Addressing Emergency Neuro- Pharmacologic Controversies Head-On. What dose of IV benzodiazepine makes you uncomfortable?
|
|
|
- Milo Hancock
- 5 years ago
- Views:
Transcription



1 Addressing Emergency Neuro- Pharmacologic Controversies Head-On 38 y/o 136 bpm Bryan D. Sz, tremor, hallucinations Which benzodiazepine would you administer first? Why? Diazepam Lorazepam Other What dose of IV benzodiazepine makes you uncomfortable? Diazepam 20 mg Diazepam 40 mg Lorazepam 10 mg Lorazepam 20 mg What additional medications would you use in refractory EtOH withdrawal? Phenobarbital Propofol Dexmedetomidine Other 1
2 2

3 NMDA GABA excitatory inhibitory Benzodiazepines Barbiturates Propofol 3



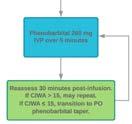
4 Biggest Mistake We Make UNDERDOSING 24 Hours Mean: 234 mg Highest: 2600 mg Individual: 200 mg +/- phenobarbital GABA Range: mg Gold JA, et al. Crit Care Med 2007;35: Wojnar M, et al. Alcohol Clin Exp Res 1997;21: Spies CD, et al. Intensive Care Med 2003;29: Phenobarbital mg Onset min Avoid stacking Ives TJ, et al. South Med J 1991;84: Hill A, et al. J Subst Abuse Treat 1993;10: Rosenson J, et al. J Emerg Med 2013;44:
:18-21. Tangmose K, et al. Dan Med Bull 2010;57(8):A4141. Kramp P, et al. Acta Psychiatr Scand 1978;58(2):174-90.")

:724-30. 95 patients, pre/post-new guideline Indiv Diazepam Total Diazepam Phenobarb Use 32 mg 248 mg 17% 86 mg 562 mg 58% 50% reduction in MV (47% vs.")
5 1. Less delirium 2. No paradoxical reactions 3. Linear dose to concentration 4. Supporting RCT data vs benzos Moore PW, et al. J Med Toxicol 2014;10(2): Ives TJ, et al. South Med J 1991;84(1): Tangmose K, et al. Dan Med Bull 2010;57(8):A4141. Kramp P, et al. Acta Psychiatr Scand 1978;58(2): Phenobarbital for acute alcohol withdrawal: a prospective randomized double-blind placebo-controlled study. Rosenson J, et al. J Emerg Med 2013;44(3): patients 10 mg/kg + lorazepam symptom-triggered ICU admission (8% vs. 25%) No difference in adverse effects A strategy of escalating doses of benzodiazepines and phenobarbital administration reduces the need for mechanical ventilation in delirium tremens. Gold JA, et al. Crit Care Med 2007;35(3): patients, pre/post-new guideline Indiv Diazepam Total Diazepam Phenobarb Use 32 mg 248 mg 17% 86 mg 562 mg 58% 50% reduction in MV (47% vs. 22%) GABA NMDA Use of propofol infusion in alcohol withdrawal-induced refractory delirium tremens. Lorentzen K, et al. Dan Med J 2014;61(5):A patients Diazepam 1,500 mg or Phenobarbital 1,200 mg Mean Propofol dose: 70 mcg/kg/min 12 patients treated successfully 5



6 Focus on GABA ICU pts Dexmedetomidine HR/BP Benzos 1.5 mcg/kg/hr A randomized, double-blind, placebo-controlled, dose range study of dexmedetomidine as adjunctive therapy for alcohol withdrawal. Mueller SW, et al. Crit Care Med 2014;42(5): ICU pts Lorazepam requirements 209 excluded A randomized, double-blind, placebo-controlled, dose range study of dexmedetomidine as adjunctive therapy for alcohol withdrawal. Mueller SW, et al. Crit Care Med 2014;42(5): Lorazepam 24 hrs prior to study initiation Placebo Low Dose High Dose 39 mg 94 mg 75 mg Lorazepam 24 hrs after study initiation Placebo Low Dose High Dose 77 mg 28 mg 15 mg 6




7 24 hrs before randomization 11 pts already intubated Endpoint selection 1. Adjunct only 2. Preserved respiratory drive 3. Future study outcomes No effect: Severity Seizures Wilson A, et al. Alcohol Clin Exp Res 1984;8: Baclofen Gabapentin Cochrane Database Syst Rev 2013;2:CD Bonnet U, et al. Alcohol Alcohol 2010;45(2):



![Crit Care Med 2018. [Epub ahead of print] 63 pts Mean 0.](/docs-images/88/115303234/images/8-4.jpg "2 mg/kg/hr (19 loading dose) ICU LOS 3 days intubation benzo (2,525 vs")
8 NMDA Evaluation of adjunctive ketamine to benzodiazepines for management of alcohol withdrawal syndrome. Wong A, et al. Ann Pharmacother 2015;49(1): pts Median 0.2 mg/kg/hr BZD -40 & mg (12/24 hr) Reduction of BZD requirements Adjunctive ketamine us in the management of severe ethanol withdrawal. Pizon A, et al. Crit Care Med [Epub ahead of print] 63 pts Mean 0.2 mg/kg/hr (19 loading dose) ICU LOS 3 days intubation benzo (2,525 vs 1,508 mg) DTs Severe EtOH w/d Benzos, benzos, benzos Phenobarb & propofol Dexmedetomidine adjunctive Ketamine on horizon? 8




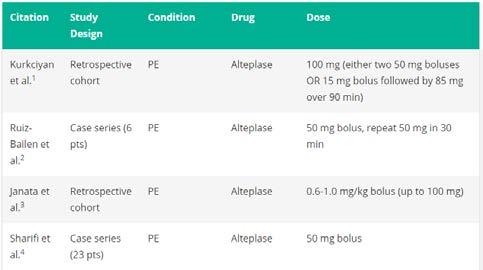
9 What s the Code- Dose of tpa? 9







10 Courtesy of Courtesy of Courtesy of Courtesy of 10







11 50 mg IV push, may repeat X 1 CPR not a contraindication; continue 15 min Evidence best for PE; NOT undifferentiated Migraine +/- anticoagulants Recommendation Conclusion About Efficacy Should offer (Level B) May offer (C) May avoid (C) No recs (U) Highly likely to be effective Possibly/likely effective Likely ineffective/ Possibly ineffective/ Insufficient evidence/ Possibly effective/ Insufficient evidence Orr SL, et al. Headache 2016;56: Metoclopramide mg IV Prochlorperazine 10 mg IV Sumatriptan 6 mg subcut Droperidol/haloperidol IM/IV Valproic Acid IV NSAIDS/APAP IV Dexamethasone should be offered to prevent recurrence in adults discharged from an ED Orr SL, et al. Headache 2016;56: Should Offer Orr SL, et al. Headache 2016;56: May Offer 11




12 Diphenhydramine * Lidocaine Opioids Adjunctive Metoclopramide 10 mg AVOID Metoclopramide 20 mg CONSIDER Prochlorperazine 10 mg GIVE Orr SL, et al. Headache 2016;56: May Avoid Magnesium Ketamine Propofol 1. tpa 50 mg for PE; CPR 15 min 2. Migraine: prochlorperazine or metoclopramide +/- diphenhydramine +/- dexamethasone Orr SL, et al. Headache 2016;56: Addressing Emergency Neuro- Pharmacologic Controversies Head-On Bryan D. Hayes, PharmD, FAACT, FASHP MGH/Harvard Medical School bryanhayes13@gmail.com 12
STOPPING THE SHAKES: Advanced Concepts in Alcohol Withdrawal Management. Michael Levine, MD 14 March, 2013
 STOPPING THE SHAKES: Advanced Concepts in Alcohol Withdrawal Management Michael Levine, MD 14 March, 2013 DISCLOSURES No financial, litigational, or other conflicts of interest to disclose OBJECTIVES Briefly
STOPPING THE SHAKES: Advanced Concepts in Alcohol Withdrawal Management Michael Levine, MD 14 March, 2013 DISCLOSURES No financial, litigational, or other conflicts of interest to disclose OBJECTIVES Briefly
Disclosures. Learning Objective 4/26/2017
 Management of acute alcohol withdrawal at a community hospital in an area with a high prevalence of alcoholism { Melissa Cirillo, Pharm.D. 4/29/2017 Financial: None Nonfinancial: None Disclosures List
Management of acute alcohol withdrawal at a community hospital in an area with a high prevalence of alcoholism { Melissa Cirillo, Pharm.D. 4/29/2017 Financial: None Nonfinancial: None Disclosures List
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Can t Stop the Seizing!
 Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Can t Stop the Seizing! Joseph Miller, MD, MS MCEP Critical Care March, 2019 Objectives Describe the importance of time to treatment Delineate treatment based on best evidence Describe novel diagnostic
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim
Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim
Status Epilepticus: Implications Outside the Neuro-ICU
 Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Blame it on the Alcohol: Comparison of Propofol vs Dexmedetomidine for Refractory Alcohol Withdrawal
 Blame it on the Alcohol: Comparison of Propofol vs Dexmedetomidine for Refractory Alcohol Withdrawal Kristi Hargrove, PharmD PGY1 Pharmacy Resident Department of Pharmacotherapy and Pharmacy Services,
Blame it on the Alcohol: Comparison of Propofol vs Dexmedetomidine for Refractory Alcohol Withdrawal Kristi Hargrove, PharmD PGY1 Pharmacy Resident Department of Pharmacotherapy and Pharmacy Services,
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Current Practice Patterns in the Management Of Alcohol Withdrawal Syndrome
 Current Practice Patterns in the Management Of Alcohol Withdrawal Syndrome Yoonsun Mo, MS, PharmD, BCPS, BCCCP; Michael C. Thomas, PharmD, BCPS, FCCP; Corey S. Laskey, PharmD, BCPP; Natalia Shcherbakova,
Current Practice Patterns in the Management Of Alcohol Withdrawal Syndrome Yoonsun Mo, MS, PharmD, BCPS, BCCCP; Michael C. Thomas, PharmD, BCPS, FCCP; Corey S. Laskey, PharmD, BCPP; Natalia Shcherbakova,
Adjunctive Use of Ketamine for Benzodiazepine-Resistant Severe Alcohol Withdrawal: a Retrospective Evaluation
 Journal of Medical Toxicology (2018) 14:229 236 https://doi.org/10.1007/s13181-018-0662-8 ORIGINAL ARTICLE Adjunctive Use of Ketamine for Benzodiazepine-Resistant Severe Alcohol Withdrawal: a Retrospective
Journal of Medical Toxicology (2018) 14:229 236 https://doi.org/10.1007/s13181-018-0662-8 ORIGINAL ARTICLE Adjunctive Use of Ketamine for Benzodiazepine-Resistant Severe Alcohol Withdrawal: a Retrospective
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Status Epilepticus: A refresher. Objectives
 Status Epilepticus: A refresher Ruben D. Villanueva, Pharm.D., BCPS OU Medical Center Trauma ICU Pharmacist Objectives Define seizures, convulsive and non convulsive status epilepticus, and refractory
Status Epilepticus: A refresher Ruben D. Villanueva, Pharm.D., BCPS OU Medical Center Trauma ICU Pharmacist Objectives Define seizures, convulsive and non convulsive status epilepticus, and refractory
Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS)
") 1 Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS) The goal of the survey is to evaluate current practices for the inpatient management of AWS in adult hospitals located
1 Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS) The goal of the survey is to evaluate current practices for the inpatient management of AWS in adult hospitals located
Refractory Status Epilepticus in Children: What are the Options?
 Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients
 Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients Timothy J. Wiegand, MD Associate Clinical Professor of Emergency Medicine,
Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients Timothy J. Wiegand, MD Associate Clinical Professor of Emergency Medicine,
NonConvulsive Seizure
 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Refractory Seizures. Dr James Edwards EMCORE May 30th 2014
 Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
The ALTO Program: A Strategy to Reduce Opioid use in the Emergency Department
 The ALTO Program: A Strategy to Reduce Opioid use in the Emergency Department The ALTO Program: A Strategy to Reduce Opioid use in the Emergency Department Steven F. Nerenberg, Pharm.D. Clinical Assistant
The ALTO Program: A Strategy to Reduce Opioid use in the Emergency Department The ALTO Program: A Strategy to Reduce Opioid use in the Emergency Department Steven F. Nerenberg, Pharm.D. Clinical Assistant
COMPARISON OF SEDATION FOR ALCOHOL WITHDRAWAL Crispo et al 911
 Comparison of Clinical Outcomes in Nonintubated Patients with Severe Alcohol Withdrawal Syndrome Treated with Continuous-Infusion Sedatives: Dexmedetomidine versus Benzodiazepines Angela L. Crispo, 1 Mitchell
Comparison of Clinical Outcomes in Nonintubated Patients with Severe Alcohol Withdrawal Syndrome Treated with Continuous-Infusion Sedatives: Dexmedetomidine versus Benzodiazepines Angela L. Crispo, 1 Mitchell
Emerging Roles for Ketamine in the ICU
 Emerging Roles for Ketamine in the ICU Amy Green, PharmD, BCPS Clinical Pharmacy Specialist, Neurocritical Care Rush University Medical Center No financial disclosures or conflicts of interest. Off-label
Emerging Roles for Ketamine in the ICU Amy Green, PharmD, BCPS Clinical Pharmacy Specialist, Neurocritical Care Rush University Medical Center No financial disclosures or conflicts of interest. Off-label
ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY?
 Psychiatry and Addictions Case Conference Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Psychiatry and Addictions Case Conference Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
From Where? Rochester, NY
 From Where? Rochester, NY 3 Days of Sunshine Annually Invented SAD Lights Disclosures I have no financial disclosures The feds want their money back The only bad question... Objectives Review endocrine
From Where? Rochester, NY 3 Days of Sunshine Annually Invented SAD Lights Disclosures I have no financial disclosures The feds want their money back The only bad question... Objectives Review endocrine
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Anesthesia for OutPatient Spine Surgery. Michael A. Kellams, D.O.
 Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
CrackCast Episode 18 Seizures
 CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
CrackCast Episode 18 Seizures Episode overview: 1) Define status epilepticus 2) List the doses of common medications used for status epilepticus 3) List 10 differential diagnoses for seizures 4) List 10
Multiple Choice Questions
 Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Alcohol withdrawal. Clinical features
 Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Absence seizures, 6 in childhood, 95 Adults, seizures and status epilepticus in, management of, 34 35 with first-time seizures. See Seizure(s),
Index Note: Page numbers of article titles are in boldface type. A Absence seizures, 6 in childhood, 95 Adults, seizures and status epilepticus in, management of, 34 35 with first-time seizures. See Seizure(s),
ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
WHAT SHOULD WE DO ABOUT BENZODIAZEPINES? Miriam Komaromy, MD Associate Director, Project ECHO August 2014
 WHAT SHOULD WE DO ABOUT BENZODIAZEPINES? Miriam Komaromy, MD Associate Director, Project ECHO August 2014 EPIDEMIOLOGY OF BENZO USE 7-18% of US population uses a benzo for medical purposes each year Average
WHAT SHOULD WE DO ABOUT BENZODIAZEPINES? Miriam Komaromy, MD Associate Director, Project ECHO August 2014 EPIDEMIOLOGY OF BENZO USE 7-18% of US population uses a benzo for medical purposes each year Average
Acute Postoperative Pain. David Radvinsky, MD March 24, 2016
 Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Drug. Alcohol is one of the most frequently abused drugs in American society. Update
 AACN Advanced Critical Care Volume 28, Number 3, pp. 233-238 2017 AACN Drug Update Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Pharmacologic Management of Alcohol Withdrawal
AACN Advanced Critical Care Volume 28, Number 3, pp. 233-238 2017 AACN Drug Update Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Pharmacologic Management of Alcohol Withdrawal
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
EM Cases Course 2017 Toxicology Module
 EM Cases Course 2017 Toxicology Module quick IV access and diazepam is administered. The seizure stops. The first set of vitals show: HR 30bpm, BP 70/40. His ECG is shown below. Margaret Thompson & JP
EM Cases Course 2017 Toxicology Module quick IV access and diazepam is administered. The seizure stops. The first set of vitals show: HR 30bpm, BP 70/40. His ECG is shown below. Margaret Thompson & JP
PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW
 PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW Dana Bartlett, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU
PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW Dana Bartlett, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU
SEEING KETAMINE IN A NEW LIGHT
 SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1
 Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1 Presenter Eric Ketcham, MD, MBA Reuben J. Strayer, MD emergency department management of the patient with opioid withdrawal OD is
Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1 Presenter Eric Ketcham, MD, MBA Reuben J. Strayer, MD emergency department management of the patient with opioid withdrawal OD is
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Guideline of status epilepticus management 2017
 Guideline of status epilepticus management 2017 Kanitpong Phabphal Professor of Neurology Guideline 1966 to Jan 2005 European Foundation Neurology Society 2010 Hong Kong Epilepsy Society Society 2017 Published
Guideline of status epilepticus management 2017 Kanitpong Phabphal Professor of Neurology Guideline 1966 to Jan 2005 European Foundation Neurology Society 2010 Hong Kong Epilepsy Society Society 2017 Published
Correlation Between Partial Pressure of Arterial Carbon Dioxide and End Tidal Carbon Dioxide in Patients with Severe Alcohol Withdrawal
 ORIGINAL RESEARCH The Ochsner Journal 15:418 422, 2015 Ó Academic Division of Ochsner Clinic Foundation Correlation Between Partial Pressure of Arterial Carbon Dioxide and End Tidal Carbon Dioxide in Patients
ORIGINAL RESEARCH The Ochsner Journal 15:418 422, 2015 Ó Academic Division of Ochsner Clinic Foundation Correlation Between Partial Pressure of Arterial Carbon Dioxide and End Tidal Carbon Dioxide in Patients
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
MR04A3 An isoindoline derivative, New Sedative/Anesthetic Agent
 MR04A3 An isoindoline derivative, ew Sedative/Anesthetic Agent ovember 2009 1 Introduction Sedatives are widely used in: Settings providing stressful and painful procedures Gastroenterology (colonoscopy
MR04A3 An isoindoline derivative, ew Sedative/Anesthetic Agent ovember 2009 1 Introduction Sedatives are widely used in: Settings providing stressful and painful procedures Gastroenterology (colonoscopy
Delirium: Prevention with Melatonin
 Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Dean Olsen, DO Director, Medical Education and Emergency Medicine Residency Nassau University Medical Center Faculty, New York City Poison Control
 Dean Olsen, DO Director, Medical Education and Emergency Medicine Residency Nassau University Medical Center Faculty, New York City Poison Control Center Professor, Toxicology NYIT College of Osteopathic
Dean Olsen, DO Director, Medical Education and Emergency Medicine Residency Nassau University Medical Center Faculty, New York City Poison Control Center Professor, Toxicology NYIT College of Osteopathic
5/11/2016. Alcohol, Sedative & Opioid Withdrawal Challenging Patients. Case 1. Case 1 continued
 Case 1 Alcohol, Sedative & Opioid Withdrawal Challenging Patients Timothy J. Wiegand, MD, DABAM, FACMT, FAACT, FASAM Director of Toxicology -URMC 41-year-old businessman admitted for chest pain. Overnight
Case 1 Alcohol, Sedative & Opioid Withdrawal Challenging Patients Timothy J. Wiegand, MD, DABAM, FACMT, FAACT, FASAM Director of Toxicology -URMC 41-year-old businessman admitted for chest pain. Overnight
Status Epilepticus. Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital. Pediatrics
 Status Epilepticus Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital Objectives Define the various stages of status epilepticus and explain the proposed pathophysiology
Status Epilepticus Mindy M. Messinger, PharmD Clinical Pharmacy Specialist Neurology Texas Children s Hospital Objectives Define the various stages of status epilepticus and explain the proposed pathophysiology
Please review the following slides prior to class. Information from these slides will be used to answer patient cases. Come prepared!
 Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Seizures Emergency Treatment
 Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Interprofessional Trauma Conference September 28th 2018 Montreal
 Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Pediatric Procedural Sedation
 Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
The First Fork in the Road
 Characteristics that Contribute to Medevac ADAP Medical Evacuations: What to Do Once the Decision is Made Stephen A. Young, MD Lorie J. Morris, Psy.D. US Department of State MED/MHS/ADAP 1 The First Fork
Characteristics that Contribute to Medevac ADAP Medical Evacuations: What to Do Once the Decision is Made Stephen A. Young, MD Lorie J. Morris, Psy.D. US Department of State MED/MHS/ADAP 1 The First Fork
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation. Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project
 Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Project: Ghana Emergency Medicine Collaborative. Document Title: Seizures. Author(s): Ryan LaFollette, MD (University of Cincinnati), 2013
: Ryan LaFollette, MD (University of Cincinnati), 2013") Project: Ghana Emergency Medicine Collaborative Document Title: Seizures Author(s): Ryan LaFollette, MD (University of Cincinnati), 2013 License: Unless otherwise noted, this material is made available
Project: Ghana Emergency Medicine Collaborative Document Title: Seizures Author(s): Ryan LaFollette, MD (University of Cincinnati), 2013 License: Unless otherwise noted, this material is made available
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium. Management of acute seizure settings from infancy to adolescence
 Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium Management of acute seizure settings from infancy to adolescence Consequences of prolonged seizures Acute morbidity and
Lieven Lagae Department of Paediatric Neurology Leuven University Leuven, Belgium Management of acute seizure settings from infancy to adolescence Consequences of prolonged seizures Acute morbidity and
Outcomes of Patients with Alcohol Withdrawal Syndrome Treated with High-Dose Sedatives and Deferred Intubation
 Outcomes of Patients with Alcohol Withdrawal Syndrome Treated with High-Dose Sedatives and Deferred Intubation Robert Stewart 1, Ricardo Perez 2, Bogdan Musial 2, Carrie Lukens 3, Yaw Amoateng Adjepong
Outcomes of Patients with Alcohol Withdrawal Syndrome Treated with High-Dose Sedatives and Deferred Intubation Robert Stewart 1, Ricardo Perez 2, Bogdan Musial 2, Carrie Lukens 3, Yaw Amoateng Adjepong
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Alcohol Withdrawal: Assessment and Symptom-Triggered Treatment
 Alcohol Withdrawal: Assessment and Symptom-Triggered Treatment 2016 Alcohol, or ethanol, is produced by the fermentation of yeast, sugars and starches. Yeast breaks sugar down into ethanol and carbon dioxide.
Alcohol Withdrawal: Assessment and Symptom-Triggered Treatment 2016 Alcohol, or ethanol, is produced by the fermentation of yeast, sugars and starches. Yeast breaks sugar down into ethanol and carbon dioxide.
Procedural Sedation and Analgesia in the ED
 Overview Procedural Sedation and Analgesia in the ED Susan Lambe, MD Assistant Clinical Professor UCSF Division of Emergency Medicine Terminology Goals Indications Presedation Assessment Consent Issues
Overview Procedural Sedation and Analgesia in the ED Susan Lambe, MD Assistant Clinical Professor UCSF Division of Emergency Medicine Terminology Goals Indications Presedation Assessment Consent Issues
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
DRAFT FOR CONSULTATION
 1) What is the accuracy of a tool and/or clinical judgement for the a) assessment b) monitoring of patients at risk of acute alcohol withdrawal? 2) Does the assessment and monitoring of patients with acute
1) What is the accuracy of a tool and/or clinical judgement for the a) assessment b) monitoring of patients at risk of acute alcohol withdrawal? 2) Does the assessment and monitoring of patients with acute
The Difficult to Sedate ICU Patient
 The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Episode 74 Rationale Use of Opioids
 Prepared by Dr. Keerat Grewal, edited by Dr. Anton Helman, Dec 2015 Episode 74 Rationale Use of Opioids Drs. David Juurlink & Reuben Strayer Opioid Use and Misuse Opioid misuse has become a major public
Prepared by Dr. Keerat Grewal, edited by Dr. Anton Helman, Dec 2015 Episode 74 Rationale Use of Opioids Drs. David Juurlink & Reuben Strayer Opioid Use and Misuse Opioid misuse has become a major public
2012 AAHPM & HPNA Annual Assembly
 Barnstorming, Directing, & Producing: Integration of a Clinical Pharmacist Across the Continuum of Palliative Care and Hospice Services Disclosures Drs. Moore and Radwany have no relevant financial relationships
Barnstorming, Directing, & Producing: Integration of a Clinical Pharmacist Across the Continuum of Palliative Care and Hospice Services Disclosures Drs. Moore and Radwany have no relevant financial relationships
Medicating the Melon: Adjunctive Therapy after Traumatic Brain Injury
 Medicating the Melon: Adjunctive Therapy after Traumatic Brain Injury Kirstin Kooda, Pharm.D., BCPS, BCCCP Critical Care Pharmacist Pharmacy Grand Rounds January 24 th, 2017 Disclosures No financial relationships
Medicating the Melon: Adjunctive Therapy after Traumatic Brain Injury Kirstin Kooda, Pharm.D., BCPS, BCCCP Critical Care Pharmacist Pharmacy Grand Rounds January 24 th, 2017 Disclosures No financial relationships
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Objectives. History of Ketamine First synthesized at Parke Davis Alternative to phencyclidine Veterinary medicine. Mechanism. Mechanism 9/13/2016
 Objectives Keeping Things Calm and Cool: A Pharmacotherapy Update Describe the pharmacology and recognize the adverse effects of ketamine Select an appropriate patient to sedate with ketamine to facilitate
Objectives Keeping Things Calm and Cool: A Pharmacotherapy Update Describe the pharmacology and recognize the adverse effects of ketamine Select an appropriate patient to sedate with ketamine to facilitate
Resuscitation Articles 2017
 Resuscitation Articles 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Annal Emerg Med 2017;Epub ahead of print
Resuscitation Articles 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Annal Emerg Med 2017;Epub ahead of print
Specific Care Question : Question Originator: Plain Language Summary from The Office of Evidence Based Practice: Conditional Recommendation
 Ketorolac for Refractory Migraine in the ED Specific Care Question : In the pediatric patient diagnosed with refractory migraine is ketorolac an effective treatment? Question Originator: Migraine Therapy
Ketorolac for Refractory Migraine in the ED Specific Care Question : In the pediatric patient diagnosed with refractory migraine is ketorolac an effective treatment? Question Originator: Migraine Therapy
Session 2: Mental Health A: Alcohol Dependency: The Pharmacist s Role in Detox and Treatment 1:45pm - 2:45pm
 January 20-22, 2012 Des Moines Marrio, 700 Grand Avenue, Des Moines, IA Session 2: Mental Health A: Alcohol Dependency: The Pharmacist s Role in Detox and Treatment 1:45pm - 2:45pm ACPE UAN 107-000-12-015-L01-P
January 20-22, 2012 Des Moines Marrio, 700 Grand Avenue, Des Moines, IA Session 2: Mental Health A: Alcohol Dependency: The Pharmacist s Role in Detox and Treatment 1:45pm - 2:45pm ACPE UAN 107-000-12-015-L01-P
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
11/1/2018 STATUS EPILEPTICUS DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS. November is National Epilepsy Awareness Month
 STATUS EPILEPTICUS ALBERTO PINZON, MD, MSBE, PhD November is National Epilepsy Awareness Month DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS 1 SEIZURE A transient occurrence of signs and/or symptoms
STATUS EPILEPTICUS ALBERTO PINZON, MD, MSBE, PhD November is National Epilepsy Awareness Month DISCLOSURE SPEAKER FOR SUNOVION AND UCB PHARMACEUTICALS 1 SEIZURE A transient occurrence of signs and/or symptoms
Iroquois Healthcare Association (IHA) Opioid Alternative Project. Clinician Training Materials
 Opioid Alternative Project. Clinician Training Materials") Iroquois Healthcare Association (IHA) Opioid Alternative Project Clinician Training Materials Introduction IHA Opioid Alternative Project Clinician Toolkit Course Overview Thank you for participating
Iroquois Healthcare Association (IHA) Opioid Alternative Project Clinician Training Materials Introduction IHA Opioid Alternative Project Clinician Toolkit Course Overview Thank you for participating
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Results of a one-year, retrospective medication use evaluation. Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital
 Results of a one-year, retrospective medication use evaluation Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital Briefly review ketamine s history, mechanism of action, and unique properties
Results of a one-year, retrospective medication use evaluation Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital Briefly review ketamine s history, mechanism of action, and unique properties
Refractory Status Elipticus
 Refractory Status Elipticus In the 13 th round Laufey Yr Sigurdardottir MD Nemours Children s Hospital Department of Neurology NCH ED on Nov 29 th 2015 at 11:02 am First triage: fam here on vacation. pt
Refractory Status Elipticus In the 13 th round Laufey Yr Sigurdardottir MD Nemours Children s Hospital Department of Neurology NCH ED on Nov 29 th 2015 at 11:02 am First triage: fam here on vacation. pt
Recognition and Management of Withdrawal Delirium (Delirium Tremens)
") Review Article Dan L. Longo, M.D., Editor Recognition and Management of Withdrawal Delirium (Delirium Tremens) Marc A. Schuckit, M.D. At some time in their lives, 20% of men and 10% of women in most Western
Review Article Dan L. Longo, M.D., Editor Recognition and Management of Withdrawal Delirium (Delirium Tremens) Marc A. Schuckit, M.D. At some time in their lives, 20% of men and 10% of women in most Western
What the s wrong with this person?
 Ketamine for Prehospital Management of Excited Delirium Syndrome: Is it all just a bunch of hype?!? Financial Disclosure Asa M. Margolis, DO, MPH, MS, FACEP Assistant Professor Division of Special Operation
Ketamine for Prehospital Management of Excited Delirium Syndrome: Is it all just a bunch of hype?!? Financial Disclosure Asa M. Margolis, DO, MPH, MS, FACEP Assistant Professor Division of Special Operation
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
The Game Plan. Should I Be Doing This? The Perfect Drug. Procedural Sedation
 Procedural Sedation Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 The Game Plan Who shouldn t get sedation
Procedural Sedation Sanjay Arora MD Associate Professor of Emergency Medicine Keck School of Medicine at USC Los Angeles County + USC Medical Center May 23, 2012 The Game Plan Who shouldn t get sedation
Management of Acute Pain in the Chronic Pain Patient. Eric Cannon, MD Mountain West Anesthesia December 1, 2017
 Management of Acute Pain in the Chronic Pain Patient Eric Cannon, MD Mountain West Anesthesia December 1, 2017 Objectives 1. Describe the unique challenges of managing acute pain episodes in patients being
Management of Acute Pain in the Chronic Pain Patient Eric Cannon, MD Mountain West Anesthesia December 1, 2017 Objectives 1. Describe the unique challenges of managing acute pain episodes in patients being
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology
 A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology Acute NeuroCare Symposium & Expo 10/20/2017 Conflict of Interest Statement Conflict of Interest Declaration: I am a paid consultant
A. LeBron Paige, M.D. Director, Epilepsy Program UT Erlanger Neurology Acute NeuroCare Symposium & Expo 10/20/2017 Conflict of Interest Statement Conflict of Interest Declaration: I am a paid consultant
Dyspnea: Should we use BIPAP?
 Dyspnea: Should we use BIPAP? Thomas R. Gildea MD, MS FCCP Head Section of Bronchoscopy Respiratory Institute Transplant Center Disclosure SuperDimension Inc. PI for single center study Others: Aeris,
Dyspnea: Should we use BIPAP? Thomas R. Gildea MD, MS FCCP Head Section of Bronchoscopy Respiratory Institute Transplant Center Disclosure SuperDimension Inc. PI for single center study Others: Aeris,
Treatment of Headache in the ED
 Treatment of Headache in the ED Benjamin W. Friedman, MD, MS, FAAEM Associate professor of Emergency Medicine Albert Einstein College of Medicine Montefiore Medical Center Disclosure Topics of Discussion
Treatment of Headache in the ED Benjamin W. Friedman, MD, MS, FAAEM Associate professor of Emergency Medicine Albert Einstein College of Medicine Montefiore Medical Center Disclosure Topics of Discussion
Anxiolytic, Sedative and Hypnotic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming