BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
|
|
|
- Lee Chase
- 6 years ago
- Views:
Transcription


1 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative

2 Fraser Health Guide To Person-Centered Medication Decisions
3 Factors to Consider When Systematically Reviewing Medications Goals of Care Co-Morbidities, Disease Trajectory, Functional Status, Quality of Life Stats on Benefit and Harm- Event Rates, % and NNT for Benefit, % and NNT for Harm As May Apply to: Drug Initiation Drug Maintenance Drug Discontinuation Adverse Drug Effects Remaining Life Expectancy - Time Until Benefit/Time to Lose Benefit Treatment (Management) Targets 3
4 RC Med Reviews Opportunities Occasions for Full RC Medication Reviews Scheduled Med Reviews regular, but effective? When first admitted or during admissions process Transitions e.g. from Acute/ED, Special Care Unit Goals of Care (MOST +) Review of standing orders e.g. Gravol 50mg Occasions for Focused RC Medication Reviews Addressing Polypharmacy in the Elderly Episode of decline symptom-directed, e.g. fall, delirium Request by staff e.g. behaviour, med concerns, etc Request by resident/family education opportunity
5 Medication Review- Evidence of Benefit Case-control study over 1 year, mod-severe demented Israeli facility residents on ~ 7 drugs* (Garfinkel) 2.8 drugs/patient stopped Only 18% drugs / 10% patients had the stopped meds restarted over a year Decr mortality (21 vs 45%) NNT 4.1 Decr acute care transf (12 vs 30%) NNT 5.5 This is when average stay is ~ 1 yr! * IMAJ 2009;9:
6 So, if common side effects of most medications include. Fatigue, weakness, muscle aches Anorexia, nausea, bloating, cramps, constipation, diarrhea Dizziness, postural instability Headaches 6

7 Accumulation of minor side effects leads to feeling 7
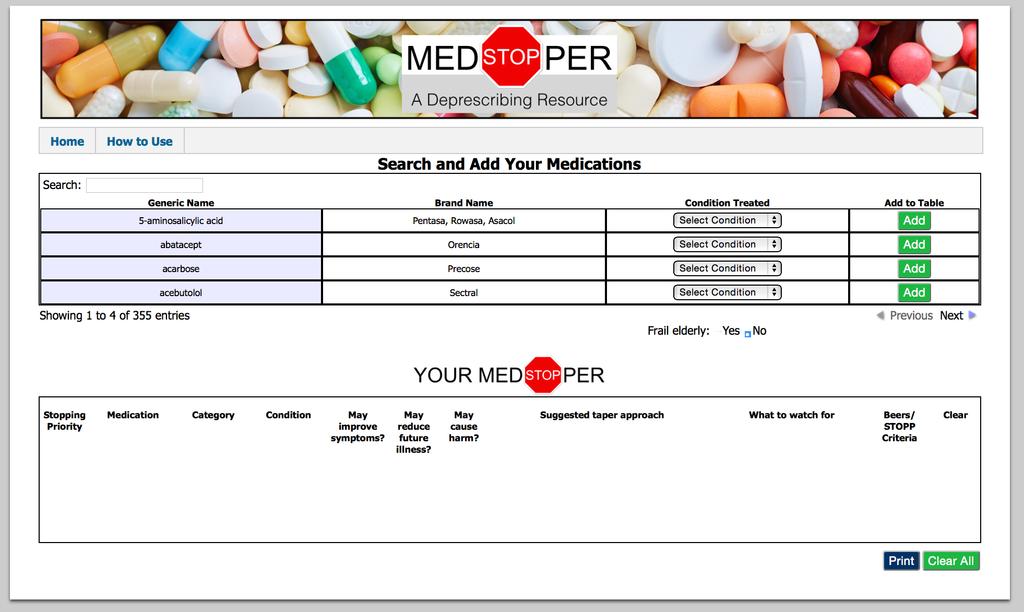
8 Tools You Decide sheets Medstopper ( Med review template (Rosenberg) 8
9 You Decide Sheets On web site ( PPIs Statins Antipsychotics In preparation: Antihypertensive medications Osteoporosis medications Depression meds with dementia -?Hypnotics
10

11 Potential Adverse Consequences of Medications with Anticholinergic Properties Can t see Can t pee Can t spit Can t sh Can t stand Can t think 11
12 Using Statistics For Decision-Making Event rates NNT/NNH % benefit and harm 12
13 13 Statins-You Decide
14
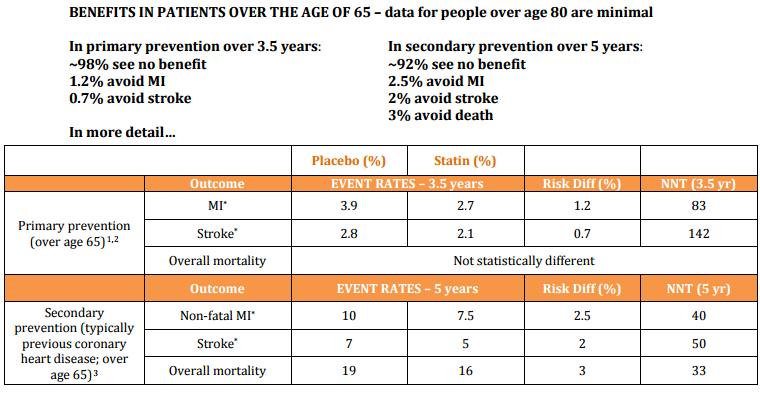
15 Statins for Primary Prevention in >65 year olds over 3.5 years Placebo Statin Risk Difference NNT MI 3.9% 2.7% 1.2% 84 Stroke 2.8% 2.1% 0.7% % avoided an MI 0.7% avoided a stroke ~98% had no benefit from the statins they took
16 Benefits of statin for primary prevention of MI % who have an MI % do not have MI regardless of tx % % do not have MI- due to tx 2.7% 0 Placebo Statin 2.7% have MI regardless of tx
17 Medstopper: 17
18

19 May improve symptoms? pain, insomnia, depression May reduce future illness? blood pressure, glucose, lipids May cause harm? relative harm Beers/ STOPP Criteria SUGGESTED TAPER APPROACH If used daily for more than 3-4 weeks. Reduce dose by 50% every 1 to 2 weeks. Once at 25% of the original dose and no withdrawal symptoms have been seen, stop the drug. If any withdrawal symptoms occur, go back to approximately 75% of the previously tolerated dose. WHAT TO WATCH FOR chest pain, pounding heart, heart rate, blood pressure (re-measure for up to 6 months), anxiety, tremor
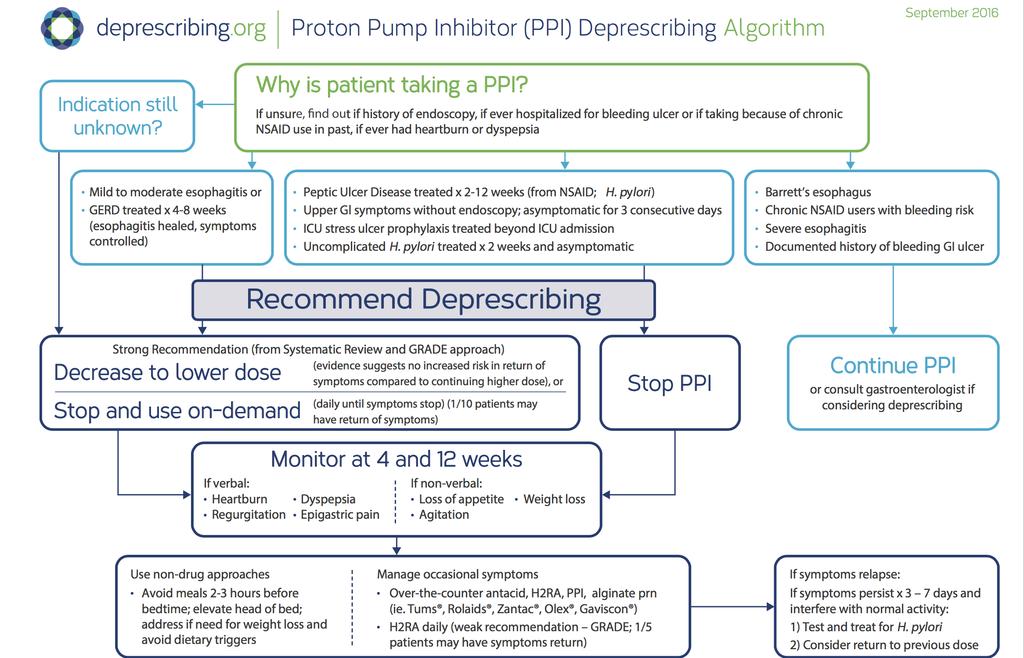
20 Deprescribing Network Algorithms Antipsychotics PPIs Benzos Antihyperglycemics
21
22
23 Set the Context in GOC - Symptoms, Function Health Care CG burden Focus on Clinical Issues/Symptoms Agents/Factors (Adapted from Template of Dr. Actions Ted Rosenberg, Victoria, BC) Monitoring Plan/Impact of Change (Adapted from Template of Dr. Ted Rosenberg,
24
25 EDNA-GOC Outcomes- Symptoms, Function Health Care CG burden Focus on Clinical Issues/Symptoms Orthostatic Hypotension Agents/Factors Actions Monitoring Plan/Impact of Change AC=Oxybutynin*, Fluoxetine + BP Meds Fall Above meds + Temazepam Reduced mobility Constipation Mild memory loss Simvastatin, Omeprazole, Alendronate Calcium*, AC- Oxybutynin, Fluoxetine CNS (Fluoxetine, Temazepam) + AC drugs: Oxybytinin, Metorpolol STOP-Oxybutynin, HCT TAPER to D/C- Metoprolol (AC), Fluvoxetine +REDUCE- Temazepam STOP- Simvastatin, Alendronate Taper to D/C- Omeprazole STOP-Calcium, Oxybutynin Taper to D/C- Fluoxetine CNS meds and, Metoprolol, Oxybutynin as above No orthostatic BP drop Feels more stable No falls Moving around better Constipation resolved Feels clearer Drug-Drug Interaction Drug cascade Prevention Ibuprofen and BP med Lactulose Aspirin STOP- Ibuprofen REVIEW-Lactulose STOP-Aspirin ONLY DRUGS LEFT: Vit D, ENALAPRIL, ACETAMINOPHEN, Monitor arthritis pain (Template developed by Dr. Ted Rosenberg, Victoria, BC)
26 Resources and Links Shared Care Polypharmacy Risk Reduction Support Thennt.com Medstopper: Anticholinergic Cognitive Burden Scale:
27
28 91 Y.O. WOMAN-MODERATE DEMENTIA: Drug Medications Indications Oxazepam 30mg - Insomnia Galantamine 16mg Dementia Risperidone 0.5mg BID Agitation/Aggression/Paranoia Citalopram 20mg Depression, irritability Felodipine 10mg HTN HCTZ 25mg TN Atorvastatin 20mg Hyperlipidemia (no IHD/CVA) Ecasa-81mg od Primary Prevention stroke and MI Metformin 1000mg BID DM Allopurinol 300mg Gouty arthritis Alendronate, Ca, Vit. D Osteoporosis Other Clinical findings BP -124/64 sitting and 106/60 standing HGB -104 ;Ferritin 30 A1C 5.5 GFR 54 Reconciliation Problems Identified at the Review - Dementia MMSE 11; Functional Review - Engages with family and will speak with some paraphrasia - will do a.m. care with standby - Toilets self - Can find and walk to common area and dining room - Still feeds self Behaviour no reported problems, some anxiety at pill time - Unsteady, Forgets to use walker - Anorexia, Poor intake, Weight loss 5 lbs. - Constipation - Edema - +3 with some stasis dermatitis - Caregiver Stress - husband and daughters exhausted Goals of Care: QofL, maintain function, control symptoms, not survival, expected life expectancy <2 years
29 GOC Outcomes- Symptoms, Function Health Care CG burden Used with permission from Dr. Ted Rosenberg, Victoria, BC Focus on Clinical Issues/Symptoms Agents/Factors Actions Monitoring Plan/Impact of Change Fall, Orthostatic BP BP meds, CNS meds Stop (taper): Felodipine, HCT; Stop: Naproxen Reduce: Citalopram 10mg OD, Respiridone 0.25mg OD, Oxazepam 7.5mg Edema BP meds Stop (taper): Felodipine, HCT Anorexia, Nausea, Swallowing, Anemia Calcium, Alendronate, Atorvastatin, ASA, Metformin, Allopurinol, Galantamine Stop: Ca, Alendronate, Atorvastatin, ASA Reduce: Metformin, Allopurinol Galantamine re-started Add Fe Gluc. BP: 146/72 Balance better, no falls Mood stable Sleeping OK Edema +1 Appetite and weight up Hb 136 Constipation Calcium Stop Calcium Less laxative Reduced GFR Naproxen Allopurinol Stop Naproxen Reduce Allopurinol Inc. GFR Pill Burden All meds As above Reduced pill burden
Polypharmacy in the Elderly
 Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
Polypharmacy in the Elderly Or How Scotland invented the Modern World Sir William Ferguson Anderson 1914-2001 Became the first Professor of Geriatrics in the world when he was appointed to the David Cargill
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Wiser Meds: Deprescribing for Older People. Dr. Rita McCracken, MD, PhD(c) Declaration of Conflicts of Interest
 Declaration of Conflicts of Interest") Wiser Meds: Deprescribing for Older People Dr. Rita McCracken, MD, PhD(c) rita.mccracken@ubc.ca / @DrRitaMc Declaration of Conflicts of Interest Faculty: Dr. Rita McCracken Relationships with commercial
Wiser Meds: Deprescribing for Older People Dr. Rita McCracken, MD, PhD(c) rita.mccracken@ubc.ca / @DrRitaMc Declaration of Conflicts of Interest Faculty: Dr. Rita McCracken Relationships with commercial
Polypharmacy and the Older Adult. Leslie Baker, PharmD, BCGP Umanga Sharma, MD
 Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Polypharmacy and the Older Adult Leslie Baker, PharmD, BCGP Umanga Sharma, MD Objectives Identify what polypharmacy is Identify factors leading to polypharmacy Discuss consequences of polypharmacy Identify
Appropriate prescribing and deprescribing for older people getting it right. Alan Davis Northland District Health Board
 Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
Appropriate prescribing and deprescribing for older people getting it right Alan Davis Northland District Health Board Unused returns Potentially inappropriate medication use in the elderly 15% of older
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018
 From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
From MCI to Dementia DR YU- MIN LIN GERIATRICIAN AUG 2018 Overview What is dementia? Common causes Normal cognitive decline Abnormal decline and mild cognitive impairment How do we manage dementia Can
Medication Reviews within Care Homes. Catherine Armstrong
 Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
Medication Reviews within Care Homes Catherine Armstrong What is a Medication Review? A structured, critical examination of a patient s medicines with the objective of reaching an agreement with the patient
PRESCRIBING IN THE ELDERLY. CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas
 PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
PRESCRIBING IN THE ELDERLY CARE HOME PHARMACY TEAM Bhavini Shah, Eleesha Pentiah & Puja Vyas LEARNING OUTCOMES Medicines Optimisation The effects of aging on health and medicines. Polypharmacy Acute Kidney
Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice. with you at every step
 Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice Objectives Review current policy and environmental issues influencing medication choices at end of life Discuss
Danielle Pierotti RN, PhD, AOCN, CHPN Chief Nurse/Director of Clinical Practice HCI Hospice Objectives Review current policy and environmental issues influencing medication choices at end of life Discuss
Deprescribing Unnecessary Medications: A Four-Part Process
 Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
Deprescribing Unnecessary Medications: A Four-Part Process Scott Endsley, MD Fam Pract Manag. 2018;25(3):28-32. Abstract and Introduction Introduction www.medscape.com Ms. Horatio is a 76-year-old patient
If a bad thing is happening to a patient, a drug did it until proven otherwise
 Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Dr Vicki s First Rule of Geriatrics Deprescribing in the Elderly Victoria Braund MD, FACP, CMD Director, Division of Geriatrics NorthShore University HealthSystem Medical Director, Brandel Health & Rehab
Meds and Falls: Keep in Step with your Meds
 Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Meds and Falls: Keep in Step with your Meds Donna Bartlett PharmD, CGP, RPh Associate Professor-Pharmacy Practice MCPHS University Clinical Pharmacist-MCPHS University- Pharmacy Outreach Program donna.bartlett@mcphs.edu
Black holes taped on floor Redirection Music and activities Yellow straps across the door Remind other residents to use call bell when she comes in
 Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Intrusive Wandering Case study........................................... A 97 year old woman with dementia lives in a mixed 23 bed LTC unit. She is independently mobile in her wheelchair and goes in and
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Repetitive Vocalizations
 Repetitive Vocalizations Case study........................................... A 77 year old woman developed a variety of behaviours after a diagnosis of Pott s Puffy Tumor (frontal lobe) in April 2015.
Repetitive Vocalizations Case study........................................... A 77 year old woman developed a variety of behaviours after a diagnosis of Pott s Puffy Tumor (frontal lobe) in April 2015.
