Opiate Use among Ohio Medicaid Recipients
|
|
|
- Erik Barker
- 6 years ago
- Views:
Transcription
1 Opiate Use among Ohio Medicaid Recipients July 12, 2012 Ohio Colleges of Medicine Government Resource Center The Ohio State University College of Public Health Sponsored by The Ohio Department of Alcohol and Drug Addiction Services In Partnership with Ohio Medicaid
2 FOCUS I. Prevalence II. III. IV. High Risk Patterns of Use Patterns of Use Related to Poor Patient Outcomes Costs Related to High Risk Patterns and Negative Outcomes
3 METHODOLOGY Inclusion Criteria Medicaid Claims 2001 through 2010, including beneficiaries not receiving services FFS and MCP monthly eligibility and demographics Age range 12 years and over Non dual eligible Excluding individuals with terminal malignancy and death within one year

4 MORPHINE EQUIVALENT DOSE (MED) Equianalgesic Dose 120 mg Morphine 6 mg Buprenorphine 800 mg Codeine 120 mg Hydrocodone 30 mg Hydromorphone 40 mg Methadone 80 mg Oxycodone 833 mg Tramadol 800 mg Adetaminophen with Codine 50 mg Fentanyl 1200 mg Meperidine 120 mg Nalbuphine 40 mg Oxymorphone Schedule II and III opiates, plus Tramadol No Daily Dose data for MCPs. Estimated Daily Dose = Total mgs days between scripts (median estimates within 4 mgs) Equianalgesic conversion factors consistent with Washington State


5 PREVALENCE OF OPIATE USE Opiate use increased steadily over the past 10 years From 1 in 5 beneficiaries in 2001 to 1 in 3 beneficiaries in % 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% Proportion of all eligible Medicaid beneficiaries with an Opiate Claim
6 PREVALENCE BY AGE 60% 50% Rate of use tops 50% among beneficiaries ages 45 to 64 40% 30% 20% 10% 0% Total 12 to to to to 64 Proportion of all eligible Medicaid beneficiaries with an Opiate Claim
7 PREVALENCE BY GENDER Rate of opiate use is higher among women 51% of women between ages 45 and 64 received opiates in % 40% 35% 30% 25% 20% 15% 10% 5% 0% Total Male Female Proportion of all eligible Medicaid beneficiaries with an Opiate Claim
8 Higher rate of use among whites compared to other racial and ethnic groups 40% 35% 30% 25% 20% 15% 10% 5% 0% PREVALENCE BY RACE & ETHNICITY Total White Black Hispanic Other Proportion of all eligible Medicaid beneficiaries with an Opiate Claim
9 PREVALENCE BY ELIGIBILITY Opiate use is more prevalent among individuals with ABD Medicaid eligibility status 50% 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% Total CFC ABD Waiver Proportion of all eligible Medicaid beneficiaries with an Opiate Claim
10 Among individuals with selected pain diagnoses, the rate of opiate use is higher than that among other eligible beneficiaries Note that the specific reason for opiate use among these groups is unknown PREVALENCE AMONG INDIVIDUALS WITH SELECTED PAIN CONDITIONS 70% 60% 50% 40% 30% 20% 10% 0% Total Back Abdominal Ortho Ocular Migraine Proportion of all eligible Medicaid beneficiaries with a pain condition diagnosis and an opiate claim in the same year
11 Opiate claims following diagnosis of a new pain condition are on the rise, suggesting opiates are increasingly common treatment for pain Opiates are a common treatment for approx. 35% of abdominal, back, and migraine conditions OPIATE USE FOLLOWING DIAGNOSIS OF A PAIN CONDITION 40% 35% 30% 25% 20% 15% 10% 5% 0% Back Abdominal Ocular Migraine Ortho Opiate claim within 7 days of the beginning of a diagnostic episode (preceded by a clean period)
12 OPIATE USE FOLLOWING DIAGNOSIS OF A NEW PAIN CONDITION Opiate claims following diagnosis of a new pain condition are on the rise, suggesting opiates are increasingly common first-line treatment for pain Prescription of opiates at the first diagnosis of a new pain condition increased from < 10% to over 20%. 40% 35% 30% 25% 20% 15% 10% 5% 0% Back Migraine Ortho Abdominal Opiate claim within 4 days of the beginning of a diagnostic episode (preceded by a 90-day clean period)
 120mg MED.")

13 MORPHINE EQUIVALENT DAILY DOSE Evidence that -50 to 99 MED increases risk of overdose by 370%; MED increases risk of overdose by 890% (Dunn, K.M. et al., 2010, Annals of Internal Medicine) 120mg MED. Washington State Yellow Flag warning for providers 60% 50% 40% 30% 20% 10% 0% 29.3% 51.8% 10.3% 5.2% YEAR 2010 MEDIAN = 30 MG MEAN = 40.1 MG SD = 54.6 MG 0.7% 0.3% 0.3% 0.4% 0.2% 0.3% 0.3% 0.1% Daily MED in mgs Table values represent percent of opiate claims
14 PREVALENCE OF HIGH OPIATE USE High opiate use is rare, but on the rise. PROPORTION OF SCRIPTS* 48% HYDROCO 23% OCYCODO 15% TRAMADO 11% CODEINE <1% MORPHINE <1% METHADO <1% BUPRENO <1% HYDROMO <1% MEPERID <1% OXYMORP <1% NALBUPH 10.0% 9.0% 8.0% 7.0% 6.0% 5.0% 4.0% 3.0% 2.0% 1.0% 0.0% mg 50+ mg 80+ mg 100+ mg 120+ mg 111,319 people 55,602 people 22,308 people *LEVEL II & III OPIATES AND TRAMADOL Proportion of all eligible Medicaid beneficiaries in each use category
15 Chronic high use is also rare, yet increased since % 2.5% CHRONIC HIGH USE 120 MG, 90 DAYS 20,518 people 17% of opiate use episodes are greater than 90 days duration Evidence of increased risk of dependence, withdrawal, and hyperalgesia after 90 days of opiate use (Ballantyne J., 2007, Pain Physician) 2.0% 1.5% 1.0% 0.5% 0.0% Proportion of beneficiaries with opiate use episode 90 days with a daily dose reaching 120 MED
16 HIGH RISK DRUG COMBINATIONS Opiate drug combinations known to increase risk of overdose death are rare, but on the rise. 10,000 8,000 6,000 4,000 The most frequent combinations include - opiates with benzodiazapines - opiates with muscle relaxers 2,000 0 Benzo Muscle Relax Sedatives Co-Occur Stimulants Suboxone Sedatives Number of beneficiaries with at least two co-occurring claims for a benzo, muscle relaxer, sedative, stimulant, or suboxone during the same opiate use episode
17 BENEFICIARIES WITH MULTIPLE PRESCRIBERS The number of beneficiaries with opiate claims from multiple prescribers is on the rise. Evidence that 16% to 21% of opiate overdose deaths occur among individuals with 5 prescribers in a year (Hall AJ, et al. 2008, JAMA; ODH, org/diseaseprevention/dpoison/ drugdata.aspx.) 45,000 40,000 35,000 30,000 25,000 20,000 15,000 10,000 5, % of. beneficiaries 2.9% of beneficiaries Total number of beneficiaries with opiate claims from 5 or more prescribers within the same year (with MCP rates estimated)
18 BENEFICIARIES WITH MULTIPLE PHARMACIES The number of beneficiaries with opiate claims from multiple pharmacies is on the rise % of. beneficiaries.4% of beneficiaries Total number of beneficiaries with opiate claims from 5 or more pharmacies within the same year (with MCP rates estimated)
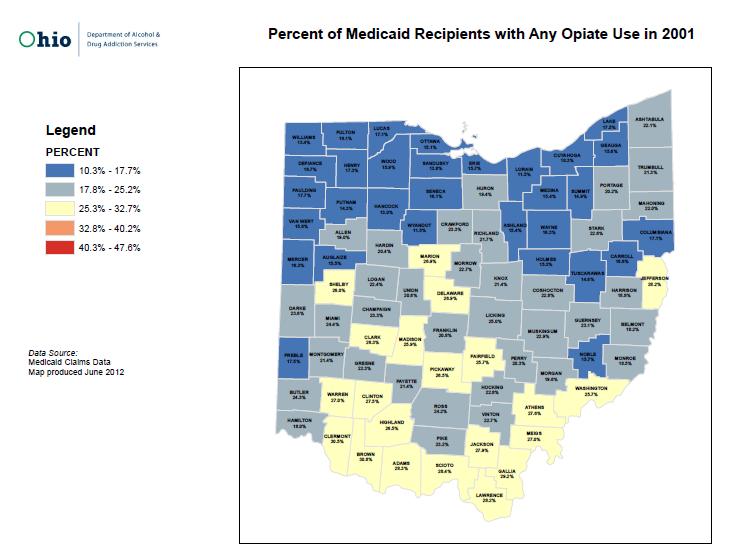
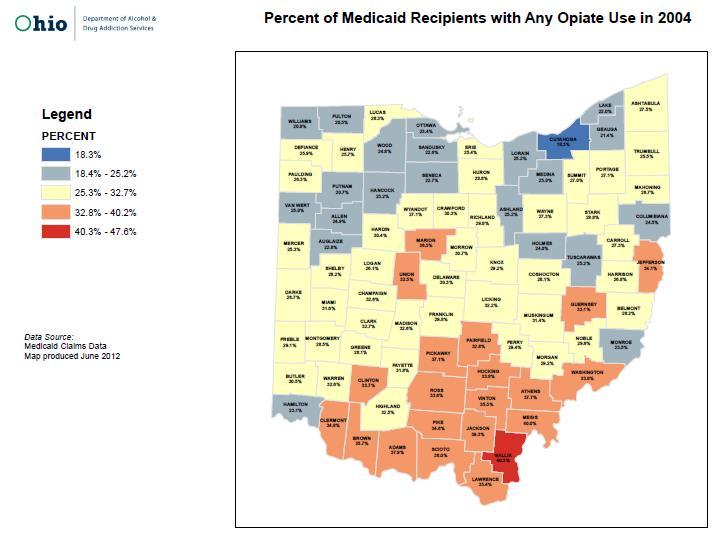
19 GEOGRAPHIC DISTRIBUTION I. Any Opiate Use II. III. Chronic High Use (120 MED, 90 days) Co-occurring Use of Opiates and Drugs Known to Increase Risk
20
21
22
23
24

25
26
27
28

29
30
31
32 NEGATIVE OPIATE USE OUTCOMES Negative outcomes of opiate use increased over time, particularly opiate dependence & abuse X, 305.5X, 304.7X - Opioid dependence and abuse 965.0X Poisoning by opiates & related narcotics* Total number of beneficiaries with a negative outcome of opiate use * Excluding poisoning by heroin
33 NEGATIVE OPIATE USE OUTCOMES In 2010, 40% of individuals with an opioid dependence diagnosis had no Medicaid claim for opiates CDC reports 25% to 66% of opiate overdose deaths are attributed to opiates obtained without a prescription (CDC Director s Grand Rounds, 2011) X - Opioid dependence, no Medicaid script 304.0x - Opioid dependence, with a Medicaid script Total number of beneficiaries with a negative outcome of opiate use
34 ED VISITS RELATED TO NEGATIVE OPIATE OUTCOMES Increased prevalence of ED visits attributed to negative opiate outcomes (opiate dependence, abuse, poisoning) Cost of nearly $2 million in $1,092,799 per year $1,862,382 per year Table values represent the total number and annual cost of ED visits associated with negative opiate outcomes (opiate dependence, abuse, and poisoning)
35 OPIATES PRESCRIBED IN ED* The emergency department increasingly a source for opiate medication In 2010, a total of176,423 Medicaid beneficiaries (14%) filled an opiate prescription within four days of an ED visit 16% 14% 12% 10% 8% 6% 4% 2% 0% N=24,439 N=90,276 N=176, Proportion of beneficiaries with an opiate claim 4 days of an ED visit. *excluding opiates provided in the ED and ED visits preceding hospitalization
36 Factors Associated with Negative Outcomes Beneficiaries odds of having a negative outcome* were 1.6 times higher the they used a benxodiazepine and an opiate concurrently 2.1 times higher if they received opiates from 5 or more prescribers or pharmacies 2.9 times higher white versus black 6.8 times higher if they used over 120 MED daily 6.2 times higher if they used over 50 MED daily * Negative outcomes include diagnosis of opiate abuse, dependence or poisoning
37 CONCLUSIONS I. Prevalence of opiate use among Ohio Medicaid beneficiaries has increased steadily from 2001 to II. III. Highest use among 45 to 64 year olds, whites, and women. Opiates have become increasingly common treatment for a variety of pain conditions, including back, abdominal, ocular migraine, and orthopedic conditions. IV. High risk patterns of opiate use increased between 2001 and 2010, including High dose, chronic opiate use (120 mg, 90 days) High risk drug combinations Multiple prescribers and multiple pharmacies
38 CONCLUSIONS V. Steady growth in opiate use and high risk patterns in all geographic regions of Ohio. Annual rates of opiate use above 40% in many SE counties. VI. VII. VIII. Increase in negative outcomes related to opiates (opiate dependence, abuse, and poisoning). Three-fold increase in ED visits for negative opiate use outcomes Factors associated with negative opiate use outcomes include high daily dose, multiple pharmacies, and multiple ordering providers. A three-fold increase in opiates prescribed in the ED, a possible indication of increased opiate seeking
39 POSSIBLE NEXT STEPS Cohort analysis to assess risk of reaching dosage and chronicity thresholds and outcomes. Engage other health and human service sectors (e.g., BWC, ODH vital statistics). Assess risk to individuals with serious mental illness, particularly depression. Track impact of state policy initiatives on patterns of use.
USE OF OPIODS AT HIGHER DOSES IN PERSONS WITHOUT CANCER: MORPHINE EQUIVALENT DOSE EDIT
 BACKGROUND: USE OF OPIODS AT HIGHER DOSES IN PERSONS WITHOUT CANCER: MORPHINE EQUIVALENT DOSE EDIT Approximately 10% of patients who are prescribed opioids and seek care from multiple doctors, are prescribed
BACKGROUND: USE OF OPIODS AT HIGHER DOSES IN PERSONS WITHOUT CANCER: MORPHINE EQUIVALENT DOSE EDIT Approximately 10% of patients who are prescribed opioids and seek care from multiple doctors, are prescribed
A nation in pain: Focus on Medicaid
 DATA INSIGHTS A nation in pain: Focus on Medicaid Opioid pain medications have become one of the most controversial classes of prescription therapy. While they provide great benefits in controlling both
DATA INSIGHTS A nation in pain: Focus on Medicaid Opioid pain medications have become one of the most controversial classes of prescription therapy. While they provide great benefits in controlling both
Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities
 Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities Svetla Slavova, PhD Sara LaMantia, MS Terry Bunn, PhD Tracey Corey, MD 2016 Safe States Annual Meeting April 13, 2016, Albuquerque,
Identification of Specific Drugs and Drug Diversion in Drug Overdose Fatalities Svetla Slavova, PhD Sara LaMantia, MS Terry Bunn, PhD Tracey Corey, MD 2016 Safe States Annual Meeting April 13, 2016, Albuquerque,
Montgomery County Poisoning Death Review, 2016: Quarter I Updated June 20, 2016
 Montgomery County Poisoning Death Review, 2016: Quarter I Updated June 20, 2016 Prepared by: Robert G. Carlson, Ph.D., Professor and Director, Project Director Linna Li, M.S., Data Manager Raminta Daniulaityte,
Montgomery County Poisoning Death Review, 2016: Quarter I Updated June 20, 2016 Prepared by: Robert G. Carlson, Ph.D., Professor and Director, Project Director Linna Li, M.S., Data Manager Raminta Daniulaityte,
PRESCRIBING GUIDELINES
 Ohio Department of Health RESPONSE TO OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: PRESCRIBING GUIDELINES MIPA CONFERENCE PREVENTING INJURY: FROM RESEARCH TO PRACTICE TO PEOPLE SEPTEMBER 30, 2013 Christy
Ohio Department of Health RESPONSE TO OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: PRESCRIBING GUIDELINES MIPA CONFERENCE PREVENTING INJURY: FROM RESEARCH TO PRACTICE TO PEOPLE SEPTEMBER 30, 2013 Christy
The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH 6/30/2017
 The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH 6/30/2017 The Mississippi Drug Abuse Project, Mississippi State Department of Health Working Group Manuela Staneva, MPH, Project Epidemiologist Meg
The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH 6/30/2017 The Mississippi Drug Abuse Project, Mississippi State Department of Health Working Group Manuela Staneva, MPH, Project Epidemiologist Meg
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
Clinical Policy: Opioid Analgesics Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid
 Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup. Opioid Prescribing Metrics - DRAFT
 Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Medicare-Medicaid Data Integration (MMDI) Use Case: Profiling Potential Opioid Misuse among Dual Eligibles
 Use Case: Profiling Potential Opioid Misuse among Dual Eligibles") Medicare-Medicaid Data Integration (MMDI) Use Case: Profiling Potential Opioid Misuse among Dual Eligibles Contract: HHSN-316-2012-00139W Order: HHSM-500-2014-00114U December 12, 2017 Prepared by: FEi
Medicare-Medicaid Data Integration (MMDI) Use Case: Profiling Potential Opioid Misuse among Dual Eligibles Contract: HHSN-316-2012-00139W Order: HHSM-500-2014-00114U December 12, 2017 Prepared by: FEi
Proposed Changes to Existing Measure for HEDIS : Use of Opioids at High Dosage (UOD)
") Proposed Changes to Existing Measure for HEDIS 1 2020: Use of Opioids at High Dosage (UOD) NCQA seeks comments on proposed revisions to the Use of Opioids at High Dosage HEDIS measure. The current measure
Proposed Changes to Existing Measure for HEDIS 1 2020: Use of Opioids at High Dosage (UOD) NCQA seeks comments on proposed revisions to the Use of Opioids at High Dosage HEDIS measure. The current measure
Appendix A. Socio-demographic Characteristics of Survey Respondents Compared to Current Population Survey (2013) Data
 Data") Data Supplement for Kennedy-Hendricks et al. (10.1176/appi.ps.201600056) Appendix A. Socio-demographic Characteristics of Survey Respondents Compared to Current Population Survey (2013) Data Un-weighted
Data Supplement for Kennedy-Hendricks et al. (10.1176/appi.ps.201600056) Appendix A. Socio-demographic Characteristics of Survey Respondents Compared to Current Population Survey (2013) Data Un-weighted
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
2017 PGIP Fact Sheet Electronic Prescribing of Controlled Substances (EPCS)
") 2017 PGIP Fact Sheet Electronic Prescribing of Controlled Substances (EPCS) Overview Value Partnerships, in conjunction with the Blue Cross Pharmacy team, has created the Electronic Prescribing of Controlled
2017 PGIP Fact Sheet Electronic Prescribing of Controlled Substances (EPCS) Overview Value Partnerships, in conjunction with the Blue Cross Pharmacy team, has created the Electronic Prescribing of Controlled
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Montgomery County Poisoning Death Review
 Wright State University CORE Scholar Unintentional Prescription Drug Poisoning Project Center for Interventions, Treatment and Addictions Research Montgomery County Poisoning Death Review - Center for
Wright State University CORE Scholar Unintentional Prescription Drug Poisoning Project Center for Interventions, Treatment and Addictions Research Montgomery County Poisoning Death Review - Center for
BC Coroners Service Prescription Opiate-Related Overdose Deaths
 This report summarises prescription opiate-related overdose deaths reported to the BC Coroners Service between 2005 and 2010 with a classification of accidental, suicide, or undetermined. Cases were included
This report summarises prescription opiate-related overdose deaths reported to the BC Coroners Service between 2005 and 2010 with a classification of accidental, suicide, or undetermined. Cases were included
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
New Guidelines for Prescribing Opioids
 New Guidelines for Prescribing Opioids Keeping Your Claimants Safe Presented by: Dr. Mitch Freeman, Pharm.D. Chief Clinical Officer, Pharmacy Solutions Agenda The Opioid Challenge Today How We Got Here
New Guidelines for Prescribing Opioids Keeping Your Claimants Safe Presented by: Dr. Mitch Freeman, Pharm.D. Chief Clinical Officer, Pharmacy Solutions Agenda The Opioid Challenge Today How We Got Here
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
CDC s Efforts to End the Opioid Epidemic
 Amy Insert Peeples, CIO Name MPA Here Deputy Director, National Center for Injury Prevention and Control NCSL Opioid Policy Fellows Kick Off CDC s Efforts to End the Opioid Epidemic The Epidemic in America
Amy Insert Peeples, CIO Name MPA Here Deputy Director, National Center for Injury Prevention and Control NCSL Opioid Policy Fellows Kick Off CDC s Efforts to End the Opioid Epidemic The Epidemic in America
Michael M. Miller, MD, FASAM, FAPA
 Michael M. Miller, MD, FASAM, FAPA mmiller@rogershospital.org Medical Director, Herrington Recovery Center (HRC) Rogers Memorial Hospital Oconomowoc, Wisconsin Vice Speaker Wisconsin Medical Society Clinical
Michael M. Miller, MD, FASAM, FAPA mmiller@rogershospital.org Medical Director, Herrington Recovery Center (HRC) Rogers Memorial Hospital Oconomowoc, Wisconsin Vice Speaker Wisconsin Medical Society Clinical
What is the strategy?
 What is the strategy? Multi-pronged approaches to reducing the health consequences of opioid use, New York City Northeast Epidemiology Conference Public health approach Track drug use and associated health
What is the strategy? Multi-pronged approaches to reducing the health consequences of opioid use, New York City Northeast Epidemiology Conference Public health approach Track drug use and associated health
The Epidemiology of Opioid Abuse. Thomas Dobbs, MD, MPH Mississippi State Department of Health
 The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH Mississippi State Department of Health 1/12/2018 ACKNOWLEDGEMENTS DRUG ABUSE WORKING GROUP MISSISSIPPI STATE DEPARTMENT OF HEALTH Manuela Staneva,
The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH Mississippi State Department of Health 1/12/2018 ACKNOWLEDGEMENTS DRUG ABUSE WORKING GROUP MISSISSIPPI STATE DEPARTMENT OF HEALTH Manuela Staneva,
Curbing Prescription Drug Abuse in Medicaid
 Curbing Prescription Drug Abuse in Medicaid Joint Legislative Health Care Oversight Committee October 12, 2010 Dr. Lisa Weeks, BSPharm, PharmD Pharmacy and Ancillary Services Division of Medical Assistance
Curbing Prescription Drug Abuse in Medicaid Joint Legislative Health Care Oversight Committee October 12, 2010 Dr. Lisa Weeks, BSPharm, PharmD Pharmacy and Ancillary Services Division of Medical Assistance
Opioid Addiction Statistics
 May 2017 Opioid Addiction Statistics Definitions Heroin Epidemic - As pill mills close, prescribing is becoming tighter, demand among younger users rise, and dealer s profits rise, addicts are turning
May 2017 Opioid Addiction Statistics Definitions Heroin Epidemic - As pill mills close, prescribing is becoming tighter, demand among younger users rise, and dealer s profits rise, addicts are turning
Pain Management Wrap-Up Chronic Care. David Tauben, MD Medicine Anesthesia & Pain Medicine
 Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
Pain Management Wrap-Up Chronic Care David Tauben, MD Medicine Anesthesia & Pain Medicine Objectives Understand that Pain is Complex Know how to select Rx based on Pain type Be aware that Rx only reduces
ARKANSAS DEPARTMENT OF HEALTH
 Thank you for taking an interest in the Arkansas Prescription Monitoring Program (PMP). The goal of the PMP is to enhance patient care by ensuring the legitimate use of controlled substances. The following
Thank you for taking an interest in the Arkansas Prescription Monitoring Program (PMP). The goal of the PMP is to enhance patient care by ensuring the legitimate use of controlled substances. The following
using analytics to identify and strategically manage patient opioid abuse
 using analytics to identify and strategically manage patient opioid abuse Philip Finocchiaro, MD, FACP Senior Medical Director, Quality and Clinical Outcomes Verscend Olivia Mapplethorpe Senior Client
using analytics to identify and strategically manage patient opioid abuse Philip Finocchiaro, MD, FACP Senior Medical Director, Quality and Clinical Outcomes Verscend Olivia Mapplethorpe Senior Client
The Population is Abusing Drugs, but are Drugs Abusing Insurance?
 Image licensed from Shutterstock The Population is Abusing Drugs, but are Drugs Abusing Insurance? 01/30/2018 Gina C. Guzman, MD, DBIM, FALU, FLMI, VP and Chief Medical Director Tim Morant, FSA, MAAA,
Image licensed from Shutterstock The Population is Abusing Drugs, but are Drugs Abusing Insurance? 01/30/2018 Gina C. Guzman, MD, DBIM, FALU, FLMI, VP and Chief Medical Director Tim Morant, FSA, MAAA,
PRESCRIPTION DRUG MONITORING PROGRAM
 PRESCRIPTION DRUG MONITORING PROGRAM ST. LOUIS COUNTY Q2 2017 Contents Executive Summary... 2 User Registration & System Utilization... 4 Dispensation Rates... 6 Dispensation Rates by Geography... 6 Dispensation
PRESCRIPTION DRUG MONITORING PROGRAM ST. LOUIS COUNTY Q2 2017 Contents Executive Summary... 2 User Registration & System Utilization... 4 Dispensation Rates... 6 Dispensation Rates by Geography... 6 Dispensation
Recognizing Narcotic Abuse and Addiction and Helping Those With It
 Recognizing Narcotic Abuse and Addiction and Helping Those With It Michael McNett, MD Medical Director for Chronic Pain Member, WI Med Society Opioid Subcommittee Ancient History 1995: OxyContin approved
Recognizing Narcotic Abuse and Addiction and Helping Those With It Michael McNett, MD Medical Director for Chronic Pain Member, WI Med Society Opioid Subcommittee Ancient History 1995: OxyContin approved
Prescription Drug Monitoring Program Update. Rebecca R. Poston, BPharm., MHL Program Manager August 26, 2017
 Prescription Drug Monitoring Program Update Rebecca R. Poston, BPharm., MHL Program Manager August 26, 2017 Objectives Brief historical overview of opioids Review of PDMP information Discuss ideas from
Prescription Drug Monitoring Program Update Rebecca R. Poston, BPharm., MHL Program Manager August 26, 2017 Objectives Brief historical overview of opioids Review of PDMP information Discuss ideas from
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
NARxCHECK Score as a Predictor of Unintentional Overdose Death
 NARxCHECK Score as a Predictor of Unintentional Overdose Death Huizenga J.E., Breneman B.C., Patel V.R., Raz A., Speights D.B. October 2016 Appriss, Inc. NOTE: This paper was previously published with
NARxCHECK Score as a Predictor of Unintentional Overdose Death Huizenga J.E., Breneman B.C., Patel V.R., Raz A., Speights D.B. October 2016 Appriss, Inc. NOTE: This paper was previously published with
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
Patient Review and Coordination Program
 Patient Review and Coordination Program For Medical Assistance Clients Who Need Assistance In Appropriate Use of Phyllis Coolen, RN, MN Division of Healthcare Health and Recovery Administration January
Patient Review and Coordination Program For Medical Assistance Clients Who Need Assistance In Appropriate Use of Phyllis Coolen, RN, MN Division of Healthcare Health and Recovery Administration January
Drug-Related Deaths in Yolo County,
 Drug-Related Deaths in Yolo County, 2007-2015 May 2017 Authors: Ron Chapman, MD, MPH Haydee Dabritz, PhD Emma Middlemiss, MPH intern Yolo County Health & Human Services Agency (HHSA), Community Health
Drug-Related Deaths in Yolo County, 2007-2015 May 2017 Authors: Ron Chapman, MD, MPH Haydee Dabritz, PhD Emma Middlemiss, MPH intern Yolo County Health & Human Services Agency (HHSA), Community Health
Understanding the Opioid Crisis: What s at the Heart of the Matter?
 National Center for Injury Prevention and Control Understanding the Opioid Crisis: What s at the Heart of the Matter? Sara Patterson Associate Director for Policy National Center for Injury Prevention
National Center for Injury Prevention and Control Understanding the Opioid Crisis: What s at the Heart of the Matter? Sara Patterson Associate Director for Policy National Center for Injury Prevention
Managing Narcotics on Workers Comp Claims. Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc.
 Managing Narcotics on Workers Comp Claims Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc. October 21, 2014 Outline Rationale Scope list drug list Recommended
Managing Narcotics on Workers Comp Claims Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc. October 21, 2014 Outline Rationale Scope list drug list Recommended
REB CLOSE, MD Community Hospital of the Monterey Peninsula
 REB CLOSE, MD Community Hospital of the Monterey Peninsula The Scope of the Problem 1-5 Opiate use in the US 80% of the world s prescription opiate supply 99% of the world s hydrocodone supply From 1997
REB CLOSE, MD Community Hospital of the Monterey Peninsula The Scope of the Problem 1-5 Opiate use in the US 80% of the world s prescription opiate supply 99% of the world s hydrocodone supply From 1997
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Opioid Deaths Quadruple Since 1999
 THE COUNCIL OF STATE GOVERNMENTS CAPITOL RESEARCH AUGUST 2017 HEALTH POLICY Opioid Deaths Quadruple Since 1999 Since 1999, the number of overdose deaths involving opioids (including prescription opioids
THE COUNCIL OF STATE GOVERNMENTS CAPITOL RESEARCH AUGUST 2017 HEALTH POLICY Opioid Deaths Quadruple Since 1999 Since 1999, the number of overdose deaths involving opioids (including prescription opioids
Summit County Public Health
 Page 1 Death and Life Expectancy Summit County Public Health Population Health Vital Statistics Brief: VOLUME 1: DEATH AND LIFE EXPECTANCY Summit County Public Health Population Health Division 1867 W.
Page 1 Death and Life Expectancy Summit County Public Health Population Health Vital Statistics Brief: VOLUME 1: DEATH AND LIFE EXPECTANCY Summit County Public Health Population Health Division 1867 W.
9/5/2011. Outline. 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A
 Prescription Drug Abuse Crises Outline 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A 1 1970s 1980s 2 The 1990s OXYCODONE Oxycodone/APAP OxyContin
Prescription Drug Abuse Crises Outline 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A 1 1970s 1980s 2 The 1990s OXYCODONE Oxycodone/APAP OxyContin
Linking Opioid Treatment in Primary Care. Roxanne Lewin M.D.
 Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Oregon s PDMP: An epidemiological assist tool
 Oregon s PDMP: An epidemiological assist tool Todd Beran Center for Prevention and Health Promotion Oregon Health Authority PDMP TTAC Webinar February 13, 2013 1 Acknowledgements Lisa Millet, MSH, Section
Oregon s PDMP: An epidemiological assist tool Todd Beran Center for Prevention and Health Promotion Oregon Health Authority PDMP TTAC Webinar February 13, 2013 1 Acknowledgements Lisa Millet, MSH, Section
Opioid Analgesics. Recommended starting dose for opioid-naïve patients
 Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
TRIBAL HEALING OPIOID RESPONSE MAY 23, 2018
 TRIBAL HEALING OPIOID RESPONSE MAY 23, 2018 PGST HEALTH SERVICES Only Indian Health Care provider in Kitsap County, Washington Primary Care & Urgent Care, Outpatient FT Family Medicine, FT PA,.2 FTE Pediatrician
TRIBAL HEALING OPIOID RESPONSE MAY 23, 2018 PGST HEALTH SERVICES Only Indian Health Care provider in Kitsap County, Washington Primary Care & Urgent Care, Outpatient FT Family Medicine, FT PA,.2 FTE Pediatrician
PACIFICSOURCE COMMUNITY SOLUTIONS AND GORGE COORDINATED CARE ORGANIZATION. Chronic Pain and Opiate Management Initiatives
 PACIFICSOURCE COMMUNITY SOLUTIONS AND GORGE COORDINATED CARE ORGANIZATION Chronic Pain and Opiate Management Initiatives Objectives To enhance understanding of current concepts, guidelines and risks of
PACIFICSOURCE COMMUNITY SOLUTIONS AND GORGE COORDINATED CARE ORGANIZATION Chronic Pain and Opiate Management Initiatives Objectives To enhance understanding of current concepts, guidelines and risks of
Putnam County. West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report
 West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
Embeda. Embeda (morphine sulfate and naltrexone hydrochloride) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.39 Subject: Embeda Page: 1 of 6 Last Review Date: March 18, 2016 Embeda Description Embeda (morphine
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.39 Subject: Embeda Page: 1 of 6 Last Review Date: March 18, 2016 Embeda Description Embeda (morphine
Greenbrier County. West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report
 West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
10 mg hydrocodone equals how much oxycodone
 Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC:
 Cuyahoga County Board of Health OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: NOVEMBER 5, 2014 CONTRIBUTING FACTORS AND ONGOING PREVENTION EFFORTS DEFINITIONS Opiate- originate from naturally-occurring elements
Cuyahoga County Board of Health OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: NOVEMBER 5, 2014 CONTRIBUTING FACTORS AND ONGOING PREVENTION EFFORTS DEFINITIONS Opiate- originate from naturally-occurring elements
Understanding and Addressing the Public Health Epidemic of Opioid Abuse
 Understanding and Addressing the Public Health Epidemic of Opioid Abuse LEWIS S. NELSON, M.D. PROFESSOR AND CHAIR OF EMERGENCY MEDICINE DIRECTOR, DIVISION OF MEDICAL TOXICOLOGY RUTGERS NEW JERSEY MEDICAL
Understanding and Addressing the Public Health Epidemic of Opioid Abuse LEWIS S. NELSON, M.D. PROFESSOR AND CHAIR OF EMERGENCY MEDICINE DIRECTOR, DIVISION OF MEDICAL TOXICOLOGY RUTGERS NEW JERSEY MEDICAL
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
Ohio s State Innovation Model: Using Episodes of Care to Impact the Opioid Crisis (and Other Public Health Priorities)
") Ohio s State Innovation Model: Using Episodes of Care to Impact the Opioid Crisis (and Other Public Health Priorities) Greg Moody, Director Ohio Governor s Office of Health Transformation NASHP Preconference:
Ohio s State Innovation Model: Using Episodes of Care to Impact the Opioid Crisis (and Other Public Health Priorities) Greg Moody, Director Ohio Governor s Office of Health Transformation NASHP Preconference:
Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk
 Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk Randy Brown MD, PhD, FASAM Associate Professor, Dept of Family Medicine Director, Center for Addictive Disorders, UWHC Director, UW Addiction
Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk Randy Brown MD, PhD, FASAM Associate Professor, Dept of Family Medicine Director, Center for Addictive Disorders, UWHC Director, UW Addiction
White Paper on. Prescription Drug Abuse
 White Paper on Prescription Drug Abuse October 22, 2014 Table of Contents: I. Introduction II. Scope of the Problem III. Most Common Drugs Involved in Overdoses IV. Efforts in Tennessee V. Prescription
White Paper on Prescription Drug Abuse October 22, 2014 Table of Contents: I. Introduction II. Scope of the Problem III. Most Common Drugs Involved in Overdoses IV. Efforts in Tennessee V. Prescription
Lisa Marzilli, PharmD, CDOE TOP 3 REASONS PEOPLE VISIT THEIR DOCTOR
 Lisa Marzilli, PharmD, CDOE TOP 3 REASONS PEOPLE VISIT THEIR DOCTOR 1 1. Skin disorders, including cysts, acne, and dermatitis. 2. Joint disorders, including osteoarthritis. 3. Back problems. Source: Mayo
Lisa Marzilli, PharmD, CDOE TOP 3 REASONS PEOPLE VISIT THEIR DOCTOR 1 1. Skin disorders, including cysts, acne, and dermatitis. 2. Joint disorders, including osteoarthritis. 3. Back problems. Source: Mayo
Opioid Task Force Kick-Off Meeting. February 29, 2016
 Opioid Task Force Kick-Off Meeting February 29, 2016 Scope of the Opioid Problem and Data Review Olivia Kasirye, MD, MS County Public Health Officer OVERVIEW The Opioid Epidemic Opioid Task Force Development
Opioid Task Force Kick-Off Meeting February 29, 2016 Scope of the Opioid Problem and Data Review Olivia Kasirye, MD, MS County Public Health Officer OVERVIEW The Opioid Epidemic Opioid Task Force Development
What do they have in common?
 What do they have in common? Opioid use in USA Approximately 9 million people on long term opioids Approximated 5 million people reporting non-medical use of opioids 1997: 96mg/person morphine eq dispensed
What do they have in common? Opioid use in USA Approximately 9 million people on long term opioids Approximated 5 million people reporting non-medical use of opioids 1997: 96mg/person morphine eq dispensed
OPQC Learning Session: High Risk Moms & Infants. Mary Applegate, MD, FACP, FAAP Medical Director, Ohio Department of Medicaid September 2016
 OPQC Learning Session: High Risk Moms & Infants Mary Applegate, MD, FACP, FAAP Medical Director, Ohio Department of Medicaid September 2016 OLD: 9/19/2016 2 Collaboration, Cooperation & Coordination Microsystems
OPQC Learning Session: High Risk Moms & Infants Mary Applegate, MD, FACP, FAAP Medical Director, Ohio Department of Medicaid September 2016 OLD: 9/19/2016 2 Collaboration, Cooperation & Coordination Microsystems
An Evaluation of the DoD Transdermal Fentanyl Pharmacy Edit. LTC Stacia Spridgen, MSC, USA Director, DoD Pharmacoeconomic Center
 An Evaluation of the DoD Transdermal Fentanyl Pharmacy Edit LTC Stacia Spridgen, MSC, USA Director, DoD Pharmacoeconomic Center 1 TRICARE Eligible Beneficiaries Monthly Average, FY08 Retirees & Family
An Evaluation of the DoD Transdermal Fentanyl Pharmacy Edit LTC Stacia Spridgen, MSC, USA Director, DoD Pharmacoeconomic Center 1 TRICARE Eligible Beneficiaries Monthly Average, FY08 Retirees & Family
Mandatory PDMP Use PDMP Use STATE Prescriber Dispenser Conditions, if applicable
 Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Population Health Vital Statistics Brief:
 Page 1 Death and Life Expectancy Summit County Public Health Population Health Vital Statistics Brief: VOLUME 1: DEATH AND LIFE EXPECTANCY Summit County Public Health Populaon Health Division 1867 W. Market
Page 1 Death and Life Expectancy Summit County Public Health Population Health Vital Statistics Brief: VOLUME 1: DEATH AND LIFE EXPECTANCY Summit County Public Health Populaon Health Division 1867 W. Market
Abuse, Misuse, and Diversion of Prescription Opioids: Evaluating the Problem and Proposed Solutions
 Abuse, Misuse, and Diversion of Prescription Opioids: Evaluating the Problem and Proposed Solutions Eric Lavonas, MD, FACEP, FACMT, FAACT Associate Director, Rocky Mountain Poison & Drug Center Denver
Abuse, Misuse, and Diversion of Prescription Opioids: Evaluating the Problem and Proposed Solutions Eric Lavonas, MD, FACEP, FACMT, FAACT Associate Director, Rocky Mountain Poison & Drug Center Denver
Opioid epidemic and PEHP
 Opioid epidemic and PEHP Agenda Overview of opioid crisis Utah perspective PEHP: clinical interventions Impact of interventions Why are we here? In the 1990s, the medical establishment came to believe
Opioid epidemic and PEHP Agenda Overview of opioid crisis Utah perspective PEHP: clinical interventions Impact of interventions Why are we here? In the 1990s, the medical establishment came to believe
Changing Course: statewide efforts to combat the opioid epidemic in California
 Changing Course: statewide efforts to combat the opioid epidemic in California Kelly Pfeifer, MD kpfeifer@chcf.org April 26, 2018 State of Reform conference STAT Special Report: 52 weeks, 52 faces Obituaries
Changing Course: statewide efforts to combat the opioid epidemic in California Kelly Pfeifer, MD kpfeifer@chcf.org April 26, 2018 State of Reform conference STAT Special Report: 52 weeks, 52 faces Obituaries
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
Long-Acting Opioid Analgesics
 Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Shining a Light on MEDs Understanding morphine equivalent dose
 Shining a Light on MEDs Understanding morphine equivalent dose In the workers compensation industry, 60.2 percent of claimants utilize opioid analgesics for the treatment of pain caused by a workplace
Shining a Light on MEDs Understanding morphine equivalent dose In the workers compensation industry, 60.2 percent of claimants utilize opioid analgesics for the treatment of pain caused by a workplace
Preventing Prescription Drug and Heroin Abuse and Deaths: Practical Strategies. July 12, 2015
 Preventing Prescription Drug and Heroin Abuse and Deaths: Practical Strategies July 12, 2015 What are Opioids? Natural opioids are contained in the resin of opium poppy (e.g., morphine, codeine) Semi-synthetic
Preventing Prescription Drug and Heroin Abuse and Deaths: Practical Strategies July 12, 2015 What are Opioids? Natural opioids are contained in the resin of opium poppy (e.g., morphine, codeine) Semi-synthetic
RP PERCOCET STREET VALUE
 RP 5 325 PERCOCET STREET VALUE Rp 5 325 Percocet Street Value Max dose of percocet a day Urgent care percocet bothell wa 98012 directions I need a substitute for percocet 10/325 percocet Percocet constipation
RP 5 325 PERCOCET STREET VALUE Rp 5 325 Percocet Street Value Max dose of percocet a day Urgent care percocet bothell wa 98012 directions I need a substitute for percocet 10/325 percocet Percocet constipation
Long-Acting Opioid Analgesics
 Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Welcome - we will begin the webinar shortly Please read the participation tips below:
 Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
PRESCRIPTION DRUG MONITORING PROGRAM ST. CHARLES COUNTY Q1 2018
 PRESCRIPTION DRUG MONITORING PROGRAM ST. CHARLES COUNTY Q1 2018 Contents Executive Summary... 2 User Registration & System Utilization... 4 Dispensation Rates... 6 Dispensation Rates by Geography... 6
PRESCRIPTION DRUG MONITORING PROGRAM ST. CHARLES COUNTY Q1 2018 Contents Executive Summary... 2 User Registration & System Utilization... 4 Dispensation Rates... 6 Dispensation Rates by Geography... 6
Opioid Prescription and Illicit Drug Overdoses: On the Rise
 Opioid Prescription and Illicit Drug Overdoses: On the Rise Cindy Haynes, MSA-PA, CHES Chronic Pain Program Coordinator Northern Piedmont Community Care Duke Division of Community Health Objectives Define
Opioid Prescription and Illicit Drug Overdoses: On the Rise Cindy Haynes, MSA-PA, CHES Chronic Pain Program Coordinator Northern Piedmont Community Care Duke Division of Community Health Objectives Define
15 mg morphine 10 mg hydrocodone
 Cari untuk: Cari Cari 15 mg morphine 10 mg hydrocodone 3-2-2013 Convert From CALCULATED MORPHINE EQUIVALENT BY RESOURCE: Average ( mg ) Range ( mg ) Standard Deviation of Sample ( mg ) Hydrocodone. I usually
Cari untuk: Cari Cari 15 mg morphine 10 mg hydrocodone 3-2-2013 Convert From CALCULATED MORPHINE EQUIVALENT BY RESOURCE: Average ( mg ) Range ( mg ) Standard Deviation of Sample ( mg ) Hydrocodone. I usually
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
MEDICARE Program Policies & Procedures POLICY NUMBER: Medicare D-111
 POLICY: Medicare Part D Formulary-Level Cumulative Opioid and Opioid/Buprenorphine POS Edits MEDICARE Program Policies & Procedures POLICY NUMBER: Medicare D-111 Policy for contracts H3351, S3521 and H3335
POLICY: Medicare Part D Formulary-Level Cumulative Opioid and Opioid/Buprenorphine POS Edits MEDICARE Program Policies & Procedures POLICY NUMBER: Medicare D-111 Policy for contracts H3351, S3521 and H3335
Oxycontin conversion to ms contin
 Oxycontin conversion to ms contin The Borg System is 100 % Oxycontin conversion to ms contin Ms contin to morphine conversion MS Contin is. The patient s current dose of 240 mg per day of oral oxycodone
Oxycontin conversion to ms contin The Borg System is 100 % Oxycontin conversion to ms contin Ms contin to morphine conversion MS Contin is. The patient s current dose of 240 mg per day of oral oxycodone
Opioid Step Policy. Description. Section: Prescription Drugs Effective Date: April 1, 2018
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention
 The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
Aetna s Initiative on the Opioid Epidemic
 Aetna s Initiative on the Opioid Epidemic Christopher James D.O., M.P.H. Medical Director, BH- Mid-Atlantic Territory (JamesC1@aetna.com) July 23, 2017 HHS Data on Epidemic Every Day in the U.S. More than
Aetna s Initiative on the Opioid Epidemic Christopher James D.O., M.P.H. Medical Director, BH- Mid-Atlantic Territory (JamesC1@aetna.com) July 23, 2017 HHS Data on Epidemic Every Day in the U.S. More than
Barbour County. West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report Barbour County
 County West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report County The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with
County West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report County The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
Prescription Opioid Overdose in Oregon: A public health perspective
 Prescription Opioid Overdose in Oregon: A public health perspective Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Health Authority All-Cause Mortality,
Prescription Opioid Overdose in Oregon: A public health perspective Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Health Authority All-Cause Mortality,
OHIO S OPIOID DRUG OVERDOSE EPIDEMIC: CONTRIBUTING FACTORS AND ONGOING PREVENTION EFFORTS
 OHIO S OPIOID DRUG OVERDOSE EPIDEMIC: CONTRIBUTING FACTORS AND ONGOING PREVENTION EFFORTS DEFINITIONS Opiate- originate from naturally-occurring elements found in the opium poppy plant. These drugs are
OHIO S OPIOID DRUG OVERDOSE EPIDEMIC: CONTRIBUTING FACTORS AND ONGOING PREVENTION EFFORTS DEFINITIONS Opiate- originate from naturally-occurring elements found in the opium poppy plant. These drugs are
Interventions in Prescription Opioid Abuse Do (or can) Prescription Monitoring Programs Make a Difference?
 Prescription Monitoring Programs Make a Difference?") Interventions in Prescription Opioid Abuse Do (or can) Prescription Monitoring Programs Make a Difference? Richard C. Dart, MD, PhD Executive Director of RADARS System, Denver, Colorado Professor, University
Interventions in Prescription Opioid Abuse Do (or can) Prescription Monitoring Programs Make a Difference? Richard C. Dart, MD, PhD Executive Director of RADARS System, Denver, Colorado Professor, University
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot
 Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot") National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
National Drug Early Warning System (NDEWS) Sentinel Community Site (SCS) Drug Use Patterns and Trends: SCS Snapshot The SCS Snapshot is prepared by NDEWS Coordinating Center staff and contains graphics
Advancing Addiction Science to Address the Opioid Crisis
 Advancing Addiction Science to Address the Opioid Crisis National Institute on Drug Abuse Bringing the full power of science to bear on drug abuse and addiction Nora D. Volkow, M.D. Director National Institute
Advancing Addiction Science to Address the Opioid Crisis National Institute on Drug Abuse Bringing the full power of science to bear on drug abuse and addiction Nora D. Volkow, M.D. Director National Institute
Mingo County. West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report
 West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE
 BACKGROUND PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE In March, 2016, the CDC released the final version of their Guidelines for Prescribing Opioids for Chronic Pain.
BACKGROUND PROPOSED DUR CRITERIA FOR MANAGING OPIOID USE AND MINIMIZING RISK OF OVERDOSE In March, 2016, the CDC released the final version of their Guidelines for Prescribing Opioids for Chronic Pain.
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Opioid Crisis, Our Response Massachusetts Coalition for the Prevention of Medical Errors. October 31, 2016
 Opioid Crisis, Our Response Massachusetts Coalition for the Prevention of Medical Errors October 31, 2016 Introduction: The Team Dr. Tony Dodek, Vice President, Medical Quality & Strategy, and Associate
Opioid Crisis, Our Response Massachusetts Coalition for the Prevention of Medical Errors October 31, 2016 Introduction: The Team Dr. Tony Dodek, Vice President, Medical Quality & Strategy, and Associate