Arvind R. Murali, MD Assistant Professor of Medicine Gastroenterology & Hepatology Organ Transplant Center UIHC, Carver College of Medicine
|
|
|
- Briana Jones
- 5 years ago
- Views:
Transcription

1 Arvind R. Murali, MD Assistant Professor of Medicine Gastroenterology & Hepatology Organ Transplant Center UIHC, Carver College of Medicine
2 No financial disclosures No conflicts of interest No affiliations with any pharmaceutical company Recommendations on HCV treatment regimens are based on AASLD/IDSA guidelines

3 Epidemiology of HCV infection Who to screen for HCV infection? Clinical Manifestations of HCV Factors influencing treatment of HCV Treatment of HCV HCV in pregnancy Acute HCV infection

4 56 yo male with past history of HCV infection is referred to you for evaluation. Hepatitis C antibody test is positive AND hepatitis C RNA test is negative. What is the next step? a. Start Sofosbuvir-Ledipasvir for 12 weeks b. Start Sofosbuvir and ribavirin for 24 weeks c. Check hepatitis C genotype to help determine anti-viral regimen d. No evidence of current HCV infection and no treatment is required
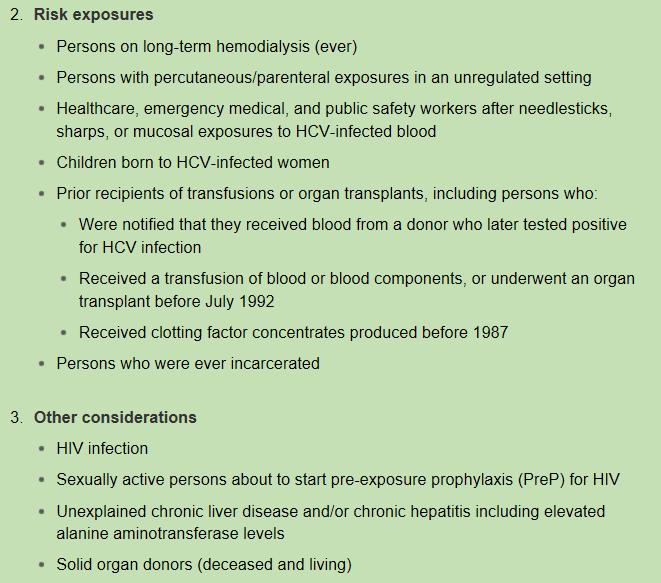
5 All but which of the following patients should be offered one-time HCV testing? a. All persons born between 1965 and 1985 b. 45-yo male using intravenous drugs c. 55 yo female on maintanence hemodialysis d. Child born to a HCV-infected mother
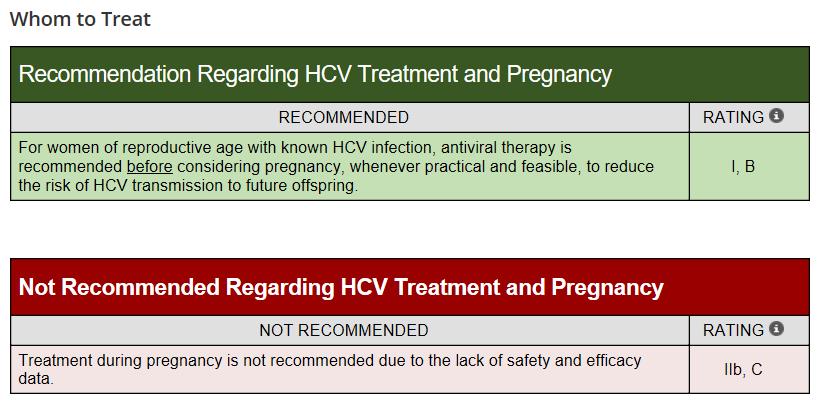
6 A 26 year old pregnant woman at 28 weeks gestational age is noted to have positive hepatitis C RNA. HCV genotype is 1b. What is your next step in management? a. Start elbasvir/grazoprevir for 12 weeks b. Start glecaprevir/pibrentasvir for 8 weeks c. Start sofosbuvir/velpatasvir for 12 weeks d. Treatment is not recommended during pregnancy
7 You see a 55 yo old male with history of IVDU in your clinic. HCV antibody is positive and HCV PCR indicates high viral load. You obtain a liver ultrasound which shows a 2cm liver lesion. What do you do next? 1. Repeat Ultrasound in 6 months. 2. Start treatment for hepatitis C. 3. Obtain MRI and if suggestive of HCC refer to a transplant center. 4. Start treatment for HCV, obtain MRI, and refer to a transplant center.
8 HCV - One of the main causes of chronic liver disease worldwide Long-term impact of HCV infection on liver disease is highly variable ranging from minimal histological changes extensive fibrosis and cirrhosis hepatocellular carcinoma (HCC)
9 About 180 million chronically infected persons worldwide An estimated 3.5 million persons in the United States are HCV-infected 2.7 million in the general non-institutionalized population 800,000 - incarcerated, institutionalized, or homeless Most people infected with HCV are unaware of their infection - In the US, about half of all infected people are unaware they are infected
10
11
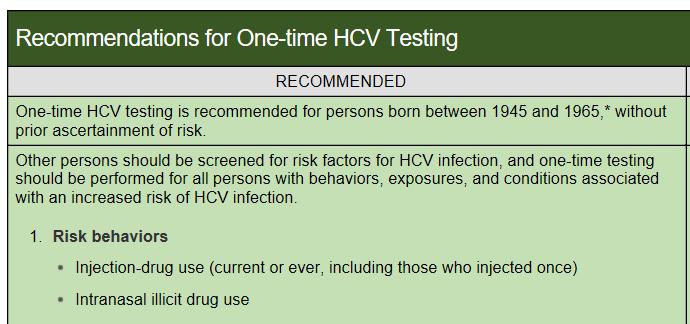
12 In 2012, CDC recommended to offer a one-time HCV test to all persons born from 1945 through 1965, without prior ascertainment of HCV riskfactors. Reasoning? Persons in the 1945 to 1965 birth cohort accounted for nearly three-fourths of all HCV infections, a five-time higher HCV prevalence (3.25%)
13
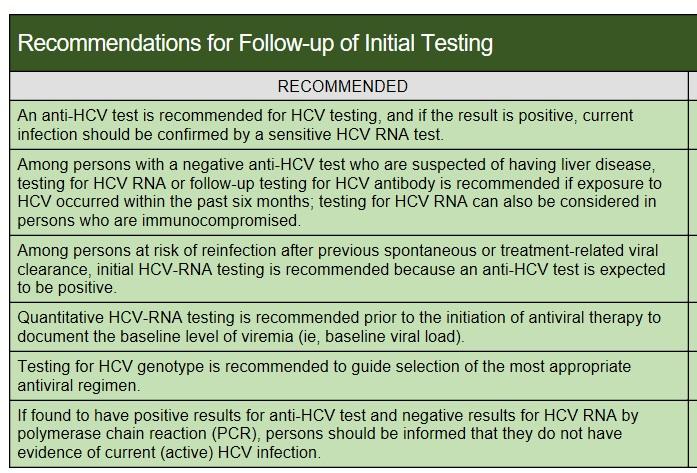
14 All persons requiring HCV testing should first be tested for HCV antibody (anti-hcv) using an FDAapproved test A positive test result for anti-hcv usually but not always imply current infection Positive HCV antibody test indicates either current (active) HCV infection (acute or chronic) past infection that has resolved, or a false-positive test result
15 All patients with HCV antibody positive HCV nucleic acid test (NAT) to detect viremia to confirm current (active) HCV infection In patients with negative anti-hcv ab test but are immunocompromised (HIV, chronic hemodialysis) exposure to HCV within the last six months To detect re-infection in persons after previous spontaneous or treatment-related viral clearance Get HCV RNA directly in these patients
