Thyroid carcinoma. Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec.
|
|
|
- Liliana Singleton
- 6 years ago
- Views:
Transcription



1 Thyroid carcinoma Assoc. prof. V. Marković, MD, PhD Assoc. prof. A. Punda, MD, PhD D. Brdar, MD, nucl. med. spec.
2 Thyroid tumors PRIMARY TUMORS Tumors of the follicular epithelium : - Tumors of the follicular cell: benign follicular adenoma malignant: well differentiated: papillary carcinoma follicular carcinoma Hürtle cell carcinoma poorly differentiated: insular,tall-cell, diffuse sclerosing. undifferentiated : anaplastic carcinoma - Tumor of the parafollicular C cells: medullary carcinoma Nonepithelial tumors: sarcoma, malignant lymphoma... SECONDARY TUMORS
3 Tumor thyroid disease Benign tumors- adenomas (scintigraphic "hot" or "cold"), adenomatous goiter, cysts Malignant tumors- carcinoma papillary 80% follicular 10% (+ Hürthl cell ca. 2%) medullary 7% (5%) poorly differentiated 2% anaplastic <1% metastasis of other tumors in the thyroid
4 Malignant tumors of the thyroid the annual incidence 0,5-10/ people 1% of all malignant carcinomas 90% of all malignant endocrine tumors very good prognosis for differentiated tumors of the thyroid
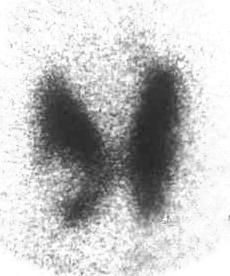
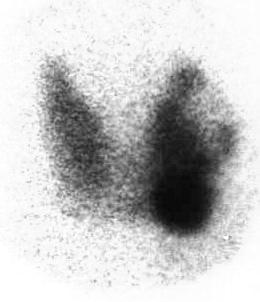
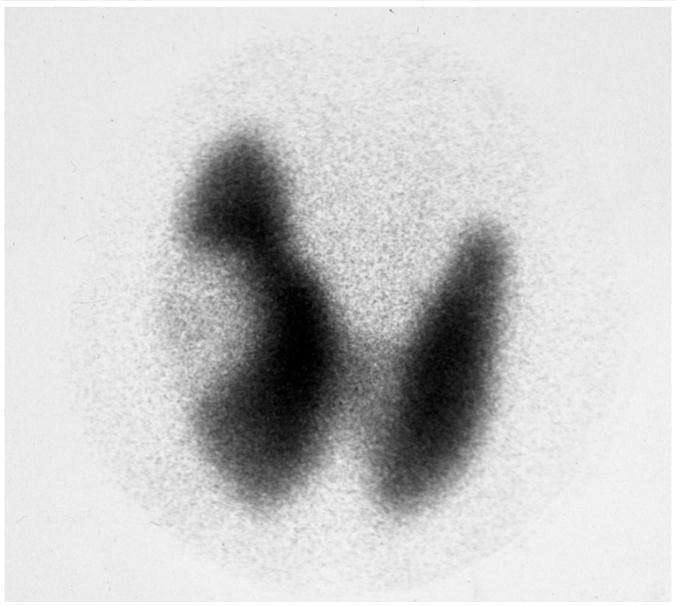
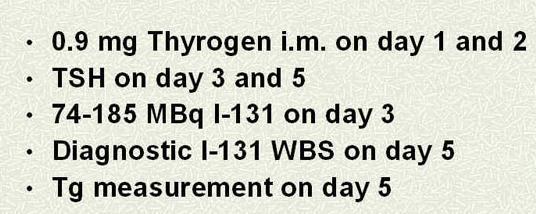
5 Scintigraphic cold nodules



 3.")
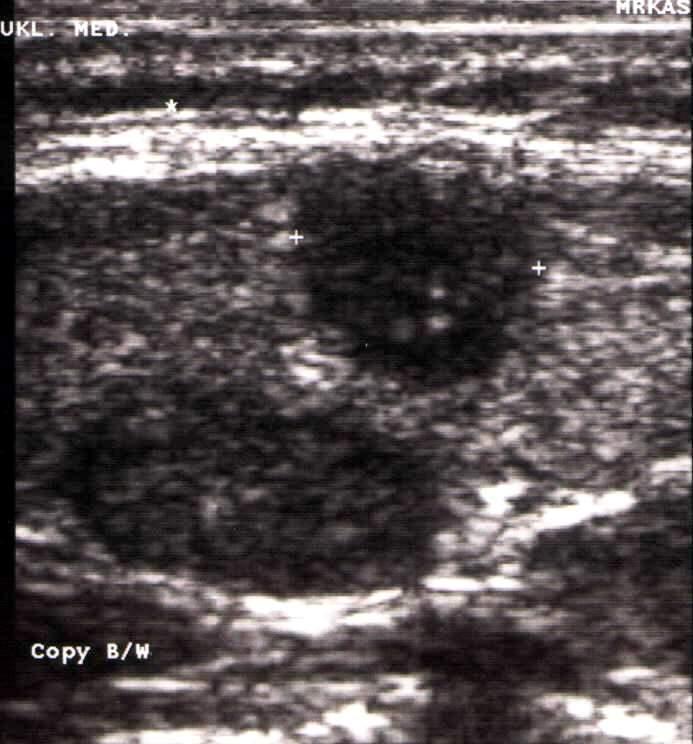
6 NODULAR CHANGES The number, size, echostructure, location 1. cysts and cystic changed nodes 2. solitary nodes- hypoechoic, isoechogenic, degeneratively changed (benign goiter) 3. multinodular goiter 4. nodes in lymphomatous goiter

7 NODULAR CHANGES: adenomas, carcinomas




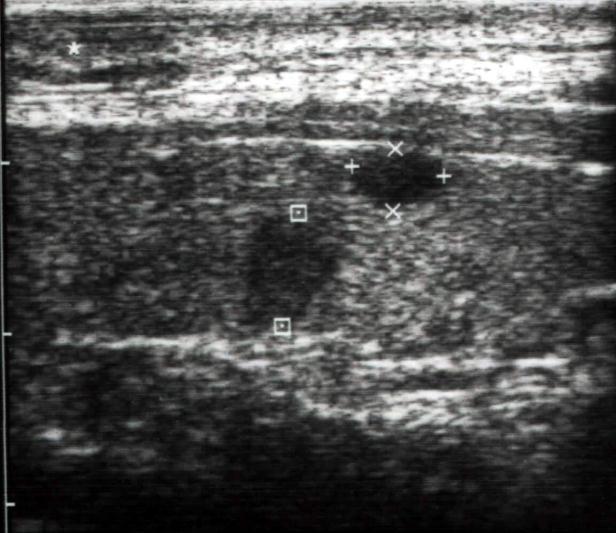
8 Echographical criteria of malignancy Hypoehogenicity Microcalcifications Without hypoehogenic edge, irregular borders Intranodular vascularisation Regional lymphadenopathy



9 Papillary carcinoma: The most common carcinoma of the thyroid (80%). Today, owing to ultrasonography, they are detected early in the course (about half of the detected papillary carcinoma is up to 1 cm).
10 Subtypes of thyroid papillary carcinoma: - follicular variant - tall cell- columnar cell - solid trabecular - diffuse sclerosing -Some of them have aggressive behavior
11 Papillary carcinoma at the time of diagnosis

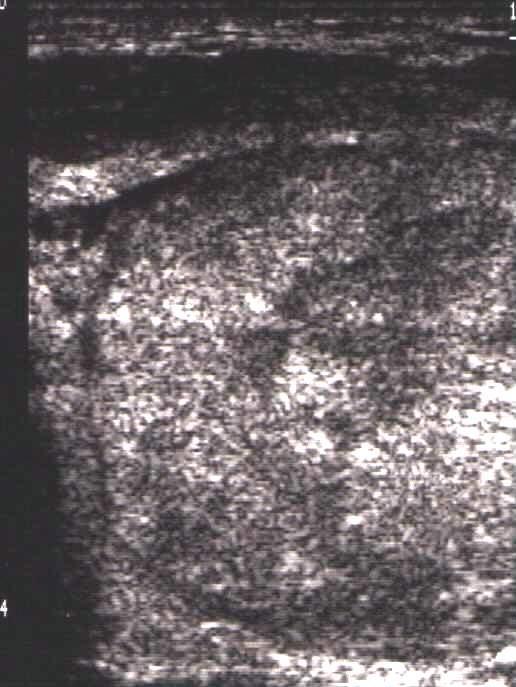
12 Follicular carcinoma It occurs much less frequently (10%), older age, more common in areas with endemic goiter. No reliable diagnostic possibility to distinguish them from adenoma, except possibly present metastases. It may have a similar echographic image as papillary carcinoma (hypoechogenicity, irregular margin, invasive growth, small calcifications-microcalcifications), but it is usually larger than papillary carcinoma. Sometimes it appears as isoechogenic or degeneratively changed node. Hürthl carcinoma (2%) is frequently isoechogenic on US, does not differ from the nodular goiter.
13 Subtypes of thyroid follicular carcinoma: - minimally-invasive - invasive - Hürthle cell - insular - Some of them have aggressive behavior
14 Follicular carcinoma The prognosis is good if no distant metastases. Distant metastases, in the lungs and in the bones. Metastases are usually functional and can be treated with radioiodine. Large doses of iodine, particularly in bone metastases can lead to damage to the bone marrow. Distant metastases - worse prognosis.

15 Follicular adenoma or carcinoma Impossibility of cytological diagnosis. Diagnostic criteria of minimally invasive carcinoma: complete invasion through the capsule and intravascular invasion.
16 Follicular carcinoma at the time of diagnosis
, the invasion of the trachea or esophagus (rarely seen), or")

17 Poor prognostic sign for differentiated thyroid carcinomas: interruption of the lobe capsule (capsule invasion), the invasion of the trachea or esophagus (rarely seen), or invasion of blood vessels, due to tumor or metastases to lymph nodes. Preoperative diagnosis of metastatic lymph nodes - required extensive surgery. Metastatic lymph node Infiltrative growth



18 Poorly differentiated and anaplastic thyroid carcinomas Insular carcinoma Trabecular Solid
19 Anaplastic carcinoma <1% one of the most malignant cancers in humans the elderly with pre-existing goiter rapidly growing tumor, hard consistency already at diagnosis inoperable because of extensive invasion of surrounding structures; regional and distant metastases prognosis is poor, median survival of 3-4 months, most dying in 6-12 months. dd: sarcoma, metastasis, parathyroid carcinoma, Riedel's struma- immunohistochemistry, clinical data
20 Mucoepidermoid thyroid cancer is rare; two variants: mucoepidermoid carcinoma and sclerosing mucoepidermoid carcinoma Rare tumors of the thyroid: SETTLE tumori: spindled and epithelial tumor with thymus like differentiation CASTLE tumori: tumor-carcinoma with thymus like differentiation
21 Microcarcinoma of the thyroid gland Well differentiated thyroid carcinomas <1 cm Detected by ultrasound and FNAC (owing to US a significant number of nowday detected thyroid cancers are smaller than 1 cm) Incidental microcarcinoma: histologically detected in thyroid tissue, which is operated for another reason Clinical (former Occult) microcarcinoma: discovered as a source (starting point) of metastases in the neck lymph nodes or distant metastases Latent microcarcinoma which is detected accidentally at autopsy
22 Medullary carcinoma Malignant tumor originated from parafollicular C cells Produces calcitonin and many other peptides 70-80% sporadic 20-30% hereditary: younger age, multicenter, bilateral


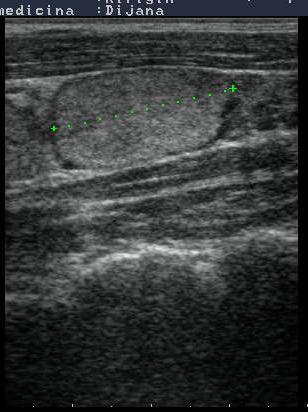
23 Medullary carcinoma 5-10% of patients with ca. thyroid; echographically hypoechogenic nodules, of varying sizes, often with calcification, irregular margin, with the infiltration of the neighbouring tissues. Medullary carcinoma with tiny calcifications Preoperatively, except with FNAC, medullary ca. can be diagnosed with calcitonin measurement in the serum and aspirate.
24 - Sporadic form % - Family form %, a examination of relatives (ultrasonography, determination of basal calcitonin in serum and after provocation, and genetic testing) for early diagnosis and preventive surgical therapy. Prognosis - good: if early detected and operated without local metastases and without elevated serum calcitonin. - worse: metastases present at the time of surgery, not enough radical surgery, calcitonin elevated after surgery (dissemination of disease- local recurrences and distant metastases).
25

26 MEN llb- tongue neurinomas
 aggressive")
27 Primary lymphoma of the thyroid Rare primary tumor Associated with Hashimoto's thyroiditis Women, middle-aged B immunophenotype indolent (MALT) aggressive (tall-cell)
28 PRIMARY THYROID LYMPHOMA - Rare neoplasm % of all lymphomas - 5% of all neoplasms of the thyroid - incidence - 3-5/1.000,000

29 Metastatic tumors Lung adenocarcinoma Breast cancer Melanoma Renal cancer
 Complications: hypoparathyroidism (5%) and paresis of recurent laryngeal nerve (1-2%) 2.")
30 Treatment of thyroid tumors Benign tumors: extirpation, lobectomy Malignant tumors: 1. total thyroidectomy (with neck dissection in the case of lymph node metastasis) Complications: hypoparathyroidism (5%) and paresis of recurent laryngeal nerve (1-2%) 2. radioiodine ablation and therapy 3. suppressive therapy 4. chemotherapy, external radiation- rarely (mostly anaplastic ca., incomplete because of extensive invasion of surrounding structures or widespread disease with iodine-negative metastases.)

31 v. int. jugular metastasis a.c.c.-partially occluded Metastases on the left side of the neck

32 Metastases on the left side of the neck Metastatic lymph node Papillary ca Metastasis Metastasis v. jug. int.


33 Metastatic lymph nodes

34 Neck metastases
35 Neck dissection Paratracheal neck dissection- region VI selective neck dissections modified radical neck dissection type I, II and III radical neck dissection extended radical neck dissection
36 Basic treatment of differentiated thyroid cancer: a total or near-total thyroidectomy and radioiodine ablation of thyroid remnant - ablation dose: 1,1-3,7 GBq J-131 ( mci) -low iodine diet : < 50 μg/day, uptake 68%, (Maxon 1983., Maruca 1984.) - diagnostic whole body scintigraphy with MBq I-131 (2-5 mci) before ablation?? (stunning)
37 Procedure after thyroid carcinoma surgery - 4 weeks after total thyroidectomy ablation dose of mci 131I for residual thyroid tissue - TSH above 30 µu/ml (possibly exogenous TSH-Thyrogen) - whole body scintigraphy - therapeutic dose of mci for the treatment of metastases - measurement of Tg
38 Total thyroidectomy 2%

39 Something always remains" (98%) thyroid remnant tissue after "total" thyroidectomy - scintigraphy with I- 131
 Why is the ablation of thyroid remnant with a I-131 necessary?")
40 (Mazzaferri and Massoll, 2002.) Why is the ablation of thyroid remnant with a I-131 necessary? Why radioiodine ablation? number of recurrences, metastases and mortality.
41 Why is the ablation of thyroid remnant with a I-131 necessary? Ablation of thyroid remnant destroys possible microfoci of thyroid ca., destroys possible micrometastases and promotes Tg to tumor marker (the only source of Tg is thyroid tissue or metastases). It creates conditions for the detection and treatment of possible metastases.
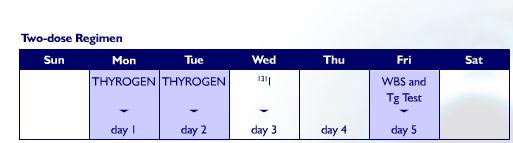
42 Exogenous stimulation with rhtsh (Thyrogen)
43 Exogenous stimulation with rhtsh (Thyrogen) 1. day injection of Thyrogen 2. day injection of Thyrogen 3. day - diagnostic (or ablative- therapeutic ) dose of I day - Tg and whole body scintigraphy

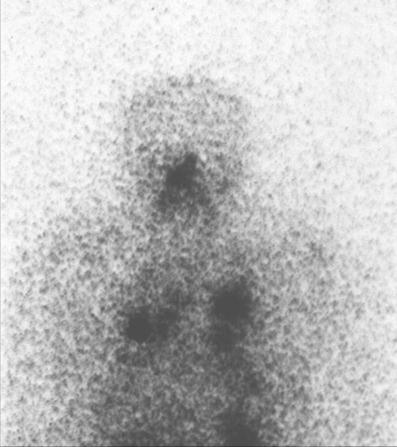
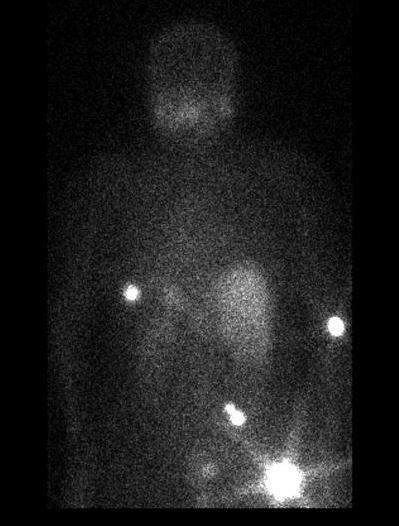
44 Treatment of functional metastases with I-131


45 Metastases in the lymph nodes - Therapy with I-131 Metastases in the lymph nodes of the neck - Scan after therapy with 100 mci J-131

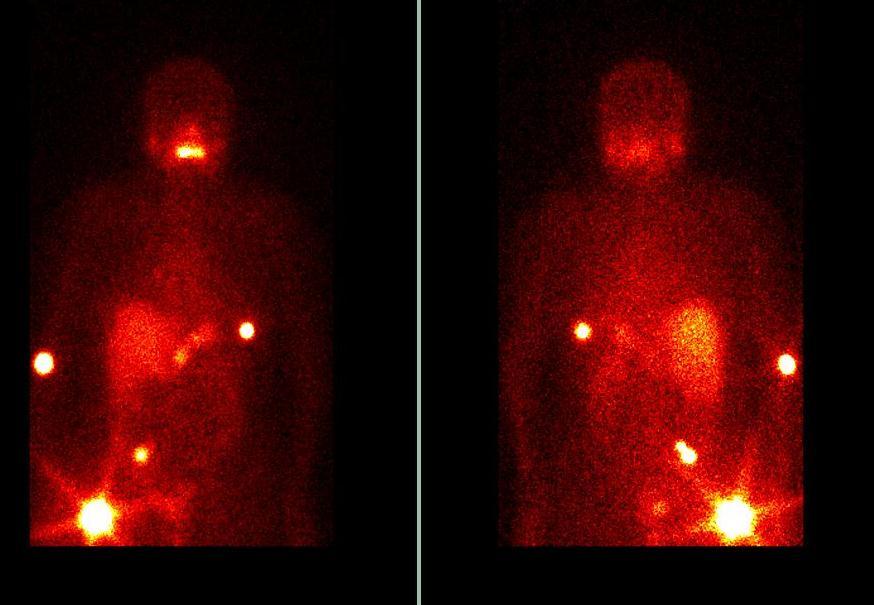
46 Functional metastases in the lung- Therapy with I-131 Metastases in the lung- scan after 200 mci I-131

47 Functional metastases in the bones - Therapy with I-131 Metastases in the bones - scan after 200 mci I-131
48 Bone metastases
49 inoperable tumor External radiation residual, deeply infiltrating tumor of the esophagus, trachea bone metastases: a) after J-131 b) prevention of pathological fractures brain metastases with massive mediastinal metastases for which there is low probability of total control with I-131 Recurrent metastases after the maximum therapeutic dose of I-131 (1Ci or 37 GBq) obstruction of the vena cava superior dose: Gy for bone metastases, 65 Gy for inoperable tm.
50 Chemotherapy * Progressive disease after surgery, therapy application of I-131 and external radiation * The most commonly used adriamycin * The therapeutic response is partial
51 Good prognosis: Prognosis and follow-up no accumulation of I-131, unmeasurable Tg, normal echographic findings in the neck Poor prognosis: Distant metastases (lung, bones). High thyroglobulin. Nonfunctional distant metastases (that don t accumulate radioiodine). A lot of residual tissue after surgery, residual local metastases. Residual tissue on the neck after total thyroidectomy

52 Why does it take a long follow-up of patients with thyroid carcinoma?
53 Follow-up of patients with differentiated thyroid carcinoma Methods in the follow-up Follow-up strategy
54 The most important methods in the follow-up: Thyroglobulin (Tg) Scintigraphy with I-131 Neck ultrasonography
55 Thyroglobulin - negative Tg (T4 or TSH) =<0,5 ng/ml - sensitivity * : - TgAb # Tg/T4= 78% Tg/TSH= 96% (hypothyroidism ) Tg/rhTSH= 92% - Tg> 2 ng/ml: recurrence? metastases? where are they? are they iodine positive or negative? Eustatia-Rutten CF et al. Diagnostic value of serum thyroglobulin mesurements... ClinEndocrrinol (Oxf). 2004; # Cooper DS et al. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. The American Thyroid Association Guidlines Taskoforce. Thyroid. 2006;16:1-33.
56 Thyroid antibodies
57 The new definition of successful ablation!? Negative Tg (<0,5 ng/ml) under TSH stimulation (thyroxine ex or rhtsh) * * Schlumberger M et al. Follow-up of low-risk patients with differentiated thyroid carcinoma: a European perspective. Eur J Endocrinol. 2004;150:
58 Whole body scintigraphy with I diagnostic: - withdrawal of thyroid hormon: hypothyroidism... - rhtsh MBq (5 mci) I if high dose therapy is intended with I-131, only 74 MBq or ommited (stunning) - post-ablation and post-therapy (10-26% additional meta. foci): 3,7-1 GBq I-131 ( mci)? - sensitivity * : - d-wbs = 49% - pt-wbs= 79% * Mazzaferri EL et al. A consensus report of the role... J Clin Endocrinol Metab. 2003;99:
59 The percentage of false negatives results (%) Negative d-wbs s 4 mci I-131 Negative Tg (<2 ng/ml) d-wbs/tsh d-wbs/rhtsh Tg/T4 Tg/rhTSH Tg/TSH The percentage of false negative results in patients with metastases diagnosed at pt- WBS (N=35) (Haugen BR et al. A comparison of recombinant human thyrotropin... J Clin Endocrinol Metab.1999;84: )
60 Neck ultrasonography % patients with differentiated thyroid carcinoma have metastases in cervical lymph nodes * - negative Tg---- US positive - fine needle aspiration (FNA) + Tg in aspirate (Tg/a) - sensitivity # : - FNAC= 85-91% - FNA + Tg/a = 100% * Cooper DS et al. Management guidelines... The American Thyroid Association Guidelines Taskoforce. Thyroid :1-33. # Pacini F et al. Detection of thyroglobuin in fine needle aspirates.. J Clin Endocrinol Metab. 1992;74:
61 New definition of successful ablation!? NegativeTg (<0,5 ng/ml) under TSH stimulation (thyroxine ex or rhtsh) * + Disease free patients Negative neck US!? * Schlumberger M, et al. Follow-up of low-risk patients with differentiated thyroid carcinoma: a European perspective. Eur J Endocrinol. 2004;150:
62 Follow-up strategy for patients with differentiated thyroid carcinoma Preoperative staging * 1. Low-risk patients (80%): T1, N0, M0 2. High-risk patients (20%) :T>1, or N1, M1 Postoperatively and after ablation 1. Low-risk: tm. removed completely, no invasion tm. in the surrounding structures, tm. no aggressive histology, no accumulation of I-131 outside the thyroid bed on the neck, no local nor distant metastases. 2. High-risk: incomplete tm. resection, tm. invasion in the surrounding structures, aggressive histology, accumulation of I-131 outside the thyroid bed on the neck, distant metastases. * Cooper DS et al. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. The American Thyroid Association Guidelines Taskoforce. Thyroid. 2006;16:1-33.

63 AMES criteria for the definition of low and high risk groups in papillary and follicular carcinoma
64
65 Patients without signs of disease - disease free patients * - Most of the patients after tot. thyroidectomy and radioiodine ablation, without clinical and scintigraphic evidence of disease, with negative Tg / T4 and Tg / TSH and negative neck US - Follow-up: Tg/T4 and neck US per year - d-wbs not required: sensitivity of Tg/T4 is higher than sensitivity of d-wbs (78% vs. 49%) * Cooper DS et al. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. The American Thyroid Association Guidelines Taskoforce. Thyroid. 2006;16:1-33.
66 Follow-up high-risk patients * The follow-up strategy for these patients is more aggressive, and in case of recurrence or metastatic disease, the following procedures are applied, depending on iodine positive or negative recurrences or metastases: -curative or palliative surgery - I-131 therapy - external radiation - experimental chemoterapeutic trial - watchful waiting in patients with stable, asymptomatic and slow progressive disease * Cooper DS et al. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. The American Thyroid Association Guidelines Taskoforce. Thyroid. 2006;16:1-33.
67 Metastases Iodine - positive metastases - 66% - The treatment of choice: I-131 every 6-12 months - dedifferentiation Iodine - negative, Tg positive meta. - 33% - diagnosis - Tl-201, Sestamibi, Tetrofosfin, bone sc., rtg., MR, CT, F18-FDG PET - treatment: a) single meta.: surgery., radiation, I-131? (6-9%) b) multiple: redifferentiation using retinoic acid? 26% uptake, 16% meta. * c) chemotherapy-partial, modest response (25%) * Simon D et al. Clinical impact of retinoids in redifferentiation therapy of advanced thyroid cancer: final results of o pilot study. Eur J Nucl Med Mol Imag.2002;29:
68
69 Why suppressive therapy?
70 Suppressive therapy - The aim of TSH suppression therapy (TSH<0.1 mu / L) with supraphysiological doses of T4 is to reduce the risk of recurrence or metastasis - Improves outcomes in high risk patients while there is no evidence for improving outcomes in low risk patients - suppressive therapy = subclinical, latent thyrotoxicosis Recommendation * : - low-risk patients without evidence of disease: mu / L - high-risk patients without evidence of disease: mu / L - patients with persistent disease: <0.1 mu / L * The American Thyroid Association Guidelines Taskforce, 2009.
71 Suppressive therapy - Thyroxine (Euthyrox, Letrox) µg daily - The goal of therapy : suppressed TSH and normal values of thyroid hormones - Treatment of hypoparathyroidism: Vitamin D (AT 10 drops or Rocaltrol)
72 The end!
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
What you need to know about Thyroid Cancer
 What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Thyroid Cancer. With 51 Figures and 30 Tables. Springer
 H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
THYROID CANCER IN CHILDREN
 THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update
 thyroid carcinoma-an update") Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Thyroid Cancer & rhtsh: When and How?
 Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Thyroid Ultrasonography: clinical and radiological correlations
 Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma.
 ORIGINAL ARTICLE Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma. Md. Sayedur Rahman Miah, Md. Reajul Islam, Tanjim Siddika Institute of Nuclear Medicine & Allied Sciences,
ORIGINAL ARTICLE Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma. Md. Sayedur Rahman Miah, Md. Reajul Islam, Tanjim Siddika Institute of Nuclear Medicine & Allied Sciences,
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium
 European Journal of Endocrinology (2006) 154 787 803 ISSN 0804-4643 CONSENSUS STATEMENT European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium
European Journal of Endocrinology (2006) 154 787 803 ISSN 0804-4643 CONSENSUS STATEMENT European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium
Thyroid Cancer: Imaging Techniques (Nuclear Medicine)
") Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Multi-Organ Distant Metastases in Follicular Thyroid Cancer- Rare Case Report
 Multi-Organ Distant Metastases in Follicular Thyroid Cancer- Rare Case Report Dr. Mohammed Raza 1, Dr. Sindhuri K 2, Dr. Dinesh Reddy Y 3 1 Professor, Department of Surgery, JSS University, Mysore, India
Multi-Organ Distant Metastases in Follicular Thyroid Cancer- Rare Case Report Dr. Mohammed Raza 1, Dr. Sindhuri K 2, Dr. Dinesh Reddy Y 3 1 Professor, Department of Surgery, JSS University, Mysore, India
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer
 THYROID Volume 16, Number 2, 2006 American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association Guidelines Taskforce*
THYROID Volume 16, Number 2, 2006 American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer The American Thyroid Association Guidelines Taskforce*
RESEARCH ARTICLE. Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer
 RESEARCH ARTICLE Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer Zekiye Hasbek 1 *, Bulent Turgut 1, Fatih Kilicli 2,
RESEARCH ARTICLE Importance of Postoperative Stimulated Thyroglobulin Level at the Time of 131 I Ablation Therapy for Differentiated Thyroid Cancer Zekiye Hasbek 1 *, Bulent Turgut 1, Fatih Kilicli 2,
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules
 Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
Long-term Follow-up for Patients with Papillary Thyroid Carcinoma Treated as Benign Nodules YASUHIRO ITO, TAKUYA HIGASHIYAMA, YUUKI TAKAMURA, AKIHIRO MIYA, KAORU KOBAYASHI, FUMIO MATSUZUKA, KANJI KUMA
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Thyroid and Parathyroid Cancers
 Thyroid and Parathyroid Cancers Overview Endocrine malignancies, although relatively uncommon, are often difficult to diagnose and treat effectively. This chapter will focus on thyroid and parathyroid
Thyroid and Parathyroid Cancers Overview Endocrine malignancies, although relatively uncommon, are often difficult to diagnose and treat effectively. This chapter will focus on thyroid and parathyroid
NODULAR GOITRE EVALUATIONIN THE REGION OF THE HEALTHCARE CENTER OF NOVI PAZAR
 48 MEDICINSKI GLASNIK / str. 48-57 Mersudin Mulić *, Bilsana Mulić NODULAR GOITRE EVALUATIONIN THE REGION OF THE HEALTHCARE CENTER OF NOVI PAZAR Summary: The term thyroid nodus refers to any irregular
48 MEDICINSKI GLASNIK / str. 48-57 Mersudin Mulić *, Bilsana Mulić NODULAR GOITRE EVALUATIONIN THE REGION OF THE HEALTHCARE CENTER OF NOVI PAZAR Summary: The term thyroid nodus refers to any irregular
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer
 Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Disseminated bone
Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Disseminated bone
A Review of Differentiated Thyroid Cancer
 A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Oncogenes/Growth Factors & Environment
 Oncogenes/Growth Factors & Environment 8 th Postgraduate Course in Endocrine Surgery Crete, Greece September, 2006 Orlo H. Clark M.D. Thyroid Cancer Thyroid cancer is the 8 th most common and most rapidly
Oncogenes/Growth Factors & Environment 8 th Postgraduate Course in Endocrine Surgery Crete, Greece September, 2006 Orlo H. Clark M.D. Thyroid Cancer Thyroid cancer is the 8 th most common and most rapidly
14 Clinical Review Volume 2 No. 1, 2004
 14 Clinical Review Volume 2 No. 1, 2004 CLINICAL REVIEW Well-Differentiated Thyroid Carcinoma: A Review of the Available Follow-Up Modalities Taryn Davids, MD Ally P.H. Prebtani, MD ABSTRACT Well-differentiated
14 Clinical Review Volume 2 No. 1, 2004 CLINICAL REVIEW Well-Differentiated Thyroid Carcinoma: A Review of the Available Follow-Up Modalities Taryn Davids, MD Ally P.H. Prebtani, MD ABSTRACT Well-differentiated
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Chapter 14: Thyroid Cancer
 The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
Imaging in Thyroid Cancer
 Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation
 Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
Case Report American Journal of Cancer Case Reports http://ivyunion.org/index.php/ajccr/ Page 1 of 6 Papillary Thyroid Microcarcinoma Presenting as Horner s Syndrome: A Novel Clinical Presentation Ammara
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Case 5: Thyroid cancer in 42 yr-old woman with Graves disease
 Case 5: Thyroid cancer in 42 yr-old woman with Graves disease Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Thyroid cancer in 42 yr-old woman with
Case 5: Thyroid cancer in 42 yr-old woman with Graves disease Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Thyroid cancer in 42 yr-old woman with
The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis
 The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis Poster No.: C-2229 Congress: ECR 2014 Type: Educational Exhibit Authors: T. González de la Huebra Labrador, A. Herrero
The Thyroid Nodule: From the Ultrasound Image to the Anatomopathological Diagnosis Poster No.: C-2229 Congress: ECR 2014 Type: Educational Exhibit Authors: T. González de la Huebra Labrador, A. Herrero
Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries
 REVIEW ARTICLE J Korean Thyroid Assoc Vol. 4, No. 2, November 2011 Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries Yasuhiro Ito, MD and Akira Miyauchi, MD
REVIEW ARTICLE J Korean Thyroid Assoc Vol. 4, No. 2, November 2011 Surgical Treatment for Papillary Thyroid Carcinoma in Japan: Differences from Other Countries Yasuhiro Ito, MD and Akira Miyauchi, MD
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do?
 Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
Key Topics in Thyroid Cancer Worldwide epidemic What Should the Endocrinologist and Surgeon do? Martin Schlumberger Gustave Presenter Roussy Name and Université Paris Saclay, Villejuif, France 1 Disclosure
B Berry, J. 25 see also suspensory ligament of Berry biopsy see fine-needle aspiration biopsy (FNAB); open wedge biopsy
; open wedge biopsy") 174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Citation Auris, nasus, larynx (2011), 38(3):
, 38(3):") TitleManagement of metastasis to the thy Author(s) Ishikawa, Masaaki; Hirano, Shigeru; Citation Auris, nasus, larynx (2011), 38(3): Issue Date 2011-06 URL http://hdl.handle.net/2433/139807 Right 2010 Elsevier
TitleManagement of metastasis to the thy Author(s) Ishikawa, Masaaki; Hirano, Shigeru; Citation Auris, nasus, larynx (2011), 38(3): Issue Date 2011-06 URL http://hdl.handle.net/2433/139807 Right 2010 Elsevier
Dr J K Jekel Dept. Surgery University of Pretoria
 Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
YCN Thyroid NSSG. *** VALID ON DATE OF PRINTING ONLY - all guidelines available at *** page 1 of 8 version number: 1.
 YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
International Czech and Slovak cooperation in the treatment of patients with differentiated thyroid cancer
 Nuclear Medicine Review 2006 Vol. 9, No. 1, pp. 84 88 Copyright 2006 Via Medica ISSN 1506 9680 International Czech and Slovak cooperation in the treatment of patients with differentiated thyroid cancer
Nuclear Medicine Review 2006 Vol. 9, No. 1, pp. 84 88 Copyright 2006 Via Medica ISSN 1506 9680 International Czech and Slovak cooperation in the treatment of patients with differentiated thyroid cancer
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta
 Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Adina Alazraki, MD, FAAP Assistant Professor Radiology and Pediatrics Emory University and Children s Healthcare of Atlanta Review recently published pediatric guidelines for management of thyroid nodules
Thyroid Nodule. N. Rojanapithayakorn P. Prasarttong-Osoth
 Thyroid Nodule N. Rojanapithayakorn P. Prasarttong-Osoth A Brief History of the Thyroid A Brief History of the Thyroid Fabricius Wharton Von Haller A Brief History of the Thyroid Kendall Enrico Fermi A
Thyroid Nodule N. Rojanapithayakorn P. Prasarttong-Osoth A Brief History of the Thyroid A Brief History of the Thyroid Fabricius Wharton Von Haller A Brief History of the Thyroid Kendall Enrico Fermi A
 To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered
To the Patient and Family This booklet has been written for people who have received a diagnosis of thyroid cancer or who are being tested for this illness. If you have questions that are not answered