS Protocol 2032-ALS Ernest Yeh, M.D. Division of EMS Department of Emergency Medicine Temple University Hospital and School of Medicine Medical
Capnography: Not just for confirmation Pennsylvania DOH ALS Protocol 2032-ALS Ernest Yeh, M.D. Division of EMS Department of Emergency Medicine Temple University Hospital and School of Medicine Medical
C l i n i c a lcpap. Advanced Solutions in Acute Respiratory Care
 C l i n i c a lcpap Advanced Solutions in Acute Respiratory Care This is tex which explains in moderate clinicsal detail, the background and structure of the patient indication for CPAP. This is tex which
C l i n i c a lcpap Advanced Solutions in Acute Respiratory Care This is tex which explains in moderate clinicsal detail, the background and structure of the patient indication for CPAP. This is tex which
Respiratory Physiology. Manuel Otero Lopez Department of Anaesthetics and Intensive Care Hôpital Européen Georges Pompidou, Paris, France
 Respiratory Physiology Manuel Otero Lopez Department of Anaesthetics and Intensive Care Hôpital Européen Georges Pompidou, Paris, France Programme Functional respiratory anatomy Ventilation Mechanics of
Respiratory Physiology Manuel Otero Lopez Department of Anaesthetics and Intensive Care Hôpital Européen Georges Pompidou, Paris, France Programme Functional respiratory anatomy Ventilation Mechanics of
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq
 Dr.Ahmad farooq") Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
Postoperative Respiratory failure( PRF) Dr.Ahmad farooq Is it really or/only a postoperative issue Multi hit theory first hits second hits Definition Pulmonary gas exchange impairment that presents after
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center
 FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
FOCUS Fall 2018 CAPNOGRAPHY in the SLEEP CENTER Julie DeWitte, RCP, RPSGT, RST Assistant Department Administrator Kaiser Permanente Fontana Sleep Center 1 Learning Objectives The future of in laboratory
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Home Mechanical Ventilation. Anthony Bateman
 Home Mechanical Ventilation Anthony Bateman What is Long Term Ventilation? LTV is the provision of respiratory support to individuals with non-acute respiratory failure Progression of expected disease
Home Mechanical Ventilation Anthony Bateman What is Long Term Ventilation? LTV is the provision of respiratory support to individuals with non-acute respiratory failure Progression of expected disease
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Course n : (ex: Course 6) Sub-category: (ex: 6.4.) Date: ( ) Language:English/Romanian City:Bucharest Country:Romania Speaker: (Radu T.
 Sub-category: (ex: 6.4.) Date: ( ) Language:English/Romanian City:Bucharest Country:Romania Speaker: (Radu T.") Course n : (ex: Course 6) Sub-category: (ex: 6.4.) Date: (9-12-2015) Language:English/Romanian City:Bucharest Country:Romania Speaker: (Radu T. Stoica) Dificulties in Pediatric Thoracic Anesthesia Dr.
Course n : (ex: Course 6) Sub-category: (ex: 6.4.) Date: (9-12-2015) Language:English/Romanian City:Bucharest Country:Romania Speaker: (Radu T. Stoica) Dificulties in Pediatric Thoracic Anesthesia Dr.
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Oxygenation. Chapter 45. Re'eda Almashagba 1
 Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Post Arrest Ventilation/Oxygenation Management
 Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Respiratory Pathophysiology Cases Linda Costanzo Ph.D.
 Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
It costs you nothing, but gains everything for your patient!
 It costs you nothing, but gains everything for your patient! Attend the entire presentation Complete and submit the evaluation This session is approved for: ANCC hours CECBEMS hours No partial credit will
It costs you nothing, but gains everything for your patient! Attend the entire presentation Complete and submit the evaluation This session is approved for: ANCC hours CECBEMS hours No partial credit will