1. Patient safety 2. Patient comfort. Minimal Sedation (anxiolysis) Moderate Sedation Deep Sedation Anesthesia
|
|
|
- Britney Willis
- 5 years ago
- Views:
Transcription
1 Goals of sedation: 1. Patient safety 2. Patient comfort Conscious Sedation Minimal Sedation (anxiolysis) Moderate Sedation Deep Sedation Anesthesia 1
2 Minimal Sedation (Anxiolysis) Patients respond normally to commands Cognitive function and coordination may be impaired Ventilatory and cardiovascular functions are unaffected Moderate Sedation Depressed consciousness Patients respond purposefully to verbal commands No interventions are required to maintain airway Spontaneous ventilation is adequate Cardiovascular function is usually maintained 2
3 Deep Sedation Depressed consciousness Patients cannot be easily aroused but will respond after repeated or painful stimuli Ventilatory function may be impaired May required airway assistance Spontaneous ventilation may be inadequate Cardiovascular function is usually maintained General anesthesia Patients are not arousable even with painful stimuli Ventilatory function is often impaired Often require airway assistance May require mechanical ventilation Cardiovascular function may be impaired 3
4 The sedation plan must be clearly articulated among all members of the procedure team 4
5 Pre-sedation history Cardiac conditions Pulmonary conditions Renal disease Hepatic disease Endocrine disorders Head trauma Prior surgical or airway issues Prior intubation Stridor Snoring Sleep apnea Previous reactions to sedative medications STOP-BANG S Snore: have you been told you snore T Tired: are you tired during the day O Obstruction: do you stop breathing at night P Pressure: do you have high blood pressure B BMI: is your BMI greater than 28 A Age: 50 or over N Neck: circumference greater than 17 inches G Gender: male Yes to 3 or more = increased risk for sleep apnea 5
6 Other key elements of the history: Current medications Allergies Pregnancy status Last oral intake Need for isolation for infections Alcohol, tobacco, and drug use Physical examination Cardiac exam Pulmonary exam Ability to lay in the proper procedure position Airway assessment 6
7 ASA Physical Status P1 - normal healthy patient P2 mild systemic disease P3 severe systemic disease P4 severe systemic disease that is a constant threat to life P5 moribund and likely to die P6 brain dead organ donor When to consider anesthesia consult? Significant co-morbid disease Significant sleep apnea History of airway problems during sedation History of adverse reaction to sedation High risk airway Chronic opioid or sedative use 7
8 Coding and billing for sedation For the physician doing both the procedure and the sedation: 99152: Initial 15 minutes of sedation services 99153: Each subsequent 15 minutes of sedation services For the physician doing only the sedation: 99156: Initial 15 minutes of sedation services 99157: Each subsequent 15 minutes of sedation services Airway Assessment John S. Rogoski, DO Assistant Professor Clinical Anesthesiology The Ohio State University Wexner Medical Center 8
9 Four Types of Difficulty Difficult to bag/mask ventilate/oxygenate Difficult laryngoscopy Difficult intubation Difficult to perform cricothyroidotomy How Does the ASA Define the Difficult Airway? Difficult mask ventilation - Impossible for an unassisted anesthesiologist to prevent or reverse signs of inadequate ventilation during positive pressure mask ventilation 9
10 How Does the ASA Define the Difficult Airway? Difficult rigid laryngoscopy - It is not possible to visualize any portion of the vocal cords with conventional laryngoscopy Difficult intubation - proper insertion of an endotracheal tube requires more than 3 attempts or greater than 10 minutes Causes of Difficulty Anatomical Obesity Short neck Protruding teeth, long high arched palate Receding mandible Decreased distance between occiput and spinous process Increased alveolar-mental distance 10
11 Causes of Difficulty Acquired Acute neck swelling: trauma, infection, post-operative bleeding Restricted jaw opening: Trismus, fibrosis, rheumatoid arthritis, mandibular fracture Restricted neck movement: osteoarthritis, scarring, C-spine tumor, ankylosing spondylitis Predicting Difficult Bag & Mask Ventilation B - bearded O - obese /obstetric N - no teeth E - elderly S - snores/sleep apnea 11
: 863 871.")
12 Predicting Difficult Intubation Mallampati Classification Class 1: view of the entire posterior oropharynx to the bases of the tonsillar pillars Class 4 : no view of the posterior oropharynx or uvula Korean J Pediatr October; 53(10): Published online 2010 October 31 12
13 Predicting Difficult Intubation Rule 3 finger mouth opening 3 fingers mentum to hyoid distance 2 fingers hyoid to thyroid Predicting Difficult Intubation Review medical record, history Assess teeth especially protruding incisors patent nares open mouth & extend tongue (mallampati) protrude mandible thyromental distance, submental space neck - short, thick?, overall mobility & sniffing position body habitus 13

14 Video of Airway Examination Airway Management 14


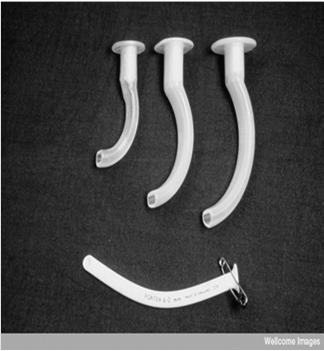
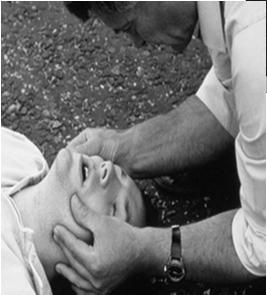
15 Supplemental Oxygen Nasal cannula Simple mask Non-rebreather mask Creative Commons Attribution-ShareAlike 3.0 Unported Airway Support Jaw thrust Nasal airways Oral airways 15





16 Bag / Mask Ventilation Technique dependent Mask seal essential 2 are better than 1 Incorporate jaw thrust Nasal / Oral airways Assist spontaneous ventilation Creative Commons Attribution-ShareAlike 3.0 Unported Video of Airway Maneuvers 16
17 Before the procedure There must be signed written consent for: The procedure The sedation If 2 procedures are planned, get consent for both before giving sedation A time-out must be performed Q 5 minutes during the procedure: Level of consciousness Blood pressure Oxygen saturation Respiratory rate Cardiac rhythm (only required in patients with known heart disease) 17
18 Monitoring every 15 minutes until: Patient is awake, alert, and oriented Recovered protective reflexes Vital signs returned to normal Oxygen saturation > 95% or at baseline Post-procedure transport: Accompanying personnel trained in sedation monitoring Pulse oximeter Supplemental oxygen Ventilation equipment Nasal and/or oral airways Emergency drug supplies Cardiac monitor (in patients with heart disease) 18
19 Post-procedure discharge: Instruction sheet No driving No alcohol or sedatives No operating machinery Phone number for questions A responsible adult to accompany (taxis do not count!) Pharmacology of Sedatives and Reversal Agents Mary Beth Shirk, PharmD, RPh Clinical Associate Professor The Ohio State University College of Pharmacy Specialty Practice Pharmacist, Emergency Medicine The Ohio State University Wexner Medical Center 19
20 Agents for Procedural Sedation Opioids Benzodiazepines Etomidate Ketamine Methohexital Propofol Dexmedetomidine Opioids Class II Controlled Substances Mu receptor agonists Fentanyl Hydromorphone Morphine Meperidine Hepatic metabolism with varying t ½ 20
21 Opioids Adverse Effects Respiratory depression Hypotension Miosis Decreased GI motility Urinary retention Opioids Estimated IV Potency Fentanyl micrograms Hydromorphone 1.5 mg Meperidine 75 mg Morphine 10 mg 21
22 Fentanyl Phenylpiperidine opioid agonist Preferred opioid for procedural sedation Precautions Skeletal muscle and chest wall rigidity Dose and administration rate related Reversible with naloxone Bradycardia Black box warning with CYP3A4 inhibitors Benzodiazepines Class IV Controlled Substances GABA and Benzodiazepine agonists Midazolam Lorazepam Diazepam Hepatic metabolism with varying t ½ 22
23 Benzodiazepines Adverse Effects Respiratory depression Hypotension Paradoxical reactions Nausea/vomiting Hiccoughs Benzodiazepines Estimated Potency Diazepam 5 mg Lorazepam 1 mg Midazolam 2 mg 23
24 Midazolam Preferred BZD for procedural sedation CYP3A4 substrate Elimination t ½ prolonged CHF Renal function impairment Hepatic function impairment Obesity Elderly Etomidate Not currently controlled substance Nonbarbiturate benzylimidazole hypnotic mg / kg IVP over seconds 24
25 Etomidate Inhibits 11-β hydroxylase Blocks cortisol production Myoclonus (up to 33%) Injection site pain (30-80%) Propylene glycol Minimal effect on hemodynamics Decreases ICP and seizure threshold Ketamine Class III Controlled Substance NMDA receptor antagonist and PCP derivative Analgesic properties appealing IM or IV administration mg/kg IVP over at least 60 seconds 25
26 Ketamine Respiratory drive maintained Three concentrations available 10 mg/ml 50 mg/ml 100 mg/ml (dilute if administered IV) Ketamine Emergence reaction (12-50%) Severity varies Less common in < 15 yrs and > 65 yrs Less frequent with IM administration Minimize verbal, tactile, visual stimulation during recover?pretreat with BZD or butyrophenone 26
27 Ketamine Emergence reaction (12-50%) Hypersalivation? pretreat? Nystagmus Increases ICP/IOP Minimal affect on BP/HR or increase Increased skeletal muscle tone Methohexital Class IV controlled substance Ultrashort acting IV barbiturate anesthetic ph of 1% solution is Contraindicated in porphyria Hypotension Respiratory depression Dose mg/kg at <10mg/5 seconds 500 mg vials! 27
28 Propofol Currently not controlled substance Patient can transition in unpredictable fashion to deeper level of sedation At OSUWMC physician must be credentialed for deep sedation Cardiovascular depressant hypotension! Propofol Contraindicated if egg allergy (?) soy intolerance (?) peanut allergy (?) mg/kg IV over 2-3 min once then 0.5 mg/kg every 3-5 min if needed 28
29 Dexmedetomidine relatively selective alpha 2 adrenergic agonist FDA approval in 2008 Sedation of nonintubated patients prior to and/or during surgical and other procedures Limited published experience for procedural sedation (ablation, hysteroscopy, etc) Dexmedetomidine Hypotension 54% vs 30% (Placebo) SBP<80 or DBP <50 or >30% from baseline 72% in 65yo patients (n=131) Bradycardia/sinus arrest 14% vs 4% (Placebo) <40BPM or >30% from baseline 29
30 Approaches Being Explored Alternative routes of administration Intranasal Nebulized Alternative combinations of medications Ketamine + Propofol Ketamine + Dexmedetomidine Onset Peak Duration Elimination (Min) (Min (Min) Fentanyl Immed Immed Hepatic Midazolam Hepatic + (Renal) Etomidate < Hepatic Ketamine Hepatic Active Metabolite Methohexital Immed Immed Hepatic Propofol ½ Hepatic Dexmedetomidine 4 hours Hepatic 30
31 Amnestic Analgesic Anxiolytic Benzodiazepines Opioids - + -/+ Etomidate Ketamine + + Dissociative properties Methohexital Propofol +/- - + Dexmedetomidine Recommended Agents at OSUWMC Midazolam ± fentanyl agents of choice Propofol limited to physicians credentialed in deep sedation Meperidine not for routine use Alternative agents used by physician experienced in their use 31
32 Dose No universally safe & effective dose Variable dose requirements Age (especially >65 yrs) Weight Medical condition Medication history Previous requirements during procedures Goal depth of sedation Dose Combination agents have added risks/benefits TITRATE Small incremental doses Sufficient time must elapse between doses to evaluate effect of previous dose Time between doses longer for nonintravenous routes 32
33 Fentanyl: Typical Initial Regimen* micrograms SLOW IVP IVP over at 1-2 minutes Dilute to permit slower administration Additional doses in 2 minutes if needed Administer prior to midazolam if using combination regimen *Dose is highly variable Midazolam: Typical Initial Regimen* mg IVP IVP over at least 2 minutes Dilute to permit slower administration Additional dose(s) in 3 minutes if needed Administer after opioid if using combination regimen *Dose is highly variable 33
34 JCAHO & Medication Administration During Procedures Sterile technique! Proper product labeling Label: drug name, strength, and amount Single individual process and immediate administration = no label Two individual process = product verification with vial and label JCAHO & Medication Administration During Procedures Document waste of Controlled Substances Complete charting Medication Dose Route Time of administration Who administers 34
35 Reversal Agents Used to reverse sedatives or treat overdose Half lives can be shorter than sedative Can precipitate withdrawal symptoms May not completely reverse all complications of sedatives Flumazenil Onset of action 1-2 minutes Half life minutes Flumazenil use requires 90 min monitored recovery time Hepatic clearance 35
36 Flumazenil Adverse Effects Seizures Panic attacks and emotional lability Withdrawal symptoms Dizziness Reversal of Procedural Sedation 0.2mg IVP q 1 min prn to MAX of 1mg Repeat every 20 min as needed Naloxone Opiate receptor antagonist Onset of action 2-3 minutes Half life minutes Naloxone use requires 90 min monitored recovery time Duration of effect varies (45min 4 hrs) Hepatic clearance 36
37 Naloxone Dosing mg IVP every 1-2 minutes Doses up to 2 mg may be required May need to redose if naloxone wears off before opiate Adverse Effects Opiate withdrawal Pulmonary edema Acute hypertension and dysrhythmias Seizures Moderate and Deep Sedation 37
38 Deep sedation Emergency medicine Pulmonary medicine Critical care Oral maxillary facial surgery Or demonstrated advanced airway expertise and intubation skill Case #1: 50 year-old man undergoing screening colonoscopy 38
39 Case #2: 60 year-old woman with COPD exacerbation and respiratory failure requiring intubation Case #3: 50 year-old man with HIV on anti-retroviral medications needs a colonoscopy 39
40 Case #4: 23 year-old undergoing dental procedure requires oxygen then develops bradycardia Case #5: 21 year-old man with pneumothorax needs a chest tube 40
41 Case #6: patient with atrial fibrillation needs external cardioversion Case #7: after TEE, patient develops cyanosis, headache, and SaO2 = 85%. Blood looks brown 41
Conscious Sedation. Educational goals of this webcast. Moderate and Deep Sedation. Goals of any sedation: Patient safety Patient comfort
 Educational goals of this webcast Moderate and Deep Sedation The Ohio State University Medical Center Sedation Taskforce Pre-procedure assessment Airway assessment Consent Monitoring Post-procedure management
Educational goals of this webcast Moderate and Deep Sedation The Ohio State University Medical Center Sedation Taskforce Pre-procedure assessment Airway assessment Consent Monitoring Post-procedure management
PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older)
") Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Name Score PHYSICIAN COMPETENCY FOR ADULT DEEP SEDATION (Ages 14 and older) 1. Pre-procedure evaluation for moderate sedation should involve all of the following EXCEPT: a) Airway Exam b) Anesthetic history
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ
 PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ 1. Which of the following statements are TRUE? (Select ALL that apply) o Sedative/analgesic drugs should be given in small, incremental doses that are titrated
PHYSICIAN PROCEDURAL SEDATION AND ANALGESIA QUIZ 1. Which of the following statements are TRUE? (Select ALL that apply) o Sedative/analgesic drugs should be given in small, incremental doses that are titrated
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY. Procedural Sedation Questions
 Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; 10/09; 10/10 Manual of Administrative Policy Source Sedation Committee
 Code No. 711 Section Subject Moderate Sedation (formerly termed Conscious Sedation ) Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; Manual of Administrative Policy Source
Code No. 711 Section Subject Moderate Sedation (formerly termed Conscious Sedation ) Date 8/95; Rev.12/97; 7/98; 2/99; 5/01, 3/03, 9/03; 5/04; 8/05; 3/07; 10/08; Manual of Administrative Policy Source
DEEP SEDATION TEST QUESTIONS
 Mailing Address: Phone: Fax: The Study Guide is provided for those physicians eligible to apply for Deep Sedation privileges. The Study Guide is approximately 41 pages, so you may consider printing only
Mailing Address: Phone: Fax: The Study Guide is provided for those physicians eligible to apply for Deep Sedation privileges. The Study Guide is approximately 41 pages, so you may consider printing only
I. Subject. Moderate Sedation
 I. Subject II. III. Moderate Sedation Purpose To establish criteria for the monitoring and management of patients receiving moderate throughout the hospital Definitions A. Definitions of three levels of
I. Subject II. III. Moderate Sedation Purpose To establish criteria for the monitoring and management of patients receiving moderate throughout the hospital Definitions A. Definitions of three levels of
Procedural Sedation and Analgesia in the ED
 Overview Procedural Sedation and Analgesia in the ED Susan Lambe, MD Assistant Clinical Professor UCSF Division of Emergency Medicine Terminology Goals Indications Presedation Assessment Consent Issues
Overview Procedural Sedation and Analgesia in the ED Susan Lambe, MD Assistant Clinical Professor UCSF Division of Emergency Medicine Terminology Goals Indications Presedation Assessment Consent Issues
Pain & Sedation Management in PICU. Marut Chantra, M.D.
 Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Pain & Sedation Management in PICU Marut Chantra, M.D. Pain Diseases Trauma Procedures Rogers Textbook of Pediatric Intensive Care, 5 th ed, 2015 Emotional Distress Separation from parents Unfamiliar
Chapter 004 Procedural Sedation and Analgesia
 Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Chapter 004 Procedural Sedation and Analgesia NOTE: CONTENT CONTAINED IN THIS DOCUMENT IS TAKEN FROM ROSEN S EMERGENCY MEDICINE 9th Ed. Italicized text is quoted directly from Rosen s. Key Concepts: 1.
Sedation is a dynamic process.
 19th Annual Mud Season Nursing Symposium Timothy R. Lyons, M.D. 26 March 2011 To allow patients to tolerate unpleasant procedures by relieving anxiety, discomfort or pain To expedite the conduct of a procedure
19th Annual Mud Season Nursing Symposium Timothy R. Lyons, M.D. 26 March 2011 To allow patients to tolerate unpleasant procedures by relieving anxiety, discomfort or pain To expedite the conduct of a procedure
Moderate and Deep Sedation Pathway
 A Quick Reference to the Advocate System Sedation Policy *This information is meant as a guideline only and not a substitute for physician order or clinical judgment Introduction: This Pediatric Emergency
A Quick Reference to the Advocate System Sedation Policy *This information is meant as a guideline only and not a substitute for physician order or clinical judgment Introduction: This Pediatric Emergency
Conscious Sedation. Edited by D. John Doyle MD PhD FRCPC
 Conscious Sedation Edited by D. John Doyle MD PhD FRCPC In memory of: J. Michael de Ungria, MD 1969-2009 Anesthesia Institute The Cleveland Clinic Goals and Objectives: 1. Define Conscious Sedation. 2.
Conscious Sedation Edited by D. John Doyle MD PhD FRCPC In memory of: J. Michael de Ungria, MD 1969-2009 Anesthesia Institute The Cleveland Clinic Goals and Objectives: 1. Define Conscious Sedation. 2.
ADMINISTRATIVE POLICY AND PROCEDURE MANUAL. Subject: Moderate Sedation/Analgesia- Procedural ( Conscious Sedation ) Policy
 Policy") BRYN MAWR HOSPITAL LANKENAU HOSPITAL PAOLI HOSPITAL Working Together to Serve the Community ADMINISTRATE POLICY AND PROCEDURE MANUAL Subject: Moderate Sedation/Analgesia- Procedural ( Conscious Sedation
BRYN MAWR HOSPITAL LANKENAU HOSPITAL PAOLI HOSPITAL Working Together to Serve the Community ADMINISTRATE POLICY AND PROCEDURE MANUAL Subject: Moderate Sedation/Analgesia- Procedural ( Conscious Sedation
Attestation for Completion of Procedural Sedation Course for Level I Moderate Procedural Sedation Privileges
 Attestation for Completion of Procedural Sedation Course for Level I Moderate Procedural Sedation Privileges I certify that I have completed the following: I have read the PHSW Procedural Sedation Policy
Attestation for Completion of Procedural Sedation Course for Level I Moderate Procedural Sedation Privileges I certify that I have completed the following: I have read the PHSW Procedural Sedation Policy
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Adult Procedural Sedation A Training Program for Providers
 Adult Procedural Sedation A Training Program for Providers Adult Procedural Sedation by the Non-Anesthesiologist Guidelines for adult procedural sedation promote safe and effective medical practice: Many
Adult Procedural Sedation A Training Program for Providers Adult Procedural Sedation by the Non-Anesthesiologist Guidelines for adult procedural sedation promote safe and effective medical practice: Many
Sedation-Analgesia Patient Evaluation
 Getting Started A health care provider with current privileges to administer sedation-analgesia must conduct a pre-procedure evaluation, and obtain informed consent for sedation-analgesia Only patients
Getting Started A health care provider with current privileges to administer sedation-analgesia must conduct a pre-procedure evaluation, and obtain informed consent for sedation-analgesia Only patients
Medical Coverage Policy Monitored Anesthesia care (MAC) EFFECTIVE DATE: POLICY LAST UPDATED:
 EFFECTIVE DATE: POLICY LAST UPDATED:") Medical Coverage Policy Monitored Anesthesia care (MAC) EFFECTIVE DATE: 09 01 2004 POLICY LAST UPDATED: 01 08 2013 OVERVIEW Monitored anesthesia care is a specific anesthesia service for a diagnostic or
Medical Coverage Policy Monitored Anesthesia care (MAC) EFFECTIVE DATE: 09 01 2004 POLICY LAST UPDATED: 01 08 2013 OVERVIEW Monitored anesthesia care is a specific anesthesia service for a diagnostic or
CalvertHealth Medical Center s Moderate Sedation Competency Examination
 Medical Staff Office Use Only: Congratulations! You passed the Moderate Sedation Competency Examination. Enclosed is the test for your follow-up review. Test Results: % ( of 35 correct) Your test result
Medical Staff Office Use Only: Congratulations! You passed the Moderate Sedation Competency Examination. Enclosed is the test for your follow-up review. Test Results: % ( of 35 correct) Your test result
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
POST TEST: PROCEDURAL SEDATION
 POST TEST: PROCEDURAL SEDATION Name: Date: Instructions: Complete the Post-Test (an 85% is required to pass). If there are areas that you are unsure of, please review the relevant portions of the learning
POST TEST: PROCEDURAL SEDATION Name: Date: Instructions: Complete the Post-Test (an 85% is required to pass). If there are areas that you are unsure of, please review the relevant portions of the learning
Adult Procedural Moderate and Deep Sedation: A Training Program for Emergency Medicine Physicians
 Adult Procedural Moderate and Deep Sedation: A Training Program for Emergency Medicine Physicians Adult Procedural Sedation by the Non-Anesthesiologist Guidelines for adult procedural sedation promote
Adult Procedural Moderate and Deep Sedation: A Training Program for Emergency Medicine Physicians Adult Procedural Sedation by the Non-Anesthesiologist Guidelines for adult procedural sedation promote
Pediatric Sedation Pocket Reference
 Pediatric Sedation Pocket Reference No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopy, recording,
Pediatric Sedation Pocket Reference No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopy, recording,
Title/Description: Department: Personnel: Effective Date: Revised: PURPOSE DEFINITIONS
 Title/Description: Moderate Sedation and Anesthesia Care Department: Organization-wide Personnel: All Individuals Involved in Anesthesia Care Effective Date: 9/90 Revised: 3/94, 12/96, 4/00, 11/02, 02/03,
Title/Description: Moderate Sedation and Anesthesia Care Department: Organization-wide Personnel: All Individuals Involved in Anesthesia Care Effective Date: 9/90 Revised: 3/94, 12/96, 4/00, 11/02, 02/03,
Pediatric Dental Sedation
 Pediatric Dental Sedation L. Stephen Long, MD Pediatric Anesthesiologist Children s Dental Anesthesia Group UCSF Benioff Children s Hospital Oakland Part 1: Pediatric Airways and Lungs 1 Three questions:
Pediatric Dental Sedation L. Stephen Long, MD Pediatric Anesthesiologist Children s Dental Anesthesia Group UCSF Benioff Children s Hospital Oakland Part 1: Pediatric Airways and Lungs 1 Three questions:
Emergency Department Guideline. Procedural Sedation and Analgesia Policy for the Registered Nurse
 Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Emergency Department Guideline Purpose: To ensure safe, consistent patient monitoring and documentation standards when procedure related sedation and analgesia is indicated. Definitions: Minimal Sedation
Procedural Sedation in the Rural ER
 Procedural Sedation in the Rural ER Hal Irvine MD FCFP Rural FP Anesthetist Sundre, Alberta June 17, 2011 Disclosure I do not have any affiliations (financial or otherwise) with a commercial organization
Procedural Sedation in the Rural ER Hal Irvine MD FCFP Rural FP Anesthetist Sundre, Alberta June 17, 2011 Disclosure I do not have any affiliations (financial or otherwise) with a commercial organization
To the Medical Staff/Allied Health Professional of Nationwide Children s Hospital:
 To the Medical Staff/Allied Health Professional of Nationwide Children s Hospital: As many of you know, our medical practices in various areas are coming under closer scrutiny of credentialing organizations
To the Medical Staff/Allied Health Professional of Nationwide Children s Hospital: As many of you know, our medical practices in various areas are coming under closer scrutiny of credentialing organizations
Avoiding Procedural Sedation Errors
 Avoiding Procedural Sedation Errors Sanjay Arora MD Associate Professor of Clinical Emergency Medicine Keck School of Medicine USC+Los Angeles County Hospital Pitfall #1 Forgetting the Goals of PS&A 1
Avoiding Procedural Sedation Errors Sanjay Arora MD Associate Professor of Clinical Emergency Medicine Keck School of Medicine USC+Los Angeles County Hospital Pitfall #1 Forgetting the Goals of PS&A 1
Airway Management. Teeradej Kuptanon, MD
 Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Airway Management Teeradej Kuptanon, MD Outline Anatomy Detect difficult airway Rapid sequence intubation Difficult ventilation Difficult intubation Surgical airway access ICU setting Intubation Difficult
Pain Module. Opioid-RelatedRespiratory Depression (ORRD)
") Pain Module Opioid-RelatedRespiratory Depression (ORRD) Characteristics of patients who are at higher risk for Opioid- Related Respiratory Depression (ORRD) Sleep apnea or sleep disorder diagnosis : typically
Pain Module Opioid-RelatedRespiratory Depression (ORRD) Characteristics of patients who are at higher risk for Opioid- Related Respiratory Depression (ORRD) Sleep apnea or sleep disorder diagnosis : typically
Pain: 1-2µg/kg q30-60min prn. effects in 10 minutes. Contraindications: Morphine is preferred in. Duration of Action: minutes. renal failure.
 Procedural Sedation / Analgesia / Anaesthesia Chart - Page 1 Diazepam (Valium) Anxiolytic / Sedative Etomidate (Amidate) Hypnotic / Anesthetic Fentanyl Citrate (Sublimaze) Narcotic Analgesic Dose Pediatric:
Procedural Sedation / Analgesia / Anaesthesia Chart - Page 1 Diazepam (Valium) Anxiolytic / Sedative Etomidate (Amidate) Hypnotic / Anesthetic Fentanyl Citrate (Sublimaze) Narcotic Analgesic Dose Pediatric:
Pediatric Procedural Sedation
 Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pharmacological methods of behaviour management
 Pharmacological methods of behaviour management Pharmacological methods CONCIOUS SEDATION?? Sedation is the use of a mild sedative (calming drug) to manage special needs or anxiety while a child receives
Pharmacological methods of behaviour management Pharmacological methods CONCIOUS SEDATION?? Sedation is the use of a mild sedative (calming drug) to manage special needs or anxiety while a child receives
Administrative Policies and Procedures. Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916
 Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Administrative Policies and Procedures Originating Venue: Provision of Care, Treatment and Services Policy No.: PC 2916 Title: Sedation Cross Reference: Date Issued: 05/09 Date Reviewed: 04/11 Date: Revised:
Case scenarios. We want to do head CT in an middle-aged woman with agitation and confusion. She does not stay still in the CT table.
 Procedural sedation Khrongwong Musikatavorn, M.D. Emergency Medicine Unit, King Chulalongkorn Memorial Hospital and Faculty of Medicine, Chulalongkorn University Case scenarios We need to rule out acute
Procedural sedation Khrongwong Musikatavorn, M.D. Emergency Medicine Unit, King Chulalongkorn Memorial Hospital and Faculty of Medicine, Chulalongkorn University Case scenarios We need to rule out acute
1. Pre-procedure preparation:
 Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists 1 1. Pre-procedure preparation: There is insufficient published evidence to evaluate the relationship between sedation / analgesia
Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists 1 1. Pre-procedure preparation: There is insufficient published evidence to evaluate the relationship between sedation / analgesia
PROCEDURAL SEDATION AND ANALGESIA
 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 260 PROCEDURAL SEDATION AND ANALGESIA
Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Braam de Klerk VICTORIA BC 260 PROCEDURAL SEDATION AND ANALGESIA
Rapid Sequence Induction
 Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Rapid Sequence Induction Virtual simultaneous administration, after preoxygenation, of a potent sedative agent and a rapidly acting neuromuscular blocking agent to facilitate rapid tracheal intubation
Sedative-Hypnotics. Sedative Agents (General Considerations)
") Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Sedation For Cardiac Procedures A Review of
 Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Note: Press F11 to maximize. Physician Education Procedural Sedation for ESJH
 Note: Press F11 to maximize. Physician Education Procedural Sedation for ESJH 1 Definitions along the Sedation Continuum Responsiveness Airway Spontaneous Ventilation Cardiovascular Function Minimal Sedation
Note: Press F11 to maximize. Physician Education Procedural Sedation for ESJH 1 Definitions along the Sedation Continuum Responsiveness Airway Spontaneous Ventilation Cardiovascular Function Minimal Sedation
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA
 AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
AIRWAY MANAGEMENT SUZANNE BROWN, CRNA OBJECTIVE OF LECTURE Non Anesthesia Sedation Providers Review for CRNA s Informal Questions encouraged 2 AIRWAY MANAGEMENT AWARENESS BASICS OF ANATOMY EQUIPMENT 3
Procedural Sedation. Conscious Sedation AAP Sedation Guidelines: Disclosures. What does it mean for my practice? We have no disclosures
 2016 AAP Sedation Guidelines: What does it mean for my practice? Amber P. Rogers MD FAAP Assistant Professor of Section of Hospital Medicine and Anesthesiology Corrie E. Chumpitazi MD FAAP FACEP Assistant
2016 AAP Sedation Guidelines: What does it mean for my practice? Amber P. Rogers MD FAAP Assistant Professor of Section of Hospital Medicine and Anesthesiology Corrie E. Chumpitazi MD FAAP FACEP Assistant
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Bayshore Community Hospital. Riverview Medical Center. Divisions of Meridian Hospitals Corporation
 Bayshore Community Hospital Riverview Medical Center Divisions of Meridian Hospitals Corporation Regional Hospital Policy for Moderate Sedation for Non-Anesthesiologists I. Policy: This policy will explain
Bayshore Community Hospital Riverview Medical Center Divisions of Meridian Hospitals Corporation Regional Hospital Policy for Moderate Sedation for Non-Anesthesiologists I. Policy: This policy will explain
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Analgo sedation in Pediatric Emergency Medicine. Juliusz Jakubaszko
 Analgo sedation in Pediatric Emergency Medicine Juliusz Jakubaszko COI Disclosure I have no relevant relationship or financial/ material support to disclose. PRESENTER: JULIUSZ JAKUBASZKO Wroclaw University
Analgo sedation in Pediatric Emergency Medicine Juliusz Jakubaszko COI Disclosure I have no relevant relationship or financial/ material support to disclose. PRESENTER: JULIUSZ JAKUBASZKO Wroclaw University
Moderate Sedation- What Is It? Objectives
 Objectives Upon completion of this presentation, the learner will: Recognize indications and contraindication for moderate sedation. State appropriate monitoring techniques and safety requirements for
Objectives Upon completion of this presentation, the learner will: Recognize indications and contraindication for moderate sedation. State appropriate monitoring techniques and safety requirements for
Question: Is this patient an infant? A patient less than 12 months old is considered an infant. Please check the box next to the appropriate choice.
 Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Question: Date of Intubation (Month, Day, Year): Question: Date of Data Entry This should be within 4 weeks to the day of intubation: Question: Is this patient an infant? A patient less than 12 months
Airway Management. Key points. Rapid Sequence Intubation. Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway
 Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Airway Management Prasha Ramanujam and Guy Shochat Department of Emergency Medicine UCSF Medical Center Key points Rapid Sequence Intubation Recognizing difficult airway Managing difficult airway Rapid
Diagnosis & Management of the Difficult Airway
 Diagnosis & Management of the Difficult Airway Dr. E. Rawlings Plymouth Anaesthetic Department Complications of Airway Management Medicolegal Serious morbidity Mortality Complications of Airway Management
Diagnosis & Management of the Difficult Airway Dr. E. Rawlings Plymouth Anaesthetic Department Complications of Airway Management Medicolegal Serious morbidity Mortality Complications of Airway Management
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Date Dear UCSD Health Care Provider:
 Date Dear UCSD Health Care Provider: The use of moderate sedation has increased considerably over recent years. As a result, medical centers are under obligation by regulatory requirements, JCAHO, and
Date Dear UCSD Health Care Provider: The use of moderate sedation has increased considerably over recent years. As a result, medical centers are under obligation by regulatory requirements, JCAHO, and
CENTRAL IOWA HEALTHCARE Marshalltown, Iowa
 CENTRAL IOWA HEALTHCARE Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.44 Subject: Purpose: Policy: Procedural Sedation (Adult/Pediatric) To establish appropriate standards for
CENTRAL IOWA HEALTHCARE Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.44 Subject: Purpose: Policy: Procedural Sedation (Adult/Pediatric) To establish appropriate standards for
SEDATION FOR PROCEDURES- MODERATE AND DEEP CLINICAL POLICY/PROCEDURES MANUAL AND MEDICAL STAFF. Approval
 TITLE: MANUAL: SEDATION FOR PROCEDURES- MODERATE AND DEEP CLINICAL POLICY/PROCEDURES MANUAL AND MEDICAL STAFF Effective Date: 3/90 Revised: 2/93, 1/96, 5/96, 4/98, 11/98, 10/00, 1/01, 6/03, 12/04, 5/11,
TITLE: MANUAL: SEDATION FOR PROCEDURES- MODERATE AND DEEP CLINICAL POLICY/PROCEDURES MANUAL AND MEDICAL STAFF Effective Date: 3/90 Revised: 2/93, 1/96, 5/96, 4/98, 11/98, 10/00, 1/01, 6/03, 12/04, 5/11,
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Airway Workshop Lecture. University of Ottawa
 Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Airway Workshop Lecture Department of Anesthesiology University of Ottawa Overview Ventilation Airway assessment Difficult airways Airway management equipment aids Intubation/Improving Intubation Success
Case. You plan to perform an EGD for further evaluation. Footer text is edited under "view/header and footer" menu August 11, 2018 Page 2
 Procedural Sedation Daniela Jodorkovsky M.D. Gastroenterology Fellowship Director Assistant Professor Medicine Columbia University Medical Center-New York Presbyterian NYSGE First Year Fellow Course 2018
Procedural Sedation Daniela Jodorkovsky M.D. Gastroenterology Fellowship Director Assistant Professor Medicine Columbia University Medical Center-New York Presbyterian NYSGE First Year Fellow Course 2018
IV Sedation & Analgesia Update 2012
 IV Sedation & Analgesia Update 2012 Hospital Directive No. 94 1 Read all content before taking test. Click on Right Arrow at top or bottom to advance to next page. 1 Hospital Directive No. 94 Purpose:
IV Sedation & Analgesia Update 2012 Hospital Directive No. 94 1 Read all content before taking test. Click on Right Arrow at top or bottom to advance to next page. 1 Hospital Directive No. 94 Purpose:
SEDATION IN CHILDREN
 Overview Definition Indications Risks Contraindications Pre-sedation Evaluation NBM / fasting recommendations for elective procedures Procedures relating to sedation Call for Help Recovery and Discharge
Overview Definition Indications Risks Contraindications Pre-sedation Evaluation NBM / fasting recommendations for elective procedures Procedures relating to sedation Call for Help Recovery and Discharge
Trust Policy. Title: Sedation Policy for Adult Patients. Key Points
 Trust Policy Title: Sedation Policy for Adult Patients Authors: Barry Nicholls, Consultant Anaesthetist & Jon Beard, Chief Pharmacist Policy Lead: Barry Nicholls, Consultant Anaesthetist Ratified by: Policy
Trust Policy Title: Sedation Policy for Adult Patients Authors: Barry Nicholls, Consultant Anaesthetist & Jon Beard, Chief Pharmacist Policy Lead: Barry Nicholls, Consultant Anaesthetist Ratified by: Policy
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
VANDERBILT UNIVERSITY MEDICAL CENTER DIVISION OF ANESTHESIOLOGY CRITICAL CARE MEDICINE AIRWAY MANAGEMENT
 These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
These guidelines are based upon medical literature review and expert opinion and are intended to provide recommendations for in the care of critically ill patients. Best Practice Guidelines Checklist for
CHAPTER 4 Procedural Sedation and Analgesia
 CHAPTER 4 Procedural Sedation and Analgesia David B. Burbulys PERSPECTIVE The performance of painful diagnostic and therapeutic procedures is common in emergency care. Many of these are associated with
CHAPTER 4 Procedural Sedation and Analgesia David B. Burbulys PERSPECTIVE The performance of painful diagnostic and therapeutic procedures is common in emergency care. Many of these are associated with
The goal of deep sedation is to achieve a medically controlled state of depressed consciousness from which the patient is not easily aroused.
 SUBJECT: Deep Sedation POLICY NUMBER: PAMC/MS 951.139 Policy Type: Patient Care New Revised Reviewed EXECUTIVE Approval: Date Signed: 10.29.2014 /s/ Richard D. Mandsager, MD, Chief Executive Providence
SUBJECT: Deep Sedation POLICY NUMBER: PAMC/MS 951.139 Policy Type: Patient Care New Revised Reviewed EXECUTIVE Approval: Date Signed: 10.29.2014 /s/ Richard D. Mandsager, MD, Chief Executive Providence
Moderate Sedation: Risks and Challenges
 Moderate Sedation: Risks and Challenges WWW.RN.ORG Reviewed May, 2017, Expires May, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited Developed by Melissa
Moderate Sedation: Risks and Challenges WWW.RN.ORG Reviewed May, 2017, Expires May, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited Developed by Melissa
See Policy CPT CODE section below for any prior authorization requirements. This policy applies to:
 Effective Date: 1/1/2019 Section: MED Policy No: 108 Medical Officer 1/1/19 Date Medical Policy Committee Approved Date: 6/12; 9/12; 7/13; 10/13; 12/13; 11/14; 1/15; 12/15; 4/16; 12/16; 7/17; 8/17; 12/17;
Effective Date: 1/1/2019 Section: MED Policy No: 108 Medical Officer 1/1/19 Date Medical Policy Committee Approved Date: 6/12; 9/12; 7/13; 10/13; 12/13; 11/14; 1/15; 12/15; 4/16; 12/16; 7/17; 8/17; 12/17;
MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa
 MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.44 Subject: Policy: Purpose: Moderate (Conscious) Sedation Conscious sedation will be ordered
MARSHALLTOWN MEDICAL & SURGICAL CENTER Marshalltown, Iowa CARE OF PATIENT POLICY & PROCEDURES Policy Number: 4.44 Subject: Policy: Purpose: Moderate (Conscious) Sedation Conscious sedation will be ordered
PEDIATRIC ANALGESIA AND SEDATION DRUG MANUAL
 PEDIATRIC ANALGESIA AND SEDATION DRUG MANUAL HARBOR-UCLA MEDICAL CENTER PEDIATRIC ANALGESIA AND SEDATION DRUG MANUAL SECTION Preface Disclaimer Nonpharmacologic Methods Table of Contents PAGE i ii iii
PEDIATRIC ANALGESIA AND SEDATION DRUG MANUAL HARBOR-UCLA MEDICAL CENTER PEDIATRIC ANALGESIA AND SEDATION DRUG MANUAL SECTION Preface Disclaimer Nonpharmacologic Methods Table of Contents PAGE i ii iii
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate
 Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
10/20/2009. Ann Emerg Med, Feb 2005
 Critical Decisions in ED Procedural Sedation and Analgesia Why is ED procedural sedation important? Susan Lambe, MD Assistant Clinical Professor UCSF Department of Emergency Medicine Why is procedural
Critical Decisions in ED Procedural Sedation and Analgesia Why is ED procedural sedation important? Susan Lambe, MD Assistant Clinical Professor UCSF Department of Emergency Medicine Why is procedural
Preoperative Assessment. Block Prof JLA Rantloane Department of Anaesthesiology
 Preoperative Assessment Block 18 2013 Prof JLA Rantloane Department of Anaesthesiology!1 Principles All patients scheduled to undergo surgery should have a preoperative evaluation to assist in planning
Preoperative Assessment Block 18 2013 Prof JLA Rantloane Department of Anaesthesiology!1 Principles All patients scheduled to undergo surgery should have a preoperative evaluation to assist in planning
The Game Plan. Should I Be Doing This? The Perfect Drug. Procedural Sedation
 Procedural Sedation Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 The Game Plan Who shouldn t get sedation
Procedural Sedation Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 The Game Plan Who shouldn t get sedation
BSUH ED PROCEDURAL SEDATION WORKBOOK
 BSUH ED PROCEDURAL SEDATION WORKBOOK Introduction: Procedural sedation is the process of inducing an altered level of consciousness in a patient, usually to allow us to perform an otherwise painful or
BSUH ED PROCEDURAL SEDATION WORKBOOK Introduction: Procedural sedation is the process of inducing an altered level of consciousness in a patient, usually to allow us to perform an otherwise painful or
Sedation in Children
 CHILDREN S SERVICES Sedation in Children See text for full explanation and drug doses Patient for Sedation Appropriate staffing Resuscitation equipment available Monitoring equipment Patient suitability
CHILDREN S SERVICES Sedation in Children See text for full explanation and drug doses Patient for Sedation Appropriate staffing Resuscitation equipment available Monitoring equipment Patient suitability
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
May 2013 Anesthetics SLOs Page 1 of 5
 May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
May 2013 Anesthetics SLOs Page 1 of 5 1. A client is having a scalp laceration sutured and is to be given Lidocaine that contains Epinephrine. The nurse knows that this combination is desgined to: A. Cause
Pre anaesthetic evaluation of difficult tracheal intubation
 Pre anaesthetic evaluation of difficult tracheal intubation Dr. AL. Meenakshi Sundaram M.D., D.A., GC Member,ISA National Professor of Anesthesiology Thanjavur Medical College Thanjavur, TamilNadu Phone:
Pre anaesthetic evaluation of difficult tracheal intubation Dr. AL. Meenakshi Sundaram M.D., D.A., GC Member,ISA National Professor of Anesthesiology Thanjavur Medical College Thanjavur, TamilNadu Phone:
Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia
 DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
DIFFICULT AIRWAY CANNOT VENTILATE, CANNOT INTUBATE. Dr.Bharghavi.M 2 nd year post graduate Dept of Anaesthesia Difficult airway According to AMERICAN SOCIETY OF ANAESTHESIOLOGISTS Difficult Airway is defined
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
General Pediatric Approach to Sedation in a Community Hospital
 General Pediatric Approach to Sedation in a Community Hospital Guideline developed by Sarah Tariq, MD, in collaboration with the ANGELS team. Last reviewed by Sarah Tariq, MD, September 14, 2016. Preface
General Pediatric Approach to Sedation in a Community Hospital Guideline developed by Sarah Tariq, MD, in collaboration with the ANGELS team. Last reviewed by Sarah Tariq, MD, September 14, 2016. Preface
The following criteria must be met in order to obtain pediatric clinical privileges for pediatric sedation.
 Pediatric Sedation Sedation of children is different from sedation of adults. Sedatives are generally administered to gain the cooperation of the child. The ability of the child to cooperate depends on
Pediatric Sedation Sedation of children is different from sedation of adults. Sedatives are generally administered to gain the cooperation of the child. The ability of the child to cooperate depends on
POLICY and PROCEDURE
 Misericordia Community Hospital Administration of Intravenous FentaNYL During Labour POLICY and PROCEDURE Labour and Delivery Manual Original Date Revised Date Approved by: Director, Women s Health, Covenant
Misericordia Community Hospital Administration of Intravenous FentaNYL During Labour POLICY and PROCEDURE Labour and Delivery Manual Original Date Revised Date Approved by: Director, Women s Health, Covenant
Naloxone Intranasal EMT OPTIONAL SKILL. Cell Phones and Pagers. Course Outline 09/2017
 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Conscious sedation in children
 Michael Sury FRCA PhD Matrix reference 2D06, 3A07, 3D00 Key points Effective sedation techniques are specific to the procedure. Conscious sedation in children can be time-consuming but may save anaesthesia
Michael Sury FRCA PhD Matrix reference 2D06, 3A07, 3D00 Key points Effective sedation techniques are specific to the procedure. Conscious sedation in children can be time-consuming but may save anaesthesia
Utilization of Ketamine for Pain, Excited Delirium, and Procedural Sedation in the Emergent Setting
 Utilization of Ketamine for Pain, Excited Delirium, and Procedural Sedation in the Emergent Setting Daniel Yousef, Pharm.D. Emergency Medicine Clinical Specialist Residency Program Director, PGY-2 Emergency
Utilization of Ketamine for Pain, Excited Delirium, and Procedural Sedation in the Emergent Setting Daniel Yousef, Pharm.D. Emergency Medicine Clinical Specialist Residency Program Director, PGY-2 Emergency
Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off.
 1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
Supportive Data: Purpose:
 Sedation/Analgesia Administration for Procedures ~ Pediatric Moderate/Procedural Sedation Manual: Patient Care Category: Pain Management/Sedation & Analgesia Review responsibility: SVP - Medical Affairs;
Sedation/Analgesia Administration for Procedures ~ Pediatric Moderate/Procedural Sedation Manual: Patient Care Category: Pain Management/Sedation & Analgesia Review responsibility: SVP - Medical Affairs;
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Appendix A: Pharmacologic approaches to pain management during MVA
 Pain medication Though the medications shown below are commonly used for pain management during uterine evacuation, many other options exist. This table does not cover general anesthetic agents. Both anxiolytics
Pain medication Though the medications shown below are commonly used for pain management during uterine evacuation, many other options exist. This table does not cover general anesthetic agents. Both anxiolytics
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012
 Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
Dr Alireza Yarahmadi and Dr Arvind Perathur Mercy Medical Center - Winter Retreat Des Moines February 2012 Why screen of OSA prior to surgery? What factors increase the risk? When due to anticipate problems?
How to Predict and Avoid Airway Disasters. Muhammad Umer Ihsan
 How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
Results of a one-year, retrospective medication use evaluation. Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital
 Results of a one-year, retrospective medication use evaluation Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital Briefly review ketamine s history, mechanism of action, and unique properties
Results of a one-year, retrospective medication use evaluation Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital Briefly review ketamine s history, mechanism of action, and unique properties
Community Paediatric Policy for minimal sedation
 Community Paediatric Policy for minimal sedation Classification: Policy Lead Author: Amy Wilson Consultant Community Paediatrician Additional author(s): Trust Sedation Comittee Authors Division: Salford
Community Paediatric Policy for minimal sedation Classification: Policy Lead Author: Amy Wilson Consultant Community Paediatrician Additional author(s): Trust Sedation Comittee Authors Division: Salford
CHE X CHN X CHS X CHVH X CWH 1 9 CANCELS: 8/6/07; 10/26/10; 5/1/13; 10/23/13 EFFECTIVE:
 Approved For: X CHE X CHN X CHS X CHVH X CWH Page 1 of 9 TITLE: MODERATE/CONSCIOUS SEDATION Purpose This policy assures the standard of care is consistent for all patients receiving moderate/conscious
Approved For: X CHE X CHN X CHS X CHVH X CWH Page 1 of 9 TITLE: MODERATE/CONSCIOUS SEDATION Purpose This policy assures the standard of care is consistent for all patients receiving moderate/conscious