Review of Pain Management with Clinical and Regulatory Updates
|
|
|
- Rebecca McLaughlin
- 5 years ago
- Views:
Transcription
1 Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and Palliative Care John D. Dingell Veterans Administration Hospital Detroit, Michigan
2 Disclosure Dr. Stellini has no financial or other conflicts of interest related to this presentation to report. Any mention of off-label use of drugs will be identified as such.
3 Objectives Attendees will know general techniques of pharmacological and non-pharmacological treatment of pain Attendees will be aware of recent changes in scheduling of opioids and their effect on access to medications for patients Attendees will know the rationale and impact of FDA initiatives to control diversion and harmful effects of opioids
4 PALLIATION The physician s duty is to cure when possible, relieve suffering often, comfort always.
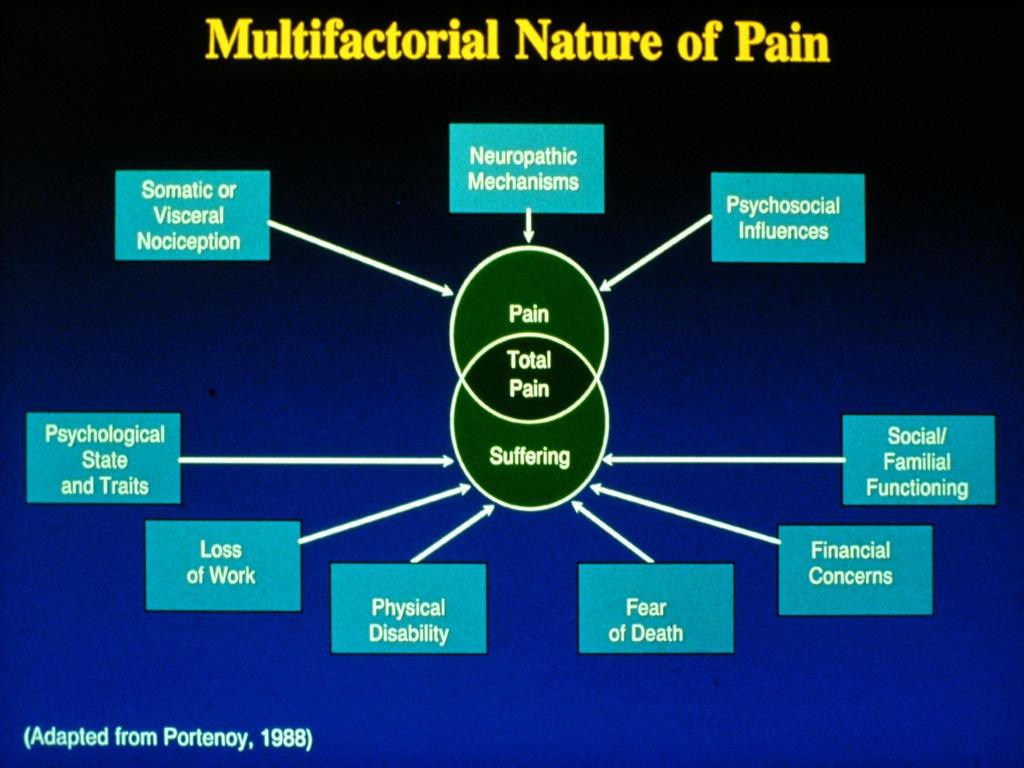
5 Pain is part of suffering Physical pain is part of total pain
6 How do we assess pain? Verbal report 0-10 scale Benefit changes over time (with or w/o tx) Limitations person specific, cognitive impairment, numbers challenged How are we doing with your pain control?
7 How do we assess pain? Observation e.g. Pain Assessment Behavior Scale Grimacing, Restlessness, Consolability,etc A lot of non-verbal patients are in pain Dementia, delirium, encephalopathy, intubated, children, etc.
8 What kind of pain is it? Acute pain injury, post-op Chronic malignant pain Non-malignant chronic pain
9 What kind of pain is it? Somatic Visceral Neuropathic Combined
10 Components of Pain Physical Psycological Spiritual
11 INTERVENTIONS FOR PAIN CONTROL
12 Non-Pharmacological Treatment Physical Therapy Heat Acupuncture Relaxation, Biofeedback, Imagery Counseling, Psychotherapy TENS Chiropractic Aromatherapy Healing Touch
13 Pharmacologic Interventions

14 Before we try assisted suicide, Mrs. Rose, let s give aspirin a chance.
15 Non-Opioid Analgesics Acetaminophen (analgesic, anti-pyretic, renal, liver toxicity) ASA (analgesic, anti-pyretic, anti-inflammatory, antiplatelet, Toxicities:GI, ulcer, bleeding,renal, Reyes) NSAIDS (see aspirin) 17 compounds in clinical use in U.S. Ketorolac (Toradol) COX-2 inhibitors (1 currently on market) analgesic, antipyretic, anti-inflammatory, little anti-platelet activity) Tramadol (Ultram ) (lowers seizure threshold, drug-drug interactions) Lidocaine Patch (Lidoderm) Capscacin Topical NSAIDS Cannabinoids? (Sativex)
16 Morphine Conjugated in liver. Morphine glucuronide is active. Excreted in urine. Decrease dose with renal impairment. May want to titrate dose down near end of life because of renal shut-down.
17 Hydromorphone More potent than morphine Oral or IV Safer in renal disease Mostly hepatic metabolism
18 Hydrocodone Only oral Always coupled with Acetaminophen or NSAID until now. About equipotent with morphine The most commonly prescribed opioid (Vicodin, Lortab, Norco, others)
19 Adjuvant Analgesics Anti-depressants - neuropathic Anti-convulsants - neuropathic Corticosteroids bone mets, large tumors, bowel obstruction Nerve blocks anesthetic lytic Epidural, intrathecal opiods local anesthetics Nerve stimulators
20 WHO Analgesic Ladder for Cancer Pain Management Pain - Non-opioid +/- adjuvant Pain persisting or increasing low-dose opioid +/-non-opioid +/-adjuvant Pain persisting or increasing increase dose of opioid +/- non-opioid.. Freedom from pain
21 Rational Use of Opioids
22
23 Among the remedies which it has pleased Almighty God to give to man to relieve his sufferings, none is so universal and so efficacious as opium. Thomas Sydenham (17 th century)
24 Among the remedies which it has pleased Almighty God to give to man to relieve his sufferings, none is so universal and so efficacious as opium. Amen Mike Stellini (2014) Thomas Sydenham (17 th century)
25 Opioids 1. Analgesia 2. Sedation 3. Respiratory Depression (RARE) (These effects occur in this order!)
26 Opioids Tolerance need higher dose of drug to get same previous effect. (In cancer patients, increased need often due to increased disease) A cancer patient on 300 mg/day morphine wide awake; me not likely. Physical Dependence defined by abstinence/withdrawal syndrome Psychological dependence = addiction
27 Opioids - Addiction Non-medicinal use Use despite negative physical, social, legal consequences Pre-occupation with obtaining the substance Not likely in cancer patients

28
29 Morphine Conjugated in liver. Morphine glucuronide is active. Excreted in urine. Decrease dose with renal impairment. May want to titrate dose down near end of life because of renal shut-down.
30 Hydromorphone More potent than morphine Oral or IV Safer in renal disease Mostly hepatic metabolism
31 Hydrocodone Only oral Coupled with Acetaminophen or NSAID About equipotent with morphine The most commonly prescribed opioid (Vicodin, Lortab, Norco, others)
32 Codeine Oral Coverts to morphine Effect ceiling (about 60 mg) Side effect ceiling higher than effect ceiling.
33 Fentanyl Much more potent than morphine/hydromorphone Oral (lollipop, orally dissolving tabs) IV - less hemodynamic effects than morphine Transdermal generally change every 72 hours; 80% of original dose remains in the used patch. Flush! (or sharps container)
34 Meperidine Limited use FORGET ABOUT IT! Toxic metabolite normeperidine seizures, hallucinations, bronchospasm, Death. Some hospitals have eliminated from formulary APS Guidelines procedure related pain; <48 hrs.; <600mg; not for chronic or prolonged post-op pain.
35 Methadone Unique opioid Intrinsically long half-life can be problematic Multiple pain receptor activity (mu, delta, NMDA, serotonin and norepi reuptake) Inexpensive Probably best opioid for neuropathic pain Conversion ratio varies inversely with higher morphine doses Hepatic metabolism
36 Conversion ratio of Morphine po to Methadone po Daily MS po dose (mg) < 100 mg mg mg mg mg > 1000 mg Conversion ratio 3:1 5:1 10:1 12:1 15:1 20:1
37 Methadone Cautions: Get supervised experience LONG half-life Only titrate every four days Very high doses Qt prolongation/torsades de pointes (observed but rare)

38 We can give you enough medicine to alleviate the pain, but not enough to make it fun.
39 Opioids Side Effects Constipation No tolerance Prophylax - Laxative (senna) and softener (docusate). Treatment Other stimulants (bicosadyl) Osmotics (lactulose, Miralax) Mg Citrate, Enemas Methylnaltrexone (new) sub-q injection, non-centrally acting mu receptor antagonist
40 Opioids - Side Effects Pruritis probably most common with morphine Not thought to be histamine mediated Treat with ondansetron or naltrexone or change drug.
41 Opioids - Side Effects Nausea Sedation (consider methylphenidate) Respiratory depression TOLERANCE DEVELOPS TO ALL
42 Opioids - Side Effects Neuro/neuro-excitatory effects sedation, confusion, delirium; High dose - myoclonus can develop and may be a dose limiting effect of morphine - May want to add benzodiazepine - Switch opioid. Methadone may be best alternative
43 Opioids - Side Effects Hyperalgesia Allodynia Painful sensation from normally non-painful stimulus Hyperesthesia dramatically increased sensitivity to painful stimulus?related to tolerance
44
45 Opioid Pharmacokinetics
46 Opioid Pharmacokinetics Oral Short acting - almost all opioids oral dose - peak 90 minutes duration 2-4 hours Methadone - intinsically long acting accumulates with repeat dosing Long acting preps - morphine, oxycodone fentanyl (patch)
47 Opioid Pharmacology Oral Dose escalation hours mild/mod pain - 25% - 50% severe pain 50% - 100% Maximum dose - none except meperidine (avoid), propoxyphene (now off the market), combo with APAP, NSAID
48 Opioid Pharmacokinetics Intravenous Push - Peaks in 6-10 min. IV; 30 min. subq/im Continuous - Give a loading bolus at the start and with each increase in basal rate Administer bolus slowly


49 Plasma Concentration IV SC / IM Cmax po / pr 0 Half-life (t 1/2 ) Time
50 Switching Opioids Use conversion table (see handout) Allow for incomplete cross-tolerance start with 50-75% of published dose ( safety factor ) Transdermal Fentanyl - Approx mg morphine/day -> 25 mcg/hr patch (Difficult to calculate in reverse)
51 Equi-analgesic Ratios Oral Parenteral Morphine 30mg 10mg Hydrocodone 30mg - Oxycodone 20mg - Hydromorphone
52 Opioids and Chronic Pain Getting started Start with short acting to determine need and tolerance Don t start an opioid naïve patient on long acting first! (How do you know where to start?) Mild/elderly w/moderate pain: 2-5 mg morphine every three hours PRN Moderate to severe pain: 5-10 mg morphine If pt has known pre-existing tolerance start higher
53 Opioids and Chronic Pain Escalate dose at appropriate interval until pain relief achieved For oral determine 24 hr need after hours. This determines long acting daily dose. For IV find effective bolus dose and start continuous at half of bolus. Monitor effect and side effects carefully
54 Opioids and Chronic Pain Long acting plus short acting for breakthrough q. 1-2 hrs. (10-20% of 24 hr. oral dose) Continuous IV breakthrough dose is usually about 50% of hourly rate q 10 minutes. Observe closely and adjust dose and frequency based on effect and side effects
55 Opioids and Chronic Pain If frequent breakthrough dosing needed, adjust daily long acting/continuous dose. Monitor and control side effects constipation - treat proactively nausea - short lived pruritis - ondansetron resp depression - RARE with proper titration
56 Opioids and Chronic Pain One long acting One short acting Opioid rotation may be needed if high doses are reached and pain not very well controlled NOTE: doses of morphine required for relief of dyspnea are usually smaller than those used for pain.
57 Opioids - Withdrawal Cruel to let patient withdrawal Dilated pupils, piloerection, nasal flaring ABDOMINAL PAIN Avoid naloxone if at all possible. If used dilute, administer slowly Naloxone has short half-life. If used for a patient overdosed on long acting opioid, overdose side-effects will recur when naloxone wears off.
58 Opioid rotation Improved pain control Incomplete cross tolerance Conversion charts Decrease dose
59 Bone Pain NSAIDS Corticosteroids Plus opioids Bisphosphenates
60 Recent Regulatory Activity Based on: Increasing deaths due to hydrocodone, methadone overdoses, common/inappropriate prescribing primarily hydrocodone, misuse of sustained/extended release preparations Heroin overdoses also increased
61 Recent Regulatory Activity REMS Hydrocodone re-scheduled to Schedule 2 No refills, no phone-ins Acetaminophen content of hydrocodone/apap limited to 325 mg per dose Extra-strength Tylenol rec only 3 gm/day max. New drug hydrocodone extended release Zohydro Tramadol rescheduled to Schedule 4 Tamper-proof ER preparations NOT Zohydro!
62
63
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
CHAMP: Bedside Teaching TREATING PAIN. Stacie Levine MD. What is the approach to treating pain in the aging adult patient?
 CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
Equianalgesic Dosing: Making Opioid Interchange Easier. Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine
 Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio (740) ~
 ~") 2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14. Cynthia Kim and Stephen Wilson
 UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
PAIN MANAGEMENT PGY-1. Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC
 PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
OPIOID- INDUCED NEUROTOXICITY*
 OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Pain Management in Hospice and Palliative Care
 Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Pain Management Management in Hepatic Hepatic and and Renal Dysfunction
 Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Managing Care at End of Life:
 Managing Care at End of Life: Physical Suffering Pain & Dyspnea Verna Sellers, MD, MPH, AGSF Medical Director Centra PACE Lynchburg, Virginia 1 Speaker Disclosures: Dr. Sellers has disclosed that she has
Managing Care at End of Life: Physical Suffering Pain & Dyspnea Verna Sellers, MD, MPH, AGSF Medical Director Centra PACE Lynchburg, Virginia 1 Speaker Disclosures: Dr. Sellers has disclosed that she has
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
disease or in clients who consume alcohol on a regular basis. bilirubin
 NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
Opioid Use in Serious Illness
 Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Objectives. What is pain? 9/27/2017. Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP
 Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP Photo credit: http://multiple-sclerosis-research.blogspot.com/2013/10/pain-and-unemployment.html Objectives Consider personal goal of pain management
Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP Photo credit: http://multiple-sclerosis-research.blogspot.com/2013/10/pain-and-unemployment.html Objectives Consider personal goal of pain management
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Cancer Pain. Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center
 Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
10 mg hydrocodone equals how much oxycodone
 Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008
 Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
B. Long-acting/Extended-release Opioids
 4 Opioid tolerance is assumed in patients already taking fentanyl 25 mcg/hr OR daily doses of the following oral agents for 1 week: 60 mg oral morphine, 30 mg oxycodone, 8 mg hydromorphone, 25 mg of oxymorphone
4 Opioid tolerance is assumed in patients already taking fentanyl 25 mcg/hr OR daily doses of the following oral agents for 1 week: 60 mg oral morphine, 30 mg oxycodone, 8 mg hydromorphone, 25 mg of oxymorphone
Appendix D: Drug Tables
 Appendix D: Drug Tables A. Short-acting, Orally Administered Opioids Table D-1: Use of Short-acting, Orally Administered Opioids in Adults [198] Additional Maximum APAP dose: 4000 mg/d (2000 mg/d in chronic
Appendix D: Drug Tables A. Short-acting, Orally Administered Opioids Table D-1: Use of Short-acting, Orally Administered Opioids in Adults [198] Additional Maximum APAP dose: 4000 mg/d (2000 mg/d in chronic
Objectives: What is your Definition of Pain? 8/16/2017
 Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
PAIN MANAGEMENT COMPETENCY
 PAIN MANAGEMENT COMPETENCY What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective.
PAIN MANAGEMENT COMPETENCY What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective.
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Opioid Case Studies. Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN. September 29, MFMER slide-1
 Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Interprofessional Webinar Series
 Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in the Hospital
 E P E C O Pain Management in the Hospital Denise Waugh, MD FACEP FAAHPM Medical Director of Palliative Care Services Scott and White Healthcare 724-6859 Pain is a more terrible lord of mankind than even
E P E C O Pain Management in the Hospital Denise Waugh, MD FACEP FAAHPM Medical Director of Palliative Care Services Scott and White Healthcare 724-6859 Pain is a more terrible lord of mankind than even
Opioids: Use, Abuse and Cause of Death. Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory
 Opioids: Use, Abuse and Cause of Death Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory jharmon@occl.ocgov.com Opioid: Any psychoactive chemical that resembles morphine
Opioids: Use, Abuse and Cause of Death Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory jharmon@occl.ocgov.com Opioid: Any psychoactive chemical that resembles morphine
Methadone: Essential Hospice Analgesic or Too Risky for Prime Time?
 Methadone Background Methadone: Essential Hospice Analgesic or Too Risky for Prime Time? Developed originally as an antispasmodic and later used as an analgesic, starting in late 1940 s Used extensively
Methadone Background Methadone: Essential Hospice Analgesic or Too Risky for Prime Time? Developed originally as an antispasmodic and later used as an analgesic, starting in late 1940 s Used extensively
Objectives. Controversy. Pain. Risk Stratification 1/7/2012
 Objectives Strategies in Pain Management: Scheduled, Breakthrough, and Dose Adjustments Tamara M. Green, Pharm.D PGY-1 Resident Florida A & M University Classify and distinguish between different types
Objectives Strategies in Pain Management: Scheduled, Breakthrough, and Dose Adjustments Tamara M. Green, Pharm.D PGY-1 Resident Florida A & M University Classify and distinguish between different types
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management
 Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Clinical Guideline. Guidelines for the use of opioid analgesics in the management of acute pain in adults
 Clinical Guideline Guidelines for the use of opioid analgesics in the management of acute pain in adults Document detail Document location West Kent and MTW Formulary Version 1.0 Effective from July 2017
Clinical Guideline Guidelines for the use of opioid analgesics in the management of acute pain in adults Document detail Document location West Kent and MTW Formulary Version 1.0 Effective from July 2017
FDA hormone replacement therapy Web site 6
 TABLE OF CONTENTS Caring for pain at UIMCC 1-5 FDA hormone replacement therapy Web site 6 P&T Committee Formulary Action - September 2003 6 Caring for pain at UIMCC The International Association for the
TABLE OF CONTENTS Caring for pain at UIMCC 1-5 FDA hormone replacement therapy Web site 6 P&T Committee Formulary Action - September 2003 6 Caring for pain at UIMCC The International Association for the
RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
OST. Pharmacology & Therapeutics. Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO
 OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
Advanced Pain Management LYRA SIHRA MD
 Advanced Pain Management LYRA SIHRA MD Objectives Describe the importance of pain management Define the types of pain Discuss opioid pharmacology Identify barriers to pain management Discuss ethical responsibilities
Advanced Pain Management LYRA SIHRA MD Objectives Describe the importance of pain management Define the types of pain Discuss opioid pharmacology Identify barriers to pain management Discuss ethical responsibilities
Analgesia for Patients with Substance Abuse Disorders. Lisa Jennings CN November 2015
 Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults
 SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
Using Evidence Based Medicine to Ethically Provide End of Life Symptom Control
 Using Evidence Based Medicine to Ethically Provide End of Life Symptom Control Erin Zimny, MD Emergency Medicine Hospice and Palliative Medicine Henry Ford Hospital Disclosures I do NOT have any financial
Using Evidence Based Medicine to Ethically Provide End of Life Symptom Control Erin Zimny, MD Emergency Medicine Hospice and Palliative Medicine Henry Ford Hospital Disclosures I do NOT have any financial
Multi Modal Analgesia
 Analgesic Drugs and Pharmacology Richard Craig R.N. B.N. M. Sci. Med (Pain Mgmt) Nurse Consultant Acute Pain Management Service Christchurch Hospital Multi Modal Analgesia Patients benefit from multi modal
Analgesic Drugs and Pharmacology Richard Craig R.N. B.N. M. Sci. Med (Pain Mgmt) Nurse Consultant Acute Pain Management Service Christchurch Hospital Multi Modal Analgesia Patients benefit from multi modal
What to do when you are called to see a patient with... PAIN. Susan Merel, MD Division of General Internal Medicine July 2018
 What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
What s New 2003? What new treatments? What have you discontinued? More information please!
 What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
PAIN MANAGEMENT IN PATIENTS WITH CANCER, PART II
 Learning Objectives PAIN MANAGEMENT IN PATIENTS WITH CANCER, PART II MINA LEE UNIVERSITY OF WASHINGTON MEDICAL CENTER/ SEATTLE CANCER CARE ALLIANCE CLINICAL PHARMACIST, GENERAL ONCOLOGY Understand the
Learning Objectives PAIN MANAGEMENT IN PATIENTS WITH CANCER, PART II MINA LEE UNIVERSITY OF WASHINGTON MEDICAL CENTER/ SEATTLE CANCER CARE ALLIANCE CLINICAL PHARMACIST, GENERAL ONCOLOGY Understand the
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Module 2 Pain Management. Handouts. Pain Is... Please click the links button under the video. You can print and/or save the handouts.
 E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
Pain Management: Overview of A Practical Approach
 Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
Prescription Pain Management. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D
 Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Drugs Used In Management Of Pain. Dr. Aliah Alshanwani
 Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4
![OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4](/thumbs/90/104143670.jpg "OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4") Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Sharon A Stephen, PhD, ARNP, ACHPN. September 23, 2014
 Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
PAIN & ANALGESIA. often accompanied by clinical depression. fibromyalgia, chronic fatigue, etc. COX 1, COX 2, and COX 3 (a variant of COX 1)
") Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain and Chemical Dependency Fathy Nasr
 Pain and Chemical Dependency Fathy Nasr Email: fathynasr@lycos.com WEB SITE: profathynasr.com Opioid Receptors Adenosine Guanosine Inositol PHAMACOTHERAPY, Step ladder Analgesic pyramids WHO Nociceptive
Pain and Chemical Dependency Fathy Nasr Email: fathynasr@lycos.com WEB SITE: profathynasr.com Opioid Receptors Adenosine Guanosine Inositol PHAMACOTHERAPY, Step ladder Analgesic pyramids WHO Nociceptive
Understanding pain in 5 minutes
 Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Pain and the MGH Promise
 Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
A PATIENT GUIDE FOR MANAGING PAIN
 A PATIENT GUIDE FOR MANAGING PAIN PAIN MANAGEMENT Knowing the Facts Pain can be controlled. Pain is common after surgery and with many types of illnesses. Most patients with acute and chronic pain can
A PATIENT GUIDE FOR MANAGING PAIN PAIN MANAGEMENT Knowing the Facts Pain can be controlled. Pain is common after surgery and with many types of illnesses. Most patients with acute and chronic pain can
! Somatic! Visceral! Neuropathic! Psychogenic. ! Analgesic! Relief without sedation! Works on peripheral pain receptors
 PAIN, PAIN, GO AWAY. TYPES OF PAIN! Somatic! Visceral! Neuropathic! Psychogenic Jill Autry, OD, RPh Eye Center of Texas, Houston drjillautry@tropicalce.com ANALGESIA! Mild! Aspirin! Paracetamol! Moderate!
PAIN, PAIN, GO AWAY. TYPES OF PAIN! Somatic! Visceral! Neuropathic! Psychogenic Jill Autry, OD, RPh Eye Center of Texas, Houston drjillautry@tropicalce.com ANALGESIA! Mild! Aspirin! Paracetamol! Moderate!
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly
 Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Clinical pharmacological aspects of heroin and fentanyl overdoses
 Clinical pharmacological aspects of heroin and fentanyl overdoses Ola Dale Professor Norwegian University of Technology of Science St. Olav s University Hospital, Trondheim, Norway 1 Opioids Sydenham 1680:
Clinical pharmacological aspects of heroin and fentanyl overdoses Ola Dale Professor Norwegian University of Technology of Science St. Olav s University Hospital, Trondheim, Norway 1 Opioids Sydenham 1680:
Opioid Rotation. Dr Bruno Gagnon, M.D., M.Sc.
 Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Introduction To Pain Management In Palliative Care
 Introduction To Pain Management In Palliative Care May 9, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Professor, University of Manitoba
Introduction To Pain Management In Palliative Care May 9, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Professor, University of Manitoba
Postoperative Pain Management. Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
") Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Charles P. O Brien, MD, PhD University of Pennsylvania No financial conflicts, patents, speakers bureaus
 Pain & Opioid Epidemic 2018 Charles P. O Brien, MD, PhD University of Pennsylvania No financial conflicts, patents, speakers bureaus Opioids 3400 BC Mesopotamia, Joy plant 1843 morphine by syringe 1874
Pain & Opioid Epidemic 2018 Charles P. O Brien, MD, PhD University of Pennsylvania No financial conflicts, patents, speakers bureaus Opioids 3400 BC Mesopotamia, Joy plant 1843 morphine by syringe 1874
No Pain, No Gain Pharmacy Patient Pain Counseling Competition
 No Pain, No Gain Pharmacy Patient Pain Counseling Competition Offered by the Maine Pharmacy Association as part of the 2010 MPA Fall Conference Sponsored by an educational grant by NASPA and Purdue Pharma,
No Pain, No Gain Pharmacy Patient Pain Counseling Competition Offered by the Maine Pharmacy Association as part of the 2010 MPA Fall Conference Sponsored by an educational grant by NASPA and Purdue Pharma,
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014
 Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
Berkshire West Area Prescribing Committee Guidance
 Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Pain Management in the
 Pain Management in the Elderly Meri Hix, PharmD, CGP, BCPS Associate Professor of Pharmacy Practice Midwestern University Chicago College of Pharmacy No conflicts of interest to declare Objectives Discuss
Pain Management in the Elderly Meri Hix, PharmD, CGP, BCPS Associate Professor of Pharmacy Practice Midwestern University Chicago College of Pharmacy No conflicts of interest to declare Objectives Discuss
Analgesia is a labeled indication for all of the approved drugs I will be discussing.
 Comparative Opioid Pharmacology Disclosure Analgesia is a labeled indication for all of the approved drugs I will be discussing. I ve consulted with Glaxo (remifentanil), Abbott (remifentanil), Janssen
Comparative Opioid Pharmacology Disclosure Analgesia is a labeled indication for all of the approved drugs I will be discussing. I ve consulted with Glaxo (remifentanil), Abbott (remifentanil), Janssen
Management of Post Operative Pain. Presented by Laura Marks PharmD, RP, CPHIMS 2016
 Management of Post Operative Pain Presented by Laura Marks PharmD, RP, CPHIMS 2016 Pain Defined Pain is whatever the experiencing person says it is, existing whenever they say it does. McCaffrey 1968 An
Management of Post Operative Pain Presented by Laura Marks PharmD, RP, CPHIMS 2016 Pain Defined Pain is whatever the experiencing person says it is, existing whenever they say it does. McCaffrey 1968 An
PAIN PODCAST SHOW NOTES:
 PAIN PODCAST SHOW NOTES: Dallas Holladay, DO Ultrasound Fellow Cook County Hospital Rush University Medical Center Jonathan D. Alterie, DO PGY-2, Emergency Medicine Midwestern University An overview of
PAIN PODCAST SHOW NOTES: Dallas Holladay, DO Ultrasound Fellow Cook County Hospital Rush University Medical Center Jonathan D. Alterie, DO PGY-2, Emergency Medicine Midwestern University An overview of