16 An FDA-approved quantitative or qualitative NAT with a detection level of 25 IU/mL or lower should be used to detect HCV RNA Positive HCV viral load confirms current infection Positive anti-hcv test and negative HCV RNA PCR No evidence of current (active) HCV infection, additional HCV testing is typically unnecessary Only when there is a high index of suspicion for recent infection, HCV RNA test can be repeated (3-6 months)
17 Hepatic Acute hepatitis, cirrhosis, HCC Non-hepatic manifestations Mixed Cryoglobulinemic Syndrome B-Cell Non-Hodgkins Lymphoma Type 2 MPGN Sicca Syndrome Porphyria Cutanea Tarda Lichen Planus Moorens Corneal Ulcers
18 MCS is a small to medium vessel vasculitis characterized by production of cryoglobulins Cryoglobulins - immune complexes of polyclonal immunoglobulin (Ig)G and monoclonal or polyclonal IgM with rheumatoid factor that precipitate at lower temperatures Fix complement - lead to endothelial tissue damage and vasculitis As high as 90 % of cases of MCS are associated with chronic HCV

19 Dermatological manifestations palpable purpura Other manifestations Arthritis Non-healing ulcers Peripheral neuropathy Central nervous involvement, and Glomerulonephritis Diagnosis confirmed by the presence of - cryoglobulins - elevated rheumatoid factor & - immunofluorescence of complement fixing IgM in tissues
20 HCV RNA viral load HCV genotype Co-existing HIV infection Co-existing Hepatitis B infection Presence or absence of cirrhosis If cirrhosis, compensated or decompensated Do they have CKD/ESRD Presence of HCC Transplant Candidate
21 There are currently 11 different genetic strains (genotypes) of hepatitis C virus (HCV) in the world Highest prevalence is seen with genotypes 1 through 7 Testing for HCV genotype helps to guide selection of the most appropriate treatment regimen
22 Genotype 1 is the most common HCV genotype in North America and Europe Accounts for nearly 80% of all infections in the U.S HCV genotype 1 - subtypes 1a, 1b, and 1c Genotype 2 is the second most common HCV genotype in the U.S. About 10% of all infection Genotype 2 - subtypes 2a, 2b, and 2c
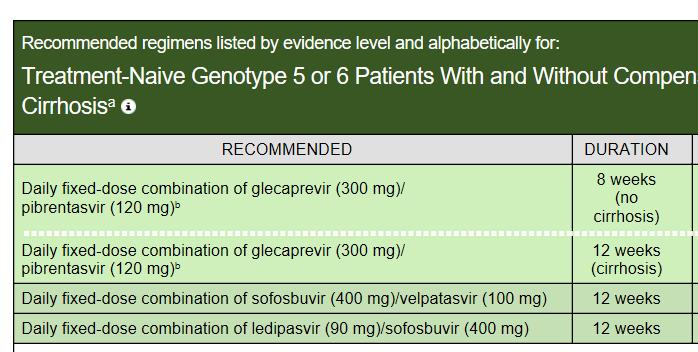
23 Genotype 3 endemic to southeast Asia and some parts of Australia, and India HCV genotype 3 - about 6% of Americans Genotype 3 - two main subtypes: 3a and 3b Genotype 4 - Africa, Middle East, Egypt Genotype 5 Southern Africa Genotype 6 China, Hong Kong Genotype 7 Thailand, Congo
24 All patients considered for HCV treatment must have testing hepatitis B surface antigen and surface antibody hepatitis B core antibody HbsAg positive treat HBV prior to starting HCV treatment HbsAg and HbsAb are negative but HBV core Ab positive significant risk of re-activation of hepatitis B while on treatment for HCV HBV re-activation can lead to liver failure and death. 24 cases of re-activation were identified by FDA 2 deaths and 1 LT Closely monitor liver enzymes and liver function tests while on HCV treatment
25 Severity of liver disease - A key factor in determining treatment and follow up evaluation of patients with HCV Patients with advanced liver disease may have a lower response to HCV therapy but they are the most likely to derive the greatest survival benefit A liver biopsy is the gold standard in estimating the severity of liver inflammation/fibrosis but is rarely used due to risk of complications
26 Blood tests platelet count, INR, APRI index Liver imaging (eg, ultrasound, CT scan) can be used to assess liver surface nodularity and spleen size Serum fibrosis marker panels such as Fib4, Fibrospect Liver Elastography measurement (Fibroscan/US/MRI) provides instant information regarding liver stiffness can reliably distinguish patients with a high versus low likelihood of cirrhosis
27 ***If there is a liver lesion on ultrasound and HCC is suspected, do not start treatment for HCV. Patients with suspected HCC should be referred to a transplant center for evaluation and management of HCC.
28 Sustained Virological Response (virologic cure) continued absence of detectable HCV RNA for at least 12 weeks after completion of therapy SVR durable in more than 99% of patients followedup for 5 years Patients in whom SVR is achieved have HCV antibodies but no longer have detectable HCV RNA in serum, liver tissue, or mononuclear cells
29 SVR is associated with Substantial improvement in liver histology, decrease in the risk of progression to cirrhosis >70% reduction in the risk of liver cancer (hepatocellular carcinoma [HCC]) 90% reduction in the risk of liver-related mortality and liver transplantation
30 Reduces symptoms from cryoglobulinemic vasculitis, a condition affecting 10% to 15% of HCV-infected patients HCV-infected persons with non-hodgkin lymphoma and other lymphoproliferative disorders achieve complete or partial remission in up to 75% of cases Substantially improved quality of life, which spans their physical, emotional, and social health Persons who have successfully achieved SVR (virologic cure) no longer transmit the virus to others
31
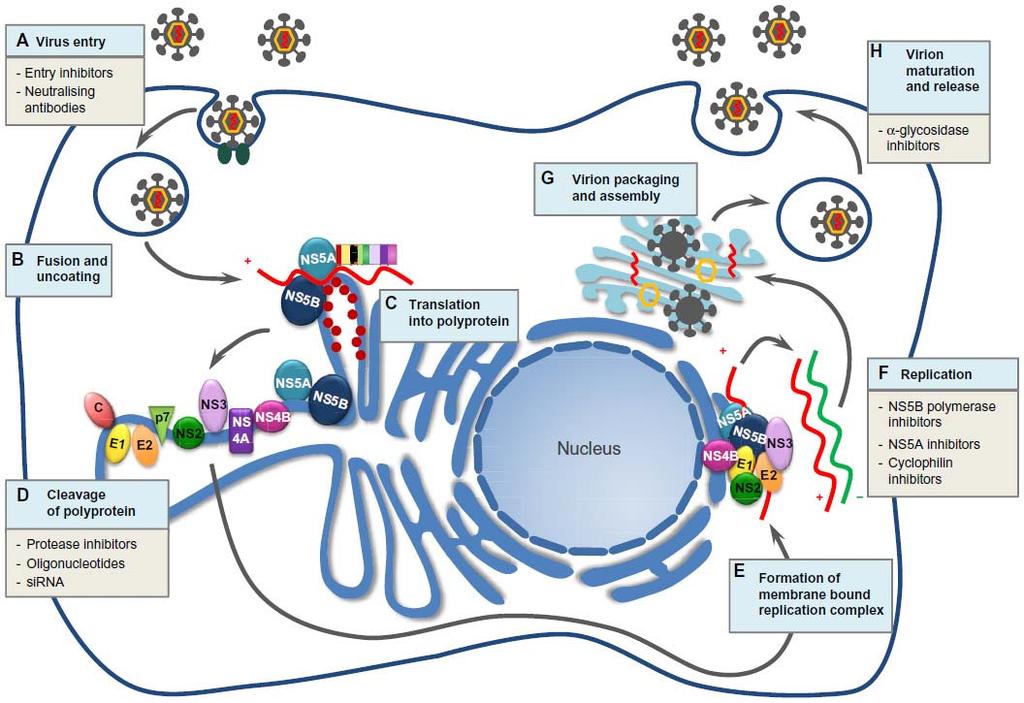
32 1. NS3/4A Protease Inhibitors - Inhibits cleavage of polyprotein - Ends with previr 2. NS5A Inhibitors - Blocks virus protein NS5A needed for virus reproduction and infection Ends with asvir 3. NS5B polymerase Inhibitors - Inhibits RNA polymerase NS5B thus preventing virus replication - Ends with buvir
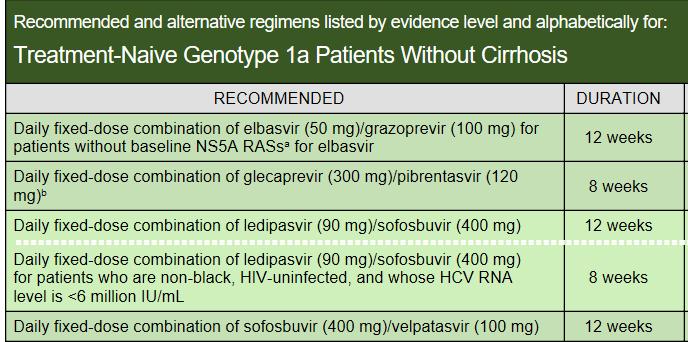
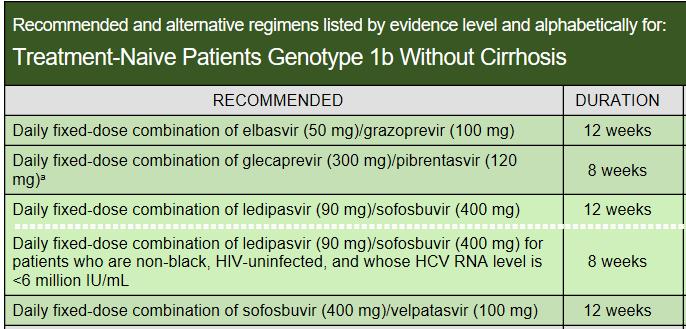
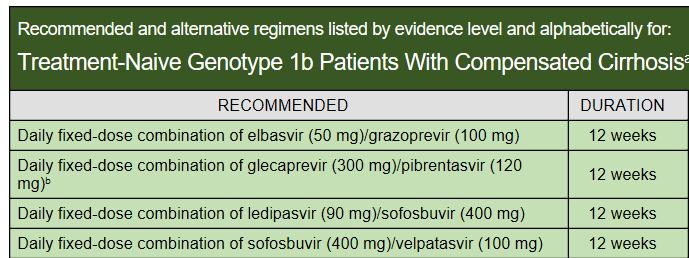
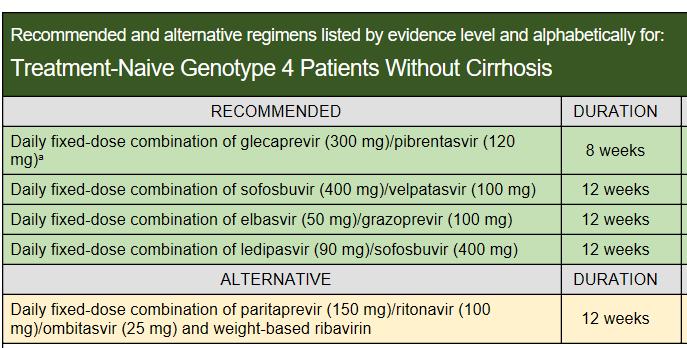
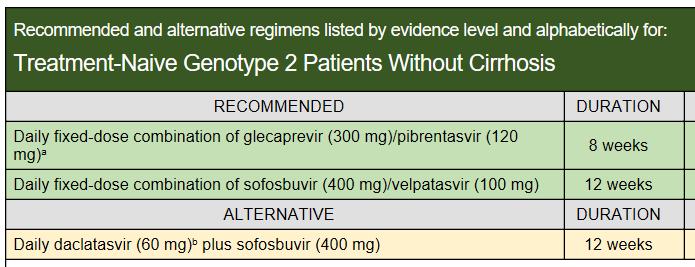
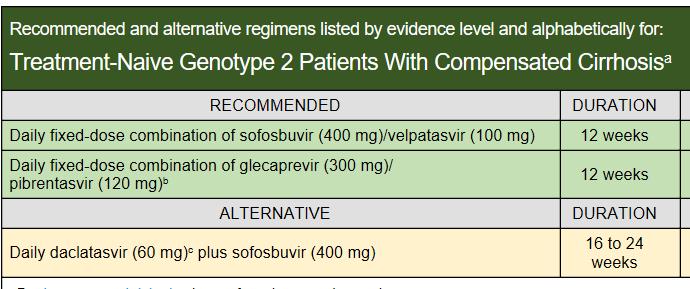
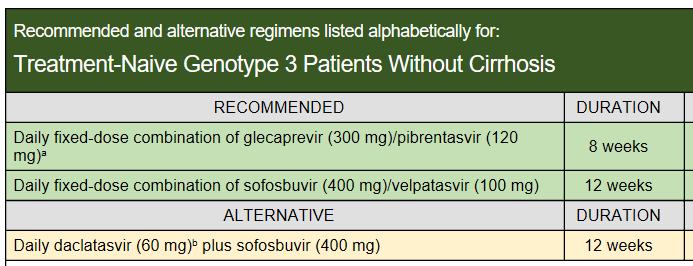
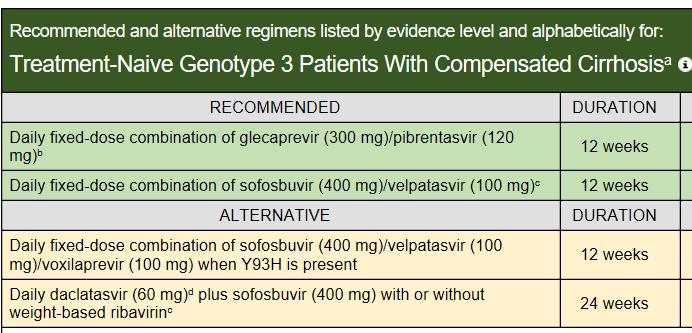
33 Elbasvir-Grazoprevir (Zepatier) Genotypes 1, 4 (12 weeks *no cirrhosis/comp cirrhosis) Ledipasvir-Sofosbuvir (Harvoni) Geno 1, 4, 5, 6 (12 weeks *no cirrhosis/comp cirrhosis) Glecaprevir-Pibrentasvir (Mavyret) Geno 1-6 (8 wks no cirrhosis, 12 wks comp cirrhosis) Sofosbuvir-Velpatasvir (Epclusa) Genotypes 1-6 (12 wks *no cirrhosis/comp cirrhosis) *All treatment naïve

34
35

36
37
38
39
40
41 Treatment experienced Peg-interferon/ribavirin experienced NS3 protease inhibitor (telaprevir, boceprevir, simeprevir) NS5B inhibitors (eg: sofosbuvir) NS5A inhibitors (eg: ledipasvir, elbasvir, daclatasvir) HCV/HIV co-infection Post-Liver Transplant Chronic Kidney disease HCV in Pregnancy

42
43
44
45 Acute HCV infection - defined as presenting within 6 months of the exposure Both HCV antibody and HCV RNA testing are recommended when acute HCV infection is suspected Pre-exposure or post-exposure prophylaxis with antiviral therapy is not recommended 20% to 50% chance of spontaneous clearance of the infection in 6 months
46 Counsel patients with acute HCV infection to avoid hepatotoxic insults - hepatotoxic drugs (eg, acetaminophen) and alcohol consumption Counseling to reduce the risk of HCV transmission Referral to an addiction medicine specialist is recommended for patients with acute HCV infection related to substance use Repeat HCV RNA in 6 months to determine if spontaneous clearance of HCV has occurred If HCV RNA is persistent beyond 6 months after diagnosis of acute HCV then patient has chronic HCV and needs to be treated
47 A vast number of people infected with HCV are unaware of their infection Patients born between 1945 to 1965 should be screened for HCV even without any risk factors Patients with anti HCV antibody positive should receive HCV RNA test to confirm current infection. No treatment indicated if HCV RNA is negative Provide recommendations for counseling those with active HCV infection

48
49 Several DAA regimens are available to treat HCV. Treatment should be based on HCV viral load, genotype, presence or absence of cirrhosis and if they treatment naïve or experienced HCV treatment is recommended before considering pregnancy if possible, avoid during pregnancy 20-50% spontaneous clearance of HCV after acute infection, do not treat unless the HCV RNA is persistent at 6-12 months (chronic HCV)
50 56 yo male with past history of HCV infection is referred to you for evaluation. You obtain hepatitis C antibody test and it is positive but the hepatitis C RNA test is negative. What is the next step? a. Start Sofosbuvir-Ledipasvir for 12 weeks b. Start Sofosbuvir and ribavirin for 24 weeks c. Check hepatitis C genotype to help determine anti-viral regimen d. Inform patient that there is no evidence of current HCV infection and no treatment is required
51 All but which of the following patients should be offered one-time HCV testing? a. All persons born between 1965 and 1985 b. 45-yo male with history of intravenous drug abuse c. 55 yo female on hemodialysis d. Child born to a HCV-infected mother
52 A 26 year old pregnant woman at 28 weeks gestational age is noted to have positive hepatitis C RNA. HCV genotype is 1b. What is your next step in management? a. Start elbasvir/grazoprevir for 12 weeks b. Start glecaprevir/pibrentasvir for 8 weeks c. Start sofosbuvir/velpatasvir for 12 weeks d. Inform patient that treatment is not recommended during pregnancy due to lack of safety and efficacy data
53 You see a 55 yo old male with history of IVDU in your clinic. HCV antibody is positive and HCV PCR indicates high viral load. You obtain a liver ultrasound which shows a 2cm liver lesion. What do you do next? 1. Repeat Ultrasound in 6 months 2. Start treatment for hepatitis C and repeat Ultrasound in 3-6 months 3. Obtain MRI and if suggestive of HCC refer to a transplant center 4. Start treatment for HCV, obtain MRI, and refer to a transplant center

54
55
56 Alcohol HCV patients be counseled regarding the deleterious effects of alcohol Strong association between use of excess alcohol and the development of/progression of liver fibrosis and HCC in patients with HCV infection Daily consumption of more than 50 grams of alcohol has a high likelihood of worsening fibrosis
57 Hepatitis B virus (HBV) infection and human immunodeficiency virus-1 (HIV) co-infection - associated with poorer prognosis of HCV Persons with HCV should be tested for HIV antibody and hepatitis B surface antigen (HBsAg)/ core antibody using standard assays for screening Counseled on how to reduce their risk of acquiring these infections, including through HBV vaccination
58 Patients with obesity and metabolic syndrome having underlying insulin resistance are more prone to have nonalcoholic fatty liver disease NAFLD is a risk factor for fibrosis progression in HCV-infected persons HCV-infected persons who are overweight (BMI> 25 kg/m 2 ) or obese (BMI > 30 kg/m 2 ) be counseled regarding strategies to reduce weight and improve insulin resistance via diet, exercise, and/or medical therapies
59 Patients with HCV infection and hyperlipidemia or cardiovascular comorbidities may also benefit from various hypolipidemic drugs Prospective studies - demonstrated the safety and efficacy of statins in patients with chronic HCV even in those with compensated cirrhosis Statins and other hypolipidemic agents should not be withheld in HCV-infected patients
60 Persons with HCV infection should be counseled to avoid sharing toothbrushes and dental or shaving equipment, and be cautioned to cover any bleeding wound to prevent the possibility of others coming into contact with their blood. Persons should be counseled to stop using illicit drugs and enter substance abuse treatment. Those who continue to inject drugs should be counseled to avoid reusing or sharing syringes, needles, water, cotton, and other drug preparation equipment; use new sterile syringes and filters and disinfected cookers; clean the injection site with a new alcohol swab; and dispose of syringes and needles after one use in a safe, puncture-proof container. Persons with HCV infection should be advised not to donate blood and to discuss HCV serostatus prior to donation of body organs, other tissue, or semen. Persons with HIV infection and those with multiple sexual partners or sexually transmitted infections should be encouraged to use barrier precautions to prevent sexual transmission. Other persons with HCV infection should be counseled that the risk of sexual transmission is low and may not warrant barrier protection. Household surfaces and implements contaminated with visible blood from an HCV-infected person should be cleaned using a dilution of 1 part household bleach to 9 parts water. Gloves should be worn when cleaning up blood spills.
Hepatitis C Virus (HCV)
") Clinical Practice Guidelines Hepatitis C Virus (HCV) OBJECTIVE The purpose is to guide the appropriate diagnosis and management of Hepatitis C Virus (HCV). GUIDELINE These are only guidelines, and are
Clinical Practice Guidelines Hepatitis C Virus (HCV) OBJECTIVE The purpose is to guide the appropriate diagnosis and management of Hepatitis C Virus (HCV). GUIDELINE These are only guidelines, and are
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
SASKATCHEWAN FORMULARY BULLETIN Update to the 62nd Edition of the Saskatchewan Formulary
 April 1, 2017 Bulletin #165 ISSN 1923-0761 SASKATCHEWAN FORMULARY BULLETIN Update to the 62nd Edition of the Saskatchewan Formulary Related Information for Prescribers: Only prescribers who have completed
April 1, 2017 Bulletin #165 ISSN 1923-0761 SASKATCHEWAN FORMULARY BULLETIN Update to the 62nd Edition of the Saskatchewan Formulary Related Information for Prescribers: Only prescribers who have completed
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Brief Review of HIV and Hepatitis C Virus (HCV) Infection (with focus on HCV)
 Infection (with focus on HCV)") Brief Review of HIV and Hepatitis C Virus (HCV) Infection (with focus on HCV) James Morrill, MD, PhD MGH Charlestown HealthCare Center Massachusetts General Hospital www.mghcme.org Disclosures Neither
Brief Review of HIV and Hepatitis C Virus (HCV) Infection (with focus on HCV) James Morrill, MD, PhD MGH Charlestown HealthCare Center Massachusetts General Hospital www.mghcme.org Disclosures Neither
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure appropriate
Length of Authorization: 8-16 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
1/16/2019. Goals of HCV Therapy. Objectives. Treating Hepatitis C and HIV Co Infection. Cure Defined as sustained virologic response (SVR)
") HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
HCV ECHO WESTERN STATES HCV ECHO WESTERN STATES Treating Hepatitis C and HIV Co Infection Paulina Deming, Pharm D Associate Professor, College of Pharmacy Assistant Director, Viral Hepatitis Programs,
Commonly Asked Questions About Chronic Hepatitis C
 Commonly Asked Questions About Chronic Hepatitis C From the American College of Gastroenterology 1. How common is the hepatitis C virus? The hepatitis C virus is the most common cause of chronic viral
Commonly Asked Questions About Chronic Hepatitis C From the American College of Gastroenterology 1. How common is the hepatitis C virus? The hepatitis C virus is the most common cause of chronic viral
Outline. Updates in the Clinical Management of Hepatitis B and C. Who should be screened for HBV? Chronic Hepatitis B 10/7/2018
 Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy
 Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Hepatitis C. No disclosures. 1. The USPSTF recommends Hepatitis C screening in which patient populations?
 Hepatitis C Jennifer Acosta PA-C No disclosures 1. The USPSTF recommends Hepatitis C screening in which patient populations? a. All adults at least once b. Immigrants to the US and those over age 65 c.
Hepatitis C Jennifer Acosta PA-C No disclosures 1. The USPSTF recommends Hepatitis C screening in which patient populations? a. All adults at least once b. Immigrants to the US and those over age 65 c.
New York State HCV Provider Webinar Series. Side Effects of Therapy
 New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
New York State HCV Provider Webinar Series Side Effects of Therapy Objectives Understand the basics of HCV therapy Review the currently available regimens for treatment of HCV Appreciate side effects related
ACTIVITY DISCLAIMER. Kurt Cook, MD, MSc DISCLOSURE. Audience Engagement System. Learning Objectives
 On the Liver Disease Front Lines: Hepatitis A, B and C Prevention and Treatment Kurt Cook, MD, MSc ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family
On the Liver Disease Front Lines: Hepatitis A, B and C Prevention and Treatment Kurt Cook, MD, MSc ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family
Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18
 Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18 Overview Hepatitis C Virus Prevalence Effects of Hepatitis C Prevention Diagnosis
Hepatitis C Infection: Updated Information for Front Line Workers in Primary Care Settings MAMTA K. JAIN, MD, MPH 2/14/18 Overview Hepatitis C Virus Prevalence Effects of Hepatitis C Prevention Diagnosis
Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, :00 pm 1:00 pm
 & Infectious Disease 101 for Hubs & Spokes April 24, :00 pm 1:00 pm") Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, 2018 12:00 pm 1:00 pm Presenters: Thomas E. Freese, PhD, Larissa Mooney, MD, & Rachel McLean, MPH, Chief, Office of Viral Hepatitis
Hepatitis C Virus (HCV) & Infectious Disease 101 for Hubs & Spokes April 24, 2018 12:00 pm 1:00 pm Presenters: Thomas E. Freese, PhD, Larissa Mooney, MD, & Rachel McLean, MPH, Chief, Office of Viral Hepatitis
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: November 14, 2018 Effective Date: January 1, 2019 This drug class prior authorization criteria have been
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: November 14, 2018 Effective Date: January 1, 2019 This drug class prior authorization criteria have been
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
HEPATITIS C UPDATES. Sanaa S. Said 10 th April, 2014
 HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
Genotype 1 Treatment Naïve No Cirrhosis Options
 Genotype 1 Treatment Naïve No Cirrhosis Options Elbasvir/Grazoprevir (Zepatier ) x 12 weeks 1 Glecaprevir/Pibrentasvir (Mavyret ) x 8 weeks Ledipasvir/Sofosbuvir (Harvoni ) x 8-12 weeks 2 1 If genotype
Genotype 1 Treatment Naïve No Cirrhosis Options Elbasvir/Grazoprevir (Zepatier ) x 12 weeks 1 Glecaprevir/Pibrentasvir (Mavyret ) x 8 weeks Ledipasvir/Sofosbuvir (Harvoni ) x 8-12 weeks 2 1 If genotype
Transmission. Transmission Counseling
 Learning Objectives Upon completion, participants should be able to: Outline critical components of comprehensive care for patients with chronic HCV infection Counsel patients about reasonable expectations
Learning Objectives Upon completion, participants should be able to: Outline critical components of comprehensive care for patients with chronic HCV infection Counsel patients about reasonable expectations
WHEN HCV TREATMENT IS DEFERRED WV HEPC ECHO PROJECT
 WHEN HCV TREATMENT IS DEFERRED WV HEPC ECHO PROJECT October 13, 2016 Reminder - treatment is recommended for all patients with chronic HCV infection Except short life expectancies that cannot be remediated
WHEN HCV TREATMENT IS DEFERRED WV HEPC ECHO PROJECT October 13, 2016 Reminder - treatment is recommended for all patients with chronic HCV infection Except short life expectancies that cannot be remediated
Hepatitis C Management and Treatment
 Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
Hepatitis C Best Practice Guidelines For Local Health Departments
 Hepatitis C Best Practice Guidelines For Local Health Departments LHDs are responsible for investigating and reporting all physician reported cases of acute hepatitis C (HCV). For clients known to have
Hepatitis C Best Practice Guidelines For Local Health Departments LHDs are responsible for investigating and reporting all physician reported cases of acute hepatitis C (HCV). For clients known to have
Hepatitis C Policy Discussion
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Update: Screening, Diagnosis, and Treatment
 Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Vosevi) Reference Number: CP.HNMC.41 Effective Date: 07.26.17 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Vosevi) Reference Number: CP.HNMC.41 Effective Date: 07.26.17 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Hepatitis C Direct-Acting Antivirals
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O.
 Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Primary Care Approach to Diagnosis and Management of Chronic Hepatitis C Brian Viviano, D.O. Objectives Epidemiology of chronic hepatitis C CDC guidelines on screening or hepatitis C Diagnosing hepatitis
Length of Authorization: 8-12 weeks. Requires PA: All direct-acting antivirals for treatment of Hepatitis C. Approval Criteria
 Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C Direct-Acting Antivirals Goals: Approve use of cost-effective treatments supported by the medical evidence. Provide consistent patient evaluations across all hepatitis C treatments. Ensure
Hepatitis C in Australia:
 Hepatitis C in Australia: Epidemiology and Clinical Presentation (and a bit of virology ) A/Prof Mark Douglas Hepatitis C - Distribution Te and Jensen 2010 Clin Liver Dis Hepatitis C Epidemiology Estimated
Hepatitis C in Australia: Epidemiology and Clinical Presentation (and a bit of virology ) A/Prof Mark Douglas Hepatitis C - Distribution Te and Jensen 2010 Clin Liver Dis Hepatitis C Epidemiology Estimated
HEPATITIS C. Whitney Dickson, PharmD, BCPS October 12 th, 2017
 HEPATITIS C Whitney Dickson, PharmD, BCPS October 12 th, 2017 MY BACKGROUND Pharmacy School: University of California San Diego Pharmacy Practice Residency (PGY1): University of Illinois at Chicago HIV/Hep
HEPATITIS C Whitney Dickson, PharmD, BCPS October 12 th, 2017 MY BACKGROUND Pharmacy School: University of California San Diego Pharmacy Practice Residency (PGY1): University of Illinois at Chicago HIV/Hep
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 20 Last Review Date: March 16, 2018 Hepatitis C Agents Description
Hepatitis C Agents
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.41 Subject: Hepatitis C Agents Page: 1 of 19 Last Review Date: December 8, 2017 Hepatitis C Agents
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir) PHARMACY PRI AUTHIZATION Hepatitis C Clinical Guideline Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir) Harvoni
Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir) PHARMACY PRI AUTHIZATION Hepatitis C Clinical Guideline Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir) Harvoni
HCV Treatment in 2016: Genotypes 1, 2, and 3. Cody A. Chastain, MD October 12, 2016
 HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
HCV Treatment in 2016: Genotypes 1, 2, and 3 Cody A. Chastain, MD October 12, 2016 Disclosures I have no financial disclosures. Caveats I will only discuss treatment of GT 1-3. Majority of US population
What is Hepatitis C Virus (HCV)?
?") HEPATITIS C VIRUS (HCV) What is Hepatitis C Virus (HCV)? Hepatitis is an inflammation (swelling or tenderness) of the liver. Hepatitis C virus (HCV) is the most common form of viral hepatitis and usually
HEPATITIS C VIRUS (HCV) What is Hepatitis C Virus (HCV)? Hepatitis is an inflammation (swelling or tenderness) of the liver. Hepatitis C virus (HCV) is the most common form of viral hepatitis and usually
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Molina Healthcare of Texas Hepatitis C Drugs (Medicaid)
") Texas Standard Prior Authorization Form Addendum Molina Healthcare of Texas Hepatitis C Drugs (Medicaid) This fax machine is located in a secure location as required by HIPAA Regulations. Complete / Review
Texas Standard Prior Authorization Form Addendum Molina Healthcare of Texas Hepatitis C Drugs (Medicaid) This fax machine is located in a secure location as required by HIPAA Regulations. Complete / Review
World Health Organization. Western Pacific Region
 Basic modules for HCV 1 HCV Module 1 Hepatitis C serological markers and virology 2 HCV Markers 3 Test Anti HCV (Anti hepatitis C virus antibody) HCV RNA (quantitative or qualitative) (Nucleic acid test)
Basic modules for HCV 1 HCV Module 1 Hepatitis C serological markers and virology 2 HCV Markers 3 Test Anti HCV (Anti hepatitis C virus antibody) HCV RNA (quantitative or qualitative) (Nucleic acid test)
Hepatitis C Policy Discussion
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Management of Chronic HCV 2017 and Beyond
 Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Selecting HCV Treatment
 Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
Selecting HCV Treatment Caveats Focus on treatment selection for genotypes 1, 2, and 3. Majority of US population infected with GT 1, 2, or 3 GT 4 treatment closely reflects GT 1 treatment GT 5 and 6 are
All Hands on Deck: Taking on Hepatitis C in Tennessee
 All Hands on Deck: Taking on Hepatitis C in Tennessee Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
All Hands on Deck: Taking on Hepatitis C in Tennessee Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Sovaldi (sofosbuvir)
") Market DC Sovaldi (sofosbuvir) Override(s) Prior Authorization Quantity Limit Approval Duration Based on Genotype, Treatment status, Cirrhosis status, or Ribavirin Eligibility status **IN, SC, WA Medicaid
Market DC Sovaldi (sofosbuvir) Override(s) Prior Authorization Quantity Limit Approval Duration Based on Genotype, Treatment status, Cirrhosis status, or Ribavirin Eligibility status **IN, SC, WA Medicaid
Hepatitis C Update on New Treatments
 Hepatitis C Update on New Treatments Kevork M. Peltekian, MD, FRCPC 44th Annual Dalhousie Spring Refresher Course - Therapeutics April 5 - April 7, 2018 Halifax Convention Centre Disclosures Conflicts
Hepatitis C Update on New Treatments Kevork M. Peltekian, MD, FRCPC 44th Annual Dalhousie Spring Refresher Course - Therapeutics April 5 - April 7, 2018 Halifax Convention Centre Disclosures Conflicts
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 32 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Pegylated Interferon Agents for Hepatitis C
 Applicable X X X X X X X Pegylated Interferon Agents for Hepatitis C Override(s) Prior Authorization Quantity Limit Initial for Monotherapy or Combination with Ribavirin based on Genotype, Status, or Co-Infection
Applicable X X X X X X X Pegylated Interferon Agents for Hepatitis C Override(s) Prior Authorization Quantity Limit Initial for Monotherapy or Combination with Ribavirin based on Genotype, Status, or Co-Infection
Clinical Policy: Glecaprevir/Pibrentasvir (Mavyret) Reference Number: GA.PMN.24 Product: Medicaid Effective Date: 9/17
 Reference Number: GA.PMN.24 Product: Medicaid Effective Date: 9/17") Clinical Policy: Glecaprevir/Pibrentasvir (Mavyret) Reference Number: GA.PMN.24 Product: Medicaid Effective Date: 9/17 Last Review Date: 9/17 Revision Log See Important Reminder at the end of this policy
Clinical Policy: Glecaprevir/Pibrentasvir (Mavyret) Reference Number: GA.PMN.24 Product: Medicaid Effective Date: 9/17 Last Review Date: 9/17 Revision Log See Important Reminder at the end of this policy
Hepatitis C Prior Authorization Policy
 Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE
 THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE The following content is provided for informational purposes only. Diagnosing and Managing Hepatitis C Sandy Van Sant MPH, APN Hepatitis C virus
THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE The following content is provided for informational purposes only. Diagnosing and Managing Hepatitis C Sandy Van Sant MPH, APN Hepatitis C virus
Updates in the Treatment of HCV
 Updates in the Treatment of HCV Misty Miller, Pharm.D., BCPS, AAHIVP Associate Professor University of Oklahoma College of Pharmacy September 21 st, 2018 Overview HCV Review and Definitions HCV Genotypes
Updates in the Treatment of HCV Misty Miller, Pharm.D., BCPS, AAHIVP Associate Professor University of Oklahoma College of Pharmacy September 21 st, 2018 Overview HCV Review and Definitions HCV Genotypes
Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner
 Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner Annie Luetkemeyer, MD Division of HIV,ID & Global Medicine San Francisco General Hospital Disclosures I have received research grant
Hepatitis C: the 2015 Perspective for the Family Medicine Practitioner Annie Luetkemeyer, MD Division of HIV,ID & Global Medicine San Francisco General Hospital Disclosures I have received research grant
Hepatitis C ew Medications, New Hope and New. V. Opportunities for Primary Care. Outline. HCV Disease Outcomes in the US 9/21/2016
 Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Hepatitis C ew Medications, New Hope and New Opportunities for Primary Care Primary Care Principles and Practice October 14, 2016 Disclosures: Grant support Gilead Sciences, Inc Quality improvement Systematized
Glecaprevir-Pibrentasvir in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2)
") Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
i Screening and Natural History
 HCV Epidemiology, i Screening and Natural History BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Hepatitis
HCV Epidemiology, i Screening and Natural History BRUCE A. LUXON, MD, PHD, FACG ANTON AND MARGARET FUISZ CHAIR IN MEDICINE PROFESSOR AND CHAIRMAN DEPARTMENT OF MEDICINE GEORGETOWN UNIVERSITY Hepatitis
RATIONALE FOR INCLUSION IN PA PROGRAM
 RATIONALE FOR INCLUSION IN PA PROGRAM Background Hepatitis C is a viral disease that causes inflammation of the liver that can lead to diminished liver function or liver failure. Most people infected with
RATIONALE FOR INCLUSION IN PA PROGRAM Background Hepatitis C is a viral disease that causes inflammation of the liver that can lead to diminished liver function or liver failure. Most people infected with
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Mavyret) Reference Number: CP.HNMC.39 Effective Date: 08.15.17 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Mavyret) Reference Number: CP.HNMC.39 Effective Date: 08.15.17 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy
End Stage Liver Disease & Disease Specific Indications for Liver Transplant. Susan Kang, RN, MSN, ANP-BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES
 HARVARD PILGRIM HEALTH CARE Generic Brand HICL GCN Exception/Other DACLATASVIR DAKLINZA 41377 ELBASVIR/GRAZOPREVIR ZEPATIER 43030 GLECAPREVIR/PIBRENTASVIR MAVYRET 44453 OMBITASVIR/PARITAPREVIR/ RITONAVIR
HARVARD PILGRIM HEALTH CARE Generic Brand HICL GCN Exception/Other DACLATASVIR DAKLINZA 41377 ELBASVIR/GRAZOPREVIR ZEPATIER 43030 GLECAPREVIR/PIBRENTASVIR MAVYRET 44453 OMBITASVIR/PARITAPREVIR/ RITONAVIR
Pharmacy Medical Necessity Guidelines: Medications for the Treatment of Hepatitis C
 Pharmacy Medical Necessity Guidelines: Medications for the Treatment of Hepatitis C Effective: March 13, 2018 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical
Pharmacy Medical Necessity Guidelines: Medications for the Treatment of Hepatitis C Effective: March 13, 2018 Prior Authorization Required Type of Review Care Management Not Covered Type of Review Clinical
Physical Aspects of Substance Misuse in Older People. Jane Collier Consultant Hepatology John Radcliffe Hospital Oxford
 Physical Aspects of Substance Misuse in Older People Jane Collier Consultant Hepatology John Radcliffe Hospital Oxford Areas to cover Hepatitis C Curable disease New drugs (goodbye interferon) Drug Interactions
Physical Aspects of Substance Misuse in Older People Jane Collier Consultant Hepatology John Radcliffe Hospital Oxford Areas to cover Hepatitis C Curable disease New drugs (goodbye interferon) Drug Interactions
Clinical Policy: Sofosbuvir/Velpatasvir/Voxilaprevir (Vosevi) Reference Number: GA.PMN.25 Product: Medicaid Effective Date: 9/17
 Reference Number: GA.PMN.25 Product: Medicaid Effective Date: 9/17") Clinical Policy: Sofosbuvir/Velpatasvir/Voxilaprevir (Vosevi) Reference Number: GA.PMN.25 Product: Medicaid Effective Date: 9/17 Last Review Date: 9/17 Revision Log See Important Reminder at the end of
Clinical Policy: Sofosbuvir/Velpatasvir/Voxilaprevir (Vosevi) Reference Number: GA.PMN.25 Product: Medicaid Effective Date: 9/17 Last Review Date: 9/17 Revision Log See Important Reminder at the end of
New York State HCV Provider Webinar Series
 New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Dost Sarpel, MD Division of Infectious Disease Viral Hepatology Milford Regional Medical Center Objectives Review the epidemiology
New York State HCV Provider Webinar Series Treatment of HCV/HIV Co-Infection Dost Sarpel, MD Division of Infectious Disease Viral Hepatology Milford Regional Medical Center Objectives Review the epidemiology
Management of the Patient with Chronic Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY
 Management of the Patient with Chronic Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY Disclosures Nothing to disclose Management of the Patient with Chronic Hepatitis C Communicate
Management of the Patient with Chronic Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY Disclosures Nothing to disclose Management of the Patient with Chronic Hepatitis C Communicate
Transmission of HCV in the United States (CDC estimate)
") Transmission of HCV in the United States (CDC estimate) Past and Future US Incidence and Prevalence of HCV Infection Decline among IDUs Overall incidence Overall prevalence Infected 20+ years Armstrong
Transmission of HCV in the United States (CDC estimate) Past and Future US Incidence and Prevalence of HCV Infection Decline among IDUs Overall incidence Overall prevalence Infected 20+ years Armstrong
EXAMINING THE 3 Cs OF HEPATITIS C: CARE, CURE, CO$T
 EXAMINING THE 3 Cs OF HEPATITIS C: CARE, CURE, CO$T Update presented by Lisa Townshend-Bulson, MSN, FNP-C Followed by Round Table Discussion: ANTHC Liver Disease & Hepatitis Program Staff and Audience
EXAMINING THE 3 Cs OF HEPATITIS C: CARE, CURE, CO$T Update presented by Lisa Townshend-Bulson, MSN, FNP-C Followed by Round Table Discussion: ANTHC Liver Disease & Hepatitis Program Staff and Audience
Hepatits C Criteria Direct Acting Antiviral Medications
 Hepatits C Criteria Direct Acting Antiviral Medications Harvoni-Formulary PA required 1. Is the patient being treated for a funded condition by the Oregon Health Plan? 2. Does the member have a diagnosis
Hepatits C Criteria Direct Acting Antiviral Medications Harvoni-Formulary PA required 1. Is the patient being treated for a funded condition by the Oregon Health Plan? 2. Does the member have a diagnosis
Assessing the patient with a new diagnosis of Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY
 Assessing the patient with a new diagnosis of Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY Disclosures Nothing to Disclose Assessing the patient with a new diagnosis of Hepatitis
Assessing the patient with a new diagnosis of Hepatitis C LAUREN MYERS MMSC, PA-C OREGON HEALTH & SCIENCE UNIVERSITY Disclosures Nothing to Disclose Assessing the patient with a new diagnosis of Hepatitis
Treating Hepatitis C in Patients with Advanced Renal Disease
 Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
Treating Hepatitis C in Patients with Advanced Renal Disease Seyed Moayed Alavian M.D. Professor of Medicine, Hepatologist alavian@thc.ir Hemodialysis Patients hemodialysis Preventive Strategies Strict
Hepatitis C: a treatment revolution
 Sunday, 10th July 2016 Michaelmas Cay 2 Room Concurrent 11 Health Innovation Hepatitis C: a treatment revolution Dr. Heather McNamee Hepatitis C a treatment revolution Dr Heather McNamee Medical Director
Sunday, 10th July 2016 Michaelmas Cay 2 Room Concurrent 11 Health Innovation Hepatitis C: a treatment revolution Dr. Heather McNamee Hepatitis C a treatment revolution Dr Heather McNamee Medical Director
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
National Clinical Guidelines for the treatment of HCV in adults. Version 4
 National Clinical Guidelines for the treatment of HCV in adults Version 4 November 2017 Sponsors and Authorship The guidelines have been authored on behalf of the viral hepatitis clinical leads and MCN
National Clinical Guidelines for the treatment of HCV in adults Version 4 November 2017 Sponsors and Authorship The guidelines have been authored on behalf of the viral hepatitis clinical leads and MCN
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
Hepatitis C Second Generation Antivirals Page 1 of 30 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C Second Generation Antivirals Through
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Harvoni) Reference Number: CP.CPA.175 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Harvoni) Reference Number: CP.CPA.175 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Learning Objectives: Hepatitis Update. Primary Causes of Chronic Liver Disease in the U.S. Hepatitis Definition. Hepatitis Viruses.
 Learning Objectives: Hepatitis Update ASCLS-Michigan March 31, 2016 Dr. Kathleen Hoag Upon attendance of this seminar and review of material provided, the attendees will be able to: 1. List hepatitis viruses
Learning Objectives: Hepatitis Update ASCLS-Michigan March 31, 2016 Dr. Kathleen Hoag Upon attendance of this seminar and review of material provided, the attendees will be able to: 1. List hepatitis viruses
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
Hepatitis C Update: A Growing Challenge With Evolving Management Solutions
 Pts (%) Hepatitis C Update: A Growing Challenge With Evolving Management Solutions A Growing Challenge With Evolving Management Solutions Introduction Magda Houlberg, MD Chief Clinical Officer Howard Brown
Pts (%) Hepatitis C Update: A Growing Challenge With Evolving Management Solutions A Growing Challenge With Evolving Management Solutions Introduction Magda Houlberg, MD Chief Clinical Officer Howard Brown
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors.
 Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Thompson AJV; Expert panel representing the Gastroenterological
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Thompson AJV; Expert panel representing the Gastroenterological
Clinical Policy: Daclatasvir (Daklinza) Reference Number: ERX.SPMN.180
 Reference Number: ERX.SPMN.180") Clinical Policy: (Daklinza) Reference Number: ERX.SPMN.180 Effective Date: 10/16 Last Review Date: 09/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Daklinza) Reference Number: ERX.SPMN.180 Effective Date: 10/16 Last Review Date: 09/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important
ABCs of Viral Hepatitis What Primary Care Physicians Need to Know
 ABCs of Viral Hepatitis What Primary Care Physicians Need to Know Dr Kenny C.P. Sze Associate Consultant Division of Gastroenterology Department of General Medicine Outline and Keypoints Hepatitis A Recap;
ABCs of Viral Hepatitis What Primary Care Physicians Need to Know Dr Kenny C.P. Sze Associate Consultant Division of Gastroenterology Department of General Medicine Outline and Keypoints Hepatitis A Recap;
2017 UnitedHealthcare Services, Inc.
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 1146-7 Program Prior Authorization/Notification Medication Harvoni (ledipasvir/sofosbuvir) P&T Approval Date 10/2014, 2/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 1146-7 Program Prior Authorization/Notification Medication Harvoni (ledipasvir/sofosbuvir) P&T Approval Date 10/2014, 2/2015,
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Hepatitis C (Direct Acting Antiviral Medications for Treatment of Hepatitis C) Fibrosis Score Requirement QUEST Integration
 Fibrosis Score Requirement QUEST Integration") Hepatitis C (Direct Acting Antiviral Medications for Treatment of Hepatitis C) Fibrosis Score Requirement QUEST Integration Policy Number: Original Effective Date: MM.04.036 06/01/2015 Lines of Business:
Hepatitis C (Direct Acting Antiviral Medications for Treatment of Hepatitis C) Fibrosis Score Requirement QUEST Integration Policy Number: Original Effective Date: MM.04.036 06/01/2015 Lines of Business:
Harvoni (sofosbuvir/ledipasvir
 Market DC Override(s) Prior Authorization Quantity Limit (sofosbuvir/ledipasvir) Approval Duration Based on Genotype, Treatment status, Baseline HCV RNA status, Cirrhosis status, Transplant status, or
Market DC Override(s) Prior Authorization Quantity Limit (sofosbuvir/ledipasvir) Approval Duration Based on Genotype, Treatment status, Baseline HCV RNA status, Cirrhosis status, Transplant status, or
REQUEST FOR PRIOR AUTHORIZATION Hepatitis C Treatments
 Fax completed form to: 866-940-7328 Prior Authorization Phone Number: 800-310-6826 IA Medicaid Member ID # Patient name Date of Birth Patient address Patient phone Provider NPI Prescriber name Phone Prescriber
Fax completed form to: 866-940-7328 Prior Authorization Phone Number: 800-310-6826 IA Medicaid Member ID # Patient name Date of Birth Patient address Patient phone Provider NPI Prescriber name Phone Prescriber
Hepatitis C Virus Clinical Criteria Update September 18, For: New York State Medicaid
 Hepatitis C Virus Clinical Criteria Update September 18, 2014 For: New York State Medicaid 1 Purpose Characterize the place in therapy for the agents utilized for management of chronic hepatitis C (CHC)
Hepatitis C Virus Clinical Criteria Update September 18, 2014 For: New York State Medicaid 1 Purpose Characterize the place in therapy for the agents utilized for management of chronic hepatitis C (CHC)
HIV/HCV Coinfection: Why It Matters and What To Do About It. Cody A. Chastain, MD 10/26/16
 HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
HIV/HCV Coinfection: Why It Matters and What To Do About It Cody A. Chastain, MD 10/26/16 Disclosures I have no relevant financial disclosures. Objectives At the end of this lecture, the learner will be
The New World of HCV Therapy
 HCV: Assessing the Patient Prior to Treatment: Diagnostic Testing and Strategy JORGE L. HERRERA M.D., MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The New World of HCV Therapy Interferon-free
HCV: Assessing the Patient Prior to Treatment: Diagnostic Testing and Strategy JORGE L. HERRERA M.D., MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE, MOBILE, AL The New World of HCV Therapy Interferon-free
Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain
 Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain Disclosures Advisory boards and speaker s bureau for: Gilead, Merck,
Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain Disclosures Advisory boards and speaker s bureau for: Gilead, Merck,
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Epclusa) Reference Number: CP.CPA.286 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Epclusa) Reference Number: CP.CPA.286 Effective Date: 11.01.16 Last Review Date: 08.18 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Update on HCV Treatment
 Update on HCV Treatment Ajay Bharti, MD Associate Professor of Medicine Division of Infectious Diseases University of California San Diego 2018 April 28, 2018 Clinically relevant questions in HCV-HIV coinfected
Update on HCV Treatment Ajay Bharti, MD Associate Professor of Medicine Division of Infectious Diseases University of California San Diego 2018 April 28, 2018 Clinically relevant questions in HCV-HIV coinfected
Hepatitis C Update: What s New in 2017
 Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
Hepatitis C Update: What s New in 2017 Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu