End of Life Care in Renal Disease. Tara Collidge Consultant, Glasgow Renal Unit
|
|
|
- Aubrey Cross
- 5 years ago
- Views:
Transcription
1 End of Life Care in Renal Disease Tara Collidge Consultant, Glasgow Renal Unit
2 Aim to cover.. Background of end stage renal failure population Registry data (SRR) Our unit outcomes How to know when someone is better off without dialysis What to expect if you don t dialyse / stop dialysing Symptom control / managing death
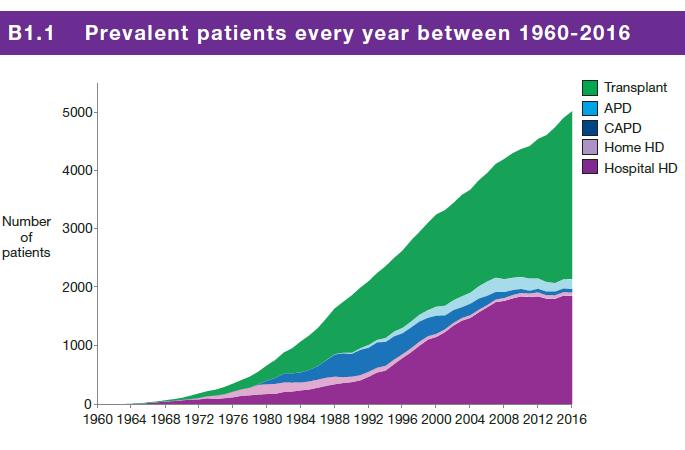
3 Factoids (1) RRT = all forms of dialysis + transplantation Since ,337 patients have started RRT in Scotland (until Dec 2016) 106 per million people start RRT in per million people start RRT age >65 Median age 2016 was 61 years 5026 prevalent patients 2016 rising due to better life expectancy + 57% have Tx SRR data 2017
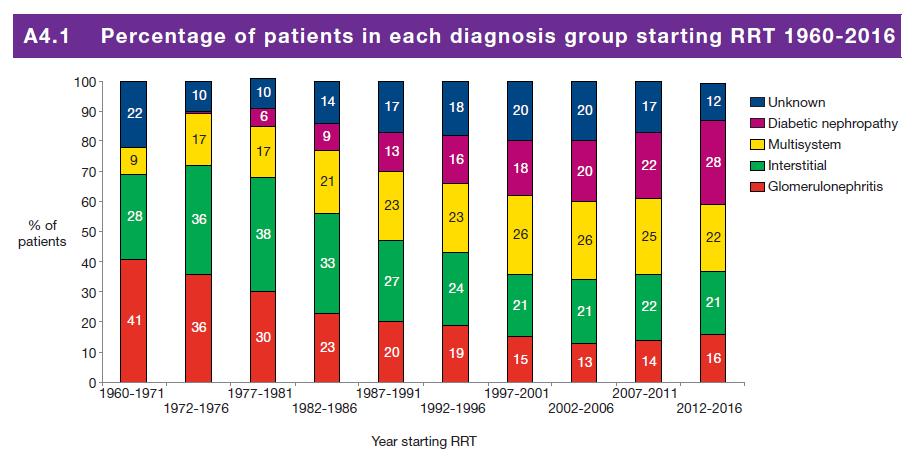
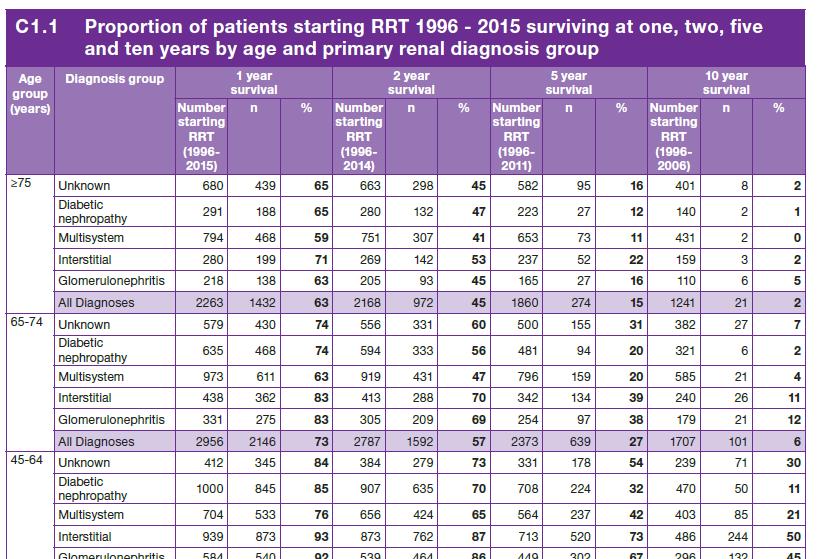
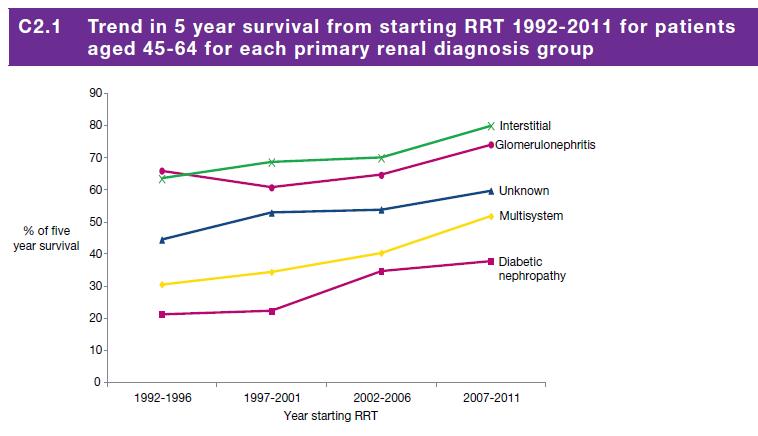
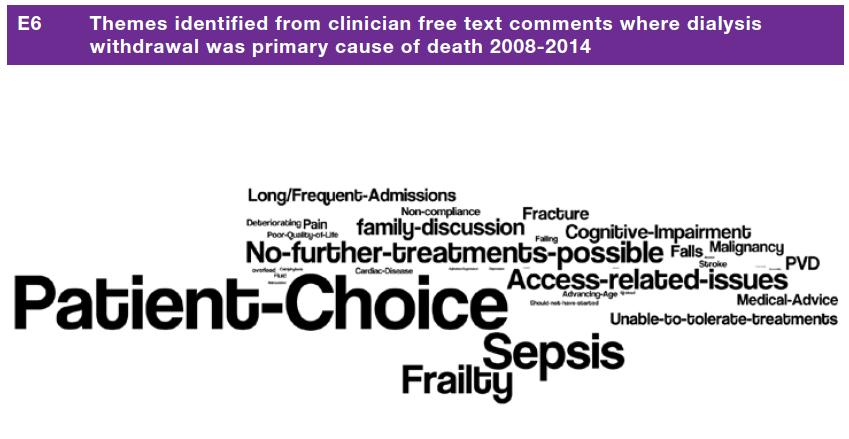
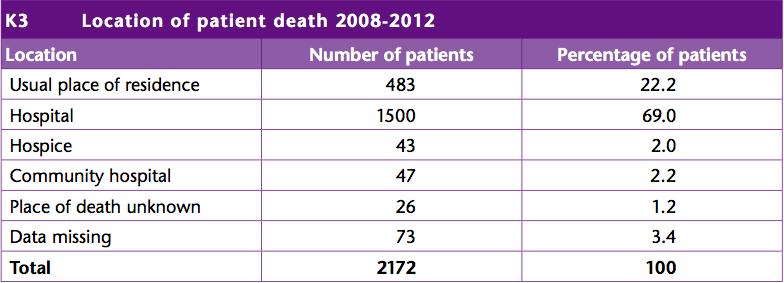
4 Factoids (2) Age + PRD + SD predict survival on RRT Overall survive on RRT 43% at 5 years Outcomes for diabetes worse 27% aged >75 die from withdrawal of dialysis. SMART audit data suggests 33% withdrawal contributes to death. 65% RRT patients die in hospital Overall dialysis population is becoming frailer SRR data 2017
5
6
7
8
9
10
11
12
13
14
15
16



17
18 Renal Replacement Therapy Frail CKD 5 (n = 98) Transplant (n = 1) Died before starting (n = 14) Started HD (n = 26) Planning dialysis Died undecided (n = 2) (n = 59) Changed (n = 10) Conservative Care (n = 36) Starting PD (n = 5) Death (n=77)
19 Demographics Mean age CC choice n=36 RRT choice Received Died before n=59 RRT RRT/changed n=31 n= (n=36) (n=24) 60 (n=12) Charleston 8 comorbidity % PPSV2 60 (n=26) % Diabetes 47
20 Survival Survival advantage of 5 months from egfr 15 for those who started RRT (21 vs 16m) 34% of RRT patients died within 1 year of starting dialysis
21 Vascular Access 39 fistulae created in 33 people 17 (43%) were used Fistula complication/failure to mature Changed to conservative care Died before starting dialysis 30 tunnelled lines in 20 patients all used 10 episodes of line sepsis (33%) 4 PD catheters for 4 patients no complications
22 Emergency admissions in last 6 months of life RRT No RRT Emergency admissions last 6m Renal admissions Mean number of days in hospital
23 Quality of Death Conservative care (n = 32) RRT received Died before RRT (n = 19) (n = 14) RRT then CC (n = 10) DNAR 75% 73.7% 14.3% 100% End of life planning 62.5% 42.1% 7.1% 50% Cause of death 9 unknown 5 ESRD alone 6 ESRD +other 10 infection 3 malignancy 7 CV disease 9 withdrawal of 5 unknown dialysis 3 ESRD +other 6 CV disease 5 CV disease 5 infection 4 sepsis/infection 1 unknown 6 ESRD alone 3 ESRD + other 2 malignancy
24 RRT Summary RRT population is getting older & more comorbid Small survival advantage for some Median survival < 2 years RRT requires intervention RRT population spend more time in hospital RRT population likely to die in hospital Big impact on quality of life
25 Dialysis is not great if you are old & frail, but is it better than the alternative? Dialysis...damned if you do, dead if you don t
26 Will patients live longer on dialysis? UK, n=38, consecutive patients from clinic >75yrs + high co-morbidity 19 conservative vs. 19 RRT After one year: RRT more admissions (14 vs 5, p=0.008) RRT more infection (8 vs 0, p=0.003) RRT more deaths (7 vs 2, p=0.12) Dasgupta et al Nat Clin Prac Nephrol (9);

27 Will patients live longer on dialysis? UK, n=844, 155 CM >75yrs + high co-mobidity 4 months survival benefit Farrington et al NDT 2011
28 Will patients live longer on dialysis? UK, n=441, >70yrs 172 CC vs 269 RRT Survival advantage lost: >80yrs Poor functional status High co-morbidity RRT group: more admissions Less EOL planning Die in hospital vs home Hussain et al Palliative Medicine (9):829
29 Is Dialysis Really Better Than The Alternative? Dialysis prolongs life for the majority of people BUT it may not do so for frail people: poor functional status nursing homes not passing the surprise question high co-morbidity DM, PVD, dementia >75yrs Cannot predict survival benefit for an individual Decision to have dialysis remains patient choice
30 Holley CJASN :1033

31 Palliative care terminal care...treatment that strives to improve quality of life and relieve suffering for patients with life-threatening illness and their families. Boyd K, Murray S A BMJ 2010;341:bmj.c4863
32 Supportive & Palliative Care Slow CKD progression Treat CKD consequences Clinical Frailty Score Holistic Assessment Social Spiritual Financial Symptoms Anticipatory Care Planning Plan for uncertainty Contacts Sick rules Just in case drugs
33 Treat CKD Progression Disease specific treatments Slow progression of CKD: BP Proteinuia Acidosis (Glycaemic control) Lifestyle activity & weight loss
34 Treat CKD Consequences Anaemia Acidosis Fluid status / BP Bone disease Hyperkalaemia Symptom management (Fertility / sexual health) (RRT planning = Tx vs other)
35 Clinical Frailty Score Simple, validated in ESRF Predicts poor outcome at onset of HD Predicts choosing CC or death prior to dialysis at RRT education stage Recently adopted this score 3 monthly in RDU CKD 5 group
36 Holistic Assessment Specific meeting with CNS Family / carers present Knowledge of linked services Signpost to appropriate services Build a relationship / trust Begin ACP GP register, DNACPR etc Deliver education & information Provide point of contact
37 Guiding Principals for Therapy Stop unnecessary drugs as health declines Don t treat things that won t improve QOL Ask about symptoms Ask about exacerbating factors Anxiety, social circumstances, nocturia Can use some drugs usually contraindicated at end of life NSAIDs Proactive care prevents admissions eg infection Start low & titrate up doses
38 Symptom Management High symptom burden from CKD & co-morbidities: dialysis patients - >50% experienced symptoms (59 studies reviewed) CKD5 managed conservatively - >33% experienced symptoms, similar to advanced cancer population Last month life - >50% physical + psychological distress, more than cancer cohort Murtagh et al Adv Chronic Kidney Dis Jan;14(1): Murtagh et al J Palliat Med Dec;10(6): Noble et al J Renal Care 2010 Mar 36(1):9-15
39
40 Patients with ESRF have a high symptom burden Uraemic Symptoms lack of energy, 76% pruritus, 74% drowsiness, 65% dyspnea, 61% oedema, 58% pain, 53% - type? dry mouth, 50% muscle cramps, 50% restless legs, 48% lack of appetite, 47% poor concentration, 44% dry skin, 42% sleep disturbance, 41% constipation, 35% Co-Morbidities Diabetic neuropathy PVD Musculoskeletal Dialysis Recovery time Hypotension Nausea Cramp Headache Access related Primary Renal Condition SLE Vasculitis Myeloma APCKD
41 Modified Pain Ladder Paracetamol NSAIDs residual function GI bleeding Opiate Sensitivity varies so warn carers re acculmulation jerking, drowsy Buprenorphine patch good as low dose Avoid long acting preps in CKD4/5 Fentanyl + alfentanyl better than morphine Co-prescribe laxatives & anti-emetics Midazolam / diazepam if agitated Gabapentin if neuropathic mg nocte or mg alt days CKD5 Probably better than amitriptyline, carbamazepine Calciphylaxis especially problematic
42 Itch Superimposed conditions Other eg TFT, amyloid etc Transplantation cure Better dialysis Control anaemia Control bone disease neuropeptides Histamine et al Uraemia Xerosis Anaemia Hyperparathyroidism (Ca, P, PTH) B2 microglobulin Opioid Receptors Antihistamines don t work Emoillients Menthol / capsaicin Steroids UV GLA/eve primrose (Naltrexone opiate Ag) Nalfurafine uopiate Ag Gabapentin Ondansetron Thalidamide
43 Restless Legs Clonazepam Dopamine Agonists eg Madopar Gabapentin
44 Nausea 1. Review diet eg regular supplements 2. Stop phosphate binders / oral iron? 3. Treat constipation Metoclopramide / Domperidone Gastric stasis common before breakfast / meals Can be good for hiccups (baclofen also) Cyclizine Levomepromazine (watch BP) Haloperidol (also agitation, delirium)
45 Breathlessness Correct anaemia Correct acidosis Treat anxiety midazolam/lorazepam Improve fluid overload salt/water/diuretics Consider cardiac / respiratory disease Opiates oramorph, sc forms Hyoscine for secretions
46 Depression SSRIs eg citalopram, sertraline TCAs if resistant Psychological therapies Talking identify fears
47 End of Life Medication Refer to Renal Palliative Care Last Days of Life document (SERPR) Work together GP / district nurses Open line of contact Family may need renal unit contact Link with palliative care teams as needed
48 Diagnosing Dying Not good at this Crisis prone & higher rates of sudden death Allows futile treatments not to be pursued Allows transition to terminal care Allows focus on QOL / symptoms / spiritual / psychosocial issues Better outcomes for bereaved Families need an alternative narrative
49 Case 1 Dialysis withdrawal Age 76, male, HD May July 2013 (7 yrs) IHD/MIs, PVD, AAA, BP, COPD Catheter & recurrent UTIs 7 admissions last 6 months life reducing QOL Patient requested withdrawal Planning with GP / family / Palliative Care ( /phone) DNACPR in place Medication plan District nurses & palliative CNS activated Access to guidelines & specialist if needed Died at home 7 days later (preferred place)
50 Case 2 Dialysis withdrawal Age 75yr, male, HD April 2012 Nov 2013 (1.5yrs) IHD(MI), RAS, PVD, Renal Cell Ca 4 admissions 7 reviews with family 2 man transport, wheelchair, leg pain, frail, initial improvement in symptoms then progressive decline + PVD symptoms + long recovery time post HD Reluctance to engage in ACP Final admission pain+, amputation, last HD 14 days prior to death
51 Stopping Dialysis discussion points What will happen to me? How long have I got? 12 days average HD vs PD May feel better initially then coma Fluid overload opiates/midazolam vs UF Renal Unit attachment Access to specialist advice Mode of death coma vs K
52 Case 3 Conservative Care Age 77 yrs, female, 1st review (10yrs, 2yrs from CKD5) DM, COPD, BP, gout 2 admissions last year of life Daughter RRT due to DN Sustained wish for conservative care Attended CC clinic tired (IV iron,esa), cramp (quinine), intermittent confusion, egfr 7 16 remote contacts with renal unit & family / GP advice re fluid, agitation, nausea, pain (alfentanil+midazolam+levomepromazine SC) Family support Died at home (preferred place) from ESRF
53 Conservative Care discussion points Crisis points can trigger admission Crisis points can trigger dialysis More likely to have residual renal function May die from an unrelated cause Often low symptom burden until late Can decline rapidly family/gp need access to help when needed May survive a long time
54 Case 4 Early death on dialysis Age 77yrs, RRT April 2013 Aug 2013 (4mo) Cirrhosis, IHD (MI+LVF), COPD Keen for HD started with AVF 7 admissions post HD start chest sepsis, IHD, c.diff, inguinal hernia Wished to continue HD + CPR 2 weeks prior to death GP + family decided to stop HD died at home 5 days later
55 Why is ACP so hard? Failure to recognise decline on part of doctor or patient surprise question Communication is difficult Denial is a coping strategy Easier to offer intervention Faster to offer intervention


56 Death remains an unpopular choice
57 Summary ESRF population is becoming older with higher comorbidity Low awareness of poor prognosis in ESRF High symptom burden - similar to cancer Illness trajectory is variable - timely ACP is important plan for uncertainty Unplanned admissions are common hospital death or dialysis Renal adjustment for drugs Good communication between primary & secondary care is essential
58 Thank You!
Regional Renal Training
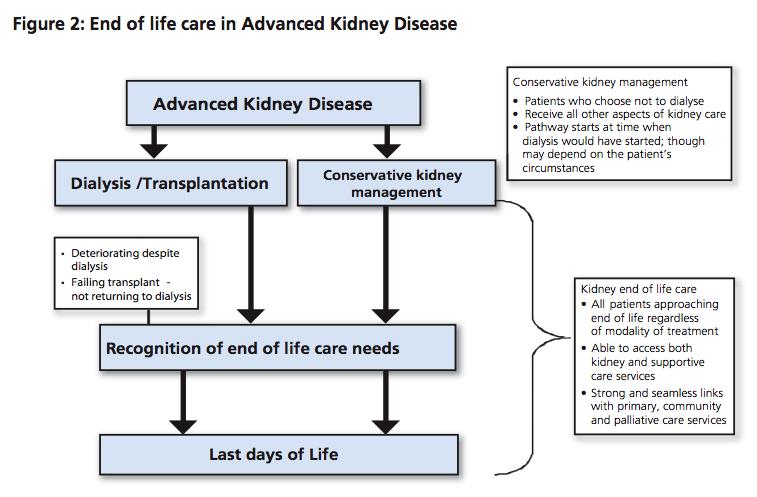
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Oxford Kidney Unit A guide to conservative kidney management. Information for Healthcare Professionals
 Oxford Kidney Unit A guide to conservative kidney management Information for Healthcare Professionals What is conservative kidney management? Some people with advanced kidney disease (chronic kidney disease
Oxford Kidney Unit A guide to conservative kidney management Information for Healthcare Professionals What is conservative kidney management? Some people with advanced kidney disease (chronic kidney disease
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital
 - Conservative. Elizabeth Josland Renal Supportive Care CNC St George Hospital") Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Care of the dying in End Stage Kidney Disease (ESKD) - Conservative Elizabeth Josland Renal Supportive Care CNC St George Hospital Introduction What does conservative management look like? How does the
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Delivering personalised care to end of life patients. Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London
 Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Delivering personalised care to end of life patients Jane Naismith Nurse Consultant in Palliative care St Joseph s Hospice London Over View This session will cover Supporting patients with long term conditions
Palliative and End of Life Care in End Stage Renal Disease
 Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Palliative and End of Life Care in End Stage Renal Disease Palliative and End of Life Care Priority for Action Regional Consensus Workshop 30.06.2010 Neal Morgan Consultant Nephrologist SHSCT Outline Introduction
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
PATIENTS WHO WITHDRAW FROM DIALYSIS. Dr Katalin Urban Palliative Care Specialist Greenwich Hospital
 PATIENTS WHO WITHDRAW FROM DIALYSIS Dr Katalin Urban Palliative Care Specialist Greenwich Hospital Registrar project for FRACP Title: Patients who withdraw from dialysis in a Sydney centre with Palliative
PATIENTS WHO WITHDRAW FROM DIALYSIS Dr Katalin Urban Palliative Care Specialist Greenwich Hospital Registrar project for FRACP Title: Patients who withdraw from dialysis in a Sydney centre with Palliative
Treating the symptoms of kidney failure
 Treating the symptoms of kidney failure Information for patients, relatives and carers Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact:
Treating the symptoms of kidney failure Information for patients, relatives and carers Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact:
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
Pain and Chronic Kidney Disease
 Pain and Chronic Kidney Disease Frank Brennan Palliative Care Physician Department of Nephrology, St George Hospital Renal Supportive Care Symposium St George Hospital August 21 2015 Epidemiology Effect
Pain and Chronic Kidney Disease Frank Brennan Palliative Care Physician Department of Nephrology, St George Hospital Renal Supportive Care Symposium St George Hospital August 21 2015 Epidemiology Effect
Supportive Care for the Person with Chronic Kidney Disease. Dr. J. Kappel May 2014
 Supportive Care for the Person with Chronic Kidney Disease Dr. J. Kappel May 2014 Objectives 1 To develop an understanding of renal replacement therapy (RRT) and comprehensive conservative management and
Supportive Care for the Person with Chronic Kidney Disease Dr. J. Kappel May 2014 Objectives 1 To develop an understanding of renal replacement therapy (RRT) and comprehensive conservative management and
If dialysis is not started, established renal failure will eventually lead to death although the time scale is variable from weeks to months.
 Supportive care for adult renal patients with Established Renal Failure : information for GPs and District Nurses RRCV CMG Nephrology Service 1. Introduction 1.1 Supportive care for renal patients Part
Supportive care for adult renal patients with Established Renal Failure : information for GPs and District Nurses RRCV CMG Nephrology Service 1. Introduction 1.1 Supportive care for renal patients Part
The John Walls Renal Unit Leicester General Hospital University Hospitals of Leicester
 The John Walls Renal Unit Leicester General Hospital University Hospitals of Leicester Supportive Care for Renal Patients Author: Renal and Palliative Care Written May 2010; updated May 2012 and Dec 2012
The John Walls Renal Unit Leicester General Hospital University Hospitals of Leicester Supportive Care for Renal Patients Author: Renal and Palliative Care Written May 2010; updated May 2012 and Dec 2012
Palliative care in long-term conditions Scottish Palliative Care Pharmacists Association
 Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Supportive and Palliative care for patients with Pancreatic Cancer. Dr Holly Taylor September 2018
 Supportive and Palliative care for patients with Pancreatic Cancer Dr Holly Taylor September 2018 Aims of this session To discuss the principles of supportive and palliative care Identification of patients
Supportive and Palliative care for patients with Pancreatic Cancer Dr Holly Taylor September 2018 Aims of this session To discuss the principles of supportive and palliative care Identification of patients
ESCALATING PATIENT & CARER NEEDS TOWARDS END OF LIFE; OVERVIEW OF END OF LIFE CARE IN THE COMMUNITY Renal Supportive Care Nursing Elizabeth Josland
 ESCALATING PATIENT & CARER NEEDS TOWARDS END OF LIFE; OVERVIEW OF END OF LIFE CARE IN THE COMMUNITY Renal Supportive Care Nursing Elizabeth Josland CNC Objectives Dialysis vs non-dialysis end of life picture
ESCALATING PATIENT & CARER NEEDS TOWARDS END OF LIFE; OVERVIEW OF END OF LIFE CARE IN THE COMMUNITY Renal Supportive Care Nursing Elizabeth Josland CNC Objectives Dialysis vs non-dialysis end of life picture
THE CONSERVATIVE CARE PATHWAY
 THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
THE CONSERVATIVE CARE PATHWAY Dr. Gaylene Hargrove Sept. 19, 2015 Island Health Renal Program End of Life Conference Learning Objectives Describe and discuss what defines conservative care. Identify key
Integrating Renal & Palliative Care Nurse-Led Intervention
 Ballarat Hospice Care Inc. & Ballarat Health Service- Dialysis Shared Care Model Integrating Renal & Palliative Care Nurse-Led Intervention SMRPCC Clinical Forum, 20 th May 2016 Vicky Smith, RN MANP Palliative
Ballarat Hospice Care Inc. & Ballarat Health Service- Dialysis Shared Care Model Integrating Renal & Palliative Care Nurse-Led Intervention SMRPCC Clinical Forum, 20 th May 2016 Vicky Smith, RN MANP Palliative
End Stage Liver Disease Regional Audit Casenote Survey
 1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
 The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
Renal Supportive Care. Renal Supportive Care Symposium 2013 Elizabeth Josland CNC
 Renal Supportive Care. Renal Supportive Care Symposium 2013 Elizabeth Josland CNC Outline Background of Renal Supportive Care Conservative Management Symptom overview Reading What does conservative management
Renal Supportive Care. Renal Supportive Care Symposium 2013 Elizabeth Josland CNC Outline Background of Renal Supportive Care Conservative Management Symptom overview Reading What does conservative management
Symptom Control in Heart Failure. Dr Claire L Hookey
 Symptom Control in Heart Failure Dr Claire L Hookey Heart Failure symptoms Class III/IV CHF, mean 67.1 years, mean EF 22.3% Most prevalent symptoms:- lack of energy (66%) dry mouth (62%) shortness of breath
Symptom Control in Heart Failure Dr Claire L Hookey Heart Failure symptoms Class III/IV CHF, mean 67.1 years, mean EF 22.3% Most prevalent symptoms:- lack of energy (66%) dry mouth (62%) shortness of breath
A tale of two specialties
 A tale of two specialties United Kingdom Annual Symposia on Renal-Palliative Care co-organised by both disciplines National Service Framework for Renal Services Part 2 (UK) - 2005 Concentrated on the
A tale of two specialties United Kingdom Annual Symposia on Renal-Palliative Care co-organised by both disciplines National Service Framework for Renal Services Part 2 (UK) - 2005 Concentrated on the
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care
 SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
SERVICE SPECIFICATION 6 Conservative Management & End of Life Care Table of Contents Page 1 Key Messages 2 2 Introduction & Background 2 3 Relevant Guidelines & Standards 2 4 Scope of Service 3 5 Interdependencies
8. Pharmacological Management
 8. Pharmacological Management Neurohormonal deactivation 1. Adrenaline Beta Blockers Dose Side Effects Monitoring Neurohormonal Deactivation 2. Angiotensin II ACE Inhibition Dose Side Effects Monitoring
8. Pharmacological Management Neurohormonal deactivation 1. Adrenaline Beta Blockers Dose Side Effects Monitoring Neurohormonal Deactivation 2. Angiotensin II ACE Inhibition Dose Side Effects Monitoring
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
End of Life Care in IJN Our journey. Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia
 End of Life Care in IJN Our journey Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia End of Life Dying is final part of everyone journey in life Deaths used to occur
End of Life Care in IJN Our journey Dato Dr. David Chew Soon Ping Consultant Cardiologist National Heart Institute Malaysia End of Life Dying is final part of everyone journey in life Deaths used to occur
Conservative Care Pathway: A Client-Centred Approach
 2016 Conservative Care Pathway: A Client-Centred Approach Abbotsford Kidney Care Clinic October 7, 2016 Bobbi Preston, MSW, RCSW Jane Valcourt, RN Susan Cooper, MD, FRCP Goals of Session 1. Introduce the
2016 Conservative Care Pathway: A Client-Centred Approach Abbotsford Kidney Care Clinic October 7, 2016 Bobbi Preston, MSW, RCSW Jane Valcourt, RN Susan Cooper, MD, FRCP Goals of Session 1. Introduce the
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
30/01/2017. Renal Palliative Medicine. Oxford General Medicine Course St. Anne s College January The Royal Free Hospital Evening News 1965
 Renal Palliative Medicine Renal Palliative Medicine Oxford General Medicine Course St. Anne s College January 2017 60% of cancer patients have CKD 2-5 Dr. Aoife Lowney K/DOQI clinical practice guidelines
Renal Palliative Medicine Renal Palliative Medicine Oxford General Medicine Course St. Anne s College January 2017 60% of cancer patients have CKD 2-5 Dr. Aoife Lowney K/DOQI clinical practice guidelines
TRAJECTORY OF ILLNESS IN END OF LIFE CARE
 TRAJECTORY OF ILLNESS IN END OF LIFE CARE By Dr Helen Fryer OBJECTIVES To be aware of the three commonest trajectories of decline in the UK To understand the challenges faced in delivering effective Palliative
TRAJECTORY OF ILLNESS IN END OF LIFE CARE By Dr Helen Fryer OBJECTIVES To be aware of the three commonest trajectories of decline in the UK To understand the challenges faced in delivering effective Palliative
Unmet palliative care needs in heart failure heart failure. Dr Claire Hookey
 Unmet palliative care needs in heart failure heart failure Dr Claire Hookey Discomfort was not necessarily greatest in those dying from cancer; patients dying of heart failure, or renal failure, or both,
Unmet palliative care needs in heart failure heart failure Dr Claire Hookey Discomfort was not necessarily greatest in those dying from cancer; patients dying of heart failure, or renal failure, or both,
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
Analgesia in patients with impaired renal function Formulary Guidance
 Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
How do we relieve uraemic symptoms?
 How do we relieve uraemic symptoms? Prof Ann Bonner PhD N School of Nursing, Queensland University of Technology Email: ann.bonner@qut.edu.au Queensland University of Technology CICOS No. 00213J [What
How do we relieve uraemic symptoms? Prof Ann Bonner PhD N School of Nursing, Queensland University of Technology Email: ann.bonner@qut.edu.au Queensland University of Technology CICOS No. 00213J [What
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges. Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009
 Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009 Objectives Highlight the relevance of palliative/supportive care
Palliative Care in Chronic Kidney Disease: Past Successes, Remaining Challenges Sara Davison BC Nephrology Days, Vancouver, BC Nov 6, 2009 Objectives Highlight the relevance of palliative/supportive care
5 key areas for research, and how to go forward. Primary Palliative Care Research Forum, University of Capetown, September, 2010
 5 key areas for research, and how to go forward Primary Palliative Care Research Forum, University of Capetown, September, 2010 Scott A Murray St Columba s Hospice Chair of Primary Palliative Care Primary
5 key areas for research, and how to go forward Primary Palliative Care Research Forum, University of Capetown, September, 2010 Scott A Murray St Columba s Hospice Chair of Primary Palliative Care Primary
Three triggers that suggest that patients could benefit from a hospice palliative care approach
 Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
Why is it important to identify people nearing the end of life? About 1% of the population dies each year. Although some deaths are unexpected, many more in fact can be predicted. This is inherently difficult,
MND Just in Case kit Information for GPs
 MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Palliative Medicine Overview. Francine Arneson, MD Palliative Medicine
 Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
Palliative Medicine Overview Francine Arneson, MD Palliative Medicine Palliative Medicine: Definition Palliative care: An approach that improves the quality of life of patients and their families facing
Palliative Medicine in Critical Care Not Just Hospice. Robin. Truth or Myth 6/11/2015. Francine Arneson, MD Palliative Medicine
 Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
Palliative Medicine in Critical Care Not Just Hospice Francine Arneson, MD Palliative Medicine Robin 45 year old female married, husband in Afghanistan. 4 children ages 17-24. Mother has been providing
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC
 CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Preventing harmful treatment
 Preventing harmful treatment How can Palliative Care prevent patients receiving overzealous or futile treatment? Antwerp, November 2010 Prof Scott A Murray, St Columba s Hospice Chair of Primary Palliative
Preventing harmful treatment How can Palliative Care prevent patients receiving overzealous or futile treatment? Antwerp, November 2010 Prof Scott A Murray, St Columba s Hospice Chair of Primary Palliative
What s New 2003? What new treatments? What have you discontinued? More information please!
 What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
ADVANCE CARE PLANNING FOR KIDNEY PATIENTS: THE IMPORTANCE OF AN ONGOING DISCUSSION
 ADVANCE CARE PLANNING FOR KIDNEY PATIENTS: THE IMPORTANCE OF AN ONGOING DISCUSSION Melissa Hale, MSW, LCSW Advance Care Planning Coordinator ProHealth Care Thank You. CMS: Conditions for Coverage Renal
ADVANCE CARE PLANNING FOR KIDNEY PATIENTS: THE IMPORTANCE OF AN ONGOING DISCUSSION Melissa Hale, MSW, LCSW Advance Care Planning Coordinator ProHealth Care Thank You. CMS: Conditions for Coverage Renal
Managing dying with chronic heart failure
 Heart failure Managing dying with chronic heart failure Chronic heart failure (CHF) is predominantly a pathology of old age affecting 5% of those over 75 years of age. It is more common than cancer and
Heart failure Managing dying with chronic heart failure Chronic heart failure (CHF) is predominantly a pathology of old age affecting 5% of those over 75 years of age. It is more common than cancer and
Palliative Approach to Chronic Disease Management versus End-of-Life Care
 Palliative Approach to Chronic Disease Management versus End-of-Life Care 1 Acknowledgements Marg Poling, RN, Palliative Pain and Symptom Management Consultant North West Community Care Access Centre (Thunder
Palliative Approach to Chronic Disease Management versus End-of-Life Care 1 Acknowledgements Marg Poling, RN, Palliative Pain and Symptom Management Consultant North West Community Care Access Centre (Thunder
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Symptom Control in the Community Setting. Dr Andrew Tysoe-Calnon
 Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Renal Supportive Care an overview. Frank Brennan, Palliative Care Physician.
 Renal Supportive Care an overview. Frank Brennan, Palliative Care Physician. 2014 Renal Palliative Care Caring for adult patients with ESKD an overview Frank Brennan Palliative Care Consultant Department
Renal Supportive Care an overview. Frank Brennan, Palliative Care Physician. 2014 Renal Palliative Care Caring for adult patients with ESKD an overview Frank Brennan Palliative Care Consultant Department
Management of the Frail Older Patients: What Are the Outcomes
 Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
Management of the Frail Older Patients: What Are the Outcomes Professor Edwina Brown Imperial College Renal and Transplant Centre Hammersmith Hospital, London Increasing prevalence of old old on RRT RRT
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
This survey aims to look at individual practice and can be completed by any healthcare professional.
 This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Non Malignant Pain: Symptom Management
 Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Acceptance onto dialysis guidelines: St George Hospital
 Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
Dementia & Palliative Care
 Dementia & Palliative Care Aspiration, Myth or Reality? A Clinicians Perspective... Lesley Jones Advanced Practitioner Dementia Care Dementia Dementia is a chronic progressive mental disorder that adversely
Dementia & Palliative Care Aspiration, Myth or Reality? A Clinicians Perspective... Lesley Jones Advanced Practitioner Dementia Care Dementia Dementia is a chronic progressive mental disorder that adversely
Pain in dementia. Prof Rowan Harwood Geriatrician, NUH. Disclaimer
 Pain in dementia Prof Rowan Harwood Geriatrician, NUH Disclaimer Pain What is pain? Pain Pain is what the patient says it is McCaffery 1968 Pain An unpleasant sensory or emotional experience associated
Pain in dementia Prof Rowan Harwood Geriatrician, NUH Disclaimer Pain What is pain? Pain Pain is what the patient says it is McCaffery 1968 Pain An unpleasant sensory or emotional experience associated
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Dialysis for everyone? Maurizio Gallieni
 Dialysis for everyone? Maurizio Gallieni Nephrology and Dialysis Unit Ospedale S. Carlo Borromeo, ASST Santi Paolo e Carlo, University of Milano, Milano, Italy Introduction NDT 2004; 19: 1357-1360 www.
Dialysis for everyone? Maurizio Gallieni Nephrology and Dialysis Unit Ospedale S. Carlo Borromeo, ASST Santi Paolo e Carlo, University of Milano, Milano, Italy Introduction NDT 2004; 19: 1357-1360 www.
Your Health Survey. Forename: Surname: Renal Unit: Type of treatment: If HD, are you: Date of birth: Home Post Code: Date completed: NHS number:
 Your Health Survey Why this questionnaire You may already have heard about renal units introducing health questionnaires. The purpose of these questionnaires is to find out how your kidney disease affects
Your Health Survey Why this questionnaire You may already have heard about renal units introducing health questionnaires. The purpose of these questionnaires is to find out how your kidney disease affects
INFORMATION FOR PATIENTS. Let s Manage Pain
 INFORMATION FOR PATIENTS Let s Manage Pain 1 About this booklet Persistent pain, also called chronic pain, is pain which continues for longer than expected. Pain can affect all areas of your life. People
INFORMATION FOR PATIENTS Let s Manage Pain 1 About this booklet Persistent pain, also called chronic pain, is pain which continues for longer than expected. Pain can affect all areas of your life. People
WHEN (AND WHEN NOT) TO START DIALYSIS. Shahid Chandna, Ken Farrington
 TO START DIALYSIS. Shahid Chandna, Ken Farrington") WHEN (AND WHEN NOT) TO START DIALYSIS Shahid Chandna, Ken Farrington Changing Perspectives Beta blockers 1980s Contraindicated in heart failure Now mainstay of therapy HRT 1990s must Now only if you have
WHEN (AND WHEN NOT) TO START DIALYSIS Shahid Chandna, Ken Farrington Changing Perspectives Beta blockers 1980s Contraindicated in heart failure Now mainstay of therapy HRT 1990s must Now only if you have
The role of the Nephrologist in Acute Kidney Injury. Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital
 The role of the Nephrologist in Acute Kidney Injury Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital Overview Impact of AKI Need for change Who needs a Nephrologist Are we making
The role of the Nephrologist in Acute Kidney Injury Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital Overview Impact of AKI Need for change Who needs a Nephrologist Are we making
Polypharmacy: Guidance for Prescribing in Frail Adults
 Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Polypharmacy: Guidance for Prescribing in Frail Adults Why is reviewing polypharmacy important? Medication is by far the most common form of medical intervention. Four out of five people aged over 75 years
Supportive and Palliative Action Register (SPAR)
") Supportive and Palliative Action Register (SPAR) Importance of Recognising Change NHSGGC Primary Care Palliative Care Team Tel: 0141 427 8254 palliative.care@ggc.scot.nhs.uk www.palliativecareggc.org.uk/primarycarepcteam/
Supportive and Palliative Action Register (SPAR) Importance of Recognising Change NHSGGC Primary Care Palliative Care Team Tel: 0141 427 8254 palliative.care@ggc.scot.nhs.uk www.palliativecareggc.org.uk/primarycarepcteam/
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
END STAGE RENAL DISEASE AND THE DISCONTINUATION OF DIALYSIS
 END STAGE RENAL DISEASE AND THE DISCONTINUATION OF DIALYSIS Dr. Nicki Apostle December 8, 2014 Disclosures: I listen to Taylor Swift (Don t lie so do you) CASE STUDY: Mrs. S 83 yo F from LTC referred to
END STAGE RENAL DISEASE AND THE DISCONTINUATION OF DIALYSIS Dr. Nicki Apostle December 8, 2014 Disclosures: I listen to Taylor Swift (Don t lie so do you) CASE STUDY: Mrs. S 83 yo F from LTC referred to
Heart Failure Vital steps for palliative care. Dr Karen J Hogg Glasgow Royal Infirmary
 Heart Failure Vital steps for palliative care Dr Karen J Hogg Glasgow Royal Infirmary Overview Why is heart failure a problem? Why do we need integrated cardiology and palliative care services? Cardiology
Heart Failure Vital steps for palliative care Dr Karen J Hogg Glasgow Royal Infirmary Overview Why is heart failure a problem? Why do we need integrated cardiology and palliative care services? Cardiology
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
Anticipatory prescribing and end of life considerations. Dr Stephanie Lippett
 Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
Geriatric Nephrology. Murtener Tage
 Geriatric Nephrology Murtener Tage 2014 Isabelle.Binet@kssg.ch www.nierenstiftung.ch Plan Geriatric nephrology The elderly with CKD The elderly on dialysis The elderly in transplantation Plan Geriatric
Geriatric Nephrology Murtener Tage 2014 Isabelle.Binet@kssg.ch www.nierenstiftung.ch Plan Geriatric nephrology The elderly with CKD The elderly on dialysis The elderly in transplantation Plan Geriatric
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Dialysis in frail and Elderly
 Dialysis in frail and Elderly Dr Shibu Jacob, Assistant Professor, Christian Medical College, Vellore. ISHDCON April 2,2017 Complications during dialysis and soon after? How to minimise these? Should
Dialysis in frail and Elderly Dr Shibu Jacob, Assistant Professor, Christian Medical College, Vellore. ISHDCON April 2,2017 Complications during dialysis and soon after? How to minimise these? Should
Outcomes of dialysis in the elderly. DNT March 2011 Dr Céline Foote
 Outcomes of dialysis in the elderly DNT March 2011 Dr Céline Foote Increasing number of elderly patients on renal replacement therapy 500 500 Patients per million 400 300 200 100 400 300 200 100 TOTAL
Outcomes of dialysis in the elderly DNT March 2011 Dr Céline Foote Increasing number of elderly patients on renal replacement therapy 500 500 Patients per million 400 300 200 100 400 300 200 100 TOTAL
Temiskaming Hospital Hospice Palliative Care. Presented by: Dr. Don Davies January 31, 2017
 Temiskaming Hospital Hospice Palliative Care Presented by: Dr. Don Davies January 31, 2017 Objectives Talk a little about Palliative Care. In general A quick look at Temiskaming District and Hospice Model
Temiskaming Hospital Hospice Palliative Care Presented by: Dr. Don Davies January 31, 2017 Objectives Talk a little about Palliative Care. In general A quick look at Temiskaming District and Hospice Model
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
Palliative Care Asking the questions that matter to me
 Palliative Care Asking the questions that matter to me THE PALLIATIVE HUB Adult This booklet has been developed by the Palliative Care Senior Nurses Network and adapted with permission from Palliative
Palliative Care Asking the questions that matter to me THE PALLIATIVE HUB Adult This booklet has been developed by the Palliative Care Senior Nurses Network and adapted with permission from Palliative
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Dudley End of Life and Palliative Care Strategy Implementation Plan 2017
 Dudley End of Life and Palliative Care Strategy Implementation Plan 2017 End of Life and Palliative Care Strategy 2017 1 Contents Page What is a strategy plan? 3 Terminology 3 Demographics 3 Definitions
Dudley End of Life and Palliative Care Strategy Implementation Plan 2017 End of Life and Palliative Care Strategy 2017 1 Contents Page What is a strategy plan? 3 Terminology 3 Demographics 3 Definitions
Approach to symptom control near the end-of-life
 Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
Approach to symptom control near the end-of-life 18 Sept 2011 Dr Alethea Yee Senior Consultant, Department of Palliative Medicine National Cancer Centre,Singapore What is end of life? No precise definition
How Can Palliative Care Help Your Patient Get Home Sooner?
 How Can Palliative Care Help Your Patient Get Home Sooner? Annette T. Carron, D.O. Director Geriatrics and Palliative Care Botsford Hospital OMED 2014 Patient Care Issues That Can Delay Your Day/ Pain
How Can Palliative Care Help Your Patient Get Home Sooner? Annette T. Carron, D.O. Director Geriatrics and Palliative Care Botsford Hospital OMED 2014 Patient Care Issues That Can Delay Your Day/ Pain
21th Budapest Nephrology School Ágnes Haris, Kálmán Polner
 21th Budapest Nephrology School Ágnes Haris, Kálmán Polner 53 years old female, -worked as computer scientist, -lived with her husband and 2 children, -in excellent financial situation. Diagnosed with
21th Budapest Nephrology School Ágnes Haris, Kálmán Polner 53 years old female, -worked as computer scientist, -lived with her husband and 2 children, -in excellent financial situation. Diagnosed with