SAVINO BRUNO, MD Director Internal Medicine and Hepatology Unit AO Fatebenefratelli e Oftalmico, Milano
|
|
|
- Edith Welch
- 5 years ago
- Views:
Transcription



1 SAVINO BRUNO, MD Director Internal Medicine and Hepatology Unit AO Fatebenefratelli e Oftalmico, Milano
2 Market wheretelaprevir has not yet launched

3 Victrelis is still launching
4 January 29 th 214 Developed by a select panel of 2 thought leaders: SOVALDI in various combinations is Recommended regimen for treatment of chronic HCV genotype 1, 2, 3, 4, 5 or 6 infection. OLYSIO with peginterferon alfa and ribavirin (PR) is Alternative regimen in select patients (interferon eligible chronic HCV genotype 1 patients with either HCV genotype 1b or HCV genotype 1a infection in whom the Q8K polymorphism is not detected at baseline; treatment naïve chronic HCV genotype 4 patients who are eligible for interferon). ROMA 12 febbraio 214 VICTRELIS with PR along with INCIVEK (telaprevir) with PR are Not Recommended for Chronic HCV genotype 1 patients. PR are Not Recommended for Chronic HCV genotype 2, 3 or 4 patients.
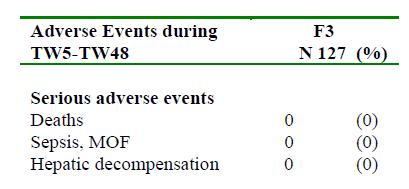
5 11 st August 214 update Treatment is assigned the highest priority for those patients with advanced fibrosis (Metavir F3), those with compensated cirrhosis (Metavir F4), liver transplant recipients, and patients with severe extrahepatic hepatitis C Based on available resources, treatment should be prioritized as necessary so that patients at high risk for liver related complications and severe ROMA extrahepatic hepatitis C complications are given high priority 12 febbraio 214

6 1.Natap.org

7 1.natap.org
8 NICE National Institute for Health and Care Exellence Summary of Appraisal Committee s key conclusions 1.3 Simeprevir, in combination with sofosbuvir (with or without ribavirin) is not recommended within its marketing authorisation for treating genotype 1 or 4 chronic hepatitis C. 1.Nice.org
9 214/15 Treatment Options: Right drug Right patient Key Factors in Deciding to Treat patients with HCV infection Risk of complications (degree of fibrosis and comorbidities) Efficacy, safety, duration, pill burden and dosing frequency of therapies Patient motivation/reluctance Affordability
10 MILD TO MODERATE FIBROSIS stage 214/15 Treatment Options Right drug Right patient HCV related disease: a condition with a wide heterogeneity of clinical features F 2 Metavir, F2 to 3 Ishak, LSM: 6 KPa < 9.5 Kpa (possible overlap with either less or more severe stage), APRI: <.5 (possible overlap) ADVANCED FIBROSIS stage (F3 Metavir, F3 to 4 Ishak, LSM: 9.5 KPa < 12.5 Kpa (possible overlap wth either less or more severe stage), APRI: >.5 <1.5 (possible overlap) WELL COMPENSATED cirrhosis (early stage: 1) F4 Metavir, F5 to 6 Ishak) or LSM: 12.5 KPa #, usually no clinically significant portal hypertension*: HVPG 6, mmhg < 1 mmhg, no esophageal varices, Child A5, MELD < 1. MARGINALLY COMPENSATED (more severe stage: 2) F4 Metavir, F5 to 6 Ishak or LSM: 12.5 KPa #, with moderate to severe portal hypertension : HVPG 1/12 mmhg, ±esophageal varices, PLT 1 /mm 3, low albumin value, Child A5, A6 rarely B7, MELD 1, in Child A5 severe portal hypertension with still preserved liver function may co exist DECOMPENSATED, Child B7 or more, MELD >15 and/or waiting for OLT for ESLD # Castera L. Gastroenterology 212 *Garcia Tsao G. et al, Hepatology 21 Qamar A. et al, Hepatology 28 Boccaccio V, Bruno S. Liver International 214 updated
11 MILD TO MODERATE FIBROSIS stage 214 Treatment Options Right drug Right patient HCV related disease: a condition with a wide heterogeneity of clinical features F 2 Metavir, F2 to 3 Ishak, LSM: 6 KPa < 9.5 Kpa (possible overlap with either less or more severe stage), APRI: <.5 (possible overlap) ADVANCED FIBROSIS stage (F3 Metavir, F3 to 4 Ishak, LSM: 9.5 KPa < 12.5 Kpa (possible overlap wth either less or more severe stage), APRI: >.5 <1.5 (possible overlap) WELL COMPENSATED cirrhosis (early stage: 1) F4 Metavir, F5 to 6 Ishak) or LSM: 12.5 KPa #, usually no clinically significant portal hypertension*: HVPG 6, mmhg < 1 mmhg, no esophageal varices, Child A5, MELD < 1. MARGINALLY COMPENSATED (more severe stage: 2) F4 Metavir, F5 to 6 Ishak or LSM: 12.5 KPa #, with moderate to severe portal hypertension : HVPG 1/12 mmhg, ±esophageal varices, PLT 1 /mm 3, low albumin value, Child A5, A6 rarely B7, MELD 1, in Child A5 severe portal hypertension with still preserved liver function may co exist DECOMPENSATED, Child B7 or more, MELD >15 and/or waiting for OLT for ESLD # Castera L. Gastroenterology 212 *Garcia Tsao G. et al, Hepatology 21 Qamar A. et al, Hepatology 28 Boccaccio V, Bruno S. Liver International 214 updated
12 TVR: SVR in naive patients with mild to moderate fibrosis (ADVANCE, ILLUMINATE, OPTIMIZE) T12(bid)/PR T12(q8h)/PR SVR % ,8 8 n=63 n=58 213/267 3/17 28/ /529 F 1 F2 F F2 All patients
13 SVR according to fibrosis score and historical response in F F2 patients in REALIZE study SVR % Relapsers Partial responders Null responders /167 1/38 34/47 3/17 24/59 1/18 Zeuzem S, et al. J Hepatol 211

14 CONCISE: SVR24 in non-cirrhotic IL28B CC treatmentnaïve patients and relapsers achieving ervr 91/16 48/52 T12/PR12 T12/PR24 Nelson DR, et al. HepDart 213. Abstract 118
15 SVR by BOC in non cirrhotic patients SVR % Naïve 72 Relapser/Partial Responders 89 8 Null Responders /11 14/38 Naïve: 63% of patients on BOC PR RGT vs 38% on PR for 48 weeks achieved SVR (p<.1) Treatment experienced: 59% of patients on BOC PR RGT vs 21% on PR for 48 weeks achieved SVR (p<.1) Early Responders (44%) Late Responders (22%) Poordad F, et al. Bacon BR, et al. NEJM 211. Vierling JM, et al. J Hepatol 214
16 SVR according to treatment week 8 virologic response* in F F2 SVR (%; 95% CI) F F2 5/78 *Treatment naïve and previous treatment failures combined Undetectable 3 log1 decline and detectable <3 log1 decline and detectable Data on file
17 SVR at a cutoff of 1, IU/mL at TW8 in the metaanalysis of 5 clinical studies in mild to moderate fibrosis Fibrosis Score* SVR [n/m (%)] TW8 <1 IU/ml TW8 1 IU/ml F/F2 175/144 (76) 13/131 (1) *Subjects in BOC arms from 5 clinical studies Data on file
18 NEUTRINO: SVR12 by Sofosbuvir + P/R (12 weeks) According to Genotype and Fibrosis Level SVR12 According to Genotype SVR12 According to Fibrosis Level p=.96 8 SVR12 (%) 6 4 SVR12 (%) n/n = 261/292 27/28 7/7 GT 1 GT 4 GT 5, /273 43/54 No Cirrhosis Cirrhosis Lawitz E, et al. NEJM 213
19
20 QUEST 1: SVR12 by Fibrosis Level, Subtype, and Baseline Resistance SMV + P/R P/R SVR12 (%) SVR12 (%) n/n = 188/229 6/113 18/31 5/17 No Cirrhosis Cirrhosis 2 15/147 36/74 GT 1a Differences in SVR12 by Subgroup (95% CIs) GT 1a/other HCV - With baseline Q8K vs Pbo - Without baseline Q8K vs Pbo GT 1b HCV Favors Placebo Favors SMV 15/117 29/56 GT 1b SMV (n) Pbo (n) 28.2 ( ) 4.7 (-14.6 to 24.1) 4.3 ( ) 42.1 ( ) Jacobson I, et al. EASL 213
21 Simeprevir plus PegIFN and Ribavirin in treatment experienced F F2 patients with HCV Genotype 1 infection (the ASPIRE trial) Relapsers Partial responders Null responders SVR 24 (%) Placebo+PR SMV 1 mg+pr* SMV 15 mg+pr* N= *duration groups pooled Zeuzem S, et al. Gastroenterology 213

22 SMV + PR: Week 4 on-treatment response* predicts high SVR rates Patients at Week 4 (%) Patients with SVR12 (%) 12/26 35/521 5/12 7/35 Relapser (PROMISE) Naïve (QUEST 1 & 2) detectable and undetectable 247/26 474/521 21/247 49/ % of patients had a Week 4 on-treatment response with a high probability of achieving SVR Patients with a Week 4 response 25 IU/mL are unlikely to achieve SVR Discontinuation of treatment is recommended according to US prescribing information in these patients HCV RNA < 25 IU/mL, detectable and undetectable Intent-to-treat population FDA backgrounder for FDA advisory committee meeting October ; Simeprevir US Prescribing information
23 MILD TO MODERATE FIBROSIS stage 214 Treatment Options Right drug Right patient HCV related disease: a condition with a wide heterogeneity of clinical features F 2 Metavir, F2 to 3 Ishak, LSM: 6 KPa < 9.5 Kpa (possible overlap with either less or more severe stage), APRI: <.5 (possible overlap) ADVANCED FIBROSIS stage (F3 Metavir, F3 to 4 Ishak, LSM: 9.5 KPa < 12.5 Kpa (possible overlap wth either less or more severe stage), APRI: >.5 <1.5 (possible overlap) WELL COMPENSATED cirrhosis (early stage: 1) F4 Metavir, F5 to 6 Ishak) or LSM: 12.5 KPa #, usually no clinically significant portal hypertension*: HVPG 6, mmhg < 1 mmhg, no esophageal varices, Child A5, MELD < 1. MARGINALLY COMPENSATED (more severe stage: 2) F4 Metavir, F5 to 6 Ishak or LSM: 12.5 KPa #, with moderate to severe portal hypertension : HVPG 1/12 mmhg, ±esophageal varices, PLT 1 /mm 3, low albumin value, Child A5, A6 rarely B7, MELD 1, in Child A5 severe portal hypertension with still preserved liver function may co exist DECOMPENSATED, Child B7 or more, MELD >15 and/or waiting for OLT for ESLD # Castera L. Gastroenterology 212 *Garcia Tsao G. et al, Hepatology 21 Qamar A. et al, Hepatology 28 Boccaccio V, Bruno S. Liver International 214 updated
24 SVR according to fibrosis score and historical response in HCV G1 F3 patients in TVR trials (ADVANCE, ILLUMINATE, OPTIMIZE, REALIZE) 1 Naïve Relapsers Partial responders Null responders 9 85 SVR % , /247 53/62 1/18 15/38 Zeuzem S, et al. J Hepatol 211. Zeuzem S, et al. AASLD 213
25 International EAP TVR: ITT SVR by previous treatment response in 552 F3 patients 1 Naïve Relapsers Partial responders Null responders SVR % ,7 77,1 58,1 41, / /21 36/62 49/119 Colombo M, et al. J Hepatol 214 in press
26 Overall SVR by F3 1 8 SVR % /17 6/22 F3 BOC PR PR Vierling JM, Bruno S, et al. J Hepatol, 214
27 SVR according to treatment week 8 virologic response in F3 patients* SVR (%, 95% CI) Undetectable 3 log HCV-RNA decline and detectable <3 log HCV-RNA decline and detectable 2 1 4/47 16/47 F3 /5 *Treatment-naïve and previous treatment failures combined Vierling JM, Bruno S, et al. J Hepatol, 214
28 The importance of TW 8 HCV RNA decline in patients with advanced fibrosis/cirrhosis (F3 and F4 pooled) during BOC therapy 1 p<.1 SVR % /238 /31 1 IU/ml (88%) >1 IU/ml (12%) Vierling JM, Bruno S, et al. J Hepatol, 214
29 SVR12 overall and according to prior response in 121 F3 patients All patients who received at least one dose of BOC included ,3% Overall F3 61,7% 61,3% 5,6% 5% 4 37,9% /137 29/47 45/89 19/31 58/153 21/42 Relapser Partial responder Null responder Bruno S, et al. JVH in press
30 SVR12 in 121 F3 according to treatment week 8 virologic response All patients who received at least one dose of BOC included HCV-RNA Undetectable 8,% SVR 39,7% HCV-RNA Detectable 2,% 6,3% PPV=8,% NPV=6.3% No SVR HCV-RNA < 1 UI/mL 67% SVR % HCV-RNA > 1 UI/mL 33% PPV=67% NPV=1% 1% No SVR Bruno S, et al. JVH in press
31
32 Simeprevir plus PegIFN and Ribavirin in treatment experienced F3 patients with HCV Genotype 1 infection (the ASPIRE trial) Relapsers Partial responders Null responders SVR 24 (%) N= Placebo+PR SMV 1 mg+pr* SMV 15 mg+pr* *duration groups pooled Zeuzem S, et al. Gastroenterology 213
33 MILD TO MODERATE FIBROSIS stage 214 Treatment Options Right drug Right patient HCV related disease: a condition with a wide heterogeneity of clinical features F 2 Metavir, F2 to 3 Ishak, LSM: 6 KPa < 9.5 Kpa (possible overlap with either less or more severe stage), APRI: <.5 (possible overlap) ADVANCED FIBROSIS stage (F3 Metavir, F3 to 4 Ishak, LSM: 9.5 KPa < 12.5 Kpa (possible overlap wth either less or more severe stage), APRI: >.5 <1.5 (possible overlap) WELL COMPENSATED cirrhosis (early stage: 1) F4 Metavir, F5 to 6 Ishak) or LSM: 12.5 KPa #, usually no clinically significant portal hypertension*: HVPG 6, mmhg < 1 mmhg, no esophageal varices, Child A5, MELD < 1. MARGINALLY COMPENSATED (more severe stage: 2) F4 Metavir, F5 to 6 Ishak or LSM: 12.5 KPa #, with moderate to severe portal hypertension : HVPG 1/12 mmhg, ±esophageal varices, PLT 1 /mm 3, low albumin value, Child A5, A6 rarely B7, MELD 1, in Child A5 severe portal hypertension with still preserved liver function may co exist DECOMPENSATED, Child B7 or more, MELD >15 and/or waiting for OLT for ESLD # Castera L. Gastroenterology 212 *Garcia Tsao G. et al, Hepatology 21 Qamar A. et al, Hepatology 28 Boccaccio V, Bruno S. Liver International 214 updated
34 SVR according to fibrosis score and historical response in HCV G1 F4 patients in TVR trials (ADVANCE, ILLUMINATE, OPTIMIZE, REALIZE) SVR % Naïve 53,5 99/185 Relapsers Partial responders Null responders /57 11/32 7/5 Zeuzem S, et al. AASLD 213. Zeuzem S, et al. J Hepatol 211
35 International EAP TVR: ITT SVR by previous treatment response in 526 F4 patients SVR % Naïve Relapsers Partial responders Null responders 62,8 64,4 53,2 28,6 59/94 94/146 41/77 5/175 Colombo M, et al. J Hepatol 214 in press
36 Overall SVR by F4 1 8 SVR % /18 6/32 F4 BOC PR PR Vierling JM, Bruno S, et al. J Hepatol, 214
37 SVR according to treatment week 8 virologic response* in F Undetectable 3 log HCV-RNA decline and detectable SVR (%, 95% CI) <3 log HCV-RNA decline and detectable 2 1 4/47 65/73 28/79 /17 *Treatment-naïve and previous treatment failures combined Vierling JM, Bruno S, et al. J Hepatol 214
38 The importance of TW 8 HCV RNA decline in patients with advanced fibrosis/cirrhosis (F3 and F4 pooled) during BOC therapy 1 p<.1 SVR % /238 /31 1 IU/ml (88%) >1 IU/ml (12%) Vierling JM, Bruno S, et al. J Hepatol, 214
39 EoTR, SVR12 and relapse rate overall and in 26 cirrhotic patients All patients who received at least one dose of BOC included Overall F % 65% 49% 45% % 25% 1 237/ /26 188/ /26 49/237 4/158 EoTR SVR12 Relapse Bruno S, et al. JVH in press
40 SVR12 overall and according to prior response in 26 cirrhotic patients All patients who received at least one dose of BOC included ,3% 61,1% Overall 5,6% F4 44,8% ,9% 33.3% 1 84/137 55/9 45/89 26/58 58/153 37/111 Relapser Partial responder Null responder Bruno S, et al. JVH in press
41 SVR12 in 26 F4 according to treatment week 8 virologic response All patients who received at least one dose of BOC included HCV-RNA Undetectable HCV-RNA Detectable HCV-RNA < 1 UI/mL HCV-RNA > 1 UI/mL ,9% 68,3% 31,7% 28,1% SVR No SVR ,7% SVR 9,1% ,3% ,9% 3 33 No SVR PPV=68,3% - NPV=71,9% PPV=51,7%-NPV=9,9% Bruno S, et al. JVH in press
42
43 CUPIC SVR12 rates and safety (ANRS CO2 CUPIC) Undetectable HCV RNA (ITT) n (%) BOC n = 212 TVR n = 299 SVR 12 (Total) 91(43) 155 (52) SVR 12 in relapsers 55/12 (54) 92/124 (74) SVR 12 in partial responders 36/94 (38) 54/135 (4) SVR 12 in null responders /1 () 6/31 (19) SAE 44.3% 53.8% Death 1.4% 2.7% Infections 3.8% 9.7% Hepatic decompensation 4.2% 4.7% Anemia <8g/dl or blood tx 9%/11.8% 12.7%/18% Fontaine H, et al. AFEF 213
 SAE: 16.1 % SVR: > 29% SAE (31) Platelets count 1,/mm 3 SAE: 12.2 % SVR SVR : > 36.5% SAE (74) SAE: 51.4 % SVR: SAE >> 27% SVR (37) 9% Hezode C, et al.")
44 Risk-benefit (SAE / SVR 12) ( number of patients ) Risk factors for SAE Albumin 35 g/l Albumin <35 g/l Missing data in 63 patients Platelets count > 1,/mm 3 SAE : 6.2 % SVR >> : 54.9% SAE (36) SAE: 16.1 % SVR: > 29% SAE (31) Platelets count 1,/mm 3 SAE: 12.2 % SVR SVR : > 36.5% SAE (74) SAE: 51.4 % SVR: SAE >> 27% SVR (37) 9% Hezode C, et al. Gastroenterology 214
45 SVR12 according to on treatment response TELAPREVIR BOCEPREVIR % 125/198 3/11 RVR P <.1 Fontaine H, France, AFEF 213, 4% NO RVR % 62/99 29/113 HCV RNA Decline 1log W4 P <.1 26% HCV RNA Decline < 1log W4 RVR W8 P <.1 72% 25% 58/81 33/131 NO RVR W8 6% 4/63 HCV RNA Decline < 3log W8
46 Simeprevir plus PegIFN and Ribavirin in treatment experienced cirrhotic (F4) patients with HCV Genotype 1 infection (the ASPIRE trial) Relapsers Partial responders Null responders SVR 24 (%) N= Placebo+PR SMV 1 mg+pr* SMV 15 mg+pr* *duration groups pooled Zeuzem S, et al. Gastroenterology 213
47
48 Is there still a role of IFN based triple therapy with first generation PI in patients with mild to moderate fibrosis and comorbities (NULLS EXCLUDED) YES Overall SVR rates quite good, Short duration of treatment in the vast majority of patients Patient s reluctance NO SMV or SOF+IFN soon available Safety profile manageable Approved futility rules useful and externally validated *SOC may be considered in naives LVL RVR after lead in

49 Is there still a role of IFN based triple therapy with first generation PI in patients with mild to moderate fibrosis and comorbities (NULLS EXCLUDED) YES Overall SVR rates quite good, Short duration of treatment in the vast majority of patients Patient s reluctance NO SMV or SOF+IFN soon available Safety profile manageable Approved futility rules useful and externally validated BASED ON FIRST GENERATION PIs COST *SOC may be considered in naives LVL RVR after lead in

50 Is there still a role of IFN based triple therapy with first generation PI in patients with mild to moderate fibrosis and comorbities (NULLS EXCLUDED) YES Overall SVR rates quite good, Short duration of treatment in the vast majority of patients Patient s reluctance NO SMV or SOF+IFN soon available Safety profile manageable Approved futility rules useful and externally validated BASED ON FIRST GENERATION PIs COST *SOC may be considered in naives LVL RVR after lead in

51 Is there still a role of IFN based triple therapy with first generation PI in patients with advanced fibrosis (F3) and early stage (F4) compensated, NULLS F2 included YES NO Overall SVR rates using early futility not that bad Safety profile quite manageable Approval of all-oral combination soon available Patient s reluctance

52 Treating vs Deferring IFN based triple therapy in marginally compensated Cirrhotic patients with moderate to severe portalhypertension TREAT Urgency of treatment well established Short-term prognosis worrying DEFER Efficacy, safety, duration of therapy, pill burden and dosing frequency unacceptable Approval of all-oral combination soon available EA program or compassionate use soon available
53 Thank you for your attention! The opinions expressed here represent the opinion of the author. All products mentioned in the presentation should be applied according to the Product Labels.
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors
 Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Optimal Treatment with Boceprevir. Michael Manns
 Optimal Treatment with Boceprevir Michael Manns 6th Paris Hepatitis Conference, 14th January 2013 Acknowledgements Benjamin Maasoumy Optimal Patient Selection Defining the Ideal Candidate Treatment Urgency
Optimal Treatment with Boceprevir Michael Manns 6th Paris Hepatitis Conference, 14th January 2013 Acknowledgements Benjamin Maasoumy Optimal Patient Selection Defining the Ideal Candidate Treatment Urgency
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy
 How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
Clinical Cases Hepatitis C Naïve Patients. Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona.
 Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Protease inhibitor based triple therapy in treatment experienced patients
 Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
CURRENT TREATMENTS. Mitchell L Shiffman, MD Director Liver Institute of Virginia. Richmond and Newport News, VA, USA
 CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy?
 Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors
 Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Treatment of genotype 4 patient. with cirrhosis. Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble
 Treatment of genotype 4 patient with cirrhosis Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble Clinical case 52 year-old patient Intra-venous drug user 1987-1989
Treatment of genotype 4 patient with cirrhosis Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble Clinical case 52 year-old patient Intra-venous drug user 1987-1989
Treatement Experienced patients without cirrhosis. Rafael Esteban Hospital Universitario Valle Hebron Barcelona
 Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) PegIFN and RBV remain vital components of HCV therapy-- selected presentations from: Program Disclosure This activity has been planned and
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) PegIFN and RBV remain vital components of HCV therapy-- selected presentations from: Program Disclosure This activity has been planned and
Personalised Treatment with Telaprevir in Graham R Foster Professor of Hepatology Queen Marys University of London
 Personalised Treatment with Telaprevir in 2014 Graham R Foster Professor of Hepatology Queen Marys University of London Telaprevir in 2014 Disclaimers I have received funds from: BI, BMS, Janssen, Novarts,
Personalised Treatment with Telaprevir in 2014 Graham R Foster Professor of Hepatology Queen Marys University of London Telaprevir in 2014 Disclaimers I have received funds from: BI, BMS, Janssen, Novarts,
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Introduction. The ELECTRON Trial
 63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Olysio (simeprivir) Policy Number: Last Review: 09/2017 Origination: 09/2013 Next Review: 09/2018
 Policy Number: Last Review: 09/2017 Origination: 09/2013 Next Review: 09/2018") Olysio (simeprivir) Policy Number: 5.01.604 Last Review: 09/2017 Origination: 09/2013 Next Review: 09/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Olysio (simeprivir)
Olysio (simeprivir) Policy Number: 5.01.604 Last Review: 09/2017 Origination: 09/2013 Next Review: 09/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Olysio (simeprivir)
Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine
 Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Pierluigi Toniutto Clinica di Medicina Interna Azienda Ospedaliero Universitaria Udine Il sottoscritto dichiara di non aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Olysio (simeprevir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/9/2014 1. Indications Drug Name: Olysio
Prior Authorization Guideline Guideline Name Olysio (simeprevir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/9/2014 1. Indications Drug Name: Olysio
Express Scripts, Inc. monograph dated 5/25/2011; selected revision 6/1/2011
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Coverage Criteria: Approval Period: Victrelis (boceprevir capsules)
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Coverage Criteria: Approval Period: Victrelis (boceprevir capsules)
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) Goals for Hepatitis C Therapy Compared to PegIFN α/rbv, new treatment regimens for chronic hepatitis C should offer: Improved efficacy Efficacy
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) Goals for Hepatitis C Therapy Compared to PegIFN α/rbv, new treatment regimens for chronic hepatitis C should offer: Improved efficacy Efficacy
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
BOCEPREVIR (BOC): EVIDENCE FROM TRIALS
: EVIDENCE FROM TRIALS") BOCEPREVIR (BOC): EVIDENCE FROM TRIALS ROME, FEBRUARY 22 nd -25 th, 212 Savino Bruno, MD Department of Internal Medicine A.O. Fatebenefratelli e Oftalmico Milan, Italy Savino Bruno, MD Director of InternalMedicine,
BOCEPREVIR (BOC): EVIDENCE FROM TRIALS ROME, FEBRUARY 22 nd -25 th, 212 Savino Bruno, MD Department of Internal Medicine A.O. Fatebenefratelli e Oftalmico Milan, Italy Savino Bruno, MD Director of InternalMedicine,
HCV Case Study. Treat Now or Wait for New Therapies
 HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Antiviral treatment in HCV cirrhotic patients on waiting list
 Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Antiviral treatment in HCV cirrhotic patients on waiting list Krzysztof Tomasiewicz Department of Hepatology and Infectious Diseases Medical University of Lublin, Poland Disclosures Consultancy/Advisory
Predictors of Response to Hepatitis C Therapy in the DAA Era. Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid
 Predictors of Response to Hepatitis C Therapy in the DAA Era Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid Why Predicting HCV Response? Select candidates for therapy Prioritizing
Predictors of Response to Hepatitis C Therapy in the DAA Era Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid Why Predicting HCV Response? Select candidates for therapy Prioritizing
Simeprevir + PEG + RBV in Treatment-Naïve Genotype 1 QUEST-1 Trial
 Phase 3 Treatment Naïve Simeprevir + in Treatment-Naïve Genotype 1 QUEST-1 Trial Jacobson IM, et al. Lancet. 2014;384:403-13. Simeprevir + PEG + Ribavirin for Treatment-Naïve HCV GT1 QUEST-1 Trial QUEST-1
Phase 3 Treatment Naïve Simeprevir + in Treatment-Naïve Genotype 1 QUEST-1 Trial Jacobson IM, et al. Lancet. 2014;384:403-13. Simeprevir + PEG + Ribavirin for Treatment-Naïve HCV GT1 QUEST-1 Trial QUEST-1
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Stick or twist management options in hepatitis C
 Stick or twist management options in hepatitis C Dr. Chris Durojaiye & Dr. Matthijs Backx SpR Microbiology and Infectious Diseases University Hospital of Wales, Cardiff Patient history 63 year old female
Stick or twist management options in hepatitis C Dr. Chris Durojaiye & Dr. Matthijs Backx SpR Microbiology and Infectious Diseases University Hospital of Wales, Cardiff Patient history 63 year old female
Hepatitis C: New Antivirals in the Liver Transplant Setting. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience
 Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience A. Coilly, B. Roche, J. Dumortier, D. Botta-Fridlund, V. Leroy,
Efficacy and safety of protease inhibitors for sever hepatitis C recurrence after liver transplantation: a first multicentric experience A. Coilly, B. Roche, J. Dumortier, D. Botta-Fridlund, V. Leroy,
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona
 Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona rrent HCV Therapy 8% % sustained response 6% 4% 2% % 54-61% 41% 34% 25% 16% 6% IFN 24w IFN 48w Peg
Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona rrent HCV Therapy 8% % sustained response 6% 4% 2% % 54-61% 41% 34% 25% 16% 6% IFN 24w IFN 48w Peg
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
Triple therapy with telaprevir or boceprevir: management of side effects
 Triple therapy with telaprevir or boceprevir: management of side effects Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Triple therapy with telaprevir or boceprevir: management of side effects Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Abbreviated Class Update: Hepatitis C
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
ABCs of Hepatitis C: What s New. The Long-Awaited New Era: Protease Inhibitors for HCV Genotype 1
 ABCs of Hepatitis C: What s New ACG Postgraduate Course Washington, DC October 30, 2011 Ira M. Jacobson, M.D. Vincent Astor Professor of Medicine Chief, Division of Gastronterology and Hepatology Medical
ABCs of Hepatitis C: What s New ACG Postgraduate Course Washington, DC October 30, 2011 Ira M. Jacobson, M.D. Vincent Astor Professor of Medicine Chief, Division of Gastronterology and Hepatology Medical
How do you optimize HCV Treatment for Cirrhotic Patients APASL STC Cebu
 How do you optimize HCV Treatment for Cirrhotic Patients APASL STC Cebu Seng Gee Lim Chairman, APASL Liver Week 2013 Professor of Medicine Dept of Gastroenterology and Hepatology NUHS, Singapore Disclosures
How do you optimize HCV Treatment for Cirrhotic Patients APASL STC Cebu Seng Gee Lim Chairman, APASL Liver Week 2013 Professor of Medicine Dept of Gastroenterology and Hepatology NUHS, Singapore Disclosures
Pegylated Interferon Agents for Hepatitis C
 Applicable X X X X X X X Pegylated Interferon Agents for Hepatitis C Override(s) Prior Authorization Quantity Limit Initial for Monotherapy or Combination with Ribavirin based on Genotype, Status, or Co-Infection
Applicable X X X X X X X Pegylated Interferon Agents for Hepatitis C Override(s) Prior Authorization Quantity Limit Initial for Monotherapy or Combination with Ribavirin based on Genotype, Status, or Co-Infection
Azienda ULSS12 Veneziana
 Azienda ULSS12 Veneziana Risultati del trattamento dei monoinfetti con Sofosbuvir, Simeprevir nella coorte veneziana. Confronto di esito con la coorte del trattamento con Boceprevir e Telaprevir Dr.ssa
Azienda ULSS12 Veneziana Risultati del trattamento dei monoinfetti con Sofosbuvir, Simeprevir nella coorte veneziana. Confronto di esito con la coorte del trattamento con Boceprevir e Telaprevir Dr.ssa
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
Treatment of chronic hepatitis C in drug-naïve patients
 Treatment of chronic hepatitis C in drug-naïve patients 8th International Workshop on HIV & Hepatitis Co-infection Madrid, 31. May 2012 Christoph Sarrazin J. W. Goethe-University Hospital Medizinische
Treatment of chronic hepatitis C in drug-naïve patients 8th International Workshop on HIV & Hepatitis Co-infection Madrid, 31. May 2012 Christoph Sarrazin J. W. Goethe-University Hospital Medizinische
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 16 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
HCV disease: treatment or deferral? Antonio Craxì Gastroenterologia & Epatologia, Di.Bi.M.I.S., Università di Palermo
 HCV disease: treatment or deferral? Antonio Craxì Gastroenterologia & Epatologia, Di.Bi.M.I.S., Università di Palermo antonio.craxi@unipa.it Key factors in deciding to treat or wait Patient factors Urgency
HCV disease: treatment or deferral? Antonio Craxì Gastroenterologia & Epatologia, Di.Bi.M.I.S., Università di Palermo antonio.craxi@unipa.it Key factors in deciding to treat or wait Patient factors Urgency
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Topic: Sovaldi, sofosbuvir Date of Origin: March 14, Committee Approval Date: August 15, 2014 Next Review Date: March 2015
 Medication Policy Manual Policy No: dru332 Topic: Sovaldi, sofosbuvir Date of Origin: March 14, 2014 Committee Approval Date: August 15, 2014 Next Review Date: March 2015 Effective Date: October 1, 2014
Medication Policy Manual Policy No: dru332 Topic: Sovaldi, sofosbuvir Date of Origin: March 14, 2014 Committee Approval Date: August 15, 2014 Next Review Date: March 2015 Effective Date: October 1, 2014
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
Virological Tools and Monitoring in the DAA Era
 Virological Tools and Monitoring in the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Virological Tools and Monitoring in the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Prior Authorization Guideline
 Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Prior Authorization Guideline Guideline Name Sovaldi (sofosbuvir) Formulary UnitedHealthcare Community & State Formulary Note Approval Date 2/19/2014 Revision Date 7/8/2014 1. Indications Drug Name: Sovaldi
Chronic Hepatitis C Drug Class Prior Authorization Protocol
 Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
Line of Business: Medi-Cal Effective Date: August 16, 2017 Revision Date: August 16, 2017 Chronic Hepatitis C Drug Class Prior Authorization Protocol This policy has been developed through review of medical
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
Treatment of Hepatitis C with sofosbuvir/ledipasvir (Harvoni )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
Case #1. Case #1. Case #1: Audience vote VS. The Great Debate: When to Treat HCV in our HIV coinfected patients
 Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
Chronic Hepatitis C Drug Class Monograph
 Chronic Hepatitis C Drug Class Monograph Line of Business: Medi-Cal Effective Date: July 10, 2017 (Interim Guidelines; Final Review and Approval by the P&T Subcommittee Pending) This policy has been developed
Chronic Hepatitis C Drug Class Monograph Line of Business: Medi-Cal Effective Date: July 10, 2017 (Interim Guidelines; Final Review and Approval by the P&T Subcommittee Pending) This policy has been developed
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira XR), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira XR), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Will difficult-to-treat patients remain difficultto-treat. generation of treatments?
 Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Optimal ltherapy in non 1 genotypes:
 Optimal ltherapy in non 1 genotypes: genotype 2 and 3 patients Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University of Palermo, Italy craxanto@unipa.it Peg IFN alpha plus ribavirin : SVR rate of >80%
Optimal ltherapy in non 1 genotypes: genotype 2 and 3 patients Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University of Palermo, Italy craxanto@unipa.it Peg IFN alpha plus ribavirin : SVR rate of >80%
Highlights of AASLD 2012 CCO Official Conference Coverage of the 2012 Annual Meeting of the American Association for the Study of Liver Diseases
 Highlights of AASLD 12 CCO Official Conference Coverage of the 12 Annual Meeting of the American Association for the Study of Liver Diseases November 9-13, 12 Boston, Massachusetts In partnership with
Highlights of AASLD 12 CCO Official Conference Coverage of the 12 Annual Meeting of the American Association for the Study of Liver Diseases November 9-13, 12 Boston, Massachusetts In partnership with
Hepatitis C Virus Clinical Criteria Update September 18, For: New York State Medicaid
 Hepatitis C Virus Clinical Criteria Update September 18, 2014 For: New York State Medicaid 1 Purpose Characterize the place in therapy for the agents utilized for management of chronic hepatitis C (CHC)
Hepatitis C Virus Clinical Criteria Update September 18, 2014 For: New York State Medicaid 1 Purpose Characterize the place in therapy for the agents utilized for management of chronic hepatitis C (CHC)
Oral combination therapy: future hepatitis C virus treatment? "Lancet Oct 30;376(9751): Oral combination therapy with a nucleoside
: Oral combination therapy with a nucleoside") Author manuscript, published in "Journal of Hepatology 2011;55(4):933-5" DOI : 10.1016/j.jhep.2011.04.018 Oral combination therapy: future hepatitis C virus treatment? Commentary article on the following
Author manuscript, published in "Journal of Hepatology 2011;55(4):933-5" DOI : 10.1016/j.jhep.2011.04.018 Oral combination therapy: future hepatitis C virus treatment? Commentary article on the following
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES
 VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
Abbreviated Class Update: Hepatitis C
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Drug Class Monograph
 Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
Drug Class Monograph Class: Chronic Hepatitis C Drugs(s): Daclatasvir (Daklinza), Dasabuvir/ombitasivir/paritaprevir/ritonavir (Viekira Pak), Elbasvir/grazoprevir (Zepatier), Peginterferon alfa-2a (Pegasys),
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING. Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona
 TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
TREATMENT OF HEPATITIS C IN THE LIVER TRANSPLANT SETTING Dra. Zoe Mariño Liver Unit. Hospital Clinic Barcelona Hepatitis C after LT Survival (%) HCV negative HCV positive Time from LT (years) HCV treatment
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Hepatitis C Prior Authorization Policy
 Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Hepatitis C Treatment in Oregon
 The Hepatitis C Advisory Group, 12/21/2014 Hepatitis C Treatment in Oregon Introduction The rising health care burden of HCV infection in Oregon is occurring at this time of growing interest in containing
The Hepatitis C Advisory Group, 12/21/2014 Hepatitis C Treatment in Oregon Introduction The rising health care burden of HCV infection in Oregon is occurring at this time of growing interest in containing
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
Accepted Manuscript. International Hepatology
 Accepted Manuscript International Hepatology HCV cirrhosis at the edge of decompensation: Will ABT-450/r, ombitasvir, dasabuvir and ribavirin solve the need for treatment? Tarik Asselah, Savino Bruno,
Accepted Manuscript International Hepatology HCV cirrhosis at the edge of decompensation: Will ABT-450/r, ombitasvir, dasabuvir and ribavirin solve the need for treatment? Tarik Asselah, Savino Bruno,
2017 UnitedHealthcare Services, Inc.
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 1146-7 Program Prior Authorization/Notification Medication Harvoni (ledipasvir/sofosbuvir) P&T Approval Date 10/2014, 2/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 1146-7 Program Prior Authorization/Notification Medication Harvoni (ledipasvir/sofosbuvir) P&T Approval Date 10/2014, 2/2015,
November 2013 AASLD Investor Event 4 November
 November 2013 AASLD Investor Event 4 November Maris Hartmanis, President and CEO Charlotte Edenius, EVP Development Bertil Samuelsson, CSA Rein Piir, EVP Corporate Affairs & IR Corporate presentation,
November 2013 AASLD Investor Event 4 November Maris Hartmanis, President and CEO Charlotte Edenius, EVP Development Bertil Samuelsson, CSA Rein Piir, EVP Corporate Affairs & IR Corporate presentation,
Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1
 Phase 3 Treatment-Naïve and Treatment-Experienced Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1 EXPEDITION-1: Study Features EXPEDITION-1 Trial Design: Open-label, single-arm,
Phase 3 Treatment-Naïve and Treatment-Experienced Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1 EXPEDITION-1: Study Features EXPEDITION-1 Trial Design: Open-label, single-arm,
Personalizzazione della Cura in Epatologia. Epatite Cronica C: Pazienti con Genotipo 2
 Monotematica AISF 213 Personalizzazione della Cura in Epatologia Pisa, 17-19 Ottobre 213 Epatite Cronica C: Pazienti con Genotipo 2 Maria Grazia Rumi U.O. Epatologia, Ospedale San Giuseppe Università degli
Monotematica AISF 213 Personalizzazione della Cura in Epatologia Pisa, 17-19 Ottobre 213 Epatite Cronica C: Pazienti con Genotipo 2 Maria Grazia Rumi U.O. Epatologia, Ospedale San Giuseppe Università degli
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient. Konstantin Zhdanov
 Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of
 Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
SUMMACARE COMMERCIAL MEDICATION REQUEST GUIDELINES
 Generic Brand HICL GCN Exception/Other TELAPREVIR INCIVEK 37629 This drug requires a written request for prior authorization. All requests for hepatitis C medications require review by a pharmacist prior
Generic Brand HICL GCN Exception/Other TELAPREVIR INCIVEK 37629 This drug requires a written request for prior authorization. All requests for hepatitis C medications require review by a pharmacist prior
Current Treatments for HCV
 Current Treatments for HCV Mitchell L. Shiffman, MD, FACG Advisory Committee/Board Member: Achillion, Anadys, Boehringer-Ingelheim, BMS, Conatus, Genentech, Gen-Probe, Gilead, Globeimmune, GSK, Janssen,
Current Treatments for HCV Mitchell L. Shiffman, MD, FACG Advisory Committee/Board Member: Achillion, Anadys, Boehringer-Ingelheim, BMS, Conatus, Genentech, Gen-Probe, Gilead, Globeimmune, GSK, Janssen,
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 14 December 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 December 2011 INCIVO 375 mg, film-coated tablet B/4 bottles of 42 tablets (CIP code: 217 378-5) B/1 bottle of 42
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 14 December 2011 INCIVO 375 mg, film-coated tablet B/4 bottles of 42 tablets (CIP code: 217 378-5) B/1 bottle of 42
ةي : لآا ةرقبلا ةروس
 سورة البقرة: اآلية HCV RELAPSERS AND NONRESPONDERS: How to deal with them? BY Prof. Mohamed Sharaf-Eldin Prof. of Hepatology and Gastroenterology Tanta University Achieving SVR The ability to achieve a
سورة البقرة: اآلية HCV RELAPSERS AND NONRESPONDERS: How to deal with them? BY Prof. Mohamed Sharaf-Eldin Prof. of Hepatology and Gastroenterology Tanta University Achieving SVR The ability to achieve a
Treatment with the New Direct Acting Antivirals for Hepatitis C
 Treatment with the New Direct Acting Antivirals for Hepatitis C Mary Olson, DNP, ANP-BC Clinical Trials Program Director Weill Cornell Medical College The Center for the Study of Hepatitis C Objectives
Treatment with the New Direct Acting Antivirals for Hepatitis C Mary Olson, DNP, ANP-BC Clinical Trials Program Director Weill Cornell Medical College The Center for the Study of Hepatitis C Objectives
29th Viral Hepatitis Prevention Board Meeting
 29th Viral Hepatitis Prevention Board Meeting Madrid, November 2006 Treatment of chronic hepatitis C José M. Sánchez-Tapias Liver Unit Hospital Clínic University of Barcelona Spain CHRONIC HEPATITIS C
29th Viral Hepatitis Prevention Board Meeting Madrid, November 2006 Treatment of chronic hepatitis C José M. Sánchez-Tapias Liver Unit Hospital Clínic University of Barcelona Spain CHRONIC HEPATITIS C
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
Michael Fried, MD University of North Carolina Chapel Hill, NC. Ira Jacobson, MD Weill Cornell Medical College New York, NY
 Nezam Afdhal, MD Beth Israel Deaconess Medical Center Boston, MA Kim Brown, MD Henry Ford Hospital Detroit, MI Michael Fried, MD University of North Carolina Chapel Hill, NC Jordan Feld, MD Toronto Western
Nezam Afdhal, MD Beth Israel Deaconess Medical Center Boston, MA Kim Brown, MD Henry Ford Hospital Detroit, MI Michael Fried, MD University of North Carolina Chapel Hill, NC Jordan Feld, MD Toronto Western
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
DAAs in the era of decompensated liver disease. Piero L. Almasio University of Palermo
 DAAs in the era of decompensated liver disease Piero L. Almasio University of Palermo piero.almasio@unipa.it HCV therapy in the era of interferon based therapy Priority Compensated cirrhosis Decompensated
DAAs in the era of decompensated liver disease Piero L. Almasio University of Palermo piero.almasio@unipa.it HCV therapy in the era of interferon based therapy Priority Compensated cirrhosis Decompensated
Treatment of chronic hepatitis C virus infection in the near future
 EDITORIAL Treatment of chronic hepatitis c virus infection in the near future., 2013; 12 (6): 00-00 November-December, Vol. 12 No. 6, 2013: 00-00 1 Treatment of chronic hepatitis C virus infection in the
EDITORIAL Treatment of chronic hepatitis c virus infection in the near future., 2013; 12 (6): 00-00 November-December, Vol. 12 No. 6, 2013: 00-00 1 Treatment of chronic hepatitis C virus infection in the
Treatment Targets HCV Genotype 1 & PIs Treating HCV G2&3 Future Therapies. Advances in treatment of HCV Dr John F Dillon
 Treatment Targets HCV Genotype 1 & PIs Treating HCV G2&3 Future Therapies Advances in treatment of HCV Dr John F Dillon Disclosure slide I have received consulting fees and Honoraria from MSD, Abbott,
Treatment Targets HCV Genotype 1 & PIs Treating HCV G2&3 Future Therapies Advances in treatment of HCV Dr John F Dillon Disclosure slide I have received consulting fees and Honoraria from MSD, Abbott,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C First Generation Agents Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Hepatitis C First Generation Agents - Through Preferred
Hepatitis C Virus Treatments: Present and Future
 Hepatitis C Virus Treatments: Present and Future Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD Charles Howell Disclosures Boehringer Ingelheim,
Hepatitis C Virus Treatments: Present and Future Charles D. Howell, M.D., A.G.A.F Professor of Medicine University of Maryland School of Medicine Baltimore, MD Charles Howell Disclosures Boehringer Ingelheim,
Management of HCV Tawesak Tanwandee
 Management of HCV 2016 Tawesak Tanwandee Topics Burden of HCV in our countries Natural history and unmet need for HCV treatment Current treatment as for 2016 Conclusion Evolution from HCV infection to
Management of HCV 2016 Tawesak Tanwandee Topics Burden of HCV in our countries Natural history and unmet need for HCV treatment Current treatment as for 2016 Conclusion Evolution from HCV infection to