The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
|
|
|
- Joella Floyd
- 6 years ago
- Views:
Transcription




1 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology
2 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Jatin P. Shah

3 Thousands Thyroid Cancer Incidence & Mortality 1974 to USA Overall Women Men Mortality Overall Incidence Incidence in Men Incidence in Women Mortality
4 Misconceptions about Thyroid Cancer All patients need subtotal or near total Thyroidectomy All patients need Post Operative Radio Active Iodine ablation Post operative TSH should be brought down to 0 Follow up requires annual whole body radio active scans




5 Pathology - Biology Cancer of the Thyroid Papillary Thyroid Follicular Cell Tall Cell, Insular, etc Poorly differentiated Anaplastic Follicular Prognosis Good Bad Ugly ~85% ~14% <1%




6 Prognosis in Thyroid Cancer A very small proportion ~ 10 % of Papillary carcinomas will undergo progression to more aggressive variants Prognosis worsens PTC Tall Cell Poorly Diff Anaplastic Size, ETE, DM, Mortalit

7 Well Differentiated Nearly All Curable Thyroid Cancer Poorly Differentiated Need Aggressive Rx Majority Curable Anaplastic Rarely Curable
8 Differentiated Thyroid Cancer Prognostic Factors Mayo Lahey Mayo Karolinska MSKCC AGES AMES MACIS DAMES GAMES Age Grade Age Metastases Metastases Age Completeness Of resection DNA Age Metastases Grade Age Metastases Extension Extension Invasion Extension Extension Size Size Size Size Size
9 Importance of Prognostic factors Allows Risk Group Stratification Permits selective surgical treatment Permits selective use of Radio active Iodine Permits appropriate follow up strategies Delivers cost effective evidence based treatment Allays anxiety on the part of the patient Delivers excellent outcomes
10 Differentiated Cancer of the Thyroid Survival - Age <45y n=845 >=45y n=915 P<0.001
11 Differentiated Cancer of the Thyroid Age Group (y) Disease Specific Survival by Age < % 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% 10y DSS
12 Differentiated Cancer of the Thyroid Survival Size T Stage (T1,T2 vs T3,T4) < 4cm n=1584 >=4 cm n=207 P<0.001
13 Differentiated Cancer of the Thyroid Survival Extra Thyroid Extension None n=1290 Microscopic n=317 Macroscopic n=203 P<0.001
14 Differentiated Cancer of the Thyroid Survival p N Stage pn0 n=1206 pn1 n=604 P< year outcomes shown

15 Differentiated Cancer of the Thyroid Age Distribution of N+ Patients
16 Differentiated Thyroid Cancer Survival N Status Age < 45 Age > 45
17 Disease Specific Survival Age 45 years cut off Age 55 years cut off Stag e 10y DSS I 100% II 97% III 97% IV 80% Stag e 10y DSS I 100% II 94% III 94% IV 72%
18 Differentiated Cancer of the Thyroid Survival M Stage M0 n=1757 M1 (Mx) n=53 P< year outcomes shown
19 Differentiated Cancer of the Thyroid Prognostic Factors Risk Groups (GAMES) Low Intermediate High Age <45 >45 <45 >45 Gender Size Extent Grade Dist. Mets. Female < 4 cms. Intraglandular Low Absent Male > 4 cms. Extraglandular High Present
20 Risk Group Stratification Based on Prognostic Factors Risk Group Stratification is the most important clinical parameter for selection of the extent of initial surgery, the need for adjuvant therapy, the degree of rigorous follow up, and for the assessment of over all prognosis, for local, regional, or distant failure and Survival.
21 Differentiated Cancer of the Thyroid Disease specific Survival Risk Groups (GAMES) Low n=576 Intermediate n=817 High n=417 P< year outcomes shown
22 Extent of Thyroidectomy for Cancer All thyroid operations done for proven or suspected Cancer should be Extra capsular Subtotal Thyroidectomy and Near Total Thyroidectomy transgress thyroid tissue, and therefore are not Cancer operations, and should not be done There are only two Oncologic operations: Lobectomy or Total Thyroidectomy
23 Extent of Thyroidectomy for Cancer Extra capsular operations leave no residual thyroid tissue behind, and thus avoid the need for RAI ablation Pay special attention to the upper pole, pyramidal lobe and the region of the cricothyroid membrane Following an extracapsular total thyroidectomy, TGb is not measurable at 6 weeks, and thus it allows bio chemical follow up
24 Lobectomy
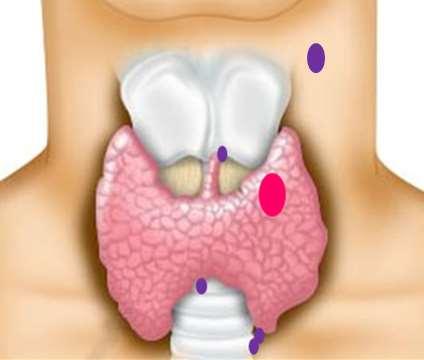
25 Total Thyroidectomy

26 Extra Thyroid Extension Most important factor impacting on the extent of Surgery

27 Differentiated Cancer of the Thyroid Extra Thyroid Extension Microscopic: Not Staged ( No impact) Minor: T3 Major: T4A Strap muscles Soft tissues Trachea Larynx Esophagus Recurrent laryngeal nerve
28 Extra Thyroid Extension T4a Disease specific Survival by completeness of Resection ( R Stage ) R0 96% R2 63% R1 60% R0 Gross Clearance R1 Micro. Residual R2 Gross Residual P<0.001 Time (Months)
29 Extrathyroid Extension Principles of Surgery All gross tumor should be removed Preserve functioning structures Preserve vital structures Balance between tumor control and best functional results Use adjuvant treatments - RAI, and/or RT
30 Cervical Lymph Nodes Micro metastases are common >50% Occult metastases have no impact on prognosis in low risk patients Elective node dissection is not recommended in low risk patients Therapeutic neck dissection is indicated for metastatic nodes identified clinically, on imaging studies or intra operatively Berry picking is not recommended Lymph node dissection should be compartmental and comprehensive


31 Patterns of Neck Metastases For differentiated cancer of the Thyroid gland AJCC/UICC 2009 Staging Nodal Staging for Thyroid Cancer N x regional lymph nodes cannot be assessed N 0 No regional lymph node metastases N 1 Regional lymph node metastases Central Compartment Node Dissection Level VI & VII N 1a Metastases to Level VI pretracheal, paratracheal, prelaryngeal, delphian N 1b Metastases to unilateral, bilateral or contralateral cervical or superior mediastinal lymph nodes Modified Neck Dissection Type III Lymph node dissection Level I not usually Level II - V Structures preserved Submandibular gland Internal jugular vein Sternocleidomastoid Spinal Accessory

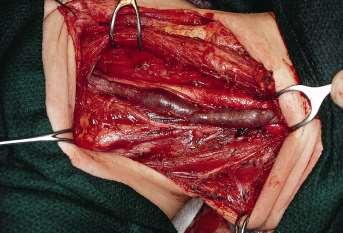
32 Central Compartment Node Dissection

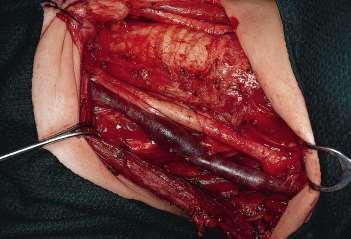

33 Lateral Neck Dissection
34 Distant Metastases Radio active Iodine External Radiotherapy ( selected cases) Surgery (Palliative) Chemotherapy?? Targeted Therapy (Investigational) Agents under study: Sorafinib, Lenvatinib, Selumetinib, Pazopanib, Vandetinib, Cabozantinib, other
35 Differentiated Cancer of the Thyroid Mortality 1810 patients ( ) Excluded M1 and unresectable N=1752 Median f/u = 100 months 165 deaths 17 died of disease 6 died from unknown causes with disease Disease specific mortality 1.3%
36 Differentiated Cancer of the Thyroid Trends in Mortality Author Year Death Rate Central Neck Disease *Tollefsen % >40%* Smith % 36% Shaha % 10% Kobayashi % <28% Ronga % 12% **Nixon % 0% ** * Locoregional recurrence was a common cause of death ** Locoregional recurrence is a rare cause of death
37 Thank You
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Disclosures Nodal Management in Differentiated Thyroid Carcinoma
 Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Disclosures Nodal Management in Differentiated Thyroid Carcinoma Nothing to disclose Jonathan George, MD, MPH Assistant Professor UCSF Head and Neck Oncologic & Endocrine Surgery Objectives Overview Describe
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Radiation Therapy for Thyroid Cancer. When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin?
 When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin? Jeanne Marie Quivey MD FACR October 200 Radiation Therapy for Thyroid Cancer Radioactive 3- I (RAI) External
When is Radiation Therapy indicated in Thyroid Cancer of Follicular or Parafollicular Cell Origin? Jeanne Marie Quivey MD FACR October 200 Radiation Therapy for Thyroid Cancer Radioactive 3- I (RAI) External
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Dr J K Jekel Dept. Surgery University of Pretoria
 Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
Dr J K Jekel Dept. Surgery University of Pretoria No Maybe ( T`s and C`s apply ) 1. Total thyroidectomy 2. Neck dissection only if nodes are involved 3. Ablative dose or doses of Radioactive Iodine 4.
40 TH EUROPEAN CONGRESS 0F CYTOLOGY LIVERPOOL, UK October 2-5, 2016
 Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Outcomes from the diagnostic approach of thyroid lesions using US-FNA and LBC in clinical practice Emmanouel Mastorakis MD PhD Cytopathologist Director in Cytopathology Laboratory Regional General Hospital
Reference No: Author(s) Approval date: October committee. September Operational Date: Review:
 Approval date: October committee. September Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer
 Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer Well Differentiated Thyroid Cancer Natural History and Prognosis EORTC AGES AMES MACIS QuickTime and a TIFF (LZW) decompressor
Treatment of Cervical Lymph Node Metastases Differentiated Thyroid Cancer Well Differentiated Thyroid Cancer Natural History and Prognosis EORTC AGES AMES MACIS QuickTime and a TIFF (LZW) decompressor
Management of Recurrent Thyroid Cancer
 Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Recurrent Thyroid Cancer Eric Genden, MD, MHA Isidore Professor and Chairman Department of Otolaryngology- Head and Neck Surgery Senior Associate Dean for Clinical Affairs The Icahn School
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer
 for Differentiated Thyroid Cancer") The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
The use of Radioactive Iodine (RAI) for Differentiated Thyroid Cancer Wendy Sacks, M.D. Cedars Sinai Medical Center California Chapter Annual Meeting, AACE Nov 5, 2016 Increasing Incidence of Thyroid Cancer
Surgery for Recurrent Thyroid cancer: Considerations and limitations
 Surgery for Recurrent Thyroid cancer: Considerations and limitations 2016 Thyroid Master Class February 13, 2016 Ara A. Chalian MD, FACS Surgical Patient Safety Officer University Of Pennsylvania Health
Surgery for Recurrent Thyroid cancer: Considerations and limitations 2016 Thyroid Master Class February 13, 2016 Ara A. Chalian MD, FACS Surgical Patient Safety Officer University Of Pennsylvania Health
External Beam Radiation Therapy for Thyroid Cancer
 External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Thyroid Carcinoma Variant 1: T1a N0 M0 papillary thyroid cancer: 40-year-old woman. 30 mci with thyrotropin 100 mci with thyrotropin 30 mci with thyroid hormone
American College of Radiology ACR Criteria Thyroid Carcinoma Variant 1: T1a N0 M0 papillary thyroid cancer: 40-year-old woman. 30 mci with thyrotropin 100 mci with thyrotropin 30 mci with thyroid hormone
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Thyroid. At-A-Glance. Papillary or follicular (differentiated) UNDER 45 YEARS Stage I Any T Any N M0 Stage II Any T Any N M1
 UNDER 45 YEARS Stage I Any T Any N M0 Stage II Any T Any N M1") 8 Thyroid At-A-Glance S U M M A R Y O F C H A N G E S Tumor staging (T1) has been subdivided into T1a ( 1 cm) and T1b ( 1 2 cm) limited to thyroid The descriptors to subdivide T categories have been changed
8 Thyroid At-A-Glance S U M M A R Y O F C H A N G E S Tumor staging (T1) has been subdivided into T1a ( 1 cm) and T1b ( 1 2 cm) limited to thyroid The descriptors to subdivide T categories have been changed
Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients
 ORIGINAL ARTICLE Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients Jianbiao Wang, MM, 1 Haili Sun, BM,
ORIGINAL ARTICLE Evaluation of thyroid isthmusectomy as a potential treatment for papillary thyroid carcinoma limited to the isthmus: A clinical study of 73 patients Jianbiao Wang, MM, 1 Haili Sun, BM,
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J.
 UvA-DARE (Digital Academic Repository) Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J. Link to publication Citation for published version (APA): Nixon, I. J. (2013).
UvA-DARE (Digital Academic Repository) Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J. Link to publication Citation for published version (APA): Nixon, I. J. (2013).
Locally advanced papillary thyroid cancer
 Locally advanced papillary thyroid cancer Educational Session 12 th October 2015 Presenters: Smith JA, Carr-Boyd E Supervisors: Palme CE, Elliott M, Navin N, Gupta R Content Case report Imaging Primary
Locally advanced papillary thyroid cancer Educational Session 12 th October 2015 Presenters: Smith JA, Carr-Boyd E Supervisors: Palme CE, Elliott M, Navin N, Gupta R Content Case report Imaging Primary
What s an NIFTP? Keeping Up To Date in Thyroid 2018
 What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
What s an NIFTP? Keeping Up To Date in Thyroid 2018 Kathleen Hands, MD, FACE, ECNU Director, Thyroid Center of South Texas Assistant Clinical Professor UTHSCSA DrHands@Thyroid-Center.com 210-844-6163 text
Review Article Management of thyroid carcinoma Alauddin M, Joarder AH
 Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Management of thyroid carcinoma Alauddin M, Joarder AH The ORION Medical Journal 2004 May;18:163-166 Overview The two most common forms of thyroid cancer, papillaryand follicular thyroid cancer, together
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
1. Protocol Summary Summary of Trial Design. IoN
 1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer
 DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
DEBATE WJOES Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Shifting Paradigms and Debates in the Management of Well-differentiated Thyroid Cancer Ashok R Shaha
New York, the nation s thyroid gland. Christopher Morley ( ), "Shore Leave"
, Shore Leave") New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
New York, the nation s thyroid gland Christopher Morley (1890-1957), "Shore Leave" Thyroid Literature Medline Thyroid disease 136,053 Thyroid tumors 33,554 New Paper on Thyroid Disease Every 3 Hours New
Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer
 Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer An emphasis on proper patient selection R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering
Minimalistic Initial Therapy Options For Low Risk Papillary Thyroid Cancer An emphasis on proper patient selection R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits?
 Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
Initial surgery for differentiated thyroid cancer: What is the appropriate extent and attendant risks and benefits? Julie Ann Sosa, MD MA FACS Professor of Surgery and Medicine Chief, Section of Endocrine
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma
 SAGE-Hindawi Access to Research Thyroid Research Volume 2011, Article ID 634170, 6 pages doi:10.4061/2011/634170 Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma Yasuhiro
SAGE-Hindawi Access to Research Thyroid Research Volume 2011, Article ID 634170, 6 pages doi:10.4061/2011/634170 Review Article Thyroidectomy and Lymph Node Dissection in Papillary Thyroid Carcinoma Yasuhiro
Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update
 thyroid carcinoma-an update") Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Bangladesh J Otorhinolaryngol 2010; 16(2): 126-130 Review Article Management of papillary and follicular (differentiated) thyroid carcinoma-an update Md. Abdul Mobin Choudhury 1, Md. Abdul Alim Shaikh
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Larynx & Thyroid 2014-2015 NAACCR Webinar Series May 7, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Changing trends in the management of well-differentiated thyroid carcinoma in Korea
 2016, 63 (6), 515-521 Original Changing trends in the management of well-differentiated thyroid carcinoma in Korea Yong Sang Lee, Hang-Seok Chang and Cheong Soo Park Thyroid Cancer Center, Department of
2016, 63 (6), 515-521 Original Changing trends in the management of well-differentiated thyroid carcinoma in Korea Yong Sang Lee, Hang-Seok Chang and Cheong Soo Park Thyroid Cancer Center, Department of
A Review of Differentiated Thyroid Cancer
 A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
A Review of Differentiated Thyroid Cancer April 21 st, 2016 FPON Webcast Jonn Wu BMSc MD FRCPC Radiation Oncologist, Vancouver Centre Chair, Provincial H&N Tumour Group, BCCA Clinical Associate Professor,
Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment
 ORIGINAL ARTICLE Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment Martínez MP, Lozano Bullrich MP, Rey M, Ridruejo MC, Bomarito MJ, Claus
ORIGINAL ARTICLE Differentiated Thyroid Cancer: Reclassification of the Risk of Recurrence Based on the Response to Initial Treatment Martínez MP, Lozano Bullrich MP, Rey M, Ridruejo MC, Bomarito MJ, Claus
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Thyroid Cancer Incidence & Image source: Thyroid ABC Health and Well Being Webinar Series 2 Anatomy
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Thyroid Cancer Incidence & Image source: Thyroid ABC Health and Well Being Webinar Series 2 Anatomy
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Title. CitationInternational Cancer Conference Journal, 4(1): Issue Date Doc URL. Rights. Type. File Information
: Issue Date Doc URL. Rights. Type. File Information") Title Lymph node metastasis in the suprasternal space from Homma, Akihiro; Hatakeyama, Hiromitsu; Mizumachi, Ta Author(s) Tomohiro; Fukuda, Satoshi CitationInternational Cancer Conference Journal, 4(1):
Title Lymph node metastasis in the suprasternal space from Homma, Akihiro; Hatakeyama, Hiromitsu; Mizumachi, Ta Author(s) Tomohiro; Fukuda, Satoshi CitationInternational Cancer Conference Journal, 4(1):
Overview. Extraglandular Thyroid Lymphatics. Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma. David W. Eisele, M.D., F.A.C.S.
 Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma David W. Eisele, M.D., F.A.C.S. Head and Neck Surgery and Oncology U.C.S.F. Comprehensive Cancer Center University of California,
Management of the Lateral Neck in Well-Differentiated Thyroid Carcinoma David W. Eisele, M.D., F.A.C.S. Head and Neck Surgery and Oncology U.C.S.F. Comprehensive Cancer Center University of California,
YCN Thyroid NSSG. *** VALID ON DATE OF PRINTING ONLY - all guidelines available at *** page 1 of 8 version number: 1.
 YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
YCN Thyroid NSSG Guidelines on Indications for Thyroid Surgery, Prophylactic Level 6 and Radioiodine plus follow-up of low risk differentiated thyroid cancer page 1 of 8 i Document Control Title Author(s)
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience
 Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Long Term Follow-Up for Differentiated Thyroid Cancer: The Mayo Experience Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Differentiated Thyroid Cancer Objectives Overview
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD
 Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
Thyroid Cancer: When to Treat? MEGAN R. HAYMART, MD ASSOCIATE PROFESSOR OF MEDICINE UNIVERSITY OF MICHIGAN MICHIGAN AACE 2018 ANNUAL MEETING Thyroid Cancer: When Not to Treat? FOCUS WILL BE ON LOW-RISK
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Frequency and pattern of central lymph node metastasis in papillary carcinoma of the thyroid isthmus
 ORIGINAL ARTICLE Frequency and pattern of central lymph node metastasis in papillary carcinoma of the thyroid isthmus Chang Myeon Song, MD, 1 Dong Won Lee, MD, 1 Yong Bae Ji, MD, PhD, 1 Jin Hyeok Jeong,
ORIGINAL ARTICLE Frequency and pattern of central lymph node metastasis in papillary carcinoma of the thyroid isthmus Chang Myeon Song, MD, 1 Dong Won Lee, MD, 1 Yong Bae Ji, MD, PhD, 1 Jin Hyeok Jeong,
Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler, MD, Roee Landsberg, MD, Dan M. Fliss, MD
 ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
ORIGINAL ARTICLE ELECTIVE PARATRACHEAL NECK DISSECTION FOR LATERAL METASTASES FROM PAPILLARY CARCINOMA OF THE THYROID: IS IT INDICATED? Avi Khafif, MD, Rami Ben-Yosef, MD, Avrum Abergel, MD, Ada Kesler,
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study
 ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
ORIGINAL ARTICLE A variation in recurrence patterns of papillary thyroid cancer with disease progression: A long-term follow-up study Joon-Hyop Lee, MD, Yoo Seung Chung, MD, PhD,* Young Don Lee, MD, PhD
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Advances in the management of thyroid cancer
 International Journal of Surgery (2005) 3, 213e220 www.int-journal-surgery.com REVIEW Advances in the management of thyroid cancer Ashok R. Shaha* Memorial Sloan-Kettering Cancer Center, 1275 York Avenue,
International Journal of Surgery (2005) 3, 213e220 www.int-journal-surgery.com REVIEW Advances in the management of thyroid cancer Ashok R. Shaha* Memorial Sloan-Kettering Cancer Center, 1275 York Avenue,
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
1. Introduction. 2. Patients and Methods
 Thyroid Research Volume 2012, Article ID 230283, 5 pages doi:10.1155/2012/230283 Clinical Study Biological Behavior of Papillary Carcinoma of the Thyroid Including Squamous Cell Carcinoma Components and
Thyroid Research Volume 2012, Article ID 230283, 5 pages doi:10.1155/2012/230283 Clinical Study Biological Behavior of Papillary Carcinoma of the Thyroid Including Squamous Cell Carcinoma Components and
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J.
 UvA-DARE (Digital Academic Repository) Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J. Link to publication Citation for published version (APA): Nixon, I. J. (2013).
UvA-DARE (Digital Academic Repository) Oncological outcomes for patients with well differentiated thyroid cancer Nixon, I.J. Link to publication Citation for published version (APA): Nixon, I. J. (2013).
PAPER. Predicting Outcome and Directing Therapy for Papillary Thyroid Carcinoma
 PAPER Predicting Outcome and Directing Therapy for Papillary Thyroid Carcinoma Sendia Kim, MD; John P. Wei, MD; Joshua M. Braveman, MD; David M. Brams, MD Hypothesis: The prognosis of papillary thyroid
PAPER Predicting Outcome and Directing Therapy for Papillary Thyroid Carcinoma Sendia Kim, MD; John P. Wei, MD; Joshua M. Braveman, MD; David M. Brams, MD Hypothesis: The prognosis of papillary thyroid
What? When? Why? (How?)
") Surgery of the Central Neck in Thyroid Cancer Dana M Hartl MD PhD Haïtham Mirghani MD Nothing to disclose Disclosure 2 Central Neck Dissection What? When? Why? (How?) What is it? Terminology for neck dissection
Surgery of the Central Neck in Thyroid Cancer Dana M Hartl MD PhD Haïtham Mirghani MD Nothing to disclose Disclosure 2 Central Neck Dissection What? When? Why? (How?) What is it? Terminology for neck dissection
Neck Dissection. Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)
, BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)") Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Chirurgie beim oligo-metastatischen NSCLC
 24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
24. Ärzte-Fortbildungskurs in Klinischer Onkologie 20.-22. Februar 2014, Kantonsspital St. Gallen Chirurgie beim oligo-metastatischen NSCLC Prof. Dr. med. Walter Weder Klinikdirektor Thoraxchirurgie, UniversitätsSpital
유두상갑상선암종에서경부림프절전이의양상및치료
 KISEP Head and Neck Korean J Otolaryngol 2005;48:506- 유두상갑상선암종에서경부림프절전이의양상및치료 태경 전성하 이현창 김경래 이형석 박용수 2 안유헌 2 김태화 2 Pattern and Treatment of Papillary Thyroid Carcinoma with Cervical Lymph Node Metastasis
KISEP Head and Neck Korean J Otolaryngol 2005;48:506- 유두상갑상선암종에서경부림프절전이의양상및치료 태경 전성하 이현창 김경래 이형석 박용수 2 안유헌 2 김태화 2 Pattern and Treatment of Papillary Thyroid Carcinoma with Cervical Lymph Node Metastasis
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Central and lateral neck dissection for differentiated thyroid cancer Diferansiye tiroid kanserlerinde santral ve lateral boyun diseksiyonu tekniği
 Central and lateral neck dissection for differentiated thyroid cancer Diferansiye tiroid kanserlerinde santral ve lateral boyun diseksiyonu tekniği Leigh Delbridge President, International Association
Central and lateral neck dissection for differentiated thyroid cancer Diferansiye tiroid kanserlerinde santral ve lateral boyun diseksiyonu tekniği Leigh Delbridge President, International Association
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Protocol for the Examination of Specimens From Patients With Carcinomas of the Thyroid Gland
 Protocol for the Examination of Specimens From Patients With Carcinomas of the Thyroid Gland Protocol applies to all carcinomas of the thyroid gland. Lymphomas, sarcomas and metastases are not included.
Protocol for the Examination of Specimens From Patients With Carcinomas of the Thyroid Gland Protocol applies to all carcinomas of the thyroid gland. Lymphomas, sarcomas and metastases are not included.
Salivary Glands tumors
 Salivary Glands tumors Sal.Gl. 1 Salivary Glands tumors Work-up procedure TNM staging Primary treatment Follow-up Treatment of recurrent and/or metastatic disease References Sal.Gl. 2 Standard clinical
Salivary Glands tumors Sal.Gl. 1 Salivary Glands tumors Work-up procedure TNM staging Primary treatment Follow-up Treatment of recurrent and/or metastatic disease References Sal.Gl. 2 Standard clinical
Central Lymph Node Dissection In Patients With Papillary Thyroid Cancer: A Population Level Analysis Of Cases
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2013 Central Lymph Node Dissection In Patients With Papillary
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2013 Central Lymph Node Dissection In Patients With Papillary
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid