Complex Decision Making in Pediatric Dysphagia
|
|
|
- Sharon Clark
- 5 years ago
- Views:
Transcription

1 Complex Decision Making in Pediatric Dysphagia Alana Lowry, MS, CCC-SLP Fletcher Allen Health Care Kara Fletcher Larson, MS, CCC-SLP Jennifer Miller, MS, CCC-SLP Children s s Hospital Boston ASHA November 17, 2006 Miami, Florida
2 Contact Information: Kara Fletcher Larson, MS, CCC-SLP Alana Lowry, MS, CCC-SLP Jennifer Miller, MS, CCC-SLP
3 Incidence of Pediatric Dysphagia 25% in all children 80% in children with developmental disabilities 3-10% of children exhibit severe feeding problems Occur with greater prevalence in children with physical disabilities, medical illness and prematurity (Manikam & Perman 2000) Summarized in Oct Brackett, Arvedson & Manno in SID #13 newsletter
4 How did we get here? Major pediatric medical center Children s s Hospital Boston, MA 2005 performed 864 pediatric videofluoroscopic swallow studies Range in ages from 38 weeks PMA- young adults with developmental disabilities (early 20 s)
5 Patient Demographics 50% of our patients fall in the age range of 6 months- 3 years of age 6 % of patients referred from Level 3 NICU 4 % of patients referred by partnership with Dana Farber Cancer Institute/ Pediatric Oncology Division 13 % of patients referred by the Otolaryngology Division
6 Trends in Referral Concerns Given high volume of VFSS performed we began to observe trends in subset of patient populations Pediatric Oncology Increased incidence in identification and diagnosis of the Type 1 laryngeal cleft
7 Complex Decision Making Low incidence problems in pediatric dysphagia High stakes for safe and effective management of oropharyngeal dysphagia Medical, surgical, ethical and clinical questions we face when treating these children Highlight the role of the SLP as the preferred provider of dysphagia services.
8 Pediatric Oncology Patients referred for VFSS with chief complaint of coughing and choking with thin liquids All patients referred were undergoing chemotherapy consisting of the drug Vincristine (enrolled in specific treatment protocol for type of cancer) Onset of symptoms occurred days during the treatment of a 6 week cycle
9 Chemotherapy Agent: Vincristine Chemotherapy treats the type of cancer with medication that is toxic to tumor cells or kills them through interaction with receptors that indicate programmed cell death or prevent cell division. Typically given in cycles Cycle typically lasts weeks Period drug administration- resting period
10 Side Effects of Vincristine: Neurotoxicity Involves peripheral, autonomic, and central neuropathy Primary and dose limiting toxicity of Vincristine Most side effects are dose related and reversible Neurotoxicity can persist for months after discontinuation of therapy Rare cases can be permanently disabling
11 Results of VFSS in Children Receiving Vincristine All patients referred were full oral feeders at the time of referral All patients undergoing intravenous administration of Vincristine Parents report onset (often sudden) of sputtering, coughing and choking mainly with liquids Attending oncologist referred patient for VFSS
12 Results of VFSS in Children Receiving Vincristine Silent aspiration with thin liquids Silent aspiration with thin and nectar thick liquids Silent aspiration with thin, nectar and honey thick liquids No evidence of aspiration with purees or solids
13 Management of Pharyngeal Dysphagia in Children with Vincristine Toxicity Results reported back to Oncology Team Based on the extent of aspiration modifications to the oral feeding regimen were initiated In cases of aspiration with all liquid consistencies discussion regarding non-oral oral supplementation took place with the MD & Dysphagia Team
14 Aspiration with Thin Liquid Only Diet of nectar thick liquids Recommend referral to nutrition to ensure adequate hydration and child acceptance Report results to Oncology Clinic Medical team to discuss changes to dose/strength of Vincristine Develop plan for repeat VFSS once team feels neurotoxicity is resolving Parents also report improved clinical status which helps guide timeline for reassessment of swallow function
15 Medical Concerns Larger medical concern whether to discontinue cycle of Vincristine to avoid further exacerbation of the toxicity vs. decreasing the dose/strength of the Vincristine. Child may be made NPO with continuation of chemotherapy with dose changes. Child put on rest from a swallowing standpoint with period of going off the drug Above decision made by attending oncologist with input from the Oncology-Dysphagia team
16 Medical-Ethical Considerations Decision to withhold chemotherapy treatment to allow neurotoxicity to improve Parental stressors regarding decision Patients taken off Vincristine for # weeks while swallow function improves Child continues to orally feed with modifications in place
17 Resolution of Swallow Function Swallow function resolved (returned to pre-vincristine status) in 100% of patients. Range of time it took for swallow function to return to normal Normal defined as back to full oral diet of thin liquids, purees and solids # of VFSS patients underwent until swallow function resolved. (at what time intervals). Recurrence once patient resumed Vincristine treatment Yes in some patients Even at reduced strength of drug (50% strength). Oncology team was very conservative with re-starting chemotherapy/ altered doses and child monitored closely
18 Case Study Vincristine Toxicity 5/10/04: 3 ½ year old girl is diagnosed with acute lymphoblastic leukemia (ALL) Immediately begins chemotherapy (including vincristine) Throughout 7 months of chemotherapy, pt. is seen frequently in clinic for chronic upper respiratory tract congestion and persistent coughing
19 Case Study Vincristine Toxicity 12/27/04: Diagnosed with pneumonia on chest x-rayx 2/3/05: Pt. referred for initial VFSS by oncology team 9 months into chemotherapy treatments VFSS revealed silent aspiration with thin liquids Patient safe to continue to receive nectar-thick thick liquids, purees, and chewable solids


20 Case Study: Vincristine Toxicity Insert VFSS # 1 of silent aspiration with thin liquids (2/3/05)
21 Case Study Vincristine Toxicity 2/4/05: Vincristine component of chemotherapy is withheld Pt. remained on nectar-thick thick liquids, purees, solids 2/28/05: Repeat VFSS continued to reveal silent aspiration with thin liquids Recommendation: remain on altered oral diet 4/21/05: Repeat VFSS revealed normal swallow function with no documentation of aspiration with thin liquids Respiratory status stable

22 Case Study: Vincristine Toxicity Insert VFSS of normal swallow function with no aspiration (4/21/05)
23 Case Study Vincristine Toxicity 4/28/05: Vincristine resumed (50% strength) (Pt. maintained nectar-thick thick liquid diet) 6/20/05: 2 mo. follow-up VFSS revealed silent aspiration with thin liquids Recommendation: Cont. nectar-thick thick liquids Pt. continues receiving vincristine Pt. was asymptomatic from respiratory standpoint during this time
24 Outcome: Case Study Vincristine Toxicity 10/1/05: Patient completed course of chemotherapy (No longer receiving vincristine) 11/3/05: Repeat VFSS was normal with no further evidence of aspiration with thin liquids Pt. cleared for full oral diet Follow-up: Patient tolerated re-introduction of thin liquids and maintained stable respiratory status
25 Complex Decision Making in Pediatric Dysphagia Part 2 Type 1 Laryngeal Cleft
26 What is a Laryngeal Cleft (LC)? Communication between the posterior larynx and esophagus Failure of tracheo-esophageal esophageal septum to develop
27 Laryngeal Embryology Trachea and esophagus share common lumen during embryogenesis 35th day of gestation Laryngeal cleft is the failure of the interarytenoid tissue or cricoid tissue to fuse in the posterior midline
28 Types of Laryngeal Clefts Four classifications of laryngeal clefts Type 3 and 4 diagnosed on first day of life due to severity Type 1 and 2 diagnosis may take months to years. Type 1 is the focus of our talk today.
29 Classification of Laryngeal Clefts According to length Type 1: interarynenoid only Type 2: partial cricoid Type 3: complete cricoid Type 4: extending into trachea


30 Classification of Laryngeal Clefts Benjamin and Inglis, 1989

31
32 Clinical Signs & Symptoms of Type 1 Laryngeal Cleft Noisy breathing Inspiratory stridor Coughing & choking with feedings Chronic pulmonary infections Aspiration A s s and B s B s with feedings Cyanosis
33 Differential Diagnosis of Type 1 LC VFSS (MBS) FEES Chest x-rayx Referral to pediatric Otolaryngologist and Pulmonologist High degree of suspicion of type 1 laryngeal cleft (LC) Direct laryngoscopy is needed for definitive diagnosis and is the gold standard for diagnosis
34 Suspicion of Type 1 LC Child presents with normal development with exception of isolated swallowing dysfunction No evidence of neurogenic,, medical, and genetic etiology for swallow dysfunction.
35 Incidence of Laryngeal Clefts (all types) Rare, less than 0.1% Incidence increases to 0.6% in patients with the co-existence of TEF and laryngeal cleft Strong association with other anomalies, but in our population has often existed in isolation (Cotton & Prescott, 1998)
36 Type 1 LC at Children s s Hospital Boston 30 patients diagnosed with type 1 laryngeal cleft from patients repaired. >90% patients with improved swallow function after repair.
37 Incidence on the rise Literature review documents incidence of type 1 laryngeal cleft higher than in the past. 7.6% (Chien et al, 2006) 6.2% (Watters & Russell,, 2003) 7.1% (Parsons et al, 1998) Are there now more patients with type 1 laryngeal cleft or are we getting better at the diagnosis?
38 Associated Congenital Anomalies with laryngeal cleft Pallister-Hall Syndrome G Syndrome TEF Esophaeal Atresia and Stenosis
39 Team Approach to Differential Diagnosis SLP (pediatric feeding & swallowing specialist) Otolaryngologist (ENT) Pulmonologist Gastroenterologist Radiologist Developmental Pediatrician
40 Center for Aerodigestive Disorders (CADD) Monthly meeting to review complex cases and collaborate on differential diagnosis Multidisciplinary team approach to diagnosis and treatment for aerodigestive cases CADD clinic meets 1x per month Patients see GI, ORL, Pulmonary and VFSS on same day
41 Typical course of patient VFSS: documentation of aspiration of thin liquids Unable to visualize laryngeal cleft on fluoroscopy Patient placed on treatment of thickened liquids PCP referral to Otolaryngologist for further assessment
42 Alternate treatments for Type 1 LC Identification and management of GERD Thickened liquids NG-tube or G-tubeG These treatments may be implemented prior to surgical repair
43 Surgical treatment of Type 1 LC Historically, an invasive surgical procedure Endoscopic procedure Robotic Procedure at Children ldren s s Hospital Boston


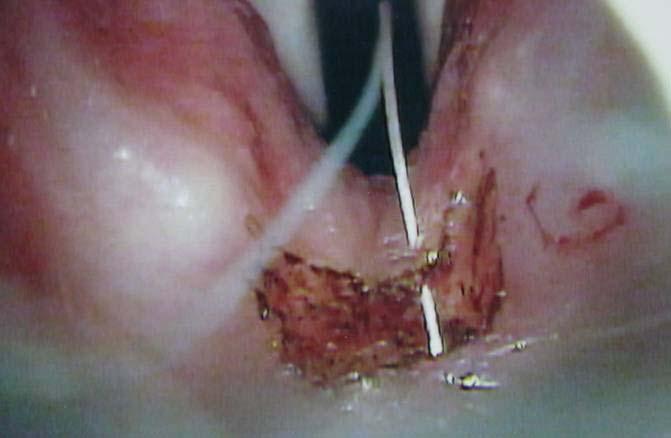


44 Laryngeal Cleft Endoscopic repair
45 Timeline from diagnosis to recovery VFSS ORL consult Direct laryngoscopy Maintenance diet Repair Repeat VFSS weeks after repair Full recovery not documented on VFSS until months post surgery
46 Case Study Laryngeal Cleft 16-month-old old boy with normal growth and development Admitted to CHB for: -respiratory distress -fever of 102 -perioral cyanosis -mother reports history of 6 episodes of pneumonia in the past 5 months (all LLL)
47 Case Study Laryngeal Cleft Videofluoroscopic swallow study performed during admission: Revealed: silent aspiration with thin liquids silent aspiration with nectar-thick thick liquids Safe to consume honey-thick liquids, purees and chewable solids orally Recommended nutrition consult to assess hydration needs on honey-thick liquids
48 INSERT VFSS HERE of pt. aspirating with thin and nectar-thick thick liquids Case Study: Laryngeal Cleft
49 Case Study Laryngeal Cleft PCP referral to Otolaryngology (ORL) Direct laryngoscopy and bronchoscopy performed Type I laryngeal cleft diagnosed. 1 month later: endoscopic repair of Type I laryngeal cleft by ORL Sent home after surgery on honey-thick liquids (same pre- operative diet) Repeat VFSS 4 ½ months s/p repair revealed no aspiration with thin and nectar-thick thick liquids Patient cleared for unrestricted oral diet
50 Summary: Vincristine Toxicity in Pediatric Pharyngeal Dysphagia Low incidence problem but with significant consequences for pulmonary health, swallow function and treatment decisions. Increased awareness to respiratory symptoms in pediatric patients undergoing chemotherapy treatment. Decreased referral time. Highlights the importance of the role of the SLP on the dysphagia-oncology team.
51 Complex Decision Making in Pediatric Dysphagia Lowry, Fletcher Larson & Miller, References Benjamin B, Inglis A. Minor congenital laryngeal clefts: diagnosis and classification. ion. Ann Otol Rhinol Laryngol 1989;98: Bermudez, M., Fuster,, JL, Llinares,, E., Galera,, A, Gonzalez, C. Intraconazole-related related increased vincristine neurtoxicity: : case report and review of literature, Journal of Pediatric Hematology & Oncology, 2005, July 27(7): Boseley,, Mark et al., The utility of fiberoptic endoscopic evaluation of swallowing (FEES) in diagnosing and treating children with Type 1 laryngeal clefts. International Journal of Pediatric Otorhinolaryngology (2006) 70, Chien,, Wade et al., Type 1 laryngeal cleft: Establishing a functional diagnostic and management algorithm, International Journal of Pediatric Otorhinolaryngology (2006). Article in press. Cotton, R.T. & Prescott, C.A.J Congenital anomalies of the e larynx. In Cotton, R.T. & Myer, C.M. (eds( eds). Prescribed paediatric otolaryngology: Philadelphia: Lippincott-Raven. Jeng,, MR, Feusner,, J. Itraconazole-enhanced enhanced vincristine neurotoxicity in a child with acute lymphoblastic leukemia. Pediatric Hematology & Oncology. 2001, March: 18 (2): Langmore,, Susan. Evaluation of oropharyngeal dysphagia: : which diagnostic tool is superior, Curr. Opin. Otolaryngol.. Head Neck Surg.. 11 (2003) Parsons, D, Stivers,, F, Giovaeto,, D, Phillips, S. Type1 posterior laryngeal clefts, Laryngoscope 108, March Schulmeister,, Lisa, RN, MN, CS, OCN. Preventing Vincristine Sulfate Medication Errors. Oncology Nursing Forum, Volume 3, No. 5, E90-E98. E98. Watters, K, Russell, J. Diagnosis and management of type 1 laryngeal cleft, Int. J. Pediatric Otorhinolaryngology.. 67, June
VIDEOFLUOROSCOPIC SWALLOWING EXAM
 VIDEOFLUOROSCOPIC SWALLOWING EXAM INDENTIFYING INFORMATION May include the following: Name, ID/medical record number, date of birth, date of exam, referred by, reason for referral HISTORY/SUBJECTIVE INFORMATION
VIDEOFLUOROSCOPIC SWALLOWING EXAM INDENTIFYING INFORMATION May include the following: Name, ID/medical record number, date of birth, date of exam, referred by, reason for referral HISTORY/SUBJECTIVE INFORMATION
Eosinophilic Esophagitis: Extraesophageal Manifestations
 Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
Eosinophilic Esophagitis: Extraesophageal Manifestations Karen B. Zur, MD Director, Pediatric Voice Program Associate Director, Center for Pediatric Airway Disorders The Children s Hospital of Philadelphia
The Role of the Speech Language Pathologist & Spinal Cord Injury
 The Role of the Speech Language Pathologist & Spinal Cord Injury Facts According to the National Spinal Cord Injury Statistical Center (NSCISC) there are approxiamtely 12,000 new spinal cord injuries (SCI)
The Role of the Speech Language Pathologist & Spinal Cord Injury Facts According to the National Spinal Cord Injury Statistical Center (NSCISC) there are approxiamtely 12,000 new spinal cord injuries (SCI)
Guideline of Videofluoroscopic Swallowing Study (VFSS) in Speech Therapy
 in Speech Therapy") Page 1 of 9 Guideline of Videofluoroscopic Swallowing Study (VFSS) in Speech Therapy Version 1.0 Effective Date Document Number HKIST-C-VFG-v1 Author HKAST AR Sub-committee Custodian Chairperson of HKIST
Page 1 of 9 Guideline of Videofluoroscopic Swallowing Study (VFSS) in Speech Therapy Version 1.0 Effective Date Document Number HKIST-C-VFG-v1 Author HKAST AR Sub-committee Custodian Chairperson of HKIST
Disclosures. Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia. Case Presentation. Case Presentation.
 Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Disclosures Repaired Esophageal Atresia and Tracheoesophageal Fistula and Chronic Dysphagia Dr. DeBoer is funded by Colorado Clinical and Translational Science Institute KL2 TR001080 Emily DeBoer MD Assistant
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Swallowing Screen Why? How? and So What? พญ.พวงแก ว ธ ต สก ลช ย ภาคว ชาเวชศาสตร ฟ นฟ คณะแพทยศาสตร ศ ร ราชพยาบาล
 Swallowing Screen Why? How? and So What? พญ.พวงแก ว ธ ต สก ลช ย ภาคว ชาเวชศาสตร ฟ นฟ คณะแพทยศาสตร ศ ร ราชพยาบาล Dysphagia in Stroke The incidence of dysphagia after stroke ranging from 23-50% 1 Location
Swallowing Screen Why? How? and So What? พญ.พวงแก ว ธ ต สก ลช ย ภาคว ชาเวชศาสตร ฟ นฟ คณะแพทยศาสตร ศ ร ราชพยาบาล Dysphagia in Stroke The incidence of dysphagia after stroke ranging from 23-50% 1 Location
Anna & John J. Sie Center for Down Syndrome Affiliates
 Anna & John J. Sie Center for Down Syndrome Affiliates Types of Medical Research Bench or basic research: done in a controlled laboratory setting using nonhuman subjects Clinical research: answer questions
Anna & John J. Sie Center for Down Syndrome Affiliates Types of Medical Research Bench or basic research: done in a controlled laboratory setting using nonhuman subjects Clinical research: answer questions
Feeding and Swallowing Problems in the Child with Special Needs
 Feeding and Swallowing Problems in the Child with Special Needs Joan Surfus, OTR/L, SWC Amy Lynch, MS, OTR/L Misericordia University This presentation is made possible, in part, by the support of the American
Feeding and Swallowing Problems in the Child with Special Needs Joan Surfus, OTR/L, SWC Amy Lynch, MS, OTR/L Misericordia University This presentation is made possible, in part, by the support of the American
New Evidence-Based Support of a 3 Ounce Water Swallow Challenge Protocol
 New Evidence-Based Support of a 3 Ounce Water Swallow Challenge Protocol Steven B. Leder, Ph.D. Yale University School of Medicine New Haven, Connecticut Debra M. Suiter, Ph.D. VA Medical Center-Memphis
New Evidence-Based Support of a 3 Ounce Water Swallow Challenge Protocol Steven B. Leder, Ph.D. Yale University School of Medicine New Haven, Connecticut Debra M. Suiter, Ph.D. VA Medical Center-Memphis
4/11/2013. & approaches to management. Disclosure. No financial support
 Laryngomalacia: ay aaca pese presentations tato s & approaches to management Hamdy El-Hakim FRCS(Ed) FRCS(ORL) Associate Professor Pediatric Otolaryngology Division of Otolaryngology Head & Neck Surgery
Laryngomalacia: ay aaca pese presentations tato s & approaches to management Hamdy El-Hakim FRCS(Ed) FRCS(ORL) Associate Professor Pediatric Otolaryngology Division of Otolaryngology Head & Neck Surgery
Clinical Study Aspiration before and after Supraglottoplasty regardless of Technique
 International Otolaryngology Volume 2010, Article ID 912814, 5 pages doi:10.1155/2010/912814 Clinical Study Aspiration before and after Supraglottoplasty regardless of Technique Jeffrey C. Rastatter, 1,
International Otolaryngology Volume 2010, Article ID 912814, 5 pages doi:10.1155/2010/912814 Clinical Study Aspiration before and after Supraglottoplasty regardless of Technique Jeffrey C. Rastatter, 1,
Department of Pediatric Otolarygnology. ENT Specialty Programs
 Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
Department of Pediatric Otolarygnology ENT Specialty Programs Staffed by fellowship-trained otolaryngologists, assisted by pediatric nurse practitioners, ENT (Otolaryngology) at Nationwide Children s Hospital
FLOOVIDEOFLUOROSCOPIC SWALLOW STUDIES: LOOKING BEYOND ASPIRATION. Brenda Sitzmann, MA, CCC-SLP (816)
") FLOOVIDEOFLUOROSCOPIC SWALLOW STUDIES: LOOKING BEYOND ASPIRATION Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 DISCLOSURES Ms. Sitzmann is speech-language pathologist at Children s Mercy
FLOOVIDEOFLUOROSCOPIC SWALLOW STUDIES: LOOKING BEYOND ASPIRATION Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 DISCLOSURES Ms. Sitzmann is speech-language pathologist at Children s Mercy
SWALLOWING: HOW CAN WE HELP
 SWALLOWING: HOW CAN WE HELP Carol Romero-Clark, M.S., CCC-SLP University of New Mexico Hospital Speech Pathology Department November 10, 2017 What happens when you swallow? Mouth (Oral Phase) Your tongue
SWALLOWING: HOW CAN WE HELP Carol Romero-Clark, M.S., CCC-SLP University of New Mexico Hospital Speech Pathology Department November 10, 2017 What happens when you swallow? Mouth (Oral Phase) Your tongue
SWALLOWING DIFFICULTIES IN HD
 Nutrition, eating and swallowing needs, challenges and solutions Workshop SWALLOWING DIFFICULTIES IN HD Angela Nuzzi Speech and Language Pathologist (SLP) EHDN Language Coordinator - Italy The role of
Nutrition, eating and swallowing needs, challenges and solutions Workshop SWALLOWING DIFFICULTIES IN HD Angela Nuzzi Speech and Language Pathologist (SLP) EHDN Language Coordinator - Italy The role of
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant. Tara Brennan, MD 2,3
 Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Multilevel airway obstruction including rare tongue base mass presenting as severe croup in an infant Tara Brennan, MD 2,3 Jeffrey C. Rastatter, MD, FAAP 1,2 1 Department of Otolaryngology, Northwestern
Dysphagia and Swallowing. Jan Adams, DNP, MPA, RN and Karen Kern
 Dysphagia and Swallowing Jan Adams, DNP, MPA, RN and Karen Kern Scope of the Problem and Incidence 15 million people in the US have some form of Dysphagia. Every year, 1 million people are diagnosed with
Dysphagia and Swallowing Jan Adams, DNP, MPA, RN and Karen Kern Scope of the Problem and Incidence 15 million people in the US have some form of Dysphagia. Every year, 1 million people are diagnosed with
Screening and Clinical Assessment for Dysphagia: How to Decide.
 Screening and Clinical Assessment for Dysphagia: How to Decide. How to Decide. ASHA Convention 2014 James L. Coyle, Ph.D., CCC-SLP, BCS-S Associate Professor, Communication Science & Disorders, University
Screening and Clinical Assessment for Dysphagia: How to Decide. How to Decide. ASHA Convention 2014 James L. Coyle, Ph.D., CCC-SLP, BCS-S Associate Professor, Communication Science & Disorders, University
Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy
 Case Report Brunei Int Med J. 2014; 10 (1): 55-59 Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy Zara
Case Report Brunei Int Med J. 2014; 10 (1): 55-59 Laryngomalacia, laryngeal cleft and congenital unilateral vocal cord palsy: A unique case treated endoscopically without intubation or tracheostomy Zara
IAEM Clinical Guideline 9 Laryngomalacia. Version 1 September, Author: Dr Farah Mustafa
 IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
IAEM Clinical Guideline 9 Laryngomalacia Version 1 September, 2016 Author: Dr Farah Mustafa Guideline lead: Dr Áine Mitchell, in collaboration with IAEM Clinical Guideline committee and Our Lady s Children
Grand Rounds: Pediatric Dysphagia Due to Anatomic & Neurologic Etiologies
 Joan C. Arvedson, PhD, BC-NCD, BRS-S Children's Hospital of Wisconsin Milwaukee Department of Pediatrics, Medical College of Wisconsin Maureen A. Lefton-Greif, PhD, CCC/SLP, BRS-S Johns Hopkins Medical
Joan C. Arvedson, PhD, BC-NCD, BRS-S Children's Hospital of Wisconsin Milwaukee Department of Pediatrics, Medical College of Wisconsin Maureen A. Lefton-Greif, PhD, CCC/SLP, BRS-S Johns Hopkins Medical
Assessing the Eating Needs of Personal Care Services (PCS) Beneficiaries Effective 12/1/2016
 Beneficiaries Effective 12/1/2016") Assessing the Eating Needs of Personal Care Services (PCS) Beneficiaries Effective 12/1/2016 The Freedom to Succeed November 22,2016 Content Introduction Signs and Symptoms Caring for Individuals with
Assessing the Eating Needs of Personal Care Services (PCS) Beneficiaries Effective 12/1/2016 The Freedom to Succeed November 22,2016 Content Introduction Signs and Symptoms Caring for Individuals with
Laryngomalacia and Swallowing Function in Children
 The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. TRIOLOGICAL SOCIETY CANDIDATE THESIS Laryngomalacia and Swallowing Function in Children Jeffrey P. Simons,
The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. TRIOLOGICAL SOCIETY CANDIDATE THESIS Laryngomalacia and Swallowing Function in Children Jeffrey P. Simons,
Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience
 1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
Unilateral Supraglottoplasty for Severe Laryngomalacia in Children. Nasser A Fageeh, MD, FRCSC, FACS*
 Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
Bahrain Medical Bulletin, Vol. 37, No. 1, March 2015 Unilateral Supraglottoplasty for Severe Laryngomalacia in Children Nasser A Fageeh, MD, FRCSC, FACS* Objective: To study the efficacy of Unilateral
Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis
 Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Otolaryngology Head and Neck Surgery (2006) 135, 318-322 ORIGINAL RESEARCH Pediatric partial cricotracheal resection: A new technique for the posterior cricoid anastomosis Mark E. Boseley, MD, and Christopher
Clinical Swallowing Exam
 Clinical Evaluation Template 1 Clinical Exam Name: ID/Medical record number: Date of exam: Referred by: Reason for referral: Medical diagnosis: Date of onset of diagnosis: Other relevant medical history/diagnoses/surgery
Clinical Evaluation Template 1 Clinical Exam Name: ID/Medical record number: Date of exam: Referred by: Reason for referral: Medical diagnosis: Date of onset of diagnosis: Other relevant medical history/diagnoses/surgery
Pediatric Modified Barium Swallow Studies. Presented by Jody Bousquet, MA, CCC- SLP Susan Shonbrun, MS, CCC- SLP November 7, 2015
 Pediatric Modified Barium Swallow Studies Presented by Jody Bousquet, MA, CCC- SLP Susan Shonbrun, MS, CCC- SLP November 7, 2015 Definition * Modified Barium Swallow Study * Assesses swallow functions
Pediatric Modified Barium Swallow Studies Presented by Jody Bousquet, MA, CCC- SLP Susan Shonbrun, MS, CCC- SLP November 7, 2015 Definition * Modified Barium Swallow Study * Assesses swallow functions
ORIGINAL ARTICLE. Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty
 ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
ORIGINAL ARTICLE Synchronous Airway Lesions and Outcomes in Infants With Severe Laryngomalacia Requiring Supraglottoplasty James W. Schroeder Jr, MD; Naveen D. Bhandarkar, MD; Lauren D. Holinger, MD Objective:
Respiratory Compromise and Swallowing
 Speech Pathology and Respiratory Care April 11, 2013 By Angela Parcaro-Tucker, MA, CCC-SLP, LSVT How can Speech Therapy help? 1 Respiratory Compromise and Swallowing Swallowing is a complex sequence of
Speech Pathology and Respiratory Care April 11, 2013 By Angela Parcaro-Tucker, MA, CCC-SLP, LSVT How can Speech Therapy help? 1 Respiratory Compromise and Swallowing Swallowing is a complex sequence of
Implementing Cough Reflex Testing in a clinical pathway for acute stroke: A pragmatic randomised control trial
 Implementing Cough Reflex Testing in a clinical pathway for acute stroke: A pragmatic randomised control trial Makaela Field 1, Rachel Wenke 1,2, Arman Sabet 1, Melissa Lawrie 1,2, Elizabeth Cardell 2
Implementing Cough Reflex Testing in a clinical pathway for acute stroke: A pragmatic randomised control trial Makaela Field 1, Rachel Wenke 1,2, Arman Sabet 1, Melissa Lawrie 1,2, Elizabeth Cardell 2
Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia Difficulty
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia Difficulty
What are the Challenges? Spreading the Word in NICU. Need for NICU Care: Impact. Baby Trachs: Use of the Passy Muir Valve in the NICU to
 What are the Challenges? Baby Trachs: Use of the Passy Muir Valve in the NICU to Optimize Swallowing and Feeding Catherine S Shaker, MS/CCC SLP, BRS S and Cari Mutnick, MS/CCC SLP Florida Hospital for
What are the Challenges? Baby Trachs: Use of the Passy Muir Valve in the NICU to Optimize Swallowing and Feeding Catherine S Shaker, MS/CCC SLP, BRS S and Cari Mutnick, MS/CCC SLP Florida Hospital for
Esophageal Cancer. Source: National Cancer Institute
 Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
MULTIPLE reports have. Prediction of Aspiration in Patients With Newly Diagnosed Untreated Advanced Head and Neck Cancer ORIGINAL ARTICLE
 ORIGINAL ARTICLE Prediction of Aspiration in Patients With Newly Diagnosed Untreated Advanced Head and Neck Cancer Arie Rosen, MD; Thomas H. Rhee, MD; Rene Kaufman, MS, CCC-SLP Objectives: To determine
ORIGINAL ARTICLE Prediction of Aspiration in Patients With Newly Diagnosed Untreated Advanced Head and Neck Cancer Arie Rosen, MD; Thomas H. Rhee, MD; Rene Kaufman, MS, CCC-SLP Objectives: To determine
RECOMMENDATIONS & UPDATES IN THE MANAGEMENT OF POST- STROKE DYSPHAGIA
 RECOMMENDATIONS & UPDATES IN THE MANAGEMENT OF POST- STROKE DYSPHAGIA Feeding in the Acute Stroke Period: - Early initiation of feeding is beneficial w/c decreases the risk of infections, improve survival
RECOMMENDATIONS & UPDATES IN THE MANAGEMENT OF POST- STROKE DYSPHAGIA Feeding in the Acute Stroke Period: - Early initiation of feeding is beneficial w/c decreases the risk of infections, improve survival
5 Things I Want You to Know About Dysphagia. Prof Maggie-Lee Huckabee The University of Canterbury Rose Centre for Stroke Recovery and Research
 5 Things I Want You to Know About Dysphagia Prof Maggie-Lee Huckabee The University of Canterbury Rose Centre for Stroke Recovery and Research 5 things 1) Why we can t diagnose dysphagia at bedside. 2)
5 Things I Want You to Know About Dysphagia Prof Maggie-Lee Huckabee The University of Canterbury Rose Centre for Stroke Recovery and Research 5 things 1) Why we can t diagnose dysphagia at bedside. 2)
DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP
 DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP OVERVIEW Decision making re: swallowing in the medically compromised patient Swallow evaluation vs. Nursing Swallow Screening Instrumental
DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP OVERVIEW Decision making re: swallowing in the medically compromised patient Swallow evaluation vs. Nursing Swallow Screening Instrumental
Ancillary care team (nursing, therapists, etc):
:") 1 A. Preliminary Information Reason for referral: Chronological age (Adjusted age): Primary caregiver: Informant for evaluation: Primary language: Interpreter Family concerns Barriers to learning: B. Background
1 A. Preliminary Information Reason for referral: Chronological age (Adjusted age): Primary caregiver: Informant for evaluation: Primary language: Interpreter Family concerns Barriers to learning: B. Background
IVOR LEWIS Esophagogastrectomy
 IVOR LEWIS Esophagogastrectomy SPEECH-LANGUAGE PATHOLOGY S ROLE MAGGIE BOYD, MS, CCC/SLP Biography Maggie Boyd, MS, CCC-SLP is a dysphagia clinical specialist at UAB hospital. She has 14 years clinical
IVOR LEWIS Esophagogastrectomy SPEECH-LANGUAGE PATHOLOGY S ROLE MAGGIE BOYD, MS, CCC/SLP Biography Maggie Boyd, MS, CCC-SLP is a dysphagia clinical specialist at UAB hospital. She has 14 years clinical
FEEDING THE MEDICAL COMPLEX PEDIATRIC PATIENT. Brenda Sitzmann, MA, CCC-SLP (816)
") FEEDING THE MEDICAL COMPLEX PEDIATRIC PATIENT Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 DISCLOSURES Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives
FEEDING THE MEDICAL COMPLEX PEDIATRIC PATIENT Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 DISCLOSURES Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives
Non-Oral Feedings. Disclosures. Feeding the Medical Complex Pediatric Patient. Pediatric Feeding Disorder. Overview.
 Feeding the Medical Complex Pediatric Patient Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 Disclosures Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives
Feeding the Medical Complex Pediatric Patient Brenda Sitzmann, MA, CCC-SLP bksitzmann@cmh.edu (816) 302-8037 Disclosures Ms. Sitzmann is speech-language pathologist at Children s Mercy for which she receives
Reluctance or refusal to feed or eat. Understanding Feeding Aversion in a City Full of Foodies. Presentation Outline. Learning Objectives
 Understanding Feeding Aversion in a City Full of Foodies Amy Houtrow, MD, MPH Pediatric Physical Medicine & Rehabilitation UCSF Department of Pediatrics June 2, 2007 Learning Objectives Learners will be
Understanding Feeding Aversion in a City Full of Foodies Amy Houtrow, MD, MPH Pediatric Physical Medicine & Rehabilitation UCSF Department of Pediatrics June 2, 2007 Learning Objectives Learners will be
When Eating Becomes A Challenge Dysphagia
 When Eating Becomes A Challenge Dysphagia 1. DYSPHAGIA, WHAT IS IT? 2. IMPLICATIONS 3. ASSESSMENT 4. COMPENSATORY SWALLOWING AND EXERCISES 5. DIET TEXTURE ADJUSTMENTS Swallowing Dysfunction = Dysphagia
When Eating Becomes A Challenge Dysphagia 1. DYSPHAGIA, WHAT IS IT? 2. IMPLICATIONS 3. ASSESSMENT 4. COMPENSATORY SWALLOWING AND EXERCISES 5. DIET TEXTURE ADJUSTMENTS Swallowing Dysfunction = Dysphagia
Feeding / Swallowing Development and Disorders in Children: For Graduate Students
 Feeding / Swallowing Development and Disorders in Children: For Graduate Students ASHA November 18, 2010 Maureen A. Lefton-Greif, PhD, CCC-SLP, BRS-S Associate Professor, Dept. of Pediatrics The Eudowood
Feeding / Swallowing Development and Disorders in Children: For Graduate Students ASHA November 18, 2010 Maureen A. Lefton-Greif, PhD, CCC-SLP, BRS-S Associate Professor, Dept. of Pediatrics The Eudowood
MY CHILD WON T EAT. Disclosure
 MY CHILD WON T EAT How to help a child with a feeding disorder Richard J Noel, MD, PhD Disclosure In the past 12 months, I have had no relevant financial relationships with the manufacturer(s) of any commercial
MY CHILD WON T EAT How to help a child with a feeding disorder Richard J Noel, MD, PhD Disclosure In the past 12 months, I have had no relevant financial relationships with the manufacturer(s) of any commercial
State of Art & Science for Evaluation of Infants & Children with Signs/Symptoms of Dysphagia. Introduction. Instrumental Swallow Evaluations
 Problem Solving with Instrumental Swallow Evaluations & Management 49 th Annual Mid-South Conference, Feb. 21, 2019 Joan C. Arvedson, PhD, CCC-SLP, BCS-S, ASHA Honors & Fellow jcarved@aol.com & jarvedson@chw.org
Problem Solving with Instrumental Swallow Evaluations & Management 49 th Annual Mid-South Conference, Feb. 21, 2019 Joan C. Arvedson, PhD, CCC-SLP, BCS-S, ASHA Honors & Fellow jcarved@aol.com & jarvedson@chw.org
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
Swallow Function: Passy-Muir Valve Use for Evaluation & Rehabilitation David A. Muir Course Outline Physiology of Swallow
 Swallow Function: Passy-Muir Valve Use for Evaluation & Rehabilitation Mary Spremulli, MA, CCC-SLP Passy-Muir Clinical Consultant spre713@hotmail.com (949) 833-8255 David A. Muir 23 year-old ventilator
Swallow Function: Passy-Muir Valve Use for Evaluation & Rehabilitation Mary Spremulli, MA, CCC-SLP Passy-Muir Clinical Consultant spre713@hotmail.com (949) 833-8255 David A. Muir 23 year-old ventilator
ORIGINAL ARTICLE. Unilateral vs Bilateral Supraglottoplasty for Severe Laryngomalacia in Children
 Unilateral vs Bilateral Supraglottoplasty for Severe Laryngomalacia in Children Deepkaran K. Reddy, MD; Bruce H. Matt, MD, MS, FAAP ORIGINAL ARTICLE Objectives: To study the efficacy of unilateral supraglottoplasty
Unilateral vs Bilateral Supraglottoplasty for Severe Laryngomalacia in Children Deepkaran K. Reddy, MD; Bruce H. Matt, MD, MS, FAAP ORIGINAL ARTICLE Objectives: To study the efficacy of unilateral supraglottoplasty
The Paediatric Voice Clinic
 The Paediatric Voice Clinic Smillie I 1, McManus K 1, Cohen W 2, Wynne D1. Department of Paediatric Otolaryngology, Royal Hospital for Sick Children, Glasgow. 2 School of Psychological Sciences and Health,
The Paediatric Voice Clinic Smillie I 1, McManus K 1, Cohen W 2, Wynne D1. Department of Paediatric Otolaryngology, Royal Hospital for Sick Children, Glasgow. 2 School of Psychological Sciences and Health,
Congenital Tracheoesophageal Anomalies: perinatal imaging findings and common complications
 Congenital Tracheoesophageal Anomalies: perinatal imaging findings and common complications Poster No.: C-2246 Congress: ECR 2013 Type: Educational Exhibit Authors: T. L. Martin, I. Maianski; Halifax,
Congenital Tracheoesophageal Anomalies: perinatal imaging findings and common complications Poster No.: C-2246 Congress: ECR 2013 Type: Educational Exhibit Authors: T. L. Martin, I. Maianski; Halifax,
Dysphagia goes International
 Sponsor Disclosure: Support for this presentation was provided by the Foodservice Express division of Med-Diet, Inc. The material herein is for educational purposes only. Reproduction or distribution of
Sponsor Disclosure: Support for this presentation was provided by the Foodservice Express division of Med-Diet, Inc. The material herein is for educational purposes only. Reproduction or distribution of
Dysphagia goes International
 Sponsor Disclosure: Support for this presentation was provided by the Foodservice Express division of Med-Diet, Inc. The material herein is for educational purposes only. Reproduction or distribution of
Sponsor Disclosure: Support for this presentation was provided by the Foodservice Express division of Med-Diet, Inc. The material herein is for educational purposes only. Reproduction or distribution of
Tracheoesophageal Fistula and Esophageal Atresia
 Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
Patient and Family Education Tracheoesophageal Fistula and Esophageal Atresia What is tracheoesophageal fistula? The word fistula means abnormal connection. Tracheoesophageal fistula (TEF) is a condition
B. Background Information B1. Summary Medical team (physicians, dentists, etc ): Ancillary care team (nursing, therapists, etc ):
: Ancillary care team (nursing, therapists, etc ):") 1 A. Preliminary Information Reason for referral: Chronological age (Adjusted age): Primary caregiver: Informant for evaluation: Primary language: Interpreter Family concerns Barriers to learning: B. Background
1 A. Preliminary Information Reason for referral: Chronological age (Adjusted age): Primary caregiver: Informant for evaluation: Primary language: Interpreter Family concerns Barriers to learning: B. Background
A Clicking Larynx: Diagnostic and Therapeutic Challenges
 The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Case Report A Clicking Larynx: Diagnostic and Therapeutic Challenges Derrek A. Heuveling, MD, PhD ; Maarten
The Laryngoscope VC 2017 The American Laryngological, Rhinological and Otological Society, Inc. Case Report A Clicking Larynx: Diagnostic and Therapeutic Challenges Derrek A. Heuveling, MD, PhD ; Maarten
Daniels SK & Huckabee ML (2008). Dysphagia Following Stroke. Muscles of Deglutition. Lateral & Mesial Premotor Area 6. Primary Sensory
. Dysphagia Following Stroke. Muscles of Deglutition. Lateral & Mesial Premotor Area 6. Primary Sensory") An Overview of Dysphagia in the Stroke Population Stephanie K. Daniels, PhD Michael E. DeBakey VA Medical Center PM & R, Baylor College of Medicine Communication Sciences and Disorders, University of Houston
An Overview of Dysphagia in the Stroke Population Stephanie K. Daniels, PhD Michael E. DeBakey VA Medical Center PM & R, Baylor College of Medicine Communication Sciences and Disorders, University of Houston
The following slides are from a. presentation given by. H. Worth Boyce, M.D. on. Specialized Studies on Diseases of the Esophagus.
 The following slides are from a presentation given by H. Worth Boyce, M.D. on Endoscopic Lumen Restoration at the 8 th OESO World Organization for Specialized Studies on Diseases of the Esophagus. Endoscopic
The following slides are from a presentation given by H. Worth Boyce, M.D. on Endoscopic Lumen Restoration at the 8 th OESO World Organization for Specialized Studies on Diseases of the Esophagus. Endoscopic
Laryngotracheoesophageal Cleft; Neonatal Presentation and Diagnostic Challenges
 CASE REPORT Laryngotracheoesophageal Cleft; Neonatal Presentation and Diagnostic Challenges AbdulRahman Alnemri 1 MD, Ashraf H. Ibraheem 2 MD, Yahia Alqahtani 3, Safar M Alshahrani 4 MD Departments of
CASE REPORT Laryngotracheoesophageal Cleft; Neonatal Presentation and Diagnostic Challenges AbdulRahman Alnemri 1 MD, Ashraf H. Ibraheem 2 MD, Yahia Alqahtani 3, Safar M Alshahrani 4 MD Departments of
Dysphagia and Self Feeding in Acute Tetraplegia
 Dysphagia and Self Feeding in Acute Tetraplegia Danielle R. Karhut, OTR/L Robert Masterson, MS, CCC-SLP Spinal Cord Rehabilitation Unit UPMC Mercy Hospital/Centers for Rehab Services Pittsburgh, PA Tetraplegia
Dysphagia and Self Feeding in Acute Tetraplegia Danielle R. Karhut, OTR/L Robert Masterson, MS, CCC-SLP Spinal Cord Rehabilitation Unit UPMC Mercy Hospital/Centers for Rehab Services Pittsburgh, PA Tetraplegia
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction. Nathan Page, MD Pediatrics in the Red Rocks June?
 Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
Stridor, Stertor, and Snoring: Pediatric Upper Airway Obstruction Nathan Page, MD Pediatrics in the Red Rocks June? I have no disclosures I do not plan to discuss unapproved or off label use of products
POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW
 CHILDREN S HOSPITAL II POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW Dr. Nguyen Thuy Hanh Ngan Neonatal Department CONTENTS 1. Background 2. Classification 3. Management 4. Complications
CHILDREN S HOSPITAL II POSTOPERATIVE CONGENITAL ESOPHAGEAL ATRESIA COMPLICATIONS: A REVIEW Dr. Nguyen Thuy Hanh Ngan Neonatal Department CONTENTS 1. Background 2. Classification 3. Management 4. Complications
10/26/2017. Diagnostic Tests vs. Screening. Dysphagia Screening: What it is and what it is not
 Dysphagia Screening: What it is and what it is not Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director University of Kentucky Voice & Swallow Clinic Lexington, Kentucky ASHA's Preferred Practice Pattern on
Dysphagia Screening: What it is and what it is not Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director University of Kentucky Voice & Swallow Clinic Lexington, Kentucky ASHA's Preferred Practice Pattern on
Dysphagia after EA repair. Disclosure. Learning objectives 9/17/2013
 Dysphagia after EA repair Christophe Faure, M.D. Professor of Pediatrics, Division of Pediatric Gastroenterology, Sainte-Justine University Health Center, Université de Montréal, Montréal, QC, Canada christophe.faure@umontreal.ca
Dysphagia after EA repair Christophe Faure, M.D. Professor of Pediatrics, Division of Pediatric Gastroenterology, Sainte-Justine University Health Center, Université de Montréal, Montréal, QC, Canada christophe.faure@umontreal.ca
Managing the Patient with Dysphagia
 Managing the Patient with Dysphagia Patricia K. Lerner, MA, CCC, ASHA Fellow Board Certified Specialist in Swallowing & Swallowing Disorders Clinical Assistant Professor New York University School of Medicine
Managing the Patient with Dysphagia Patricia K. Lerner, MA, CCC, ASHA Fellow Board Certified Specialist in Swallowing & Swallowing Disorders Clinical Assistant Professor New York University School of Medicine
Swallowing Disorders and Their Management in Patients with Multiple Sclerosis
 National Multiple Sclerosis Society 733 Third Avenue New York, NY 10017-3288 Clinical Bulletin Information for Health Professionals Swallowing Disorders and Their Management in Patients with Multiple Sclerosis
National Multiple Sclerosis Society 733 Third Avenue New York, NY 10017-3288 Clinical Bulletin Information for Health Professionals Swallowing Disorders and Their Management in Patients with Multiple Sclerosis
Original Article. Double Aortic Arch in Infants and Children CH XIE, FQ GONG, GP JIANG, SL FU. Key words. Background
 HK J Paediatr (new series) 2018;23:233-238 Original Article Double Aortic Arch in Infants and Children CH XIE, FQ GONG, GP JIANG, SL FU Abstract Key words Background: This study aimed to report the diagnosis,
HK J Paediatr (new series) 2018;23:233-238 Original Article Double Aortic Arch in Infants and Children CH XIE, FQ GONG, GP JIANG, SL FU Abstract Key words Background: This study aimed to report the diagnosis,
SILENT ASPIRATION AND SWALLOWING PHYSIOLOGY AFTER RADIOTHERAPY IN PATIENTS WITH NASOPHARYNGEAL CARCINOMA
 ORIGINAL ARTICLE SILENT ASPIRATION AND SWALLOWING PHYSIOLOGY AFTER RADIOTHERAPY IN PATIENTS WITH NASOPHARYNGEAL CARCINOMA Louisa K. Y. Ng, MSc, 1 Kathy Y. S. Lee, PhD, 1 Sung Nok Chiu, Dr.rer.nat., 2 Peter
ORIGINAL ARTICLE SILENT ASPIRATION AND SWALLOWING PHYSIOLOGY AFTER RADIOTHERAPY IN PATIENTS WITH NASOPHARYNGEAL CARCINOMA Louisa K. Y. Ng, MSc, 1 Kathy Y. S. Lee, PhD, 1 Sung Nok Chiu, Dr.rer.nat., 2 Peter
DYSPHAGIA SCREENING and CLINICAL SWALLOW EVALUATIONS. Debra M. Suiter, Ph.D., CCC-SLP, BRS-S VA Medical Center-Memphis
 DYSPHAGIA SCREENING and CLINICAL SWALLOW EVALUATIONS Debra M. Suiter, Ph.D., CCC-SLP, BRS-S VA Medical Center-Memphis Suiter, ASHA, 2012 Diagnostic Tests vs. Screening Diagnostic tests are used when a
DYSPHAGIA SCREENING and CLINICAL SWALLOW EVALUATIONS Debra M. Suiter, Ph.D., CCC-SLP, BRS-S VA Medical Center-Memphis Suiter, ASHA, 2012 Diagnostic Tests vs. Screening Diagnostic tests are used when a
Gastroesophageal Reflux Disease in Infants and Children
 Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Gastroesophageal Reflux Disease in Infants and Children 4 Marzo 2017 Drssa Chiara Leoni Drssa Valentina Giorgio pediatriagastro@gmail.com valentinagiorgio1@gmail.com Definitions: GER GER is the passage
Screening. James L. Coyle, Ph.D., CCC-SLP, BRS-S University of Pittsburgh. J. Coyle 1
 Screening James L. Coyle, Ph.D., CCC-SLP, BRS-S University of Pittsburgh J. Coyle 1 Disclosure University of Pittsburgh (salary) Continuing education Northern Speech Services State Conferences and Conventions
Screening James L. Coyle, Ph.D., CCC-SLP, BRS-S University of Pittsburgh J. Coyle 1 Disclosure University of Pittsburgh (salary) Continuing education Northern Speech Services State Conferences and Conventions
The surgical management of subglottic stenosis (SGS)
") Original Research Pediatric Otolaryngology Short- versus Long-term Stenting in Children with Subglottic Stenosis Undergoing Laryngotracheal Reconstruction Otolaryngology Head and Neck Surgery 2018, Vol.
Original Research Pediatric Otolaryngology Short- versus Long-term Stenting in Children with Subglottic Stenosis Undergoing Laryngotracheal Reconstruction Otolaryngology Head and Neck Surgery 2018, Vol.
Preface... Contributors... 1 Embryology... 3
 Contents Preface... Contributors... vii xvii I. Pediatrics 1 Embryology... 3 Pearls... 3 Branchial Arch Derivatives... 3 Branchial Arch Anomalies: Cysts, Sinus, Fistulae... 4 Otologic Development... 4
Contents Preface... Contributors... vii xvii I. Pediatrics 1 Embryology... 3 Pearls... 3 Branchial Arch Derivatives... 3 Branchial Arch Anomalies: Cysts, Sinus, Fistulae... 4 Otologic Development... 4
Palliative Care Swallowing Management HEATHER STORIE M.S.,CCC-SLP, BCS-S SPEECH LANGUAGE PATHOLOGY, BOARD CERTIFIED SWALLOWING SPECIALIST
 Palliative Care Swallowing Management HEATHER STORIE M.S.,CCC-SLP, BCS-S SPEECH LANGUAGE PATHOLOGY, BOARD CERTIFIED SWALLOWING SPECIALIST Objectives Gain a general understanding of normal swallowing Gain
Palliative Care Swallowing Management HEATHER STORIE M.S.,CCC-SLP, BCS-S SPEECH LANGUAGE PATHOLOGY, BOARD CERTIFIED SWALLOWING SPECIALIST Objectives Gain a general understanding of normal swallowing Gain
Evidence-Based Swallowing Related Issues in Patients with Tracheotomy Tubes
 Evidence-Based Swallowing Related Issues in Patients with Tracheotomy Tubes Steven B. Leder, Ph.D. Yale University School of Medicine Debra M. Suiter,, Ph.D. University of Memphis Impetus Swallowing Rx
Evidence-Based Swallowing Related Issues in Patients with Tracheotomy Tubes Steven B. Leder, Ph.D. Yale University School of Medicine Debra M. Suiter,, Ph.D. University of Memphis Impetus Swallowing Rx
Validation of the Yale Swallow Protocol: A Prospective Double-Blinded Videofluoroscopic Study
 Dysphagia (2014) 29:199 203 DOI 10.1007/s00455-013-9488-3 ORIGINAL ARTICLE Validation of the Yale Swallow Protocol: A Prospective Double-Blinded Videofluoroscopic Study Debra M. Suiter JoAnna Sloggy Steven
Dysphagia (2014) 29:199 203 DOI 10.1007/s00455-013-9488-3 ORIGINAL ARTICLE Validation of the Yale Swallow Protocol: A Prospective Double-Blinded Videofluoroscopic Study Debra M. Suiter JoAnna Sloggy Steven
A study on paediatric stridor causes and management: case series
 International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
International Journal of Otorhinolaryngology and Head and Neck Surgery Selvam DK et al. Int J Otorhinolaryngol Head Neck Surg. 2017 Oct;3(4):1031-1035 http://www.ijorl.com pissn 2454-5929 eissn 2454-5937
Dysphagia Questionnaire. Referring Doctor:
 Dysphagia Questionnaire Name: Date of Birth: Address: Referring Doctor: Diagnosis: Phone number: Email: What are your complaints regarding your swallowing: Date and onset of swallowing problems: Please
Dysphagia Questionnaire Name: Date of Birth: Address: Referring Doctor: Diagnosis: Phone number: Email: What are your complaints regarding your swallowing: Date and onset of swallowing problems: Please
COMPLICATED STAPHYLOCOCCAL INFECTION IN A NEONATE. A. Ansary*, D. Varghese, L. Jackson ROYAL HOSPITAL FOR CHILDREN, GLASGOW,UK
 COMPLICATED STAPHYLOCOCCAL INFECTION IN A NEONATE A. Ansary*, D. Varghese, L. Jackson ROYAL HOSPITAL FOR CHILDREN, GLASGOW,UK Complicated staphylococcal infection in a neonate Overview Case Radiology/biochemistry/microbiology
COMPLICATED STAPHYLOCOCCAL INFECTION IN A NEONATE A. Ansary*, D. Varghese, L. Jackson ROYAL HOSPITAL FOR CHILDREN, GLASGOW,UK Complicated staphylococcal infection in a neonate Overview Case Radiology/biochemistry/microbiology
The Clinical Swallow Evaluation: What it can and cannot tell us. Introduction
 The Clinical Swallow Evaluation: What it can and cannot tell us Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director, Voice & Swallow Clinic Associate Professor, Division of Communication Sciences & Disorders
The Clinical Swallow Evaluation: What it can and cannot tell us Debra M. Suiter, Ph.D., CCC-SLP, BCS-S Director, Voice & Swallow Clinic Associate Professor, Division of Communication Sciences & Disorders
Alyssa Brzenski MD May 2, 2012
 Alyssa Brzenski MD May 2, 2012 Overview Background Pre repair bronchoscopy Thorascopic repair To extubate or not? Esophageal atresia treatment of long gap esophageal atresia Complications following TEF/EA
Alyssa Brzenski MD May 2, 2012 Overview Background Pre repair bronchoscopy Thorascopic repair To extubate or not? Esophageal atresia treatment of long gap esophageal atresia Complications following TEF/EA
Late Oropharyngeal Dysphagia Following Head and Neck Cancer Treatment ASHA 2014 Orlando, FL
 Late Oropharyngeal Dysphagia Following Head and Neck Cancer Treatment ASHA 2014 Orlando, FL Vicki Lewis, M.A., CCC SLP Disclosure No financial interests to disclose The Disney analogy; sort of Patient
Late Oropharyngeal Dysphagia Following Head and Neck Cancer Treatment ASHA 2014 Orlando, FL Vicki Lewis, M.A., CCC SLP Disclosure No financial interests to disclose The Disney analogy; sort of Patient
Evaluation and Management of Pediatric Stridor
 Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
Evaluation and Management of Pediatric Stridor Pamela Nicklaus, MD FACS Associate Professor Fellowship Director Pediatric Otolaryngology Children s Mercy Hospital and Clinics 2013 Children's 2013 Mercy
PANELISTS. Controversial Issues In Common Interventions In ORL 4/10/2014
 Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
Controversial Issues In Common Interventions In ORL Mohamed Hesham,MD Alexandria Faculty of Medicine PANELISTS Prof. Ahmed Eldaly Prof. Hamdy EL-Hakim Prof. Hossam Thabet Prof. Maged El-Shenawy Prof. Prince
Evaluation of Salivary Aspiration in Brain- Injured Patients With Tracheostomy Yujeong Kang, MD, Min Ho Chun, MD, Sook Joung Lee, MD
 Original Article Ann Rehabil Med 2013;37(1):96-102 pissn: 2234-0645 eissn: 2234-0653 http://dx.doi.org/10.5535/arm.2013.37.1.96 Annals of Rehabilitation Medicine Evaluation of Salivary Aspiration in Brain-
Original Article Ann Rehabil Med 2013;37(1):96-102 pissn: 2234-0645 eissn: 2234-0653 http://dx.doi.org/10.5535/arm.2013.37.1.96 Annals of Rehabilitation Medicine Evaluation of Salivary Aspiration in Brain-
An Overview on Pediatric Esophageal Disorders. Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II
 An Overview on Pediatric Esophageal Disorders Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II Case report F.C. 3 year old boy Preterm born from emergency
An Overview on Pediatric Esophageal Disorders Annamaria Staiano Department of Translational Medical Sciences University of Naples Federico II Case report F.C. 3 year old boy Preterm born from emergency
Gastroesophageal Reflux in Infants. Kathleen Borowitz, MS, CCC-SLP Speech-Language Pathologist University of Virginia Children s Hospital
 Gastroesophageal Reflux in Infants Kathleen Borowitz, MS, CCC-SLP Speech-Language Pathologist University of Virginia Children s Hospital Disclaimers Speech-language pathologist, not a pediatrician Married
Gastroesophageal Reflux in Infants Kathleen Borowitz, MS, CCC-SLP Speech-Language Pathologist University of Virginia Children s Hospital Disclaimers Speech-language pathologist, not a pediatrician Married
Pediatrics Grand Rounds 25 October University of Texas Health Science Center at San Antonio, Texas
 PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
PEDIATRIC ENT & YOU A PATIENT CARE PARTNERSHIP Disclosure Timothy McEvoy, MD has no relevant relationships with commercial interests to disclose. Timothy McEvoy, MD UTHSCSA Department of Otolaryngology-
Evaluation of Failure to Thrive in a Young Child: Case Example of Jeff. Andrew Hsi, MD, MPH Family Medicine Pediatric Grand Rounds, 8 August 2012
 Evaluation of Failure to Thrive in a Young Child: Case Example of Jeff Andrew Hsi, MD, MPH Family Medicine Pediatric Grand Rounds, 8 August 2012 Objectives for Presentation At the end of this talk; the
Evaluation of Failure to Thrive in a Young Child: Case Example of Jeff Andrew Hsi, MD, MPH Family Medicine Pediatric Grand Rounds, 8 August 2012 Objectives for Presentation At the end of this talk; the
FOREIGN BODY ASPIRATION in children. Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital
 FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
FOREIGN BODY ASPIRATION in children Dr. Xayyavong Bouathongthip, M.D Emergency department, children s hospital How common is choking? About 3,000 people die/year from choking Figure remained unchanged
The Effect of a Speaking Valve on Laryngeal Aspiration and Penetration in Children With Tracheotomies
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. The Effect of a Speaking Valve on Laryngeal Aspiration and Penetration in Children With Tracheotomies Julina
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. The Effect of a Speaking Valve on Laryngeal Aspiration and Penetration in Children With Tracheotomies Julina
Analyzing Swallow Studies in Pediatrics
 Analyzing Swallow Studies in Pediatrics About the Speaker Robert Beecher, M.S., CCC-SLP was formerly senior speech-language pahologist at the Children's Hospital of Wisconsin in Milwaukee. He is specialized
Analyzing Swallow Studies in Pediatrics About the Speaker Robert Beecher, M.S., CCC-SLP was formerly senior speech-language pahologist at the Children's Hospital of Wisconsin in Milwaukee. He is specialized
Review of dysphagia in poststroke
 Review of dysphagia in poststroke patients Danielle Thompson, Speech and Language Therapist Northwick Park Hospital With acknowledgement to Mary McFarlane, Principal Speech and Language Therapist, Acute
Review of dysphagia in poststroke patients Danielle Thompson, Speech and Language Therapist Northwick Park Hospital With acknowledgement to Mary McFarlane, Principal Speech and Language Therapist, Acute
Dysphagia Outcomes for Patients with Feeding Tubes Undergoing Inpatient Rehabilitation: Follow-Up
 Dysphagia Outcomes for Patients with Feeding Tubes Undergoing Inpatient Rehabilitation: Follow-Up R. Jordan Stewart, MEd, CCC-SLP, BRS-S Susan Brady, MS, CCC-SLP, BRS-S Cari Manypenny, MS, CCC-SLP Richard
Dysphagia Outcomes for Patients with Feeding Tubes Undergoing Inpatient Rehabilitation: Follow-Up R. Jordan Stewart, MEd, CCC-SLP, BRS-S Susan Brady, MS, CCC-SLP, BRS-S Cari Manypenny, MS, CCC-SLP Richard
Where do we come from?
 Interdisciplinary Decision-Making with Patients Requiring Tracheostomy and Carrie Windhorst MS CCC-SLP Cheryl Wagoner MS CCC-SLP Ricque Harth MEd CCC-SLP Where do we come from? Welcome to Madonna Rehabilitation
Interdisciplinary Decision-Making with Patients Requiring Tracheostomy and Carrie Windhorst MS CCC-SLP Cheryl Wagoner MS CCC-SLP Ricque Harth MEd CCC-SLP Where do we come from? Welcome to Madonna Rehabilitation
Normal and Abnormal Oral and Pharyngeal Swallow. Complications.
 ESPEN Congress Gothenburg 2011 Assessment and treatment of dysphagia What is the evidence? Normal and Abnormal Oral and Pharyngeal Swallow. Complications. Pere Clavé Educational Session. Assessment and
ESPEN Congress Gothenburg 2011 Assessment and treatment of dysphagia What is the evidence? Normal and Abnormal Oral and Pharyngeal Swallow. Complications. Pere Clavé Educational Session. Assessment and
Why Can t I breathe? Asthma vs. Vocal Cord Dysfunction (VCD) Lindsey Frohn, M.S., CCC-SLP Madonna Rehabilitation Hospital (Lincoln, NE)
 Lindsey Frohn, M.S., CCC-SLP Madonna Rehabilitation Hospital (Lincoln, NE)") Why Can t I breathe? Asthma vs. Vocal Cord Dysfunction (VCD) Lindsey Frohn, M.S., CCC-SLP Madonna Rehabilitation Hospital (Lincoln, NE) Objectives Examine Vocal Cord Dysfunction Examine Exercise Induced
Why Can t I breathe? Asthma vs. Vocal Cord Dysfunction (VCD) Lindsey Frohn, M.S., CCC-SLP Madonna Rehabilitation Hospital (Lincoln, NE) Objectives Examine Vocal Cord Dysfunction Examine Exercise Induced
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation
 Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss