Emergency Toxicology. Piyachat Sasipattarapong, MD, FTCEP Emergency Medicine Khon Kaen Hospital
|
|
|
- Alfred Norton
- 6 years ago
- Views:
Transcription



1 Emergency Toxicology Piyachat Sasipattarapong, MD, FTCEP Emergency Medicine Khon Kaen Hospital
2 Dose Therapeutic index Determination of Toxicity Route of exposure GI, Inhalation, Cutaneous Host Extreme age, Pregnancy






3 Airway Skin Eye GI Tissue & Organs Decontamination Enhanced Elimination
4 Approach Attempts to identify the poison should not delay care Always start with ABC s ACLS algorithms apply with few exceptions Once stable minimize bioavailability history & physical exams
5 General Approach A : Airway B : Breathing C : Circulation D : Disability, Diagnosis history, physical exams, investigation, Decontamination E : Enhanced Elimination F : Find antidote G : Get Tox consult if needed




6 Airway Flaccid tongue, aspiration, respiratory arrest Mental status & gag/cough reflex Sniffing position, jaw thrust Head-down, left-sided position Oropharynx FB, secretions Intubation? - Naloxone first in opioids overdose

7 Breathing except Paraquat!! O 2 Correct hypoxia ABG: pco 2 > 60 intubation Lung - Bronchospasm: - Bronchorrhea/crepitations: - Stridor: Intubation? Albuterol nebulizer Atropine?

8 Circulation IV access Blood work, CBG Hypotension NS ml/kg Vasopressors if still hypotensive: Dopamine PRC if bleeding / anemic Hypertension Nitroprusside, β-blocker ECG: arrhythmias, treat accordingly

9 Disability Altered mental status Hypoxia Opioid intoxication Hypoglycemia Wernicke s encephalopathy CNS depressants Coma Cocktail

10 Coma Cocktail Diagnostic & Therapeutic - O 2 -Thiamine: 100 mg IV -Dextrose: 50%, 50 ml IV -Naloxone: 0.01 mg/kg IV


11 Seizure - Diazepam mg/kg IV - Midazolam mg/kg IM or mg/kg IV - Phenobarbital mg/kg IV over min Pyridoxine - isoniazid, Pralidoxime & Atropine - organophosphate/ carbamate Agitation Haloperidol 5-10 mg IM Trauma? Foley catheter Rectal temperature

12 Cardiac Arrest? Toxin Toxins with specific antidote Digoxin Organophosphates Envenomation Sodium channel blocker / wide-complex tachycardia Calcium channel blocker / β-blocker High-dose Local anesthetic agents Lipophilic cardiotoxins Intervention Antidote Digoxin Fab Atropine Antivenom Sodium bicarbonate Insulin IV lipid emulsion
13 Exposure Toxidrome? Poisoning? Overdose? Drug interaction? Withdrawal?
 Antipsychotics")
14 Atropine Benztropine TCA Antihistamines (CPM) Antipsychotics (Clozapine)



15 Amanita pantherina เห ดเกล ดดาว Amanita muscaria Jimson weed, angel s trumpet มะเข อบ า ดอกลาโพง แตรนางฟ า

16 Treatment Physical restraints Pharmacologic sedation: IV benzodiazepine Physostigmine - controversial

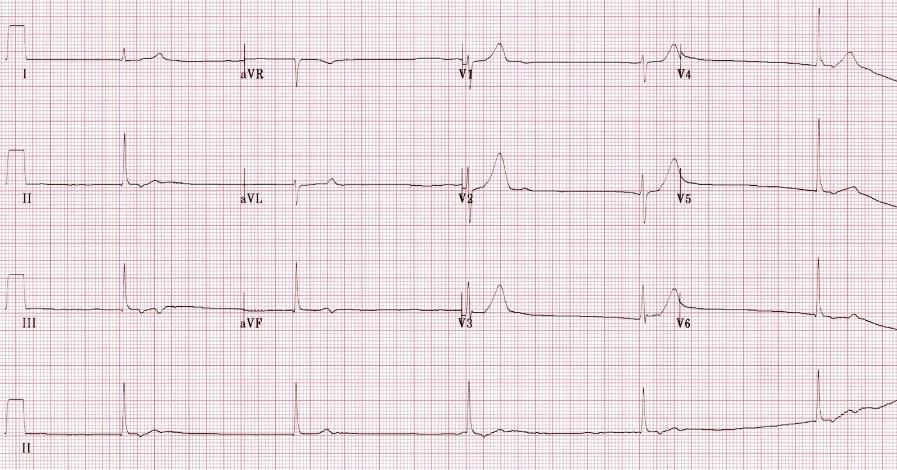
17 Normal avr Get an ECG Abnormal avr

18

19 TCA Overdose Sodium bicarbonate Wide QRS > 100 ms, ventricular dysrhythmia, hypotension refractory to fluid 1 2 meq/kg bolus (to serum ph )

20 Cholinergic

21
22 Muscarinic Salivation Lacrimation Urination Defecation GI upset Emesis Bronchospasm Bradycardia Bronchorrhea SLUDGE-BBB Pilocarpine, Mushroom Organophosphates, Carbamates Nicotinic Mydriasis Tachycardia Weakness HyperTension Fasciculation Mon - Fri Tobacco Organophosphates Carbamates



23 Pesticide, Nerve agent Organophosphates irreversible Carbamate - reversible


24


25 Inocybe Clitocybe
26 Cholinergic Antidote Atropine - muscarinic effects Pralidoxime - reverse phosphorylation of cholinesterase

27 Opioid RR, BP, BT Lethargy, coma Miosis, bowel sound Respiratory arrest, cardiac arrest DDX: Pontine / Cerebellar lesion
, IV/IM (child) - effective in 1-3 min - no response after 3 min titrate 0.")
28 Classical triad 1. Pinpoint pupils 2. Respiratory depression 3. Coma Respiratory status = indicator for response of naloxone Naloxone 0.01 mg/kg IV (Adult), IV/IM (child) - effective in 1-3 min - no response after 3 min titrate , Max mg - Completely reverse symptom min


29 Naloxone Potent opioid receptor antagonist Acute withdrawal syndrome Rarely life-threatening Hypertension, tachycardia, piloerection, vomiting, agitation, drug cravings Minimize; use lowest effective dose, opioid dependency



30 BLS 2015
 Cardiac Arrest?")
31 ACLS 2015 Respiratory Arrest Bag-mask ventilation Naloxone: perfusing cardiac rhythm Ventilation until spontaneous breathing, standard ACLS if no spontaneous breathing (Class I, LOE C-LD) Cardiac Arrest? No recommendation, Standard ACLS



32 Sympathomimetic CNS excitation, convulsion Hypertension, tachycardia, fever Mydriasis, bowel sound Diaphoriasis, hyperreflexia β-adrenergic- theophylline, caffeine, albuterol α-adrenergic- phenylephrine, ท ฟฟ -ด คอลเจน Mixed- amphetamine, cocaine

33
34

35

36 CHIPES C : Chloral hydrate, Calcium H : Heavy metals I : Iron P : Phenothiazines, Packers E : Enteric-coated S : Sustained-release
37 Decontamination Skin decontamination Eyes decontamination GI decontamination osyrup of Ipecac ogastric lavage oactivated charcoal owhole Bowel Irrigation




38 Skin decontamination Protect yourself & HC workers Remove clothing Corrosive agents- skin, systemic effect Flush with water / NS Soap & shampoo - oily


39 Eyes decontamination Corrosive agents & hydrocarbon Remove contact lens Irrigate with full eyelids retraction 20 min, > 1-2 hr for base Medial to lateral, > 1 L ph paper : 7.4 Slit lamp



40
41 GI decontamination Syrup of ipecac Not recommended Gastric lavage Not routine!! Within 60 min after ingestion Reduce small pill, pill fragment Effective %
42 Gastric Lavage Contraindication - Alteration of consciousness (need intubation) - Corrosive except hydrofluoric, paraquat, phenol - Hydrocarbon - Sustained-release / enteric-coated - Non toxic Complication - Perforation, nosebleed, vomiting, aspiration


43

44

45 Activated charcoal Within 60 min, 1 g / kg orally Superior to lavage Awake / intubated Contraindication: bowel obstruction, ileus, GI perforation, not absorbed by AC Complication: vomiting, aspiration, bezoar formation

46 Not good for CHAMPS C : caustics H : hydrocarbons A : alcohols M : metals P : Pb S : Salts


47


48 Whole bowel irrigation L/h - adults 25 ml/kg/h - children NG tube / oral ingestion End point : Clear rectal effluent
49 Indication Enteric coated / sustained-release tablets Foreign body Iron, Lithium, heavy metal Body packers / stuffers Contraindication Unprotected / compromised airway Bowel obstruction / ileus Adverse effects Nausea & bloating, regurgitation & aspiration


50

51

52 Enhanced Elimination Multidose activated charcoal Indication Enterohepatic recirculation Dose Initial loading : 1 g/kg orally / gastric tube then 0.5 g/kg q 2-3 hr for hr followed by stool softening agent
53 These People Drink Charcoal Quickly Theophylline Phenobarbital Dapsone Carbamazepine Quinine Contraindication Intestinal obstruction Ileus Complication Fluid & electrolyte disturbance

54 Urine alkalinization Ion trap ; weak acid Salicylate, phenobarbital, 2,4D, TCA, methotrexate Dose: NaHCO meq/kg then infusion, keep urine ph (TCA; serum ) Contraindication: volume / sodium overload, hypokalemia, renal insufficiency Complication: pulmonary edema, ph shift, hypokalemia

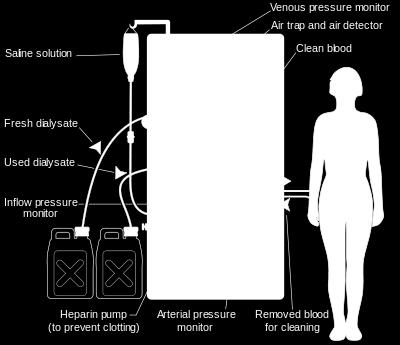

55 Extracorporeal Removal Technique Hemodialysis
 -Cyanide -Cyanide Dextrose 1 gm/kg IV Insulin Oral hypoglycemics Digoxin Fab 5 10")
56 Find Antidote Adult Dose Indication Calcium gluconate 10%, ml IV Hypermagnesemia Hypocalcemia Cyanide antidote kit -Amyl nitrite -Sodium nitrite -Sodium thiosulfate -1 ampule O 2 chamber of ventilation bag 30 s on/30 s off -3%, 10 ml IV -25%, 50 ml IV -Cyanide Hydrogen sulfide (use only sodium nitrite) -Cyanide -Cyanide Dextrose 1 gm/kg IV Insulin Oral hypoglycemics Digoxin Fab 5 10 vials Digoxin & other cardioactive steroids Flumazenil 0.2 mg IV Benzodiazepines Glucagon 3 10 mg IV CCB β-blockers

57 Antidote Adult Dose Indication benzocaine, sulfonamides) Methylene blue 1 2 mg/kg IV Oxidizing toxins (nitrites, Pyridoxine Gm for gm if known Isoniazid amount of isoniazid Gyromitra esculenta 5 gm IV Sodium bicarbonate 1 2 meq/kg IV bolus followed by 2 meq/kg/h IV infusion Hydrazine Sodium channel blockers Urinary alkalinization Thiamine 100 mg IV Wernicke s syndrome Wet beriberi IV lipid emulsion 20% 100-mL IV bolus over 1 min, follow by 400 ml IV over 20 min Local anesthetic toxicity Rescue therapy for lipophilic cardiotoxins
 cardiovascular collapse")

58 Intravenous Lipid Emulsion Local Anesthetic Systemic Toxicity (LAST) CNS (agitation seizure/ CNS depression) cardiovascular collapse Cardiovascular collapse refractory to standard therapy Neurologic & cardiovascular monitoring, dose fractionation, slow injection, epinephrine / ultrasound

59 ACLS 2015 Concomitant with standard resuscitative care- LAST, particularly neurotoxicity/ cardiac arrest due to bupivacaine Other forms of drug toxicity failing standard resuscitation TCA, β-blocker, CCB Class IIb, LOE C-EO
60 Disposition? Patients with potentially serious overdose -observed for at least 6 8 hrs Beware of delayed complications from slow absorption of medications Psychiatric consultation - suicide risk

61 SI RA 1367
Chapter 13. Learning Objectives. Learning Objectives 9/11/2012. Poisonings, Overdoses, and Intoxications
 Chapter 13 Poisonings, Overdoses, and Intoxications Learning Objectives Discuss use of activated charcoal in treatment of poisonings List treatment options for acetaminophen overdose List clinical manifestations
Chapter 13 Poisonings, Overdoses, and Intoxications Learning Objectives Discuss use of activated charcoal in treatment of poisonings List treatment options for acetaminophen overdose List clinical manifestations
Clinical Pathway: Management Of The Life-Threatening Overdose
 Clinical Pathway: Management Of The Life-Threatening Overdose Intravenous access Oxygen Pulse oximetry n-invasive blood pressure monitoring Accu-Check ECG monitoring and ECG Chest x-ray Respiratory depression?
Clinical Pathway: Management Of The Life-Threatening Overdose Intravenous access Oxygen Pulse oximetry n-invasive blood pressure monitoring Accu-Check ECG monitoring and ECG Chest x-ray Respiratory depression?
POISON ANTIDOTE DOSE* COMMENTS
 Antidotes Acetaminophen N-acetylcysteine 140 mg/kg initial oral dose, followed Most effective within 16 24 hr; may by 70 mg/kg every 4 hr 17 doses be useful after chronic intoxication or intravenously
Antidotes Acetaminophen N-acetylcysteine 140 mg/kg initial oral dose, followed Most effective within 16 24 hr; may by 70 mg/kg every 4 hr 17 doses be useful after chronic intoxication or intravenously
Poison (Toxicant): any substance or agent capable of producing a deleterious response in a biological system or living organism.
: any substance or agent capable of producing a deleterious response in a biological system or living organism.") Poison (Toxicant): any substance or agent capable of producing a deleterious response in a biological system or living organism. Poisoning= overdose toxicity intoxication= toxicity due to foreign substance
Poison (Toxicant): any substance or agent capable of producing a deleterious response in a biological system or living organism. Poisoning= overdose toxicity intoxication= toxicity due to foreign substance
INTRODUCTION OBJECTIVES. When the student has finished this module, he/she will be able to:
 Care of the Poisoned Patient WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A.,
Care of the Poisoned Patient WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A.,
POISONING AND DRUG OVERDOSAGE
 POISONING AND DRUG OVERDOSAGE Department of Internal Medicine WAN Weiguo General Info All chemicals have potential to be poisons if given a large enough dose Poisoning occurs when exposure to a substance
POISONING AND DRUG OVERDOSAGE Department of Internal Medicine WAN Weiguo General Info All chemicals have potential to be poisons if given a large enough dose Poisoning occurs when exposure to a substance
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
Antidotes in acute intoxications P. De Paepe and W. Buylaert - 25/08/2007
 Antidotes in acute intoxications Antidotes: warnings Antidotes are only one aspect of treatment In case of uncommon antidotes: seek expert advice These slides only discuss the general principles, not the
Antidotes in acute intoxications Antidotes: warnings Antidotes are only one aspect of treatment In case of uncommon antidotes: seek expert advice These slides only discuss the general principles, not the
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
2/1/2013. Anti dos and don ts: Pearls and pitfalls in the use of antidotes. The first rule of surfing... The ABC s of the poisoned patient
 According to the American Academy of Poison Control Centers, what is the most common intervention performed in the management of acutely poisoned patients? Anti dos and don ts: Pearls and pitfalls in the
According to the American Academy of Poison Control Centers, what is the most common intervention performed in the management of acutely poisoned patients? Anti dos and don ts: Pearls and pitfalls in the
Toxicology General Approach to the Poisoned Patient James Sinex, MD., FACEP
 General Approach to the Poisoned Patient James Sinex, MD., FACEP Definition of Terms Poisoning can be defined as exposure to a chemical or other agent that adversely affects functioning of an organism.
General Approach to the Poisoned Patient James Sinex, MD., FACEP Definition of Terms Poisoning can be defined as exposure to a chemical or other agent that adversely affects functioning of an organism.
Welcome Applicants! FRIDAY, OCTOBER 24
 Welcome Applicants! FRIDAY, OCTOBER 24 Friday Prep A 3-year-old girl is brought to your office for re-evaluation of a fever that began 6 days ago. Her mother tells you that her daughter s temperature has
Welcome Applicants! FRIDAY, OCTOBER 24 Friday Prep A 3-year-old girl is brought to your office for re-evaluation of a fever that began 6 days ago. Her mother tells you that her daughter s temperature has
CLINICAL TOXICOLOGY. Gábor Zacher Dept. Emergency Medicine Central Military Hospital
 CLINICAL TOXICOLOGY Gábor Zacher Dept. Emergency Medicine Central Military Hospital LEARNING OBJECTIVES To understand the general principles of clinical toxicology To know general factors that influence
CLINICAL TOXICOLOGY Gábor Zacher Dept. Emergency Medicine Central Military Hospital LEARNING OBJECTIVES To understand the general principles of clinical toxicology To know general factors that influence
EMT. Chapter 19 Review
 EMT Chapter 19 Review Review 1. Which of the following questions is of LEAST pertinence for the EMT to ask a patient who intentionally overdosed on a medication? A. How much do you weigh? B. How much did
EMT Chapter 19 Review Review 1. Which of the following questions is of LEAST pertinence for the EMT to ask a patient who intentionally overdosed on a medication? A. How much do you weigh? B. How much did
PHARMACOLOGY NOTES: TOXICOLOGY
 FREE GPAT QUSTION PAPERS & GPAT NOTES AVAILABLE ON www.destinationpharmagens.com Page 1 Definition of poison. Poisoning is commonly due to ingestion but can result from injection, inhalation, or exposure
FREE GPAT QUSTION PAPERS & GPAT NOTES AVAILABLE ON www.destinationpharmagens.com Page 1 Definition of poison. Poisoning is commonly due to ingestion but can result from injection, inhalation, or exposure
Cholinesterase-inhibiting Chemicals C 1
 BASF Chemical Emergency Medical Guidelines Cholinesterase-inhibiting Chemicals C 1 Information and recommendations for doctors at hospitals/emergency departments Patients whose vomitus, skin or clothing
BASF Chemical Emergency Medical Guidelines Cholinesterase-inhibiting Chemicals C 1 Information and recommendations for doctors at hospitals/emergency departments Patients whose vomitus, skin or clothing
Yolo County Health & Human Services Agency
 Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
Yolo County Health & Human Services Agency Kristin Weivoda EMS Administrator John S. Rose, MD, FACEP Medical Director DATE: December 28, 2017 TO: Yolo County Providers and Agencies FROM: Yolo County EMS
PDP 406 CLINICAL TOXICOLOGY
 PDP 406 CLINICAL TOXICOLOGY Pharm.D Fourth Year Mr.D.Raju.M.Pharm., Lecturer INTRODUCTION It is the process of freeing of a person or object of some contaminating substance from intestine which further
PDP 406 CLINICAL TOXICOLOGY Pharm.D Fourth Year Mr.D.Raju.M.Pharm., Lecturer INTRODUCTION It is the process of freeing of a person or object of some contaminating substance from intestine which further
Updates on clinical management of recreational drug use: what s new and how do we treat it?
 Updates on clinical management of recreational drug use: what s new and how do we treat it? Matt Noble, MD MPH Oregon Poison Center OHSU Department of Emergency Medicine Objectives Review the basic conceptual
Updates on clinical management of recreational drug use: what s new and how do we treat it? Matt Noble, MD MPH Oregon Poison Center OHSU Department of Emergency Medicine Objectives Review the basic conceptual
Episode 90 Low and Slow Poisoning
 Hyperkalemia Myxedema coma Spinal cord injury Hypothermia Episode 90 Low and Slow Poisoning With Drs. Margaret Thompson & Emily Austin Prepared by Dr. Keerat Grewal, edited by Dr. Anton Helman, Jan 2017
Hyperkalemia Myxedema coma Spinal cord injury Hypothermia Episode 90 Low and Slow Poisoning With Drs. Margaret Thompson & Emily Austin Prepared by Dr. Keerat Grewal, edited by Dr. Anton Helman, Jan 2017
The Hypotensive Poisoned Patient. Robert S. Hoffman, MD Director, NYC PCC
 The Hypotensive Poisoned Patient Robert S. Hoffman, MD Director, NYC PCC Some Definitions Hypotension = Low blood pressure Failure of macrocirculation Shock = Poor tissue perfusion Failure of microcirculation
The Hypotensive Poisoned Patient Robert S. Hoffman, MD Director, NYC PCC Some Definitions Hypotension = Low blood pressure Failure of macrocirculation Shock = Poor tissue perfusion Failure of microcirculation
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
By Dr. Magdy M. Awny. (nerve agent)
") By Dr. Magdy M. Awny (nerve agent) Pesticides Is any chemical substance or mixture of substances intended for preventing, destroying, repelling, or mitigating any pest are a group of insecticides or Organophosphorous
By Dr. Magdy M. Awny (nerve agent) Pesticides Is any chemical substance or mixture of substances intended for preventing, destroying, repelling, or mitigating any pest are a group of insecticides or Organophosphorous
Salicylates commonly cause tinnitus, deafness, nausea and vomiting (salicylism). Hyperventilation results from stimulation of respiratory centre.
. Hyperventilation results from stimulation of respiratory centre.") Aspirin poisoning CLINICAL FEATURES Salicylates commonly cause tinnitus, deafness, nausea and vomiting (salicylism). Hyperventilation results from stimulation of respiratory centre. Severe poisoning causes
Aspirin poisoning CLINICAL FEATURES Salicylates commonly cause tinnitus, deafness, nausea and vomiting (salicylism). Hyperventilation results from stimulation of respiratory centre. Severe poisoning causes
Pediatric Pearls. Shon A Remich, MD Dir. Translational Medicine Branch
 Pediatric Pearls Shon A Remich, MD Dir. Translational Medicine Branch shon.a.remich.mil@mail.mil Assumptions Limited experience Limited resources Limited time First things First Know
Pediatric Pearls Shon A Remich, MD Dir. Translational Medicine Branch shon.a.remich.mil@mail.mil Assumptions Limited experience Limited resources Limited time First things First Know
You. Let s Talk Hazmat. Clues to Hazmat
 Me You Let s Talk Hazmat Clues to Hazmat Location and Occupancy Container Shapes and Sizes Placards and Labels Markings and Colors Shipping Papers Senses CDC NIOSH Guide 1 The purpose of chemical protective
Me You Let s Talk Hazmat Clues to Hazmat Location and Occupancy Container Shapes and Sizes Placards and Labels Markings and Colors Shipping Papers Senses CDC NIOSH Guide 1 The purpose of chemical protective
Substance Abuse and Poisonings. Chapter 17
 Substance Abuse and Poisonings Chapter 17 Identifying the Patient and the Poison Poison- any substance who s chemical reaction can damage body structures or impair body functions Poisons act by changing
Substance Abuse and Poisonings Chapter 17 Identifying the Patient and the Poison Poison- any substance who s chemical reaction can damage body structures or impair body functions Poisons act by changing
Contra Costa County Emergency Medical Services Drug Reference. Indication Dosing Cautions Comments
 Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Toxicologic Emergencies. Objectives. Priorities. CAPA 2015 Annual Conference
 Toxicologic Emergencies Jed Grant, MPAS, PA-C Staff PA, Emergency Department, Mercy San Juan Medical Center, Sacramento, CA Assistant Professor, University of the Pacific PA Program, Sacramento, CA Vice
Toxicologic Emergencies Jed Grant, MPAS, PA-C Staff PA, Emergency Department, Mercy San Juan Medical Center, Sacramento, CA Assistant Professor, University of the Pacific PA Program, Sacramento, CA Vice
MICHIGAN. Table of Contents. State Protocols. Adult Treatment Protocols
 MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
