CRIOGLOBULINEMIA MISTA E LINFOMI NELL ERA DEI DAAs DI II GENERAZIONE. Anna Linda Zignego
|
|
|
- Violet Ellis
- 5 years ago
- Views:
Transcription


1 CRIOGLOBULINEMIA MISTA E LINFOMI NELL ERA DEI DAAs DI II GENERAZIONE Anna Linda Zignego

2 Eur J Gastroenterol Hepatol, 2017


3 MC: in the setting of HCV-related pathologies, a typically female disease
4 Direct medical costs of extrahepatic manifestations of HCV in USA Younossi et al Evaluation of the annual costs (inpatient, outpatient, and pharmacy) associated with extrahepatic manifestations of HCV Total direct medical costs of extrahepatic manifestations of HCV in 2014 US dollars, were estimated to be $1506 million (range, $922 million $2208 million in sensitivity analysis) These estimates should be added to the liverrelated burden of disease to obtain a more accurate assessment of the total burden of HCV infection
5 Direct medical costs of extrahepatic manifestations of HCV in EUROPE


6 ISG-EHCV Ferri C, Ramos-Casals M, Zignego AL, et al, Autoimmun Rev 2016

7




8 These results, for the first time showed the real-life variability of the MC diagnostic approach, suggesting that MC prevalence in HCV+ is generally underestimated Total Piter cohort no subjects: the presence of MC was never tested in 80% of cases in spite of its clinical and therapeutical importance. Among the centres that considered MC= -64% evaluated cryoglobulinemia only following a clinical suspicion -58% evaluated routinely cryoglobulinemia at admission with Complement / RF levels -42% only in case of RF positivity -Cryo testing was not adequate in 39% of centres Kondili et al, Liver Intern.2017
 Endocrinologic: Thyroid and DM 2")
9 CLASSIFICATION OF HCV EHDS ACCORDING TO THE STRENGTH OF SPECIFIC DATA SUPPORTING THE CURATIVE EFFECT OF AVT Mixed Cryoglobulinemia* Effectiveness of both IFN-based and IFNfree AVT Marginal Zone NHL Effectiveness of both IFN- and DAA-based AVT Other low-grade B-cell NHL // HRQOL High-grade NHL= DLBCL CKD Neuropsychiatric disorders Curaneous= PCT and LP (OLP) Endocrinologic: Thyroid and DM 2 Available data also in DAA-based AVT Insufficient, but positive data Sufficient specific data only for MC-CKD* Problematic IFN-based AVT; Insufficient data with DAAs Problematic IFN/RBV-based AVT; Insufficient data with DAAs Insufficient specific data with DAAs Zignego et al. 2017
10 Antiviral Treatment (AVT) of MC in the IFN Era AVT of MC followed the evolution of hepatitis C AVT with frequent adjustments essentially due to the possible side-effects of IFN and/or RBV therapy (i.e. IFN neurotoxicity and myelo-inhibitory action and RBV hemolytic effects) Virological and clinical results progressively improved in spite of frequent side-effects Clinical remission was generally correlated with virological response IFN-based AVT was recommended as the first-line option in mild to moderate MC Long follow-up showed that the majority (57%) of SVR pts cleared all MC stigmata Landau DA, et al. Arthritis Rheum 2008; Montalbano M, et al. J Clin Gastroenterol 2007; Cacoub P, et al. Arthritis Rheum 2002; Mazzaro C, et al..j Rheumatol 2003; Zignego AL, et al Hepatology 2016; Gragnani L, et al. Hepatology 2015; Pietrogrande M, et al. Autoimmun Rev 2011.
 and low rates of serious adverse events was reported Zignego AL, Ramos-Casals M, Ferri C et al, Autoimmun.")
11 Antiviral Treatment (AVT) of MC: IFN-free regimens Limited data, so-far concordant, are available regarding IFN-free AVT in MC patients Available data suggest that IFN-free AVT is safe, generally well tolerated and effective in MC patients: high rate of clinical response (87%) and low rates of serious adverse events was reported Zignego AL, Ramos-Casals M, Ferri C et al, Autoimmun.Reviews 2017
 and 65 asymptomatic MC treated with DAAs. SVR: 88.")
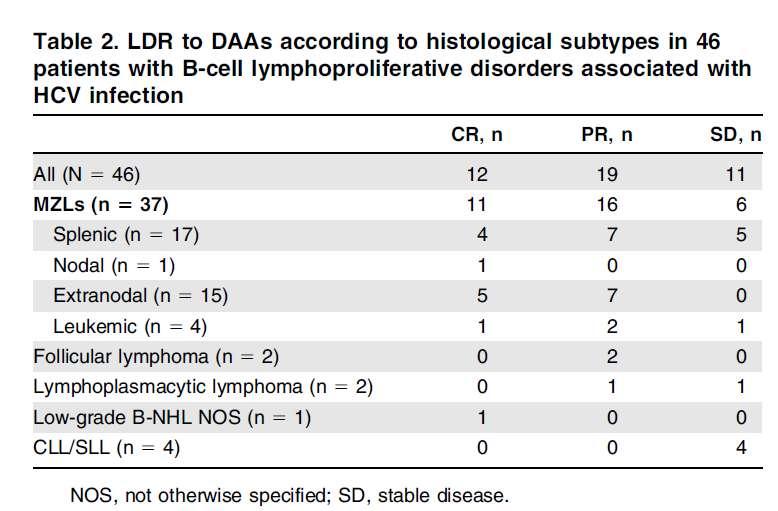
12 Antiviral Treatment (AVT) of MC: IFN-free regimens Lauletta et al, MCS treated with DAAs, including 2 HCC and 2 NHL. 100% SVR12. Clinical R in 100% (64% CR and 36% PR). Progression of the small lymphocytic lymphoma. Emery CS et al, 2017 Retrospective analysis: 17 MCS (10 with severe/life-threatening vasculitis) and 65 asymptomatic MC treated with DAAs. SVR: 88.9% MCS and 90.8% asymptomatic pts. In MCS clinical R in 11/17 (CR in 7/11) Lower clinical R in severe/life-threatening especial renal and neurological- vasculitis Saadoun D et al, 2017 Open-label, prospective, multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS. SVR in 100% and clinical CR in 90.2% Disappearance of CGs in 50% of pts. No serious adverse event or relapse of vasculitis. Fumiaki et al, 2017 A case of rapid amelioration of HCV-associated cryoglobulinemic MPGN treated by IFN-free DAAs for HCV in the absence of immunosuppressant
13 Zignego et al. 2017

 Health Survey (SF-36); the Functional Assessment of Chronic Illness")

14 Gragnani et al. AASLD 2017 Evaluation of The Impact on HRQol of IFN-free AVT In HCV CM TIME POINTS baseline, EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively) HRQoL EVALUATION THROUGH PROs the Short Form (36) Health Survey (SF-36); the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial Outcome Index (TOI) **=p<0.01 vs baseline scores; =p<0.01 and =p<0.001 vs EOT scores 1. Physical Component Summary Score (PCS) A HCV (43) B MC (54) C CV (85) * ** ** * 2. Mental Component Summary Score (MCS) HCV D HCV E MC F CV ** ***



15 MCS Therapy in the IFN and DAAs Era: from the complex to the simplified flow-chart HCV Eradication with DAAs To be preceded or combined with non-etiological, pathogenetic therapy in severe/catastrophic MCS Dammacco F, Sansonno D, NEJM 2013 Zignego AL, Pawlotsky JM, Cacoub P, Antiviral Ther, in press; Cacoub P et al, Am J Med 2015

16 Mechanisms of HCV-related lymphomagenesis DLBC: HCV- induced direct transformation? MC/indolent NHL: accumulation of B RF following BCR activation and BC apoptosis inhibition? Zignego AL, Ramos-Casals M, Ferri C et al, Autoimmun. Rev. 2017; Wang et al. Hepatology. 2016; Canioni et al, Plos one. 2016
17 NS3 immunostaining positive in 12/14 DLBCL vs only 4/14 MZL (p = 0.006); moreover, 2/4 NS3+ MZL were enriched in large cells This study supports a new mechanism of transformation with a direct oncogenic role of HCV proteins in the occurrence of high-grade B lymphomas IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS. Danielle Canioni et al 2016 In addition to the role of chronic antigenic stimulation in HCV related lymphomagenesis, this study supports a second mechanism of transformation due to a direct oncogenic role of HCV infection of B-cells promoting the occurrence of highgrade Bcell lymphomas Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36% and MZL 34%)

18 Cohort study of 704 consecutive HIV-negative, HCV-positive patients with indolent NHL from 1993 to 2009 in 39 centers of the FIL

19 Arcaini et al. 2016

20 THERAPY OF HCV+ DLBCL DLBC: HCV- induced direct transformation? No place of AVT as 1st line! Need of immediate delivery of chemotherapy or concomitant (NHL + HCV targets)!
21

22 ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTER SURVIVAL IN PATIENTS WITH HCV AND B-CELL NON- HODGKIN LYMPHOMAS, ANRS HC-13 LYMPHO-C STUDY Michot JM et al Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5 64)
23 Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C. Ewers et al, 2016 absolute neutrophil count and Hgb ALT and HCV viral load Both complete response and SVR of HCV-associated DLBCL, after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen
24 DAA-treatment in concomitance with chemotherapy showed to be safe and effective in influencing the remission of aggressive lymphomas in HCV patients Persico M et al, 2017 Antiviral response rates in DAA treated patients DFS in DAA treated and historical, not-treated pts
25 ANTIVIRAL THERAPY IN HCV+ B CELL NHL IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially MZL) Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional treatment (i.e., systemic symptoms, bulky disease or symptomatic splenomegaly) (ESMO, NCCN,EASL guidelines) In aggressive lymphomas antiviral therapy after induction treatment is to be considered the standard at the moment, but in the next years (months), the association of immunochemotherapy and antiviral therapy will be considered the standard! Zignego AL, Ramos-Casals M, Ferri C et al, Autoimmun. Rev. 2017


26 The Masve group BASIC RESEARCH Laura Gragnani Patrizio Caini Serena Lorini Antonella Simone Università degli Studi di Firenze Dipartimento di Medicina Sperimentale e Clinica Centro Manifestazioni Sistemiche da Virus Epatitici MASVE Anna Linda Zignego MASVE CLINICAL RESEARCH Monica Monti Luisa Petraccia Sinan Sadalla Guia Cerretelli Cristina Stasi Adela Xheka UNDERGRADUATE STUDENTS: Andrea Genovese, Adrian Piscopo
27
28
29
30
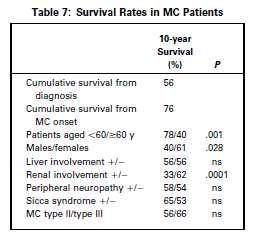
31
 Recent data with IFN-free regimens in HCV-associated LPDs suggest their")
 (ESMO, NCCN, EASL guidelines)")
32 ANTIVIRAL THERAPY IN HCV+ B CELL NHL IFN-based AVT induced hematological response along with SVR in patients with HCV-related indolent NHLs (especially MZL) Recent data with IFN-free regimens in HCV-associated LPDs suggest their anti-lymphoma activity too AVT should be considered the first-line approach in HCV low grade lymphomas if there is no urgency of a conventional treatment (i.e., systemic symptoms, bulky disease or symptomatic splenomegaly) (ESMO, NCCN, EASL guidelines)
33 Main drugs for HCV-related MCS according to the target HCV= DAAs B-cell Expansion= (a) B cell-depleting Mabs -First-generation: Rituximab (anti-cd20) -Second-generation: Ofatumumab (anti-cd20); Veltuzumab (humanized anti-cd20) -Third-generation: Obinutuzumab (GA101); Oceratuzumab (humanized anti-cd20) Inflammation= (b) Alkylating agents -Cyclophosfamide Antiinflammatory agents Altered regulatory T-cell activity= - Corticosteroids - IL-2
 and naïve (30), treated with SOF/RBV for 12/24wks.")
34 The impact on HRQoL of IFN-free AVT was prospectively evaluated in a cohort of HCV CV patients with limited influencing variables linked to therapeutic schedules/viral GT: 44 HCV GT2 CV patients, mostly F0-F2 (29) and naïve (30), treated with SOF/RBV for 12/24wks. TIME POINTS baseline, EOT and week 12 and 24 of post-treatment f-up (SVR12 and SVR24 respectively) HRQoL EVALUATION THROUGH PROs the Short Form (36) Health Survey (SF-36); the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) from which we computed the Trial Outcome Index (TOI)

35 IN SITU HEPATITIS C NS3 PROTEIN DETECTION IS ASSOCIATED WITH HIGH GRADE FEATURES IN HCV-ASSOCIATED B-CELL NON-HODGKIN LYMPHOMAS. Danielle Canioni et al 2016 In addition to the role of chronic antigenic stimulation in HCV related lymphomagenesis, this study supports a second mechanism of transformation due to a direct oncogenic role of HCV infection of B-cells promoting the occurrence of highgrade Bcell lymphomas Observational study on in situ expression of the oncogenic HCV NS3 protein on 116 HCV patients with B-NHL (DLBCL 36% and MZL 34%) NS3 immunostaining positive in 12/14 DLBCL vs only 4/14 MZL (p = 0.006); moreover, 2/4 NS3+ MZL were enriched in large cells This study supports a new mechanism of transformation with a direct oncogenic role of HCV proteins in the occurrence of high-grade B lymphomas
36


37 ANTIVIRAL THERAPY IS ASSOCIATED WITH A BETTER SURVIVAL IN PATIENTS WITH HCV AND B-CELL NON- HODGKIN LYMPHOMAS, ANRS HC-13 LYMPHO-C STUDY Michot JM et al Outcomes of HCV-associated B-NHL according to HCV AVT in prospective patients only (n 5
38 Concurrent Systemic Chemoimmunotherapy and Sofosbuvir-Based Antiviral Treatment in a Hepatitis C Virus-Infected Patient With Diffuse Large B-Cell Lymphoma Evan C. Ewers et al, 2016 (A) absolute neutrophil count and Hgb (B) ALT and HCV viral load This patient had HCV-associated DLBCL, achieving both complete response and SVR after concurrent chemoimmunotherapy and antiviral therapy using a sofosbuvir-based regimen.
39 Cumulative Mortality (%) Extrahepatic Manifestations of HCV HCV-EHDs are responsible for increasing morbidity and mortality, with important consequences in terms of social costs The analysis of mortality rates in large cohorts confirmed the association of HCV with several EHDs including cardiovascular, neurologic, metabolic or renal diseases and tumors Viral eradication significantly reduced the rate of extra-hepatic deaths Anti-HCV+, HCV RNA detectable Anti-HCV+, HCV RNA undetectable Anti-HCV All Causes (n=2394) Follow-Up (Years) 30.1%* 12.8% 12.4% Liver Cancer (n=115) 0.3% Follow-Up (Years) 10.4%* (Years) Con il contributo di Cacoub P, et al. DLD 2014; Lee MH, et al J Infect Dis 2012; Backus LI, et al. Clin Gastroenterol Hepatol 2011; El-Kamary S, et al. Clin Infect Dis 2011; Hsu YC, et al. Hepatology 2014; Kawamura Y, et al. Am J Med 2007; Adinolfi LE, et al. WJG % Lee M-H, et al. J Infect Dis. 2012;206: Extrahepatic Diseases (n=2199) Follow-Up 19.8%* 12.2% 11.0%
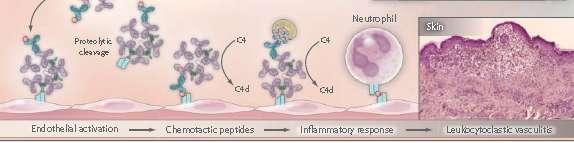
40 MC is clinically benign, but sometimes severe HCV EHD; invalidating symptoms occur and it may evolve into lymphoma Mixed Cryoglobulinemia-MC CGs reversibly precipitate when the temperature is lower than 37 C and comprise IgMs with RF activity [mono- or oligo-clonal in type II MC, or polyclonal in type III MC] and polyclonal IgGs MC pathological substrate is an HCV-driven B-cell proliferation with consequent production of cryo- and noncryoprecipitable CICs, in turn responsible for vasculitic manifestations Most (70 90%) MC patients are HCV+ and HCV-patients are CGs+ (40 60%), while 5 30% of CGs+ have symptomatic MC: since HCV infects about 170 million individuals worldwide, the number of patients at risk for developing MC is substantial Type II CGs Type III CGs Cacoub P, et al. DLD 2014; Zignego AL, et al. DLD 2007; Zignego AL, et al. Intern Emerg Med 2012; Zignego AL, et al. Clin Dev Immunol 2012; Zignego AL, et al. Expert Rev Clin Immunol 2015; Sene D, et al. J Rheumatol 2004.
41

42 MC clinical aspects: MC Syndrome MCS is characterized by the clinical triad -purpura, weakness, and arthralgias-, low complement C4 and various organ/system involvement, including cutaneous, articular, renal, neurological, cardiac or digestive It ranges from mild disease to severe, even life-threatening conditions More serious lesions are generally characterized by neurologic and renal involvement Prognosis is highly dependent on renal involvement or on the extent of vasculitis lesions Zignego AL et al, Autoimmun Rev, 2017; Ferri C et al, Autoimmunity rev. 2016; Zignego AL, et al. DLD 2007; Cacoub P, et al. DLD 2014; Zignego AL, et al. DLD 2007; Zignego AL, et al. Intern Emerg Med 2012; Zignego AL, et al. Clin Dev Immunol 2012; Zignego AL, et al. Expert Rev Clin Immunol 2015.


43 1: HCV is the From main P etiopathological Cacoub, 2015 agent as concordantly demonstrated by epidemiological, clinico-pathological, virological, and laboratory investigations 2: the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogenetic studies; 3: the association is suggested by cohort studies; a possible causative role may be limited to a small number of patients and/or possibly more relevant in specific geographical areas; 4: a number of anecdotal observations suggested a possible role of HCV; further investigations are required

