Disclosures. I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences.
|
|
|
- Darleen Garrison
- 5 years ago
- Views:
Transcription
1 Disclosures I have given sponsored lectures for the following pharmaceutical companies: Gilead, Abbvie and MSD. I own shares of Gilead Sciences.

2 Chronic Hepatitis C Prof CL Lai University Department of Medicine Queen Mary Hospital, Hong Kong
3 Epidemiology, esp Asia Pacific areas When and who to treat The Direct Acting Antivirals Treatment for renal failure patients
4 Epidemiology of HCV million people have chronic hepatitis C globally Annual mortality 500,000 WHO 2016
5 Epidemiology of HCV in the Asia-Pacific region Asia, Australia and Egypt Largest population of HCV infected persons ~ million adults are anti-hcv positive China alone has more HCV infected persons than all of Europe or the Americas High prevalence areas in Asia & Africa Especially high in Egypt (15%), Vietnam (6.1%) Pakistan (4.7%) and Taiwan (4.4%) Prevalence rises across age and peaks at age in Asia Sievert W, et al. Liver Int 2011;31 Suppl 2:61 80
6 Prevalence (%) HCV prevalence rises across age and peaks at age in Asia Asia Pacific Asia East Asia Southeast Asia Central Asia South High prevalence necessitates: Age group (years) More efforts in primary prevention (needle usage, transfusion services) Enforcement of early HCC screening and alcohol cessation Changes in treatment strategies for infected carriers *** Hanafiah KM, et al. Hepatology 2013;57:

7 HCV prevalence in Asia Pacific Country Prevalence (%) Vietnam 6.1 Pakistan 5.31 Taiwan 4.4 Mainland China 3.2 Cambodia 2.3 Thailand 2.2 Indonesia 2.1 Korea 1.3 Laos 1.1 Myanmar 0.95 India 0.87 Japan 0.49 Philippines Singapore 0.37 Hong Kong 0.08 Nguyen LH, Nguyen MH. Aliment Pharmacol Ther 2013;37:921 36

8 HCV prevalence and genotype in Asia, Australia and Egypt GT1 GT2 GT3 GT4 GT5 GT6 GT 1: Australia, China, Taiwan and North Asia GT 2: Japan, Korea and Taiwan GT 3: India and Pakistan GT 4: Middle Eastern countries such as Egypt, Saudi Arabia and Syria GT 5: rare in Asia; small number in Syria GT 6: Vietnam and other Southeast Asia Sievert W, et al. Liver Int 2011;31 Suppl 2:61 80
9 HCV in China Incidence 1-1.9% ~13 million people, more than the whole of Europe and the Americas Genotype distribution: GT 1: 67.6% GT 2: 14.4% GT 3: 4.3% GT 6: 13% Others: 0.7% Sievert W, et al. Liver Int 2011;31 Suppl 2:61 80
10 Limitations of epidemiological data Reliable reports on new infections are rare, dependent on the size of the population Considerable variability in the type and quality of prevalence studies among the countries Australia, Egypt and Taiwan have large population studies, while data from other countries, like India and China, only have studies in subgroups Over-representation among men in studies from Egypt, Saudi Arabia and Pakistan make estimates for women less certain Accurate data from individual countries is crucial to developing effective preventive measures Sievert W, et al. Liver Int 2011;31 Suppl 2:61 80
11 Wide variability in prevalence due to variety of risk factors: Egypt Previous use of IV injections for schistosomiasis Pakistan Public shaving of beards and other body hair Tattooing, sexually transmitted HCV infection, acupuncture Japan blood transfusion (before screening), resulting in the bulk of HCV infection in older patients Australia Intravenous drug use most common route Sievert W, et al. Liver Int 2011;31 Suppl 2:61 80
12 Risk factors in HK Study: Incidence % from blood transfusion services ~50% blood transfusion (prior to HCV screening from 1 July 1991) ~25% IV drug users Leung N et al. Intervirology 2006;49.

13 Genotype 6
14 Focus on genotype 6 First identified in SE Asia: 212 HCV blood donors from HK: GT 1a: 6.2% GT 1b: 58.8% GT 2a: 1.4% GT 2b: 1.4% GT 3a: 1.9% GT 6a: 27.0% Prescott LE et al. J Med Virol 1996; 50. Prescott LE et al. J Med Virol 1996;50:68 75
15 Focus on genotype 6 HCV genotype 6 is estimated to be as high as 50% in some regions of Southeast Asia Significantly more common in IV drug users and thalassemia major patients Chao DT et al. Aliment Pharmacol Ther 2011;34:286 96
16 Focus on genotype 6 GT 6 is unique for its extreme subtype diversity, currently 22 recognised subtypes from 6a to 6v Accurate diagnosis of GT 6 requires core sequencing assays or newer INNO-LiPA assays, as older line probe assays often mistaken as GT 1 Chao DT et al. Aliment Pharmacol Ther 2011;34:286 96
17 Phylogenetic relationships among hepatitis C genotypes and genotype 6 subtypes GT 6 shows great diversity with 22 subtypes Chao DT et al. Aliment Pharmacol Ther 2011;34:286 96
18 Genotype 6 prevalence in Southeast Asia As high as ~50% Author Country Prevalence, % Lao et al Hong Kong Nguyen et al Vietnam (south) 36 Kanistanon et al Thailand 18 Lwin et al Burma 49 Oh et al Korea 1.4 Al Namaani K, et al. Can J Gastroenterol 2013;27(1):e8 e12
19 Very high prevalence of genotype 6 variants in southern Vietnam Genotypic distribution of HCV in Ho Chi Minh City, Vietnam 25 23,6 22 Number tested = , ,4 10 8, ,3 3,2 1,8 0,7 0,2 0,2 0,4 0,1 1,2 1,5 0,5 1 0,1 0,1 0,7 1a 1b 1e 2a 2c 2i 2j 2k 6a 6c 6e 6f 6h 6k 6l 6n 6o 6p 6r 6t 256 (30.4%) 128 (15.2%) 458 (54.4%) Pham V, et al. Jpn J Infect Dis. 2011; 64(6):537 39
20 Summary Asia-Pacific region has broad representation of most of the HCV genotypes Need for: Education to prevent spread in those at risk Effective screening to accurately diagnose people who are affected **Access to simple and effective pangenotypic treatment strategies that can be applied across the region

21 HCV Treatment
22 HCV Treatment Potential sites of targets for DAAs: 1. Viral entry into hepatocytes 2. HCV replication with 10 viral proteins 3. Viral assembly and release 4. Host targets on host factors required for replication Rice CM. Topics in Antiviral Med, 2011; 19: 117
23 HCV Treatment Potential sites of targets for DAAs: 1. Viral entry into hepatocytes 2. HCV replication with 10 viral proteins 3. Viral assembly and release 4. Host targets on host factors required for replication Rice CM. Topics in Antiviral Med, 2011; 19: 117
 inhibitor - sofosbuvir, dasabuvir NS5A inhibitors - velpatasvir, ledipasvir, elbasvir, ombitasvir,")
24 Direct Acting Antivirals (DAAs) Protease inhibitors - grazoprevir, paritaprevir, simeprevir, asunaprevir RNA polymerase (NS5B) inhibitor - sofosbuvir, dasabuvir NS5A inhibitors - velpatasvir, ledipasvir, elbasvir, ombitasvir, daclatasvir
25 The Changes in SVR % in HCV Patients 6 IFN 6 m 1986
26 The Changes in SVR % in HCV Patients IFN 6 m IFN + RBV 12 m PEG 12 m PEG + RBV 12 m PI + PEG + RVB 12 m SOF + PEG + RVB 12 wk Pangenotypic 12 wk ORAL DAAs for G1 12 wk

27 Who to Treat and With What Drugs
28 AASLD and EASL Guidelines 2016 The Goal - to reduce all-cause mortality, including end-stage disease and HCC through CURE as evidenced by SVR
29 AASLD and EASL Guidelines 2016 The Goal - proven to be effective: - meta-analysis of 6 studies (n = 443) 137 pts achieved SVR 53% had cirrhosis regression risk ratio of regression 2.69 Aktar E et al. Liver International 2015; Late relapse rate over 4-5 yrs of FU 1-2% - SVR associated with reduction in HCC and liver-related mortality (RR ; ) Smith-Palmer J et al. BMC Infect Dis 2015; 15.
30 AASLD and EASL Guidelines 2016 Who to treat? - ALL patients with chronic HCV, except those with short life expectancy due to non-hcv disease(s) - Patients with end-stage liver disease due to HCV should still be treated
31 AASLD and EASL Guidelines 2016 Pre-treatment assessment - evaluation of fibrosis, by non-invasive methods, e.g., Fibroscan, non-invasive markers (APR index). For treatment strategy and screening for HCC
+ sofosbuvir (400 mg) *")
 +")
 - dasabuvir (NS5B")

32 3 Recommended Licensed Agents Harvoni: ledipasvir (90 mg)+ sofosbuvir (400 mg) * licensed by FDA on 10 Oct viekira pak: - paritaprevir (PI) + ritonavir (P450 inhibitor) + ombitasvir (NS5A inhibitor) - dasabuvir (NS5B inhibitor) * licensed by FDA on 19 Dec If patient is on other drugs, check:
33 3 Recommended Licensed Agents Zapatier: grazoprevir (PI) + elbasvir (NS5A inhibitor) Grazoprevir 100mg Elbasvir 50 mg
34 3 Recommended Licensed Agents Zapatier: grazoprevir (PI) + elbasvir (NS5A inhibitor) Grazoprevir 100mg Elbasvir 50 mg * licensed by FDA on 28 Jan 2016 Screening for resistance-associated variants (RAV) recommended before treatment.
35 Recommended Treatment for GT1 a & b Harvoni (ledipasvir + sofosbuvir ) viekira pak (paritaprevir + ritonavir + ombitasvir, and dasabuvir ) Zapatier (grazoprevir + elbasvir) 12 weeks 12 weeks 12 weeks (without RAV) 16 weeks (with RAV for GT!a) Recommended Treatment for GT4 Same 3 combinations, all for 12 weeks
36 Recommended Treatment for GT2 Sofosbuvir + ribavirin (RBV) Daclatasvir + sofosbuvir 12 weeks 12 weeks Recommended Treatment for GT3 Daclatasvir + sofosbuvir Sofosbuvir + RBV + PEG IFN 12 weeks 12 weeks Recommended Treatment for GT5/6 Harvoni (ledipasvir + sofosbuvir ) 12 weeks

37 As-Yet-Unlicensed Pangenotypic Drug
38 Sofosbuvir + Velpatasvir SOF Nucleotide polymerase inhibitor Sofosbuvir (SOF) Potent antiviral activity against HCV GT 1 6 Once-daily, oral, 400-mg tablet SOF VEL NS5A inhibitor VEL Velpatasvir (VEL; GS-5816) Picomolar potency against GT 1 6 Second generation inhibitor with improved resistance profile SOF/VEL FDC Once daily, oral, FDC (400/100 mg)
39 Velpatasvir (VEL) HCV NS5A inhibitor Potent pangenotypic antiviral activity High barrier to resistance in vitro EC 50 Values in HCV Genotype 1-6 Replicons, nm 1a 1b 2a 2a* 2b 3a 4a 5a 6a 6e Cheng, EASL, 2013, Poster #1191
40 Velpatasvir (VEL) HCV NS5A inhibitor Potent pangenotypic antiviral activity High barrier to resistance in vitro EC 50 Values in HCV Genotype 1-6 Replicons, nm 1a 1b 2a 2a* 2b 3a 4a 5a 6a 6e Cheng, EASL, 2013, Poster #1191

41 VEL: Activity Against NS5A RAVs (resistance-associated variants) EC 50 versus genotype 1 RAPs and RAVs EC 50 versus genotypes 2 and 3 RAPs and RAVs Cheng, EASL, 2013, Poster #1191

42 VEL: Activity against other DAA RAVS RAVs of other DAAs including NS3/4a protease inhibitor RAV R155K or D1687, and NS5B RAV S282T Cheng, EASL, 2013, Poster #1191

43 The ASTRAL Studies
44 Available at
45 Study Design: ASTRAL-1 Week 0 Week 12 Week 24 n=500 SOF/VEL SVR12 n=100 Placebo SVR12 5:1 randomization to SOF/VEL or placebo Stratified by HCV genotype and cirrhosis (presence/absence) GT 5 patients not randomized Conducted at 81 sites in US, Canada, UK, Germany, France, Italy, Belgium, and Hong Kong
46 Demographics: ASTRAL-1 Placebo n=116 SOF/VEL n=624 Mean age, y (range) 53 (25 74) 54 (18 82) Male, n (%) 68 (59) 374 (60) White, n (%) 90 (78) 493 (79) Mean BMI, kg/m 2 (range) 26 (18 40) 27 (17 57) US enrolled, n (%) 45 (39) 234 (38) Cirrhosis, n (%) 21 (18) 121 (19) Treatment experienced*, n (%) 33 (28) 201 (32) IL28B CC, n (%) 36 (31) 186 (30) Median HCV RNA, log 10 IU/mL (range) 6.4 ( ) 6.4 ( ) *Includes peg-ifn + RBV failures and PI + peg-ifn + RBV failures.
 118 (19) GT 2 21 (18) 104 (17) GT 4 22 (19) 116 (19) GT 5* 0 35 (6) GT 6 8 (7) 41 (7) *All enrolled to SOF/VEL group.")
47 HCV Genotype Distribution: ASTRAL-1 Patients, n (%) Placebo n=116 SOF/VEL n=624 GT 1 65 (56) 328 (53) 1a 46 (40) 210 (34) 1b 19 (16) 118 (19) GT 2 21 (18) 104 (17) GT 4 22 (19) 116 (19) GT 5* 0 35 (6) GT 6 8 (7) 41 (7) *All enrolled to SOF/VEL group.
48 SVR12 (%) Results: SVR Total 1a 1b Genotype
49 SVR12 (%) Results: SVR12 by Genotype Total 1a 1b Genotype
50 SVR12 (%) Results: SVR12 by Genotype relapse 2 lost to follow-up 1 withdrew consent relapse 1 death Total 1a 1b Genotype
51 SVR12 (%) Results: SVR12 by Cirrhosis or Prior Treatment Total No Yes Naïve Experienced Cirrhosis Status Treatment History 51
52 Results: Resistance Analysis (1% cut-off) Total, n= % SVR12 359/359 58% No BL NS5A RAVs n=359 42% BL NS5A RAVs n=257 99% SVR12 255/257
53 Results: Safety A 55 year old white male died in his sleep 8 days Placebo after completing SOF/VEL treatment. The death was assessed Patients, as unrelated n (%) to study n=116 drug by the investigator n=624 AE 89 (77) 485 (78) Grade 3 4 AE 1 (<1) 18 (3) Adverse Events Serious AE 0 15 (2) D/C due to AE 2 (2) 1 (<1) Death 0 1 (<1) Laboratory Abnormalities Grade (12) 45 (7) Hb <10 g/dl 0 2 (<1) Hb <8.5 g/dl year-old white male died in sleep 8 days after completing treatment; death assessed as unrelated to study drug by investigator
54 Conclusions: ASTRAL-1 SOF/VEL for 12 weeks resulted in a 99% SVR12 rate in patients with HCV GT 1, 2, 4, 5, or 6 infection 99% SVR12 rate in patients with cirrhosis 99% SVR12 rate in patients with prior treatment failure Presence of baseline NS5A RAVs did not impact SVR12 SOF/VEL for 12 weeks had a safety profile similar to that of placebo treatment

55 ASTRAL-3 Study
56 Study Design: ASTRAL-3 Week n=250 SOF/VEL SVR12 n=250 SOF + RBV SVR12 1:1 randomization to SOF/VEL or SOF + RBV Stratified by prior treatment (TN/TE) and cirrhosis (presence/absence) Conducted at 76 sites in US, Canada, UK, Germany, France, Italy, Australia, and New Zealand
57 SVR12 (%) Results: SVR12 p < / /275 SOF/VEL 12 Weeks SOF + RBV 24 Weeks
58 SVR12 (%) SVR12 by Cirrhosis or Treatment History SOF/VEL SOF + RBV No Yes Naïve Experienced Cirrhosis Status Treatment History
59 Results: Resistance Analysis Total, n=274 97% SVR12 84% No BL NS5A RAVs n=231 16% BL NS5A RAVs n=43 88% SVR12 225/231 38/43 SVR12 was 84% (21/25) in patients with Y93H 59
60 Conclusions: ASTRAL-3 SOF/VEL for 12 weeks resulted in a 95% SVR12 rate in patients with HCV GT 3 infection Statistically superior to SOF + RBV for 24 weeks (p <0.001) 91% SVR12 rate in patients with cirrhosis SOF/VEL was well tolerated and, compared with SOF + RBV, lacked toxicities commonly associated with RBV
61 SVR12 (%) Pooled Data ASTRAL 1,2,3 SOF/VEL SVR for 12 Weeks GT 1 GT 2 GT 3 GT 4 GT 5 GT 6 Total

62 ASTRAL- 4 Study
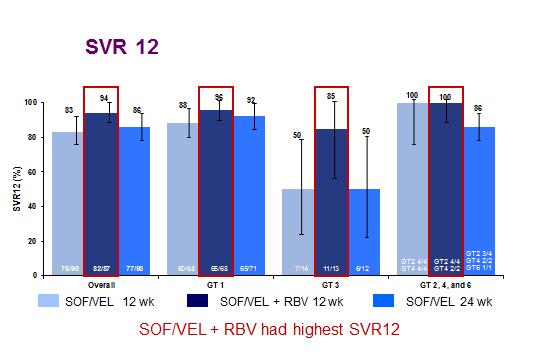
63 SOF/VEL ± RBV in Decompensated Liver Disease: GT 1, 2, 3, 4, 6 Week n=90 n=87 n=90 SOF/VEL SOF/VEL + RBV SOF/VEL RBV was weight-based (1000 or 1200 mg daily) Patients SOF/VEL 12 weeks n=90 SOF/VEL+RBV 12 weeks n=87 SOF/VEL 24 weeks n=90 Median MELD (range) 10 (6 24) 10 (6 18) 11 (6 19) MELD < 15, n (%) 86 (96) 83 (95) 85 (84) CTP B, n (%) 86 (96) 77 (89) 77 (86) Ascites, n (%) 74 (82) 65 (75) 75 (83) Encephalopathy, n (%) 52 (58) 54 (62) 59 (66)
64
65 Patients (%) Patients (%) MELD Change from Baseline to Follow Up Week % Improved 27% Worsened Baseline MELD <15 n=208 Change in MELD n= <1 < % Improved 8% Worsened 27 Baseline MELD >15 n= n= Change in MELD

66 Treatment for HCV Patients With Renal Impairment
67 Patients with Creatinine Cl ml/min No dose adjustment required with recommended agents Patients with Creatinine Cl <30 ml/min For GT 1a, 1b and 4: - viekira pak 12 weeks - Zapatier 12 weeks

68 Conclusions
69 Conclusions A substantial proportion of the world s HCV population resides in Asia Public education in prevention and diagnosis, AND greater availability of DAA treatment are urgently required
70 Conclusions SVR has improved from 6% in 1986 to % in 2016 Many DAA combinations can cure genotype 1 and 4 in 12 (-16) weeks Pangenotypic DAA will soon be available
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
The ASTRAL Program Abstracts LB-2, LB-12, 205, 209
 The ASTRAL Program Abstracts LB-2, LB-12, 5, 9 The ASTRAL Program FDC 1. 2. 3. 4. 5. SOF Nucleotide polymerase inhibitor VEL NS5A inhibitor ASTRAL1 GT1, 2, 4 6 ASTRAL2 GT2 Jacobson IM, et al. N Engl J
The ASTRAL Program Abstracts LB-2, LB-12, 5, 9 The ASTRAL Program FDC 1. 2. 3. 4. 5. SOF Nucleotide polymerase inhibitor VEL NS5A inhibitor ASTRAL1 GT1, 2, 4 6 ASTRAL2 GT2 Jacobson IM, et al. N Engl J
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Need to Assess HCV Resistance to DAAs: Is it Useful and When?
 Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
SURVEYOR-II Part 2 Study Design
 HIGH SVR RATES WITH + CO-ADMINISTERED FOR 8 WEEKS IN NON-CIRRHOTIC PATIENTS WITH HCV GENOTYPE 3 INFECTION A.J. Muir, S. Strasser, S. Wang, S. Shafran, M. Bonacini, P. Kwo, D. Wyles, E. Gane, S.S. Lovell,
HIGH SVR RATES WITH + CO-ADMINISTERED FOR 8 WEEKS IN NON-CIRRHOTIC PATIENTS WITH HCV GENOTYPE 3 INFECTION A.J. Muir, S. Strasser, S. Wang, S. Shafran, M. Bonacini, P. Kwo, D. Wyles, E. Gane, S.S. Lovell,
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
Phase 3. Treatment Experienced. Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2. Afdhal N, et al. N Engl J Med. 2014;370:
 Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Sofosbuvir-Velpatasvir-Voxilaprevir in DAA-Experienced GT 1-6 POLARIS-4
 Phase 3 Treatment Experienced Sofosbuvir-Velpatasvir-Voxilaprevir in DAA-Experienced GT 1-6 POLARIS-4 Bourlière M, et al. N Engl J Med. 217;376:2134-46. POLARIS-4: Study Features POLARIS-4 Trial Design:
Phase 3 Treatment Experienced Sofosbuvir-Velpatasvir-Voxilaprevir in DAA-Experienced GT 1-6 POLARIS-4 Bourlière M, et al. N Engl J Med. 217;376:2134-46. POLARIS-4: Study Features POLARIS-4 Trial Design:
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Hepatitis C: The New World of Treatment
 Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Hepatitis C: The New World of Treatment Aban 1395, NIOC Hospital Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences 1 Drugs NS5B polymerase
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano. Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future
 Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
HCV Treatment in 2016: Genotypes 1, 2, and 3. Cody A. Chastain, MD October 12, 2016
 HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute
 Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute Paris, January 12, 215 Disclosures Investigator, speaker, and advisory board member for: Roche, MSD, BMS, Gilead, Janssen,
Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute Paris, January 12, 215 Disclosures Investigator, speaker, and advisory board member for: Roche, MSD, BMS, Gilead, Janssen,
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
Management of HIV/HCV Coinfection. Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY
 Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Management of HIV/HCV Coinfection Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, NY Disclosure Dr. Marks has received grants and research support from Gilead Sciences
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
What do we need to know about RAVs clinically?
 14 th European HIV & Hepatitis Workshop Rome, 25-27 May, 2016 What do we need to know about RAVs clinically? Stefan Zeuzem, MD University of Frankfurt Germany Background Resistance associated variants
14 th European HIV & Hepatitis Workshop Rome, 25-27 May, 2016 What do we need to know about RAVs clinically? Stefan Zeuzem, MD University of Frankfurt Germany Background Resistance associated variants
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
New Treatments for HCV: Perspective From Asia
 REVIEW New Treatments for HCV: Perspective From Asia Ming-Lung Yu, M.D., Ph.D.,*, Wan-Long Chuang, M.D., Ph.D.*, Introduction The prevalence and number of people with antibodies to hepatitis C virus (anti-hcv)
REVIEW New Treatments for HCV: Perspective From Asia Ming-Lung Yu, M.D., Ph.D.,*, Wan-Long Chuang, M.D., Ph.D.*, Introduction The prevalence and number of people with antibodies to hepatitis C virus (anti-hcv)
Case. 63 year old woman now with:
 Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
Case 63 year old woman now with: HCV GT 1b, HCV RNA 6.2 x 10 6 IU/mL Asymptomatic except for fatigue Normal exam ALT 72 IU/mL, Bili 0.9 mg/dl, INR 1.1, Albumin 3.9 g/dl, Creatinine 0.7 mg/dl Normal EGD
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy
 Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
HCV Treatment in 2016
 HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
ICVH 2016 Oral Presentation: 28
 Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Ledipasvir/Sofosbuvir Is Safe and Effective for the Treatment of Patients with Genotype 1 Chronic HCV Infection in Both HCV Mono- and HIV/HCV Coinfected Patients A Luetkemeyer 1, C Cooper 2, P Kwo 3, K
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Hepatitis C: New Therapies in
 Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Azienda ULSS12 Veneziana
 Azienda ULSS12 Veneziana Risultati del trattamento dei monoinfetti con Sofosbuvir, Simeprevir nella coorte veneziana. Confronto di esito con la coorte del trattamento con Boceprevir e Telaprevir Dr.ssa
Azienda ULSS12 Veneziana Risultati del trattamento dei monoinfetti con Sofosbuvir, Simeprevir nella coorte veneziana. Confronto di esito con la coorte del trattamento con Boceprevir e Telaprevir Dr.ssa
Management of HCV in Prior Treatment Failure
 Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HCV Resistance Associated variants: impact on chronic hepatitis C treatment
 HCV Resistance Associated variants: impact on chronic hepatitis C treatment Dr. Stéphane Chevaliez Associate Professor of Medicine at the University of Paris-Est. History of Resistance in HCV Concern Only
HCV Resistance Associated variants: impact on chronic hepatitis C treatment Dr. Stéphane Chevaliez Associate Professor of Medicine at the University of Paris-Est. History of Resistance in HCV Concern Only
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
Hepatitis C Update: Screening, Diagnosis, and Treatment
 Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World
 Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Treating Hepatitis C-HIV Coinfected Patients Welcome to the Real World H. Nina Kim, MD MSc Associate Professor of Medicine University of Washington Division of Allergy & Infectious Diseases April 21, 2017
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Update on Hepatitis C. Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017
 Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
NS5A inhibitors: ideal candidates for combination?
 NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
Virological tools for hepatitis C: re-treatment and resistance. Joop Arends Will Irving. by author
 Virological tools for hepatitis C: re-treatment and resistance Joop Arends Will Irving Disclosures Joop Arends Advisory board: Gilead, Abbvie, Janssen, MSD, BMS (research) grants: Abbvie, BMS, MSD and
Virological tools for hepatitis C: re-treatment and resistance Joop Arends Will Irving Disclosures Joop Arends Advisory board: Gilead, Abbvie, Janssen, MSD, BMS (research) grants: Abbvie, BMS, MSD and
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Management of Chronic HCV 2017 and Beyond
 Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
How to optimize treatment for HCV Genotype 4
 How to optimize treatment for HCV Genotype 4 Paris Hepatitis Conference Pr Tarik Asselah 14 janvier 2014 MD, PhD Service d Hépatologie & INSERM U773 University Paris Diderot Hôpital Beaujon, Clichy tarik.asselah@bjn.aphp.fr
How to optimize treatment for HCV Genotype 4 Paris Hepatitis Conference Pr Tarik Asselah 14 janvier 2014 MD, PhD Service d Hépatologie & INSERM U773 University Paris Diderot Hôpital Beaujon, Clichy tarik.asselah@bjn.aphp.fr
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Patients with compensated cirrhosis: how to treat and follow-up
 Patients with compensated cirrhosis: how to treat and follow-up Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Universitätsklinikum Leipzig Leber- und Studienzentrum
Patients with compensated cirrhosis: how to treat and follow-up Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Universitätsklinikum Leipzig Leber- und Studienzentrum
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Treating HCV Prior to Liver Transplantation. What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona
 Treating HCV Prior to Liver Transplantation What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona Disclosures Unrestricted Grant Support: Janssen and Abbvie
Treating HCV Prior to Liver Transplantation What Are the Treatment Options? Xavier Forns Liver Unit Hospital Clinic, CIBEREHD, IDIBAPS Barcelona Disclosures Unrestricted Grant Support: Janssen and Abbvie
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients. Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London
 Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Hepatitis B and Hepatitis C Virus in non-liver Transplant Recipients Karim Qumosani MD, FRCPC, ABIM, MdMEd Multi-organ Transplant Unit, London Financial Disclosures Research Grants Merck, Gilead, Abbvie,
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
HEPATITIS WEB STUDY. Treatment of Hepatitis C following Liver Transplantation
 HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
HEPATITIS WEB STUDY Treatment of Hepatitis C following Liver Transplantation Terry D. Box, MD Associate Professor of Medicine Division of Gastroenterology/Hepatology University of Utah Health Sciences
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
Hepatitis C Medications Prior Authorization Criteria
 Hepatitis C Medications Authorization Criteria Epclusa (/velpatasvir), Harvoni (ledipasvir/), Sovaldi (), Daklinza (daclatasvir), Zepatier (elbasvir/grazoprevir), Olysio (simeprevir), Viekira Pak (ombitasvir/paritaprevir/ritonavir;
Hepatitis C Medications Authorization Criteria Epclusa (/velpatasvir), Harvoni (ledipasvir/), Sovaldi (), Daklinza (daclatasvir), Zepatier (elbasvir/grazoprevir), Olysio (simeprevir), Viekira Pak (ombitasvir/paritaprevir/ritonavir;
Expert Perspectives: Best of HCV from EASL 2015
 Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York
 Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Newly Approved Hepatitis C Virus Drugs: Approach to Initial Therapy Kristen M. Marks, MD Assistant Professor Weill Cornell Medical College New York, New York Learning Objectives After attending this presentation,
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Current HCV Treatment by Genotype Ira M. Jacobson, MD
 Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
Current HCV Treatment by Genotype Ira M. Jacobson, MD Director of Hepatology NYU School of Medicine Objectives To understand the prevalence of HCV and distribution of HCV genotypes Describe the HCV lifecycle
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
Cases: Management of Hepatitis C in Prior Treatment Failure
 Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Cases: Management of Hepatitis C in Prior Treatment Failure David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After
Treating Hepatitis C in Patients with Advanced Renal Disease
 Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Direct Acting Antivirals for the Treatment of Hepatitis C Infection
 Hepatitis C Core Curriculum, Module 2 Direct Acting Antivirals for the Treatment of Hepatitis C Infection Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Objectives Discuss the evolution of hepatitis C treatment
Hepatitis C Core Curriculum, Module 2 Direct Acting Antivirals for the Treatment of Hepatitis C Infection Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Objectives Discuss the evolution of hepatitis C treatment
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Virological assessment of patients candidate to DAA
 Virological assessment of patients candidate to DAA Patients characteristics Italian male patient Diagnosis of chronic HCV infection in 1994 Genotype 1b defined in 1998 Non-responder to IFN+RBV He developed
Virological assessment of patients candidate to DAA Patients characteristics Italian male patient Diagnosis of chronic HCV infection in 1994 Genotype 1b defined in 1998 Non-responder to IFN+RBV He developed
Management of HCV in Decompensated Liver Disease
 Management of HCV in Decompensated Liver Disease Michael P. Manns Hannover Medical School (MHH) Department of Gastroenterology, Hepatology and Endocrinology Helmholtz Center for Infection Research (HZI),
Management of HCV in Decompensated Liver Disease Michael P. Manns Hannover Medical School (MHH) Department of Gastroenterology, Hepatology and Endocrinology Helmholtz Center for Infection Research (HZI),
Treatment of Hepatitis C with sofosbuvir/ledipasvir (Harvoni )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient. Konstantin Zhdanov
 Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Terapie attuali. Eradicazione di HCV e nuove prospettive:
 Eradicazione di HCV e nuove prospettive: Terapie attuali Luisa Pasulo U.S.C. Gastroenterologia Epatologia e Trapiantologia Ospedale Papa Giovanni XXIII - Bergamo From Infection to liver disease Infezione
Eradicazione di HCV e nuove prospettive: Terapie attuali Luisa Pasulo U.S.C. Gastroenterologia Epatologia e Trapiantologia Ospedale Papa Giovanni XXIII - Bergamo From Infection to liver disease Infezione
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Epclusa) Reference Number: CP.CPA.286 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Epclusa) Reference Number: CP.CPA.286 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
New York State HCV Provider Webinar Series. Side Effects of Therapy
 New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related