Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
|
|
|
- Alfred Phillips
- 6 years ago
- Views:
Transcription

1 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
2 Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive or mixed forms most common 65-70% undiagnosed if routine monitoring not implemented <5% of Canadian ICUs routinely monitor for delirium Ely ICM 2001; 27: Pandharipande J Trauma 2008;65:34-41 Ouimet ICM 2007;33: Lat CCM 2009;37:
3 Sequelae of Delirium During the ICU or Hospital stay 5 fewer ventilator free days 3x greater re-intubation rate ~10 additional days in hospital $15-25K higher hospital costs Mortality Post hospital discharge Mortality 9x higher incidence of cognitive impairment Transfer to chronic care facility Functional 6 months Milbrandt CCM 2004;32: Lin CCM 2004;32: Ely JAMA 2004;291:

4
5 Delirium Treatment Am Psychiatric Association (1999) Antipsychotic medications are often the pharmacologic treatment of choice (grade I = recommended with substantial clinical confidence) Some clinicians choose to use atypical antipsychotics SCCM (2002) Haloperidol is the preferred agent for the treatment of delirium in critically ill patients (grade C recommendations) Use of antipsychotics is common practice in ICUs (25-40%) Lack of substantial evidence treatment improves clinical outcomes plus significant adverse effects associated with antipsychotics, energies should focus on prevention Trzepacz APA 1999 Jacobi CCM 2002;30: Patel CCM 2009;37: Wang NEJM 2005
6
7
8
.")
9 18767 studies reporting on medications and delirium 136 medications listed as potential causes Estimated 40% of delirium cases are caused by medications Numerous limitations in study design (e.g. size, definition of drug exposure).

10 Prevention protocols non ICU patients
11 Opioids Conflicting data! Evidence from 2 moderate quality multivariate analyses support association of increased delirium risk in medical-surgical patients Dubois et al: Morphine all doses OR & Epidural OR 3.5 ( ) Recent no sedation study (opioid offered without sedation) found this strategy to be associated with increased agitated delirium (n = 140 pt; 20% vs. 7%; p=0 0400) Inverse dose-response relationship in patients recovering from hip fracture < 10 mg morphine RR 25.2, 95% CI mg morphine RR 4.4, 95% CI Clegg Age and Ageing 2010;0:1-7 Gaudreau Psychosomatics 2005;46: Dubois Int Care Med 2001;27: Strom Lancet 2010;375:
] vs TICU [OR 1.03 (0.47, 2.25)] Exposed to morphine: SICU [OR 0.37(0.13-1.08)] vs TICU [OR 0.22(0.06-0.")
12 Opioids - Surgical & Trauma ICU patients N = 100; 70% had delirium Figure illustrates the proportion of time that pts were delirious while receiving the drug vs. those not exposed Exposed to fentanyl: SICU [OR 3.99 (1.47,10.85)] vs TICU [OR 1.03 (0.47, 2.25)] Exposed to morphine: SICU [OR 0.37( )] vs TICU [OR 0.22( )] caution low # of patients included
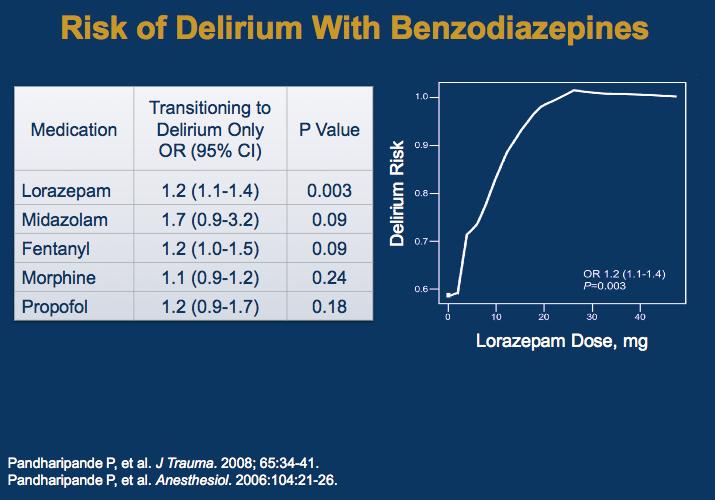
13 Benzodiazepines In a mixed ICU Dubois et al (n = 216) found lorazepam doses > 1.8 mg/day was linked to delirium OR 3.3 ( ) by univariate analysis; multivariate not significant In mixed ICUs Van Rompaey et al (n = 523) found OR 2.89 ( ) Higher doses during a 24 hr period associated with increased risk compared to lower doses OR 3.3 ( ) vs. 2.6 ( ) In a MICU Pisani et al (n = 304 > 60 years) found exposure to benzodiazepine or opioid to be associated with increased duration of delirium [RR 1.64 ( )] Clegg Age and Ageing 2010;0:1-7 Dubois Int Care Med 2001;27: Pisani Crit Care Med 2009;37:
14
] TICU [OR (2.45 (1.09,5.52, p 0.")
15 Midazolam - Surgical-Trauma ICU patients 100 surgical-trauma ICU patients Exposed to midazolam: SICU [OR ( 3.22 ( , p 0.007)] TICU [OR (2.45 (1.09,5.52, p 0.936] Most consistent & significant predictor of transitioning into delirium
16
17
18 Agents with significant anticholinergic effects Atropine Antidepressants amitriptyline, clomipramine, doxepin, phenelzine paroxetine Antipsychotics chlorpromazine, clozapine, olanzapine, thioridazine Anti-allergy diphenhydramine, hydroxyzine Antiemetics dimenhydrinate, promethazine, scopolamine Belladona alkaloids Parkinsonism amatadine, benztropine, biperidine, trihexyphenidyl
19 Strong Anticholinergics Pisani et al: N = 304 MICU; > 60 years Evaluated impact of drugs on the duration of delirium Administration of anticholinergic to 32% of patients Anticholinergics were not associated with increased duration of delirium Pandharipande et al: N = 198 MICU patients 32% (63) were administered anticholinergics; 83% (n = 52) experienced delirium Administration of anticholinergic was not associated in univariate or multivariable analysis with delirium Pandharipande Anesthesiology 2006;104(1):21-26 Han Arch Intern Med 2001;161:
20 SLEAP RCT Mehta ESICM 2012
21 SLEAP RCT Mehta ESICM 2012
22 Work in progress A prospective evaluation of the association between psychoactive medications and delirium in critically ill adults 535 mixed ICU patients from 6 sites admitted at least 24 hr Daily delirium assessment with ICDSC until discharge Pre-enrollment drug exposure, cigarettes, illicit drugs and ethanol use Captured daily drug exposure, use of sedation strategies, physical restraint use, catheters, lab values, environmental factors, mobilization, clinical outcomes Enrollment closed June 27, 2012
23 Summary Delirium is common in the ICU & associated with poor outcomes Medications are an important consideration for patients with or at risk of delirium Whether or not sufficient evidence that these medications cause delirium there are significant other benefits from reducing sedative doses (e.g. duration of MV) Further clarification of the risk of delirium following exposure to medications is important for changing prescribing practices including further evaluation of dose relationships, impact of drug titration strategies (e.g. DSI), & polypharmacy
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Delirium: Prevention with Melatonin
 Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
Delirium: Prevention with Melatonin Lisa Burry, PharmD Department of Pharmacy, Mount Sinai Hospital Leslie Dan Faculty of Pharmacy, University of Toronto Disclosures Centre for Collaborative Drug Research,
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients
 Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients 1 Determine transfer risks as per BC Ambulance Risk Stratification Tool 2 Determine required sedation level accordingly: RASS Level
Sedation Guidelines for Air Ambulance Transfer of Psychiatric Patients 1 Determine transfer risks as per BC Ambulance Risk Stratification Tool 2 Determine required sedation level accordingly: RASS Level
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Iatrogenic Delirium. Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center
 Iatrogenic Delirium Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center Objectives Discuss proposed mechanisms of medication induced delirium Identify
Iatrogenic Delirium Heather Carey, PharmD, BCPP Clinical Psychiatric Pharmacist University Hospitals Richmond Medical Center Objectives Discuss proposed mechanisms of medication induced delirium Identify
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes
 The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Supplementary Online Content
 Supplementary Online Content Gray SL, Anderson ML, Dublin S, et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med. Published online January
Supplementary Online Content Gray SL, Anderson ML, Dublin S, et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med. Published online January
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: Drugs in Older Adults: Beers Criteria Heather Sakely,
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: Drugs in Older Adults: Beers Criteria Heather Sakely,
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Interprofessional Trauma Conference September 28th 2018 Montreal
 Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
From the Department of Pharmacy (JM, CAF) and Department of Pulmonary and Critical
 and Department of Pulmonary and Critical") PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
PrintClose Impact of a clinical pharmacist-enforced intensive care unit sedation protocol on duration of mechanical ventilation and hospital stay * Author(s): Marshall, John PharmD; Finn, Christine A.
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Delirium Screening and Prevention. Faculty Disclosures. Objectives 5/13/2014. I have nothing to disclose
 Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium Screening and Prevention Faculty Disclosures
 Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Medicine Related Falls Risk Assessment Tool (MRFRAT)
") Medicine Related Falls Risk Assessment Tool (MRFRAT) The Medicine Related Falls Risk Assessment tool (MRFRAT) in Appendix 1 is designed to help identify patients at risk of falls due to their current medicine
Medicine Related Falls Risk Assessment Tool (MRFRAT) The Medicine Related Falls Risk Assessment tool (MRFRAT) in Appendix 1 is designed to help identify patients at risk of falls due to their current medicine
ALAMEDA COUNTY BEHAVIORAL HEALTH CARE SERVICES MEDICATION FORMULARY
 ANTIDEPRESSANTS Serotonin Selective Reuptake Inhibitors citalopram 10, 20, 40 mg, 10 mg/5cc $ 0.40 No escitalopram 10, 20 mg $ 2.60 Yes fluoxetine 10, 20 mg, 20 mg/5 ml $ 0.40 Yes fluvoxamine 25, 50, 100
ANTIDEPRESSANTS Serotonin Selective Reuptake Inhibitors citalopram 10, 20, 40 mg, 10 mg/5cc $ 0.40 No escitalopram 10, 20 mg $ 2.60 Yes fluoxetine 10, 20 mg, 20 mg/5 ml $ 0.40 Yes fluvoxamine 25, 50, 100
Nicotine replacement therapy for agitation and delirium management in the intensive care unit: a systematic review of the literature
 Kowalski et al. Journal of Intensive Care (2016) 4:69 DOI 10.1186/s40560-016-0184-x RESEARCH Nicotine replacement therapy for agitation and delirium management in the intensive care unit: a systematic
Kowalski et al. Journal of Intensive Care (2016) 4:69 DOI 10.1186/s40560-016-0184-x RESEARCH Nicotine replacement therapy for agitation and delirium management in the intensive care unit: a systematic
Juliana Barr, MD, FCCM
 Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
Juliana Barr, MD, FCCM Staff Anesthesiologist and Intensivist, VA Palo Alto Health Care System Associate Professor, Anesthesiology, Perioperative, and Pain Medicine Stanford University School of Medicine
The Difficult to Sedate ICU Patient
 The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
The Difficult to Sedate ICU Patient Dan Burkhardt, M.D. Associate Professor Department of Anesthesia and Perioperative Care University of California San Francisco burkhard@anesthesia.ucsf.edu Richmond
Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients
 Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients Timothy J. Wiegand, MD Associate Clinical Professor of Emergency Medicine,
Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients Timothy J. Wiegand, MD Associate Clinical Professor of Emergency Medicine,
Dementia Pharmacotherapy
 Dementia Pharmacotherapy 1 early therapeutic interventions can maximize pharmacologic efficacy with these agents 2 Selecting a Medication Not enough evidence to recommend one agent over another based on
Dementia Pharmacotherapy 1 early therapeutic interventions can maximize pharmacologic efficacy with these agents 2 Selecting a Medication Not enough evidence to recommend one agent over another based on
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Brain dysfunction in the ICU
 High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
High cortisol levels are associated with brain dysfunction but low prolactin cortisol ratio levels are associated with nosocomial infection in severe sepsis Duc Nam Nguyen Luc Huyghens Johan Schiettecatte
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Disclosures No financial conflicts of interest. Key Questions
 Hospital Delirium: New Evidence in Diagnosis & Treatment Ethan Cumbler MD, FHM, FACP Professor of Medicine Medical Director Acute Care For Elderly Unit University of Colorado School of Medicine Disclosures
Hospital Delirium: New Evidence in Diagnosis & Treatment Ethan Cumbler MD, FHM, FACP Professor of Medicine Medical Director Acute Care For Elderly Unit University of Colorado School of Medicine Disclosures
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc.
 MSc.") Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Sleep in the ICU: helped by drugs? Yoanna Skrobik MD FRCP(c) MSc. Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee Vice-chair, SCCM Pain, Agitation, Delirium,
Delirium is a frequent complication in the ICU setting.
 Clinical Investigations Dexmedetomidine for the Treatment of Hyperactive Delirium Refractory to Haloperidol in Nonintubated ICU Patients: A Nonrandomized Controlled Trial* Genís Carrasco, PhD, MD; Nacho
Clinical Investigations Dexmedetomidine for the Treatment of Hyperactive Delirium Refractory to Haloperidol in Nonintubated ICU Patients: A Nonrandomized Controlled Trial* Genís Carrasco, PhD, MD; Nacho
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES
 WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
WAKE UP AND TREAT DELIRIUM : PITFALLS OF THE PAD GUIDELINES Tudy Hodgman, Pharm D, FCCM, BCPS The goal of this discussion will be to review the literature published since the PAD guidelines were released
SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD
 SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD OVERVIEW Correctable causes of agitation Pain assessment opioids Agitation assessment BZNs, propofol, precedex comparisons Delirium haldol, antipsychotics
SEDATION, AGITATION, DELIRIUM Daniel Lollar, MD OVERVIEW Correctable causes of agitation Pain assessment opioids Agitation assessment BZNs, propofol, precedex comparisons Delirium haldol, antipsychotics
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Monday, October 17 3:45 p.m. 5:45 p.m. Convention Center: Spirit of Pittsburgh Ballroom A
 Critical Care PRN and Society of Critical Care Medicine Focus Session Sedation and Delirium in the ICU: Update on the Status of the 2011 SCCM Guidelines Activity No. 0217-0000-11-079-L01-P (Application-Based
Critical Care PRN and Society of Critical Care Medicine Focus Session Sedation and Delirium in the ICU: Update on the Status of the 2011 SCCM Guidelines Activity No. 0217-0000-11-079-L01-P (Application-Based
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Preventing Delirium in the IntensiveCareUnit
 Preventing Delirium in the IntensiveCareUnit Nathan E. Brummel, MD a,b,c, *, Timothy D. Girard, MD, MSCI a,b,c,d KEYWORDS Delirium Intensive care unit Prevention Sedation KEY POINTS Delirium in the intensive
Preventing Delirium in the IntensiveCareUnit Nathan E. Brummel, MD a,b,c, *, Timothy D. Girard, MD, MSCI a,b,c,d KEYWORDS Delirium Intensive care unit Prevention Sedation KEY POINTS Delirium in the intensive
( delirium ) 15%- ( extrapyramidal syndrome ) risperidone olanzapine ( extrapyramidal side effect ) olanzapine ( Delirium Rating Scale, DRS )
 15%- ( extrapyramidal syndrome ) risperidone olanzapine ( extrapyramidal side effect ) olanzapine ( Delirium Rating Scale, DRS )") 2005 6 48-52 Olanzapine 30% ( delirium 5%- Haloperidol ( extrapyramidal syndrome risperidone ( extrapyramidal side effect ( Delirium Rating Scale, DRS ( Delirium ( Olanzapine ( Delirium Rating Scale, DRS
2005 6 48-52 Olanzapine 30% ( delirium 5%- Haloperidol ( extrapyramidal syndrome risperidone ( extrapyramidal side effect ( Delirium Rating Scale, DRS ( Delirium ( Olanzapine ( Delirium Rating Scale, DRS
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium
 ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
ICU Liberation ABCDEF Bundle Implementation: Focus on Delirium Diane Byrum MSN RN CCRN-K CCNS FCCM Quality Implementation Consultant Innovative Solutions For Healthcare Education, LLC Oak Island, NC ICU
Appendix E: Cohort studies - methodological quality: Non pharmacological risk factors
 Appendix E: studies - methodological quality: n pharmacological risk factors Study Andersson 2001; 51/24 (=2) All patients followed up until discharge but in numbers of number of variables studied; 4/4
Appendix E: studies - methodological quality: n pharmacological risk factors Study Andersson 2001; 51/24 (=2) All patients followed up until discharge but in numbers of number of variables studied; 4/4
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013
 A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
A17/B17: Delirium Can Be Deadly: Save Lives With a Standardized Approach to Delirium IHI 25th Annual National Forum, December 10, 2013 Clay Angel, MD, Hospital Medicine; Chief of Continuum/SNF Kristen
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Drugs, Sleep & Wakefulness. Brian Koo Reena Mehra MD MS Kingman Strohl MD
 Drugs, Sleep & Wakefulness Brian Koo Reena Mehra MD MS Kingman Strohl MD Things To Keep In Mind Many drugs effect sleep either causing insomnia or sedation Disruption of sleep and wakefulness may not be
Drugs, Sleep & Wakefulness Brian Koo Reena Mehra MD MS Kingman Strohl MD Things To Keep In Mind Many drugs effect sleep either causing insomnia or sedation Disruption of sleep and wakefulness may not be
Quality ID #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety
: Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety") Quality ID #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Quality ID #238 (NQF 0022): Use of High-Risk Medications in the Elderly National Quality Strategy Domain: Patient Safety 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Approach to agitated patient in ICU
 Approach to agitated patient in ICU 12-2-2016 Kodati Rakesh Senior resident Pulmonary medicine Agitation Psychomotor disturbance characterized by a marked increase in both motor and psychological activities,
Approach to agitated patient in ICU 12-2-2016 Kodati Rakesh Senior resident Pulmonary medicine Agitation Psychomotor disturbance characterized by a marked increase in both motor and psychological activities,
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Policy Evaluation: Low Dose Quetiapine Safety Edit
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University 500 Summer Street NE, E35, Salem, Oregon 97301 1079 Phone 503 947 5220 Fax 503
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist
 Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Practical Management of the Delirious Patient with Mental Retardation by the Nurse Anesthetist 1. Basic Facts on Delirium The nurse anesthetist plays an important role in prevention of delirium among surgical
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Use of Anti-Psychotic Agents in Irish Long Term Care Residents with Dementia
 Use of Anti-Psychotic Agents in Irish Long Term Care Residents with Dementia Aine Leen, Kieran Walsh, David O Sullivan, Denis O Mahony, Stephen Byrne, Margaret Bermingham Pharmaceutical Care Research Group,
Use of Anti-Psychotic Agents in Irish Long Term Care Residents with Dementia Aine Leen, Kieran Walsh, David O Sullivan, Denis O Mahony, Stephen Byrne, Margaret Bermingham Pharmaceutical Care Research Group,
Medicine Related Falls Risk Assessment Tool (MrFRAT) User Guide for Age Related Residential Care Facility Staff in Hawke s Bay
 User Guide for Age Related Residential Care Facility Staff in Hawke s Bay") Medicine Related Falls Risk Assessment Tool (MrFRAT) User Guide for Age Related Residential Care Facility Staff in Hawke s Bay (Revised edition November 2015) The Medicine Related Falls Risk Assessment
Medicine Related Falls Risk Assessment Tool (MrFRAT) User Guide for Age Related Residential Care Facility Staff in Hawke s Bay (Revised edition November 2015) The Medicine Related Falls Risk Assessment
Delirium in Critically Ill Mechanically Ventilated Patients Enrolled in the SLEAP Multicenter Randomized Trial
 Delirium in Critically Ill Mechanically Ventilated Patients Enrolled in the SLEAP Multicenter Randomized Trial Geeta Mehta MD, FRCPC And The SLEAP Investigators For the Canadian Critical Care Trials Group
Delirium in Critically Ill Mechanically Ventilated Patients Enrolled in the SLEAP Multicenter Randomized Trial Geeta Mehta MD, FRCPC And The SLEAP Investigators For the Canadian Critical Care Trials Group
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Medicines Management and the Unwell Parkinson s Patient
 Medicines Management and the Unwell Parkinson s Patient Belinda Kessel Geriatrician and Movement Disorder Specialist Princess Royal University Hospital Orpington, Kent The Society for Acute Medicine, 7
Medicines Management and the Unwell Parkinson s Patient Belinda Kessel Geriatrician and Movement Disorder Specialist Princess Royal University Hospital Orpington, Kent The Society for Acute Medicine, 7
Occurrence of delirium is severely underestimated in the ICU during daily care
 Intensive Care Med (2009) 35:1276 1280 DOI 10.1007/s00134-009-1466-8 BRIEF REPORT Peter E. Spronk Bea Riekerk José Hofhuis Johannes H. Rommes Occurrence of delirium is severely underestimated in the ICU
Intensive Care Med (2009) 35:1276 1280 DOI 10.1007/s00134-009-1466-8 BRIEF REPORT Peter E. Spronk Bea Riekerk José Hofhuis Johannes H. Rommes Occurrence of delirium is severely underestimated in the ICU
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment
 Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Analgesia, Sedation and Delirium The Latest Evidence in Assessment & Treatment Julie Miller, RN, BSN, CCRN How many of you routinely assess for delirium in your patients? 2013 SCCM Guidelines Pain Recommend
Restraint as a Last Resort in Acute Care. Seniors Health Strategic Clinical Network in collaboration with Health Professions Strategy and Practice
 Restraint as a Last Resort in Acute Care Seniors Health Strategic Clinical Network in collaboration with Health Professions Strategy and Practice 2017 Alberta Health Services, Health Professions, Strategy
Restraint as a Last Resort in Acute Care Seniors Health Strategic Clinical Network in collaboration with Health Professions Strategy and Practice 2017 Alberta Health Services, Health Professions, Strategy