Conscious Sedation Permit Evaluation. General Comments Emergency Algorithms
 General Comments Emergency Algorithms These algorithms delineate appropriate responses to the simulated emergencies listed in Article 5, Section 1043.4c of the California Code of Regulations. Each algorithm
General Comments Emergency Algorithms These algorithms delineate appropriate responses to the simulated emergencies listed in Article 5, Section 1043.4c of the California Code of Regulations. Each algorithm
99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018
 99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018 ER Admit 17 yo F reported intentional overdose handful of her mother s
99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018 ER Admit 17 yo F reported intentional overdose handful of her mother s
Medication Overdoses. By LT Jimson & Shawn Hunsberger
 Medication Overdoses By LT Jimson & Shawn Hunsberger Pharmacology Review First, some terms: Affinity - the tendency of a drug to combine with its receptor Efficacy the drugs ability to initiate biological
Medication Overdoses By LT Jimson & Shawn Hunsberger Pharmacology Review First, some terms: Affinity - the tendency of a drug to combine with its receptor Efficacy the drugs ability to initiate biological
EMS Region Medication List 2010
 EMT-B MEDICATIONS Patient Assisted Medications (PAM) and Ambulance Stock Medications Medication Protocol/Use Dose Auto-injector (Epi-pen) Glucose (Oral) Metered-Dose Inhaler (MDI) Allergic/Anaphylactic
EMT-B MEDICATIONS Patient Assisted Medications (PAM) and Ambulance Stock Medications Medication Protocol/Use Dose Auto-injector (Epi-pen) Glucose (Oral) Metered-Dose Inhaler (MDI) Allergic/Anaphylactic
CRACKCast Episode Hydrocarbons (Ch th )
") CRACKCast Episode Hydrocarbons (Ch. 152 9 th ) Episode Overview Key Concepts: Aspiration is the major toxic risk of hydrocarbon poisoning. Hydrocarbons may cause systemic toxicity, burns, seizures, cardiac
CRACKCast Episode Hydrocarbons (Ch. 152 9 th ) Episode Overview Key Concepts: Aspiration is the major toxic risk of hydrocarbon poisoning. Hydrocarbons may cause systemic toxicity, burns, seizures, cardiac
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
General Anesthesia. Mohamed A. Yaseen
 General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
General Anesthesia Mohamed A. Yaseen M.S,c Surgery Before Anesthesia General Anesthesia ( GA ) Drug induced absence of perception of all sensation allowing surgery or other painful procedure to be carried
1/29/2014. Objectives. The unstable overdose patient. Unstable overdose case #1. Outline
 Objectives The unstable overdose patient Craig Smollin MD Associate Medical Director California Poison Control Center, SF Division Discuss clinical scenarios unique to the acutely poisoned patient and
Objectives The unstable overdose patient Craig Smollin MD Associate Medical Director California Poison Control Center, SF Division Discuss clinical scenarios unique to the acutely poisoned patient and
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Toxicologic Emergencies
 INTRODUCTION Poisoning from drugs, chemicals, or exposure is a major cause of morbidity and mortality worldwide, and is the leading cause of non-traumatic cardiac arrest under the age of 35. Poisoning
INTRODUCTION Poisoning from drugs, chemicals, or exposure is a major cause of morbidity and mortality worldwide, and is the leading cause of non-traumatic cardiac arrest under the age of 35. Poisoning
Intermediate Medications. Epinephrine cardiac Epinephrine anaphylaxis Dextrose Atropine Narcan Thiamine Albuterol
 Intermediate Medications Epinephrine cardiac Epinephrine anaphylaxis Dextrose Atropine Narcan Thiamine Albuterol Needle Handling Precautions Minimize the tasks performed in a moving ambulance Balance the
Intermediate Medications Epinephrine cardiac Epinephrine anaphylaxis Dextrose Atropine Narcan Thiamine Albuterol Needle Handling Precautions Minimize the tasks performed in a moving ambulance Balance the
GENERAL MANAGEMENT OF POISONED PATIENTS: INTRODUCTION
 Print Close Window Note: Large images and tables on this page may necessitate printing in landscape mode. Copyright The McGraw-Hill Companies. All rights reserved. Tintinalli's Emergency Medicine > Chapter
Print Close Window Note: Large images and tables on this page may necessitate printing in landscape mode. Copyright The McGraw-Hill Companies. All rights reserved. Tintinalli's Emergency Medicine > Chapter
Change in Practice PCP Autonomous IV OBHG Education Subcommittee
 Change in Practice PCP Autonomous IV Intravenous and Fluid Therapy Medical Directive Auxiliary Ability to initiate IV access and Ability to administer fluid and fluid boluses in general IV Therapy Actual
Change in Practice PCP Autonomous IV Intravenous and Fluid Therapy Medical Directive Auxiliary Ability to initiate IV access and Ability to administer fluid and fluid boluses in general IV Therapy Actual
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
2
 1 2 3 4 5 6 7 8 Please check regional policy on Tetracaine and Morgan Lens this may be optional in your region. *Ketamine and Fentanyl must be added to your controlled substance license if required by
1 2 3 4 5 6 7 8 Please check regional policy on Tetracaine and Morgan Lens this may be optional in your region. *Ketamine and Fentanyl must be added to your controlled substance license if required by
Cardiotoxic Medications
 Cardiotoxic Medications Dean Olsen, DO Faculty, New York City Poison Control Center Director Emergency Medicine Residency Nassau University Medical Center Assistant Professor Pharmacology, Toxicology New
Cardiotoxic Medications Dean Olsen, DO Faculty, New York City Poison Control Center Director Emergency Medicine Residency Nassau University Medical Center Assistant Professor Pharmacology, Toxicology New
Prehospital Resuscitation for the 21 st Century Simulation Case. VF/Asystole
 Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Prehospital Resuscitation for the 21 st Century Simulation Case VF/Asystole Case History 1 (hypovolemic cardiac arrest secondary to massive upper GI bleed) 56 year-old male patient who fainted in the presence
Salicylate (Aspirin) Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes
 Ingestion California Poison Control Background 1. The prevalence of aspirin-containing analgesic products makes") Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
Salicylate (Aspirin) Ingestion California Poison Control 1-800-876-4766 Background 1. The prevalence of aspirin-containing analgesic products makes these agents, found in virtually every household, common
1 Chapter 19 Toxicology 2 Introduction Each day, we come into contact with things that are potentially poisonous. Acute poisoning affects 5 million
 1 Chapter 19 Toxicology 2 Introduction Each day, we come into contact with things that are potentially poisonous. Acute poisoning affects 5 million people each year. Chronic is much more common. Caused
1 Chapter 19 Toxicology 2 Introduction Each day, we come into contact with things that are potentially poisonous. Acute poisoning affects 5 million people each year. Chronic is much more common. Caused
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
PARACOD Tablets (Paracetamol + Codeine phosphate)
") Published on: 22 Sep 2014 PARACOD Tablets (Paracetamol + Codeine phosphate) Composition PARACOD Tablets Each effervescent tablet contains: Paracetamol IP...650 mg Codeine Phosphate IP... 30 mg Dosage Form/s
Published on: 22 Sep 2014 PARACOD Tablets (Paracetamol + Codeine phosphate) Composition PARACOD Tablets Each effervescent tablet contains: Paracetamol IP...650 mg Codeine Phosphate IP... 30 mg Dosage Form/s
EM Cases Course 2017 Toxicology Module
 EM Cases Course 2017 Toxicology Module quick IV access and diazepam is administered. The seizure stops. The first set of vitals show: HR 30bpm, BP 70/40. His ECG is shown below. Margaret Thompson & JP
EM Cases Course 2017 Toxicology Module quick IV access and diazepam is administered. The seizure stops. The first set of vitals show: HR 30bpm, BP 70/40. His ECG is shown below. Margaret Thompson & JP
Notes on Antidotes Insulin/Glucose for CCB overdose
 Overview Notes on Antidotes for CCB overdose for cyanide poisoning Rob Gair, BSc (Pharm), CSPI CSHP Spring Therapeutics Update April 23, 2009 Lipid rescue for local anesthetic toxicity BC Drug & Poison
Overview Notes on Antidotes for CCB overdose for cyanide poisoning Rob Gair, BSc (Pharm), CSPI CSHP Spring Therapeutics Update April 23, 2009 Lipid rescue for local anesthetic toxicity BC Drug & Poison
Pediatric Toxicologic Emergencies
 Pediatric Toxicologic Emergencies Martin Belson, MD Department of Pediatrics Georgia Poison Center Emory University I. Epidemiology A. Over 2 million poison exposures reported in 2003 B. 53% of these exposures
Pediatric Toxicologic Emergencies Martin Belson, MD Department of Pediatrics Georgia Poison Center Emory University I. Epidemiology A. Over 2 million poison exposures reported in 2003 B. 53% of these exposures
Chapter 19 Toxicology Introduction Definitions Consider Poisoning In Patients With: Identifying the Patient and the Poison
 1 2 3 4 5 Chapter 19 Toxicology Introduction Each day, we come into contact with things that are potentially poisonous. Acute poisoning affects 5 million people each year. Chronic is much more common.
1 2 3 4 5 Chapter 19 Toxicology Introduction Each day, we come into contact with things that are potentially poisonous. Acute poisoning affects 5 million people each year. Chronic is much more common.
ABAT STUDY GUIDE - LIST OF EXAM TOPICS
 ABAT STUDY GUIDE - LIST OF EXAM TOPICS The attached list of topics provides some direction as to what types of topics are usually tested. While this list may seem exhaustive, it truly reflects the wide
ABAT STUDY GUIDE - LIST OF EXAM TOPICS The attached list of topics provides some direction as to what types of topics are usually tested. While this list may seem exhaustive, it truly reflects the wide
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
2
 1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
SUMMARY OF PRODUCT CHARACTERISTICS 2. QUALITATIVE AND QUANTITATIVE COMPOSITION
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Charcodote 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Activated charcoal 200mg/ml 3. PHARMACEUTICAL FORM Oral suspension 4. CLINICAL
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Charcodote 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Activated charcoal 200mg/ml 3. PHARMACEUTICAL FORM Oral suspension 4. CLINICAL
ECMO for treatment of cardiotoxic intoxications
 ECMO for treatment of cardiotoxic intoxications Bruno Mégarbane, MD, PhD Medical and Toxicological Critical Care Department Lariboisiere Hospital, INSERM UMRS-1144, Paris-Diderot University Paris France
ECMO for treatment of cardiotoxic intoxications Bruno Mégarbane, MD, PhD Medical and Toxicological Critical Care Department Lariboisiere Hospital, INSERM UMRS-1144, Paris-Diderot University Paris France
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
Parasympathetic Nervous System Part I
 Parasympathetic Nervous System Part I Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828 2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia
Parasympathetic Nervous System Part I Edward JN Ishac, Ph.D. Professor Smith Building, Room 742 eishac@vcu.edu 828 2127 Department of Pharmacology and Toxicology Medical College of Virginia Campus of Virginia
Neither activated charcoal nor whole bowel irrigation (WBI) is indicated in the routine management of acute or chronic lithium toxicity.
 is indicated in the routine management of acute or chronic lithium toxicity.") CRACKCast E160 Lithium Key concepts; The clinical pattern of acute and chronic toxicity is different. Gastrointestinal symptoms occur early and neurological toxicity manifest late in acute toxicity. Neurological
CRACKCast E160 Lithium Key concepts; The clinical pattern of acute and chronic toxicity is different. Gastrointestinal symptoms occur early and neurological toxicity manifest late in acute toxicity. Neurological
A Primer on Chemical Nerve Agents. Information for Public Health and EMS Workers
 A Primer on Chemical Nerve Agents Information for Public Health and EMS Workers This information was adapted and developed from a presentation by: Area Health Education Center of Southern Nevada 2 Chemical
A Primer on Chemical Nerve Agents Information for Public Health and EMS Workers This information was adapted and developed from a presentation by: Area Health Education Center of Southern Nevada 2 Chemical
Caring for the Poisoned Patient
 #34442 Caring for the Poisoned Patient COURSE #34442 5 CONTACT HOURS Release Date: 04/01/18 Expiration Date: 03/31/21 Caring for the Poisoned Patient HOW TO RECEIVE CREDIT Read the enclosed course. Complete
#34442 Caring for the Poisoned Patient COURSE #34442 5 CONTACT HOURS Release Date: 04/01/18 Expiration Date: 03/31/21 Caring for the Poisoned Patient HOW TO RECEIVE CREDIT Read the enclosed course. Complete
Protocol for Angiotensin converting enzyme inhibitors (ACEIs) poisoning management
 poisoning management") Protocol for Angiotensin converting enzyme inhibitors (ACEIs) poisoning management Category/Use Treatment of hypertension, congestive heart failure (CHF), diabetic nephropathy, and post myocardial infarction
Protocol for Angiotensin converting enzyme inhibitors (ACEIs) poisoning management Category/Use Treatment of hypertension, congestive heart failure (CHF), diabetic nephropathy, and post myocardial infarction
Chapter 23 Outline. Chapter 23: Emergency Drugs. General Measures. Categories of Emergencies. Preparation for Treatment 12/12/2011.
 Chapter 23 Outline Chapter 23: Emergency General measures Categories of emergencies Emergency kit for the dental office Emergency 2 Emergency General Measures Haveles (p. 290) Haveles (pp. 290-291) (Boxes
Chapter 23 Outline Chapter 23: Emergency General measures Categories of emergencies Emergency kit for the dental office Emergency 2 Emergency General Measures Haveles (p. 290) Haveles (pp. 290-291) (Boxes
Dancing with Death: MDMA, PMMA and other 4 letter words
 Dancing with Death: MDMA, PMMA and other 4 letter words Mark Yarema, MD FRCPC Poison and Drug Information Service Alberta Health Services AARC Community Intervention Series March 15, 2016 Objectives At
Dancing with Death: MDMA, PMMA and other 4 letter words Mark Yarema, MD FRCPC Poison and Drug Information Service Alberta Health Services AARC Community Intervention Series March 15, 2016 Objectives At
2/1/2013. Poisoning pitfalls. The original pitfall
 The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
SALICYLATES. Anthony F. Pizon, M.D. Associate Professor Division Medical Toxicology University of Pittsburgh School of Medicine
 SALICYLATES Anthony F. Pizon, M.D. Associate Professor Division Medical Toxicology University of Pittsburgh School of Medicine Overview: Salicylates Found in Willow bark (Salix alba vulgaris) Widely used
SALICYLATES Anthony F. Pizon, M.D. Associate Professor Division Medical Toxicology University of Pittsburgh School of Medicine Overview: Salicylates Found in Willow bark (Salix alba vulgaris) Widely used
Cholinergic receptors( cholinoceptors ) are two families muscarinic and nicotinic depending on their affinities to cholinomimetic agents(agents that
 are two families muscarinic and nicotinic depending on their affinities to cholinomimetic agents(agents that") Cholinergic drugs Cholinergic drugs Are drugs act on receptors that are activated by acetylcholine(ach) which is the neurotransmitter of the parasympathetic nervous system. ACH is synthesized in the cholinergic
Cholinergic drugs Cholinergic drugs Are drugs act on receptors that are activated by acetylcholine(ach) which is the neurotransmitter of the parasympathetic nervous system. ACH is synthesized in the cholinergic
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8061.19 PROGRAM DOCUMENT: Initial Date: 10/26/94 Decreased Sensorium Last Approved Date: 05/01/17 Effective Date: 05/01/19 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8061.19 PROGRAM DOCUMENT: Initial Date: 10/26/94 Decreased Sensorium Last Approved Date: 05/01/17 Effective Date: 05/01/19 Next Review
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Methamphetamine Abuse During Pregnancy
 Methamphetamine Abuse During Pregnancy Robert Davis, MD / r.w.davismd@gmail.com ❶ Statistics ❷ Pregnancy Concerns ❸ Postpartum Concerns ❹ Basic Science ❺ Best Practice Guidelines ❻ Withdrawal ❼ Recovery
Methamphetamine Abuse During Pregnancy Robert Davis, MD / r.w.davismd@gmail.com ❶ Statistics ❷ Pregnancy Concerns ❸ Postpartum Concerns ❹ Basic Science ❺ Best Practice Guidelines ❻ Withdrawal ❼ Recovery
Prevention and Treatment Patrick Levelle, MD
 Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
Update in Poison Management. Update in Poison Management. Antidote Use. Fomepizole. Pediatric Ingestions 1. No financial disclosures
 Update in Poison Management No financial disclosures Robert J. Hoffman, MD,MS FACMT, FACEP, FAAEM, FAAP Department of Emergency Medicine Albert Einstein College of Medicine New York, New York Update in
Update in Poison Management No financial disclosures Robert J. Hoffman, MD,MS FACMT, FACEP, FAAEM, FAAP Department of Emergency Medicine Albert Einstein College of Medicine New York, New York Update in
Opioid Overdose Best Practices Guideline. Table of Contents. A. General description: B: Typical signs and symptoms:
 Opioid Overdose Best Practices Guideline Table of Contents A. General description B. Typical signs and symptoms C. Expected course D. Making the diagnosis E. Recommended treatment F. Criteria for hospital
Opioid Overdose Best Practices Guideline Table of Contents A. General description B. Typical signs and symptoms C. Expected course D. Making the diagnosis E. Recommended treatment F. Criteria for hospital
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL
 CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
CALL US...TM. Anticholinesterase (Organic Phosphorus and Carbamate) Pesticide Poisoning
 Pesticide Poisoning") CALL US...TM The Official Newsletter of the California Poison Control System Volume 6, Number 2 Summer 2008 Anticholinesterase (Organic Phosphorus and Carbamate) Pesticide Poisoning Introduction Organic
CALL US...TM The Official Newsletter of the California Poison Control System Volume 6, Number 2 Summer 2008 Anticholinesterase (Organic Phosphorus and Carbamate) Pesticide Poisoning Introduction Organic
Oral poisoning: an update
 : an update Catherine Ward MBBS BSc Hons FRCA Mark Sair PhD MRCP FRCA Key points The mainstay treatment of poisoning is resuscitation and supportive care. Poisoning should be considered in any patient
: an update Catherine Ward MBBS BSc Hons FRCA Mark Sair PhD MRCP FRCA Key points The mainstay treatment of poisoning is resuscitation and supportive care. Poisoning should be considered in any patient
Ah S%#T!!! Deadly Overdoses That Die En Route. Jamie Syrett, MD Office of Prehospital Care Rochester General Health System
 Ah S%#T!!! Deadly Overdoses That Die En Route Jamie Syrett, MD Office of Prehospital Care Rochester General Health System Case 1 (and 2) Male - mid 30s, pulled from a burning building by a fire-fighter
Ah S%#T!!! Deadly Overdoses That Die En Route Jamie Syrett, MD Office of Prehospital Care Rochester General Health System Case 1 (and 2) Male - mid 30s, pulled from a burning building by a fire-fighter
Protocol for Iron poisoning management Category/Use: Iron supplements are used for the prevention and treatment of iron deficiency
 Protocol for Iron poisoning management Category/Use: Iron supplements are used for the prevention and treatment of iron deficiency anemia, and as a nutritional supplement to provide additional iron during
Protocol for Iron poisoning management Category/Use: Iron supplements are used for the prevention and treatment of iron deficiency anemia, and as a nutritional supplement to provide additional iron during
Nerve Agent/Organophosphate Pesticide Exposure Treatment
 Nerve Agent/Organophosphate Pesticide Exposure Treatment Purpose: This Protocol is intended for EMS personnel at all levels to assess and treat patients exposed to nerve agents and organophosphate pesticides.
Nerve Agent/Organophosphate Pesticide Exposure Treatment Purpose: This Protocol is intended for EMS personnel at all levels to assess and treat patients exposed to nerve agents and organophosphate pesticides.
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
Appendix A: Pharmacologic approaches to pain management during MVA
 Pain medication Though the medications shown below are commonly used for pain management during uterine evacuation, many other options exist. This table does not cover general anesthetic agents. Both anxiolytics
Pain medication Though the medications shown below are commonly used for pain management during uterine evacuation, many other options exist. This table does not cover general anesthetic agents. Both anxiolytics
Toxic Chemical Threats
 Toxic Chemical Threats John Devlin, MD, FACEP GA Poison Center / Emory University / Centers for Disease Control and Prevention Objectives To give you tools to help recognize what chemical agent is present
Toxic Chemical Threats John Devlin, MD, FACEP GA Poison Center / Emory University / Centers for Disease Control and Prevention Objectives To give you tools to help recognize what chemical agent is present
Weapons of Mass Destruction. Lesson Goal. Lesson Objectives 9/10/2012
 Weapons of Mass Destruction Lesson Goal To become familiarize with the concept of weapons of mass destruction (WMD), how these weapons might be used, and the type of treatment that would be appropriate
Weapons of Mass Destruction Lesson Goal To become familiarize with the concept of weapons of mass destruction (WMD), how these weapons might be used, and the type of treatment that would be appropriate
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
How effective is chelation? contrasts in iron and digoxin poisoning. Nick Bateman Edinburgh
 How effective is chelation? contrasts in iron and digoxin poisoning Nick Bateman Edinburgh Chelation Chemical chelating agents chemical that bind metal ions and other toxic groups e.g. desferrioxamine
How effective is chelation? contrasts in iron and digoxin poisoning Nick Bateman Edinburgh Chelation Chemical chelating agents chemical that bind metal ions and other toxic groups e.g. desferrioxamine
CalvertHealth Medical Center s Moderate Sedation Competency Examination
 Medical Staff Office Use Only: Congratulations! You passed the Moderate Sedation Competency Examination. Enclosed is the test for your follow-up review. Test Results: % ( of 35 correct) Your test result
Medical Staff Office Use Only: Congratulations! You passed the Moderate Sedation Competency Examination. Enclosed is the test for your follow-up review. Test Results: % ( of 35 correct) Your test result
Welcome to ACLS with Medical Education Angels!
 Welcome to ACLS with Medical Education Angels! For your greatest success, please be aware that the AHA assumes those taking ACLS have the ability to interpret and determine appropriate treatments for a
Welcome to ACLS with Medical Education Angels! For your greatest success, please be aware that the AHA assumes those taking ACLS have the ability to interpret and determine appropriate treatments for a
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Small Doses, Big Problems: Deadly Pediatric Poisons
 Small Doses, Big Problems: Deadly Pediatric Poisons Adam Algren, MD Departments of Pediatrics and Emergency Medicine Children s Mercy Hospital and Truman Medical Center Medical Director University of Kansas
Small Doses, Big Problems: Deadly Pediatric Poisons Adam Algren, MD Departments of Pediatrics and Emergency Medicine Children s Mercy Hospital and Truman Medical Center Medical Director University of Kansas
Respiratory Pharmacology. Manuel Otero Lopez Department of Anaesthetics and Intensive Care Hôpital Européen Georges Pompidou, Paris, France
 Respiratory Pharmacology Manuel Otero Lopez Department of Anaesthetics and Intensive Care Hôpital Européen Georges Pompidou, Paris, France Programme Bronchomotor tone Drugs and factors influencing airway
Respiratory Pharmacology Manuel Otero Lopez Department of Anaesthetics and Intensive Care Hôpital Européen Georges Pompidou, Paris, France Programme Bronchomotor tone Drugs and factors influencing airway
Chapter 149 Aspirin and Nonsteroidal Agents
 Chapter 149 Aspirin and Nonsteroidal Agents Episode overview: Core questions: 1. What is the pathophysiology of ASA toxicity? 2. What is the toxic dose of ASA? 3. How is aspirin eliminated from the body?
Chapter 149 Aspirin and Nonsteroidal Agents Episode overview: Core questions: 1. What is the pathophysiology of ASA toxicity? 2. What is the toxic dose of ASA? 3. How is aspirin eliminated from the body?