Mucky Meds: A (practical) approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP
 approach the nightmare med list. Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP") Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Mucky Meds: A (practical) approach the nightmare med list Michelle Gibson, MD, CCFP (COE), FCFP and Erin Beattie, MD, CCFP Faculty/Presenter Disclosure Faculty: Michelle Gibson Relationships with financial
Residents Who Don t Sleep
 Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Residents Who Don t Sleep Case study........................................... An 86 yr. old woman has diagnoses of Alzheimer s disease, congestive heart failure, constipation, depression, hypertension
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks
 Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Polypharmacy and Polymorbid Patients: Practical Tips and Tricks November 2, 2013 Faculty/Presenter Disclosure Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine Clinical Practice
Driving and Dementia Case Study
 Driving and Dementia Case Study Review the following case study one section at a time, responding to the questions posed following the information provided. Expert opinion about how to respond to the case
Driving and Dementia Case Study Review the following case study one section at a time, responding to the questions posed following the information provided. Expert opinion about how to respond to the case
Pharmaceutical Interventions. Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007
 Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Pharmaceutical Interventions Collaborative Model of Mental Health Care for Older Iowans Des Moines May 18, 2007 Outline Overview Overview of initial workup and decisions in elderly depressed individual
Reviewing Medicines in at risk patients care homes
 Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Reviewing Medicines in at risk patients care homes Clinical Medication Reviews by Pharmacists in Collaboration with GP Surgeries across Brighton and Hove CCG Liz Butterfield FRPharmS 19th April 2016 NICE:
Polypharmacy, Medication Nihilism, and the art of de-prescribing
 Polypharmacy, Medication Nihilism, and the art of de-prescribing Temple Family Practice Review Course Leon S. Kraybill, MD, CMD Geriatrics, Lancaster General Hospital Physicians Division Chief, LGH Division
Polypharmacy, Medication Nihilism, and the art of de-prescribing Temple Family Practice Review Course Leon S. Kraybill, MD, CMD Geriatrics, Lancaster General Hospital Physicians Division Chief, LGH Division
Resident Assessment Best Practices M E G A N M. G R A E S E R, D N P, G N P - BC P H Y S I C I A N H O U S E C A L L S, L L C
 Resident Assessment Best Practices M E G A N M. G R A E S E R, D N P, G N P - BC P H Y S I C I A N H O U S E C A L L S, L L C Who are you assessing? Elders that needing to make a transition in their care
Resident Assessment Best Practices M E G A N M. G R A E S E R, D N P, G N P - BC P H Y S I C I A N H O U S E C A L L S, L L C Who are you assessing? Elders that needing to make a transition in their care
Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY
 Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY Panel Moderator & Panelists: Edward Perrin, MD Banner icare Scott Bolhack, MD, MBA Sandra Brownstein, PharmD Paige Hector,
Case Study #1 GUIDING PRINCIPLES FOR THE CARE OF OLDER ADULTS WITH MULTIMORBIDITY Panel Moderator & Panelists: Edward Perrin, MD Banner icare Scott Bolhack, MD, MBA Sandra Brownstein, PharmD Paige Hector,
Polypharmacy and Deprescribing for Older People
 Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Polypharmacy and Deprescribing for Older People Sarah Hilmer Head of Department, Clinical Pharmacology and Senior Staff Specialist Aged Care, RNSH Conjoint Professor of Geriatric Pharmacology, Sydney University
Geriatric Pharmacology
 Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
Geriatric Pharmacology Janice Scheufler R.Ph.,PharmD, FASCP Clinical Pharmacist Hospice of the Western Reserve Objectives List three risk factors for adverse drug events in the elderly Discuss two physiological
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION. Building Partnerships for Successful Aging
 MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
Adjusting and Withdrawing Medications in the Elderly
 Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
Adjusting and Withdrawing Medications in the Elderly Louise Mallet, B.Sc.Pharm., Pharm.D., CGP Professor in Clinical Pharmacy, Faculty of Pharmacy, University of Montreal Clinical Pharmacist in Geriatrics,
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future
 DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
DRUG THERAPY CHOICES FOR THE DEMENTED PATIENT Past, Present and Future Daniel S. Sitar Professor Emeritus University of Manitoba Email: Daniel.Sitar@umanitoba.ca March 6, 2018 INTRODUCTION EPIDEMIOLOGY
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic
 Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams
 Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Early Intervention the Key to Geriatric Assessment: Geriatric Assessment Outreach Teams Regional Geriatric Program of Eastern Ontario Outpatient Clinics Geriatric Rehabilitation Unit Community Referrals
Polypharmacy: A Rational Evidence-informed Approach with a Touch of Common Sense
 Polypharmacy: A Rational Evidence-informed Approach with a Touch of Common Sense KEEP CALM BECAUSE LESS IS MORE James McCormack B.Sc. (Pharm), Pharm.D. Professor Faculty of Pharmaceutical Sciences University
Polypharmacy: A Rational Evidence-informed Approach with a Touch of Common Sense KEEP CALM BECAUSE LESS IS MORE James McCormack B.Sc. (Pharm), Pharm.D. Professor Faculty of Pharmaceutical Sciences University
Great Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association
 Great Care @ Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association Principles Best interest of the patient (SNF) and resident (NF) comes first. Lowest cost to achieve the same care.
Great Care @ Low Cost in SNF-NF Jabbar Fazeli, MD Maine Medical Directors Association Principles Best interest of the patient (SNF) and resident (NF) comes first. Lowest cost to achieve the same care.
Case Studies in T2DM A Comprehensive Management Approach
 Case Studies in T2DM A Comprehensive Management Approach John E. Anderson, MD The Frist Clinic Nashville, TN 43 yo Latina woman with 5 yrs T2DM. Originally diagnosed with PCOS and IGT by GYN at 32 yo.
Case Studies in T2DM A Comprehensive Management Approach John E. Anderson, MD The Frist Clinic Nashville, TN 43 yo Latina woman with 5 yrs T2DM. Originally diagnosed with PCOS and IGT by GYN at 32 yo.
Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii
 Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Individualized Diabetes Treatment for the Elderly Jennifer Loh, MD, FACE Chief of Endocrinology KP Hawaii AAMD of Medical Education, KP Hawaii Extremely Relevant Baby Boomers are aging! ¼ of people age
Public Dissemination Effective: January 2018
 Board of Pharmacy Specialties Board Certified Geriatric Pharmacist (BCGP) Detailed Content Outline 1. GENERAL PRINCIPLES OF AGING (20%) A. Apply the knowledge of physiologic changes associated with aging
Board of Pharmacy Specialties Board Certified Geriatric Pharmacist (BCGP) Detailed Content Outline 1. GENERAL PRINCIPLES OF AGING (20%) A. Apply the knowledge of physiologic changes associated with aging
Polypharmacy and Elders. Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging
 Polypharmacy and Elders Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging Prescription Medication Use In Elders 1 13% of the US population is age 65+ Age 65 years 13% Age 65+ account for 34% of
Polypharmacy and Elders Leslie Baker, Pharm. D., RPh, CGP Sanford Center for Aging Prescription Medication Use In Elders 1 13% of the US population is age 65+ Age 65 years 13% Age 65+ account for 34% of
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018
 Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
Transitions of Care & Medication Reconciliation Ashley King, PharmD, BCGP Clinical Pharmacist LECOM Health March 2018 Objectives Identify when to complete medication reconciliation Understand the importance
The Geriatrician in the Trauma Service. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013
 Annual Scientific Meeting and Training 2013") The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
The Geriatrician in the Trauma Service Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2013 Challenges of the Geriatric Trauma Patient Challenges of the Geriatric Patient
Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital. November /20/ Safety: Falls/Cooking/Unsafe Behaviour. 2.
 How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
How To Decide if an Elderly Person Can Stay at Home: The Interval of Need Concept Dr. W. Dalziel Professor, Geriatric Medicine Ottawa Hospital November 2013 3 Factors 1. Safety: Falls/Cooking/Unsafe Behaviour
Managing medicines in older people. Jane Noble and Caroline Ralph
 Managing medicines in older people Jane Noble and Caroline Ralph Where? Community Hospital Care Home What? Prescribing Dispensing Administering Case 1 84 year old lady Admitted with reduced mobility Recurrent
Managing medicines in older people Jane Noble and Caroline Ralph Where? Community Hospital Care Home What? Prescribing Dispensing Administering Case 1 84 year old lady Admitted with reduced mobility Recurrent
:{ic0fp'16. Geriatric Medicine: Optimal Heart Health Amid Changing Guidelines. (and the Evidence for When to Stray) Kevin Overbeck, DO
 Kevin Overbeck, DO") :{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Optimal Heart Health Amid Changing Guidelines (and the Evidence for When to Stray) Kevin Overbeck, DO Optimal Heart Health
:{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Optimal Heart Health Amid Changing Guidelines (and the Evidence for When to Stray) Kevin Overbeck, DO Optimal Heart Health
Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD
 2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
2016 Deprescribing in CKD patients: Is less more? Speaker: Dr. Judith G. Marin, PharmD Case Mr. Kid Ney is a 75 y/o patient who has been on dialysis for the last 4 years (PD, then HD). PMHx: HTN, DM,
The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability
 with Learning Disability") The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability Danielle Adams Principal Clinical Pharmacist Pharmacy and Medicines Optimisation Team HPFT July 2017 1
The Deprescribing of Psychotropic Medication in Service Users (Patients) with Learning Disability Danielle Adams Principal Clinical Pharmacist Pharmacy and Medicines Optimisation Team HPFT July 2017 1
Polypharmacy: Guidance for Prescribing Figure 2: A Practical Guide to Stopping Medication in the Elderly
 Polypharmacy: Guidance for Prescribing Figure 2: A Practical Guide to Stopping Medication in the Elderly July 2014 This guidance has been prepared by Emyr Jones, Macmillan Palliative Care Pharmacist, Aneurin
Polypharmacy: Guidance for Prescribing Figure 2: A Practical Guide to Stopping Medication in the Elderly July 2014 This guidance has been prepared by Emyr Jones, Macmillan Palliative Care Pharmacist, Aneurin
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Managing Polypharmacy in the Elderly March 21, Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital
 Managing Polypharmacy in the Elderly March 21, 2012 Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital Objectives Participants will be able to: Describe the impact of polypharmacy
Managing Polypharmacy in the Elderly March 21, 2012 Barbara Farrell BScPhm, PharmD, FCSHP Pharmacist, Bruyère Geriatric Day Hospital Objectives Participants will be able to: Describe the impact of polypharmacy
Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial
 Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
Dr Kyra Neubauer Define frailty Recognise the consequences of frailty Know why CGA important and what are the main components of a CGA that can be done in an initial assessment Understand what are potential
STOPP and START criteria October 2011
 # START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
# START and STOPP are newer criteria to identify potentially inappropriate medications in elderly, including drug drug and drug disease interactions, drugs which increase risk of falls and drugs which
Falls most commonly seen in RACFs are due to tripping, slipping and stumbling (21.6%). Falling down stairs is relatively uncommon in
. Falling down stairs is relatively uncommon in") This Presentation Medications and Falls Dr Peter Tenni M Pharm (Curtin), PhD (UTAS) AACPA Director, CPS A fall is an event which results in a person coming to rest inadvertently on the ground or floor
This Presentation Medications and Falls Dr Peter Tenni M Pharm (Curtin), PhD (UTAS) AACPA Director, CPS A fall is an event which results in a person coming to rest inadvertently on the ground or floor
Medications and the I/DD Population
 Medications and the I/DD Population A Supplemental Document to Session 4 in Webinar Series ADR Symptoms that Mimic Age Related/Associated Changes and Diseases Biological Changes Impaired senses Cardiovascular
Medications and the I/DD Population A Supplemental Document to Session 4 in Webinar Series ADR Symptoms that Mimic Age Related/Associated Changes and Diseases Biological Changes Impaired senses Cardiovascular
Talking to patients with osteoporosis about initiating therapy
 Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK
 COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
COMMON DRUG RELATED PROBLEMS SEEN IN PACE AND MECHANISMS TO MITIGATE RISK Robert L Alesiani, PharmD, CGP Chief Pharmacotherapy Officer CareKinesis, Inc. (a Tabula Rasa Healthcare Company) 2 3 4 5 Pharmacogenomics
The future is here. It s just not widely distributed yet. William Gibson
 The future is here. It s just not widely distributed yet. William Gibson CHRONIC KIDNEY DISEASE MANAGEMENT A NEW PARADIGM Aaron Cass, MD, FRCPC Nephrologist, Fraser Health January 22, 2014 Where Are We
The future is here. It s just not widely distributed yet. William Gibson CHRONIC KIDNEY DISEASE MANAGEMENT A NEW PARADIGM Aaron Cass, MD, FRCPC Nephrologist, Fraser Health January 22, 2014 Where Are We
Falls Prevention Best Practice
 Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Falls Prevention Best Practice Prepared by Denise Tomassini Falls Prevention A case study : Mr Tony Topples ISLHD Clinical Quality Manager Clinical Governance Unit November 2011 Falls Prevention Best Practice
Basics of Benzodiazepine Use Disorder. DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Basics of Benzodiazepine Use Disorder DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Deprescribing with Confidence Dr Sanjay Suman MD FRCP
 Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
Deprescribing with Confidence Dr Sanjay Suman MD FRCP Clinical Director Elderly Care and Stroke Medway NHS Foundation Trust Kent 45% of all medications prescribed for 65 years 1 1. Wynne et al Maturitas
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
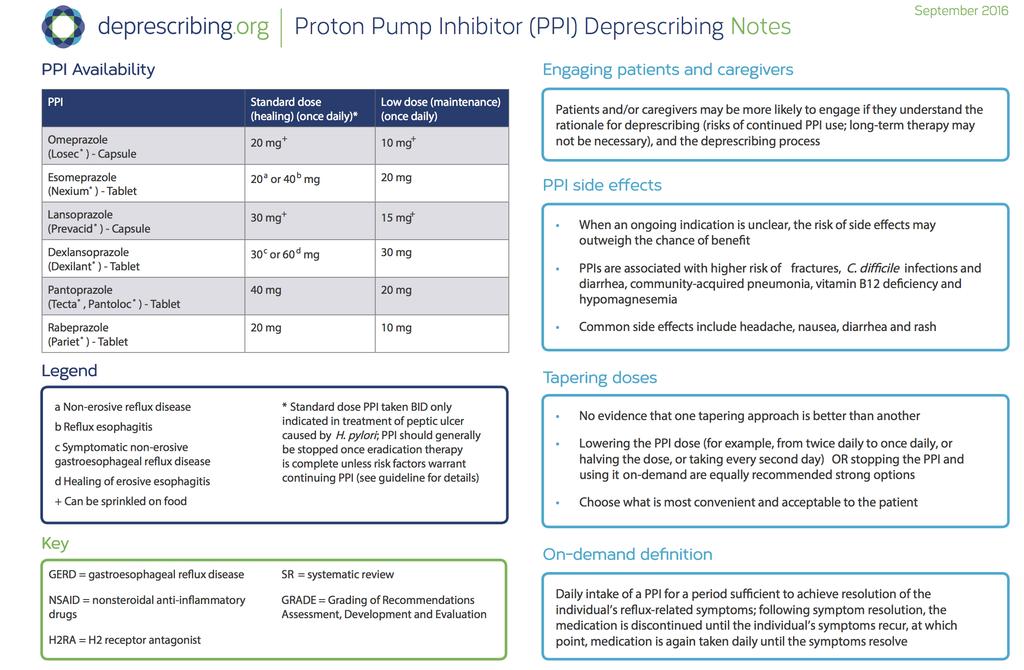
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
Overview of Psychoactive Drug use
 Overview of Psychoactive Drug use By Dr. Oladosu Ahmed Kayode Specialist in mental health Attending physician Dept. of psychiatry, GH Ilorin & Hopeville Psychiatric Hospital, Ilorin. Learning objectives
Overview of Psychoactive Drug use By Dr. Oladosu Ahmed Kayode Specialist in mental health Attending physician Dept. of psychiatry, GH Ilorin & Hopeville Psychiatric Hospital, Ilorin. Learning objectives
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE
 POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
POLYPHARMACY IN OLDER ADULTS AND BEERS CRITERIA UPDATE Jeannie Kim Lee, PharmD, BCPS, CGP Clinical Pharmacy Director College of Pharmacy The University of Arizona Learning Objectives: State the risks of
Medicines save lives
 Optimizing Aging Collaborative Disclosures Too much of a good thing: No financial interests to disclose John Newman, MD, PhD Assistant Professor Division of Geriatrics, UCSF Kirby Lee, PharmD, MAS Associate
Optimizing Aging Collaborative Disclosures Too much of a good thing: No financial interests to disclose John Newman, MD, PhD Assistant Professor Division of Geriatrics, UCSF Kirby Lee, PharmD, MAS Associate
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions
 Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
Health Outcome Prioritization as a Tool for Decision Making Among Older Persons With Multiple Chronic Conditions Mary Tinetti, M.D. Canadian Geriatrics Society May, 2013 CFPC CoI Templates: Slide 1 Faculty/Presenter
11/20/2014. Suggested Optimization of Medications for the frail Elderly (SOME) Polypharmacy. SOME* Polypharmacy. SOME Polypharmacy
 Polypharmacy. SOME* Polypharmacy. SOME Polypharmacy") SOME* Polypharmacy Suggested Optimization of Medications for the frail Elderly (SOME) Polypharmacy Information for Nursing Home Stakeholders Joint Venture between Nova Scotia Department of Health and Wellness
SOME* Polypharmacy Suggested Optimization of Medications for the frail Elderly (SOME) Polypharmacy Information for Nursing Home Stakeholders Joint Venture between Nova Scotia Department of Health and Wellness
Roy Zagieboylo, MD Assistant Professor University of Connecticut Family Medicine Department
 Roy Zagieboylo, MD Assistant Professor University of Connecticut Family Medicine Department That weight gaining diet I put you on is really working! This won t hurt me a bit. You re in good shape for the
Roy Zagieboylo, MD Assistant Professor University of Connecticut Family Medicine Department That weight gaining diet I put you on is really working! This won t hurt me a bit. You re in good shape for the
About ISMP Canada. Analysis Outputs: Safety Bulletins. Less is More: An Introduction to Deprescribing. canada.org
 Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Less is More: An Introduction to Deprescribing Lindsay Yoo, BSc, BScPhm, RPh, CDE, CGP, PharmD Medication Safety Analyst, ISMP Canada About ISMP Canada The Institute for Safe Medication Practices Canada
Disclosure and Acknowledgements
 Greetings from Penn Nursing SOHN 37 TH ANNUAL CONGRESS AND NURSING SYMPOSIUM POLYPHARMACY AND OLDER ADULTS: HIGH RISK MEDS, TOO MANY MEDS, AND TOO FEW MEDS Sarah H. Kagan PhD, RN University of Pennsylvania,
Greetings from Penn Nursing SOHN 37 TH ANNUAL CONGRESS AND NURSING SYMPOSIUM POLYPHARMACY AND OLDER ADULTS: HIGH RISK MEDS, TOO MANY MEDS, AND TOO FEW MEDS Sarah H. Kagan PhD, RN University of Pennsylvania,
Basics of Benzodiazepine Use Disorder. DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Basics of Benzodiazepine Use Disorder DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
GRADE, EBM and Deprescribing. Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa
 GRADE, EBM and Deprescribing Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa Research is like turning on the light before you clean up the room: it doesn t
GRADE, EBM and Deprescribing Kevin Pottie MD CCFP, MClSc, FCFP Associate Professor, Family Medicine, University of Ottawa Research is like turning on the light before you clean up the room: it doesn t
Finding the sweet spot: Individualized targets for older adults with Type 2 DM
 Finding the sweet spot: Individualized targets for older adults with Type 2 DM Samuel C. Durso, M.D., M.B.A. Mason F. Lord Professor of Medicine Director, Division of Geriatric Medicine and Gerontology
Finding the sweet spot: Individualized targets for older adults with Type 2 DM Samuel C. Durso, M.D., M.B.A. Mason F. Lord Professor of Medicine Director, Division of Geriatric Medicine and Gerontology
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
PATIENT INFORMATION LEAFLET ZOXADON TABLETS RANGE
 SCHEDULING STATUS: S5 PROPRIETARY NAME, STRENGTH AND PHARMACEUTICAL FORM: ZOXADON 0,5 mg: Each tablet contains 0,5 mg risperidone. ZOXADON 1 mg: Each tablet contains 1 mg risperidone. ZOXADON 2 mg: Each
SCHEDULING STATUS: S5 PROPRIETARY NAME, STRENGTH AND PHARMACEUTICAL FORM: ZOXADON 0,5 mg: Each tablet contains 0,5 mg risperidone. ZOXADON 1 mg: Each tablet contains 1 mg risperidone. ZOXADON 2 mg: Each
Preventing Medication Related Falls
 A Team Approach to Deprescribing and Preventing Medication Related Falls Wednesday, February 13 th 2019 Pam Howell THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE EMAILED AFTER THE
A Team Approach to Deprescribing and Preventing Medication Related Falls Wednesday, February 13 th 2019 Pam Howell THIS WEBINAR IS BEING RECORDED. THE SLIDE DECK AND RECORDING WILL BE EMAILED AFTER THE
PSYCHOTROPIC SOLUTIONS
 PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
PSYCHOTROPIC SOLUTIONS A proactive approach to antipsychotic medication management A Quality Use of Medicines initiative by Choice Aged Care Copyright 2018 Key Senate Committee Recommendations: All RACF
Patient Name Date of Birth Page 1 of 6
 2545 W. Hillcrest Dr. #205 Thousand Oaks, CA 91320 Admissions: 888.822.8938 Fax: 805.273.5246 Dear Medical Professional, This patient is seeking care to address eating disorder behaviors. For the patient
2545 W. Hillcrest Dr. #205 Thousand Oaks, CA 91320 Admissions: 888.822.8938 Fax: 805.273.5246 Dear Medical Professional, This patient is seeking care to address eating disorder behaviors. For the patient
LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA
 LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018 Objectives 1. Identify common preventable causes of hypoglycemia
LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018 Objectives 1. Identify common preventable causes of hypoglycemia
Thank You to Our Sponsors: Evaluations & CE Credits. Featured Speakers. Conflict of Interest & Disclosure Statements 10/18/2016
 Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Conflict of Interest & Disclosure Statements The planners and presenters do not have any financial arrangements
< = > less is more. De-diagnosing De-prescribing Non-testing
 < = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
< = > less is more De-diagnosing De-prescribing Non-testing Who says? Overdiagnosis Polypharmacy False positives Too much medicine Risk aversion $$$ Sources Prof David Le Couteur, Clin Pharm and Aged Care
Managing Pharmacy Expenses in PACE: A Case Based Discussion. Valencia P. Covington, MD, MPH Jennifer Keller, PharmD, BCPS, CGP June 5, 2016
 Managing Pharmacy Expenses in PACE: A Case Based Discussion Valencia P. Covington, MD, MPH Jennifer Keller, PharmD, BCPS, CGP June 5, 2016 Disclosure: Valencia Covington I have no relationships, financial
Managing Pharmacy Expenses in PACE: A Case Based Discussion Valencia P. Covington, MD, MPH Jennifer Keller, PharmD, BCPS, CGP June 5, 2016 Disclosure: Valencia Covington I have no relationships, financial
It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia
 It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia Jacqueline LaManna, PhD, ANP BC, BC ADM, CDE Holly Divine, PharmD, BCACP, CGP, CDE, FAPhA Disclosures Dr. Jacqueline LaManna
It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia Jacqueline LaManna, PhD, ANP BC, BC ADM, CDE Holly Divine, PharmD, BCACP, CGP, CDE, FAPhA Disclosures Dr. Jacqueline LaManna
Discontinuing Dementia Medications Case April Patient Case
 Discontinuing Dementia Medications Case April 2017 Patient Case MJ is an 86 year-old female with a primary diagnosis of Alzheimer s disease and history of anemia, cystitis, depression, Type II DM, HTN,
Discontinuing Dementia Medications Case April 2017 Patient Case MJ is an 86 year-old female with a primary diagnosis of Alzheimer s disease and history of anemia, cystitis, depression, Type II DM, HTN,
Alternatives to Physical Restraints
 Alternatives to Physical Restraints Case study. A 78 yr. old resident has a history of dementia (possibly Korsakoff s), chronic atrial fibrillation, CHF, COPD, frequent chest infections, obesity, heavy
Alternatives to Physical Restraints Case study. A 78 yr. old resident has a history of dementia (possibly Korsakoff s), chronic atrial fibrillation, CHF, COPD, frequent chest infections, obesity, heavy
NURSING HOME MEDICINE UPDATE
 NURSING HOME MEDICINE UPDATE - 2018 Bryan Primary Care Conference, Spring 2018 DISCLOSURES No financial disclosures I will mention non-fda approved use of medications OBJECTIVES 1. Review the new CMS rules
NURSING HOME MEDICINE UPDATE - 2018 Bryan Primary Care Conference, Spring 2018 DISCLOSURES No financial disclosures I will mention non-fda approved use of medications OBJECTIVES 1. Review the new CMS rules
David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy
 David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy It s no dream. Sleep well without sleeping pills. Outline Baby boomers & beyond: medication use Deprescribing
David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy It s no dream. Sleep well without sleeping pills. Outline Baby boomers & beyond: medication use Deprescribing
Katee Kindler, PharmD, BCACP
 Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Speaker Introduction Katee Kindler, PharmD, BCACP Current Practice: Clinical Pharmacy Specialist Ambulatory Care, St. Vincent Indianapolis Assistant Professor of Pharmacy Practice, Manchester University,
Rational Medication Use in Dementia
 Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Dr. Adeniyi Mofoluwake and Stacy Kramer
 Dr. Adeniyi Mofoluwake and Stacy Kramer Definition of Alzheimer s Disease Alzheimer's disease is a neurological disorder in which insidious onset of the death of brain cells causes memory loss and cognitive
Dr. Adeniyi Mofoluwake and Stacy Kramer Definition of Alzheimer s Disease Alzheimer's disease is a neurological disorder in which insidious onset of the death of brain cells causes memory loss and cognitive
Deprescribing: The Solution to Irrational Polypharmacy
 CAPA Annual Conference Victoria, BC October 21, 2018 Deprescribing: The Solution to Irrational Polypharmacy Thomas L. Perry MD, FRCPC UBC Therapeutics Initiative tom.perry@ti.ubc.ca Faculty/Presenter Disclosure
CAPA Annual Conference Victoria, BC October 21, 2018 Deprescribing: The Solution to Irrational Polypharmacy Thomas L. Perry MD, FRCPC UBC Therapeutics Initiative tom.perry@ti.ubc.ca Faculty/Presenter Disclosure
Hypertension and Cholesterol in the Elderly
 Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Perfect Endings. Home Alone. Senior Estimate. Staying Alive. Medication Madness
 Senior Estimate Home Alone Staying Alive Perfect Endings Medication Madness 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 Senior Estimate - 10 Patients who have multiple interacting
Senior Estimate Home Alone Staying Alive Perfect Endings Medication Madness 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 Senior Estimate - 10 Patients who have multiple interacting
Preventing Falls in Older Adults A Matter of Safety
 Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
Preventing Falls in Older Adults A Matter of Safety Roger Tam, BSc. Pharm. Wal-Mart Clinical Designated Pharmacist Falls Prevention Pharmacist Specialist NCCHC-Pre/Post Test Educator Q.U.I.T Educator Overview
1/16/2018. Disclosure Information. Objectives. Geriatric Scalpel: Improving Lives of Older Adults Through Rational Deprescribing
 Geriatric Scalpel: Improving Lives of Older Adults Through Rational Deprescribing Abhilash K. Desai, MD Geriatric Psychiatrist Idaho Memory & Aging Center, PLLC Adjunct Associate Professor Saint Louis
Geriatric Scalpel: Improving Lives of Older Adults Through Rational Deprescribing Abhilash K. Desai, MD Geriatric Psychiatrist Idaho Memory & Aging Center, PLLC Adjunct Associate Professor Saint Louis
Development of a Validated Enhanced Geriatric Assessment (ecga ) in a Primary Home-Based Interdisciplinary Practice"
 in a Primary Home-Based Interdisciplinary Practice") Development of a Validated Enhanced Geriatric Assessment (ecga ) in a Primary Home-Based Interdisciplinary Practice" Measuring Frailty in Primary Care Ted Rosenberg MD MSc FRCP (C) Fiona Manning MD MSc.
Development of a Validated Enhanced Geriatric Assessment (ecga ) in a Primary Home-Based Interdisciplinary Practice" Measuring Frailty in Primary Care Ted Rosenberg MD MSc FRCP (C) Fiona Manning MD MSc.
Community Pharmacy Dementia Audit
 Community Pharmacy Dementia Audit Introduction To comply with the NHS contractual requirements associated with the Clinical Governance Essential Service, pharmacy contractors must perform an annual practice
Community Pharmacy Dementia Audit Introduction To comply with the NHS contractual requirements associated with the Clinical Governance Essential Service, pharmacy contractors must perform an annual practice
Controlled Substance and Wellness Agreement
 Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate
 Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Doreen Wan-Chow-Wah, MD, FRCPC Assistant Professor, Division of Geriatric Medicine, Department of Medicine McGill University Health Center Associate member, Department of Oncology McGill University Medical
Chitra Fernando, MD March 18, 2008
 Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
Chitra Fernando, MD March 18, 2008 Definition Statistics Risk factors Why older adults are more prone to ADE Manifestations Inappropriate medications for older adults What can be done to minimize adverse
Travel Health Conference. April 27, 2018 Jamie Falk, BScPharm, PharmD
 Travel Health Conference April 27, 2018 Jamie Falk, BScPharm, PharmD Presenter: Jamie Falk Drug interactions in travelers with chronic conditions I have no conflicts to disclose By attending this session
Travel Health Conference April 27, 2018 Jamie Falk, BScPharm, PharmD Presenter: Jamie Falk Drug interactions in travelers with chronic conditions I have no conflicts to disclose By attending this session
Everolimus (Afinitor )
") Everolimus (Afinitor ) ( e-ver-oh-li-mus ) How drug is given: By mouth Purpose: to slow the growth of cancer cells in kidney cancer and other cancers How to take the drug Take with or without food and
Everolimus (Afinitor ) ( e-ver-oh-li-mus ) How drug is given: By mouth Purpose: to slow the growth of cancer cells in kidney cancer and other cancers How to take the drug Take with or without food and
Primary Care Prescribing Protocol to Support the Diagnosis and Management of People with Dementia
 Primary Care Prescribing Protocol to Support the Diagnosis and Management of People with Dementia This prescribing guideline provides the necessary information and guidance to support clinicians in the
Primary Care Prescribing Protocol to Support the Diagnosis and Management of People with Dementia This prescribing guideline provides the necessary information and guidance to support clinicians in the