Approach to Pulmonary Nodules
|
|
|
- Rodger Houston
- 6 years ago
- Views:
Transcription
1 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University Wexner Medical Center Pulmonary Nodules Treatment and follow up of pulmonary nodules are often a clinical challenge. The primary goal of pulmonary nodule management is to determine if the nodule is malignant or benign. 1
2 Approach to Pulmonary Nodules Successful management is about relationships Your relationship with the patient Your relationship with your colleagues Your relationship with the guidelines and current recommendations Approach to Pulmonary Nodules Definitions Growth Rate Etiology Lung Cancer Classification Characteristics Risk Factors Fleishner Society 2017 ACR Lung RADS Approach 2
3 Pulmonary Nodule (Definition) Well circumscribed round lesion measuring up to 3 cm in diameter surrounded by aerated lung. Pulmonary lesions > 3 cm are lung masses Pulmonary Nodule Courtesy of E. Jackson
4 Etiologies of Pulmonary Nodules Benign Infectious granuloma (80%) Endemic Fungi Atypical mycobacterium Tuberculosis Hamartoma AV malformation Intrapulmonary lymph node Malignant Adenocarcinoma (50%) Squamous cell carcinoma Small cell carcinoma Metastasis Lymphoma Carcinoid Lung Cancer Leading cause of cancer mortality in both men and women in the US 3 rd most common cause of cancer 225,000 new diagnosis per year 160,000 deaths per year 4
5 Risk Factors for Lung Cancer Cigarette smoking Age COPD Pulmonary fibrosis Exposures Genetic predisposition Classification Solid: More common Sub-solid: Pure ground glass: nodule with higher density than surrounding tissue but does not obscure the underlying lung Part solid: Nodule with at least part ground glass appearance 5



6 Classification Solid: Most common type of nodule Blocks out the lung tissue under it Classification Pure Ground Glass Part Solid

 Characterization of Nodules (Margins) Smooth:")
7 Classification (Sub-solid) Most sub-solid nodules are transient and represent infection or hemorrhage Persistent sub-solid nodules can represent primary lung cancer (adenocarcinoma) Characterization of Nodules (Margins) Smooth: Less likely malignant 7
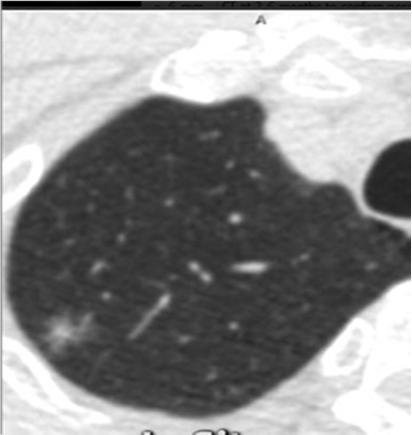
 Spiculated: sun")


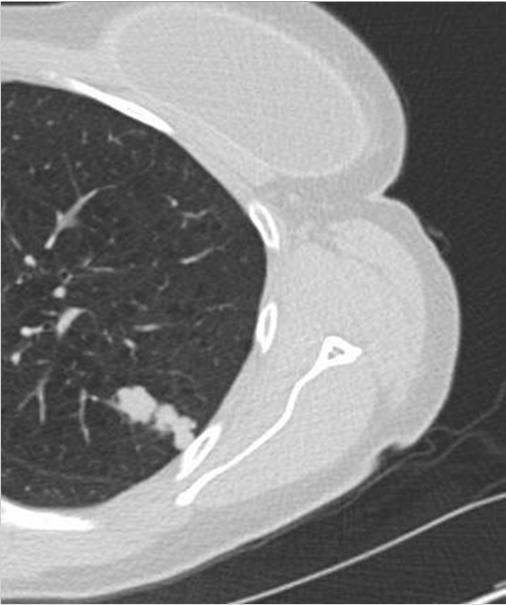

8 Characterization of Nodules (Margins) Spiculated: sun burst Not diagnostic but highly associated with malignancy Characterization of Nodules (Margins) Lobulated: intermediate probability of malignancy Courtesy of E. Jackson
 Based on the average of long and short axis diameters Measurements")

9 Characterization of Nodules (Size) Likelihood of malignancy correlates with nodule diameter. Nodule size is the dominant factor in management 75% of nodules > 2.0 cm are malignant 1% of nodules between 2-5 mm are malignant Characterization of Nodules (Size) Based on the average of long and short axis diameters Measurements should be made with electronic calipers Measurements should be rounded to the nearest whole millimeter Onno Mets and Robin Smithuis the Academical Medical Centre, Amsterdam and the Alrijne Hospital, Leiderdorp, the Netherlands 9
10 Characterization of Nodules (Doubling Time) Doubling time: Assessed based on the volume of the nodule. One doubling time: 26% increase in diameter Solid malignant nodules: Average doubling time of days & range days Characterization of Nodules (Doubling Time) Sub-solid malignant nodules: Longer doubling times. Average 1346 days (3.6 years) to double in volume. Nodules should be followed at least 5 years before being considered benign. 10


11 Characterization of Nodules (Location) Nodules in the upper lobes are more likely to be malignant Characterization (Benign) Calcification Diffuse Central Laminated Popcorn 11
12 Risk Assessment Low Risk: Young age Non smoker Smaller nodule size Regular margins Location other than the upper lobe Risk Assessment High risk: Older age Smoking History of extra thoracic malignancy Larger size Irregular margins Upper lobe location 12
13 Risk Assessment Models Most commonly used model (Mayo Clinic model) 3 clinical predicators Smoking history Age Extra thoracic cancer 3 Imaging predicators Nodule diameter Spiculated margin Upper lobe predominance Risk Assessment Signs and Symptoms Clubbing Hemoptysis Weight loss Night sweats New diffuse bone pain 13
14 Nodule Management Guidelines Determine which nodules are benign and need no further evaluation Determine which nodules are suspicious for malignancy Fleischner Society 2017: ACR Lung RADS: Fleischner Society 2017 Incidentally encountered lung nodules detected on Chest CT in adults who are 35 years or older. Should not be used for Patients with known primary cancers who are at risk for metastases Immune compromised patients Patients younger than 35 Lung cancer screening 14
15 Solid Nodules < 6mm Nodules < 6 mm (5mm) do not require routine follow up in most patients High risk patients: with suspicious nodules may warrant 12 month follow-up Upper lobe location Suspicious morphology Solid Nodules 6-8 mm Low risk: Follow-up CT in 6-12 months depending on morphology and patient preference A3 rd CT at months is optional 15
16 Solid Nodules 6-8 mm High risk: Follow-up CT in 6-12 months depending on morphology and patient preference The 3 rd CT should be obtained in months The cancer risk is 0.5% - 2.0% for nodules in this size range Solid Nodules > 8mm Low and High risk: 3 month follow up combined with PET/CT and or tissue sampling Average risk of cancer in a 8 mm solitary nodule is 3.0% 16
17 Tissue Sampling CT guided biopsy EBUS TBNA Surgical Resection Multiple Solid Nodules < 6 mm Low Risk patients: No routine follow up 17
18 Multiple Solid Nodules < 6 mm High Risk patients: Optional CT in 12 months based on morphology and patient preference Multiple Solid Nodules 6-8 mm Low Risk patients: Follow up CT at 3-6 months Consider a 3 rd CT at months 18
19 Multiple Solid Nodules 6-8 mm High Risk patients: Follow up CT in 3-6 months 3 rd CT at months Multiple Solid Nodules >8 mm Low and High Risk patients: Repeat CT in 3-6 months 3 rd CT at months 19

20 Solid Nodules Onno Mets and Robin Smithuis the Academical Medical Centre, Amsterdam and the Alrijne Hospital, Leiderdorp, the Netherlands Solitary Sub-solid Nodule < 6 mm Low Risk: No routine follow up is recommended High Risk: follow up CT at 2 and 4 years 20
21 Solitary Sub-solid Nodule > 6 mm Follow up CT scan at 6-12 months 3 rd CT in 2 years ( year 3) 4 th CT in 2 years ( year 5) Total follow up is 5 years Solitary Sub-solid Nodule > 6 mm Pure ground glass nodules that are 6 mm or larger may be followed safely for 5 years. Growth is seen in an average of 3-4 years or less 21
22 Solitary Part Solid Nodules < 6 mm No routine follow up is recommended Solitary Part Solid Nodules > 6 mm Solid component less than 6 mm in diameter Follow up CT is recommended at 3-6 months Follow up CT scans annually for a minimum of 5 years to assess the solid component 22
23 Solitary Part Solid Nodules > 6 mm Solid component greater than 6 mm in diameter Follow up CT in 3-6 months Solid component greater than 8 mm or suspicious characteristics PET/CT Biopsy Resection Solitary Part Solid Nodules > 6 mm The larger the solid component the greater the risk of Malignancy Invasiveness Metastasis 23
24 Multiple Sub-solid Nodules < 6 mm Follow up CT in 3-6 months Consider CT at 2 years Consider CT at 4 years Multiple Sub-solid Nodules > 6 mm Follow up CT at 3-6 months Subsequent management based on most suspicious nodule 24

25 Sub-Solid Nodules by Onno Mets and Robin Smithuis the Academical Medical Centre, Amsterdam and the Alrijne Hospital, Leiderdorp, the Netherlands Lung Cancer Screening In February of 2015 The Centers for Medicare & Medicaid Services (CMS) added lung cancer screening with low dose computed tomography (LDCT), as an additional preventive service benefit under the Medicare program. 25

26 Lung Cancer Screening Source: Final Update Summary: Lung Cancer: Screening. U.S. Preventive Services Task Force. July Lung Cancer Screening Population Age 55-80* Current and former smokers within the last 15 years At least 30 pack years of smoking No signs or symptoms of lung cancer Medically fit for surgery 26
27 Lung RADS Lung imaging Reporting And Data System Classification system to aid low dose CT screening examinations Standardizes follow up and management decisions Similar to Fleisher criteria but designed for high risk population Lung RADS Category 1 Negative screen ( < 1% chance of malignancy) No nodules Lung nodules with specific findings favoring benign nodules Complete calcification Central calcification Popcorn calcification Laminated calcification 27

28 Characterization (Benign) Calcification Diffuse Central Laminated Popcorn Lung RADS Category 1 Repeat LDCT in 12 months in accordance with lung cancer screening guidelines 28
29 Lung RADS Category 2 Benign appearance (< 1% chance of malignancy) Solid nodules < 6mm New nodules < 4mm Part-solid nodules < 6 mm on base line screening Ground glass nodules < 20 mm > 20 mm and unchanged Lung RADS Category 2 Repeat LDCT in 12 months in accordance with lung cancer screening guidelines 29
30 Lung RADS Category 3 Probably Benign 1-2% chance of malignancy Solid nodules > 6mm < 8 mm New nodule 4-6 mm Part-solid nodules > 6mm with a solid component of < 6 mm New < 6 mm total diameter Ground glass nodules > 20 mm on baseline CT Lung RADS Category 3 6 month follow up with low-dose CT 30
31 Lung RADS Category 4A Suspicious 5-15% chance of malignancy Solid nodules > 8 mm to < 15 mm baseline New nodule >6 mm but <8 mm Part-solid nodules > 6 mm total diameter solid component >6mm < 8 mm New or growing < 4mm solid component Lung RADS Category 4A 3 month follow up with low-dose CT PET/CT may be considered based on nodule characteristics and size 31
32 Lung RADS Category 4B Suspicious > 15% chance of malignancy Solid nodule > 15 mm New or growing nodule >8mm Part-solid nodules Solid component > 8 mm New or growing > 4mm solid component Lung RADS Category 4B Chest CT with or without contrast, as appropriate. PET/CT and/or tissue sampling should be considered. 32
33 Lung RADS Category 4X Suspicious > 15% chance of malignancy Category 3-4 nodules with additional features that increase suspicion of malignancy Spiculation Ground glass nodules that double in size in 1 year Enlarged regional lymph nodes Lung RADS Category 4X Chest CT with or without contrast, as appropriate. PET/CT and/or tissue sampling should be considered. 33
34 CT with or without Contrast CT with contrast: Indicated for patients with suspected hilar, mediastinal or pleural abnormalities. PET Solid Nodules: PET has sensitivity and specificity of approximately 90% for detecting malignant nodules with a diameter of 10 mm or larger Sub-Solid Nodules: Sensitivity of 90% specificity of 71% 34
35 PET False Negatives: Nodules less than 10 mm Well differentiated Cancers Carcinoid False Positives: Infectious/Inflammatory granulomas Approach 1. Compare old images if available 2. Risk stratify your patient and the nodule 3. Learn your patients preferences 4. Apply appropriate guidelines 35
36 References 1. Albert, Ross H., and John J. Russell. "Evaluation of the solitary pulmonary nodule." American family physician 80.8 (2009): Ost D, Fein AM, Feinsilver SH. Clinical practice. The solitary pulmonary nodule. N Engl J Med. 2003;348(25): Silvestri GA, Gonzalez AV, Jantz MA, et al. Methods for staging non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd Ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e211S-50S Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society Truong, M. T., Ko, J. P., Rossi, S. E., Rossi, I., Viswanathan, C., Bruzzi, J. F.,... & Erasmus, J. J. (2014). Update in the evaluation of the solitary pulmonary nodule. Radiographics, 34(6), Pulmonary Nodules Onno Mets and Robin Smithuis the Academical Medical Centre, Amsterdam and the Alrijne Hospital, Leiderdorp, the Netherlands 36
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES
 Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI
 Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES. https://tinyurl.com/hmpn2018
 PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
LUNG NODULES: MODERN MANAGEMENT STRATEGIES
 Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Lung Cancer Screening: To Screen or Not to Screen?
 Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
DENOMINATOR: All final reports for CT imaging studies with a finding of an incidental pulmonary nodule for patients aged 35 years and older
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Evidence based approach to incidentally detected subsolid pulmonary nodule. DM SEMINAR July 27, 2018 Harshith Rao
 Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art
 SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
SCBT-MR 2015 Incidentaloma on Chest CT
 SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE?
 PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
SCBT-MR 2015 LungRADS : Basics
 SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
Pulmonary Nodules. Michael Morris, MD
 Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Abstract Submission Form
 Abstract Submission Form All abstracts must be submitted to the AOCR by September 15 th. All information included must be the original work of the author(s) and be in typed form. Incomplete or handwritten
Abstract Submission Form All abstracts must be submitted to the AOCR by September 15 th. All information included must be the original work of the author(s) and be in typed form. Incomplete or handwritten
Published Pulmonary Nodule Guidelines A Synthesis
 Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
Pulmonary Nodules: When to worry, when to chill. Douglas Arenberg Associate Professor Pulmonary & Critical Care
 Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule
 Original Article Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule Xuan Zhang*, Hong-Hong Yan, Jun-Tao Lin, Ze-Hua Wu, Jia Liu, Xu-Wei Cao, Xue-Ning Yang From
Original Article Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule Xuan Zhang*, Hong-Hong Yan, Jun-Tao Lin, Ze-Hua Wu, Jia Liu, Xu-Wei Cao, Xue-Ning Yang From
Lung Cancer Diagnosis for Primary Care
 Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
A Chronology of Advancements in the Diagnosing of Lung Nodules
 November 17, 2017 A Chronology of Advancements in the Diagnosing of Lung Nodules Presenter: Daniel P. Harley, MD, MSB, FACS Surgical Director of the Angelos Center for Lung Diseases 1 Pulmonary Nodules
November 17, 2017 A Chronology of Advancements in the Diagnosing of Lung Nodules Presenter: Daniel P. Harley, MD, MSB, FACS Surgical Director of the Angelos Center for Lung Diseases 1 Pulmonary Nodules
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Current Approach to Screening for Lung Cancer. James R Jett M.D.
 Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
Lung Cancer Screening
 Lung Cancer Screening Steven Leh, MD, FCCP Diplomat of the American Association for Bronchology and Interventional Pulmonology Aurora Medical Group Pulmonary and Sleep Medicine February 10, 2018 Disclosures
Lung Cancer Screening Steven Leh, MD, FCCP Diplomat of the American Association for Bronchology and Interventional Pulmonology Aurora Medical Group Pulmonary and Sleep Medicine February 10, 2018 Disclosures
The small subsolid pulmonary nodules. What radiologists need to know.
 The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
Lung Cancer-a primer. Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo
 Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Lung Cancer Screening
 Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
GROUP 1: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases. Including: Excluding:
 GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
The Maine Lung Cancer Coalition. Working Together to Reduce Lung Cancer in Maine
 The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
Research Article The Advantage of PET and CT Integration in Examination of Lung Tumors
 Hindawi Publishing Corporation International Journal of Biomedical Imaging Volume 2007, Article ID 17131, 5 pages doi:10.1155/2007/17131 Research Article The Advantage of PET and CT Integration in Examination
Hindawi Publishing Corporation International Journal of Biomedical Imaging Volume 2007, Article ID 17131, 5 pages doi:10.1155/2007/17131 Research Article The Advantage of PET and CT Integration in Examination
Positron Emission Tomography in Lung Cancer
 May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
May-Lin Wilgus. A. Study Purpose and Rationale
 Utility of a Computer-Aided Diagnosis Program in the Evaluation of Solitary Pulmonary Nodules Detected on Computed Tomography Scans: A Prospective Observational Study May-Lin Wilgus A. Study Purpose and
Utility of a Computer-Aided Diagnosis Program in the Evaluation of Solitary Pulmonary Nodules Detected on Computed Tomography Scans: A Prospective Observational Study May-Lin Wilgus A. Study Purpose and
Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture
 Cronicon OPEN ACCESS EC PULMONOLOGY AND RESPIRATORY MEDICINE Case Report Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture Swan Lee 1 and Rolando Sanchez Sanchez
Cronicon OPEN ACCESS EC PULMONOLOGY AND RESPIRATORY MEDICINE Case Report Lung Cancer Screening in the Midwest of the US: When Histoplasmosis Complicates the Picture Swan Lee 1 and Rolando Sanchez Sanchez
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
CLINICAL GUIDELINES. Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P.
 CLINICAL GUIDELINES Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P. 3/14/2015 Introduction: The purpose of a lung-cancer screening program is to detect
CLINICAL GUIDELINES Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P. 3/14/2015 Introduction: The purpose of a lung-cancer screening program is to detect
Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center
 You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
SHARED DECISION MAKING AND LUNG CANCER SCREENING
 SHARED DECISION MAKING AND LUNG CANCER SCREENING DISCLOSURES Cathleen E. Morrow, MD None William C. Black, MD No financial disclosure Co-investigator for NLST Member of the ACR Lung-RADS Screening Registry
SHARED DECISION MAKING AND LUNG CANCER SCREENING DISCLOSURES Cathleen E. Morrow, MD None William C. Black, MD No financial disclosure Co-investigator for NLST Member of the ACR Lung-RADS Screening Registry
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Diagnostic challenge: Sclerosing Hemangioma of the Lung. Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and
 Diagnostic challenge: Sclerosing Hemangioma of the Lung. S. Arias M.D, R. Loganathan M.D, FCCP Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and Mental Health Center/Weill
Diagnostic challenge: Sclerosing Hemangioma of the Lung. S. Arias M.D, R. Loganathan M.D, FCCP Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and Mental Health Center/Weill
Lung Cancer Risk Associated With New Solid Nodules in the National Lung Screening Trial
 Cardiopulmonary Imaging Original Research Pinsky et al. Lung Cancer Risk Associated With New Nodules Cardiopulmonary Imaging Original Research Paul F. Pinsky 1 David S. Gierada 2 P. Hrudaya Nath 3 Reginald
Cardiopulmonary Imaging Original Research Pinsky et al. Lung Cancer Risk Associated With New Nodules Cardiopulmonary Imaging Original Research Paul F. Pinsky 1 David S. Gierada 2 P. Hrudaya Nath 3 Reginald
Screening Programs background and clinical implementation. Denise R. Aberle, MD Professor of Radiology and Engineering
 Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms
 Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society
 This copy is for personal use only. To order printed copies, contact reprints@rsna.org Heber MacMahon, MB, BCh David P. Naidich, MD Jin Mo Goo, MD, PhD Kyung Soo Lee, MD, PhD Ann N. C. Leung, MD John R.
This copy is for personal use only. To order printed copies, contact reprints@rsna.org Heber MacMahon, MB, BCh David P. Naidich, MD Jin Mo Goo, MD, PhD Kyung Soo Lee, MD, PhD Ann N. C. Leung, MD John R.
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
Right infrahilar nodule
 Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Lung Cancer Screening: Current Status
 Lung Cancer Screening: Current Status I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of investigational or off-label use of a product
Lung Cancer Screening: Current Status I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of investigational or off-label use of a product
A Summary from the 2013World Conference on Lung Cancer Sydney, Australia
 A Summary from the 2013World Conference on Lung Cancer Sydney, Australia In 2011, the U.S. National Lung Screening Trial (NLST) has demonstrated that low-dose computed tomography (LDCT) screening of high
A Summary from the 2013World Conference on Lung Cancer Sydney, Australia In 2011, the U.S. National Lung Screening Trial (NLST) has demonstrated that low-dose computed tomography (LDCT) screening of high
Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer
 November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
Lung Cancer Screening
 Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
The solitary pulmonary nodule: Assessing the success of predicting malignancy
 The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
Lung Cancer Update. Disclosures. None
 Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
Screening for Lung Cancer: New Guidelines, Old Problems
 Screening for Lung Cancer: New Guidelines, Old Problems Robert Schilz DO, PhD Associate Professor of Medicine Interim Chief of the Division of Pulmonary, Critical Care and Sleep Medicine University Hospitals
Screening for Lung Cancer: New Guidelines, Old Problems Robert Schilz DO, PhD Associate Professor of Medicine Interim Chief of the Division of Pulmonary, Critical Care and Sleep Medicine University Hospitals
THORACIK RICK. Lungs. Outline and objectives Richard A. Malthaner MD MSc FRCSC FACS
 THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
None
 2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer
 Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for
Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD. November 18, 2017
 Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Screening for Lung Cancer: Are We There Yet?
 Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2
 Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
FDG-PET/CT imaging for mediastinal staging in patients with potentially resectable non-small cell lung cancer.
 FDG-PET/CT imaging for mediastinal staging in patients with potentially resectable non-small cell lung cancer. Schmidt-Hansen, M; Baldwin, DR; Zamora, J 2018 American Medical Association. All Rights Reserved.
FDG-PET/CT imaging for mediastinal staging in patients with potentially resectable non-small cell lung cancer. Schmidt-Hansen, M; Baldwin, DR; Zamora, J 2018 American Medical Association. All Rights Reserved.
Objectives. Why? Why? Background 11/5/ % incurable disease at presentation Locally advanced disease Metastasis. 14% 5 year survival
 Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
Lung Cancer Screening: Who, What, Why? Myths Dispelled
 Lung Cancer Screening: Who, What, Why? Myths Dispelled Presented By: MaryAnn Tateosian, RT (R), M, MM, CIIP MGH Lung Screening Program Manager December 11, 2018 1 Lung Screening Objectives History of Smoking
Lung Cancer Screening: Who, What, Why? Myths Dispelled Presented By: MaryAnn Tateosian, RT (R), M, MM, CIIP MGH Lung Screening Program Manager December 11, 2018 1 Lung Screening Objectives History of Smoking
NCCN Guidelines as a Model of Extended Criteria for Lung Cancer Screening
 444 Original Research NCCN Guidelines as a Model of Extended Criteria for Lung Cancer Screening Brady J. McKee, MD; Shawn Regis, PhD; Andrea K. Borondy-Kitts, MS, MPH; Jeffrey A. Hashim, MD; Robert J.
444 Original Research NCCN Guidelines as a Model of Extended Criteria for Lung Cancer Screening Brady J. McKee, MD; Shawn Regis, PhD; Andrea K. Borondy-Kitts, MS, MPH; Jeffrey A. Hashim, MD; Robert J.
MANAGEMENT RECOMMENDATIONS
 1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL
 The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
Lung Cancer Screening
 Lung Cancer Screening Ravi Salgia, M.D., Ph.D. Professor and Chair Medical Oncology and Therapeutics Research City of Hope Nothing to disclose Disclosure Lung Cancer 2016 >200,000 cases projected >160,000
Lung Cancer Screening Ravi Salgia, M.D., Ph.D. Professor and Chair Medical Oncology and Therapeutics Research City of Hope Nothing to disclose Disclosure Lung Cancer 2016 >200,000 cases projected >160,000
Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!!
 The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
Imaging Decisions Start Here SM
 Owing to its high resolution and wide anatomic coverage, dynamic first-pass perfusion 320-detector-row CT outperforms PET/CT for distinguishing benign from malignant lung nodules, researchers from Japan
Owing to its high resolution and wide anatomic coverage, dynamic first-pass perfusion 320-detector-row CT outperforms PET/CT for distinguishing benign from malignant lung nodules, researchers from Japan
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer?
 CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer? Diagnosis and Management of Lung Cancer, 3rd
CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer? Diagnosis and Management of Lung Cancer, 3rd
Imaging Evaluation of the Solitary Pulmonary Nodule
 Imaging Evaluation of the Solitary Pulmonary Nodule Item Type Thesis Authors Van Tassel, Lora Publisher The University of Arizona. Rights Copyright is held by the author. Digital access to this material
Imaging Evaluation of the Solitary Pulmonary Nodule Item Type Thesis Authors Van Tassel, Lora Publisher The University of Arizona. Rights Copyright is held by the author. Digital access to this material
DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS
 DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS December 2018 Page 1 of 18 Document Title: Document Ref. Number: DOH Lung Cancer Screening Service Specifications PH/NCD/LCSC/SR/0.9 Version: 0.9 Approval
DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS December 2018 Page 1 of 18 Document Title: Document Ref. Number: DOH Lung Cancer Screening Service Specifications PH/NCD/LCSC/SR/0.9 Version: 0.9 Approval
Criteria USPSTF CMS. Frequency Annual screening Annual screening. No signs or symptoms of lung cancer
 Lung Cancer Screening Guidelines with low- dose computed tomography (LDCT): USPSTF and CMS February 6, 2015 Kentucky Cancer Consortium and Kentucky LEADS Component 3 Jennifer Redmond Knight, DrPH, jredknight@kycancerc.org
Lung Cancer Screening Guidelines with low- dose computed tomography (LDCT): USPSTF and CMS February 6, 2015 Kentucky Cancer Consortium and Kentucky LEADS Component 3 Jennifer Redmond Knight, DrPH, jredknight@kycancerc.org
18-FDG Uptake in Pulmonary Dirofilariasis
 Michael Stone 1*, Ishani Dalal 1, Chad Stone 2, Bhavin Dalal 3 1. Department of Radiology, Henry Ford Hospital, Detroit, USA 2. Department of Pathology, Henry Ford Hospital, Detroit, USA 3. Division of
Michael Stone 1*, Ishani Dalal 1, Chad Stone 2, Bhavin Dalal 3 1. Department of Radiology, Henry Ford Hospital, Detroit, USA 2. Department of Pathology, Henry Ford Hospital, Detroit, USA 3. Division of