44 HCV and MC HCV and MC HCV infection is closely related to LPDs, mostly MC 40 to 60% of HCV patients show circulating CGs; among this latter population, 5-30% develop a symptomatic CV AVT has been considered the first-line option in HCV-CV patients; in fact, in the majority of cases, viral eradication leads to CV clinical remission Data about IFN-free regimens for the treatment of CV patients are still limited Zignego, 2015;Ferri, 2016;Pozzato, 2016; Sise, 2016;Saadoun, 2015;Gragnani, 2016;Gragnani, 2016; Bonacci, 2016;Hegazy, 2016;Kondili 2016;Emery, 2017.
45 Younossi et al The annual costs (inpatient, outpatient, and pharmacy) associated with extrahepatic manifestations of HCV were evaluated Total direct medical costs of extrahepatic manifestations of HCV in 2014 US dollars, were estimated to be $1506 million (range, $922 million $2208 million in sensitivity analysis) These estimates should be added to the liver-related burden of disease to obtain a more accurate assessment of the total burden of HCV infection
46 The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France, Germany, Italy, United Kingdom, Spain)
47 Extrahepatic Manifestations of HCV
48
, classified according to the number and strength of supporting")
49 Extrahepatic Manifestations of HCV HCV may cause extrahepatic disorders (HCV-EHDs), classified according to the number and strength of supporting scientific data
50 Cumulative Mortality (%) HCV-EHDs are responsible for increasing morbidity and mortality, with important consequences in terms of social costs The analysis of mortality rates in large cohorts confirmed the association of HCV with several EHDs including cardiovascular, neurologic, metabolic or renal diseases and tumors Viral eradication significantly reduced the rate of extra-hepatic deaths Anti-HCV+, HCV RNA detectable Anti-HCV+, HCV RNA undetectable Anti-HCV All Causes (n=2394) Extrahepatic Manifestations of HCV Follow-Up (Years) 30.1%* 12.8% 12.4% Liver Cancer (n=115) 0.3% Follow-Up (Years) 10.4%* (Years) Con il contributo di Cacoub P, et al. DLD 2014; Lee MH, et al J Infect Dis 2012; Backus LI, et al. Clin Gastroenterol Hepatol 2011; El-Kamary S, et al. Clin Infect Dis 2011; Hsu YC, et al. Hepatology 2014; Kawamura Y, et al. Am J Med 2007; Adinolfi LE, et al. WJG % Lee M-H, et al. J Infect Dis. 2012;206: Extrahepatic Diseases (n=2199) Follow-Up 19.8%* 12.2% 11.0%
51 Younossi et al The annual costs (inpatient, outpatient, and pharmacy) associated with extrahepatic manifestations of HCV were evaluated Total direct medical costs of extrahepatic manifestations of HCV in 2014 US dollars, were estimated to be $1506 million (range, $922 million $2208 million in sensitivity analysis) These estimates should be added to the liver-related burden of disease to obtain a more accurate assessment of the total burden of HCV infection
 had an annual cost of $443.")
52 Younossi et al Costs up to $71,000 per patient per year (ESRD) Among the most frequent EHM, depression (24.5% in HCV vs 17.2 % in non-hcv) had estimated annual cost of $430.7 million DM (15% vs 10% in non- HCV) had an annual cost of $443.4 million in the USA= given the importance of DM and its association with CVDs and mortality, the clinical and economic impacts of HCV-related DM are substantial
53 The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France, Germany, Italy, United Kingdom, Spain)
54 The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France, Germany, Italy, United Kingdom, Spain)
55 The most studied and frequent HCV-EHDs are B-LPDs and/or autoimmune disorders 1: HCV is the main etiopathological agent as concordantly demonstrated by epidemiological, clinico-pathological, virological, and laboratory investigations 2: the association between HCV and disease is demonstrated in a significant proportion of patients and supported by in depth clinico-pathogenetic studies; 3: the association is suggested by cohort studies; a possible causative role may be limited to a small number of patients and/or possibly more relevant in specific geographical areas; 4: a number of anecdotal observations suggested a possible role of HCV; further investigations are required Their prototype is Mixed Cryoglobulinemia (MC): from researches on MC derived most of the available information: MC as a precious model for all the HCV-EHDs and to evaluate the effects of viral eradication.

56 Few side effects, absence major contraindications Standard interferon 1991 Anti-HCV Treatment Evolution Ribavirin Peginterferon Direct-acting antivirals > IFN 6 mos IFN 12 mos IFN/RBV 6 mos IFN/RBV 12 mos PegIFN 12 mos PegIFN/ RBV 12 mos PegIFN/ RBV/ DAA DAAs 8/26 weeks
57 Younossi et al The annual costs (inpatient, outpatient, and pharmacy) associated with extrahepatic manifestations of HCV were evaluated Total direct medical costs of extrahepatic manifestations of HCV in 2014 US dollars, were estimated to be $1506 million (range, $922 million $2208 million in sensitivity analysis) These estimates should be added to the liver-related burden of disease to obtain a more accurate assessment of the total burden of HCV infection
58 The OBJECTIVE of the study was to estimate the annual direct medical costs associated with HCV related EHM in the EU5 (France, Germany, Italy, United Kingdom, Spain)
59 Antiviral Treatment (AVT) of MC: IFN-free regimens Lauletta et al, MCS treated with DAAs, including 2 HCC and 2 NHL. 100% SVR12. Clinical CR in 64% and PR in remaining 36%. The small lymphocytic lymphoma progressed despite viral clearance. Saadoun D et al, 2017 Open-label, prospective, multi-center study on sofosbuvir plus daclatasvir treatment of 41 HCV MCS. SVR in 100% and clinical CR in 90.2% Disappearance of CGs in 50% of pts. No serious adverse event or relapse of vasculitis. Emery CS et al, 2017 Retrospective analysis: 17 MCS (10 with severe/life-threatening vasculitis) and 65 asymptomatic CGs+ pts treated with DAAs. SVR: 88.9% MCS and 90.8% asymptomatic pts. In MCS clinical response in 11/17 (complete in 7/17) In severe/life-threatening vasculitis, lower clinical response, especially in renal and neurological symptoms
60 Mixed Cryoglobulinemia-MC MC is clinically benign, but sometimes severe HCV EHD; invalidating symptoms occur and it may evolve into lymphoma MC pathological substrate is an HCV-driven B-cell proliferation with consequent production of cryo- and noncryoprecipitable CICs, in turn responsible for vasculitic manifestations Type II CGs: monoclonal RF+policlonal IgG Type III CGs: both RF and IgG polyclonal Most (70 90%) MC patients are HCV+ and HCV-patients are CGs+ (40 60%), while 5 30% of CGs+ have symptomatic MC or cryoglobulinemic vasculitis: since HCV infects about 170 million individuals worldwide, the number of patients at risk for developing MC is substantial Cacoub P, et al. DLD 2014; Zignego AL, et al. DLD 2007; Zignego AL, et al. Intern Emerg Med 2012; Zignego AL, et al. Clin Dev Immunol 2012; Zignego AL, et al. Expert Rev Clin Immunol 2015; Sene D, et al. J Rheumatol 2004.
This is an AbbVie sponsored educational webinar which is being presented
 Presented by Joseph Lim, MD April 5 th, 2017 AbbVie disclosures This is an AbbVie sponsored educational webinar which is being presented by Joseph Lim, MD, on behalf of AbbVie The purpose of the medical
Presented by Joseph Lim, MD April 5 th, 2017 AbbVie disclosures This is an AbbVie sponsored educational webinar which is being presented by Joseph Lim, MD, on behalf of AbbVie The purpose of the medical
Management of Extrahepatic Manifestations of Hepatitis C Virus in the Era of DAA
 Management of Extrahepatic Manifestations of Hepatitis C Virus in the Era of DAA Pr Patrice CACOUB, MD Dept of Internal Medicine and Clinical Immunology CNRS UMR 7087, INSERM UMR S-959, DHU I2B Université
Management of Extrahepatic Manifestations of Hepatitis C Virus in the Era of DAA Pr Patrice CACOUB, MD Dept of Internal Medicine and Clinical Immunology CNRS UMR 7087, INSERM UMR S-959, DHU I2B Université
Professor Patrice Cacoub
 Five Nations Conference on HIV and Hepatitis in partnership with Professor Patrice Cacoub La Pitié-Salpêtrière Hospital, Paris, France HCV and its Extra Hepatic Manifestations: From Immune- to Inflammatory-Related
Five Nations Conference on HIV and Hepatitis in partnership with Professor Patrice Cacoub La Pitié-Salpêtrière Hospital, Paris, France HCV and its Extra Hepatic Manifestations: From Immune- to Inflammatory-Related
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient. Konstantin Zhdanov
 Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain
 Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain Disclosures Advisory boards and speaker s bureau for: Gilead, Merck,
Is prioritization the best way to treat hepatitis C? Vicente Soriano Infectious Diseases Unit La Paz University Hospital Madrid, Spain Disclosures Advisory boards and speaker s bureau for: Gilead, Merck,
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Should Elderly CHC Patients (>70 years old) be Treated?
 be Treated?") Should Elderly CHC Patients (>70 years old) be Treated? Deepak Amarapurkar Consultant Gastroenterologist & Hepatologist Bombay Hospital & Medical Research Center, Mumbai & Jagjivanram Western Railway Hospital,
Should Elderly CHC Patients (>70 years old) be Treated? Deepak Amarapurkar Consultant Gastroenterologist & Hepatologist Bombay Hospital & Medical Research Center, Mumbai & Jagjivanram Western Railway Hospital,
Department of Internal Medicine, Pordenone General Hospital, Italy; 2
 Le Infezioni in Medicina, n. 4, 337-341, Caso clinico Case reports Recombinant Human Erythropoietin (RHuEpo) and Granular Colony Stimulating Factor (G-CSF) in hepatitis C virus (HCV) related to mixed cryoglobulinaemia
Le Infezioni in Medicina, n. 4, 337-341, Caso clinico Case reports Recombinant Human Erythropoietin (RHuEpo) and Granular Colony Stimulating Factor (G-CSF) in hepatitis C virus (HCV) related to mixed cryoglobulinaemia
Hepatitis C Management and Treatment
 Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
Correspondence should be addressed to Anna Linda Zignego;
 Case Reports in Immunology Volume 2015, Article ID 816424, 5 pages http://dx.doi.org/10.1155/2015/816424 Case Report Combined Treatment with Antiviral Therapy and Rituximab in Patients with Mixed Cryoglobulinemia:
Case Reports in Immunology Volume 2015, Article ID 816424, 5 pages http://dx.doi.org/10.1155/2015/816424 Case Report Combined Treatment with Antiviral Therapy and Rituximab in Patients with Mixed Cryoglobulinemia:
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
La sindrome metabolica e il suo impatto dopo la guarigione nel paziente HIV/HCV
 WORKSHOP HCV: la guarigione e il parallelismo tra risposta virologica sostenuta e outcome clinico Milano, 25 Ottobre 2018 Ospedale San Raffaele IRCCS - Sede Turro La sindrome metabolica e il suo impatto
WORKSHOP HCV: la guarigione e il parallelismo tra risposta virologica sostenuta e outcome clinico Milano, 25 Ottobre 2018 Ospedale San Raffaele IRCCS - Sede Turro La sindrome metabolica e il suo impatto
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Chronic viral hepatitis and liver disease in Belgium Pierre Deltenre
 Chronic viral hepatitis and liver disease in Belgium Pierre Deltenre Brussels, November 7, 2017 Hepatitis B and C in Belgium What we need to know 1. Who is at risk of infection? 2. What is the natural
Chronic viral hepatitis and liver disease in Belgium Pierre Deltenre Brussels, November 7, 2017 Hepatitis B and C in Belgium What we need to know 1. Who is at risk of infection? 2. What is the natural
2.0 Synopsis. ABT-450/r, ABT-267 M Clinical Study Report R&D/17/0539. (For National Authority Use Only)
") 2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-450, ritonavir, ABT-267, ribavirin, pegylated interferon Name of Active Ingredient: ABT-450, Ritonavir, ABT-267, Ribavirin, Pegylated interferon Individual
2.0 Synopsis AbbVie Inc. Name of Study Drug: ABT-450, ritonavir, ABT-267, ribavirin, pegylated interferon Name of Active Ingredient: ABT-450, Ritonavir, ABT-267, Ribavirin, Pegylated interferon Individual
HEPATITIS C UPDATES. Sanaa S. Said 10 th April, 2014
 HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
HEPATITIS C UPDATES Sanaa S. Said 10 th April, 2014 CONTENTS Introduction Epidemiology Transmission and Natural history Kenyan guidelines What is new? References INTRODUCTION Hepacivirus genus, Flaviviridae
The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (1), Page
 Vol. 73 (1), Page") The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (1), Page 5743-5747 Impact of Direct Acting Antiviral Drugs (DAADs) on Cognitive function among Hepatitis C Virus Infected Patients Hassan
The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (1), Page 5743-5747 Impact of Direct Acting Antiviral Drugs (DAADs) on Cognitive function among Hepatitis C Virus Infected Patients Hassan
A Practical Guide to Hepatitis C Management
 A Practical Guide to Hepatitis C Management David C. Wolf, M.D., FACP, FACG, AGAF Medical Director of Liver Transplantation Westchester Medical Center Professor of Clinical Medicine New York Medical College
A Practical Guide to Hepatitis C Management David C. Wolf, M.D., FACP, FACG, AGAF Medical Director of Liver Transplantation Westchester Medical Center Professor of Clinical Medicine New York Medical College
Impatto della clearance virale e rischio di carcinoma epatocellulare
 EPATITE CRONICA DA HCV: Impatto della clearance virale e rischio di carcinoma epatocellulare Rodolfo Sacco, M.D., PhD Direttore U.O.C. Gastroenterologia ed Endoscopia Digestiva A.O.U. Ospedali Riuniti"
EPATITE CRONICA DA HCV: Impatto della clearance virale e rischio di carcinoma epatocellulare Rodolfo Sacco, M.D., PhD Direttore U.O.C. Gastroenterologia ed Endoscopia Digestiva A.O.U. Ospedali Riuniti"
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Personalizzazione della Cura in Epatologia. Epatite Cronica C: Pazienti con Genotipo 2
 Monotematica AISF 213 Personalizzazione della Cura in Epatologia Pisa, 17-19 Ottobre 213 Epatite Cronica C: Pazienti con Genotipo 2 Maria Grazia Rumi U.O. Epatologia, Ospedale San Giuseppe Università degli
Monotematica AISF 213 Personalizzazione della Cura in Epatologia Pisa, 17-19 Ottobre 213 Epatite Cronica C: Pazienti con Genotipo 2 Maria Grazia Rumi U.O. Epatologia, Ospedale San Giuseppe Università degli
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
The impact of the treatment of HCV in developing Hepatocellular Carcinoma
 The impact of the treatment of HCV in developing Hepatocellular Carcinoma Paul Y Kwo, MD Professor of Medicine Medical Director, Liver Transplantation Gastroenterology/Hepatology Division Indiana University
The impact of the treatment of HCV in developing Hepatocellular Carcinoma Paul Y Kwo, MD Professor of Medicine Medical Director, Liver Transplantation Gastroenterology/Hepatology Division Indiana University
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
HEPATITIS C TREATMENT UPDATE
 HEPATITIS C TREATMENT UPDATE Hepatitis C: Burden of Disease in USA HCV is generally asymptomatic until advanced liver disease 4.1 million persons ever infected; 3.2 million chronic infections Up to 75%
HEPATITIS C TREATMENT UPDATE Hepatitis C: Burden of Disease in USA HCV is generally asymptomatic until advanced liver disease 4.1 million persons ever infected; 3.2 million chronic infections Up to 75%
1.0 Abstract. Title. Keywords
 1.0 Abstract Title Real World Evidence of the Effectiveness of Paritaprevir/r Ombitasvir, ± Dasabuvir, ± Ribavirin in Patients with Chronic Hepatitis C - An Observational Study in Austria (REAL) Keywords
1.0 Abstract Title Real World Evidence of the Effectiveness of Paritaprevir/r Ombitasvir, ± Dasabuvir, ± Ribavirin in Patients with Chronic Hepatitis C - An Observational Study in Austria (REAL) Keywords
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Hepatitis: A Global Health. Concern
 Chapter 5 Hepatitis: A Global Health Extra-Hepatic Manifestations of Hepatitis C Virus Infection Clodoveo Ferri*; Michele Colaci 1 ; DiliaGiuggioli 1 1 Rheumatology Unit, University of Modena and Reggio
Chapter 5 Hepatitis: A Global Health Extra-Hepatic Manifestations of Hepatitis C Virus Infection Clodoveo Ferri*; Michele Colaci 1 ; DiliaGiuggioli 1 1 Rheumatology Unit, University of Modena and Reggio
Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London
 Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London IFN free therapy Disclosures I have received personal and institutional funding from companies that sell drug
Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London IFN free therapy Disclosures I have received personal and institutional funding from companies that sell drug
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
ANTIVIRAL THERAPY FOR HCV. Alfredo Alberti
 CLINICAL IMPACT OF SVR AFTER ANTIVIRAL THERAPY FOR HCV Alfredo Alberti Department of Histology,Microbiology and Medical Biotechnologies Molecular Hepatology Unit Venetian Institute of Molecular Medicine
CLINICAL IMPACT OF SVR AFTER ANTIVIRAL THERAPY FOR HCV Alfredo Alberti Department of Histology,Microbiology and Medical Biotechnologies Molecular Hepatology Unit Venetian Institute of Molecular Medicine
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
Hepatitis C: New Antivirals in the Liver Transplant Setting. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Intron A Hepatitis B. Intron A (interferon alfa-2b) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.01 Subject: Intron A Hepatitis B Page: 1 of 7 Last Review Date: November 30, 2018 Intron A Hepatitis
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.01 Subject: Intron A Hepatitis B Page: 1 of 7 Last Review Date: November 30, 2018 Intron A Hepatitis
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Olysio (simeprevir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/9/2014 1. Indications Drug Name: Olysio
Prior Authorization Guideline Guideline Name Olysio (simeprevir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/9/2014 1. Indications Drug Name: Olysio
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
HCV Viremia Was Associated With Increased Mortality in a Prospective Taiwanese Cohort Study
 Tram T. Tran, MD, FACG Approach to HCV Treatment in Patients with HCC Tram T. Tran, MD, FACG Professor of Medicine Medical Director, Liver Transplant Cedars Sinai Medical Center Natural History of HCV
Tram T. Tran, MD, FACG Approach to HCV Treatment in Patients with HCC Tram T. Tran, MD, FACG Professor of Medicine Medical Director, Liver Transplant Cedars Sinai Medical Center Natural History of HCV
Virological Tools and Monitoring in the DAA Era
 Virological Tools and Monitoring in the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Virological Tools and Monitoring in the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
HCV Treat now! Robert G Gish MD. Professor Consultant Stanford University
 HCV Treat now! Robert G Gish MD Professor Consultant Stanford University Steering committee and Executive Board NVHR National Viral Hepatitis Roundtable Founding Member CEVHAP Singapore Viral Hepatitis
HCV Treat now! Robert G Gish MD Professor Consultant Stanford University Steering committee and Executive Board NVHR National Viral Hepatitis Roundtable Founding Member CEVHAP Singapore Viral Hepatitis
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity. Cody A. Chastain, MD
 Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
Hepatitis C in Correctional Facilities: Big Problem, Bigger Opportunity Cody A. Chastain, MD Disclosures Research supported by Gilead Sciences Inc.: Site investigator for HIV/HCV SWITCH Registry Study
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Clinical Cases Hepatitis C Naïve Patients. Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona.
 Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Direct acting anti-virals: the near future
 Direct acting anti-virals: the near future Heiner Wedemeyer Hannover Medical School Germany Will IFN-free treatment be possible in the near future? Interferon-free regimens to treat hepatitis C What should
Direct acting anti-virals: the near future Heiner Wedemeyer Hannover Medical School Germany Will IFN-free treatment be possible in the near future? Interferon-free regimens to treat hepatitis C What should
Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1
 Phase 3 Treatment-Naïve and Treatment-Experienced Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1 EXPEDITION-1: Study Features EXPEDITION-1 Trial Design: Open-label, single-arm,
Phase 3 Treatment-Naïve and Treatment-Experienced Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1 EXPEDITION-1: Study Features EXPEDITION-1 Trial Design: Open-label, single-arm,
CHRONIC HCV TREATMENT: In Special Populations.
 CHRONIC HCV TREATMENT: In Special Populations. By Taher EL-ZANATY Prof. of Internal Medicine CAIRO UNIVERSITY Introduction: HCV is the major cause of chronic hepatitis in Egypt. Its end stage is liver
CHRONIC HCV TREATMENT: In Special Populations. By Taher EL-ZANATY Prof. of Internal Medicine CAIRO UNIVERSITY Introduction: HCV is the major cause of chronic hepatitis in Egypt. Its end stage is liver
Hepatitis C. Core slides
 Hepatitis C Core slides This material was prepared by the Viral Hepatitis Prevention Board The slides (or subsets) can be reproduced for educational use only, with reference to the original source and
Hepatitis C Core slides This material was prepared by the Viral Hepatitis Prevention Board The slides (or subsets) can be reproduced for educational use only, with reference to the original source and
Treatment of Hepatitis C in HIV-Coinfected Patients. Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain
 Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Approach to HCV Treatment in Patients with HCC Mark W. Russo, MD, MPH, FACG Carolinas HealthCare System Charlotte Worldwide Causes of HCC 60% 50% 40% 30% 20% 10% 0% 54% 31% 15% Hepatitis B Hepatitis C
Worldwide Causes of HCC
 Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Approach to HCV Treatment in Patients with HCC JORGE L. HERRERA, MD, MACG UNIVERSITY OF SOUTH ALABAMA COLLEGE OF MEDICINE Worldwide Causes of HCC 60% 50% 40% 54% 30% 20% 10% 31% 15% 0% Hepatitis B Hepatitis
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR
 Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis C No Barriers to Cure
 2018 Digestive Diseases Conference Kansas Hepatitis C No Barriers to Cure Dr. Mauricio Lisker Melman Professor of Medicine Director Hepatology Program Division of Gastroenterology Disclosure The following
2018 Digestive Diseases Conference Kansas Hepatitis C No Barriers to Cure Dr. Mauricio Lisker Melman Professor of Medicine Director Hepatology Program Division of Gastroenterology Disclosure The following
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
CURRENT TREATMENTS. Mitchell L Shiffman, MD Director Liver Institute of Virginia. Richmond and Newport News, VA, USA
 CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
Treatment of Hepatitis C and Renal Disease
 Treatment of Hepatitis C and Renal Disease David E. Bernstein, MD, FACG Vice Chair of Medicine for Clinical Trials Chief, Division of Hepatology and Director, Sandra Atlas Bass Center for Liver Diseases
Treatment of Hepatitis C and Renal Disease David E. Bernstein, MD, FACG Vice Chair of Medicine for Clinical Trials Chief, Division of Hepatology and Director, Sandra Atlas Bass Center for Liver Diseases
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update in hepatitis C virus infection
 Update in hepatitis C virus infection Eoin Feeney Consultant in Infectious Diseases St. Vincent s University Hospital Overview Natural history Diagnosis, screening, staging Management Barriers going forward
Update in hepatitis C virus infection Eoin Feeney Consultant in Infectious Diseases St. Vincent s University Hospital Overview Natural history Diagnosis, screening, staging Management Barriers going forward
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
All Hands on Deck: Taking on Hepatitis C in Tennessee
 All Hands on Deck: Taking on Hepatitis C in Tennessee Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
All Hands on Deck: Taking on Hepatitis C in Tennessee Cody A. Chastain, MD Assistant Professor of Medicine Viral Hepatitis Program Division of Infectious Diseases Vanderbilt University Medical Center Cody.a.Chastain@Vanderbilt.edu
HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER LONDON
 HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER 2015 - LONDON The need Decreasing prevalence of chronic hepatitis C in French people living
HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER 2015 - LONDON The need Decreasing prevalence of chronic hepatitis C in French people living
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING. Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona
 TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
DISCLOSURES. This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Services
 DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Services Cardea Services is approved as a provider of continuing nursing education by Montana Nurses
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Services Cardea Services is approved as a provider of continuing nursing education by Montana Nurses
Hepatitis C 17 months experience with Sofosbuvir/Ledipasvir (Harvoni)
") Hepatitis C 17 months experience with Sofosbuvir/Ledipasvir (Harvoni) Prof. Dr. Markus Cornberg Klinik für Gastroenterologie, Hepatologie und Endokrinologie Antalya, 13.05.2016 Markus Cornberg, Hannover
Hepatitis C 17 months experience with Sofosbuvir/Ledipasvir (Harvoni) Prof. Dr. Markus Cornberg Klinik für Gastroenterologie, Hepatologie und Endokrinologie Antalya, 13.05.2016 Markus Cornberg, Hannover
10/4/2016. Management of Hepatitis C Virus Genotype 2 or 3 Infection
 Management of Hepatitis C Virus Genotype 2 or 3 Infection Kenneth E. Sherman, MD, PHD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati Cincinnati, Ohio FORMATTED:
Management of Hepatitis C Virus Genotype 2 or 3 Infection Kenneth E. Sherman, MD, PHD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati Cincinnati, Ohio FORMATTED:
ةي : لآا ةرقبلا ةروس
 سورة البقرة: اآلية HCV RELAPSERS AND NONRESPONDERS: How to deal with them? BY Prof. Mohamed Sharaf-Eldin Prof. of Hepatology and Gastroenterology Tanta University Achieving SVR The ability to achieve a
سورة البقرة: اآلية HCV RELAPSERS AND NONRESPONDERS: How to deal with them? BY Prof. Mohamed Sharaf-Eldin Prof. of Hepatology and Gastroenterology Tanta University Achieving SVR The ability to achieve a
DAA-based treatment in cirrhotic and post-transplanted patients. Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France
 DAA-based treatment in cirrhotic and post-transplanted patients Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France Cirrhosis and transplantation 2 populations with similar issues Hepatic impairment
DAA-based treatment in cirrhotic and post-transplanted patients Audrey Coilly, MD Hôpital Paul Brousse, Villejuif, France Cirrhosis and transplantation 2 populations with similar issues Hepatic impairment
Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine
 Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Supportive Care for NHL Tumor Lysis Syndrome (TLS) Laboratory hallmarks of TLS:
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Supportive Care for NHL Tumor Lysis Syndrome (TLS) Laboratory hallmarks of TLS:
ABCs of Viral Hepatitis What Primary Care Physicians Need to Know
 ABCs of Viral Hepatitis What Primary Care Physicians Need to Know Dr Kenny C.P. Sze Associate Consultant Division of Gastroenterology Department of General Medicine Outline and Keypoints Hepatitis A Recap;
ABCs of Viral Hepatitis What Primary Care Physicians Need to Know Dr Kenny C.P. Sze Associate Consultant Division of Gastroenterology Department of General Medicine Outline and Keypoints Hepatitis A Recap;
29th Viral Hepatitis Prevention Board Meeting
 29th Viral Hepatitis Prevention Board Meeting Madrid, November 2006 Treatment of chronic hepatitis C José M. Sánchez-Tapias Liver Unit Hospital Clínic University of Barcelona Spain CHRONIC HEPATITIS C
29th Viral Hepatitis Prevention Board Meeting Madrid, November 2006 Treatment of chronic hepatitis C José M. Sánchez-Tapias Liver Unit Hospital Clínic University of Barcelona Spain CHRONIC HEPATITIS C
Treatment of Hepatitis C Recurrence after Liver Transplantation. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
FINANCIAL DISCLOSURE
 FINANCIAL DISCLOSURE People who work at NIH only dream about having financial disclosures Wait, this just in. The US government has now banned dreaming CRITICAL NON-FINANCIAL DISCLOSURES Nothing I say
FINANCIAL DISCLOSURE People who work at NIH only dream about having financial disclosures Wait, this just in. The US government has now banned dreaming CRITICAL NON-FINANCIAL DISCLOSURES Nothing I say
Bristol-Myers Squibb. HCV Full Development Portfolio Overview. Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013
 Bristol-Myers Squibb HCV Full Development Portfolio Overview Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013 1 BMS Agents in Clinical Development: DAAs and INF Lambda Lambda
Bristol-Myers Squibb HCV Full Development Portfolio Overview Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013 1 BMS Agents in Clinical Development: DAAs and INF Lambda Lambda
EPIDEMIOLOGY, CLINICAL FEATURES AND OUTCOME OF ACUTE HEPATITIS C IN HIV-POSITIVE PATIENTS: PRESENTATION OF OUR EXPERIENCE
 EPIDEMIOLOGY, CLINICAL FEATURES AND OUTCOME OF ACUTE HEPATITIS C IN HIV-POSITIVE PATIENTS: PRESENTATION OF OUR EXPERIENCE E. Angeli, A. Mainini, C. Atzori, G. Gubertini and G. Rizzardini II Dept. Infectious
EPIDEMIOLOGY, CLINICAL FEATURES AND OUTCOME OF ACUTE HEPATITIS C IN HIV-POSITIVE PATIENTS: PRESENTATION OF OUR EXPERIENCE E. Angeli, A. Mainini, C. Atzori, G. Gubertini and G. Rizzardini II Dept. Infectious
SYNOPSIS Final Clinical Study Report for Study AI444031
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Name of Active Ingredient: () Individual Study Table Referring to the Dossier (For National Authority Use Only) SYNOPSIS for Study
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Name of Active Ingredient: () Individual Study Table Referring to the Dossier (For National Authority Use Only) SYNOPSIS for Study
The Dawn of a New Era: Hepatitis C
 The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
The Dawn of a New Era: Hepatitis C Naudia L. Jonassaint Assistant Professor of Medicine and Surgery University Pittsburgh School of Medicine December 1, 2015 Objectives After presentation the learner should
Health Without Barriers. HCV in prison Barriers to treatment, new Strategies and Outcomes
 Health Without Barriers The European Federation for Prison Health HCV in prison Barriers to treatment, new Strategies and Outcomes Roberto Monarca HWBs President Vice President of the Italian Society for
Health Without Barriers The European Federation for Prison Health HCV in prison Barriers to treatment, new Strategies and Outcomes Roberto Monarca HWBs President Vice President of the Italian Society for
Interferon-based and interferon-free new treatment options
 Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
How to optimize treatment for HCV Genotype 4
 How to optimize treatment for HCV Genotype 4 Paris Hepatitis Conference Pr Tarik Asselah 14 janvier 2014 MD, PhD Service d Hépatologie & INSERM U773 University Paris Diderot Hôpital Beaujon, Clichy tarik.asselah@bjn.aphp.fr
How to optimize treatment for HCV Genotype 4 Paris Hepatitis Conference Pr Tarik Asselah 14 janvier 2014 MD, PhD Service d Hépatologie & INSERM U773 University Paris Diderot Hôpital Beaujon, Clichy tarik.asselah@bjn.aphp.fr
HCV Treatment in 2016: is there still a role for IFNa and ribavirin?
 HCV Treatment in 2016: is there still a role for IFNa and ribavirin? Heiner Wedemeyer Hannover Medical School Germany 1 Disclosures Honoraria for consulting or speaking (last 5 years): Abbott, AbbVie,
HCV Treatment in 2016: is there still a role for IFNa and ribavirin? Heiner Wedemeyer Hannover Medical School Germany 1 Disclosures Honoraria for consulting or speaking (last 5 years): Abbott, AbbVie,
Hepatocellular Carcinoma: Can We Slow the Rising Incidence?
 Hepatocellular Carcinoma: Can We Slow the Rising Incidence? K.Rajender Reddy M.D. Professor of Medicine Director of Hepatology Medical Director of Liver Transplantation University of Pennsylvania Outline
Hepatocellular Carcinoma: Can We Slow the Rising Incidence? K.Rajender Reddy M.D. Professor of Medicine Director of Hepatology Medical Director of Liver Transplantation University of Pennsylvania Outline
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Viral Hepatitis And Liver Transplantation
 Viral Hepatitis And Liver Transplantation Dr.Zeki KARASU Ege University Medical School Dep. Gastroenterology Hepatitis B 3-7 10 % HBV infection in liver transplant recipients, in western countries. 120
Viral Hepatitis And Liver Transplantation Dr.Zeki KARASU Ege University Medical School Dep. Gastroenterology Hepatitis B 3-7 10 % HBV infection in liver transplant recipients, in western countries. 120
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Healthy Liver Cirrhosis
 Gioacchino Angarano Clinica delle Malattie Infettive Università degli Studi di Foggia Healthy Liver Cirrhosis Storia naturale dell epatite HCVcorrelata in assenza di terapia Paestum 13-15 Maggio 24 The
Gioacchino Angarano Clinica delle Malattie Infettive Università degli Studi di Foggia Healthy Liver Cirrhosis Storia naturale dell epatite HCVcorrelata in assenza di terapia Paestum 13-15 Maggio 24 The