Analgesic Prescribing with Renal or Liver Impairment for Palliative Care Patients. Dr Thiru Thirukkumaran
|
|
|
- Neil Cook
- 5 years ago
- Views:
Transcription
 Palliative Care Services NW THO Parkside, Burnie Northwest")
1 Analgesic Prescribing with Renal or Liver Impairment for Palliative Care Patients Dr Thiru Thirukkumaran Senior Clinical Lecturer in Palliative Medicine Rural Clinical School Burnie University of Tasmania Palliative care Physician (CMO) Palliative Care Services NW THO Parkside, Burnie Northwest Tasmania
2 Learning Objectives Understand the impact of renal and liver impairment on analgesic prescribing in palliative care Learn about referral options for patients with renal and liver impairment on the NW Coast

3 Outline the Session What are the issues with Kidney / Liver Impairment and using Analgesics? Clinical Scenario with Renal Impairment Renal Impairment Available Analgesics in Renal impairment Clinical Scenario with Liver Impairment Liver Impairment Available Analgesics in Liver impairment Referral Options in NW Tasmania MCQ x 3
4 History: 57 years old Mr R with Metastatic Prostate Carcinoma with Bony metastasis. Had DXT; now on Hormone therapy. Stable disease (PSA = 23) 3/12 ago. He is admitted with 2/52 history of drowsiness, jerks & ache in back & legs. Unable to walk with movement related pain. Previously, he was reasonably active (AKPS = 90%) and admitted with poor functional-status (AKPS = 40%). Investigations: B/L Hydronephrosis; egfr = 25 & Cr = 234 & PSA = 210. Current Pain Medications: He is on MS Contin 60 mg BD + Endone (5mg x 2) prn + Panamax 2 tab tds What are the issues you find in this patient? What is your immediate management? What are the next step of management?


5 What are the issues you find in this patient? Prostate cancer disease progression leads to B/L Hydronephrosis. B/L Hydronephrosis renal impairment Accumulation of opioid metabolites His usual opioid dose become toxic Toxic Symptoms Increased pain despite of current medications

6 How do we manage Opioid Toxicity? Opioid Toxicity Toxic Symptoms & No Pain Toxic Symptoms & Increasing Pain Reduce the current Opioid by 30-50% Opioid Switch
7 What is the aim of immediate management in this patient? Pain Control Use renal friendly opioid and prevent further Renal damage It helps in Toxicity, Drowsiness & Improve AKPS How are you going to do? Opioid Switch
8 Opioid Switch Available renal friendly opioids for this patient s egfr (= 25) are: Hydromorphone - oral } Short acting drug - sub cut Inj } - Syringe Driver over 24 hours Fentanyl - Patch (long Acting) - Durogesic Patch - Lozenge (Short Acting) - Actiq Lozenge - Injection (short acting) Alfentanyl Injection (only form) - Syringe Driver for 24 hour - Sub cut Inj (short acting - prn) Weekly Norspan patch Max dose: 40mcg / hour; if more than 40mcg/hr required, we switch to fentanyl patch!
9 How to do the Calculation for this patient? The equivalent dose is MS Contin 60mg po BD = Total of 120mg Morphine (Oral) Hydromorphone [ 120mg / 6 ] = Total 20mg Hydromorphone (Oral) = Total of 7mg Hydromorphone in the Syringe Driver over 24 hours (3:1) Alfentanyl [ 120mg / 30] = Alfentanyl 4mg sc in syringe Driver Fentanyl [90mg Morphine = 25mcg/hr Fentanyl patch] = Fentanyl Patch approx. 33.3mcg /hr (Next available patch is mcg/hr) Why NOT Norspan Patch Here? The required Norspan patch exceed 40mcg/hr
10 How to Calculate the Patch dose.? Transdermal Fentanyl patch and oral Morphine Conversion Ratio: Transdermal Fentanyl patch : Oral Morphine = 1 : 150 (Ratio varies from 100 to 150 But taken as 150; Reference: APM; European Pal Care guidelines) E. g.: Patient is on 25 mcg/hr Fentanyl patch; What is the equivalent Morphine? = 25 [mcg / hour patch] x 24 [hours] x 150 [conversion ratio] = 90 mg Oral Morphine 1000 [to make milligrams] Transdermal Buprenorphine patch and oral Morphine Conversion Ratio: Transdermal Norspan patch : Oral Morphine = 1 : 60 (Ratio varies from 60 to 100 But taken as 60 ; Reference: APM; European Pal Care guidelines) E.g.: Patient is on 10 mcg/hr Norspan patch; What is the equivalent Morphine? = 10 [mcg / hour patch] x 24 [hours] x 60 [conversion ratio] = 14.4 mg Oral Morphine 1000 [to make milligrams]
11 Next step of management for this patient... Opioid Titration to achieve better pain control Using adjuvant medications according to opioid response Contact Oncology Team; inform the admission symptoms; Patient s functional status & his PSA level on this time! for further active treatment.?
12 Drug Metabolism Drug Metabolism The liver is the primary organ for clearance of most drugs. Non-polar, lipid-soluble drugs are converted to more polar and water-soluble compounds. Water soluble drugs are excreted unchanged in the kidneys by glomerular filtration and / or renal tubular secretion. Drug metabolism in Liver is classified in two phases: Phase I: reactions involve oxidative, reductive or hydrolytic reactions that are commonly catalysed by the mixed function oxidase system. The cytochrome P450 is the major enzyme system for oxidation of drugs. Phase II: reactions "conjugate" a water soluble entity, forming a more polar and water soluble metabolite that can be more easily excreted in the urine and/or bile.
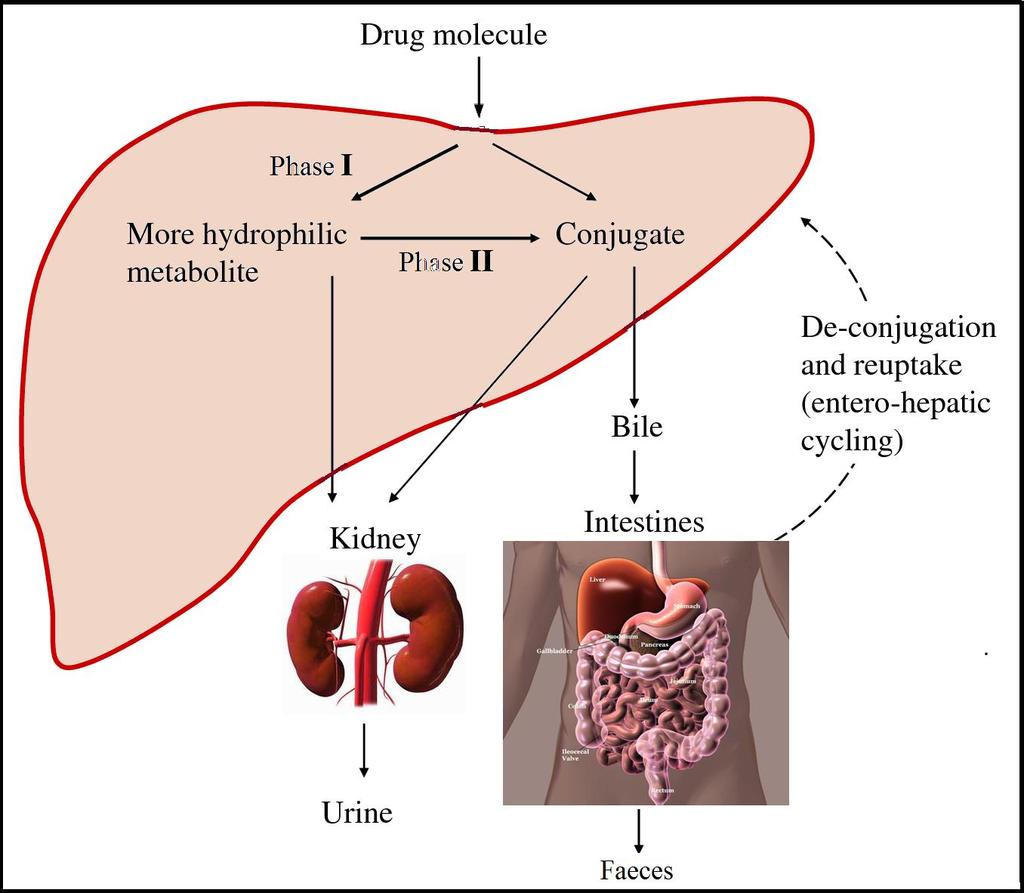
13 Drug Metabolism
14 Drug Metabolism in Renal/Liver impairment In patients with liver failure, reduced metabolism usually results in accumulation of the parent drug in the body with repeated administration. When patients with renal or hepatic dysfunction receive opioid analgesics, it is essential to understand and consider how opioid pharmacokinetics can be altered? This is necessary to ensure appropriate pain relief for the patient while limiting serious and potentially preventable adverse effects such as respiratory depression, hypotension, or CNS toxicity from either the parent drug or its metabolites.
15 Vicious Cycle of Opioid-Induced Neurotoxicity Opioid tolerance Mild myoclonus (e.g.: with sleeping) Severe myoclonus Seizures, Death Delirium Hyperalgesia Opioids Increased Misinterpreted as Pain Agitation Opioids Increased Misinterpreted as Disease-Related Pain


16 ANALGESIC USE IN RENAL IMPAIRMENT
17 How to measure Renal function? Traditionally serum Creatinine has been used as a measure of renal function. This is inaccurate as patients may have a clinically significant deterioration in renal function while still having a serum Creatinine within the normal reference range.(lamb et al) Glomerular filtration rate (GFR) is a preferable measure of renal function. There are two generally accepted methods of estimating GFR 1. Cockcroft + Gault equation 2. 4 variant modification of diet in renal disease equation (4vMDRD) Both methods are inaccurate at extremes of age and body weight. Estimated GFR (egfr) is now provided with biochemistry results and is based on the 4vMDRD calculation. (It will not have been adjusted for body total surface area).
18 egfr classification of Renal impairment Degree impairment Chronic Kidney Disease (CKD) stage egfr ml/min/1.73m 2 Creatinine Clearance ml/min Normal renal function 1 > Mildly reduced renal function in presence of renal disease. In absence of renal disease egfr > 60 is considered normal Moderately reduced renal function Severely reduced renal function <10 Very severe. Established (end-stage) renal failure 5 <15 <10

19 Renal failure can make patients more susceptible to adverse effects of drugs. In particular..., it causes: An increased bleeding tendency, therefore the risks of NSAIDs and anticoagulants are increased. Increased blood-brain barrier permeability, therefore increased sensitivity to CNS side effects of drugs e.g. sedation Renal failure can change analgesic pharmacokinetics in the following ways: Reduced excretion of drug or metabolites Altered drug distribution: especially if drug is plasma protein bound Reduced oral absorption: vomiting diarrhoea or mucosal oedema

20 Analgesics can still be prescribed according to the WHO analgesic ladder
 GFR <10 = Reduced dose ( 500mg-1g tds) NSAIDs: Should be avoided even in mild renal")
21 STEP 1 - ANALGESICS in Renal Impairment Paracetamol: GFR = no dose adjustment (1gram Qid) GFR = no dose adjustment (1gram Qid) GFR <10 = Reduced dose ( 500mg-1g tds) NSAIDs: Should be avoided even in mild renal impairment.
22 STEP 2 ANALGESICS in Renal Impairment Codeine / Panadeine / Panadeine forte (Half life significantly prolonged in chronic renal failure). Mild RF maintain normal dose Moderate RF 75% dose Severe RF 50% dose Tramadol: ( Usually, not recommended in Palliative care!) (Active metabolite excreted via kidney) Mild RF - normal dose mg Qid Moderate RF increase dosing interval mg bd Severe RF avoid Buprenorphine: Metabolised in the liver to inactive norbuprenorphine; Therefore, safe to use in patients with renal impairment. No dose adjustments in Transdermal preparations. (Reduce dose of SL buprenorphine by 25% in severe renal impairment).
23 STEP 3 ANALGESICS in Renal Impairment -1 Morphine: Morphine and its metabolites accumulate in renal failure and should therefore be avoided. (In my Practice, I monitor patient s renal impairment (up to egfr =40-50with morphine; If they are clinically deteriorated or showing toxic symptoms I switch the opioids. Another set of patients with mild renal impairment & on morphine are comfortable / pain-free & egfr is stable at the same level we continue the morphine but monitor them carefully with periodical check of egfr). Oxycodone: Half life shown to be mildly prolonged. Suggest use with great caution in severe renal failure GFR = no dose adjustment GFR = no dose adjustment but avoid MR- Release GFR < 10 = avoid
24 STEP 3 ANALGESICS in Renal Impairment -2 Fentanyl: Alfentanil: Metabolised to norfentanyl and inactive metabolites. Theoretical and clinically observed reduction in toxicity in renal failure. Although metabolites are inactive there is some concern that the parent drug may accumulate in moderate-severe renal impairment hence the recommendation to reduce dose: GFR = normal dose GFR = 75% dose GFR<10 = 50% dose Similar pharmacologically to fentanyl. Inactive metabolites. 30 times as potent as oral morphine. Can be administered via CSCI and is safe even in severe renal impairment. No dose adjustment is required. Methadone: Renal impairment does not affect methadone clearance. Can be used in severe renal failure but dose adjustment required. GFR = no dose adjustment GFR = no dose adjustment GFR <10 = 50% dose reduction

25 ADJUVANT ANALGESICS in Renal Impairment -1 Amitriptyline: Starting dose needs no adjustment but must be titrated carefully to avoid sedation / hypotension. Gabapentin: Requires significant dose reduction! GFR = 300mg bd maximum GFR10-20 = 300mg od maximum GFR<10 = 300mg alternate days maximum Pregabalin: Require significant dose reduction! GFR = starting dose 75mg od (Max 300mg/day in divided doses) GFR = starting dose 25-50mg od (Max 150mg/day in divided doses) GFR <10 = starting dose 25mg od (Max 75mg od)
26 ADJUVANT ANALGESICS in Renal Impairment -2 Sodium Valproate: Start with normal dose but titrate carefully. Beware increased sedation in renal failure. Dexamethasone: Does not require dose adjustment but may be complicated by fluid retention Clonazepam: No dose adjustment required but beware increased risk of sedation.
27 ADJUVANT ANALGESICS in Renal Impairment -3 Ketamine: Inactive metabolites. Safe in renal failure. No dose adjustments required

28 Clinical Scenario with Liver Impairment
29 55 years of Mrs W admitted with confusion / drowsiness, Constant RUQ pain and back pain for 3/52 duration. She is a known patient with carcinoma of the colon. The last staging scan (3 months ago) revealed liver & peritoneal metastasis. Examination: Palpable Tender Liver, Ascites, B/L leg Oedema noted. Investigations: Bilirubin = 39; ALT = 112; δ-gt = 583; Alkaline Phos = 291; Albumin = 20; egfr = 85; Cr = 109; K+ = 4.2 & Na+ = 143 Current Medications: Kapanol (Morphine SR) 40mg BD + Ordine Suspension 5mg prn + Paracetamol 1 gr Oid What are the issues you find in this patient? What is your immediate management? What are the next step of management?
30 What are the issues you find in this patient? Liver impairment with pain Tender Liver indicate Liver Capsular pain Opioid of choice cause more symptoms Wrong prn dose of Ordine Suspension
31 What is your immediate pain management? Either we can reduce the opioid dose or do a opioid switch; considering her drowsiness / confusion and still having pain, I will consider switching the opioid in this case. I will try Fentanyl patch What is the dose? & Why? What medication you consider as prn dose? Why? and What is the dose?
32 What are the next step of management? Confused liver impairment patients Management of encephalopathy is usually straightforward if you remember the checklist! Check for sepsis Lactulose Fluids Replace electrolytes Check drug chart Do not sedate them!! Contact the Gastro - team

33 ANALGESIC USE IN LIVER IMPAIRMENT
34 Opioid Use in Hepatic Dysfunction -1 The liver is the major site for transformation of opioids from parent compounds to active or inactive metabolites. In patients with liver failure, reduced metabolism usually results in accumulation of the parent drug in the body with repeated administration. In general, patients with severe liver disease should be prescribed lower doses of opioids, with extended dosing intervals when multiple daily doses of opioids are needed.
35 Opioid Use in Hepatic Dysfunction -2 Oxidation and other hepatocellular processes seem to be more affected by liver dysfunction than glucuronidation which does not require hepatocellular enzymes. However, morphine is primarily transformed via glucuronidation [Duramorph PI 1994], and its accumulation has been problematic in some patients with hepatic failure. Hydromorphone also may accumulate and should be used cautiously. Fentanyl appears to be more affected by reduced hepatic blood flow than by severe hepatic dysfunction [Duragesic PI 2003]. Codeine should be avoided since the liver is required for biotransformation of the drug into the active metabolite, morphine, so pain control could be compromised [Gasche et al. 2004]. Methadone is not advised in severe liver dysfunction [Dolophine PI 2006].
36 Recommended Use of Opioids in Hepatic Dysfunction Demerol PI 2002; Dolophine PI 2006; Guay et al.1988; Klein and Magida, 1971; Murphy 2005; Tegeder et al Opioid Recommended Usage Comment Dosing Recommendations* Morphine Use cautiously and monitor patient for sedation. In severe hepatic impairment, the parent drug may not be readily converted to metabolites. Increase the dosing interval by twice the usual time period. Hydromorphone Use cautiously and monitor patient carefully for symptoms of opioid overdose. In severe hepatic impairment, the parent drug may not be readily converted to inactive metabolites. Decrease initial dose by 50% of the usual amount. Oxycodone Use cautiously and monitor patient carefully for symptoms of opioid overdose. In severe hepatic impairment, the parent drug may not be readily converted to inactive metabolites. Decrease initial dose by 1/2 to 1/3 of the usual amount. Codeine Avoid use. In severe hepatic impairment, codeine may not be converted to the active metabolite, morphine. Methadone Not advised. Not advised in severe liver failure due to risk of methadone accumulation. Fentanyl Appears safe, generally no dose adjustment necessary. Decreased hepatic blood flow affects metabolism more than hepatic failure. Dosing adjustment usually not needed.
37 Referral System In the community (Home +N/homes), GPs are responsible for patients and in the hospitals, the relevant medical team. Examples: In the Hospital: If you find, poor renal functions and patient is on inappropriate opioids, you can raise the concerns, talking to the team, express your concerns Community: Quite Challenging! But still, if I were you, I will talk to the relevant GP & express my concerns!
38 MCQ x 3 1. Mr JB is on MS Contin 30mg po BD; Achieved Good pain control & no B/Ts needed. He renal functions rapidly declined with cancer progression with B/L Hydronephrosis (egfr = 25 now); What is the appropriate Hydromorphone dose / 24 hours (1) 40mg (2) 30mg (3) 20mg (4) 10mg 2. Mrs S is on Gabapentin 300mg po BD for her cancer related neuropathic pain. She developed renal impairment (egfr=30). What her current safe Gabapentin dose at present? (1) 300mg BD (2) 300mg OD (3) 100mg BD (4) 50mg BD 3. Mr B is on OxyContin 30mg BD for his cancer pain. His liver functions deteriorated with cancer spread to the liver (moderate to severe dysfunction) & he is getting more pain now. What is your choice of analgesics? (1) Convert to Methadone (2) Keep the same opioid drug/dose (3) Stop opioids & start a NSAID + Steroids (for liver capsular pain) (4) Reduce the 24 hr dose by half and consider steroid trial

39
:201-205 Davies G, Kingswood C, Street M. pharmacokinetics of opioids in renal dysfunction. Clinical Pharmacokinetics 1996; 31(6):410-422 Kaiko D, Benziger C, Cheng Y et al.")
40 References: Ashley C, Currie A The Renal Drug Handbook Second Edition. Oxford Radcliffe Medical Press Farrell A, Rich A. Analgesic use in patients with renal failure.eur J.Pall.Care 2000; 7(6): Davies G, Kingswood C, Street M. pharmacokinetics of opioids in renal dysfunction. Clinical Pharmacokinetics 1996; 31(6): Kaiko D, Benziger C, Cheng Y et al. Clinical pharmacokinetics of controlled release oxycodone in renal impairment. Clin Pharmacol Ther 1996; 59: Hunt R, Fazekas B, Thorne D et al. A comparison of subcutaneous morphine and fentanyl in hospice cancer patients. Journal Pain and Symptom Management. 1999; 18: Farrell A and Rich A. Analgesic use in patients with renal failure. European Journal of Palliative care. 2000; 7(6) Dean M. Opioids in renal failure. Journal of pain and symptom management. 2004; 28 (5) Davies G, Kingswood C and Street M. Pharmacokinetics of opioids in renal dysfunction. Clinical Pharmacokinetics. 1996; Dec 31(6) Lamb, Tomson, Roderick. Annals of clinical biochemistry (5): Devaney A, Ashley C, Tomson C. How the reclassification of kidney disease impacts on dosing adjustments. Pharmaceutical journal 2006; 277: Mueller, BA. Pain Treatment Topics Opioid Safety in Renal & Hepatic Dysfunction pain-topics.org/pdf/opioids-renal-hepatic-dysfunction.pdf 2007
41 Durnin C, Hind ID, Wickens MM, et al. Pharmacokinetics of oral immediate-releasehydromorphone (Dilaudid IR) in subjects with renal impairment. Proc West Pharmacol Soc. 2001;44: Fitzgerald J. Narcotic analgesics in renal failure. Connecticut Med. 1991;55: Foral PA, Ineck JR, Nystrom KK. Oxycodone accumulation in a hemodialysis patient. South Med J. 2007;100: Furlan V, Hafi A, Dessalles MC, et al. Methadone is poorly removed by haemodialysis. Nephrol Dial Transplant. 1999;14:254. Gasche Y, Daali Y, Fathi M, et al. Codeine intoxication associated with ultrapid CYP2D6 metabolism. N Engl J Med. 2004;351: Guay DRP, Awni WM, Findlay JWA, et al. Pharmacokinetics and pharmacodynamics of codeine in endstage renal disease. Clin Pharmacol Ther. 1988;43: Hassan H, Bastani B, Kurella M. Analgesia in patients with ESRD: A review of available evidence. Am J Kidney Dis. 2003;42: Lurcott G. The effects of the genetic absence and inhibition of CYP2D6 on the metabolism of codeine and its derivatives, hydrocodone and oxycodone. Anesth Prog. 1998;45: Matzke GR, Chan GL, Abraham PA. Codeine dosage in renal failure [letter]. Clinical Pharmacy. 1986;5: Murphy EJ. Acute pain management pharmacology for the patient with concurrent renal or hepatic disease. Anaesth Intensive Care. 2005;33: Talbott GA, Lunn AM, Levy FH, et al. Respiratory arrest precipitated by codeine in a child with chronic renal failure. Clin Pediatrics. 1997;36(3): Tegeder I, Lotsch J, Geisslinger G. Pharmacokinetics of opioids in liver disease. Clin Pharmacokinet. 1999;37:17-40.
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Pain Management Management in Hepatic Hepatic and and Renal Dysfunction
 Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Pain and Chronic Kidney Disease
 Pain and Chronic Kidney Disease Frank Brennan Palliative Care Physician Department of Nephrology, St George Hospital Renal Supportive Care Symposium St George Hospital August 21 2015 Epidemiology Effect
Pain and Chronic Kidney Disease Frank Brennan Palliative Care Physician Department of Nephrology, St George Hospital Renal Supportive Care Symposium St George Hospital August 21 2015 Epidemiology Effect
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
Analgesia in patients with impaired renal function Formulary Guidance
 Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Opioid Conversion Guidelines
 Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Non Malignant Pain: Symptom Management
 Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
Pharmacokinetics of strong opioids. Susan Addie Specialist palliative care pharmacist
 Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Palliative Patient in Emergency Department
 Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
Palliative Patient in Emergency Department Dr Thiru Thirukkumaran Palliative Care Services NW THO Northwest Regional Hospital, Burnie Northwest Tasmania Outline the Session Introduction What is palliative
Berkshire West Area Prescribing Committee Guidance
 Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Opioid Rotation. Dr Bruno Gagnon, M.D., M.Sc.
 Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC
 CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
CARE OF THE DYING PATIENT WITH ESKD ELIZABETH JOSLAND - RSC CNC OBJECTIVES UNDERSTANDING OF: POTENTIAL COMPLEXITIES OF ESKD PATIENTS IMPORTANCE OF COMMUNICATION CONSIDERATIONS AT END-OF-LIFE END-OF-LIFE
Opioid Use in Serious Illness
 Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Guidelines for the Management of Chronic Non-Malignant Pain (CNMP) in Primary Care (not including neuropathic pain (NeP).
 in Primary Care (not including neuropathic pain (NeP).") Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4
![OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4](/thumbs/90/104143670.jpg "OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4") Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Opioid Case Studies. Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN. September 29, MFMER slide-1
 Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
Enhanced Community Palliative Support Services. Lynne Ghasemi St Luke s Hospice
 Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
B. Long-acting/Extended-release Opioids
 4 Opioid tolerance is assumed in patients already taking fentanyl 25 mcg/hr OR daily doses of the following oral agents for 1 week: 60 mg oral morphine, 30 mg oxycodone, 8 mg hydromorphone, 25 mg of oxymorphone
4 Opioid tolerance is assumed in patients already taking fentanyl 25 mcg/hr OR daily doses of the following oral agents for 1 week: 60 mg oral morphine, 30 mg oxycodone, 8 mg hydromorphone, 25 mg of oxymorphone
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
Prescribing in Renal Failure: Re-audit
 Prescribing in Renal Failure: Re-audit Happy World Kidney Day! March 14 th 2013 2 Audit Group Dr Julie Raj Consultant, University Hospital Aintree Dr Clare Horlick- StR, University Hospital Aintree Helen
Prescribing in Renal Failure: Re-audit Happy World Kidney Day! March 14 th 2013 2 Audit Group Dr Julie Raj Consultant, University Hospital Aintree Dr Clare Horlick- StR, University Hospital Aintree Helen
21 st June BDS BASHD Therapeutics Pain and Analgesia. BASHD Therapeutics Analgesics and Pain Management. Links to other BASHD content
 Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Session II. Learning Objectives for Session II. Key Principles of Safe Prescribing. Benefits and Limitations of ER/LA Opioids
 Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
Pharmacogenetics of Codeine. Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA
 Pharmacogenetics of Codeine Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA 1 Codeine Overview Naturally occurring opium alkaloid Demethylated to morphine for analgesic effect
Pharmacogenetics of Codeine Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA 1 Codeine Overview Naturally occurring opium alkaloid Demethylated to morphine for analgesic effect
What s New 2003? What new treatments? What have you discontinued? More information please!
 What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
Clinical Guideline. Guidelines for the use of opioid analgesics in the management of acute pain in adults
 Clinical Guideline Guidelines for the use of opioid analgesics in the management of acute pain in adults Document detail Document location West Kent and MTW Formulary Version 1.0 Effective from July 2017
Clinical Guideline Guidelines for the use of opioid analgesics in the management of acute pain in adults Document detail Document location West Kent and MTW Formulary Version 1.0 Effective from July 2017
Peritoneal dosing recommendation gabapentin
 Peritoneal dosing recommendation gabapentin Search Latest news from AFSPA on Federal Employees Health. 8-4-2010 Information for Health Care Professionals : Cannabis (marihuana, marijuana) and the cannabinoids
Peritoneal dosing recommendation gabapentin Search Latest news from AFSPA on Federal Employees Health. 8-4-2010 Information for Health Care Professionals : Cannabis (marihuana, marijuana) and the cannabinoids
Opioid Conversions Mixture of Science and Art
 Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
CHAMP: Bedside Teaching TREATING PAIN. Stacie Levine MD. What is the approach to treating pain in the aging adult patient?
 CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Drug Dosing in Renal Insufficiency. Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila
 Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Pain. November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine
 Internal Medicine, Palliative Medicine") Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
PAIN MANAGEMENT PGY-1. Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC
 PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
Chapter-V Drug use in renal and hepatic disorders. BY Prof. C.Ramasamy, Head, Dept of Pharmacy Practice SRM College of Pharmacy, SRM University
 Chapter-V Drug use in renal and hepatic disorders. BY Prof. C.Ramasamy, Head, Dept of Pharmacy Practice SRM College of Pharmacy, SRM University Estimating renal function An accurate estimation of renal
Chapter-V Drug use in renal and hepatic disorders. BY Prof. C.Ramasamy, Head, Dept of Pharmacy Practice SRM College of Pharmacy, SRM University Estimating renal function An accurate estimation of renal
Geriatric Pharmacology. Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center
 Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Geriatric Pharmacology Kwi Bulow, M.D. Clinical Professor of Medicine Director, Academic Geriatric Resource Center Silver Tsunami 2010: 40 million (13%) 2030: 72 million (20%) Baby Boomers (1946-1964)
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio (740) ~
 ~") 2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
disease or in clients who consume alcohol on a regular basis. bilirubin
 NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
Opioid rotation or switching may be considered if a patient obtains pain relief with one opioid and is suffering severe adverse effects.
 Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
CHRONIC PAIN MANAGEMENT
 CHRONIC PAIN MANAGEMENT Betty J Harris, PharmD. 2014 Objectives Explain the consequences of untreated pain. Identify common causes of chronic non-malignant pain in adults. Identify steps to assessing pain,
CHRONIC PAIN MANAGEMENT Betty J Harris, PharmD. 2014 Objectives Explain the consequences of untreated pain. Identify common causes of chronic non-malignant pain in adults. Identify steps to assessing pain,
Approach to Acute Pain Management
 Approach to Acute Pain Management Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Approach to Acute Pain Management Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Duragesic patch. Duragesic patch (fentanyl patch) Description
 Description") 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.31 Subject: Duragesic patch Page: 1 of 6 Last Review Date: March 18, 2016 Duragesic patch Description Duragesic patch (fentanyl
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.31 Subject: Duragesic patch Page: 1 of 6 Last Review Date: March 18, 2016 Duragesic patch Description Duragesic patch (fentanyl
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Prior Authorization Guideline
 Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Pain and the MGH Promise
 Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
ESCALATING PATIENT & CARER NEEDS TOWARDS END OF LIFE; OVERVIEW OF END OF LIFE CARE IN THE COMMUNITY Renal Supportive Care Nursing Elizabeth Josland
 ESCALATING PATIENT & CARER NEEDS TOWARDS END OF LIFE; OVERVIEW OF END OF LIFE CARE IN THE COMMUNITY Renal Supportive Care Nursing Elizabeth Josland CNC Objectives Dialysis vs non-dialysis end of life picture
ESCALATING PATIENT & CARER NEEDS TOWARDS END OF LIFE; OVERVIEW OF END OF LIFE CARE IN THE COMMUNITY Renal Supportive Care Nursing Elizabeth Josland CNC Objectives Dialysis vs non-dialysis end of life picture
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Adult Opioid Prescribing Guidelines for Acute or Persistent Pain
 Adult Opioid Prescribing Guidelines for Acute or Persistent Pain Author: Sponsor/Executive: Responsible committee: Consultation & Approval: (Committee/Groups which signed off the policy, including date)
Adult Opioid Prescribing Guidelines for Acute or Persistent Pain Author: Sponsor/Executive: Responsible committee: Consultation & Approval: (Committee/Groups which signed off the policy, including date)
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Dose equivalent of fentanyl patch to oxycontin
 Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
PARACOD Tablets (Paracetamol + Codeine phosphate)
") Published on: 22 Sep 2014 PARACOD Tablets (Paracetamol + Codeine phosphate) Composition PARACOD Tablets Each effervescent tablet contains: Paracetamol IP...650 mg Codeine Phosphate IP... 30 mg Dosage Form/s
Published on: 22 Sep 2014 PARACOD Tablets (Paracetamol + Codeine phosphate) Composition PARACOD Tablets Each effervescent tablet contains: Paracetamol IP...650 mg Codeine Phosphate IP... 30 mg Dosage Form/s
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
SYRINGE DRIVER MEDICATIONS
 SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Drug Information Common to the Class of Extended-Release and Long-Acting Opioid Analgesics (ER/LA opioid analgesics) Avinza Butrans
 Avinza Butrans") FDA Blueprint for Prescriber Education for Extended-Release and Long-Acting Opioid Analgesics 7/9/2012 Drug Information Common to the Class of Extended-Release and Long-Acting Opioid Analgesics (ER/LA
FDA Blueprint for Prescriber Education for Extended-Release and Long-Acting Opioid Analgesics 7/9/2012 Drug Information Common to the Class of Extended-Release and Long-Acting Opioid Analgesics (ER/LA
Equianalgesic Dosing: Making Opioid Interchange Easier. Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine
 Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Objectives. Patient Controlled Analgesia (PCA) Management in the Seriously Ill. Discuss principles for opioid dosing and titration for acute pain
 Management in the Seriously Ill. Discuss principles for opioid dosing and titration for acute pain") Patient Controlled Analgesia (PCA) Management in the Seriously Ill Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Director, Colorado
Patient Controlled Analgesia (PCA) Management in the Seriously Ill Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Director, Colorado
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Review of Pain Management with Clinical and Regulatory Updates
 Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and
Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and
Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia.
 Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia. Created: Monday, March 12. Online calculator to convert equianalgesic
Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia. Created: Monday, March 12. Online calculator to convert equianalgesic
Long-Acting Opioid Analgesics
 Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Supportive and Palliative care for patients with Pancreatic Cancer. Dr Holly Taylor September 2018
 Supportive and Palliative care for patients with Pancreatic Cancer Dr Holly Taylor September 2018 Aims of this session To discuss the principles of supportive and palliative care Identification of patients
Supportive and Palliative care for patients with Pancreatic Cancer Dr Holly Taylor September 2018 Aims of this session To discuss the principles of supportive and palliative care Identification of patients
1/29/2013. Schedule II Controlled Substances: Basics and Beyond. Controlled Substances. Controlled Substances, Schedule I
 chedule II Controlled ubstances: Basics and Beyond James L. Besier, Ph.D., R.Ph., FAHP Adjunct Associate Professor College of Nursing Adjunct Assistant Professor James L. Winkle College of Pharmacy University
chedule II Controlled ubstances: Basics and Beyond James L. Besier, Ph.D., R.Ph., FAHP Adjunct Associate Professor College of Nursing Adjunct Assistant Professor James L. Winkle College of Pharmacy University
Long-Acting Opioid Analgesics
 Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required