Delirium, Dementia, and Amnestic Disorders. Dr.Al-Azzam 1
|
|
|
- Horace Stephens
- 6 years ago
- Views:
Transcription
1 Delirium, Dementia, and Amnestic Disorders Dr.Al-Azzam 1
2 Introduction Disorders in which a clinically significant deficit in cognition or memory exists The number of people with these disorders is growing because more people now survive into the high-risk period for dementia, which is middle age and beyond. Dr.Al-Azzam 2
3 Delirium Characterized by a disturbance of consciousness and a change in cognition that develop rapidly over a short period. Its a mental state characterized by a disturbance of cognition, which is manifested by confusion, excitement, disorientation, and a clouding of consciousness. Hallucinations and illusions are common. Dr.Al-Azzam 3
4 Delirium Usually begins abruptly Can have a slower onset if underlying etiology is systemic illness or metabolic imbalance Duration usually brief and subsides completely on recovery from underlying determinant Dr.Al-Azzam 4
5 The duration of delirium is usually brief (e.g., 1 week; rarely more than 1 month) and, on recovery from the underlying determinant, symptoms usually diminish over a 3- to 7-day period, but in some instances may take as long as 2 weeks The age of the client and duration of the delirium influence rate of symptom resolution. Delirium may transition into a more permanent cognitive disorder (e.g., dementia) and is associated with a high mortality rate Dr.Al-Azzam 5
6 Predisposing Factors Delirium due to a General Medical Condition Substance-Induced Delirium Substance-Intoxication Delirium Substance-Withdrawal Delirium Delirium due to Multiple Causes Dr.Al-Azzam 6
7 Dementia Defined by a loss of previous levels of cognitive, executive, and memory function in a state of full alertness. Primary dementias: dementia itself is the major sign of some organic brain disease not directly related to any other organic illness (Alzheimer) Secondary dementias: caused by or related to another disease or condition, such as human immunodeficiency virus (HIV) disease or a cerebral trauma. Dr.Al-Azzam 7
8 Symptoms As the disease progresses, apraxia is evident. the inability to carry out motor activities despite intact motor function, may develop. Memory Function Dr.Al-Azzam 8
9 Etiological Implication Dementia of the Alzheimer s type Vascular dementia Dementia due to HIV disease Dementia due to head trauma Dementia due to Parkinson s disease Dementia due to Huntington s disease Dementia due to Pick s disease Dementia due to Creutzfeldt-Jakob Dr.Al-Azzam disease 9
10 Alzheimer s disease accounts for 60 to 80 percent of all cases of dementia AD can be described in stages: Stage 1. No apparent symptoms Stage 2. Forgetfulness Stage 3. Mild cognitive decline Stage 4. Mild-to-moderate cognitive decline; confusion Stage 5. Moderate cognitive decline; early dementia Stage 6. Moderate-to-severe cognitive decline; middle dementia Stage 7. Severe cognitive decline; late dementia Dr.Al-Azzam 10
11 Dementia of the Alzheimer s type Onset is slow and insidious, and the course of the disorder is generally progressive and deteriorating. Early onset (first symptoms at age 65 or before) Late onset (first symptoms after age 65) Etiologies may include Acetylcholine alterations Plaques and tangles Head trauma Genetic factors Dr.Al-Azzam 11
12 Vascular dementia Dementia is due to significant cerebrovascular disease. There is a more abrupt onset than is seen in association with Alzheimer s disease, and the course is more variable. Etiologies may include Arterial hypertension Cerebral emboli Cerebral thrombosis Dr.Al-Azzam 12
13 Dementia due to HIV disease Dementia results from brain infections caused by opportunistic organisms or the HIV-1 virus directly. Symptoms may range from barely perceptible changes to acute delirium to profound dementia. Dr.Al-Azzam 13
14 Dementia due to head trauma Serious head trauma can result in symptoms associated with the syndrome of dementia. * Amnesia is the most common symptom Repeated head trauma can result in dementia pugilistica with symptoms of: * Dysarthria * Emotional lability * Ataxia * Impulsivity Dr.Al-Azzam 14
15 Dementia due to Huntington s Disease Dementia due to Huntington s disease Damage from this disease occurs in the areas of the basal ganglia and the cerebral cortex. The client usually declines into a profound state of dementia and ataxia. Average course of the disease to complete incapacitation and death is about 15 years. Dr.Al-Azzam 15
16 Dementia Due to Pick s Disease Etiology of Pick s disease is unknown Clinical picture similar to that of Alzheimer s disease Pathology results from atrophy in the frontal and temporal lobes of the brain Dr.Al-Azzam 16
17 Dementia due to Creutzfeldt- Jakob disease - Clinical symptoms typical of syndrome of dementia Symptoms also include involuntary movements, muscle rigidity, and ataxia Onset of symptoms typically occurs between ages 40 and 60 years; course is extremely rapid, with progressive deterioration and death within 1 year Etiology is thought to be a transmissible agent known as a slow virus. There is a genetic component in 5 to 15 percent. Dr.Al-Azzam 17
18 Dementia due to other medical conditions Endocrine disorders Pulmonary disease Hepatic or renal failure Cardiopulmonary insufficiency Fluid and electrolyte imbalance Nutritional deficiencies Frontal lobe or temporal lobe lesions CNS or systemic infection Uncontrolled epilepsy or other neurological conditions Dr.Al-Azzam 18
19 Substance-induced persisting dementia Related to the persistent effects of abuse of substances such as: Alcohol Inhalants Sedatives, hypnotics, and anxiolytics Medications (e.g., anticonvulsants, intrathecal methotrexate) Toxins (e.g., lead, mercury, carbon monoxide, organophosphate insecticides, industrial solvents) Dr.Al-Azzam 19
20 Amnestic Disorders Amnestic disorders are characterized by an inability to Learn new information despite normal attention Recall previously learned information Symptoms Disorientation to place and time (rarely to self) Confabulation, the creation of imaginary events to fill in memory gapsdenial that a problem exists or acknowledgment that a problem exists, but with a lack of concern Apathy, lack of initiative, and emotional blandness Dr.Al-Azzam 20
21 Onset may be acute or insidious, depending on underlying pathological process. Duration and course may be quite variable and are also correlated with extent and severity of the cause. Dr.Al-Azzam 21
22 Dr.Al-Azzam 22
23 Amnestic Disorder due to a General Medical Condition Head trauma Cerebrovascular disease Cerebral neoplastic disease Cerebral anoxia Herpes simplex virus related encephalitis Poorly controlled diabetes Surgical intervention to the brain Dr.Al-Azzam 23
24 Substance-Induced Persisting Amnestic Disorder Related to - Alcohol abuse Sedatives, hypnotics, and anxiolytics Medications (e.g., anticonvulsants, intrathecal methotrexate) Toxins (e.g., lead, mercury, carbon monoxide, organophosphate insecticides, industrial solvents) Dr.Al-Azzam 24
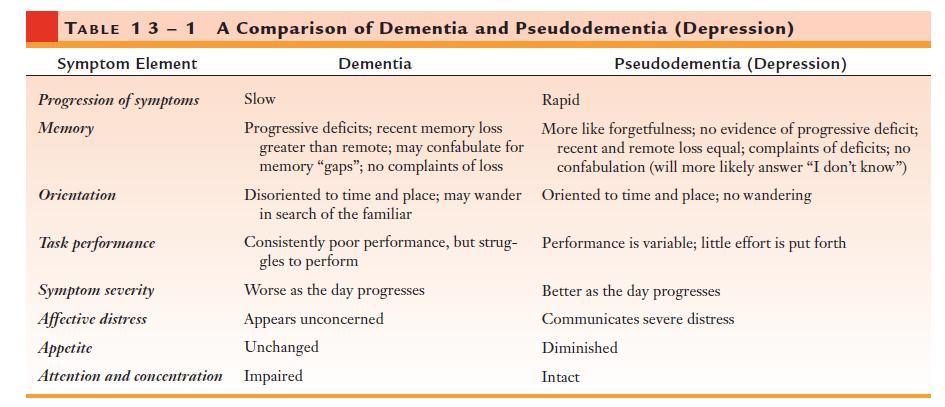
25 Assessment Client history: type, frequency, and severity of mood swings, personality and behavioral changes, and catastrophic emotional reactions Cognitive changes, such as problems with attention span, thinking process, problem-solving, and memory (recent and remote language difficulties orientation to person, place, time, and situation Appropriateness of social behavior. Dr.Al-Azzam 25
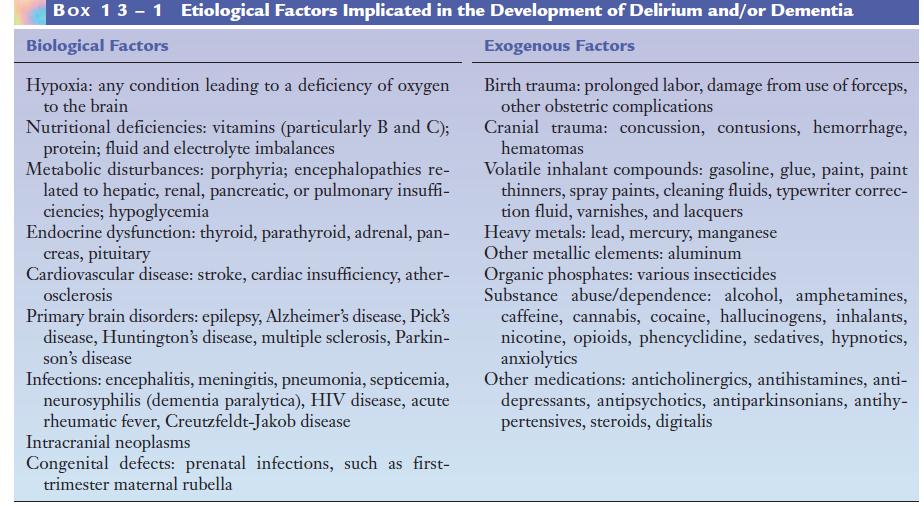
26 Physical Assessment signs of damage to the nervous system and evidence of diseases of other organs that could affect mental function Mental status examination Box Dr.Al-Azzam 26
27 Dr.Al-Azzam 27
28 Diagnostic Laboratory Evaluations Blood and Urine tests CT EEG MRI PET (positron emission tests) Dr.Al-Azzam 28
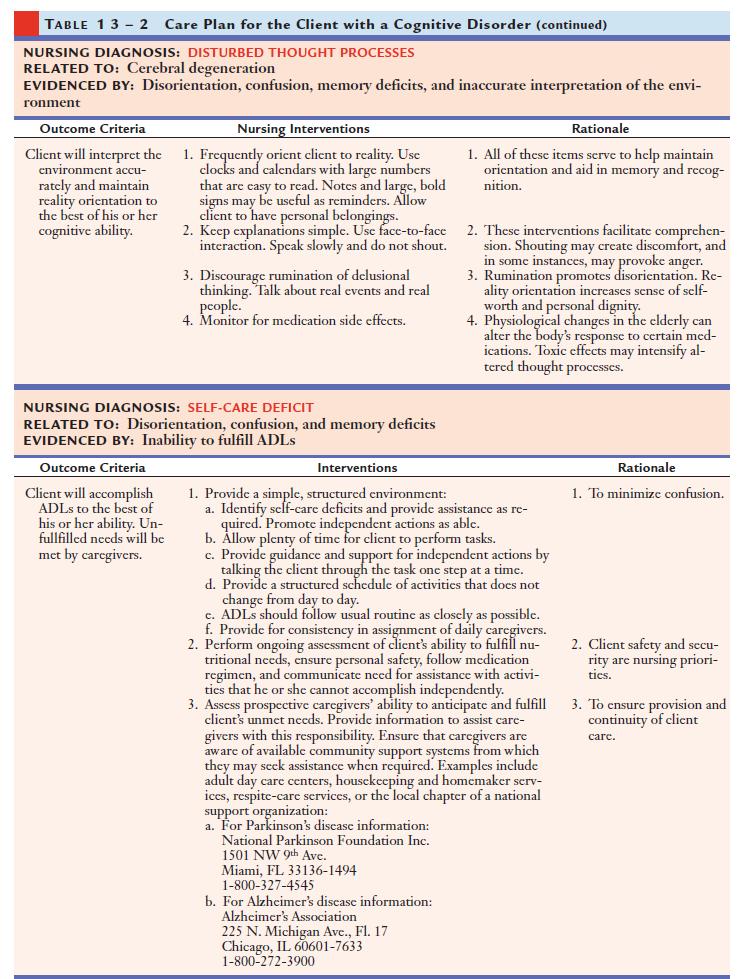
29 Nursing Diagnosis Risk for trauma related to impairments in cognitive and psychomotor functioning Risk for suicide related to depressed mood secondary to awareness in decline of mental and/or physical capability Risk for other-directed violence related to impairment of impulse control; hallucinations Disturbed thought processes related to cerebral degeneration evidenced by disorientation, confusion memory deficits, and inaccurate interpretation of the environment Low self-esteem related to loss of independent functioning evidenced by expressions of shame and self degradation and progressive social isolation Self-care deficit related to disorientation, confusion, memory deficits evidenced by inability to fulfill Dr.Al-Azzam ADLs 29
30 Outcomes Has not experienced physical injury. Has not harmed self or others. Has maintained reality orientation to the best of his or her capability. Discusses positive aspects about self and life. Fulfills activities of daily living with assistance. Dr.Al-Azzam 30
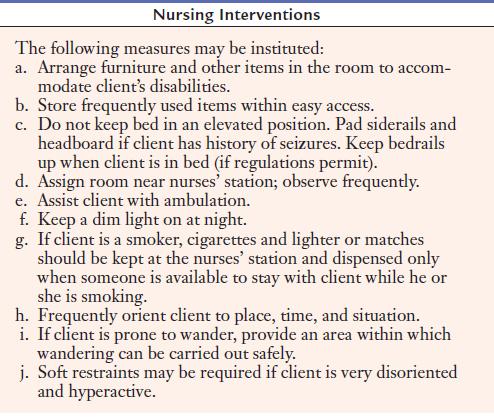
31 Planning/Implementation Dr.Al-Azzam 31
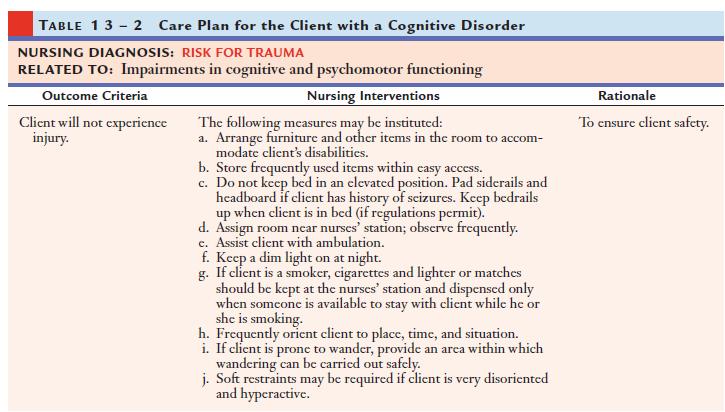
32 Dr.Al-Azzam 32
33 Dr.Al-Azzam 33

34 Client/Family Education Dr.Al-Azzam 34
35 Treatment Modalities Delirium: Correction underlying cause attention must be given to fluid and electrolyte status, hypoxia, anoxia, and diabetic problems. Staff members should remain with the client at all times to monitor behavior and provide reorientation and assurance. The room should maintain a low level of stimuli. Some physicians prefer not to prescribe medications for the delirious client, reasoning that additional agents may only compound the syndrome of brain dysfunction. Dementia: Focus must be directed to the identification and resolution of potentially reversible processes. The need for general supportive care, with provisions for security, stimulation, patience, and nutrition, Dr.Al-Azzam has been recognized and accepted 35
36 Pharmaceutical Agents For agitation, aggression, hallucinations, thought disturbances, and wandering Risperidone (Risperdal) Olanzapine (Zyprexa) Quetiapine (Seroquel) Ziprasidone (Geodon) Haloperidol (Haldol) For depression Fluoxetine (Prozac) Sertraline (Zoloft) Citalopram (Celexa) Paroxetine (Paxil) Dr.Al-Azzam 36
37 For anxiety (should not be used routinely for prolonged periods) Chlordiazepoxide (Librium) Alprazolam (Xanax) Lorazepam (Ativan) Oxazepam (Serax) Diazepam (Valium) For sleep disturbances (for short-term therapy only) Flurazepam (Dalmane) Temazepam (Restoril) Triazolam (Halcion) Zolpidem (Ambien) Aleplon (Sonata) Trazodone (Desyrel) Dr.Al-Azzam 37
Dementia. Assessing Brain Damage. Mental Status Examination
 Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Dementia Assessing Brain Damage Mental status examination Information about current behavior and thought including orientation to reality, memory, and ability to follow instructions Neuropsychological
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Using Benzodiazepines in Primary Care
 Using Benzodiazepines in Primary Care Spencer A. Tighe MD, FRCPC Saturday, Feb. 16, 2008 Overview Historical context Drug information Indications Side effects Abuse vs. physical dependence Clinical practice
Using Benzodiazepines in Primary Care Spencer A. Tighe MD, FRCPC Saturday, Feb. 16, 2008 Overview Historical context Drug information Indications Side effects Abuse vs. physical dependence Clinical practice
Understanding Alzheimer s Disease
 Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Understanding Alzheimer s Disease Alzheimer s disease is an irreversible, progressive brain disorder that slowly impacts memory, thinking, skills and, eventually, the ability to carry out the simplest
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State
 The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State RAI/MDS Coordinator Objectives Upon completion of this training,
The Basics of Psychoactive/Psychotropic Medications Tina Sanchez, RN, SMQT New Mexico Department of Health Division of Health Improvement State RAI/MDS Coordinator Objectives Upon completion of this training,
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Richard Heidenfelder M.D. Child, Adolescent and Adult Psychiatry 447 9th Ave San Diego, CA
 *We are not accepting any New Patients who are currently taking any controlled pain medications *We are *Note: not completion accepting of the any following New Patients paperwork who and Initial are Screening
*We are not accepting any New Patients who are currently taking any controlled pain medications *We are *Note: not completion accepting of the any following New Patients paperwork who and Initial are Screening
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
PSYCHIATRY INTAKE FORM
 Please complete all information on this form. PSYCHIATRY INTAKE FORM Name Date Date of Birth Primary Care Physician Current Therapist/Counselor What are the problem(s) for which you are seeking help? 1.
Please complete all information on this form. PSYCHIATRY INTAKE FORM Name Date Date of Birth Primary Care Physician Current Therapist/Counselor What are the problem(s) for which you are seeking help? 1.
Clinical Diagnosis. Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV)
") Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Step 1: Dementia or not? Diagnostic criteria for dementia (DSM-IV) A. The development of multiple cognitive deficits manifested by both 1 and 2 1 1. Memory impairment 2. One (or more) of the following
Psychiatric Illness. In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis
 Psychiatric Illness In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis 12,000,000 children infants through 18 y/o nation wide 5,000,000 suffer severely Serious
Psychiatric Illness In the medical arena psychiatry is a fairly recent field A challenging field Numerous diagnosis 12,000,000 children infants through 18 y/o nation wide 5,000,000 suffer severely Serious
Antidepressants and Sedatives. David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School
 Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Antidepressants and Sedatives David G. Standaert, M.D., Ph.D. Massachusetts General Hospital Harvard Medical School Depression A frequent problem, affecting up to 5% of the population Common presentations
Review of Psychotrophic Medications. (An approved North Carolina Division of Health Services Regulation Continuing Education Course)
") Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
7/3/2013 ABNORMAL PSYCHOLOGY SEVENTH EDITION CHAPTER FOURTEEN CHAPTER OUTLINE. Dementia, Delirium, and Amnestic Disorders. Oltmanns and Emery
 ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
ABNORMAL PSYCHOLOGY SEVENTH EDITION Oltmanns and Emery PowerPoint Presentations Prepared by: Ashlea R. Smith, Ph.D. This multimedia and its contents are protected under copyright law. The following are
Treat mood, cognition, and behavioral disturbances associated with psychological disorders. Most are not used recreationally or abused
 Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Old Age and Stress. Disorders of Aging and Cognition. Disorders of Aging and Cognition. Chapter 18
 Disorders of Aging and Cognition Chapter 18 Slides & Handouts by Karen Clay Rhines, Ph.D. Northampton Community College Comer, Abnormal Psychology, 8e Disorders of Aging and Cognition Dementia deterioration
Disorders of Aging and Cognition Chapter 18 Slides & Handouts by Karen Clay Rhines, Ph.D. Northampton Community College Comer, Abnormal Psychology, 8e Disorders of Aging and Cognition Dementia deterioration
Mental Health Nursing: Organic Disorders. By Mary B. Knutson, RN, MS, FCP
 Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
Mental Health Nursing: Organic Disorders By Mary B. Knutson, RN, MS, FCP A Definition of Cognition Mental process characterized by knowing, thinking, learning, and judging Cognitive disorders include delirium
PSYCHIATRIC DRUGS. Mr. D.Raju, M.pharm, Lecturer
 PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*
 DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*") COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
11/1/2010. Psychology 472 Pharmacology of Psychoactive Drugs. Listen to the audio lecture while viewing these slides
 Treatment for Anxiety Disorders Benzodiazepines and Other Anxiolytics Psychology 472 Pharmacology of Psychoactive Drugs Listen to the audio lecture while viewing these slides Ethanol Barbiturates and related
Treatment for Anxiety Disorders Benzodiazepines and Other Anxiolytics Psychology 472 Pharmacology of Psychoactive Drugs Listen to the audio lecture while viewing these slides Ethanol Barbiturates and related
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation. Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project
 Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
Benzodiazepines: Comparative Effectiveness and Strategies for Discontinuation Ann M. Hamer, PharmD, BCPP Rural Oregon Academic Detailing Project This project is funded through a grant from the Pew Charitable
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Dementia. Aetiology, pathophysiology and the role of neuropsychological testing. Dr Sheng Ling Low Geriatrician
 Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Dementia Aetiology, pathophysiology and the role of neuropsychological testing Dr Sheng Ling Low Geriatrician Topics to cover Why is dementia important What is dementia Differentiate between dementia,
Psychobiology Handout
 Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Nsg 85A / Psychiatric Page 1 of 7 Psychobiology Handout STRUCTURE AND FUNCTION OF THE BRAIN Psychiatric illness and the treatment of psychiatric illness alter brain functioning. Some examples of this are
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Psychotropic Strategies Handout Package
 Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
Psychotropic Strategies Handout Package Psychotropic Strategies Learning Objectives Utilize all clinical information available Assess the patient s overall condition this is essential Basic Principles
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias
 What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
What APS Workers Need to Know about Frontotemporal, Lewy Body and Vascular Dementias Presenter: Kim Bailey, MS Gerontology, Program & Education Specialist, Alzheimer s Orange County 1 1 Facts About Our
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Appendix: Psychotropic Medication Reference Tables
 Appendix: Psychotropic Medication Reference Tables How to Use these Tables These reference tables are designed to provide clinic staff with specific medication related criteria for the Polypharmacy, Cardiometabolic
Appendix: Psychotropic Medication Reference Tables How to Use these Tables These reference tables are designed to provide clinic staff with specific medication related criteria for the Polypharmacy, Cardiometabolic
WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient
 DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
DEMENTIA WHAT IS DEMENTIA? An acquired syndrome of decline in memory and other cognitive functions sufficient to affect daily life in an alert patient Progressive and disabling Not an inherent aspect of
Mental Health Intake Form
 38600 Van Dyke Ave., Suite 200 Sterling Heights, MI 48313 Phone: (586) 933-5395 Fax: (586) 935-0159 Mental Health Intake Form Please complete all information on this form and bring it to the first visit.
38600 Van Dyke Ave., Suite 200 Sterling Heights, MI 48313 Phone: (586) 933-5395 Fax: (586) 935-0159 Mental Health Intake Form Please complete all information on this form and bring it to the first visit.
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Palliative Approach to the Person with Advanced Dementia
 Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
Mid North Coast Rural Palliative Care Project Link Nurse Education 2004 Palliative Approach to the Person with Advanced Dementia Anne Sneesby CNC - ACAT To care for the dying is a very human opportunity
The Person: Dementia Basics
 The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
The Person: Dementia Basics Objectives 1. Discuss how expected age related changes in the brain might affect an individual's cognition and functioning 2. Discuss how changes in the brain due to Alzheimer
Test Bank for Essentials of Psychiatric Mental Health Nursing 1st Edition by Varcarolis
 Test Bank for Essentials of Psychiatric Mental Health Nursing 1st Edition by Varcarolis Link download full: https://testbankservice.com/download/test-bankforessentials-of-psychiatric-mental-health-nursing-1st-editionbyvarcarolis/
Test Bank for Essentials of Psychiatric Mental Health Nursing 1st Edition by Varcarolis Link download full: https://testbankservice.com/download/test-bankforessentials-of-psychiatric-mental-health-nursing-1st-editionbyvarcarolis/
Psychotropic Medication Use in Dementia
 Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Psychotropic Medication Use in Dementia Marie A DeWitt, MD Diplomate of the American Board of Psychiatry and Neurology, Specialization in Psychiatry & Subspecialization in Geriatric Psychiatry Staff Physician,
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event
 Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
Cumbria Partnership NHS Foundation Trust Memory Matters Service Dementia, Depression and Delerium Cancer Awareness Toolkit Evaluation Event Andrew Milburn Occupational Therapy Clinical Lead, Dementia Pathways
What s Causing Your Memory Loss?
 What s Causing Your Memory Loss? It s Not Necessarily Alzheimer s More than 50 conditions can cause or mimic the symptoms of dementia, and a small percentage of dementias are reversible. Two common examples
What s Causing Your Memory Loss? It s Not Necessarily Alzheimer s More than 50 conditions can cause or mimic the symptoms of dementia, and a small percentage of dementias are reversible. Two common examples
Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA
 Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA Goals of Medications Use least number at lowest dose to get
Psychotropic Medications Archana Jhawar, PharmD, BCPP Clinical Faculty of UIC Pharmacy Practice Clinical Psychiatric Pharmacist Jesse Brown VA Goals of Medications Use least number at lowest dose to get
Mental Health Intake Form
 Current Symptoms Checklist: (check once for any symptoms present, twice for major symptoms) ( ) ( ) Depressed mood ( ) ( ) Racing thoughts ( ) ( ) Excessive worry ( ) ( ) Unable to enjoy activities ( )
Current Symptoms Checklist: (check once for any symptoms present, twice for major symptoms) ( ) ( ) Depressed mood ( ) ( ) Racing thoughts ( ) ( ) Excessive worry ( ) ( ) Unable to enjoy activities ( )
SEDATIVE-HYPNOTIC AGENTS
 SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
SEDATIVE-HYPNOTIC AGENTS Documentation A. FDA approved indications 1. Insomnia 2. Sedation for an agitated patient in an inpatient setting Documentation B. Non-FDA approved, commonly used indications 1.
Alzheimer s disease dementia: a neuropsychological approach
 Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
Alzheimer s disease dementia: a neuropsychological approach Dr. Roberta Biundo, PhD Neuropsychology Coordinator at Parkinson s disease and movement disorders unit of San Camillo rehabilitation hospital
IMPORTANT NOTICE. Changes to dispensing of some Behavioral Health Medications for DC Healthcare Alliance members
 IMPORTANT NOTICE Changes to dispensing of some Behavioral Health Medications for DC Healthcare Alliance members These changes apply only to members covered under the DC Healthcare Alliance program Alliance
IMPORTANT NOTICE Changes to dispensing of some Behavioral Health Medications for DC Healthcare Alliance members These changes apply only to members covered under the DC Healthcare Alliance program Alliance
MO Medicaid Foster Care Drugs FY10-FY14
 MO Medicaid Foster Care Drugs FY10-FY14 Medicaid (MO HealthNet) Cost of Drugs given to Missouri Foster Care Children by combinations of Age, Gender, Drug Class and Fiscal Year [Raw Data Provided by Missouri
MO Medicaid Foster Care Drugs FY10-FY14 Medicaid (MO HealthNet) Cost of Drugs given to Missouri Foster Care Children by combinations of Age, Gender, Drug Class and Fiscal Year [Raw Data Provided by Missouri
New life Collage of nursing Karachi
 New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
New life Collage of nursing Karachi Presenter: Zafar ali shah Faculty: Raja khatri Subject: Pathophysiology Topic :Alzheimer s Disease Post RN BScN semester 2 nd Objective Define Alzheimer s Describe pathophysiology
Use of Psychotropic Medications in Older Adults with Dementia!
 Use of Psychotropic Medications in Older Adults with Dementia! Deepa Pattani, PharmD, RPh Owner: PrevInteract Health Deepa.Pattani@PrevInteract.com 972-372-9775 About Me Deepa Pattani, PharmD, RPh with
Use of Psychotropic Medications in Older Adults with Dementia! Deepa Pattani, PharmD, RPh Owner: PrevInteract Health Deepa.Pattani@PrevInteract.com 972-372-9775 About Me Deepa Pattani, PharmD, RPh with
Dementia. Understanding 9/20/2010. Jan Robson Coordinator of the Alzheimer Society's Dementia Helpline
 Understanding Dementia Jan Robson Coordinator of the Alzheimer Society's Dementia Helpline Marc Labrecque Provincial Coordinator of Programs and Services 1 Understanding Dementia What is dementia Alzheimer
Understanding Dementia Jan Robson Coordinator of the Alzheimer Society's Dementia Helpline Marc Labrecque Provincial Coordinator of Programs and Services 1 Understanding Dementia What is dementia Alzheimer
Diagnosis and Treatment of Alzhiemer s Disease
 Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Diagnosis and Treatment of Alzhiemer s Disease Roy Yaari, MD, MAS Director, Memory Disorders Clinic, Banner Alzheimer s Institute 602-839-6900 Outline Introduction Alzheimer s disease (AD)Guidelines -revised
Happy Daisy Ltd. New Client intake Form. What are the issues for which you are seeking care?
 Happy Daisy Ltd. New Client intake Form Name Date Preferred name Pronouns Referred by Date of birth Age Race What are the issues for which you are seeking care? 1. 2. 3. Please check of any of the symptoms
Happy Daisy Ltd. New Client intake Form Name Date Preferred name Pronouns Referred by Date of birth Age Race What are the issues for which you are seeking care? 1. 2. 3. Please check of any of the symptoms
DEMENTIA? 45 Million. What is. WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: 70% Dementia is not a disease
 What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
What is PRESENTS DEMENTIA? WHAT IS DEMENTIA Dementia is a disturbance in a group of mental processes including: Memory Reasoning Planning Learning Attention Language Perception Behavior AS OF 2013 There
New Patient Questionnaire
 4 Embarcadero Center, Suite 1400, San Francisco, CA 94111 (415) 926-7774 phone; (415) 591-7760 office@sanfranciscopsych.com New Patient Questionnaire Thank you for trusting San Francisco Psychiatry with
4 Embarcadero Center, Suite 1400, San Francisco, CA 94111 (415) 926-7774 phone; (415) 591-7760 office@sanfranciscopsych.com New Patient Questionnaire Thank you for trusting San Francisco Psychiatry with
Management of Behavioral Problems in Dementia
 Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Management of Behavioral Problems in Dementia Ghulam M. Surti, MD Clinical Assistant Professor Department of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Definition of
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Mental Health Disorders Civil Commitment UNC School of Government
 Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
Mental Health Disorders 2017 Civil Commitment UNC School of Government Edward Poa, MD, FAPA Chief of Inpatient Services, The Menninger Clinic Associate Professor, Baylor College of Medicine NC statutes
GENI Jeopardy: Geriatric Mental Health. Part of the brain responsible for executive functioning
 GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
GENI Jeopardy: Geriatric Mental Health Part of the brain responsible for executive functioning Dementia: It is not just forgetfulness GENI February 20, 2008 Marcia Carr - CNS Dementia Dementia means brain
ALZHEIMER S DISEASE. Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey
 ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
ALZHEIMER S DISEASE Mary-Letitia Timiras M.D. Overlook Hospital Summit, New Jersey Topics Covered Demography Clinical manifestations Pathophysiology Diagnosis Treatment Future trends Prevalence and Impact
Is it Alzheimer s or Another Dementia? Reversible dementias. Key Points. Delirium. Toxic reactions to drugs
 Is it Alzheimer s or Another Dementia? Bonus Article for HELPGUIDE.ORG from Harvard Health Publications For physicians and families intent on pinning down a diagnosis, one major complicating factor is
Is it Alzheimer s or Another Dementia? Bonus Article for HELPGUIDE.ORG from Harvard Health Publications For physicians and families intent on pinning down a diagnosis, one major complicating factor is
Have You Ever Wondered
 Have You Ever Wondered A few facts about medication use and related falls The Number of Medications You Take & The Connection to Falls CONCERN: As you increase the number of medications that you take,
Have You Ever Wondered A few facts about medication use and related falls The Number of Medications You Take & The Connection to Falls CONCERN: As you increase the number of medications that you take,
Organic mental disorders
 Organic mental disorders F00-F09 Organic, including symptomatic, mental disorders This block comprises a range of mental disorders grouped together on the basis of their having in common a demonstrable
Organic mental disorders F00-F09 Organic, including symptomatic, mental disorders This block comprises a range of mental disorders grouped together on the basis of their having in common a demonstrable
Mental Illness. Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling
 Mental Illness Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling Moodiness Changing Bodies Narcissism Self-Esteem Ignorant Naïve Insecure Self-Centered Independent Adolescence Disorders Affecting
Mental Illness Doreen L. Rasp, APN, FNP, PMHNP Advanced Behavioral Counseling Moodiness Changing Bodies Narcissism Self-Esteem Ignorant Naïve Insecure Self-Centered Independent Adolescence Disorders Affecting
AACN PCCN Review. Behavioral
 AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
Medications and Children Disorders
 Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
Mental Health Comprehensive Services Providing Family Stability and Developing Life Coping Skills Medications and Children Disorders Psychiatric medications can be an effective part of the treatment for
Differentiating Dementia Diagnoses
 Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
Differentiating Dementia Diagnoses Waitemata PHO 21 October 2014 Dr Michal Boyd, RN, NP, ND Nurse Practitioner Older Adults School of Nursing & Freemasons Dept. of Geriatric Medicine The University of
4/2/13 COMMON CLASSES OF MEDICATIONS. Child & Adolescent Behavioral Medicine & Medication Therapies. Behavioral Medicine & Medication Therapies
 Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders. William L. Bograkos, MA, DO, FACOEP
 Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders Toxic Brain Disorders William L. Bograkos, MA, DO, FACOEP TBI: Traumatic Brain Injury / Toxic Brain Injury (Trauma and Substance
Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders Toxic Brain Disorders William L. Bograkos, MA, DO, FACOEP TBI: Traumatic Brain Injury / Toxic Brain Injury (Trauma and Substance
You May Be at Risk. You are taking one of the following sedative-hypnotic medications: Diazepam (Valium ) Estazolam. Flurazepam.
 Estazolam. Flurazepam.") You May Be at Risk You are taking one of the following sedative-hypnotic medications: Alprazolam (Xanax ) Diazepam (Valium ) Temazepam (Restoril ) Chlorazepate Estazolam Triazolam (Halcion ) Chlordiazepoxide
You May Be at Risk You are taking one of the following sedative-hypnotic medications: Alprazolam (Xanax ) Diazepam (Valium ) Temazepam (Restoril ) Chlorazepate Estazolam Triazolam (Halcion ) Chlordiazepoxide
Psychiatric Distress in Chronic & Terminal Illness Barb Henry, ARNP, MSN
 Psychiatric Distress in Chronic & Terminal Illness Barb Henry, ARNP, MSN Psycho-Oncology Consultants, LLC & The University of Cincinnati Central Clinic University of Cincinnati Central Clinic www.centralclinic.org
Psychiatric Distress in Chronic & Terminal Illness Barb Henry, ARNP, MSN Psycho-Oncology Consultants, LLC & The University of Cincinnati Central Clinic University of Cincinnati Central Clinic www.centralclinic.org
RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING
 RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING Alex Hishaw, MD Department of Neurology University of Arizona Objectives: Recognize the impact of history and presentation on the diagnosis
RECOGNITION AND MANAGEMENT OF DEMENTIA IN THE ACUTE CARE SETTING Alex Hishaw, MD Department of Neurology University of Arizona Objectives: Recognize the impact of history and presentation on the diagnosis
The ABCs of Dementia Diagnosis
 The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
The ABCs of Dementia Diagnosis Dr. Robin Heinrichs, Ph.D., ABPP Board Certified Clinical Neuropsychologist Associate Professor, Psychiatry & Behavioral Sciences Director of Neuropsychology Training What
Benzodiazepines. Benzodiazepines
 : History 1950s - Invented by Swiss chemists who identified its sedative effects 1950s 60s - Chlordiazepoxide (Librium) marketed as a safer alternative to barbiturates; along with newer benzodiazepines
: History 1950s - Invented by Swiss chemists who identified its sedative effects 1950s 60s - Chlordiazepoxide (Librium) marketed as a safer alternative to barbiturates; along with newer benzodiazepines
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Clonazepam temazepam clonazepam temazepam compared temazepam clonazepam klonopin temazepam Clonazepam vs Temazepam Clonazepam Temazepam Temazepam
 Compare Clonazepam vs. Temazepam, which is better for uses like: Anxiety and Insomnia. Compare head-to-head ratings, side effects, warnings, dosages, interactions and patient reviews. Patients rated Clonazepam
Compare Clonazepam vs. Temazepam, which is better for uses like: Anxiety and Insomnia. Compare head-to-head ratings, side effects, warnings, dosages, interactions and patient reviews. Patients rated Clonazepam
Geriatric Alterations Associated with Neurological Conditions
 Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
Geriatric Alterations Associated with Neurological Conditions I have no conflicts of interest. Julie Bronson The Older Adult According to the World Health Organization Africa 50-55 or 50-65 United Nations
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Insomnia: Updates in Medical Management. Michael Newnam M.D.
 Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Insomnia: Updates in Medical Management Michael Newnam M.D. Sleep Neurobiology Delicate balance of excitatory and inhibitory neurotransmitters that control the switch between wakefulness and sleep Circadian
Safe and Effective Medication Approaches for Anxiety and Insomnia
 Safe and Effective Medication Approaches for Anxiety and Insomnia Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free monthly
Safe and Effective Medication Approaches for Anxiety and Insomnia Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free monthly
DSM-5 MAJOR AND MILD NEUROCOGNITIVE DISORDERS (PAGE 602)
") SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
SUPPLEMENT 2 RELEVANT EXTRACTS FROM DSM-5 The following summarizes the neurocognitive disorders in DSM-5. For the complete DSM-5 see Diagnostic and Statistical Manualof Mental Disorders, 5th edn. 2013,
Delirium Assessment. February 24, Susan Schumacher, MS, APRN-BC
 Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
Delirium Assessment February 24, 2016 Susan Schumacher, MS, APRN-BC Objectives Define delirium Differentiate delirium from dementia Identify predisposing and precipitating factors leading to delirium.
John E. Kraus, M.D., Ph.D.
 John E. Kraus, M.D., Ph.D. Chief, Adult Psychiatry, Dorothea Dix Hospital, Raleigh, NC Assistant Professor/Associate Director of Residency Training, Dept. of Psychiatry, UNC Hospitals, Chapel Hill, NC
John E. Kraus, M.D., Ph.D. Chief, Adult Psychiatry, Dorothea Dix Hospital, Raleigh, NC Assistant Professor/Associate Director of Residency Training, Dept. of Psychiatry, UNC Hospitals, Chapel Hill, NC
Medications and Non-Pharma Approaches to Treatment. David J. Irwin, MD Penn Frontotemporal Degeneration Center
 Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
Medications and Non-Pharma Approaches to Treatment David J. Irwin, MD Penn Frontotemporal Degeneration Center Outline Non-Pharmacological Treatment Strategies Behavior Language Motor Supportive Care Check-points
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
BEHAVIORAL PROBLEMS IN DEMENTIA
 BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
BEHAVIORAL PROBLEMS IN DEMENTIA CLINICAL FEATURES Particularly as dementia progresses, psychiatric symptoms may develop that resemble discrete mental disorders such as depression or mania The course and
Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials
 SPEAKER NOTES Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials Summarized by Thomas T. Thomas New psychotropic medications are coming on the
SPEAKER NOTES Overview and Update on Current Psychopharmacological Medications, Including New Medications in Clinical Trials Summarized by Thomas T. Thomas New psychotropic medications are coming on the
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines
 Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines Program Learning Objectives At the conclusion of the activity, participants should be able to: Have a basic understanding
Friend or Foe? Review of the Regulations & Benefits: Risk Profiles of the Benzodiazepines Program Learning Objectives At the conclusion of the activity, participants should be able to: Have a basic understanding
Dementia. Stephen S. Flitman, MD Medical Director 21st Century Neurology
 Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Dementia Stephen S. Flitman, MD Medical Director 21st Century Neurology www.neurozone.org Dementia is a syndrome Progressive memory loss, plus Progressive loss of one or more cognitive functions: Language
Study Guidelines for Quiz #1
 Annex to Section J Page 1 Study Guidelines for Quiz #1 Theory and Principles of Psychopharmacology, Classifications and Neurotransmitters, Anxiolytics/Antianxiety/Minor Tranquilizers, Stimulants, Nursing
Annex to Section J Page 1 Study Guidelines for Quiz #1 Theory and Principles of Psychopharmacology, Classifications and Neurotransmitters, Anxiolytics/Antianxiety/Minor Tranquilizers, Stimulants, Nursing
Westminster Memory Services Pathways Toolkit (updated October 2016)
") Westminster Memory Services Pathways Toolkit (updated October 2016) Contents Aims... 2 Memory loss experienced by service users... 2 Signs of memory loss... 2 Alcohol dependency and memory loss... 3 Other
Westminster Memory Services Pathways Toolkit (updated October 2016) Contents Aims... 2 Memory loss experienced by service users... 2 Signs of memory loss... 2 Alcohol dependency and memory loss... 3 Other
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
2/12/2016. Drugs and Dementia in the Hospice Patient. Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources
 Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Drugs and Dementia in the Hospice Patient Jim Joyner, Pharm.D., C.G.P. Director of Clinical Operations Outcome Resources 1 Drug Therapy: Targeted at Symptoms Cognitive: Impaired abstract thinking Impaired
Resources: Types of dementia
 1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.
1/5 Dementia is an umbrella term for a number of progressive conditions affecting the functioning of the brain. Different types of dementia have different causes. There are a great number of rare forms.