Eastern Health and Social Services Board Palliative Care
|
|
|
- Amelia Wood
- 5 years ago
- Views:
Transcription
1 Eastern Health and Social Services Board Palliative Care Out of Hours Symptom advice leaflets Adult Palliative care patients (Compiled by Macmillan GP Facilitators March 2008) 1
2 CONTENTS PAIN Control of Pain in Patients with Cancer 3 Treatment of Pain WHO analgesic ladder 4 Morphine 5 Diamorphine parenteral administration 6 Alternative Opioids 7 Management of Pain, Patient unable to take oral medication, 8 no pain at present/pain currently controlled Management of Pain, Patient unable to take oral medication, 9 experiencing pain Transdermal analgesia 10 Transdermal analgesia conversion guides 11 Opioid Conversion guides 12 SYRINGE DRIVER GUIDELINES 13/14 NAUSEA AND VOMITING 15 AGITATION AND RESTLESSNESS IN THE END STAGES OF LIFE 16 MANAGEMENT OF NOISY SECRETIONS 17 NICaN POST-CHEMOTHERAPY GUIDELINES 18/19 USEFUL OUT OF HOURS CONTACTS 20 Reference 20 2
3 Control of Pain in Patients with Cancer Assessment of Pain Pain not purely physical may include: 1 psychological 2 social 3 cultural 4 financial 5 spiritual aspects Assessment, includes: 1. History from the patient and determine: Number and site of pain(s) Intensity / severity of pain(s) Radiation of pain Timing of pain Duration of pain Quality of pain Aggravating / relieving factors / sensory disturbances / associated power loss Type of pain e.g. neuropathic, visceral, somatic or mixed Analgesic drug history including dose and route of administration Impact of psychological factors e.g. anxiety or depression Effect on activities of daily living. 2. Carry out a physical examination 3. Identify the likely cause of pain 4. Arrange for appropriate diagnostic investigations. 5. Arrange for multidisciplinary professional assessment to include physiotherapy and occupational therapy. 6. Review frequently for effectiveness and / or adverse effects of medication 3
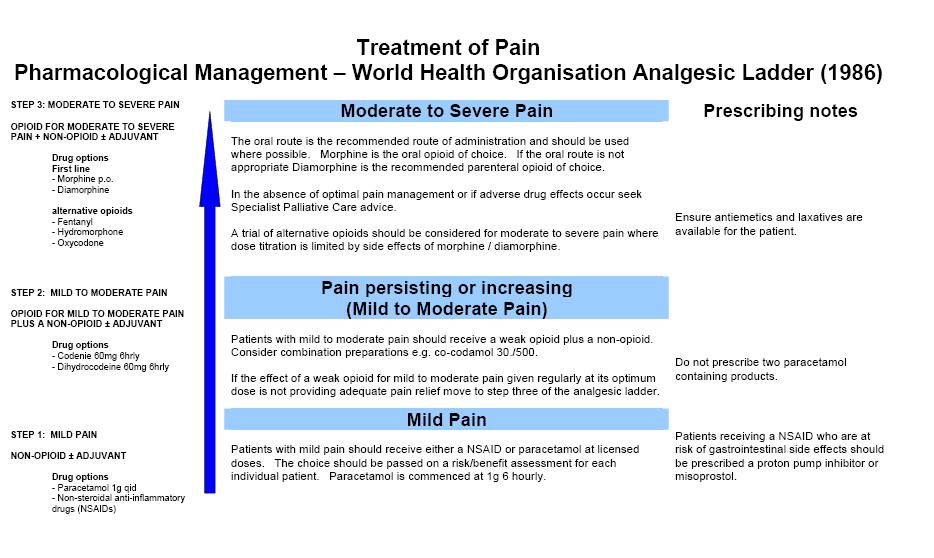
4 4
5 MORPHINE Initiating and Titrating Oral Morphine When initiating normal release morphine (ie Sevredol/Oramorph), start with 5-10mg orally at four hourly intervals (six times in 24 hours) with access to prn dosing, (Cautions: Patients with renal impairment or the elderly and frail may require reduced dose or alternative opioid.) Each day assess the pain control, severity of side effects and total amount of morphine required, including breakthrough doses, in the previous 24 hours. Divide the total amount required in the previous 24 hours by six. Prescribe this dose every four hours and alter the breakthrough analgesia dose accordingly (this is the same as the four hourly dose) i.e. one sixth of the total daily regular morphine dose. If a patient is unable or unwilling to use breakthrough doses but is still in pain, the dose of normal release morphine prescribed four hourly should be increased. The increase depends on the individual but is usually in 30-50% increments. If still in pain after 2-3 doses have been taken, increase by one third to one half. Caution: Pain may not be opioid sensitive and adjuvants may need to be considered. Once suitable pain control is achieved by the use of normal release morphine, conversion to the same total daily dose of modified release morphine (MST or MXL) should be considered e.g. normal release morphine 5mg 4 hourly = 30mg in 24 hours = MST 15mg bd = MXL 30mg od. If pain control is not achieved in 48 hours or there are excessive side effects, contact your local Specialist Palliative Care Team for advice. Specialist Palliative Medical advice is recommended when initiating analgesic therapy in patients who have renal impairment, are on dialysis or are stopping dialysis. OPIOID TOXICITY: Presence of confusion, drowsiness, myoclonic jerks and often pin-point pupils. Can occur when dose has been markedly increased OR when renal failure ensues and active metabolites accumulate.
6 DIAMORPHINE PARENTERAL ADMINISTRATION Patients requiring parenteral opioids (i.e. a patient who is vomiting or unable to swallow) should receive the appropriate dose of diamorphine via the subcutaneous route. To calculate the 24 hour dose of subcutaneous diamorphine, divide the total 24 hour oral dose of morphine by three (see chart page 12). Administer this dose of diamorphine subcutaneously in syringe driver over 24 hours. Patient should also be prescribed appropriate breakthrough dose of subcutaneous Diamorphine (i.e. 1/6 of 24 hour diamorphine dose) Breakthrough analgesia (prn dosing) Every patient on an opioid should have access to breakthrough analgesia (i.e. 1/6 of total daily opioid dose) Following the delivery of oral breakthrough analgesia, wait 30 minutes to assess the response. If pain persists, repeat analgesia and reassess in a further 30 minutes. If pain still persists, full reassessment of the patient is required. 6
7 ALTERNATIVE OPIOIDS OXYCODONE 90% metabolised by the Liver and 10% metabolised by the kidneys. Accumulates less than morphine in patients with renal failure. Immediate release oral preparation: OxyNorm capsules and liquid titrated every 4-6 hours Modified release oral preparation: OxyContin tablet titrated every 12 hours Parenteral oxycodone preparations: OxyNorm injection Conversion ratios: Oral Morphine to Oral Oxycodone is approximately 2:1. If a patient is already on morphine then the total 24-hour morphine dose should be divided by two for the equivalent 24-hour Oxycodone dose e.g. 80mg morphine / 24 hours = 40 mg Oxycontin /24 hours Oral Oxycodone to SC Oxycodone Divide by 2 or 1.5 (See conversion chart page 12) 7
8 MANAGEMENT OF PAIN PATIENT UNABLE TO TAKE ORAL ANALGESIA NO PAIN AT PRESENT/PAIN CURRENTLY CONTROLLED NO ANALGESIA PRESCRIBED ALREADY ON REGULAR WEAK OPIOID CO-CODAMOL 30/500, DIHYDROCODEINE TRAMADOL ALREADY ON ORAL MORPHINE ALREADY ON A FENTANYL PATCH Prescribe for prn use MORPHINE 2.5-5mg s/c 2-4 hourly Review after 24 hours. If patient has required 2 or more doses consider prescribing this total Morphine dose as a 24 hour syringe driver Prescribe MORPHINE 15mg s/c via a syringe driver over 24 hours instead of current oral analgesia Prescribe MORPHINE 2.5mg s/c 4 hourly for breakthrough pain. Convert from total daily oral MORPHINE to s/c MORPHINE or other opioid. Prescribe via a syringe driver over 24 hours Prescribe breakthrough analgesia. i.e. Divide the total Morphine or other opioid dose by 6 and give 2-4 hourly prn Continue prescribing the patch Prescribe s/c MORPHINE for breakthrough pain and give 2-4 hrly prn (See conversion chart page 12) 8
9 MANAGEMENT OF PAIN PATIENT UNABLE TO TAKE ORAL ANALGESIA PATIENT CURRENTLY EXPERIENCING PAIN NO ANALGESIA PRESCRIBED ALREADY ON ORAL MORPHINE OR OTHER OPIOID ALREADY ON A FENTANYL PATCH Give 2.5-5mg MORPHINE s/c stat and prn 4-6 hourly Prescribe MORPHINE mg s/c via a syringe driver over 24 hours Prescribe 2.5-5mg MORPHINE s/c 2-4 hourly PRN for breakthrough pain Convert from total daily oral opioid dose to s/c MORPHINE. Give s/c via syringe driver over 24 hours. Prescribe for breakthrough pain. MORPHINE s/c 2-4 hourly prn i.e. divide new total total daily s/c MORPHINE dose by 6. Give a stat dose. Review after 24 hours If two or more prn doses give in 24 hours increase syringe driver by 30 % to control pain Give a stat prn dose of morphine Continue prescribing patch Add additional MORPHINE (or other opioid) for uncontrolled pain as a s/c infusion via a syringe driver (equivalent of 2 breakthrough doses of MORPHINE) Prescribe s/c MORPHINE for breakthrough pain and give 2-4 hrly prn (See conversion chart page 12) If problems persist, contact the palliative care team for advice. 9
10 TRANSDERMAL FENTANYL ANALGESIA eg Durogesic DTrans Best used for Stable Pain A steady state of a FENTANYL patch is only achieved after 15-18hrs (short acting opiates will be required until pain is controlled) After removing a patch, there is a delay of many hours before circulating levels of drug drop to sub-therapeutic level Each patch lasts 72 hours, and should be replaced after this time i.e. every 3 days. It is not possible to ensure the interchangeability of different makes of Fentanyl transdermal patches in individual patients. Prescribe by brand name to minimise the risk of medication error due to inadvertent switching. How to convert to Fentanyl Patch There is no direct conversion between Fentanyl dose and Morphine dose, therefore always consult tables (and use clinical judgement). (See conversion chart page 12) After application of patch, therapeutic levels are achieved slowly, breakthrough (prn) doses will be required during this time. Therapeutic levels are reached and continue between 24 and 72 hours. Therefore after application assess efficacy of patch after hours, if breakthrough doses are required regularly, it may be an indication to either increase the strength of the Fentanyl patch or convert to other opioid formulation. From short acting (4 hourly) oral Morphine: apply patch - monitor patient 4 hourly for analgesic requirement - expect to continue 4 hourly doses for first 12 to 16 hours. From 12 hourly oral Morphine: apply the first patch at the same time as taking the final 12 hourly tablet. From 24 hourly Morphine: apply the first patch 12 hours after taking the final tablet. Pain not controlled on a Fentanyl patch If patient has increasing pain or is moribund: Do not remove patch. Add additional opioid for uncontrolled pain as a subcutaneous infusion using syringe driver. Calculate the required dose based on equivalent breakthrough dose. If patient has increasing pain and pain is opioid sensitive use short acting opioid and then consider increasing the patch strength. Take extra care when removing patch and introducing alternative opioids e.g. consider using prn oral or subcutaneous dosing for the first hours and then retitrate as previously outlined. Caution:If converting from fentanyl patch to syringe driver or oral medication seek advice regarding breakthrough and maintenance doses if unsure regarding the conversion. If pain difficult to control or patient is vomiting, contact Specialist Palliative Care Team for advice. 10
11 24 hourly Oral Morphine Dose (mg) DUROGESIC DTRANS CONVERSION GUIDE Fentanyl Patch Strength (mcg/hr) 4 Hourly Oral Morphine (mg) (also breakthrough medication dose) <90 25 < From syringe driver: apply patch - monitor patient at least 4 hourly for signs of toxicity, then remove syringe driver once patch in place for 12 hours. ALWAYS prescribe breakthrough doses of either oral Morphine or subcutaneous Diamorphine for all patients on Fentanyl, to meet any change in analgesic requirement. Transtec Patch (Buprenorphine) Conversion Guide Buprenorphine Matrix Patch/Patches micrograms/hr 24 hr Oral Morphine Dose (mg) Transtec Patch is replaced twice weekly, every 3 or 4 days e.g. every Monday and Thursday. BuTrans Patch (Buprenorphine) Conversion Guide 5 micrograms/hr 10 micrograms/hr 20 micrograms/hr Oral Tramadol 50mg/day mg/day mg/day Oral Codeine ~30 60mg/day ~60-120mg/day ~ mg/day Oral Dihydrocodeine ~60mg/day ~60-120mg/day ~ mg/day Butrans Patch is replaced every 7 days 11
12 OPIOID DOSE CONVERSION GUIDE (APPROXIMATE EQUIVALENT DOSES) Oral Weak Opioid 24 hours Oral Morphine dose 24 hours Co-Codamol 30 / tabs qds = 240mg codeine 30mg Dihydrocodeine 30mg 2 tabs qds = 240mg codeine 30mg Co-Dydramol 10/500 2 tabs qds = 80mg codeine 10mg Tramadol 100mg 1 tab qds = 400mg tramadol 40 60mg Approximate Equivalent Opioid Doses oral SC SC oral SC 24 h total dose (mg) Morphine 4 h dose (mg) Morphine 24 h total dose (mg) Diamorphine 24 h total dose (mg) 4 h dose (mg) Oxycodone 24 h total dose (mg) 4 h dose (mg) Oxycodone 24 h total dose (mg) 4 h dose (mg) Conversion factors: Oral Codeine to Oral Morphine Divide by 10 Oral Morphine to SC Diamorphine Divide by 3 Oral Morphine to Oral Oxycodone Divide by 2 Oral Morphine to Oral Hydromorphone Divide by 7.5 Oral Morphine to SC Morphine Divide by 2 Oral Oxycodone to SC Oxycodone Divide by 2 DOH recommends SC Diamorphine: SC Oxycodone as 1:1 Oral Tramadol to oral Morphine Divide by 5 Oral Hydromorphone to SC Hydromorphone Divide by 2 SC Diamorphine to SC Oxycodone Treat as equivalent up to doses of 60mg/24hrs. Caution should be used when converting higher doses SC Diamorphine to SC Alfentanil Divide by 10 SC Diamorphine to SC Morphine Ratio is between 1:1.5 and 1:2, Multiply by 1.5 ALWAYS REVIEW PATIENT REGULARLY AFTER OPIOID SWITCH AS CONVERSION RATIOS ARE APPROXIMATE IF UNSURE OF THE CONVERSION ALWAYS SEEK SPECIALIST ADVICE 12
 Example 48mm = Set dial at 48 1 day (24hrs) The MS16a BLUE MS16A = is set in millimetres of length per hour mm Start Rate Indicator scale button setting lamp POINTS TO REMEMBER")
13 SYRINGE DRIVER GUIDELINES Actuator Securing strap NOTE - There are 2 different types of Graseby Syringe Driver commonly used in the community - The MS 26 GREEN MS26 = is set in millimetres of length per 24hrs (1 day) Example 48mm = Set dial at 48 1 day (24hrs) The MS16a BLUE MS16A = is set in millimetres of length per hour mm Start Rate Indicator scale button setting lamp POINTS TO REMEMBER Always use a Luer lock, 20 or 30 ml syringe Infusion sites Anterior aspect upper arm and thigh, anterior chest and abdominal wall, scapula region. Use water for injection to dilute drugs unless otherwise stated. Prime giving set, MEASURE the fluid length in the syringe barrel, SET the rate (some Trusts recommend SET, measure the fluid length, then prime check local guidelines). Subcutaneous Butterfly inserted with needle at 45. Soft-Set inserted at 90 and remove inner needle. Ensure syringe finger grip is correctly placed in groove seen on front side of driver. Indicator light flashes every 25 seconds. Boost/Start button only to be used when starting infusion NOT for extra pain relief. Common Drug Combinations Compatible Not compatible! Possibly incompatible Key 1. Cyclizine can crystallize at higher doses always use water for injection and maximum dilution. 2. Do not combine Metoclopramide (Prokinetic) with Cyclizine (Antimuscarinic) Example 48mm = Set dial at 02 24hrs Always use a Luer Lock, 20 or 30mls syringe DIAMORPHINE HALOPERIDOL(SERENACE)!!! HYOSCINE(SCOPOLAMINE)!! LEVOMEPRAZINE(NOZINAN)!!!!!! CYCLIZINE(VALOID)!!! METOCLOPRAMIDE(MAXOLON)!!!!! MIDAZOLAM(HYPNOVEL)!! DEXAMETHASONE(DECADRON)!!!!!! OXYNORM INJECTION! DIAMORPHINE HALOPERIDOL/SERENACE HYOSCINE/ SCOPOLAMINE LEVOMEPRAZINE/ NOZINAN CYCLIZINE/VALOID METOCLOPRAMIDE/ MAXOLON MIDAZOLAM/ HYPNOVEL DEXAMETHASONE NB Good practice suggests a maximum of 3 drug combinations. If 4 drugs are required seek further guidance. 13
14 Drugs for Subcutaneous Administration in Palliative Care setting Drug Indications for Use PRN/ 24 hour dose Side Effects Stat dose METOCLOPRAMIDE Prokinetic anti-emetic Nausea and vomiting due to delay in gastric emptying/irritation 10mg 30 90mg Abdominal cramping Diarrhoea Dystonia CYCLIZINE HALOPERIDOL Anti-emetic for: Motion sickness Bowel obstruction Raised intracranial pressure Anti-emetic Anti-psychotic 50mg mg Sedation Confusion Dry mouth 1.5mg 2.5mg 3.0mg mg Dystonia Sedation LEVOMEPRAZINE HYOSCINE BUTYLBROMIDE HYOSCINE HYDROBROMIDE MIDAZOLAM DEXAMETHASONE 2 nd line anti-emetic Anti-psychotic Terminal agitation Anti-spasmodic (GI) Anti-secretory (GI and 6.25mg 5mg mg mg Postural hypotension Sedation 20mg mg Dry mouth Upper resp. tract) Anti-secretory 400mcg mg ( mcg) Anxiolytic/Sedation Anti-convulsant Terminal agitation Intractable nausea and vomiting Raised intracranial pressure 2.5-5mg 10mg 2.5-5mg 5-10mg 20-60mg 10-80mg - 2-8mg Up to 16mgs DIAMORPHINE Dose of Diamorphine in syringe driver given subcutaneously over 24 hours equals the daily oral dose of Morphine divided by 3. eg If on MST 30mg BD, 24 hour dose of Morphine = 60mg. Therefore the 24 dose of Diamorphine = 60 divided by 3 = 20mg When switching opioids it must be emphasized dose ratios are a guide to the equivalent dose. Inter patient variability requires that each patient is carefully titrated to the appropriate dose. OXYNORM INJECTION 10mg in 1 ml Dose of parenteral Oxycodone in syringe driver given subcutaneously over 24 hours equals the daily oral dose of Oxycodone divided by 2 e.g. If on Oxycontin 30mgs BD, 24 hour dose of oral Oxycontin = 60mgs. Therefore the 24 hour dose of parenteral Oxycodone (Oxynorm parenteral) = 60 divided by 2 = 30mgs Opioid Switch: Oral Morphine to oral Oxycodone ratio is 2:1 e.g. MST 60mgs BD = Oxycontin 30mgs BD Dry mouth Agitation Sedation Drowsiness Insomnia Consider giving as a once daily subcutaneous bolus as it can precipitate with other drugs if not enough diluent is added. Constipation Nausea and vomiting Drowsiness Consider Morphine toxicity in a restless patient Constipation Nausea and vomiting Drowsiness, Opioid toxicity Remember to consider opiate toxicity in restless patient Signs of opiate toxicity: Myoclonic jerks, agitated delirium. Hallucinations; multifocal twitching and jerking of limbs, persistent drowsiness 14
15 NAUSEA AND VOMITING Where possible assess and identify underlying cause of nausea and vomiting. If a trial of oral medication is not appropriate or control of symptoms have been difficult to achieve consider using a syringe driver to administer parenteral anti-emetics until adequate symptom control has been achieved. PATIENT UNABLE TO TAKE ORAL ANTIEMETIC No N&V at present N&V Present ORAL ANTIEMETIC NOT CURRENTLY PRESCRIBED ALREADY ON REGULAR ORAL ANTIEMETICS (i.e. symptoms controlled by current prescription) Give a stat dose of suitable s/c antiemetic. PLUS start 24 hour s/c infusion via a syringe driver PLUS s/c antiemetic for breakthrough symptoms Prescribe cyclizine s/c PRN If nausea/vomiting persist use maximum dose of current antiemetic Stop oral antiemetics. Prescribe current anti-emetic via s/c syringe driver PLUS suitable s/c antiemetic for breakthrough symptoms If nausea/vomiting still persist, replace antiemetic drugs in syringe driver with Levomepromazine 6.25g-25mg PLUS Levomepromazine 6.25mg PRN s/c for breakthrough. Review every 24 hours If nausea and vomiting not controlled go Nausea and Vomiting Present column above IDENTIFIABLE CAUSES Cause Symptoms Recommendation Chemo/radiotherapy Determine from history Ondansetron or other 5-HT3 antagonist Intestinal Obstruction Constipation, abdominal distension, colicky abdominal Cyclizine if surgical intervention inappropriate pain Hypercalcaemia Agitation, confusion, dehydration, drowsiness Consider admission Haloperidol if active treatment of hypercalcaemia inappropriate Gastric Stasis Intermittent large volume vomits Metoclopramide - Exclude bowel obstruction Medication New drug, increased opioid dose, NSAID Consider stopping causative drug. Haloperidol or cyclizine Raised ICP Headache, lateralizing signs, h/o brain mets Cyclizine and commence or increase dexamethasone NO OBVIOUS UNDERLYING CAUSE - EMPIRICAL REGIME Drug Stat Dose Maintenance Indications 1 st Line Cyclizine 25-50mg mg Raised ICP, intestinal obstruction, movement related nausea 2 nd Line add Haloperidol 1.5mg 1.5-5mg Chemical related nausea. Eg:. Hypercalcaemia and renal failure. Higher doses may cause sedation and extra-pyramidal side-effects 3 rd Line switch to Levomepromazine mg mg Sedation and hypotension at higher doses. Note: Metoclopramide and Cyclizine should not be given together. 15
16 AGITATION AND RESTLESSNESS IN THE END STAGES OF LIFE NONE AT PRESENT PRESENT Prescribe MIDAZOLAM 2.5-5mg s/c 4 hourly prn If 2 or more doses required prn Prescribe stat MIDAZOLAM 2.5mg-5mg s/c and assess response after 30 minutes If effective Prescribe 10mg via a syringe driver over 24 hours And continue to give prn doses as required and Re-assess regularly. If symptoms persist, add total s/c prn dose over 24 hours to current syringe driver dose (increase breakthrough dose accordingly) If poor response to increasing dose of MIDAZOLAM - reassess cause of agitation - consider prescribing starting dose of LEVOMEPROMAZINE mg s/c Consider possible treatable causes: Assess response and if effective add LEVOMEPROMAZINE mg via syringe driver over 24 hours Opioid Toxicity Faecal impaction Fear Urinary infection Hypercalcaemia Infection Increased pain Uraemia Urinary retention OPIOID TOXICITY Presence of confusion, drowsiness, myoclonic jerks and often pin-point pupils. Can occur when dose has been markedly increased OR when renal failure ensues and active metabolites accumulate. RECOMMENDED MANAGEMENT: Decrease opioids dose by 30 50% Hydration Use midazolam if sedation required Use haloperidol for the treatment of visual hallucinations if present and troublesome MIDAZOLAM (for agitation) Stat dose = 2.5mg 5mg s/c Maintenance dose = 10mg-60mg per 24hrs via s/c infusion 16
17 MANAGEMENT OF NOISY SECRETIONS NONE AT PRESENT PRESENT Prescribe HYOSCINE HYDROBROMIDE 0.4mg s/c 4-6hourly prn. If two or more doses of prn HYOSCINE HYDROBROMIDE required in 24 hours Give stat doses HYOSCINE HYDROBROMIDE 0.4mg s/c and prescribe HYOSCINE HYDROBROMIDE 1.2mg s/c over 24 hours via syringe driver and prescribe 0.4mg HYOSCINE HYDROBROMIDE s/c 4-6 hourly prm for breakthrough symptoms -if symptoms persist, increase total 24 hour dose to 2.4mg -If 2.4mg in 24 hours not effective consider changing to GLYCOPRRONIUM 0.6mg- 1.2mg s/c over 24 hours via syringe driver. Note REPOSITIONING MAY HELP DISLODGE CHEST SECRETIONS Naloxone for reversal of opioid induced respiratory depression (based on the recommendations of the American Pain Society) If respiratory rate 8/min and the patient is easily rousable and not cyanosed, adopt a policy of wait and see ; consider reducing or omitting the next regular dose of Morphine and reassess pain. If respiratory rate <8/min, the patient is barely rousable/unconscious and/or cyanosed: Dilute a standard ampoule containing Naloxone 400ug to 10ml with saline for injection. Administer 0.5ml (20ug) IV every 2 min until the patient s respiratory status is satisfactory. Further boluses may be necessary because Naloxone is shorter-acting than Morphine (and other opioids). 17
18 PRESENTING PROBLEM SIGNS & SYMPTOMS REQUIRED ACTION Critically Ill Patients (Unresponsive/Hypotensive) Evidence of infection Pyrexia or hypothermia within 6 weeks post chemotherapy GUIDANCE FOR THE MANAGEMENT OF PATIENTS WHO BECOME ILL WITHIN 6 WEEKS OF CHEMOTHERAPY The patient has often been informed regarding necessary actions. Please ask if they have been given advice and act accordingly. Typhlitis a rare complication due to neutropenic caecitis/colitis Multi-organ failure. Acute bleeding (DIC) Potentially life threatening Neutropenic Sepsis Potentially life threatening. May mimic acute abdomen/appendicitis Admit to nearest A&E Contact treatment unit to arrange emergency admission via 999 ambulance Contact treating unit to discuss emergency admission via 999 ambulance Delayed emesis (Occurring 24 hours after chemotherapy) Up to 5 episodes of vomiting in 24 hours > 5 episodes of vomiting in 24 hrs and/or requires IV fluids Increase of 4-6 stools/day or nocturnal stools Increase of >7 stools/day or incontinence, or needs IV fluids First liquid stool Symptoms do not settle, dehydration or pyrexia occurs Painful erythema, oedema or ulcers but can swallow Painful erythema, oedema or ulcers. Unable to swallow. Requires IV fluids If this has occurred immediately on stopping 5HT3 antagonists, then these can be continued for a further 2-3 days If occurs later than this, give Metoclopramide 10mgs tds If further problems, discuss with treating unit Admit to treating unit Loperamide 4mgs initially, then 2mgs after each loose stool up to 5 days (max 16mgs daily) Admit to treating unit Loperamide 4mgs orally initially after first liquid stool then 2mgs every 2 hours thereafter up to 12 hours after last liquid stool for maximum of 48 hours. (Ignore usual max dose 16mgs daily) Admit to treating unit Oral care & pain relief Biotene MW 10mls qds +/- paracetamol Discomfort from ulcers Adcortyl in Orabase apply a thin layer 2-4 times daily Oral candidiasis Nystatin oral suspension, 1ml to be held in mouth for at least a minute before swallowing, qds after food Fluconazole 50mgs od for systemic treatment of oral candidiasis for 7 days Admit to treating unit Version 3: Endorsed by NICaN Board Date Released: May 2007; Review Date: May 2008 Page 1 of 2 18
19 Palmar Plantar syndrome Hypomagnesaemia Redness of palms of hands/soles of feet Skin breakdown/hacks Non-specific symptoms but can include muscle weakness, cramp, carpopedal spasm. Seizures and ECG changes in severe depletion. Use simple emollient Stop capecitabine tablets and seek advice from treating Oncologist If level is mmol/l: oral magnesium (12-15mmol in divided doses). Rx: Magnaspartate sachets 6.5g - 2 sachets bd. If magnesium< 0.55mmol/l discuss with treating unit re IV infusion Radiotherapy Related Problems PROBLEM SEVERITY ACTION Patient becomes ill during or after radiotherapy Symptoms will vary depending on site being treated 9-5pm Contact Treating Oncology Team for advice. If out of hours/weekend/bank Holiday and urgent contact Non-Cancer Related Acute Problems PROBLEM Oncology patient presents with potential medical cardiac or surgical problem ACTION Refer to nearest appropriate facility after seeking advice from treating oncologist Cancer Units and Centre Contact Numbers HOSPITAL WORKING HOURS (09:00 17:00, MON-FRI) OTHER TIMES ALTNAGELVIN (Sperrin Room) (Ward 10) ANTRIM or 40 (Laurel House) (Ward B1) CANCER CENTRE AT BCH CRAIGAVON (24 hr Oncology Helpline) (24hr Haematology Helpline) or 21 (Mandeville Unit) (Haematology Ward) ULSTER (MacDermott Unit) (Ward 4) FOR PATIENTS KNOWN TO THESE SERVICES NI HOSPICE 24Hrs Symptom Advisory Service MARIE CURIE HOSPICE FOYLE HOSPICE NEWRY HOSPICE If a patient is more than 6 weeks from their last chemotherapy or radiotherapy treatment, their condition may be discussed with their oncologist. If there is no indication for anti-cancer therapy, you may be advised to refer the patient to your local medical, surgical or palliative care services. 19 Version 3: Endorsed by NICaN Board Date Released: May 2007; Review Date: May 2008 Page 2 of 2
20 Useful Out of Hours Contacts for advice Telephone Northern Ireland Hospice Nurse Specialist Northern Ireland Hospice (24 hour) Marie Curie Hospice /2034 (24 hour) Oncology Helpline Bridgewater Suite Belfast City Hospital Northern Ireland Community Pharmacy Palliative Care Network (including oxygen) List available at OOH base REFERENCES UCHT/Clin.Guide (08) 2004 UCHT/Clin/Guide (08) 2006 BCH Nursing NIPME Opioid Equivalence, August 2006 Watson M, Lucas C, Hoy A, Palliative Care Guidance (2006) NI Control of Pain Guidelines DHSSPS 2003 Opioid equilavencies NIPMG 2008 Guidance for Chemotherapy Complications NICAN 2007 Liverpool Care Pathway Version 11 (2007) (Review date March 2009) 20
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
Anticipatory Medications for End of Life Patients. Doses must be proportional to the current analgesic medication YES NO YES NO
 Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
SYRINGE DRIVER MEDICATIONS
 SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
Clatterbridge Centre for Oncology
 Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
Clatterbridge Centre for Oncology CONTENTS 1. Why and when to use a syringe driver 2. Siting the syringe driver 3. Mixing and measuring 4. Setting up the syringe driver 5. Drug information 6. Common problems
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Syringe Drivers. Back to top
 Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]
![[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]](/thumbs/92/110296570.jpg "[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]") [Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
Conservative Management of Uraemia
 Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Conservative Management of Uraemia Information for Health Professionals Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact: The Renal Specialist
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Diamorphine 4 hour. alfentanil (500microgram/mL) Calculated by dividing 24 hour oral morphine dose by 30
 Calculated by dividing 24 hour oral morphine dose by 30") If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
General Palliative Care Guidelines for the Management of Pain at the End of Life in Adult Patients
 General Palliative Care Guidelines for the Management of Pain at the End of Life in Adult Patients February 2011 Contents Introduction 3 Understanding Pain 5 Principles of Pain Management 8 Assessment
General Palliative Care Guidelines for the Management of Pain at the End of Life in Adult Patients February 2011 Contents Introduction 3 Understanding Pain 5 Principles of Pain Management 8 Assessment
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
Berkshire West Area Prescribing Committee Guidance
 Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Opioid rotation or switching may be considered if a patient obtains pain relief with one opioid and is suffering severe adverse effects.
 Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
Palliative Care Out-of-hours. A resource pack for West Dorset. Contents:
 Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Symptom Control in the Community Setting. Dr Andrew Tysoe-Calnon
 Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
ALLERGIES/ SENSITIVITIES This section must be completed before prescribing/administering any drug
 COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
Care of dying adults in the last days of life. Improving care at the very end of life.
 Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Care of dying adults in the last days of life Improving care at the very end of life. Foreword We will all experience death, whether it is our own or that of a loved one. The bereaved person s perception
Guidelines for the Management of Chronic Non-Malignant Pain (CNMP) in Primary Care (not including neuropathic pain (NeP).
 in Primary Care (not including neuropathic pain (NeP).") Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Essential Syringe Driver Training for T 34. Elaine Bird St Luke s Hospice
 Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
Essential Syringe Driver Training for T 34 Elaine Bird St Luke s Hospice Aim For all practitioners to be accountable for their individual competence and capability when caring for a resident with a T34
Enhanced Community Palliative Support Services. Lynne Ghasemi St Luke s Hospice
 Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Adult Opioid Prescribing Guidelines for Acute or Persistent Pain
 Adult Opioid Prescribing Guidelines for Acute or Persistent Pain Author: Sponsor/Executive: Responsible committee: Consultation & Approval: (Committee/Groups which signed off the policy, including date)
Adult Opioid Prescribing Guidelines for Acute or Persistent Pain Author: Sponsor/Executive: Responsible committee: Consultation & Approval: (Committee/Groups which signed off the policy, including date)
Anticipatory prescribing and end of life considerations. Dr Stephanie Lippett
 Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
Anticipatory prescribing and end of life considerations Dr Stephanie Lippett contents Pain Restlessness/agitation Nausea/vomiting Secretions Syringe driver Anticipatory prescribing Important things to
SYMPTOM CONTROL IN THE LAST DAYS OF LIFE. Bradford, Airedale, Wharfedale & Craven
 Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Bradford, Airedale, Wharfedale & Craven Managed Clinical Network SYMPTOM CONTROL IN THE LAST DAYS OF LIFE Guidelines for Healthcare Professionals Bradford, Airedale, Wharfedale & Craven Signs and symptoms
Using syringe pumps in palliative care
 Using syringe pumps in palliative care Facilitator: Barbara Stone RN Ground rules Medication matching game Learning outcomes To identify the indications for using a syringe pump To discuss the general
Using syringe pumps in palliative care Facilitator: Barbara Stone RN Ground rules Medication matching game Learning outcomes To identify the indications for using a syringe pump To discuss the general
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
PALLIATIVE CARE PRESCRIBING
 PALLIATIVE CARE PRESCRIBING LANCASHIRE AND SOUTH CUMBRIA SPECIALIST PALLIATIVE CARE SERVICES 2010 Refer to electronic verson site for latest information. Review Date September 2011 NAVIGATIONAL INSTRUCTIONS
PALLIATIVE CARE PRESCRIBING LANCASHIRE AND SOUTH CUMBRIA SPECIALIST PALLIATIVE CARE SERVICES 2010 Refer to electronic verson site for latest information. Review Date September 2011 NAVIGATIONAL INSTRUCTIONS
PALLIATIVE CARE PRESCRIBING
 PALLIATIVE CARE PRESCRIBING LANCASHIRE AND SOUTH CUMBRIA SPECIALIST PALLIATIVE CARE SERVICES 2012 Refer to electronic verson at www.cancerlancashire.org.uk for latest information. Review Date January 2014
PALLIATIVE CARE PRESCRIBING LANCASHIRE AND SOUTH CUMBRIA SPECIALIST PALLIATIVE CARE SERVICES 2012 Refer to electronic verson at www.cancerlancashire.org.uk for latest information. Review Date January 2014
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Pain Management for Adult sickle cell disease patients: Information for patients, relatives and carers
 Pain Management for Adult sickle cell disease patients: Information for patients, relatives and carers Why you should read this leaflet This leaflet will give you the information necessary to manage your
Pain Management for Adult sickle cell disease patients: Information for patients, relatives and carers Why you should read this leaflet This leaflet will give you the information necessary to manage your
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04
 Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
MND Just in Case kit Information for GPs
 MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
MND Just in Case kit Information for GPs What is the MND Just in Case kit? 2 Motor neurone disease (MND) is a progressive and terminal disease that results in degeneration of the motor neurones in the
INTEGRATED CARE PATHWAY (ICP) FOR THE DYING ADULT
 FOR THE DYING ADULT") INTEGRATED CARE PATHWAY (ICP) FOR THE DYING ADULT PLEASE INFORM THE PALLIATIVE CARE TEAM ON COMMENCEMENT OF THIS ICP (EXT 8958) ICP Start Date Patient s Name. Ward. Consultant.. Named Specialist Nurse
INTEGRATED CARE PATHWAY (ICP) FOR THE DYING ADULT PLEASE INFORM THE PALLIATIVE CARE TEAM ON COMMENCEMENT OF THIS ICP (EXT 8958) ICP Start Date Patient s Name. Ward. Consultant.. Named Specialist Nurse
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Opioid Conversion Guidelines
 Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
NHS Grampian Protocol For The Prescribing And Administration Of Oral Opioids Following Trauma Or Surgery
 Acute Sector NHS Grampian Protocol For The Prescribing And Administration Of Oral Opioids Following Trauma Or Surgery Co-ordinators: Dr Karen Cranfield, Consultant Anaesthetist, Lead Acute Pain Sector
Acute Sector NHS Grampian Protocol For The Prescribing And Administration Of Oral Opioids Following Trauma Or Surgery Co-ordinators: Dr Karen Cranfield, Consultant Anaesthetist, Lead Acute Pain Sector
SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRESCRIPTION & ADMINISTRATION RECORD (SPAR) Name: Address: Postcode: Date of Birth: NHS Number:
 Name: Address: Postcode: Date of Birth: NHS Number:") FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
Understanding pain in 5 minutes
 Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Palliative Care Formulary
 Palliative Care Formulary 2016-2019 This formulary for pain and symptom management in adults is intended as a guide for prescribers in hospital and community. Special care should be taken when prescribing
Palliative Care Formulary 2016-2019 This formulary for pain and symptom management in adults is intended as a guide for prescribers in hospital and community. Special care should be taken when prescribing
Policy/Standard Operating Procedure/ Clinical Guideline. ELHT/CP22 Version 5.1. ELHT/CP22 Version 4.1
 TRUST WIDE/DIVISIONAL DOCUMENT Delete as appropriate Policy/Standard Operating Procedure/ Clinical Guideline DOCUMENT TITLE: Policy and Procedure for the T34 Ambulatory Syringe Pump in adults (Palliative
TRUST WIDE/DIVISIONAL DOCUMENT Delete as appropriate Policy/Standard Operating Procedure/ Clinical Guideline DOCUMENT TITLE: Policy and Procedure for the T34 Ambulatory Syringe Pump in adults (Palliative
Palliative Care. Pocketbook 4
 Nottinghamshire STP EOL Programme Board 2019 Review 2022 Palliative Care Pocketbook 4 Contents Pain Guidelines page 2 Nausea and Vomiting page 9 Inoperable Bowel Obstruction page 10 Constipation page 11
Nottinghamshire STP EOL Programme Board 2019 Review 2022 Palliative Care Pocketbook 4 Contents Pain Guidelines page 2 Nausea and Vomiting page 9 Inoperable Bowel Obstruction page 10 Constipation page 11
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients.
 We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
Q&A: Opioid Prescribing for Chronic Non-Malignant Pain
 NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
West Midlands Palliative Care Physicians. Palliative care. Guidelines for the use of drugs in symptom control
 West Midlands Palliative Care Physicians Palliative care Guidelines for the use of drugs in symptom control Revised Jan 2012 1 5th Edition, 2012 Guidelines for the use of drugs in symptom control These
West Midlands Palliative Care Physicians Palliative care Guidelines for the use of drugs in symptom control Revised Jan 2012 1 5th Edition, 2012 Guidelines for the use of drugs in symptom control These
Pain management in Paediatric Palliative Care. Dr Jane Nakawesi 14 th August 2017
 Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Controlled Document Number: Version Number: 1. Controlled Document Sponsor: Controlled Document Lead (Author): On: July Review Date: July 2020
: On: July Review Date: July 2020") Guidelines for the Use of Naloxone in Palliative Care in Adult Patients CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor: Controlled
Guidelines for the Use of Naloxone in Palliative Care in Adult Patients CONTROLLED DOCUMENT CATEGORY: CLASSIFICATION: Controlled Document Number: Version Number: 1 Controlled Document Sponsor: Controlled
ADULT (>16) ACUTE SICKLE PAIN GUIDELINE
 ACUTE SICKLE PAIN GUIDELINE") ADULT (>16) ACUTE SICKLE PAIN GUIDELINE ID 2013 065 Author s Name Dr Anna Wood Author s Job Title Consultant Haematologist Division Consultant Haematologist Department Haematology Version number 3 Ratifying
ADULT (>16) ACUTE SICKLE PAIN GUIDELINE ID 2013 065 Author s Name Dr Anna Wood Author s Job Title Consultant Haematologist Division Consultant Haematologist Department Haematology Version number 3 Ratifying
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
Understanding your take home medications from the surgical ward. Information for Patients
 Understanding your take home medications from the surgical ward Information for Patients i Information for Patients Please read this leaflet before taking the medications that have been prescribed for
Understanding your take home medications from the surgical ward Information for Patients i Information for Patients Please read this leaflet before taking the medications that have been prescribed for
End Stage Liver Disease Regional Audit Casenote Survey
 1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
1. This questionnaire is an audit of clinical documentation of patients who have died of end stage liver disease. If you have any questions about how this form should be completed please contact Dr Grace
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Treating the symptoms of kidney failure
 Treating the symptoms of kidney failure Information for patients, relatives and carers Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact:
Treating the symptoms of kidney failure Information for patients, relatives and carers Renal Department The York Hospital and Scarborough Hospital Tel: 01904 725370 For more information, please contact:
Acute painful crisis in patients with sickle cell disease: Clinical Guidelines (HN-506a)
") Acute painful crisis in patients with sickle cell disease: Clinical Guidelines (HN-506a) Introduction The majority of acute painful crises in patients with sickle cell disease will be managed independently
Acute painful crisis in patients with sickle cell disease: Clinical Guidelines (HN-506a) Introduction The majority of acute painful crises in patients with sickle cell disease will be managed independently
Best Practice Statement ~ November The management of pain in patients with cancer
 Best Practice Statement ~ November 2009 The management of pain in patients with cancer NHS Quality Improvement Scotland is committed to equality and diversity. We have assessed this Best Practice Statement
Best Practice Statement ~ November 2009 The management of pain in patients with cancer NHS Quality Improvement Scotland is committed to equality and diversity. We have assessed this Best Practice Statement
Your A-Z of Pain Relief A guide to pain relief medicines. We care, we discover, we teach
 Your A-Z of Pain Relief A guide to pain relief medicines We care, we discover, we teach Which pain medicines are you taking? Abstral (see Fentanyl Instant Tablets) Amitriptyline 5 Brufen (see Ibuprofen)
Your A-Z of Pain Relief A guide to pain relief medicines We care, we discover, we teach Which pain medicines are you taking? Abstral (see Fentanyl Instant Tablets) Amitriptyline 5 Brufen (see Ibuprofen)
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Control of Pain in Patients with Cancer
 for Control of Pain in Patients with Cancer National Council for Hospice and Specialist Palliative Care Services Northern Ireland Guideline Group Department of Health, Social Services & Public Safety An
for Control of Pain in Patients with Cancer National Council for Hospice and Specialist Palliative Care Services Northern Ireland Guideline Group Department of Health, Social Services & Public Safety An
Lothian Palliative Care Guidelines POCKET EDITION 2004
 Lothian Palliative Care Guidelines POCKET EDITION 2004 These guidelines have been developed by a multidisciplinary group of specialist and non-specialist health professionals from hospital, community and
Lothian Palliative Care Guidelines POCKET EDITION 2004 These guidelines have been developed by a multidisciplinary group of specialist and non-specialist health professionals from hospital, community and
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS
 PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
SPAGG. Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation
 SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
SPAGG Coversheet for Specialist Palliative Audit and Guideline Group Agreed Documentation This sheet is to accompany all documentation agreed by SPAGG. This will assist maintenance of the guidelines as
Palliative Patient in Emergency Department
 Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
patient group direction
 CYCLIZINE v01 1/7 CYCLIZINE PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner (Nurse)
CYCLIZINE v01 1/7 CYCLIZINE PGD Details Version 1.0 Legal category Staff grades Approved by POM Paramedic (Non-ECP) Nurse (Non-ECP) Emergency Care Practitioner (Paramedic) Emergency Care Practitioner (Nurse)
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
PRIMARY CARE PALLIATIVE CARE FORMULARY
 PRIMARY CARE PALLIATIVE CARE FORMULARY This formulary has been developed between West Essex CCG and the palliative care team at St Clare Hospice. The aim of the formulary is to ensure that medicines use
PRIMARY CARE PALLIATIVE CARE FORMULARY This formulary has been developed between West Essex CCG and the palliative care team at St Clare Hospice. The aim of the formulary is to ensure that medicines use