TennCare Drug Utilization Advisory Board. October 1, 2013
|
|
|
- Aileen Higgins
- 6 years ago
- Views:
Transcription
1 TennCare Drug Utilization Advisory Board October 1, 2013
2 Agenda Call to Order Introductions Approval of Previous Minutes / Additions to the Agenda TennCare Update David Collier, MD Old Business ProDUR Max Dose Analysis Katie Lockhart, MA Medication Therapy Management Denise Barker, PharmD Blocking Outlier Prescribers Standing Business TennCare Drug Utilization Data RetroDUR and Provider Practice Activity Review Pharmacy Lock-In Review New Business Adjournment
3 Review of Minutes July 9, 2013
4 Old Business ProDUR Max Dose Analysis Katie Lockhart, MA Senior Healthcare Analyst
5 Background Currently, the Prospective DUR Maximum Dose Edit is set at 225% The general consensus amongst the DUR Board was that the limit was exceedingly high No concrete recommendations have been offered at this time due to the ambiguity surrounding the ramifications from changing the limit. The goal of this analysis is to present relevant data to assist in determining which adjustment should be made to the ProDUR Max Dose edit, if any
6 Executive Summary Approximately 3% of claims a month exceed the FDB recommended max dose which account for 3.3% of total spend for the month. Only 0.1% of claims a month meet or exceed 225% of the FDB recommended max dose which account for 0.14% of total spend for the month. At 100% or below the FDB recommended max dose 60% or more of the claims belong to adults.
7 Data Assumptions Report encompasses data from July 1 st to July 31 st Adult max dose was applied to children. Final Status of a claim was used for this analysis. Medications could be unpaid based on criteria outside of max dose.
8 Potential Impact 40,000 35,000 30,000 25,000 20,000 15,000 10,000 Over FDB Max Dose 25% and over 50% and over 100% and over 150% and over 225% and over 5,000 0 # of claims # of distinct Patients # of Adult Claims # of Adult Patients # of Ped Claims # of Ped Patients
9 Potential Impact by Percentage 12.00% 10.00% 8.00% 6.00% 4.00% Over FDB Max Dose 25% and over 50% and over 100% and over 150% and over 225% and over 2.00% 0.00% % of claims % of distinct Patients % of Adult Claims % of Adult Patients % of Ped Claims % of Ped Patients % of Total Paid % of Total Paid Adult % of Total Paid Kid
10 Age Distribution of Children 700 Number of Kids with a claim over FDB Max Dose Total
11 Paid Percentages
12 Current Paid Percentage 90% 80% 70% 60% Paid Percentage 50% 40% % Paid All % Paid Adults % Paid Kids 30% 20% 10% 0% Over FDB Max Dose 25% Above Max 50% Above Max 100% Above 150% Above 225% Above
13 Tennessee Compared to Other States High Dose ProDUR Edit Analysis Piad Percentage (Bar) % of Total Claims (Line) State 1 (5%) State 2(15%) State 3(100%) Hard Edit Tennessee State 0 Paid Percentage % of claims
14 Next Steps and Recommendations
15 Conservative Scenario Change Max dose limit to 150% of FDB Considerations: Edit may be considered more clinically relevant Paid percentage <50% Less impact at point of sale versus other limits Potentially double (~1.8x) the impact vs current edit May not be very significant overall versus other limits
16 Aggressive Scenario Change Max dose limit to 25% above FDB Max Considerations: Impacting more than 10x current number of claims for current edit Point of sale impact may/may not over-burden pharmacists based upon claim volume (1.79%) Not alerting on claims at FDB max and may allow prescribers a dose titration above the max dose
17 Very Aggressive Scenario Change limit to 100% FDB Max dose as a hard edit Considerations: Hard edit would need to be overridden by PA Prescribers would be allowed a dose titration above FDB Max Relative significant increased impact Implementation strategy may be needed due to strain on call center Potentially more PA calls per day

18 Evolution of Pharmacist-Provided Clinical Services
19 Medication Therapy Management is a distinct service or group of services that optimize therapeutic outcomes for individual patients. Medication Therapy Management services are independent of, but can occur in conjunction with, the provision of a medication product. Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model: Version March 2008
20 Med Therapy Reviews Immunizations Pharmacotherapy Consults Health, Wellness, Public Health Disease Management Coach / Support Med Safety Surveillance Pharmacogenomics Application Other Clinical Services Anticoagulation Management Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model: Version
21 A group of new services which have been offered by pharmacists for many years Reimbursable by Medicare, some state Medicaids, and some Private Payers

22 Sheet.pdf







23 MTM s Role in Health System Acute Care / Hospital Long-Term Care Ambulatory Care Accountable Care Organizations and Patient-Centered Medical Homes






24 Pharmacists Payers/ Insurers Patients Health Care Providers Employers
25 Have multiple chronic diseases Take multiple Part D drugs Incur annual costs for covered Part D drugs that exceed a predetermined level
26 Plan sponsors must offer all the following MTM services to eligible beneficiaries: Beneficiary and prescriber Interventions Comprehensive medication review (CMR) Annual Targeted medication review (TMR) Quarterly Follow-up interventions when necessary
27 Components of an MTM Service: Medication Therapy Review Personal Medication Record Medication-related Action Plan Intervention and/or Referral Documentation and follow-up Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model: Version March 2008
28 One-on-one session with individual patient (also Service delivered face-to-face, by telephone, or through other telehealth mechanisms Session may include patient s caregiver and family member(s) Full review of all medications and medication history Rx, OTC, vitamins, herbals, immunizations, etc. Review of past medical history and diseases Develop and Implement Medication-related Action Plan in collaboration with patient and primary care provider(s) Develop and Deliver Personal Medication Record to Patient May be Prompted or Requested

29 Plans work with documentation platforms to generate specific recommendations Recommendations based on Medicare criteria Overuse/underuse Suboptimal drug selection Omission of therapy Adverse side effects Patient profiles screened quarterly for Medicare plans Results in Irregular distribution to providers
30 MTM Services routinely provided by pharmacists Identifying gaps in medications and care Reducing medicationrelated adverse events Providing OTC medication recommendations Administering immunizations Educating patients on proper administration Increasing patient adherence to medications Managing Cost Effectiveness of medications Evaluating Underuse/Overuse Minimizing drug interactions Maximizing patient health outcomes And much more
31 Medicare PartD/MA-PD Platforms Mirixa OutcomesMTM PharmMD Solutions SOCRxATES Various private companies
32 Sheet.pdf
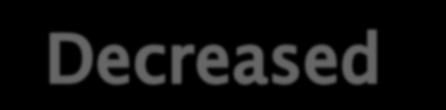
33 In 2012, 18 state Medicaid programs had some form of MTM program in place States: CA, CO, FL, IA, MN, MS, MO, MT, NM, NY, NC, OH, OR, UT, VT, VA, WI, WY Services range in scope from limited to broad Eligibility of beneficiaries ranges from small, specialized populations to all patients
34 Two Examples of Success Iowa: 31% of 3,037 eligible patients met with pharmacists 2.6 medication-related problems per patient 52% recommended new medication 31% recommended discontinuing medication Minnesota: 14% increase in meeting patient s goals 31% reduction in total health expenditures per patient (from $11,965 to $8,197) Savings exceeded cost by more than 12 to 1
35 Credentialed MTM Specialist Pharmacists Additional Services Offered by Plans to Patients Immunization Review and Administration Medication Adherence Consultations Disease Management Services Anticoagulation services, diabetes management, hypertension, hyperlipidemia, bone health, respiratory illness, mental health, etc. CLIA-Waived Testing Ex: Lipid Panels, A1C monitoring, INR monitoring, Genetic testing
36
37 Blocking Outlier Prescribers High Opiate Prescribers Ray McIntire, DPh
38 Background TennCare currently pays for prescriptions from all prescribers, regardless of their participation or network status. In 2011, TennCare pharmacy began to use a formal process to no longer pay for prescriptions from non-participating prescribers when they were found to be outliers in their prescribing habits. Process begins with identifying top narcotic prescribers, or the process has also began with a referral / complaint or when a prescriber has been in the media for being arrested or having their license disciplined.
39 Background In 2012, TennCare pharmacy moved away from the use of a list of high prescribers based on volume of opiates prescribed and percent of opiates prescribed. A new algorithm, which is still being evaluated for ways to improve, is intended to identify prescribers who: Prescribe many of the same types of opiates for many different patients, and appear to not evaluate each patient based on their own unique pain relief needs. Prescribe larger quantities of high-dose short-acting pure opiates compared with combination products and long-acting opiates Prescribe on average, more morphine equivalents than others All specialists and Suboxone prescribers are removed from the analysis
40 Background Once the top prescribers are identified, and candidates for blocking are chosen, TennCare s MCO s are notified. Once the MCO s verify that the prescriber is not needed for their network and agree to proceed, each prescriber is presented to TennCare s DUR Board, with blinded data for a final vote for either blocking or retaining. Prescribers are notified if blocked, and have 30 days to appeal. If the prescriber appeals, the DUR Board makes a final decision at the next quarterly meeting. All enrollees are notified that TennCare will no longer pay for prescriptions from their provider, and prescribers are referred to the State Board of Medical Examiners.
41 Candidates for Blocking TennCare pharmacy analyzed the opiate prescribing data for all prescribers with more than 50 opiate prescriptions in the 2 nd quarter of prescribers were analyzed The average number of opiate prescriptions per prescriber is 137. The highest number of opiate prescriptions was Four candidates selected for blocking were listed in the Top 100, and each prescriber has already been involuntary terminated from the MCO s due to their billing practices. Since they were already terminated by the MCO s it was not necessary to first refer these prescribers to the MCO s for signoff.
42 Prescriber#1 Both Prescriber#1, who is an Advance Practice Nurse, and the prescriber s Medical Director have been terminated from the MCO s for their billing practices. Prescriber#1 is not high volume, but is ranked #11 in the algorithm, and is an outlier in the following categories: Ratio of C-II to C-III opiates Ratio of Pure short-acting opiate to Combination products Average Morphine equivalents per patient per day. From TennCare claims the average MEQ per patient per day is 127mg. When claims from the CSDB are added, the total average MEQ per patient per day equals mg.
43 Prescriber#2 and Prescriber#3 Both Prescriber#2, who is an Advance Practice Nurse, and the prescriber s Medical Director (Prescriber#3) have been terminated from the MCO s for their billing practices. Prescriber#3, who is at least 80 years old, has claims in the TennCare paid algorithm, but all claims in the CSDB show up in Prescriber#2 s name. Prescriber#3 is #19 ranked in the algorithm, Prescriber#2 is #26 Due to data integrity issues, with pharmacies submitting different information to TennCare and to the CSDB, we are submitting both Prescriber#2 and Prescriber#3 for blocking. Prescriber#3 s License Verification with the State of TN shows Missionary Overseas
44 Prescriber#2 and Prescriber#3 Prescriber#2 has a higher volume and is an outlier in the following categories: Number of opiate prescriptions Average Morphine equivalents per patient per day. From TennCare claims the average MEQ per patient per day is 43.4mg. When claims from the CSDB are added, the total average MEQ per patient per day equals 95.88mg. For the 2 nd quarter, 330 additional prescriptions for CNS depressants were found on the CSMD, not found in TennCare claims.
45 Prescriber#2 and Prescriber#3 When looking at all claims, Prescriber#2 is commonly prescribing the cocktail for many patients, which is a combination of: Opiate analgesic Benzodiazepine Carisoprodol All non-opiate CNS depressants can be converted to diazepam equivalents. In addition to 96mg of MEQ per person per day, Prescriber#2 s patients also take on average 23.3mg of Diazepam equivalents per day.
46 Prescriber#4 Prescriber#4, is an Advance Practice Nurse, who has been terminated from the MCO s for because of billing practices. Prescriber#4 is high volume, and has a significantly lower percent of controlled substances to all paid claims (probably due to prescribing in a Family Practice and in a Pain Clinc), and is an outlier in the following categories: Number of Opiates Average Morphine equivalents per patient per day. From TennCare claims the average MEQ per patient per day is 91.32mg. When claims from the CSDB are added, the total average MEQ per patient per day equals mg.
47 Prescriber#4 When looking at all claims, Prescriber#4 is commonly prescribing the cocktail for many patients (opiate, benzodiazepine, carisoprodol). In addition to 216mg of MEQ per person per day, Prescriber#4 s patients also take on average 16.2mg of Diazepam equivalents per day.
48 Prescriber#5 Prescriber#5, is an Advance Practice Nurse, who has been terminated from the MCO s for because of billing practices. Prescriber#5 has a low volume of TennCare paid claims and claims on the CSMD, is ranked #85 in the algorithm and is an outlier only in the following category (borderline at that): Average Morphine equivalents per patient per day. From TennCare claims the average MEQ per patient per day is 54.95mg. When claims from the CSDB are added, the total average MEQ per patient per day equals 96.1mg. Our recommendation is to not block at this time, but to continue to monitor prescribing and utilization.
49 Standing Business
50 TennCare Pharmacy Data TennCare Statistics Utilization Data Population 2Q13 vs. 2Q12 vs. 1Q13 TennCare Utilizing members Generic Drug Utilization Total Population Drug class claim volume and payment amount Individual drug- claim volume and payment amount Adult Population (age 21 and above) Drug class claim volume and payment amount Individual drug- claim volume and payment amount Pediatric Population (ages 0 through 20) Drug class claim volume and payment amount Individual drug- claim volume and payment amount
51 Overall Population Statistics Utilizing Members 14.6% YOY reduction in Non-dual Adults without Rx Limit 5.2% YOY reduction in Utilizing members per month & 10.3% QOQ reduction in Utilizing members per month 3.8% reduction in Total amount paid / month
52 TennCare Population Eligibility 2Q2013 1Q2013 2Q2012 %Change (Quarter/ Quarter) %Change (Year/ Year) Average Total TennCare Population 1,202,313 1,204,740 1,200, % 0.2% Non-Dual Children 736, , , % -1.5% Non-Dual Adults with Rx Limit 327, , , % 1.7% Non-Dual Adults without Rx Limit 6,056 6,194 6, % -14.6% Dual Eligible Children % 13.4% Dual Eligible Adults 129, , , % -1.4% Average Pharmacy Utilizing Members per Month < 21 (Children) Average Pharmacy Utilizing Members per Month 21 (Adults) 191, , , % -13.1% 181, , , % -5.7%
53 TennCare Utilizing Members 2Q2013 1Q2013 2Q2012 % Change (Quarter/ Quarter) % Change (Year/Year) # Utilizing Members / Month 359, , , % -5.2% # Prescriptions / Month 1,048,260 1,109,823 1,063, % -1.4% Total Amount Paid / Month $63,997,773 $66,511,776 $66,514, % -3.8% Average # of Rx / Utilizing Member/ Month % 4.3% Average Amount Paid / Claim $61.05 $59.92 $ % -2.4% Average Amount Paid / Utilizing Member $ $ $ % 1.6% Average Amount Paid / Eligible Member $53.23 $55.21 $ % -3.9%
54 Utilization Data Total Population
55 Overall Utilization Highlights 1Q2013 Narcotic payment amount: ~17% QOQ ADHD payment amount: ~33% YOY PPI claims: ~40% YOY & ~35% QOQ Dexlansoprazole payment amount: ~19% YOY Adult Population Narcotic claims: ~15% YOY Narcotic payment amount:~27% YOY ( Oxymorphone payment amount 44% QOQ) Atypical payment amount: 21.5% YOY Hepatitis C Protease Inhibitors payment amount: ~33% YOY 22.7% increase payment amount QOQ ( 19% Telapravir QOQ) Child Population Antihemophilic Factors: ~60% QOQ ( ~57% Factor VII payment amount QOQ) *all percentages reported as per member per month
56 Top 10 Therapeutic Classes by Claim Volume Rank Therapeutic Class # of Claims (2Q13) Rank 2Q13 # of Claims (1Q13) Rank 2Q12 # of Claims (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Narcotic Analgesics 256, , , % -9.3% 2 Anticonvulsants 149, , , % 4.2% 3 2 nd Gen Antihistamines 125, , , % 1.2% 4 Penicillins 110, , , % -4.5% 5 NSAIDS/COX Inhibitors 107, , , % -7.7% 6 SSRIs 104, , , % -4.5% 7 Beta-Adrenergic Agents 94, , , % -6.3% 8 1 st Gen Antihistamines 83, , , % -5.2% 9 PPIs 97, , , % 40.3% 10 Adrenergics 66, , , % 3.0%
57 Top 10 Therapeutic Classes by Payment Amount Rank Therapeutic Class $ Paid (1Q13) Rank 1Q13 $ Paid (1Q13) Rank 2Q12 $ Paid (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Atypical Antipsychotics $20,199,935 1 $19,518,741 1 $23,924, % -15.7% 2 Adrenergics $10,528,225 2 $18,719,079 2 $10,594, % -0.8% 3 Anticonvulsants $10,292,067 4 $10,186,600 3 $10,503, % -2.2% 4 Insulins $8,886,280 8 $8,541,039 6 $7,884, % 12.5% 5 Narcotic Analgesics $7,767,908 5 $9,368,331 5 $8,154, % -4.9% 6 ADHD treatment $6,388,943 7 $6,738,725 4 $9,558, % -33.3% 7 PPIs $6,220, $5,731,548 9 $5,371, % 15.6% 8 Beta-Adrenergic Agents $5,591,741 8 $6,151, $5,280, % 5.7% 9 Antihemophilic Factors $5,417,520 3 $13,161,063 8 $6,248, % -13.5% 10 Inhaled Glucocorticoids $4,602, $5,825, $4,540, % 1.2%
58 Top 10 Drugs by Claim Volume Rank Drug # of Claims (1Q13) Rank 1Q13 # of Claims (1Q13) Rank 2Q12 # of Claims (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Hydrocodone/APAP 152, , , % -11.5% 2 Albuterol 91, , , % -4.8% 3 Cetirizine 82, , , % 6.0% 4 Amoxicillin 69, , , % -4.4% 5 Montelukast 61, , , % -4.0% 6 Lisinopril 53, , , % -0.9% 7 Gabapentin 50, , , % 17.7% 8 Ibuprofen 50, , , % -5.2% 9 Azithromycin 45, , , % -17.9% 10 Fluticasone Propionate 44, , , % 7.4%
59 Top 10 Drugs by Payment Amount Rank Drug $ Paid (2Q13) Rank 1Q13 $ Paid (1Q13) Rank 2Q12 $ Paid (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Aripiprazole $10,528,225 1 $10,037,678 2 $9,724, % 8.1% 2 Amphetamine Salts $6,321,383 2 $6,743,034 3 $6,243, % 1.1% 3 Albuterol $4,790,067 3 $4,891,523 6 $4,066, % 17.6% 4 Lisdexamfetamine $4,733,738 5 $4,977,443 5 $4,194, % 12.7% 5 Dexlansoprazole $4,610,172 8 $4,228,565 7 $3,877, % 18.7% 6 Methylphenidate $3,826,532 9 $4,043,633 1 $4,303, % -11.2% 7 Blood Sugar Diagnostic $3,465, $3,447,607 9 $3,165, % 9.3% 8 Telapravir $2,961, $2,597, $2,864, % 3.2% 9 Quetiapine $2,925, $2,929, $2,785, % 4.9% 10 Insulin Glargine $2,839, $2,662, $2,422, % 17.0%
60 Utilization Data Adult Population (Ages 21 and Older)
61 Top 10 Therapeutic Classes by Claim Volume - Adults Rank Therapeutic Class # of Claims (2Q13) Rank 1Q13 # of Claims (1Q13) Rank 2Q12 # of Claims (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Narcotic Analgesics 224, , , % -15.1% 2 Anticonvulsants 113, , , % 10.0% 3 SSRIs 81, , , % -1.5% 4 NSAIDS/COX Inhibitors 77, , , % -0.8% 5 ACE Inhibitors 63, , , % 0.0% 6 PPIs 61, , , % 11.7% 7 Skeletal Muscle Relaxants 55, , , % -0.3% 8 Statins 54, , , % 1.1% 9 Beta-Adrengic Agents 44, , , % -6.3% 10 Beta-Blocking Agents 43, , , % -2.8%
62 Top 10 Therapeutic Classes by Payment Amount - Adults Rank Therapeutic Class $ Paid (2Q13) Rank 1Q13 $ Paid (1Q13) Rank 2Q12 $ Paid (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Atypical Antipsychotics $13,198,953 1 $12,753,622 1 $16,790, % -21.5% 2 Narcotic Analgesics $7,546,391 2 $9,126,212 2 $10,295, % -26.8% 3 Insulins $7,437,488 3 $7,105,915 4 $6,383, % 16.3% 4 Anticonvulsants $6,844,910 4 $6,715,646 3 $6,761, % 1.1% 5 PPIs $5,101,463 5 $4,718,497 5 $4,215, % 20.8% 6 Hepatitis C Protease Inh $3,202, $2,616,412 6 $4,787, % -33.2% 7 Blood Sugar Diagnostics $2,786,583 8 $2,734,354 7 $2,527, % 10.1% 8 Narcotic Withdrawal Agents $2,688, $2,569,432 9 $2,326, % 15.3% 9 Multiple Sclerosis Agents $2,681,388 9 $2,676,493 8 $2,513, % 6.5% 10 Beta-Adrenergic Agents $2,525, $2,406, $2,193, % 14.9%
63 Top 10 Drugs by Claim Volume - Adults Rank Drug # of Claims (2Q13) Rank 1Q13 # of Claims (1Q13) Rank 2Q12 # of Claims (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Hydrocodone/APAP 129, , , % -10.7% 2 Lisinopril 52, , , % -0.8% 3 Gabapentin 49, , , % 18.1% 4 Albuterol 43, , , % -5.9% 5 Oxycodone/APAP 37, , , % -5.9% 6 Metformin 32, , , % -2.6% 7 Omeprazole 32, , , % 14.5% 8 Levothyroxine 29, , , % -2.7% 9 Amlodipine 29, , , % 2.3% 10 Citalopram 28, , , % -10.7%
64 Top 10 Drugs by Payment Amount - Adults Rank Drug $ Paid (2Q13) Rank 1Q13 $ Paid (1Q13) Rank 2Q12 $ Paid (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Aripiprazole $5,267,052 1 $4,994,818 1 $5,153, % 2.0% 2 Dexlansoprazole $4,299,043 2 $3,931,200 2 $3,581, % 19.8% 3 Telaprevir $2,900,543 6 $2,439,763 4 $2,696, % 7.4% 4 Blood Sugar Diagnostic $2,754,586 4 $2,730,968 5 $2,523, % 8.9% 5 Buprenorphine/Naloxone $2,547,557 5 $2,461,758 7 $2,227, % 14.2% 6 Inslulin Glargine $2,487,129 8 $2,349,573 8 $2,121, % 17.0% 7 Quetiapine $2,410,134 7 $2,401,451 6 $2,270, % 6.0% 8 Albuterol $2,352,689 9 $2,223, $1,998, % 17.5% 9 Oxymorphone $1,922,626 3 $3,465,591 8 $2,039, % -5.9% 10 Emtricitabine/Tenofovir $1,757, $1,725, $1,697, % 3.4%
65 Utilization Data Child Population (Ages 0 through 20)
66 Top 10 Therapeutic Classes by Claim Volume - Children Rank Therapeutic Class # of Claims (2Q13) Rank 1Q13 # of Claims (1Q13) Rank 2Q12 # of Claims (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 2 nd Generation Antihistamines 100, , , % 2.1% 2 Penicillins 81, , , % -5.5% 3 Leukotriene Receptor Antagonists 54, , , % -6.4% 4 Adrenergics 52, , , % 4.4% 5 Beta-Adrenergic Agents 50, , , % -6.3% 6 1 st Generation Antihistamines 40, , , % -6.4% 7 ADHD Medications 39, , , % 3.3% 8 Anticonvulsants 35, , , % -2.1% 9 Topical Anti-inflammatory Agents 35, , , % -12.7% 10 Glucocorticoids 33, , , % -6.7%
67 Top 10 Therapeutic Classes by Payment Amount - Children Rank Therapeutic Class $ Paid (2Q13) Rank 1Q13 $ Paid (1Q13) Rank 2Q12 $ Paid (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Adrenergics $9,362,035 1 $15,189,767 2 $8,488, % 10.1% 2 ADHD Agents $8,473,878 3 $8,768,731 3 $7,929, % 6.7% 3 Atypical Antipsychotics $7,000,982 4 $6,765,118 4 $7,133, % -2.0% 4 Antihemophilic Factors $4,007,698 2 $10,035,730 5 $5,168, % -22.6% 5 Orally Inhaled Glucocorticoids $3,750,722 6 $4,728,834 7 $3,651, % 2.5% 6 Anticonvulsants $3,451,334 8 $3,470,953 6 $3,546, % -2.9% 7 Beta-Adrenergic Agents $3,065,859 7 $3,745,232 9 $3,086, % -0.8% 8 Growth Hormones $2,688, $2,895, $2,789, % -3.8% 9 3 rd Generation Cephalosporins $2,105,042 9 $3,041, $1,759, % 19.4% 10 Insulins $1,448, $1,435, $1,261, % 14.6%
68 Top 10 Drugs by Claim Volume - Children Rank Drug # of Claims (2Q13) Rank 1Q13 # of Claims (1Q13) Rank 2Q12 # of Claims (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Cetirizine 71, , , % 5.8% 2 Amoxicillin 56, , , % -4.8% 3 Montelukast 54, , , % -6.5% 4 Albuterol 47, , , % -3.8% 5 Fluticasone Propionate 29, , , % 9.0% 6 Loratadine 28, , , % -5.6% 7 Azithromycin 28, , , % -19.7% 8 Amphetamine Salts 26, , , % 3.7% 9 Lisdexamfetamine 25, , , % 4.4% 10 Methylphenidate 24, , , % -1.8%
69 Top 10 Drugs by Payment Amount - Children Rank Drug $ Paid (2Q13) Rank 1Q13 $ Paid (1Q13) Rank 2Q12 $ Paid (2Q12) PMPM% (QOQ) PMPM% (YOY) 1 Aripiprazole $5,261,174 3 $5,042,860 3 $4,570, % 14.9% 2 Amphetamine Salts $4,890,213 2 $5,237,994 2 $4,596, % 6.2% 3 Lisdexamphetamine $4,280,427 4 $4,513,684 5 $3,782, % 13.0% 4 Methylphenidate $3,691,457 5 $3,924,025 4 $4,174, % -11.7% 5 Somatropin $2,688,465 7 $2,895,933 6 $2,789, % -3.8% 6 Albuterol $2,437,379 9 $2,667,643 7 $2,068, % 17.6% 7 Dexmethylphenidate $2,372, $2,500,728 8 $1,956, % 21.1% 8 Fluticasone Propionate $1,929, $1,814,074 9 $1,878, % 2.5% 9 Guanfacine $1,915, $1,906, $1,497, % 27.7% 10 Coagulation Factor VIIa $1,559,016 6 $3,637, $1,658, % -6.1%
70 Prospective Drug Utilization Review (ProDUR) 2 nd Quarter 2013
71 Definitions Edits / Rejections ProDUR Edit A computer system review of the member s medication history Identifies potential drug therapy problems prior to dispensing the medication. Examples would include but not limited to: Therapeutic Duplication (TD), Early Refill (ER), Max Dose, Drug to Gender, Drug to Drug, Drug to Inferred Disease, Geriatric and Pediatric Warnings Types of Rejections: Hard Reject These edits will cause the claim to deny at the point of sale (POS) Soft Reject- These edits will cause the claim to deny at the point of sale. However, with appropriate documentation the pharmacy will be able to re-submit the rejected claim using Professional Pharmacy Service (PPS) codes Message These edits will cause an alert or warning message to be returned to the dispensing pharmacist to inform them of a potential problem.
72 ProDUR Review Top 10 Therapeutic Duplication Drug Name Total % Paid ALBUTEROL SULFATE 20, % HYDROCODONE BIT/ACETAMINOPHEN 18, % LISINOPRIL 17, % AMLODIPINE BESYLATE 14, % GABAPENTIN 12, % TRAZODONE HCL 11, % OXYCODONE HCL 11, % OXYCODONE HCL/ACETAMINOPHEN 10, % MORPHINE SULFATE 10, % DEXTROAMPHETAMINE/AMPHETAMINE 10, %
73 ProDUR Review Top 10 Early Refill Drug #Edits HYDROCODONE BIT/ACETAMINOPHEN 2,613 GABAPENTIN 1,335 LISINOPRIL 1,258 ALBUTEROL SULFATE 1,175 DEXTROAMPHETAMINE/AMPHETAMINE 1,063 CETIRIZINE HCL 994 MONTELUKAST SODIUM 969 CLONIDINE HCL 967 CITALOPRAM HYDROBROMIDE 914 BUPRENORPHINE HCL/NALOXONE HCL 854
74 ProDUR Review Top 10 Max Dose Drug Total Paid% HYDROCODONE BIT/ACETAMINOPHEN 8, % CEFDINIR 7, % POLYETHYLENE GLYCOL , % PROMETHAZINE HCL 4, % AMOXICILLIN/POTASSIUM CLAV 3, % IBUPROFEN 2, % CETIRIZINE HCL 1, % OXYCODONE HCL/ACETAMINOPHEN 1, % CYCLOBENZAPRINE HCL 1, % DEXTROAMPHETAMINE/AMPHETAMINE 1, %
75 ProDUR Review Top 10 Drug to Inferred Diagnosis Pregnancy Drug Total %Paid HYDROCODONE BIT/ACETAMINOPHEN 1, % PROMETHAZINE HCL 1, % IBUPROFEN 1, % OXYCODONE HCL/ACETAMINOPHEN % METRONIDAZOLE % AZITHROMYCIN % FLUCONAZOLE % NITROFURANTOIN MONOHYDRATE % ALBUTEROL SULFATE % BUPRENORPHINE HCL %
76 ProDUR Review Top 10 Drug to Gender Drug Total Paid% ZOLPIDEM TARTRATE 3, % EMTRICITABINE/TENOFOVIR % RIZATRIPTAN BENZOATE % TAMSULOSIN HCL % SUMATRIPTAN SUCCINATE % RIBAVIRIN % EMTRICITAB/RILPIVIRINE/TENOFOV % ABACAVIR SULFATE/LAMIVUDINE % MEDROXYPROGESTERONE ACETATE % ELVITEGR/COBICIST/EMTRIC/TENOFOVIR %
77 ProDUR Review Top 10 Geriatric Precaution Drug Total % Paid AMLODIPINE BESYLATE % HYDROCODONE BIT/ACETAMINOPHEN % SIMVASTATIN % METFORMIN HCL % LEVOTHYROXINE SODIUM % LISINOPRIL % WARFARIN SODIUM % ATORVASTATIN CALCIUM % HYDROCHLOROTHIAZIDE % CITALOPRAM HYDROBROMIDE %
78 ProDUR Review Top 10 Pediatric Precaution Drug Total % Paid MONTELUKAST SODIUM 40, % CETIRIZINE HCL 15, % CLONIDINE HCL 15, % METHYLPHENIDATE HCL 13, % RISPERIDONE 11, % DEXTROAMPHETAMINE/AMPHETAMINE 11, % LISDEXAMFETAMINE DIMESYLATE 11, % IBUPROFEN 10, % HYDROCODONE BIT/ACETAMINOPHEN 10, % GUANFACINE HCL 9, %
79 Review of DUR Activities
80 RetroDUR Activities Not Done in 2Q13 Due to Transition of PBM
81 Ideas for future RetroDUR Activities?
82 Pharmacy Lock-In Program


83 Member/Pharmacy Lock-In Criteria Criteria includes a review of the following in a 90 day period: Multiple controlled substances Multiple pharmacies Multiple prescribers Targeted pharmacies and prescribers Maximum Daily Dosage Use of buprenorphine for addiction treatment
 2 pharmacies 1 targeted")

84 Lock-In Criteria CRITERIA 1 CRITERIA 2 CRITERIA 3 CRITERIA 4 CRITERIA 5 3 controlled substances 2 controlled substances 2 controlled substances 2 controlled substances 2 controlled substances 3 pharmacies 2 pharmacies 1 targeted pharmacy(ies) 2 pharmacies 1 targeted pharmacy(ies) 3 prescribers 2 prescribers 2 targeted prescribers 1 targeted prescriber(s) 1 targeted prescriber(s) Percentage of Maximum Daily Dosage - N/A 100% of Maximum Daily Dosage 90% of Maximum Daily Dosage 90% of Maximum Daily Dosage 95% of Maximum Daily Dosage
85 Pharmacy Lock-In Monthly Totals Month 2013 Lock-In 2012 Lock-In January 29 0 February 38 0 March April May June July 55 August 84 September 73 October 50 November 44 December 50 TOTAL





86 2 nd Quarter 2013 Re-reviews Remain: 57 Removed Refer Other: 1 Removed: 23 No cash prescriptions for medications covered by TennCare Utilizing only 1 pharmacy Utilizing only 1 physician Escalated to PA Members meets 3 of the 4 following criteria over a 3 month period 3 cash prescriptions (verified by CSD) 2 Physicians 2 Pharmacies Concurrently using Suboxone with another narcotic Refer to Mmb Svc: 1 Refer to MCO:2 Total Rereviewed: 100 Refer to OIG: 2 Remain PA Status: 7 Escalate: 12
87 Next Meeting December 17, 2013
TennCare Drug Utilization Review Advisory Board. November 13 th, 2012 Catamaran
 TennCare Drug Utilization Review Advisory Board November 13 th, 2012 Catamaran Agenda Call to Order Introductions Approval of Previous Minutes / Additions to the Agenda TennCare Update Guest Speaker Dr.
TennCare Drug Utilization Review Advisory Board November 13 th, 2012 Catamaran Agenda Call to Order Introductions Approval of Previous Minutes / Additions to the Agenda TennCare Update Guest Speaker Dr.
TennCare Drug Utilization Review (DUR) Board Minutes
 Board Minutes") State of Tennessee Department of Finance and Administration Bureau of TennCare 310 Great Circle Road Nashville, TN 37228 TennCare Drug Utilization Review (DUR) Board Minutes September 11, 2012 In attendance:
State of Tennessee Department of Finance and Administration Bureau of TennCare 310 Great Circle Road Nashville, TN 37228 TennCare Drug Utilization Review (DUR) Board Minutes September 11, 2012 In attendance:
Idaho DUR Board Meeting Minutes
 Idaho DUR Board Meeting Minutes Date: January 21, 2016 Time: 9am-1:30pm Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Mark Turner, M.D. Committee Members
Idaho DUR Board Meeting Minutes Date: January 21, 2016 Time: 9am-1:30pm Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Mark Turner, M.D. Committee Members
Medicaid Perspective
 Prescription Opioid Fraud and Abuse: Medicaid Perspective Presenter: Gary P. Gilmore, B.S., R.Ph. Director, Analysis & Reporting Office of Clinical Affairs Deputy Director, Pharmacy Program Objectives:
Prescription Opioid Fraud and Abuse: Medicaid Perspective Presenter: Gary P. Gilmore, B.S., R.Ph. Director, Analysis & Reporting Office of Clinical Affairs Deputy Director, Pharmacy Program Objectives:
Idaho DUR Board Meeting Minutes
 Idaho DUR Board Meeting Minutes Date: July 20, 2017 Time: 9am-12:30pm Location: Holiday Inn Boise Airport 2970 West Elder Street, Boise, Idaho, 83705 Moderator: David Agler, M.D. Committee Member Present:
Idaho DUR Board Meeting Minutes Date: July 20, 2017 Time: 9am-12:30pm Location: Holiday Inn Boise Airport 2970 West Elder Street, Boise, Idaho, 83705 Moderator: David Agler, M.D. Committee Member Present:
Idaho DUR Board Meeting Minutes
 Date: July 16, 2015 Time: 9am-1:30pm Idaho DUR Board Meeting Minutes Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Mark Turner, M.D. Committee Member Present:
Date: July 16, 2015 Time: 9am-1:30pm Idaho DUR Board Meeting Minutes Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Mark Turner, M.D. Committee Member Present:
Follow-up to Previous Reviews
 21 January 2016 1 Follow-up to Previous Reviews Patients Receiving > 1 Long-Acting Opioid Multiple Dosage Forms of Aripiprazole Prescribed Concomitantly Multiple Dosage Forms of Oral Paliperidone Prescribed
21 January 2016 1 Follow-up to Previous Reviews Patients Receiving > 1 Long-Acting Opioid Multiple Dosage Forms of Aripiprazole Prescribed Concomitantly Multiple Dosage Forms of Oral Paliperidone Prescribed
Patient Review and Coordination Program
 Patient Review and Coordination Program For Medical Assistance Clients Who Need Assistance In Appropriate Use of Phyllis Coolen, RN, MN Division of Healthcare Health and Recovery Administration January
Patient Review and Coordination Program For Medical Assistance Clients Who Need Assistance In Appropriate Use of Phyllis Coolen, RN, MN Division of Healthcare Health and Recovery Administration January
Connecticut Medical Assistance Pharmacy Program Drug Utilization Review (DUR) Program DUR Board Meeting
 Program DUR Board Meeting") March 2015 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair), Keith Lyke R.Ph., Bhupesh Mangla, MD, Richard Gannon, Pharm.D., Charles Caley Pharm.D. BCPP, Ram Illindala, MD, Carol
March 2015 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair), Keith Lyke R.Ph., Bhupesh Mangla, MD, Richard Gannon, Pharm.D., Charles Caley Pharm.D. BCPP, Ram Illindala, MD, Carol
Eligible Beneficiaries
 Therapeutic Class: Behavioral Health Medications for Adults Clinical Edit Number Long Description 4110 (May change) Quantity limit edit that is applied to atypical antipsychotics for claims identified
Therapeutic Class: Behavioral Health Medications for Adults Clinical Edit Number Long Description 4110 (May change) Quantity limit edit that is applied to atypical antipsychotics for claims identified
Drug Use Evaluation: Short Acting Opioids (SAO)
") Drug Use Evaluation: Short Acting Opioids (SAO) Summary Short acting opioid analgesics are one of the most prescribed (top 10) and highest cost (top 20) medication classes for the Oregon Fee For Service
Drug Use Evaluation: Short Acting Opioids (SAO) Summary Short acting opioid analgesics are one of the most prescribed (top 10) and highest cost (top 20) medication classes for the Oregon Fee For Service
Idaho DUR Board Meeting Minutes
 Idaho DUR Board Meeting Minutes Date: Jan. 16, 2014 Time: 9am-1pm Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Mark Turner, M.D. Committee Member Present:
Idaho DUR Board Meeting Minutes Date: Jan. 16, 2014 Time: 9am-1pm Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Mark Turner, M.D. Committee Member Present:
Curbing Prescription Drug Abuse in Medicaid
 Curbing Prescription Drug Abuse in Medicaid Joint Legislative Health Care Oversight Committee October 12, 2010 Dr. Lisa Weeks, BSPharm, PharmD Pharmacy and Ancillary Services Division of Medical Assistance
Curbing Prescription Drug Abuse in Medicaid Joint Legislative Health Care Oversight Committee October 12, 2010 Dr. Lisa Weeks, BSPharm, PharmD Pharmacy and Ancillary Services Division of Medical Assistance
Amy Larrick Chavez-Valdez, Director, Medicare Drug Benefit and C & D Data Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE TO: FROM: SUBJECT: All Part D Sponsors Amy Larrick
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard Baltimore, Maryland 21244-1850 CENTER FOR MEDICARE TO: FROM: SUBJECT: All Part D Sponsors Amy Larrick
Suboxone, Zubsolv, Bunavail (buprenorphine with naloxone sublingual tablets and film), Buprenorphine sublingual tablets
, Buprenorphine sublingual tablets") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.32 Subject: Suboxone Drug Class Page: 1 of 7 Last Review Date: June 24, 2016 Suboxone Drug Class Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.32 Subject: Suboxone Drug Class Page: 1 of 7 Last Review Date: June 24, 2016 Suboxone Drug Class Description
Idaho DUR Board Meeting Minutes
 Idaho DUR Board Meeting Minutes Date: October 16, 2014 Time: 9am-2pm Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Mark Turner, M.D. Committee Member Present:
Idaho DUR Board Meeting Minutes Date: October 16, 2014 Time: 9am-2pm Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Mark Turner, M.D. Committee Member Present:
Alabama Medicaid Pharmacy Override
 Alabama Medicaid Pharmacy Override Therapeutic Duplication, Early Refill, Maximum Unit, Prescription Limit Switchover, Dispense as Written, Accumulation Edit, Maintenance Supply Opt Out, and Maximum Cost
Alabama Medicaid Pharmacy Override Therapeutic Duplication, Early Refill, Maximum Unit, Prescription Limit Switchover, Dispense as Written, Accumulation Edit, Maintenance Supply Opt Out, and Maximum Cost
Medication Therapy Management: Improving Health and Saving Money
 Medication Therapy Management: Improving Health and Saving Money Ed Staffa, RPh Vice President, Pharmacy Mirixa Corporation estaffa@mirixa.com July 23, 2008 MTM At A Glance The U.S. health care system
Medication Therapy Management: Improving Health and Saving Money Ed Staffa, RPh Vice President, Pharmacy Mirixa Corporation estaffa@mirixa.com July 23, 2008 MTM At A Glance The U.S. health care system
Health plans are charged with the difficult balance of
 RESEARCH Measuring Economic Impact of Applying Daily Average Consumption Limits Bridget M. Flavin, PharmD; Lynn M. Nishida, RPh; Sean H. Karbowicz, PharmD; Mark E. Renner; and Ruth J. Leonard, PharmD ABSTRACT
RESEARCH Measuring Economic Impact of Applying Daily Average Consumption Limits Bridget M. Flavin, PharmD; Lynn M. Nishida, RPh; Sean H. Karbowicz, PharmD; Mark E. Renner; and Ruth J. Leonard, PharmD ABSTRACT
Wisconsin Statewide Substance Abuse Prevention Training Wisconsin Dells June 12, 2015
 Wisconsin Statewide Substance Abuse Prevention Training Wisconsin Dells June 12, 2015 1 Presenter Andrea Magermans Program Analyst of the Wisconsin PDMP Wisconsin Department of Safety and Professional
Wisconsin Statewide Substance Abuse Prevention Training Wisconsin Dells June 12, 2015 1 Presenter Andrea Magermans Program Analyst of the Wisconsin PDMP Wisconsin Department of Safety and Professional
How to Conduct an Effective Medication Therapy Management Session in the Community Pharmacy
 How to Conduct an Effective Medication Therapy Management Session in the Community Pharmacy Presented by: Dale Christensen, University of North Carolina Susmita Chavala, Humana Ed Staffa, Community MTM
How to Conduct an Effective Medication Therapy Management Session in the Community Pharmacy Presented by: Dale Christensen, University of North Carolina Susmita Chavala, Humana Ed Staffa, Community MTM
Connecticut Medical Assistance Pharmacy Program Drug Utilization Review (DUR) Program DUR Board Meeting
 Program DUR Board Meeting") December 2012 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair), Keith Lyke R.Ph., Dennis Chapron, M.S., Bhupesh Mangla, M.D., Charles Caley, Pharm.D., Ram Illindala, M.D., Richard
December 2012 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair), Keith Lyke R.Ph., Dennis Chapron, M.S., Bhupesh Mangla, M.D., Charles Caley, Pharm.D., Ram Illindala, M.D., Richard
USING MTM TO IMPROVE STAR RATINGS : CASE STUDIES
 USING MTM TO IMPROVE STAR RATINGS : CASE STUDIES Sept 13, 2015 Amanda Applegate, PharmD, BCACP Disclosures Nothing to disclose Learning Objectives Describe how MTM can improve star ratings Discuss strategies
USING MTM TO IMPROVE STAR RATINGS : CASE STUDIES Sept 13, 2015 Amanda Applegate, PharmD, BCACP Disclosures Nothing to disclose Learning Objectives Describe how MTM can improve star ratings Discuss strategies
PBMs: Impact on Cost and Quality of Pharmaceutical Care in the U.S.
 Speaker Brian K. Solow, MD, FAAFP Optum Life Sciences Irvine, CA, USA PBMs: Impact on Cost and Quality of Pharmaceutical Care in the U.S. Brian K. Solow, MD, FAAFP Chief Medical Officer, Optum Life Sciences
Speaker Brian K. Solow, MD, FAAFP Optum Life Sciences Irvine, CA, USA PBMs: Impact on Cost and Quality of Pharmaceutical Care in the U.S. Brian K. Solow, MD, FAAFP Chief Medical Officer, Optum Life Sciences
A nation in pain: Focus on Medicaid
 DATA INSIGHTS A nation in pain: Focus on Medicaid Opioid pain medications have become one of the most controversial classes of prescription therapy. While they provide great benefits in controlling both
DATA INSIGHTS A nation in pain: Focus on Medicaid Opioid pain medications have become one of the most controversial classes of prescription therapy. While they provide great benefits in controlling both
New Medicare Part D Prescription Opioid Policies for 2019 Information for Prescribers
 CENTERS FOR MEDICARE & MEDICAID SERVICES New Medicare Part D Prescription Opioid Policies for 2019 Information for Prescribers Background CMS understands the magnitude of the nation s opioid epidemic and
CENTERS FOR MEDICARE & MEDICAID SERVICES New Medicare Part D Prescription Opioid Policies for 2019 Information for Prescribers Background CMS understands the magnitude of the nation s opioid epidemic and
Cost-Effective Process to Improve Drug Adherence for Medicare 5-Star
 Cost-Effective Process to Improve Drug Adherence for Medicare 5-Star HEALTH ALLIANCE PLAN Presented by Vanita K. Pindolia, Pharm.D. VP, Ambulatory Clinical Pharmacy Programs_PCM Medicare 5-Star Rating
Cost-Effective Process to Improve Drug Adherence for Medicare 5-Star HEALTH ALLIANCE PLAN Presented by Vanita K. Pindolia, Pharm.D. VP, Ambulatory Clinical Pharmacy Programs_PCM Medicare 5-Star Rating
Idaho DUR Board Meeting Minutes. Committee Member Present: David Agler, M.D., Dawn Berheim, Pharm.D., Perry Brown, M.D., Matthew Hyde, Pharm.D.
 Idaho DUR Board Meeting Minutes Date: January 25, 2018 Time: 9am-12:00pm Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: David Agler, M.D. Committee Member
Idaho DUR Board Meeting Minutes Date: January 25, 2018 Time: 9am-12:00pm Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: David Agler, M.D. Committee Member
News & Views. Antipsychotics on Maryland Medicaid PDL and Coverage of a 30-day Emergency Supply of Atypical Antipsychotics
 Maryland Medicaid Pharmacy Program News & Views February 2011 Maryland Department of Health and Mental Hygiene /Office of Systems, Operations and Pharmacy Antipsychotics on Maryland Medicaid PDL and Coverage
Maryland Medicaid Pharmacy Program News & Views February 2011 Maryland Department of Health and Mental Hygiene /Office of Systems, Operations and Pharmacy Antipsychotics on Maryland Medicaid PDL and Coverage
BY-STATE MENTAL HEALTH SERVICES AND EXPENDITURES IN MEDICAID, 1999
 STATE-BY BY-STATE MENTAL HEALTH SERVICES AND EXPENDITURES IN MEDICAID, 1999 James Verdier,, Ann Cherlow,, and Allison Barrett Mathematica Policy Research, Inc. Jeffrey Buck and Judith Teich Substance Abuse
STATE-BY BY-STATE MENTAL HEALTH SERVICES AND EXPENDITURES IN MEDICAID, 1999 James Verdier,, Ann Cherlow,, and Allison Barrett Mathematica Policy Research, Inc. Jeffrey Buck and Judith Teich Substance Abuse
Drug Utilization Review & Cost Reduction Strategies. Esther Liu, PharmD, MSIA, CGP Clinical Pharmacist Outcome Resources
 Drug Utilization Review & Cost Reduction Strategies Esther Liu, PharmD, MSIA, CGP Clinical Pharmacist Outcome Resources Goals and Objectives Define Drug Utilization Reviews Interpret various performance
Drug Utilization Review & Cost Reduction Strategies Esther Liu, PharmD, MSIA, CGP Clinical Pharmacist Outcome Resources Goals and Objectives Define Drug Utilization Reviews Interpret various performance
Connecticut Medical Assistance Pharmacy Program Drug Utilization Review (DUR) Program DUR Board Meeting
 Program DUR Board Meeting") June 2008 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair); Dennis Chapron, M.S.; Richard Gannon, Pharm.D.; Keith Lyke R.Ph., Mike Moore, R.Ph., MPH; Bhupesh Mangla, M.D., Ram Illindala,
June 2008 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair); Dennis Chapron, M.S.; Richard Gannon, Pharm.D.; Keith Lyke R.Ph., Mike Moore, R.Ph., MPH; Bhupesh Mangla, M.D., Ram Illindala,
MARYLAND MEDICAL ASSISTANCE PROGRAM Pharmacy Transmittal No Maryland Pharmacy Assistance Program Transmittal No. 39 February 22, 1999
 1 PT17-99 MARYLAND MEDICAL ASSISTANCE PROGRAM Pharmacy Transmittal No. 160 Maryland Pharmacy Assistance Program Transmittal No. 39 February 22, 1999 TO: FROM: NOTE: RE: Physicians Pharmacists Martin P.
1 PT17-99 MARYLAND MEDICAL ASSISTANCE PROGRAM Pharmacy Transmittal No. 160 Maryland Pharmacy Assistance Program Transmittal No. 39 February 22, 1999 TO: FROM: NOTE: RE: Physicians Pharmacists Martin P.
Policy Evaluation: Substance Use Disorders
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Idaho DUR Board Meeting Minutes. Committee Member Present: Matthew Hyde, Pharm.D., Perry Brown M.D., Paul Cady, Pharm.D., Ryan Heyborne M.D.
 Date: February 16, 2017 Time: 9am-12:15pm Idaho DUR Board Meeting Minutes Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Perry Brown, M.D. Committee Member
Date: February 16, 2017 Time: 9am-12:15pm Idaho DUR Board Meeting Minutes Location: Idaho Medicaid, 3232 Elder Street, Boise, Idaho, Conference Room D-West Moderator: Perry Brown, M.D. Committee Member
Follow-up to Previous Reviews. Foster Children Prescribers (Nurse Practitioner Practice Sites)
") 15 January 2015 1 Follow-up to Previous Reviews Foster Children Prescribers (Nurse Practitioner Practice Sites) 2 Foster Children Prescribers (Nurse Practitioner Practice Sites) 3 Ongoing Reviews Buprenorphine
15 January 2015 1 Follow-up to Previous Reviews Foster Children Prescribers (Nurse Practitioner Practice Sites) 2 Foster Children Prescribers (Nurse Practitioner Practice Sites) 3 Ongoing Reviews Buprenorphine
Medicare Part D Prescription Opioid Policies for 2019 Information for Pharmacists
 CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare Part D Prescription Opioid Policies for 2019 Information for Pharmacists Background Opioid medications are effective at treating certain types of pain,
CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare Part D Prescription Opioid Policies for 2019 Information for Pharmacists Background Opioid medications are effective at treating certain types of pain,
2018 Annual Meeting & Educational Conference Opioids In Workers Compensation: Research From WCRI
 2018 Annual Meeting & Educational Conference Opioids In Workers Compensation: Research From WCRI John W. Ruser, Ph.D. NCSI 2018 Annual Meeting June 12, 2018 AGENDA Introduce WCRI Opioid dispensing to injured
2018 Annual Meeting & Educational Conference Opioids In Workers Compensation: Research From WCRI John W. Ruser, Ph.D. NCSI 2018 Annual Meeting June 12, 2018 AGENDA Introduce WCRI Opioid dispensing to injured
TennCare Joint Committee for the Review of Narcotic Management Meeting Minutes
 State of Tennessee Department of Finance and Administration Bureau of TennCare 310 Great Circle Road Nashville, TN 37228 TennCare Joint Committee for the Review of Narcotic Management Meeting Minutes April
State of Tennessee Department of Finance and Administration Bureau of TennCare 310 Great Circle Road Nashville, TN 37228 TennCare Joint Committee for the Review of Narcotic Management Meeting Minutes April
PHARMACY Section 9. Overview. Preferred Drug List. Additions and Exceptions to the Preferred Drug List
 Overview The management of outpatient prescription drugs is an integral part of the medical management program to improve the health and well-being of our members. Prescriber and member involvement is
Overview The management of outpatient prescription drugs is an integral part of the medical management program to improve the health and well-being of our members. Prescriber and member involvement is
Legislative & Regulatory Update Brad Young, RxPlus Government Affairs
 Legislative & Regulatory Update 2018 Brad Young, RxPlus Government Affairs Disclosures Brad Young reports no actual or potential conflicts of interest associated with this presentation. 2 Learning Objectives
Legislative & Regulatory Update 2018 Brad Young, RxPlus Government Affairs Disclosures Brad Young reports no actual or potential conflicts of interest associated with this presentation. 2 Learning Objectives
Prescription Drugs North Carolina Policies. Carol Steckel, MPH Medicaid Director
 Prescription Drugs North Carolina Policies Carol Steckel, MPH Medicaid Director March 19, 2013 Pharmacy Services Optional service provided each year to about 1.5 million beneficiaries by 2,200 pharmacy
Prescription Drugs North Carolina Policies Carol Steckel, MPH Medicaid Director March 19, 2013 Pharmacy Services Optional service provided each year to about 1.5 million beneficiaries by 2,200 pharmacy
90-Day Generic Drug Discount List Treatment Medication Strength Dose Quantity Price Allergy/Cold&Flu Benzonatate 100mg Tablet 42 $15.
 90-Day Generic Drug Discount List Treatment Medication Strength Dose Quantity Price Allergy/Cold&Flu Benzonatate 100mg Tablet 42 $15.00 Allergy/Cold&Flu C-Phen Drops n/a Drops 90 $15.00 Allergy/Cold&Flu
90-Day Generic Drug Discount List Treatment Medication Strength Dose Quantity Price Allergy/Cold&Flu Benzonatate 100mg Tablet 42 $15.00 Allergy/Cold&Flu C-Phen Drops n/a Drops 90 $15.00 Allergy/Cold&Flu
Clinical Policy: Opioid Analgesics Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid
 Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
WA PMP Access by Public Payers. PDMP North Regional Meeting St. Louis, MO April 23-24
 WA PMP Access by Public Payers PDMP North Regional Meeting St. Louis, MO April 23-24 Public Insurer Access PDMP Statute: Allows PDMP data to be provided to Medicaid and Workers Compensation Primary Goal:
WA PMP Access by Public Payers PDMP North Regional Meeting St. Louis, MO April 23-24 Public Insurer Access PDMP Statute: Allows PDMP data to be provided to Medicaid and Workers Compensation Primary Goal:
The Latest Prescription Trends for Controlled Prescription Drugs
 The Latest Prescription Trends for Controlled Prescription Drugs September 1, 2015 Christopher M. Jones PharmD, MPH Senior Advisor Office of Public Health Strategy and Analysis Office of the Commissioner
The Latest Prescription Trends for Controlled Prescription Drugs September 1, 2015 Christopher M. Jones PharmD, MPH Senior Advisor Office of Public Health Strategy and Analysis Office of the Commissioner
CLINICAL POLICY Clinical Policy: Extended Release Opioid Analgesics
 Reference Number: AZ.CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and
Reference Number: AZ.CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and
D. Todd Bess, PharmD 1
 s Program as a Tool to Improve Patient Care and Fight the Drug Epidemic D. Todd Bess, Pharm.D. Director April 12, 2018 Disclosure Information I have no financial relationships to disclose. I will not discuss
s Program as a Tool to Improve Patient Care and Fight the Drug Epidemic D. Todd Bess, Pharm.D. Director April 12, 2018 Disclosure Information I have no financial relationships to disclose. I will not discuss
Medication Trends in Dialysis Patients Focus on Medicare Part D
 Medication Trends in Dialysis Patients Focus on Medicare Part D Wendy L. St. Peter, PharmD, FASN, FCCP Professor, College of Pharmacy, University of Minnesota Co-investigator, USRDS Collaborators USRDS
Medication Trends in Dialysis Patients Focus on Medicare Part D Wendy L. St. Peter, PharmD, FASN, FCCP Professor, College of Pharmacy, University of Minnesota Co-investigator, USRDS Collaborators USRDS
9/5/2011. Outline. 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A
 Prescription Drug Abuse Crises Outline 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A 1 1970s 1980s 2 The 1990s OXYCODONE Oxycodone/APAP OxyContin
Prescription Drug Abuse Crises Outline 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A 1 1970s 1980s 2 The 1990s OXYCODONE Oxycodone/APAP OxyContin
ST. LOUIS COUNTY DIABETES PREVENTION PROGRAMMING. Jim Gottschald, HR Director Building Minnesota s Diabetes Prevention System September 13-14, 2016
 ST. LOUIS COUNTY DIABETES PREVENTION PROGRAMMING Jim Gottschald, HR Director Building Minnesota s Diabetes Prevention System September 13-14, 2016 Self-Insured health plan 4,456 covered lives Actives Retirees
ST. LOUIS COUNTY DIABETES PREVENTION PROGRAMMING Jim Gottschald, HR Director Building Minnesota s Diabetes Prevention System September 13-14, 2016 Self-Insured health plan 4,456 covered lives Actives Retirees
Connecticut Medical Assistance Pharmacy Program Drug Utilization Review (DUR) Program DUR Board Meeting
 Program DUR Board Meeting") September 2018 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair), Keith Lyke, R.Ph., Bhupesh Mangla, MD, Richard Gannon, Pharm.D., Ram Illindala, MD, Dennis Chapron, Pharm.D. Ex Officio
September 2018 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair), Keith Lyke, R.Ph., Bhupesh Mangla, MD, Richard Gannon, Pharm.D., Ram Illindala, MD, Dennis Chapron, Pharm.D. Ex Officio
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Arkansas Prescription Monitoring Program
 Arkansas Prescription Monitoring Program FY 2016 Third Quarter Report January-March 2016 Arkansas Prescription Monitoring Program Quarterly Report January March, Fiscal year 2016 Act 304 of 2011 authorized
Arkansas Prescription Monitoring Program FY 2016 Third Quarter Report January-March 2016 Arkansas Prescription Monitoring Program Quarterly Report January March, Fiscal year 2016 Act 304 of 2011 authorized
Proposed Changes to Existing Measure for HEDIS : Use of Opioids at High Dosage (UOD)
") Proposed Changes to Existing Measure for HEDIS 1 2020: Use of Opioids at High Dosage (UOD) NCQA seeks comments on proposed revisions to the Use of Opioids at High Dosage HEDIS measure. The current measure
Proposed Changes to Existing Measure for HEDIS 1 2020: Use of Opioids at High Dosage (UOD) NCQA seeks comments on proposed revisions to the Use of Opioids at High Dosage HEDIS measure. The current measure
New Product to Market: Lonhala Magnair
 Drug Review and The following tables list the Agenda items as well as the that are scheduled to be presented and reviewed at the May 17, 2018 meeting of the Pharmacy and Therapeutics Advisory Committee.
Drug Review and The following tables list the Agenda items as well as the that are scheduled to be presented and reviewed at the May 17, 2018 meeting of the Pharmacy and Therapeutics Advisory Committee.
Managing Narcotics on Workers Comp Claims. Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc.
 Managing Narcotics on Workers Comp Claims Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc. October 21, 2014 Outline Rationale Scope list drug list Recommended
Managing Narcotics on Workers Comp Claims Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc. October 21, 2014 Outline Rationale Scope list drug list Recommended
Federal Fiscal Year 2015
 20 October 2016 1 Federal Fiscal Year 2015 2 Background Section 1927(g)(3)(D) of the Social Security Act (the Act) requires each State to submit an annual report on the operation of its Medicaid Drug Utilization
20 October 2016 1 Federal Fiscal Year 2015 2 Background Section 1927(g)(3)(D) of the Social Security Act (the Act) requires each State to submit an annual report on the operation of its Medicaid Drug Utilization
Medicare Star Ratings and the Shift to Quality- Based Payment Models. David Nau, RPh, PhD, FAPhA PQS President
 Medicare Star Ratings and the Shift to Quality- Based Payment Models David Nau, RPh, PhD, FAPhA PQS President The shift to Value-Driven Healthcare The U.S. health care system is rapidly moving to value-based
Medicare Star Ratings and the Shift to Quality- Based Payment Models David Nau, RPh, PhD, FAPhA PQS President The shift to Value-Driven Healthcare The U.S. health care system is rapidly moving to value-based
The power of partnership.
 School Board of Clay County and UnitedHealthcare. Building health ownership together. December 13, 2017 Annual Healthplan Performance Review October 1, 2016 thru September 30, 2017 Let s get started inspiring
School Board of Clay County and UnitedHealthcare. Building health ownership together. December 13, 2017 Annual Healthplan Performance Review October 1, 2016 thru September 30, 2017 Let s get started inspiring
MICHIGAN MEDICAID DRUG UTILIZATION REVIEW ANNUAL REPORT
 State of Michigan Department of Community Health MICHIGAN MEDICAID DRUG UTILIZATION REVIEW ANNUAL REPORT Prospective and Retrospective And Cost Analysis Federal Fiscal Year 2006 I. Program Background and
State of Michigan Department of Community Health MICHIGAN MEDICAID DRUG UTILIZATION REVIEW ANNUAL REPORT Prospective and Retrospective And Cost Analysis Federal Fiscal Year 2006 I. Program Background and
An Integrated Healthcare System s Approach to Chronic Pain
 An Integrated Healthcare System s Approach to Chronic Pain Presbyterian Health Plan (PHP) Charles Baumgart M.D., Chief Medical Officer Louanne Cunico PharmD, Pharmacy Director September 20, 2011 Medical
An Integrated Healthcare System s Approach to Chronic Pain Presbyterian Health Plan (PHP) Charles Baumgart M.D., Chief Medical Officer Louanne Cunico PharmD, Pharmacy Director September 20, 2011 Medical
Medi Cal Managed Care. Melissa Lamer, PharmD, BCPP July 31 st, 2014
 Pharmacy Benefit Carve Outs in Medi Cal Managed Care Melissa Lamer, PharmD, BCPP July 31 st, 2014 2 The Behavioral Health Carve Out Services Carved Out to the County Starting 1/1/2014 Medi Cal plans now
Pharmacy Benefit Carve Outs in Medi Cal Managed Care Melissa Lamer, PharmD, BCPP July 31 st, 2014 2 The Behavioral Health Carve Out Services Carved Out to the County Starting 1/1/2014 Medi Cal plans now
Monitoring Psychotropic Use Among Foster Children EMPAA
 State Plans for Monitoring Psychotropic Use Among Foster Children EMPAA October 30, 2012 Child and Family Services Improvement and Innovation Act of 2011 Required Components of Psychotropic Oversight and
State Plans for Monitoring Psychotropic Use Among Foster Children EMPAA October 30, 2012 Child and Family Services Improvement and Innovation Act of 2011 Required Components of Psychotropic Oversight and
Mandatory PDMP Use PDMP Use STATE Prescriber Dispenser Conditions, if applicable
 Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Indiana Medicaid Drug Utilization Review Board Newsletter
 Indiana Medicaid Drug Utilization Review Board Newsletter Volume 12 Issue 4 October 2009 Indiana Medicaid DUR Board Room W382 Indiana State Government Center, South 402 West Washington Street Indianapolis,
Indiana Medicaid Drug Utilization Review Board Newsletter Volume 12 Issue 4 October 2009 Indiana Medicaid DUR Board Room W382 Indiana State Government Center, South 402 West Washington Street Indianapolis,
Connecticut Medical Assistance Pharmacy Program Drug Utilization Review (DUR) Program DUR Board Meeting
 Program DUR Board Meeting") September 2008 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair); Dennis Chapron, M.S.; Richard Gannon, Pharm.D.; Keith Lyke R.Ph., Mike Moore, R.Ph., MPH; Bhupesh Mangla, M.D., Ram
September 2008 Minutes ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair); Dennis Chapron, M.S.; Richard Gannon, Pharm.D.; Keith Lyke R.Ph., Mike Moore, R.Ph., MPH; Bhupesh Mangla, M.D., Ram
9/25/15. Pharmacy Quality Measures: Financial Support. Learning Objectives. Speaker Disclosure. Access to Preferred Networks and Clinical Performance
 Pharmacy Quality Measures: Action Steps for Improvement Financial Support Financial support was provided for this activity through an unrestricted grant from Health Mart Systems, Inc. Christine Jacobson
Pharmacy Quality Measures: Action Steps for Improvement Financial Support Financial support was provided for this activity through an unrestricted grant from Health Mart Systems, Inc. Christine Jacobson
General Providers. Tamper-Resistant Prescription Requirements
 September 2008 Provider Bulletin Number 8138 General Providers Tamper-Resistant Prescription Requirements Effective with processing dates on and after October 1, 2008, written prescriptions for Kansas
September 2008 Provider Bulletin Number 8138 General Providers Tamper-Resistant Prescription Requirements Effective with processing dates on and after October 1, 2008, written prescriptions for Kansas
April 26, New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Board of Pharmacy Prescription Monitoring Program (PMP)
 New Mexico Board of Pharmacy Prescription Monitoring Program (PMP)") New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Nurse Practitioner Council New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) Peter Ryba, PharmD PMP Director
New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) New Mexico Nurse Practitioner Council New Mexico Board of Pharmacy Prescription Monitoring Program (PMP) Peter Ryba, PharmD PMP Director
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
MICHIGAN MEDICAID DRUG UTILIZATION REVIEW ANNUAL REPORT
 State of Michigan Department of Community Health MICHIGAN MEDICAID DRUG UTILIZATION REVIEW ANNUAL REPORT Prospective and Retrospective Drug Utilization Review And Cost Analysis Federal Fiscal Year 2009
State of Michigan Department of Community Health MICHIGAN MEDICAID DRUG UTILIZATION REVIEW ANNUAL REPORT Prospective and Retrospective Drug Utilization Review And Cost Analysis Federal Fiscal Year 2009
Mandatory PDMP Use PDMP Use STATE Prescriber Dispenser Conditions, if applicable
 Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Clinical Policy: Opioid Analgesics Reference Number: CP.PMN.97 Effective Date: Last Review Date: 02.19
 Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Notice from the Executive Officer: Promoting Compliance with the Existing Limited Use Criteria for Fentanyl Transdermal Patch
 Notice from the Executive Officer: Promoting Compliance with the Existing Limited Use Criteria for Fentanyl Transdermal Patch Frequently Asked Questions 1. What is the new Health Network System feature
Notice from the Executive Officer: Promoting Compliance with the Existing Limited Use Criteria for Fentanyl Transdermal Patch Frequently Asked Questions 1. What is the new Health Network System feature
Welcome - we will begin the webinar shortly Please read the participation tips below:
 Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Florida MEDS-AD Waiver
 Florida MEDS-AD Waiver 2 nd Quarter Report April 1, 2015 June 30, 2015 Demonstration Year 10 1115 Research and Demonstration Waiver #11-W-00205/4 This page intentionally left blank Table of Contents I.
Florida MEDS-AD Waiver 2 nd Quarter Report April 1, 2015 June 30, 2015 Demonstration Year 10 1115 Research and Demonstration Waiver #11-W-00205/4 This page intentionally left blank Table of Contents I.
Connecticut Medical Assistance Pharmacy Program Drug Utilization Review (DUR) Program DUR Board Meeting
 Program DUR Board Meeting") ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair), Keith Lyke R.Ph., Dennis Chapron, M.S., Bhupesh Mangla, M.D., Ram Illindala, M.D., Richard Gannon, Pharm.D., Carol Drufva R.Ph., Angela Moemeka,
ATTENDEES Board Members Present: Kenneth Fisher, R.Ph. (Chair), Keith Lyke R.Ph., Dennis Chapron, M.S., Bhupesh Mangla, M.D., Ram Illindala, M.D., Richard Gannon, Pharm.D., Carol Drufva R.Ph., Angela Moemeka,
Prescription Monitoring Program (PMP)
") 06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
Medicare Part D Opioid Policies for 2019 Information for Patients
 CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare Part D Opioid Policies for 2019 Information for Patients Introduction Prescription opioid pain medications like oxycodone (OxyContin ), hydrocodone (Vicodin
CENTERS FOR MEDICARE & MEDICAID SERVICES Medicare Part D Opioid Policies for 2019 Information for Patients Introduction Prescription opioid pain medications like oxycodone (OxyContin ), hydrocodone (Vicodin
Alaska Medicaid 90 Day** Generic Prescription Medication List
 1 ACYCLOVIR 200 MG CAPSULE BUPROPION HCL 150 MG TAB ER 24H ACYCLOVIR 200 MG/5ML BUPROPION HCL 150 MG TABLET ER ACYCLOVIR 400 MG TABLET BUPROPION HCL 150 MG TABLET ER ACYCLOVIR 800 MG TABLET BUPROPION HCL
1 ACYCLOVIR 200 MG CAPSULE BUPROPION HCL 150 MG TAB ER 24H ACYCLOVIR 200 MG/5ML BUPROPION HCL 150 MG TABLET ER ACYCLOVIR 400 MG TABLET BUPROPION HCL 150 MG TABLET ER ACYCLOVIR 800 MG TABLET BUPROPION HCL
Drug Use Evaluation: Low Dose Quetiapine
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The STOP Measure. Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018
 The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
Amitriptyline Hydrochloride Heart Health & BP Amlodipine Besylate 5mg Norvasc Antibiotics Amoxicillin 500 mg Amoxil
 Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70 mg Fosamax Arthritis
Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70 mg Fosamax Arthritis
See Important Reminder at the end of this policy for important regulatory and legal information.
 Effective Date: 04.18 Last Review Date: 04.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description
Effective Date: 04.18 Last Review Date: 04.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description
Kentucky Department for Medicaid Services Pharmacy and Therapeutics Advisory Committee Recommendations
 Kentucky Department for Medicaid Services Pharmacy and May 17, 2018 The following chart provides a summary of the recommendations that were made by the Pharmacy and Therapeutics (P&T) Advisory Committee
Kentucky Department for Medicaid Services Pharmacy and May 17, 2018 The following chart provides a summary of the recommendations that were made by the Pharmacy and Therapeutics (P&T) Advisory Committee
Follow-up to Previous Reviews. Multiple Dosage Forms of Aripiprazole Prescribed Concomitantly
 15 October 2015 1 Follow-up to Previous Reviews Multiple Dosage Forms of Aripiprazole Prescribed Concomitantly 2 Multiple Dosage Forms of Aripiprazole Prescribed Concomitantly Usual maximum FDA approved
15 October 2015 1 Follow-up to Previous Reviews Multiple Dosage Forms of Aripiprazole Prescribed Concomitantly 2 Multiple Dosage Forms of Aripiprazole Prescribed Concomitantly Usual maximum FDA approved
Amitriptyline Hydrochloride Heart Health & BP Amlodipine Besylate 5mg Norvasc Antibiotics Amoxicillin 500 mg Amoxil
 School Corp Formulary Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70
School Corp Formulary Antiviral Acyclovir 400mg Zovirax Asthma Advair Diskus Diskus 250/50 Fluticasone/Salmeterol Asthma Albuterol Sulfate 2.5 mg/3 ml Proventil Arthritis and Pain Allendronate Sodium 70
WORKERS COMPENSATION AND PRESCRIPTION DRUGS: 2016 Update
 September 2016 By Barry Lipton and David Colón WORKERS COMPENSATION AND PRESCRIPTION DRUGS: 2016 Update INTRODUCTION Prescription drug (Rx) costs represent a significant portion of workers compensation
September 2016 By Barry Lipton and David Colón WORKERS COMPENSATION AND PRESCRIPTION DRUGS: 2016 Update INTRODUCTION Prescription drug (Rx) costs represent a significant portion of workers compensation
Hundreds of Choices. More Savings Every Day. 8 and $ 12 Generics Also Available. Based on 30-day supply at commonly prescribed doses
 4$ Hundreds of Choices. More Savings Every Day. $ 8 and $ 12 Generics Also Available. Based on 30-day supply at commonly prescribed doses EFF. DATE 09/2017 List subject to change ALLERGIES, COLD AND FLU
4$ Hundreds of Choices. More Savings Every Day. $ 8 and $ 12 Generics Also Available. Based on 30-day supply at commonly prescribed doses EFF. DATE 09/2017 List subject to change ALLERGIES, COLD AND FLU
ACO Congress Conference Pre Session Clinical Performance Measurement
 ACO Congress Conference Pre Session Clinical Performance Measurement Lynne Rothney-Kozlak, MPH Interim VP, ACO Collaborative (Independent Consultant) October 25, 2010 Agenda for Presentation 1. The Framework
ACO Congress Conference Pre Session Clinical Performance Measurement Lynne Rothney-Kozlak, MPH Interim VP, ACO Collaborative (Independent Consultant) October 25, 2010 Agenda for Presentation 1. The Framework
Evaluation of a Medicaid Psychotropic Drug Management Program in Utah
 Evaluation of a Medicaid Psychotropic Drug Management Program in Utah Dominick Esposito James M. Verdier 2008 SAMHSA/CMS Invitational Conference on Medicaid and Mental Health Service/Substance Abuse Treatment
Evaluation of a Medicaid Psychotropic Drug Management Program in Utah Dominick Esposito James M. Verdier 2008 SAMHSA/CMS Invitational Conference on Medicaid and Mental Health Service/Substance Abuse Treatment
Questions and answers about HCA s opioid clinical policy for Apple Health (Medicaid)
") Questions and answers about HCA s opioid clinical policy for Apple Health (Medicaid) This Q&A covers questions the Health Care Authority (HCA) received during webinars about the opioid clinical policy
Questions and answers about HCA s opioid clinical policy for Apple Health (Medicaid) This Q&A covers questions the Health Care Authority (HCA) received during webinars about the opioid clinical policy
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Background. CMS finalized new policies for Medicare drug plans to follow starting on January 1,2019.
 Background CMS finalized new policies for Medicare drug plans to follow starting on January 1,2019. These policies involve further partnershipwith providers and prescription drug plans. Providers are in
Background CMS finalized new policies for Medicare drug plans to follow starting on January 1,2019. These policies involve further partnershipwith providers and prescription drug plans. Providers are in
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: LA.PPA.12 Effective Date: 02/11 Last Review Date: 01/18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this policy for
Clinical Policy: Reference Number: LA.PPA.12 Effective Date: 02/11 Last Review Date: 01/18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this policy for
Clinical Policy: Opioid Analgesics Reference Number: CP.PMN.97 Effective Date: Last Review Date: 02.18
 Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Opiate Use among Ohio Medicaid Recipients
 Opiate Use among Ohio Medicaid Recipients July 12, 2012 Ohio Colleges of Medicine Government Resource Center The Ohio State University College of Public Health Sponsored by The Ohio Department of Alcohol
Opiate Use among Ohio Medicaid Recipients July 12, 2012 Ohio Colleges of Medicine Government Resource Center The Ohio State University College of Public Health Sponsored by The Ohio Department of Alcohol
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy