Anaesthesia In Thyroid Disorder. Dr. Umme Salma Ayesha Hoque MBBS, DA Medical Officer Department of Anaesthesiology and SICU BIRDEM General Hospital
|
|
|
- Nigel Snow
- 6 years ago
- Views:
Transcription
1 Anaesthesia In Thyroid Disorder Dr. Umme Salma Ayesha Hoque MBBS, DA Medical Officer Department of Anaesthesiology and SICU BIRDEM General Hospital
2 Anatomy Endocrine gland : Consist of two lobe Located : Anteriorly in neck extending from C5 to T1. Size : 5 cm long, 3 cm wide and 2 cm thick. Weight: gm in adult.
3 Blood supply : superior & inferior thyroid artery Nerve supply : superior, middle & inferior cervical ganglia of autonomic nervous system. parasympathetic from Vagus nerve
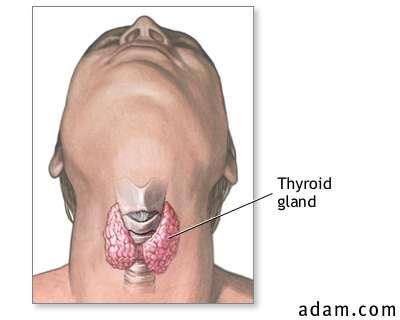
4 Anatomy
5 Physiology Hormones: 1.Thyroxine(T4) 2. Tri iodothyronine (T3) 3. Calcitonin

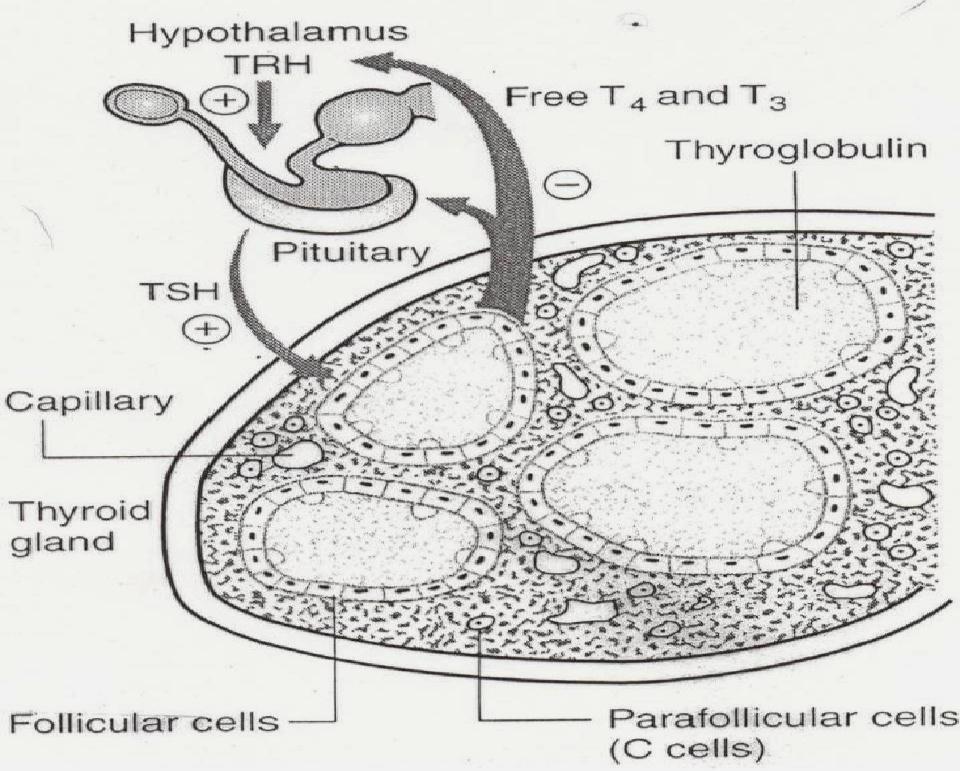
6 Thyroid hormones TRH (Hypothalamus) TSH (Ant. Pituitary) T4 thyroxine Thyroglobin (iodinated by peroxidase) back to cell
7 Thyroid gland essential for body to 1. Regulation of gene expression 2. Regulation of growth & development 3. Regulation of general metabolism 4. Regulation of tissue differentiation
8 Common disorder A. If hormone excess- 1. Graves disease 2. Multinodular goitre 3. Adenoma 4. Subacute thyroiditis B. Hormone deficiency- 1. Hashimoto s thyroiditis 2. Atrophic hypothyroidism
9 C. Hormone resistance- - Thyroid hormone resistance syndrome D. Non-functioning tumors- 1. Differentiated carcinoma 2. Medullary carcinoma 3. Lymphoma
10 Hypothyroidism Impaired secretion of thyroid hormones or under activity of the thyroid glands leading to hypometabolic state- - A high TSH level - A low Free T4 & T3 level in serum - A low total T4 & T3 level
11 Causes of Hypothyroidism 1. Primary hypothyroidism 2. Autoimmune (Hashimoto s thyroiditis) 3. Post thyroidectomy 4. Post radioactive iodine 5. Over dosage of antithyroid medication 6. Iodine deficiency 7. Secondary hypothyroidism (failure of the hypothalamic-pituitary axis)
12 Clinical features General Cardio-respiratory Tiredness, somnolence Weight gain Cold intolerance Hoarseness Goitre Bradycardia Hypertension Angina Cardiac Failure Pericardial & Pleural effusion
13 Neuromuscular - Delayed relaxation of tendon reflexes Muscle fatigue Lethargy Depression Deafness Others - Constipation Pretibial swelling Dry, flaky skin and hair
14 Diagnosis 1. Thyroid function test i. Free & total T4 low ii. Free & total T3 low iii. Serum TSH raised ( > 20 mu/l) iv. Radioactive iodine uptake test
15 2. Lactate Dehydrogenase(LDH) and Creatinine kinase(ck) - raised 3. Serum cholesterol and triglyceride raised 4. Serum sodium low 5. E.C.G Sinus bradycardia
16 Medical Treatment 1. Replacement therapy with thyroxine - Start with a dose of thyroxine 50 micgm / day for 3 weeks followed by - 100micgm / day for 3 weeks - Finally 150 micgm / day single daily dose. 2. Follow-up : Clinical checkup, serum TSH & T4 level
17 Anaesthetic consideration Euthyroid state is ideal Continue thyroid replacement medication on morning of surgery. Aspiration prophylaxis due to delayed gastric emptying times Sedative & narcotic administered more cautiously - more prone to drug induced respiratory depression
18 Preoperative Airway evaluation Patients tend to be obese Large tongue Short neck Goitre Swelling of upper airway
19 Intraoperative Patients are more sensitive to hypotensive effects of anesthetic agents because - 1. Decreased cardiac output 2. Blunted baroreceptor reflexes & 3. Decreased intravascular volume So, Invasive monitoring on a per patient basis
20 Ketamine or Etomidate may be induction agents of choice Succinylcholine and non-depolarizing muscle relaxants are generally safe for use. Used peripheral nerve stimulator for monitoring muscle relaxant.
21 Controlled ventilation is recommended as patients tend to hypoventilate Hypothermia occurs quickly Hematological (anaemia, platelet, coagulation dysfunction) disorder
22 Electrolyte imbalances Hypoglycemia is common Extubation/Emergence may be delayed secondary to hypothermia, respiratory depression, or slowed drug metabolism
23 Postoperative Try to maintain normothermia Cautiously administer Opioids, Consider regional techniques or Ketorolac for pain control
24 Emergency Myxedema Coma Rare form of decompensated Hypothyroidism Medical emergency with mortality rate of 15-20% Infection CNS depression - especially in elderly
25 Characterized by - Stupor or coma - Hypoventilation - Hypothermia - Bradycardia - Hypotension, - Severe dilutional hyponatremia (SIADH) - CHF
26 Treatment IV thyroxine is indicated (L-thyroxine loading dose ug, followed by 50ug/day for 24-48hrs) IV hydration with dextrose containing crystalloid Correction of electrolyte abnormalities Support cardiovascular and pulmonary systems as necessary
27 Hyperthyroidism Clinical syndrome which results from exposure of the body tissues to excess circulating levels of free thyroid hormones. More commons in female. - Suppressed serum TSH level( < 0.1 mu/l) - Raised serum T3 & T4 level
28 Causes of Hyperthyroidism 1. Graves disease 2. Toxic multinodular goitre 3. TSH secreting pituitary tumors 4. Toxic thyroid adenoma 5. Over dosage of thyroid replacement hormone
29 Clinical feature General Goitre Weight loss Heat intolerance Diarrhoea Exophthalmos Cardio-respiratory Palpitation Sinus tachycardia Atrial fibrillation Congestive heart failure Dysponea on exertion Exacerbation of asthma
30 Neuromuscular Muscle weakness Hyperactive reflexes Nervousness Fine tremor Periodic paralysis Others Gynaecomastia Lymphadenopathy Thirst Infertility
31 Diagnosis 1. Thyroid function test i. Free & total T4 raised ii. Free & total T3 raised iii. Serum TSH low iv. Radioactive iodine uptake test
32 2. Anti thyroid antibodies ( measurement of TSH receptor antibodies) 3. Fine needle aspiration cytology (FNAC) 4. Chest X-ray
33 Medical treatment 1. Anti-thyroid drug: Carbimazole - 15 mg 8 hourly 2-3 days, 10 mg 8 hourly 4 8 weeks 5 20 mg daily for months. 2. Subtotal thyroidectomy 3. Radioactive iodine 4. Beta-adrenoceptor antagonist- Propranolol 160 mg daily.
34 Anaesthetic consideration Ideally patient should be Euthyroid prior to any elective procedure. Antithyroid medications and beta-blockers should be continued through the morning of surgery.


35 Preoperative Careful evaluation of patients airway
36 Intraoperative Drugs that stimulate sympathetic nervous system should be avoided because of the possibility of increasing blood pressure and heart rate. Ex. Ketamine, Pancuronium, Atropine, Ephedrine.
37 Thiopental may be induction agent of choice as it possess antithyroid activity at high doses. Muscle relaxant doses may be increased. Adequate anaesthetic depth should be obtained prior to laryngoscopy or surgical stimulation to avoid tachycardia, hypertension,ventricular dysrhythmias
38 Anticipate exaggerated hypotensive response during induction as patient may be hypovolemic Eye protection
39 Muscle relaxants can be given safely. Patients with autoimmune thyrotoxicosis are associated with an increase risk of myopathies and myasthenia gravis. Reversal with glycopyrrolate instead of atropine
40 Postoperative Complication 1. Thyroid storm 2. Nerve injury 3. Heamatoma 4. Hypoparathyroidism
41 Thyroid storm Thyroid storm is most serious problem Characterized by: hyperpyrexia, tachycardia, altered consciousness, and hypertension
42 Precipitating factors: infection, trauma, surgery Onset is usually 6-24 hours after surgery, but can happen intraoperatively mimicking malignant hyperthermia
43 Treatment: ABC guideline Patient will be managed in Surgical ICU IV Hydration, cooling of patient IV Propranolol(0.5mg increments) /esmolol to control heart rate until less than 100. Propylthiouracil 250mg 6 hourly orally or by NG tube
44 Sodium Iodide 1 gram over 12 hours correction of any precipitating events (infection) Cortisol is recommended if there is any coexisting adrenal gland suppression Mortality rate is approximately 20%
45 Recurrent laryngeal nerve palsy: Unilateral hoarseness Bilateral - stridor
46 Hematoma formation : May cause airway compromise - required immediate opening of neck wound Hypoparathyroidism : May result from unintentional removal of parathyroid glands. Hypocalcemia will result within hours
47 Take home message Patient should be Euthyroid state incase of routine operation If emergency surgery consultation may be taken from Endocrinologist to get highest benefit from minimum period Our small effort can get maximum result so perioperaive period must be monitor cautiously


48 T H A N K Y O U
Non Thyroid Surgery. In patients with Thyroid disorders
 Non Thyroid Surgery In patients with Thyroid disorders The Thyroid disease problem. Is Thyroid disease a problem with anaesthetic? Why worry? The Physiology The evidence. A pragmatic approach From: The
Non Thyroid Surgery In patients with Thyroid disorders The Thyroid disease problem. Is Thyroid disease a problem with anaesthetic? Why worry? The Physiology The evidence. A pragmatic approach From: The
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY
 ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
4) Thyroid Gland Defects - Dr. Tara
 Thyroid Gland Defects - Dr. Tara") 4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
Thyroid gland defects. Dr. Tara Husain
 Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
03-Dec-17. Thyroid Disorders GOITRE. Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms
 Thyroid Disorders GOITRE Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms 1 Physiological Goiter load on thyroid supply of I - limited stress due to:
Thyroid Disorders GOITRE Grossly enlarged thyroid - in hypothyroidism in hyperthyroidism - production of anatomical symptoms 1 Physiological Goiter load on thyroid supply of I - limited stress due to:
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Effect of thyroid hormones of metabolism Thyroid Diseases
 Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Disorders of the Thyroid Gland
 Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
General surgery. Thyroid surgery. Physiological response to pneumoperitoneum. Bowel resection
 General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG
 THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG What is the difference between thyrotoxicosis and hyperthyroidism Thyrotoxicosis Thyrotoxicosis is defined as the state of thyroid hormone excess and is
THYROTOXICOSIS DR.J.BALA KUMAR 2 ND YR SURGERY PG What is the difference between thyrotoxicosis and hyperthyroidism Thyrotoxicosis Thyrotoxicosis is defined as the state of thyroid hormone excess and is
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
The Thyroid: No mystery. Just need all the pieces to the puzzle.
 The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
Pathophysiology of Thyroid Disorders. PHCL 415 Hadeel Alkofide April 2010
 Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
THE THYROID BOOK. Medical and Surgical Treatment of Thyroid Problems
 THE THYROID BOOK Medical and Surgical Treatment of Thyroid Problems Trouble with Your Thyroid Gland The thyroid is a small gland in your neck that plays a big role in how your body functions. It impacts
THE THYROID BOOK Medical and Surgical Treatment of Thyroid Problems Trouble with Your Thyroid Gland The thyroid is a small gland in your neck that plays a big role in how your body functions. It impacts
Lectures presented. 3 rd year
 Lectures presented 3 rd year-2016-2017 The metabolic response to trauma Basic concepts: Homeostasis is a mechanism by which the internal environment of the human being is driven constant. It involves a
Lectures presented 3 rd year-2016-2017 The metabolic response to trauma Basic concepts: Homeostasis is a mechanism by which the internal environment of the human being is driven constant. It involves a
CHAPTER-II Thyroid Diseases. by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university
 CHAPTER-II Thyroid Diseases by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university Aspects That Will Be Addressed Hyperthyroidism Hypothyroidism Thyroiditis Hyperthyroidism
CHAPTER-II Thyroid Diseases by: j. jayasutha lecturer department of Pharmacy practice Srm college of pharmacy srm university Aspects That Will Be Addressed Hyperthyroidism Hypothyroidism Thyroiditis Hyperthyroidism
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Thyroid and Antithyroid Drugs
 Thyroid and Antithyroid Drugs Dr. Yunita Sari Pane, MSi Department of Pharmacology HYPOTHALAMIC PITUITARY THYROID AXIS T3 and T4 are synthesized in the thyroid gland. Inorganic iodine is trapped with great
Thyroid and Antithyroid Drugs Dr. Yunita Sari Pane, MSi Department of Pharmacology HYPOTHALAMIC PITUITARY THYROID AXIS T3 and T4 are synthesized in the thyroid gland. Inorganic iodine is trapped with great
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
HYPOTHYROIDISM AND HYPERTHYROIDISM
 HYPOTHYROIDISM AND HYPERTHYROIDISM SHAHIDA PERVEEN, AMBREEN Post RN BSCN Semester II FACULTY SIR RAJA April 13, 016 Objectives: State the functions of thyroid hormone. Understand the pathologic mechanism
HYPOTHYROIDISM AND HYPERTHYROIDISM SHAHIDA PERVEEN, AMBREEN Post RN BSCN Semester II FACULTY SIR RAJA April 13, 016 Objectives: State the functions of thyroid hormone. Understand the pathologic mechanism
THE THYROID GLAND AND YOUR HEALTH
 THE THYROID GLAND AND YOUR HEALTH Your Thyroid is a gland located at the base of your neck, just below your Adam s apple. It is shaped like a butterfly each wing or lobe, of your thyroid lies on either
THE THYROID GLAND AND YOUR HEALTH Your Thyroid is a gland located at the base of your neck, just below your Adam s apple. It is shaped like a butterfly each wing or lobe, of your thyroid lies on either
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Thyroid Disorders. Hypothyroidism. Low Total T4 Antiseizure meds Glucocorticoids. Free T4. Howard J. Sachs, MD.
 Thyroid Disorders Free T4 Low Total T4 Antiseizure meds Glucocorticoids Hypothyroidism Howard J. Sachs, MD www.12daysinmarch.com Primary Hypothyroidism High TSH Low free T4 Primary = End organ failure
Thyroid Disorders Free T4 Low Total T4 Antiseizure meds Glucocorticoids Hypothyroidism Howard J. Sachs, MD www.12daysinmarch.com Primary Hypothyroidism High TSH Low free T4 Primary = End organ failure
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
Thyroid and parathyroid glands
 Thyroid and parathyroid glands Dr. Isabel Hwang Department of Physiology Faculty of Medicine University of Hong Kong May 2007 The thyroid gland straddles the esophagus, just below the larynx, in the neck.
Thyroid and parathyroid glands Dr. Isabel Hwang Department of Physiology Faculty of Medicine University of Hong Kong May 2007 The thyroid gland straddles the esophagus, just below the larynx, in the neck.
Southern Derbyshire Shared Care Pathology Guidelines. Hyperthyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
PBLD - Table #21. Claude Abdallah, MD, MSc Assistant Professor, Anesthesiology & Susan Verghese, MD Professor, Anesthesiology
 PBLD - Table #21 Persistent Tachycardia, Hypertension in a Thyrotoxic Teen Postoperatively - Is this a Hyperthyroid Crisis? - A Storm in a Tea Cup Brewing Double Trouble? Claude Abdallah, MD, MSc Assistant
PBLD - Table #21 Persistent Tachycardia, Hypertension in a Thyrotoxic Teen Postoperatively - Is this a Hyperthyroid Crisis? - A Storm in a Tea Cup Brewing Double Trouble? Claude Abdallah, MD, MSc Assistant
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia preope
 Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: ENDOCRINE 5-May-2013 DEVELOPED BY: Jonathan Serpell
Medically Compromised Patients (Part II)
") Medically Compromised Patients (Part II) Ra ed Salma BDS, MSc, JBOMFS, MFDRCSI Endocrine Disorders I. Diabetes Mellitus (DM) Definition (WHO): - Chronic disease due to absolute or relative lack of insulin
Medically Compromised Patients (Part II) Ra ed Salma BDS, MSc, JBOMFS, MFDRCSI Endocrine Disorders I. Diabetes Mellitus (DM) Definition (WHO): - Chronic disease due to absolute or relative lack of insulin
Grave s disease (1 0 )
") THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Thyroid Gland. Patient Information
 Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Thyroid Disorders. January 2019
 Thyroid Disorders January 2019 What is the Thyroid? The thyroid is a small butterfly-shaped gland inside the neck, located in front of the trachea (windpipe) and below the larynx (voicebox). It produces
Thyroid Disorders January 2019 What is the Thyroid? The thyroid is a small butterfly-shaped gland inside the neck, located in front of the trachea (windpipe) and below the larynx (voicebox). It produces
Chapter 43. Endocrine System. Negative Feedback. Hypothalamus and Pituitary Glands
 Chapter 43 Drugs for Pituitary, Thyroid, and Adrenal Disorders Endocrine System Consists of glands that secrete hormones Maintains homeostasis using hormones as chemical messengers Secreted in response
Chapter 43 Drugs for Pituitary, Thyroid, and Adrenal Disorders Endocrine System Consists of glands that secrete hormones Maintains homeostasis using hormones as chemical messengers Secreted in response
Thyroid Storm: Uncommon Presentation. Noora M. Butti, MBBcH*
 Bahrain Medical Bulletin, Vol. 36, No. 3, September 2014 Thyroid Storm: Uncommon Presentation Noora M. Butti, MBBcH* Thyroid storm could lead to mortality; it is rare and characterized by severe clinical
Bahrain Medical Bulletin, Vol. 36, No. 3, September 2014 Thyroid Storm: Uncommon Presentation Noora M. Butti, MBBcH* Thyroid storm could lead to mortality; it is rare and characterized by severe clinical
HORMONES OF THE POSTERIOR PITUITARY
 HORMONES OF THE POSTERIOR PITUITARY HORMONES OF THE POSTERIOR PITUITARY In contrast to the hormones of the anterior lobe of the pituitary, those of the posterior lobe, vasopressin and oxytocin, are not
HORMONES OF THE POSTERIOR PITUITARY HORMONES OF THE POSTERIOR PITUITARY In contrast to the hormones of the anterior lobe of the pituitary, those of the posterior lobe, vasopressin and oxytocin, are not
Hypothyroidism in Women
 Illustration istock Collection / thinkstockphotos.com T Hypothyroidism in Women Donna Dunn Thyroid disease is a major health issue in the United States. Approximately 20 million Americans have been diagnosed
Illustration istock Collection / thinkstockphotos.com T Hypothyroidism in Women Donna Dunn Thyroid disease is a major health issue in the United States. Approximately 20 million Americans have been diagnosed
GOITER and Shortness of Breath. Case A: GOITER. Learning Objectives. Common Thyroid Disorders for
 2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
Ch 8: Endocrine Physiology
 Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Endocrine System. Overview Hormones Endocrine Organs
 Endocrine System Overview Hormones Endocrine Organs Endocrine vs. Exocrine Gland Secretes hormones sweat & saliva Ductless gland has ducts Injects tissue duct is filled Chemistry of Hormones & Physiology
Endocrine System Overview Hormones Endocrine Organs Endocrine vs. Exocrine Gland Secretes hormones sweat & saliva Ductless gland has ducts Injects tissue duct is filled Chemistry of Hormones & Physiology
THYROID AWARENESS. By: Karen Carbone. January is thyroid awareness month. At least 30 million Americans
 THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
9/11/2012. Chapter 11. Learning Objectives. Learning Objectives. Endocrine Emergencies. Differentiate type 1 and type 2 diabetes
 Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
Chapter 11 Endocrine Emergencies Learning Objectives Differentiate type 1 and type 2 diabetes Explain roles of glucagon, glycogen, and glucose in hypoglycemia Learning Objectives Discuss following medications
25/10/56. Hypothyroidism Myxedema in adults Cretinism congenital deficiency of thyroid hormone Hashimoto thyroiditis. Simple goiter (nontoxic goiter)
") THERAPEUTIC USES OF THYROID HORMONE Supeecha Wittayalertpunya Wannarasmi Ketchart Nov 2013 Hyperthyroidism (Thyrotoxicosis) Grave s disease (diffuse toxic goiter) Toxic uninodular & Toxic multinodular
THERAPEUTIC USES OF THYROID HORMONE Supeecha Wittayalertpunya Wannarasmi Ketchart Nov 2013 Hyperthyroidism (Thyrotoxicosis) Grave s disease (diffuse toxic goiter) Toxic uninodular & Toxic multinodular
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY
 DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY DEVELOPMENT OF THYROID Concept of pharyngeal arch 3 rd week 4 th week Adults 7 th week HISTOGENESIS OF THYROID GLAND
DEVELOPMENT & STRUCTURE OF THYROID GLAND DR TATHEER ZAHRA ASSISTANT PROFESSOR ANATOMY DEVELOPMENT OF THYROID Concept of pharyngeal arch 3 rd week 4 th week Adults 7 th week HISTOGENESIS OF THYROID GLAND
Quality Control and Interpretation of Laboratory. Nursing and Midwifery. Dr. M. Navidhamidi
 Quality Control and Interpretation of Laboratory Tests of Thyroid Hormones for Nursing and Midwifery Dr. M. Navidhamidi Tehran University of Medical Sciences ١ Physiopathology of Thyroid Gland ٢ Thyroid
Quality Control and Interpretation of Laboratory Tests of Thyroid Hormones for Nursing and Midwifery Dr. M. Navidhamidi Tehran University of Medical Sciences ١ Physiopathology of Thyroid Gland ٢ Thyroid
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
Endocrine Crises. Fred Pieracci, MD, MPH TACS Fellow
 Endocrine Crises Fred Pieracci, MD, MPH TACS Fellow 4.14.14 Endocrine Crises Rare Highly lethal Elusive Easily treatable 1. Thyroid 1. Thyroid storm 2. Myxedema coma Outline 2. Parathyroid: 1. Severe hypercalcemia
Endocrine Crises Fred Pieracci, MD, MPH TACS Fellow 4.14.14 Endocrine Crises Rare Highly lethal Elusive Easily treatable 1. Thyroid 1. Thyroid storm 2. Myxedema coma Outline 2. Parathyroid: 1. Severe hypercalcemia
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan
 HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
Causes and management of hyperthyroidism in cats
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Causes and management of hyperthyroidism in cats Author : Emma Garnett Categories : RVNs Date : May 1, 2008 Emma Garnett VN,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Causes and management of hyperthyroidism in cats Author : Emma Garnett Categories : RVNs Date : May 1, 2008 Emma Garnett VN,
Hypothalamo-Pituitary-Thyroid Axis
 SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Endocrine Emergencies. Hyperthyroidism. What are some common ED complaints that should make us think: R/O Hyperthyroidism?
 Endocrine Emergencies Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville nternational Airport Nashville, TN Hyperthyroidism TSH Tell us what the Pituitary
Endocrine Emergencies Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville nternational Airport Nashville, TN Hyperthyroidism TSH Tell us what the Pituitary
Perioperative Management of the Patient with Endocrine Disease: A Focus on Diabetes & Thyroid Dysfunction
 Perioperative Management of the Patient with Endocrine Disease: A Focus on Diabetes & Thyroid Dysfunction Luigi Meneghini, MD, MBA Professor, Internal Medicine (Endocrinology), UT Southwestern Medical
Perioperative Management of the Patient with Endocrine Disease: A Focus on Diabetes & Thyroid Dysfunction Luigi Meneghini, MD, MBA Professor, Internal Medicine (Endocrinology), UT Southwestern Medical
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Virginia ACP Clinical Update Thyroid Clinical Pearls. University of Virginia. Richard J. Santen MD
 Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Endocrine Gland Symptoms. Chapter contents. A) Overview of endocrine glands. B) Thyroid symptoms. C) Hashimoto s thyroiditis. D) Grave s disease
 Overview of endocrine glands. B) Thyroid symptoms. C) Hashimoto s thyroiditis. D) Grave s disease") Endocrine Gland Symptoms Chapter contents A) Overview of endocrine glands B) Thyroid symptoms C) Hashimoto s thyroiditis D) Grave s disease A) Overview of endocrine glands In our modern world we use telephones,
Endocrine Gland Symptoms Chapter contents A) Overview of endocrine glands B) Thyroid symptoms C) Hashimoto s thyroiditis D) Grave s disease A) Overview of endocrine glands In our modern world we use telephones,
Hypothyroidism. Causes. Diagnosis. Christopher Theberge
 Hypothyroidism Pronunciations: (Hypothyroidism) Hypothyroidism (under active thyroid) is a condition where the thyroid gland fails to secrete enough of the thyroid hormones thyroxine (T4) and triiodothyronine
Hypothyroidism Pronunciations: (Hypothyroidism) Hypothyroidism (under active thyroid) is a condition where the thyroid gland fails to secrete enough of the thyroid hormones thyroxine (T4) and triiodothyronine
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Physiological processes controlled by hormones?
 : the study of hormones, their receptors, the intracellular signaling pathways they invoke, and the diseases and conditions associated with them. What are hormones? Major endocrine glands? Fig 7-2 Physiological
: the study of hormones, their receptors, the intracellular signaling pathways they invoke, and the diseases and conditions associated with them. What are hormones? Major endocrine glands? Fig 7-2 Physiological
Screening Babies at risk of Congenital Hyperthyroidism GL354
 1 Screening Babies at risk of Congenital Hyperthyroidism GL354 Approval and Authorisation Approved by Job Title Date Paediatric Clinical Governance Chair of paediatric Clinical Governance March 2016 Change
1 Screening Babies at risk of Congenital Hyperthyroidism GL354 Approval and Authorisation Approved by Job Title Date Paediatric Clinical Governance Chair of paediatric Clinical Governance March 2016 Change
Graves Disease in Pediatrics
 Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Approach to Thyroid Dysfunction in the Elderly
 Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Study of signs and symptoms of cardiovascular involvement in thyroid diseases.
 Original article: Study of signs and symptoms of cardiovascular involvement in thyroid diseases. 1Dr.P.K.Satpathy, 2 Dr.Anil Katdare, 3 Dr.Sridevi, 4 Dr.Ranjeet Patil 1MD Medicine Professor, Department
Original article: Study of signs and symptoms of cardiovascular involvement in thyroid diseases. 1Dr.P.K.Satpathy, 2 Dr.Anil Katdare, 3 Dr.Sridevi, 4 Dr.Ranjeet Patil 1MD Medicine Professor, Department
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid Gland 甲状腺. Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel:
, PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel:") Thyroid Gland 甲状腺 Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline Thyroid Hormones Types Biosynthesis Storage and Release
Thyroid Gland 甲状腺 Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline Thyroid Hormones Types Biosynthesis Storage and Release
Thyroid Disease Part 2
 Thyroid Disease Part 2 by H. David Bergman, Ph.D. Dean, College of Pharmacy, Southwestern Oklahoma State University Goals and Objectives Goals: To provide the pharmacist with information regarding the
Thyroid Disease Part 2 by H. David Bergman, Ph.D. Dean, College of Pharmacy, Southwestern Oklahoma State University Goals and Objectives Goals: To provide the pharmacist with information regarding the
Ovid: Oxford Textbook of Endocrinology & Diabetes
 Página 1 de 6 Copyright 2002 Oxford University Press Wass, John A.H., Shalet, Stephen M., Gale, Edwin, Amiel, Stephanie A. Oxford Textbook of Endocrinology & Diabetes, 1st Edition Surgical procedure Part
Página 1 de 6 Copyright 2002 Oxford University Press Wass, John A.H., Shalet, Stephen M., Gale, Edwin, Amiel, Stephanie A. Oxford Textbook of Endocrinology & Diabetes, 1st Edition Surgical procedure Part
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Slide notes: This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications,
 1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
1. Changed level of a certain hormone Stimulation of the oxygen consumption 3. Decoupling of oxidative phosphorylation 2.
 1. How can endocrine disorders be classified? 1. Hereditary, acquired 2. Active, passive 3. Uncompensated, overcompensated 4. Primary, secondary 5.1, 4 6.1, 2, 3, 4. ENDOCRINE SYSTEM 2. Which is the MAIN
1. How can endocrine disorders be classified? 1. Hereditary, acquired 2. Active, passive 3. Uncompensated, overcompensated 4. Primary, secondary 5.1, 4 6.1, 2, 3, 4. ENDOCRINE SYSTEM 2. Which is the MAIN
Pathophysiology of the th E d n ocr i ne S S t ys em B. Marinov, MD, PhD Endocrine system Central: Hypothalamus
 Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Pathophysiology of the Endocrine System B. Marinov, MD, PhD Pathophysiology Department Medical University of Plovdiv Endocrine system Central: Hypothalamus Pituitary Pineal Peripheral Thymus Thyroid Parathyroid
Purchase the complete book on Amazon.com
 1 Purchase the complete book on Amazon.com 2 Disclaimer Medicine and nursing are continuously changing practices. The author and publisher have reviewed all information in this book with resources believed
1 Purchase the complete book on Amazon.com 2 Disclaimer Medicine and nursing are continuously changing practices. The author and publisher have reviewed all information in this book with resources believed
THYROID ANAESTHESIA. Dr F. Raymond
 THYROID ANAESTHESIA Dr F. Raymond 2-5-07 Baroda district, India Goitre family Introduction Thyroid disease is common Endemic areas 15-30% Thyroid enlargement affects upto 10% of the British popul n. HISTORY
THYROID ANAESTHESIA Dr F. Raymond 2-5-07 Baroda district, India Goitre family Introduction Thyroid disease is common Endemic areas 15-30% Thyroid enlargement affects upto 10% of the British popul n. HISTORY
THYROID DISEASE IN PREGNANCY
 THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
HYPOTHYROIDISM IN CHILDREN. IAP UG Teaching slides
 HYPOTHYROIDISM IN CHILDREN 1 OBJECTIVES Introduction Congenital hypothyroidism Etiology, clinical features, diagnosis, approach, treatment and prognosis Acquired hypothyroidism Etiology, clinical features,
HYPOTHYROIDISM IN CHILDREN 1 OBJECTIVES Introduction Congenital hypothyroidism Etiology, clinical features, diagnosis, approach, treatment and prognosis Acquired hypothyroidism Etiology, clinical features,
Who is this leaflet for? What is hyperthyroidism? What is the thyroid gland? What causes hyperthyroidism? How is hyperthyroidism diagnosed?
 Hyperthyroidism Who is this leaflet for? This leaflet is for patients who have been diagnosed with hyperthyroidism. It aims to give you some background information about the condition, its causes and the
Hyperthyroidism Who is this leaflet for? This leaflet is for patients who have been diagnosed with hyperthyroidism. It aims to give you some background information about the condition, its causes and the
Thyroid. Introduction
 Thyroid Introduction to the thyroid: anatomy, histology, hierarchy, feed-back regulation, effect of T3- T4 on Na/K ATPase and uncoupling proteins 07 of T3-T4: thyroglobulin, iodide pump, iodination and
Thyroid Introduction to the thyroid: anatomy, histology, hierarchy, feed-back regulation, effect of T3- T4 on Na/K ATPase and uncoupling proteins 07 of T3-T4: thyroglobulin, iodide pump, iodination and
ANESTHESIA EXAM (four week rotation)
") SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
SPARROW HEALTH SYSTEM ANESTHESIA SERVICES ANESTHESIA EXAM (four week rotation) Circle the best answer 1. During spontaneous breathing, volatile anesthetics A. Increase tidal volume and decrease respiratory
LESSON ASSIGNMENT. Thyroid, Antithyroid, and Parathyroid Preparations. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 7 Thyroid, Antithyroid, and Parathyroid Preparations. LESSON ASSIGNMENT Paragraphs 7-1 through 7-12. LESSON OBJECTIVES After completing this lesson, you should be able to: 7-1.
LESSON ASSIGNMENT LESSON 7 Thyroid, Antithyroid, and Parathyroid Preparations. LESSON ASSIGNMENT Paragraphs 7-1 through 7-12. LESSON OBJECTIVES After completing this lesson, you should be able to: 7-1.
The Endocrine System. Lipid-Soluble Hormones. Bio217 Sp14 Unit 5. Bio217: Pathophysiology Class Notes Professor Linda Falkow
 Bio217: Pathophysiology Class Notes Professor Linda Falkow Mechanisms of Hormonal Regulation Unit V: Endocrine System Disorders Chapter 17 Chap. 17: Mechanisms of Hormonal Regulation Chap. 18: Alterations
Bio217: Pathophysiology Class Notes Professor Linda Falkow Mechanisms of Hormonal Regulation Unit V: Endocrine System Disorders Chapter 17 Chap. 17: Mechanisms of Hormonal Regulation Chap. 18: Alterations
Endocrine and Metabolic Disorders. Zalak Patel, MBBS Anesthesiology and Perioperative Medicine Medical College of Georgia Augusta University 2016
 Endocrine and Metabolic Disorders Zalak Patel, MBBS Anesthesiology and Perioperative Medicine Medical College of Georgia Augusta University 2016 Metabolic Syndrome Diagnosis requires at least three of
Endocrine and Metabolic Disorders Zalak Patel, MBBS Anesthesiology and Perioperative Medicine Medical College of Georgia Augusta University 2016 Metabolic Syndrome Diagnosis requires at least three of
Prepared By Margaret May RN MSN Fall 2016 Nursing 200
 Prepared By Margaret May RN MSN Fall 2016 Nursing 200 The endocrine system are glands organs and hormones that work with the nervous system to regulate body function and maintain homeostasis. Endocrine
Prepared By Margaret May RN MSN Fall 2016 Nursing 200 The endocrine system are glands organs and hormones that work with the nervous system to regulate body function and maintain homeostasis. Endocrine
Critical illness and endocrinology. ICU Fellowship Training Radboudumc
 Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight