UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HCA
|
|
|
- Christiana Atkins
- 5 years ago
- Views:
Transcription
1 UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA
2 DISCLOSURE I have no financial relationship(s) relevant to the content of this CME activity. I will not discuss off-label use of medications.
3 OBJECTIVES EPIDEMIOLOGY OF HCC ETIOLOGY AND PATHOGENISIS OF HCC DIAGNOSIS OF HCC ROLE OF SCREENING FOR HCC DIFFERENT MODALITIES OF TREATMENT ROLE OF MULTIDISCIPLINARY APPROACH IN MANAGING OF PATIENT WITH HCC CONCLUSION AND ANSWERING QUESTIONS
4 HCC IS A MAJOR HEALTH PROBLEM It is the most common type of liver cancer. It is the sixth most common cancer worldwide and It is the 5 th most common malignancy in men and the 8 th in women. Hepatocellular carcinoma is now the third leading cause of cancer-related deaths worldwide, with over 600,000 death annually. It is 2-4 times higher in men than women. 80% of patients with HCC have underlying cirrhosis
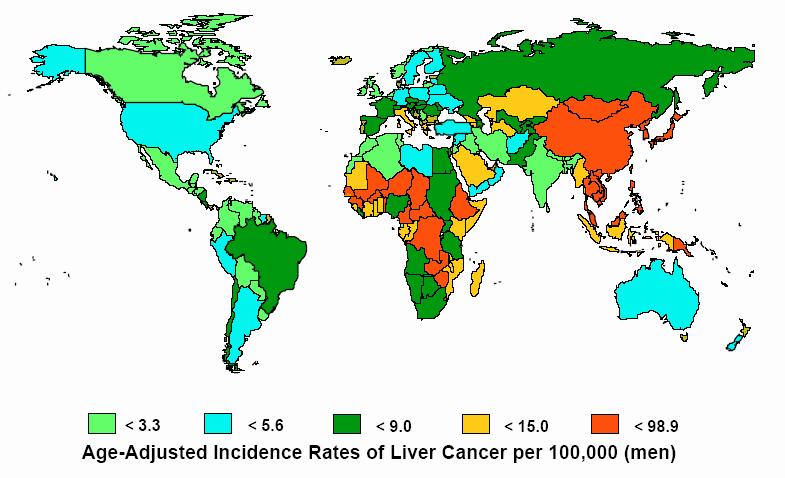
5 GEOGRAPHIC DISTRIBUTION

6 INCIDENCE AND TRENDS

7 GLOBAL VARIATION IN HCC INCIDENCE RATE Venook A P et al. The Oncologist 2010;15:5-13
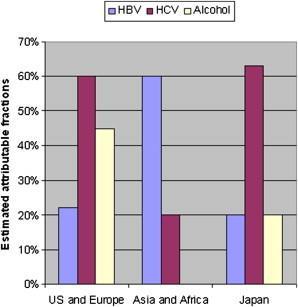
8 EPIDEMIOLOGY
9 INCIDENCE IN THE U.S.
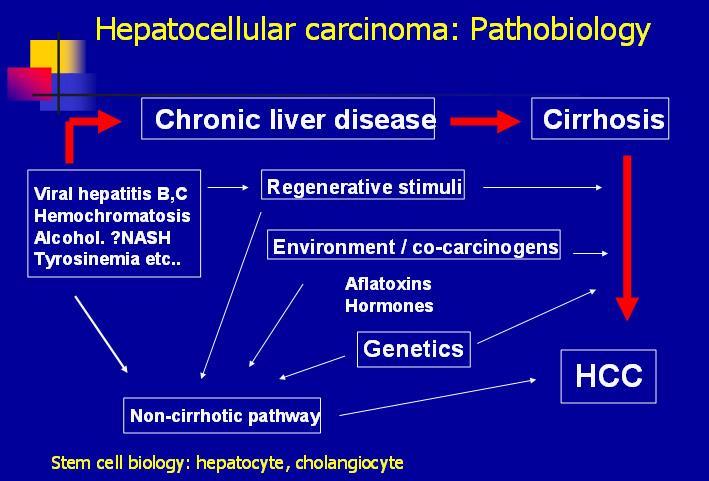
10 ETIOLOGY & PATHOBIOLOGY
11 STAGING OF HCC Staging of HCC American Joint Committee on Cancer-TNM System Stage TNM Scheme I T1N0M0 Single tumor <2cm II T2N0M0 >2cm or single tumor <2cm + vascular invasion IIIA T3N0M0 Single tumor >5cm or >2cm + vascular invasion IIIB T1-3N1M0 Positive Regional Lymph Node IVA T4N0-1M0 Multiple tumors involving major vessels/multiple lobes IVB T1-4N0-1M1 Remote Metastasis Vauthey et al., J Clin Oncol, 2002.
12 DIAGNOSIS 1- Clinical presentation 2- Radiological testing: A) US B) CT C) MRI D) ANGIO D) PET Scan 3- Laboratory 4- Pathology
13 SYMPTOMS Abdominal pain and/or swelling Fatigue/weakness Yellowing of the skin and eyes (jaundice) Darkened urine Nausea/vomiting Unexplained weight loss Loss of appetite Fever Feeling very full after a small meal Itchy skin Enlarged veins under the skin
14 DIAGNOSIS 1- Clinical presentation 2- Radiological testing: A) US B) CT C) MRI D) ANGIO D) PET Scan 3- Tumor markers 4- Pathology
15 ULTRASOUND Advantages: High availability Low cost Non-invasive High Specificity Vascular invasion can be adequately evaluated Limitations: Operator experience Obese patients Low sensitivity Limited differentiation of soft tissue

16 ULTRASOUND Our Patient: Screening Liver Ultrasound Transverse View PACS, BIDMC A hypoechoic rim is visible around the mass
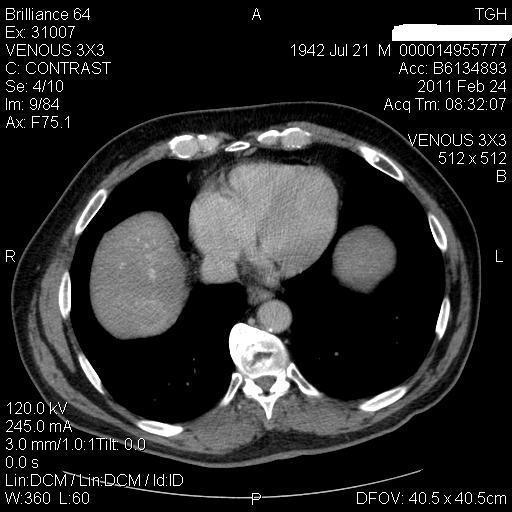
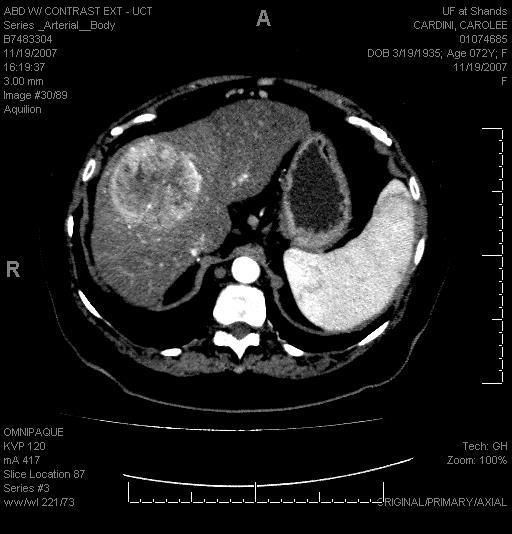
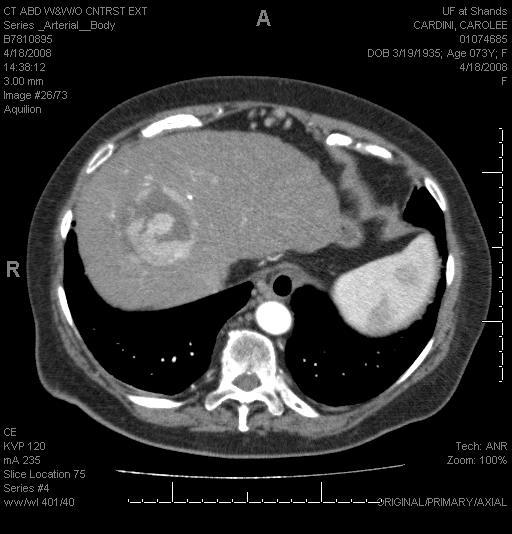
17 CT SCAN ADVANTAGES: 1- It is a highly diagnostic test for HCC. 2- Arterial enhancement and venous washout is highly diagnostic for HCC. 3- A 4-phase study is required for diagnosis. DISADVANTAGES: 1- Limitation includes false negative imaging 2- Contrast toxicity.
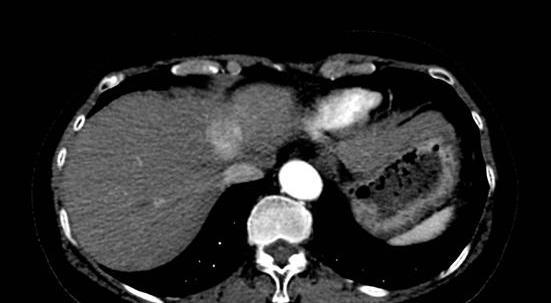
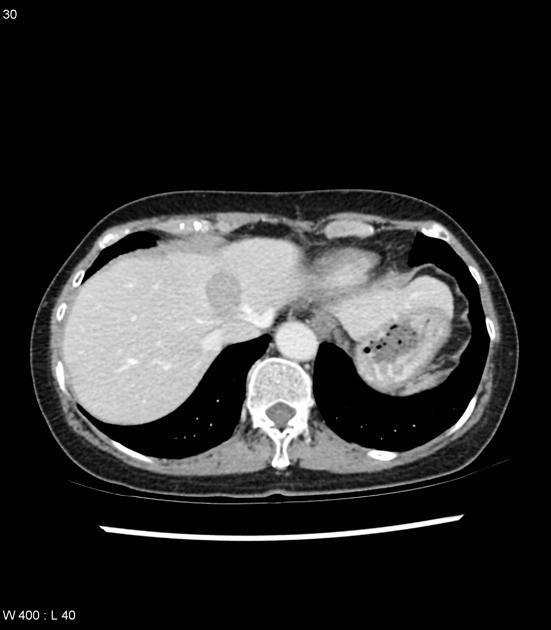
18 CT SCAN
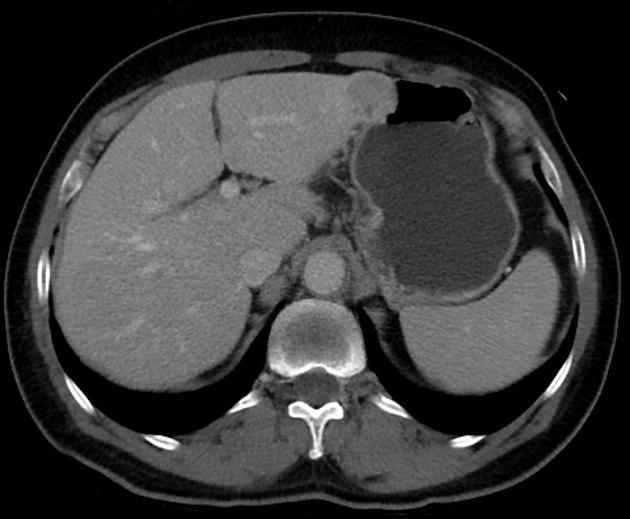
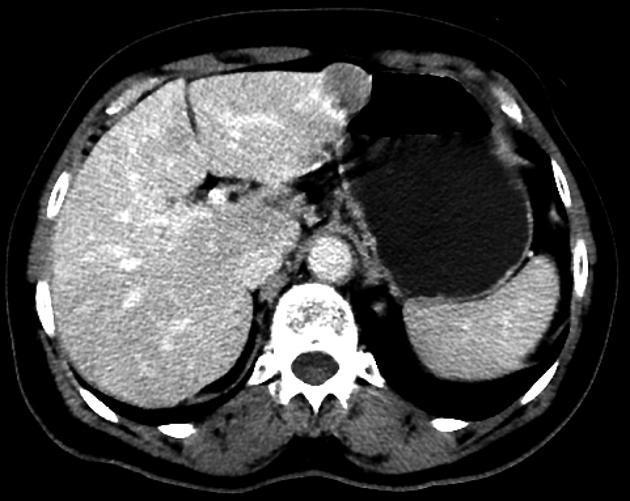
19 CT SCAN
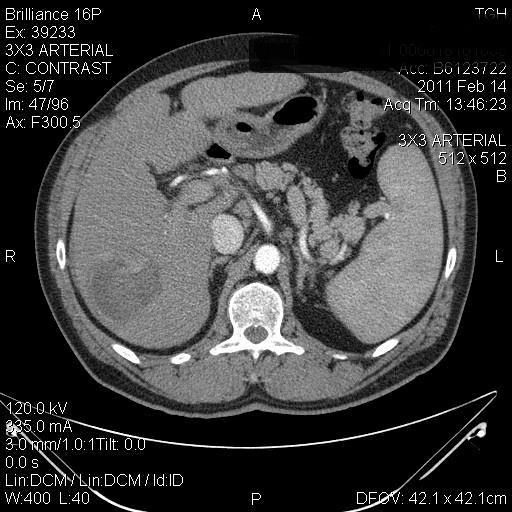
20 CT SCAN
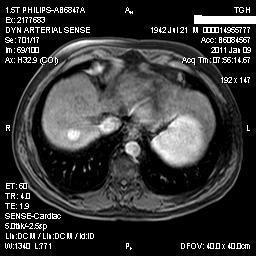
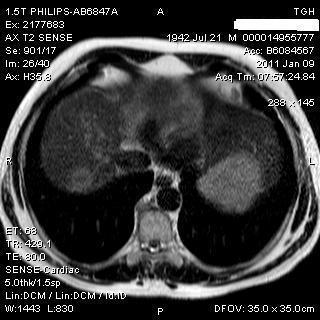
21 MRI Contrast-enhanced MRI is a highly diagnostic test for HCC Advantages: High sensitivity (82-96)% High resolution It has a better diagnostic capability in fatty liver. Limitations: Expensive Contrast allergy Patient Dependent



22 MRI Our Patient: 3 Phase Contrast Enhanced T1 MRI Arterial Phase Portal Venous Phase Delayed Phase PACS, BIDMC Lesion demonstrates enhancement during the arterial phase and washout during the venous phase
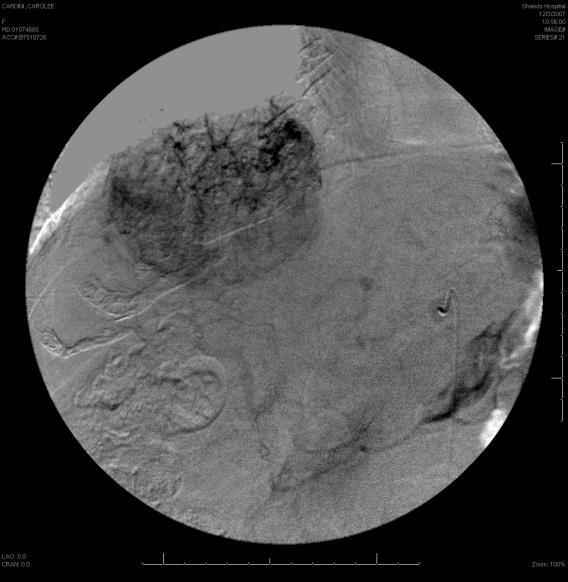
23 ANGIOGRAM ANGIOGRAPHY: 1- It is both a diagnostic and therapeutic test. 2- It has been replaced largely by cross-sectional imaging for diagnostic purposes.

24 IMAGING


25 PET SCAN Our Patient: Normal RN Bone Scan No evidence of MDP avid osseous metastases. Anterior Posterior PACS, BIDMC Bone Scintigraphy: Technetium, 99 Tc m
26 ALPHAFETOPROTEIN Alphafetoprotein (AFP): 1- It is insufficiently sensitive or specific by itself for diagnosis or surveillance. 2- It is useful in conjunction with imaging for follow up and for screening.
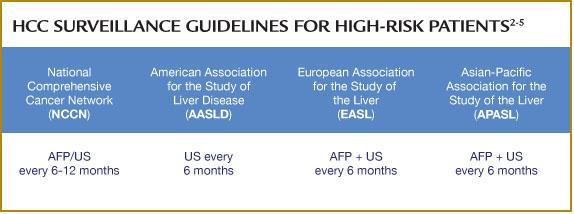
27 SURVEILLANCE
28 HIGH RISK GROUP FOR HCC 1- Hepatitis C cirrhosis. 2- Hepatitis B cirrhosis. 3- African Americans with hepatitis B. 4- Hepatitis B carrier with family history of HCC. 5- Asian male hepatitis B carriers over age Asian female hepatitis B carriers over age Stage 4 primary biliary cirrhosis. 8- Genetic hemochromatosis and cirrhosis. 9- Alpha 1-antitrypsin deficiency and cirrhosis. 10- Other cirrhosis.
29 DIAGNOSTIC ALGORITHM FOR HCC From Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology 2005;42: ; with permission.)
30 TREATMENT 1- Surgical Resection 2- Liver Transplantation 3- Loco-regional treatment: - Trans-arterial Chemo-Embolization - Trans-arterial Radio- Embolization - Ablation by RFA or Microwave - Cyberknife - Cryoablation - Percutaneous Alcohol Injection 6- Chemotherapy 7- Combination
31 SURGICAL RESECTION It is the treatment of choice for HCC in noncirrhotic patients. It can be offered for cirrhotic patients with preserved liver function. The 5-year survival after resection can exceed 50%. Pre or post-resection adjuvant therapy is not recommended.

32 SURGICAL ANATOMY Anatomy: Couinaud Classification

33 SURGICAL ANATOMY
34 SURGICAL RESECTION The Patient is a surgical candidate General condition Liver condition. The tumor is resectable
35 Child-Pugh score Measure 1 point 2 point 3 point Total bilirubin <2 2-3 >3 Serum albumin > <2.8 INR < >2.3 Ascites none mild Moderate to sever Hepatic encephalopathy none Grade I-II Grade III- IV
36 Interpretation OF Child-Pugh score Point Class One year survival Two year survival 5-6 A 100% 85% 7-9 B 81% 57% C 45% 35%
37 Child-Pugh score Measure 1 point 2 point 3 point Total bilirubin <2 2-3 >3 Serum albumin > <2.8 INR < >2.3 Ascites none mild Moderate to sever Hepatic encephalopathy none Grade I-II Grade III- IV
38 MELD SCORE Serum Bilirubin, Creatinine and INR 0.957X Log (serum creatinine) X Log (serum bilirubin) X Log ( INR) X10 Round to the nearest whole number USE OF MELD SCORE: Survival of patients with variceal hemorrhage (TIPS) General surgery outcome Liver transplantation
39 MELD SCORE MELD score is a reliable index in the preoperative evaluation of liver function in cirrhotic patients undergoing partial hepatectomy for hepatocellular carcinoma (HCC)
40 PORTAL HYPERTENTION According to international guidelines [European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD)], portal hypertension (PHTN) is considered a contraindication for liver resection for hepatocellular carcinoma (HCC), and patients should be referred for other treatments
41 PORTAL HYPERTENTION Indeed, the presence of esophageal varices as determined by endoscopy or significant splenomegaly (major diameter >12 cm) with a platelet count of < /mm3 are considered surrogate markers of clinically significant PHTN.
42 SURGICAL RESECTION The Patient is a surgical candidate General condition Liver condition. The tumor is resectable

43 HEPATIC RESECTION

44 HEPATIC RESECTION

45 HEPATIC RESECTION

46 HEPATIC RESECTION

47 HEPATIC RESECTION

48 HEPATIC RESECTION

49 HEPATIC RESECTION

50 HEPATIC RESECTION

51 HEPATIC RESECTION

52 HEPATIC RESECTION

53 HEPATIC RESECTION
54 Liver Transplantation It is an effective treatment for HCC under the following selection criteria: 1- Within Milan Criteria (solitary HCC <5 cm or with up to 3 nodules smaller than 3 cm each). 2- No extra-hepatic malignancy. 3- No vascular invasion. The 5-year survival of these early stage patients exceeds 70%. Pre-transplant TACE/ablation is recommended while the patient on the waiting list.
55 DOWN STAGING PROTOCOL Inclusion Criteria: One tumor above 5 cm and up to 6.5 cm in size Multiple tumors not exceeding total tumor size of 8 cm No vascular invasion No extra-hepatic spread. Down Staging Definition: Tumor shrink to within Milan Criteria or No viable tumor seen on imaging
56 DOWN STAGING PROTOCOL Listing Criteria: Tumor must be within successful down stage definition. Must be maintained within the down stage definition for at least 3 month. The AFP must be either decreasing and maintained at a level < 400 ng/mi at the time of listing. No evidence of extra-hepatic disease. Imaging and AFP to be done at 3 month intervals while on the list.
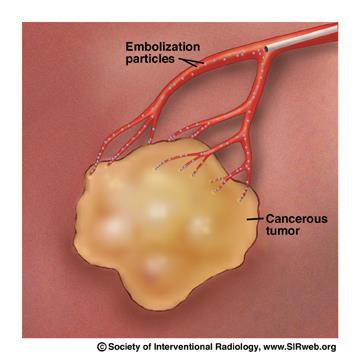

57 CHEMOEMBOLIZATION
58 CHEMOEMBOLIZATION Beads block the capillaries and chemo leaks out causing more regional cell death. Doxorubicin cell death increases with hypoxia, embolization cuts off arterial supply and oxygen and they have a SYNERGISTIC effect. TACE is recommended as first line non-curative therapy for non-surgical patients with large/ multifocal HCC who do not have vascular invasion or extrahepatic spread.
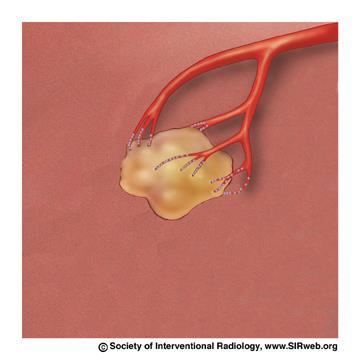
59 CHEMOEMBOLIZATION Pre embolization, HCC Post embolization, HCC
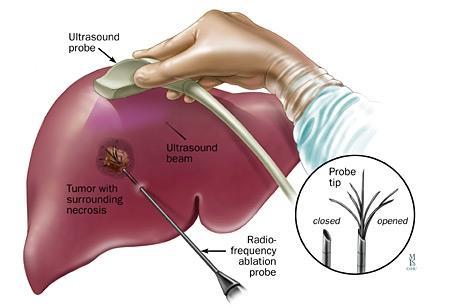
60 RADIOFREQUENCY ABLATION

61 HOW IT WORKS
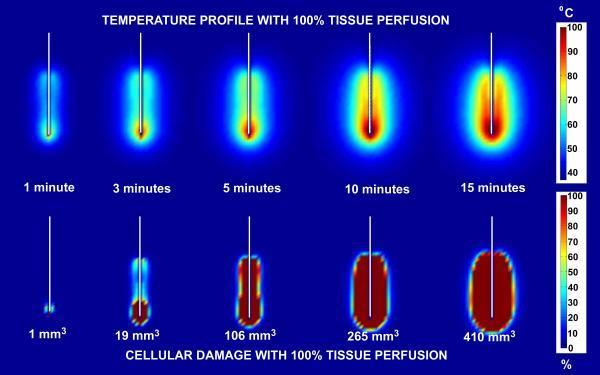
62 RADIOFREQUENCY ABLATION


63 RADIOFREQUENCY ABLATION To combat the physical limitations of a single probe several designs have been constructed. Leveen RF probe with umbrella shaped array RITA probe also has umbrella shaped array and allows infusion of saline through 4 tines Triangular shaped configuration
64 RADIOFREQUENCY ABLATION Local ablation is safe and effective therapy for patients who cannot undergo resection, or as a bridge to transplantation. Patients with HCC lesions < 2 cm subject to RFA showed a 5-year survival of 70%, comparable to that of surgical resection in optimal candidates. It is not recommended for subscapsular location and poor tumor differentiation.
65 RADIOFREQUENCY ABLATION Cons Grounding pads necessary (which can cause skin burns) Destroys tissue planes in heat field Not recommended for subcapsular lesions or close to skin Painful, usually requiring general anesthesia Very susceptible to heat sink
66 MICROWAVE ABLATION Principles of tissue heating and cell death are exactly the same as RF Probes are needle shaped and radiate MW away from the probe Size of burn is dependent on probe size Larger burns (6-7 cm) require very large probes up to 1 cm in diameter Probe technology is not perfected, early probes made teardrop shaped burns due to deflection from needle and wave-wave interactions
67 MICROWAVE ABLATION When a proper probe is used the burn is very consistent and has very little, maybe no, heat sink effect due to high energy deposition in short amount of time Shorter burn times
68 ADVANTAGES OF MICROWAVE ABLATION Does not require grounding pads No gas tanks required (cryo) Has great potential and will likely replace RF if probe size can be decreased eventually sorry LeVeen
69 SORAFENIB Sorafenib is recommended by the NCCN for the following patients with unresectable HCC and have Child-Pugh A or B disease a,b Not transplant candidates Inoperable by performance status or comorbidity, local disease only Metastatic disease
70 Sorafenib Targets Tumor Cell Proliferation and Angiogenesis Tumor Cell Endothelial Cell or Pericyte RAS HGF Apoptosis Autocrine loop Paracrine stimulation PDGFR-b PDGF-b RAS VEGF VEGFR-2 RAF MEK ERK Mcl-1 Nucleus HIF Sorafenib HGF PDGF Mitochondria VEGF Proliferation Survival RAF Mitochondria MEK Apoptosis ERK Nucleus Sorafenib Angiogenesis: Differentiation Proliferation Migration Tubule formation HGF = hepatocyte growth factor. Avila MA, et al. Oncogene. 2006;25: ; Liu L, et al. Cancer Res. 2006;66: ; Semela D, et al. J Hepatol. 2004;41: ; Wilhelm SM, et al. Cancer Res. 2004;64:
71 CLINICAL TRIAL Data from Llovet JM, et al. N Engl J Med. 2008;359:
72 Sorafenib in HCC Overall Conclusions Sorafenib prolonged OS vs. placebo in advanced HCC 1,2,3-44% increase in OS in the SHARP trial - 47% increase in OS in the Asia Pacific Trial Sorafenib prolonged TTP vs placebo 1,2,3-73% prolongation in TTP in the SHARP trial - 74% prolongation in TTP in the Asia Pacific Trial In both SHARP & AP phase III trials the AEs reported in patients on Sorafenib were predominantly grade 1 and 2 in severity and gastrointestinal, constitutional, and dermatologic in nature 2,3
73 Llovet JM, et al. J Natl Cancer Inst. 2008;100: BCLC Staging System and Treatment Strategy HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST >2, Child Pugh C Very early stage (0) Early stage (A) 1 HCC <2cm 1 HCC or 3 nodules Carcinoma in situ <3cm, PST 0 Intermediate stage (B) Multinodular, PST 0 Advanced stage (C) Portal invasion, N1, M1, PST 1 2 End stage (D) 1 HCC Portal pressure/ bilirubin Increased 3 nodules 3cm Associated diseases Normal No Yes Resection Liver transplantation Curative treatments PEI/RFA TACE Sorafenib Randomised controlled trials Symptomatic treatment
74 KEYS FOR SUCCESSFUL TREATMENT OF HCC Screening and early detection Early referral Early implication of the the most appropriate treatment Treatment using multidisciplinary approach
75 MULTIDISCIPLINARY APPROACH CENTER Radiology Oncology Hepatology Hepatobiliary surgery Coordinator Pathology Hospitalist PCP/GI Transplantation surgery
76 CONCLUSION HCC has become a cancer that can be prevented, detected at early stage, and effectively treated. Patients who are at high risk for developing HCC should be entered into surveillance programs. The BCLC staging system is effective and widely used both for staging and treatment allocation. Even though we are getting better results from TACE, RFA,MICROWAIVE ablation and PEI, individually or in combinations. Surgical resection and liver transplantation remains as the only curative modalities for treating HCC.
77 CONCLUSION Sorafenib is recommended as first line option in patients who can not benefit from resection, transplantation, ablation or TACE and still have preserved liver function. The best results can be achieved for patients with HCC when their management carried by a MULTI-DISCIPLINARY TEAM USING A MULTI- DISCIPLINARY APPROACH.
78 THANK YOU?

79 WAITING TIME ON THE LIVER TRANSPLANT LIST BY REGION
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Nexavar in advanced HCC: a paradigm shift in clinical practice
 Nexavar in advanced HCC: a paradigm shift in clinical practice Tim Greten Hanover Medical School, Germany Histopathological progression and molecular features of HCC Chronic liver disease Liver cirrhosis
Nexavar in advanced HCC: a paradigm shift in clinical practice Tim Greten Hanover Medical School, Germany Histopathological progression and molecular features of HCC Chronic liver disease Liver cirrhosis
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Tumor incidence varies significantly, depending on geographical location.
 Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC
: Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC") Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
TREATMENT ALGORITHM FOR HEPATOCELLULAR CARCINOMA
 HCC treatment : A permanent challenge! TREATMENT ALGORITHM FOR HEPATOCELLULAR CARCINOMA Michel Ducreux, MD, PhD Paul Brousse University Hospital Gustave Roussy Institute Villejuif, FRANCE A low level of
HCC treatment : A permanent challenge! TREATMENT ALGORITHM FOR HEPATOCELLULAR CARCINOMA Michel Ducreux, MD, PhD Paul Brousse University Hospital Gustave Roussy Institute Villejuif, FRANCE A low level of
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines
 Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Selection Criteria and Insertion of SIRT into HCC Treatment Guidelines 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore Pierce Chow FRCSE PhD SIRT in
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatocellular carcinoma: from guidelines to individualized treatment
 AISF 2012 Rome, 22-24 February 2012 Hepatocellular carcinoma: from guidelines to individualized treatment A.D. 1088 Luigi Bolondi Professor of Medicine, Chairman Department of Digestive Diseases and Internal
AISF 2012 Rome, 22-24 February 2012 Hepatocellular carcinoma: from guidelines to individualized treatment A.D. 1088 Luigi Bolondi Professor of Medicine, Chairman Department of Digestive Diseases and Internal
Management of HepatoCellular Carcinoma
 9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Hepatocellular Carcinoma: Transplantation, Resection or Ablation?
 Hepatocellular Carcinoma: Transplantation, Resection or Ablation? Roberto Gedaly MD Chief, Abdominal Transplantation Transplant Service Line University of Kentucky Nothing to disclose Disclosure Objective
Hepatocellular Carcinoma: Transplantation, Resection or Ablation? Roberto Gedaly MD Chief, Abdominal Transplantation Transplant Service Line University of Kentucky Nothing to disclose Disclosure Objective
Hepatocellular Carcinoma (HCC)
") Title Slide Hepatocellular Carcinoma (HCC) Professor Muhammad Umar MBBS, MCPS, FCPS (PAK), FACG (USA), FRCP (L), FRCP (G), ASGE-M(USA), AGAF (USA) Chair & Professor of Medicine Rawalpindi Medical College
Title Slide Hepatocellular Carcinoma (HCC) Professor Muhammad Umar MBBS, MCPS, FCPS (PAK), FACG (USA), FRCP (L), FRCP (G), ASGE-M(USA), AGAF (USA) Chair & Professor of Medicine Rawalpindi Medical College
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS?
 IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA. Shawn Pelletier, MD
 TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
6/16/2016. Treating Hepatocellular Carcinoma: Deciphering the Clinical Data. Liver Regeneration. Liver Regeneration
 Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Liver transplantation: Hepatocellular carcinoma
 Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Hepatocellular Carcinoma
 Hepatocellular Carcinoma Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Louisville & Louisville VAMC 2010 Magnitude of the Problem 95% of
Hepatocellular Carcinoma Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology, & Nutrition University of Louisville & Louisville VAMC 2010 Magnitude of the Problem 95% of
Percutaneous ablation: indications, techniques and results
 Percutaneous ablation: indications, techniques and results Giovan Giuseppe Di Costanzo Dipartimento dei Trapianti UOSC Epatologia AORN A Cardarelli - Napoli Treatment algorithm EASL, EORTC guidelines HCC
Percutaneous ablation: indications, techniques and results Giovan Giuseppe Di Costanzo Dipartimento dei Trapianti UOSC Epatologia AORN A Cardarelli - Napoli Treatment algorithm EASL, EORTC guidelines HCC
Surveillance for HCC Who, how Diagnosis of HCC Surveillance for HCC in Practice
 Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Liver Cancer And Tumours
 Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Guidelines for SIRT in HCC An Evolution
 Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
The Management of Advanced Stage Hepatocellular Carcinoma
 The Management of Advanced Stage Hepatocellular Carcinoma Pierce K.H Chow MD PhD Professor, Duke-NUS Graduate Medical School Singapore Senior Consultant Surgeon, National Cancer Center Singapore Senior
The Management of Advanced Stage Hepatocellular Carcinoma Pierce K.H Chow MD PhD Professor, Duke-NUS Graduate Medical School Singapore Senior Consultant Surgeon, National Cancer Center Singapore Senior
Disclosure. Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report:
 Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
Disclosure Speaker name: Prof. Maciej Pech I have the following potential conflicts of interest to report: Consulting Employment in industry Stockholder of a healthcare company Owner of a healthcare company
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung
 How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
3/22/2017. I will be discussing off label/investigational use of tivantinib for hepatocellular carcinoma.
 Grant/Research Support - AbbVie, Conatus, Hologic, Intercept, Genfit, Gilead, Mallinckrodt, Merck, Salix, Shire, Vital Therapies Consultant AbbVie, Gilead, Merck Member, Scientific Advisory Board Vital
Grant/Research Support - AbbVie, Conatus, Hologic, Intercept, Genfit, Gilead, Mallinckrodt, Merck, Salix, Shire, Vital Therapies Consultant AbbVie, Gilead, Merck Member, Scientific Advisory Board Vital
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis?
 of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis?") Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis? Poster No.: C-1634 Congress: ECR 2014 Type: Authors: Keywords: DOI:
Trans-arterial radioembolisation (TARE) of unresectable HCC using Y-90 microspheres: is it dangerous in case of portal vein thrombosis? Poster No.: C-1634 Congress: ECR 2014 Type: Authors: Keywords: DOI:
The Focal Hepatic Lesion: Radiologic Assessment
 The Focal Hepatic Lesion: Radiologic Assessment Kevin Kuo, Harvard Medical School Year III Our Patient: PS 67 y/o female w/ long history of alcohol use Drinking since age 18, up to one bottle of wine/day
The Focal Hepatic Lesion: Radiologic Assessment Kevin Kuo, Harvard Medical School Year III Our Patient: PS 67 y/o female w/ long history of alcohol use Drinking since age 18, up to one bottle of wine/day
Clinical Staging for Hepatocellular Carcinoma: Eastern Perspectives. Osamu Yokosuka, M.D. Graduate School of Medicine, Chiba University, Chiba, Japan
 Clinical Staging for Hepatocellular Carcinoma: Eastern Perspectives Osamu Yokosuka, M.D. Graduate School of Medicine, Chiba University, Chiba, Japan Why is staging system important? Cancer stage can be
Clinical Staging for Hepatocellular Carcinoma: Eastern Perspectives Osamu Yokosuka, M.D. Graduate School of Medicine, Chiba University, Chiba, Japan Why is staging system important? Cancer stage can be
Hepatocellular carcinoma in Sri Lanka - where do we stand?
 SCIENTIFIC ARTICLE Hepatocellular carcinoma in Sri Lanka - where do we stand? R.C. Siriwardana 1, C.A.H. Liyanage 1, M.B. Gunethileke 2 1. Specialist Gastrointestinal and Hepatobilliary Surgeon, Senior
SCIENTIFIC ARTICLE Hepatocellular carcinoma in Sri Lanka - where do we stand? R.C. Siriwardana 1, C.A.H. Liyanage 1, M.B. Gunethileke 2 1. Specialist Gastrointestinal and Hepatobilliary Surgeon, Senior
HCC RADIOLOGIC DIAGNOSIS
 UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma
 Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA*
 UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
9th Paris Hepatitis Conference
 9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
RESEARCH ARTICLE. Validation of The Hong Kong Liver Cancer Staging System in Patients with Hepatocellular Carcinoma after Curative Intent Treatment
 DOI:10.22034/APJCP.2017.18.6.1697 RESEARCH ARTICLE Validation of The Hong Kong Liver Cancer Staging System in Patients with Hepatocellular Carcinoma after Curative Intent Treatment Alan Chuncharunee 1,
DOI:10.22034/APJCP.2017.18.6.1697 RESEARCH ARTICLE Validation of The Hong Kong Liver Cancer Staging System in Patients with Hepatocellular Carcinoma after Curative Intent Treatment Alan Chuncharunee 1,
Liver Tumors. Patient Education. Treatment options 8 4A. About the Liver. Surgical Specialties
 Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
NAACCR Webinar Series 1
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
Assessment of Liver Function: Implications for HCC Treatment
 Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Recognizing the high prevalence of hepatocellular carcinoma
 SPECIAL COMMUNICATION Saudi Gastroenterology Association Guidelines for the Diagnosis and Management of Hepatocellular Carcinoma: Summary of Recommendations Guidelines Editors: Ayman A Abdo, Huda Al Abdul
SPECIAL COMMUNICATION Saudi Gastroenterology Association Guidelines for the Diagnosis and Management of Hepatocellular Carcinoma: Summary of Recommendations Guidelines Editors: Ayman A Abdo, Huda Al Abdul
SIRTEX Lunch Symposium, Cebu, 23 Nov Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong
 SIRTEX Lunch Symposium, Cebu, 23 Nov 2013 Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong I will not talk on Mechanism of SIRT Data on efficacy of SIRT Epidemiology
SIRTEX Lunch Symposium, Cebu, 23 Nov 2013 Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong I will not talk on Mechanism of SIRT Data on efficacy of SIRT Epidemiology
Saudi Gastroenterology Association Guidelines for the Diagnosis and Management of Hepatocellular Carcinoma: Summary of Recommendations
 Special Communication Saudi Gastroenterology Association Guidelines for the Diagnosis and Management of Hepatocellular Carcinoma: Summary of Guidelines Editors: Ayman A Abdo, Huda Al Abdul Karim, Turki
Special Communication Saudi Gastroenterology Association Guidelines for the Diagnosis and Management of Hepatocellular Carcinoma: Summary of Guidelines Editors: Ayman A Abdo, Huda Al Abdul Karim, Turki
Sorafenib in HCC. Discussion points
 Discussion points in Andrew X. Zhu, MD, PhD 214 CASL Meeting-Consensus, Controversies and Future Directions in -data from phase III trials ptimal Dosing Side effects and management strategies use in Child-Pugh
Discussion points in Andrew X. Zhu, MD, PhD 214 CASL Meeting-Consensus, Controversies and Future Directions in -data from phase III trials ptimal Dosing Side effects and management strategies use in Child-Pugh
Liver 6/5/14. Collecting Cancer Data: Liver NAACCR Webinar Series. June 5, 2014
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC
 Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
Dr Apoorva Gogna MBBS FRCR FAMS Consultant Interventional Radiology Center Department of Diagnostic Radiology SingaporeGeneral Hospital MULTI-DISCIPLINARY MANAGEMENT OF INTERMEDIATE STAGE HCC CASE HISTORY
HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT
 HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT INTRODUCTION: Hepatocellular carcinoma (HCC): Fifth most common cancer worldwide Third most common cause of cancer mortality In Egypt: 2.3%
HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT INTRODUCTION: Hepatocellular carcinoma (HCC): Fifth most common cancer worldwide Third most common cause of cancer mortality In Egypt: 2.3%
Treatment of Hepatocellular Carcinoma. Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center
 Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
In- and exclusion criteria
 In- and exclusion criteria Kerstin Schütte Department of Gastroenterology, Hepatology and Infectious Diseases University of Magdeburg Overview: Study population Inclusion criteria I - General criteria
In- and exclusion criteria Kerstin Schütte Department of Gastroenterology, Hepatology and Infectious Diseases University of Magdeburg Overview: Study population Inclusion criteria I - General criteria
First-line therapy for unresectable HCC:
 ESMO GI Cancer Preceptorship 15 November 2017 Singapore First-line therapy for unresectable HCC: an oncologist s viewpoint Chiun Hsu, MD, PhD G raduate I n stitute of Oncology, National Taiwan Univers
ESMO GI Cancer Preceptorship 15 November 2017 Singapore First-line therapy for unresectable HCC: an oncologist s viewpoint Chiun Hsu, MD, PhD G raduate I n stitute of Oncology, National Taiwan Univers
Treatment of HCC in real life-chinese perspective
 Treatment of HCC in real life-chinese perspective George Lau MBBS (HK), MRCP(UK), FHKCP, FHKAM (GI), MD(HK), FRCP (Edin, Lond), FAASLD (US) Chairman Humanity and Health Medical Group, Hong Kong SAR, CHINA
Treatment of HCC in real life-chinese perspective George Lau MBBS (HK), MRCP(UK), FHKCP, FHKAM (GI), MD(HK), FRCP (Edin, Lond), FAASLD (US) Chairman Humanity and Health Medical Group, Hong Kong SAR, CHINA
Il treatment plan nella terapia sistemica dell epatocarcinoma
 Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
RESEARCH ARTICLE. Real Life Treatment of Hepatocellular Carcinoma: Impact of Deviation from Guidelines for Recommended Therapy
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.16.6929 Real-Life HCC Treatment - Influence on Outcome of Deviation from Therapy Guidelines RESEARCH ARTICLE Real Life Treatment of Hepatocellular Carcinoma:
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.16.6929 Real-Life HCC Treatment - Influence on Outcome of Deviation from Therapy Guidelines RESEARCH ARTICLE Real Life Treatment of Hepatocellular Carcinoma:
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Comprehensive Treatment of Advanced Liver Cancer Complicated with Upper Gastrointestinal Bleeding in Multidisciplinary Team Model: A Case Report
 Journal of Surgery 2017; 5(3): 47-52 http://www.sciencepublishinggroup.com/j/js doi: 10.11648/j.js.20170503.13 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Report Comprehensive Treatment of Advanced
Journal of Surgery 2017; 5(3): 47-52 http://www.sciencepublishinggroup.com/j/js doi: 10.11648/j.js.20170503.13 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Report Comprehensive Treatment of Advanced
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
9/10/2018. Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? DISCLOSURES
: What is New? DISCLOSURES") UCSF Transplant 2018: Pioneering Advances in Transplantation DISCLOSURES Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? I have no relevant commercial interests or relationships to report
UCSF Transplant 2018: Pioneering Advances in Transplantation DISCLOSURES Liver Transplant for Hepatocellular Carcinoma (HCC): What is New? I have no relevant commercial interests or relationships to report
Sorafenib for Egyptian patients with advanced hepatocellular carcinoma; single center experience
 Journal of the Egyptian National Cancer Institute (2014) 26, 9 13 Cairo University Journal of the Egyptian National Cancer Institute www.nci.cu.adu.eg www.sciencedirect.com Original article Sorafenib for
Journal of the Egyptian National Cancer Institute (2014) 26, 9 13 Cairo University Journal of the Egyptian National Cancer Institute www.nci.cu.adu.eg www.sciencedirect.com Original article Sorafenib for
Interventional Radiologic Treatment of Hepatocellular Carcinoma
 Interventional Radiologic Treatment of Hepatocellular Carcinoma Fatih Boyvat Abstract The current treatment modalities for patients with hepatocellular carcinoma are discussed in this review. Hepatocellular
Interventional Radiologic Treatment of Hepatocellular Carcinoma Fatih Boyvat Abstract The current treatment modalities for patients with hepatocellular carcinoma are discussed in this review. Hepatocellular
Advances in percutaneous ablation for hepatocellular carcinoma
 Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
Advances in percutaneous ablation for hepatocellular carcinoma P. Nahon1,2,3 1 Hepatology, Jean Verdier Hospital, APHP, Bondy, France 2 Paris 13 university, Sorbonne Paris Cité, UFRSMBH, Bobigny, France
AllinaHealthSystems 1
 Disclosure I have no financial relationships to disclose. Dimensions in Oncology 2017 Liver Cancers Jill May, BSN, RN, OCN Hepatobiliary Cancer Care Coordinator 1 LIVER ~ Where and what is it? Located
Disclosure I have no financial relationships to disclose. Dimensions in Oncology 2017 Liver Cancers Jill May, BSN, RN, OCN Hepatobiliary Cancer Care Coordinator 1 LIVER ~ Where and what is it? Located
LiverGroup.org. Case Report Form (CRF) for STAGED procedures
 for STAGED procedures") Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Latest Developments in the Treatment of Hepatocellular Carcinoma
 Latest Developments in the Treatment of Hepatocellular Carcinoma Roniel Cabrera, MD MS Associate Professor of Medicine Director of Hepatology and Medical Director of Liver Transplantation Division of Gastroenterology,
Latest Developments in the Treatment of Hepatocellular Carcinoma Roniel Cabrera, MD MS Associate Professor of Medicine Director of Hepatology and Medical Director of Liver Transplantation Division of Gastroenterology,
Resection leads to cure in selected patients with hepatocellular
 Overview: Where Does Radiation Therapy Fit in the Spectrum of Liver Cancer Local-Regional Therapies? Laura A. Dawson, MD*, Experience with radiation therapy for the treatment of hepatocellular carcinoma
Overview: Where Does Radiation Therapy Fit in the Spectrum of Liver Cancer Local-Regional Therapies? Laura A. Dawson, MD*, Experience with radiation therapy for the treatment of hepatocellular carcinoma
HCC: SURVEILLANCE AND MANAGEMENT
 HCC: SURVEILLANCE AND MANAGEMENT Hillel Tobias, MD PhD Professor of Medicine and Surgery Medical Director, Liver Transplant Service New York University Langone Medical Center Normal hepatocytes - - - -
HCC: SURVEILLANCE AND MANAGEMENT Hillel Tobias, MD PhD Professor of Medicine and Surgery Medical Director, Liver Transplant Service New York University Langone Medical Center Normal hepatocytes - - - -
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 )
") 蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 ) 1 Sorafenib Improves Survival in Hepatocellular Carcinoma: Results of a Phase III Randomized, -Controlled Trial Josep M. Llovet, Sergio Ricci, Vincenzo Mazzaferro, Philip
蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 ) 1 Sorafenib Improves Survival in Hepatocellular Carcinoma: Results of a Phase III Randomized, -Controlled Trial Josep M. Llovet, Sergio Ricci, Vincenzo Mazzaferro, Philip
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Liver Directed Therapy for Hepatocellular Carcinoma
 Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Liver Directed Therapy for Hepatocellular Carcinoma Anil K Pillai MD, FRCR, Associate Professor, Department of Radiology UT Houston Health Science Center, Houston, TX, United States. Hepatocellular cancer
Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting?
 Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Surgical management of HCC. Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London
 Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
State-of-the-art minimally invasive interventions for liver tumors
 William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD State-of-the-art minimally invasive interventions for liver tumors William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD
William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD State-of-the-art minimally invasive interventions for liver tumors William Lo, HMS MD/PhD candidate, MS III Gillian Lieberman, MD
Unmet needs in intermediate HCC. Korea University Guro Hospital Ji Hoon Kim
 Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Therapeutic Response Assessment and Endpoints in HCC
 APASL HCC Conference, 2013 Cebu Therapeutic Response Assessment and Endpoints in HCC Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Surgery Chief of Hepatobiliary and Pancreatic Surgery The University
APASL HCC Conference, 2013 Cebu Therapeutic Response Assessment and Endpoints in HCC Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Surgery Chief of Hepatobiliary and Pancreatic Surgery The University
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days
 94% of radiation delivered within 11 days") 100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD
 UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
UNIVERSITY OF PRETORIA STEVE BIKO ACADEMIC HOSPITAL SOUTH AFRICA TRANSEARTERIAL CHEMO- EMBOLIZATION FOR HEPATIC METASTASES FROM NEURO-ENDOCINE NEOPLASIA AND HEPATOMA DR SAMIA AHMAD 1 INTRODUCTION Hepatic
Surgical resection for hepatocellular carcinoma (HCC)
") Surgical resection for hepatocellular carcinoma (HCC) Wojciech G Polak, MD, PhD, FEBS Department of Surgery, Division of HPB and Transplant Surgery, Erasmus MC, University Medical Center Rotterdam the
Surgical resection for hepatocellular carcinoma (HCC) Wojciech G Polak, MD, PhD, FEBS Department of Surgery, Division of HPB and Transplant Surgery, Erasmus MC, University Medical Center Rotterdam the
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Optimal management of HCC: in Asia
 Optimal management of HCC: in Asia Kwang-Hyub Han, MD Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea Newly diagnosed HCC : > 70% occur
Optimal management of HCC: in Asia Kwang-Hyub Han, MD Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea Newly diagnosed HCC : > 70% occur
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting