Thyroid Cancer: Imaging Techniques (Nuclear Medicine)
|
|
|
- MargaretMargaret Walton
- 5 years ago
- Views:
Transcription
 Andrei Iagaru, MD MIPS Molecular")

1 Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
2 Introduction Ø There are approximately 56,460 new cases of thyroid carcinoma annually in the United States, and the overall incidence continues to rise Ø Women are more likely to have thyroid cancer at a ratio of 3:1 Ø Thyroid cancer can occur in any age group, although it is most common after age 30 and its aggressiveness increases significantly in older patients Jemal A, et al. Cancer statistics, CA Cancer J Clin : MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
3 Incidence of thyroid cancer Thyroid cancer cases and deaths >56,460 in Total cases, women, men: Total deaths, women, men Deaths MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
4 2012 Estimated US Cancer Cases* Men 766,860 Women 678,060 Prostate 29% Lung & bronchus 14% Colon & rectum 9% Urinary bladder 7% Melanoma of skin 5% Kidney 5% Non-Hodgkin 4% lymphoma Oral cavity 3% Leukemia 3% Pancreas 3% 29% Breast 14% Lung & bronchus 9% Colon & rectum 6% Uterine corpus 5% Thyroid 4% Non-Hodgkin lymphoma 4% Melanoma of skin 3% Ovary 3% Kidney 3% Pancreas Siegel R, Naishadham D, Jemal A. Cancer statistics, CA Cancer J Clin Jan-Feb;62(1): MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
5 2012 Estimated US Cancer Deaths* Lung & bronchus 29% Colon & rectum 9% Prostate 9% Pancreas 6% Leukemia 5% Liver & bile duct 4% Esophagus 4% Non-Hodgkin 4% lymphoma Urinary bladder 3% Kidney 3% Men 289,550 Women 270,100 26% Lung & bronchus 14% Breast 9% Colon & rectum 7% Pancreas 6% Ovary 4% Leukemia 3% Non-Hodgkin lymphoma 3% Uterine corpus 2% Liver and bile duct 2% Brain/ONS Siegel R, Naishadham D, Jemal A. Cancer statistics, CA Cancer J Clin Jan-Feb;62(1): MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
6 Thyroid cancer: ethnic influence " 3.3/100,000 " 6.2/100,000 " 6.5/100,000 " 9.1/100,000 " 10.5/100,000 " 14.6/100,000 " 32.5/100,000 " African American women " Hispanic women " White women " Hawaiian women " Vietnamese women " Filipino women " Filipino women yrs MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
7 Ø Papillary thyroid cancer (PTC) is the most common of all thyroid cancers, comprising approximately 70-75% of follicular cell derived cancers Ø Papillary cancer can occur in any age group, although its peak incidence in the fourth and fifth decades of life Ø It is more common in women than in men (2.5:1) MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
8 Ø The main risk factors for the development of PTC include a history of childhood head and neck radiation for benign conditions, or a family history of papillary cancer Ø PTC typically has an excellent prognosis, with overall 10- year survival rates estimated at 80-90% Ø Age over 45 years at time of diagnosis, tumor size over 4 cm, extrathyroidal extension of tumor, lymph node recurrence, and distant metastases negatively influence survival MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology

9 PTC: FNA shows large cells and nuclei, and their cytoplasm has a ground glass appearance. Nucleoli are prominent and the nuclei have clefts, gooves and holes due to intranuclear cytoplasmic inclusions UpToDate

10 PTC: Surgical specimen showing the classical histologic appearance of papillary cancer, with papillary structure and no folicles or colloid UpToDate
11 Ø Unlike papillary and follicular thyroid cancers, which arise from thyroid hormone producing cells, medullary thyroid cancer (MTC) is a neuroendocrine tumor of the parafollicular or C cells of the thyroid gland Ø A characteristic feature of this tumor is the production of calcitonin Ø The C cells originate from the embryonic neural crest; as a result, medullary carcinomas often have the clinical and histologic features of other neuroendocrine tumors such as carcinoid and islet-cell tumors MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
12 Ø MTC constitutes about 5-10% of all thyroid malignancies Ø Most medullary thyroid carcinomas are sporadic. However, some are familial as part of the multiple endocrine neoplasia type 2 (MEN2) syndrome Ø Overall 10-year survival rates are 90% when all the disease is confined to the thyroid gland, 70% with spread to cervical lymph nodes, and 20% when spread to distant sites is present MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology

13 MTC: FNA with immunostaining for calcitonin reveals nuclei of the tumor cells placed eccentrically, larger and more pleomorphic than those of normal follicular cells. Immunocytologic staining for calcitonin is positive. The background contains many RBC s that nonspecifically take up the stain UpToDate

14 MTC: Surgical specimen showing typical histologic appearance of medullary carcinoma UpToDate

15 Imaging PTC
16 Colloid Tg Thyroperoxidase I - Tg Pendrin I-Tg L Capillary Tg Synthesis I - I - I - I - I - NIS Na + I - T4, T3 MIT, DIT T4, T3 Lysosomal Digestion
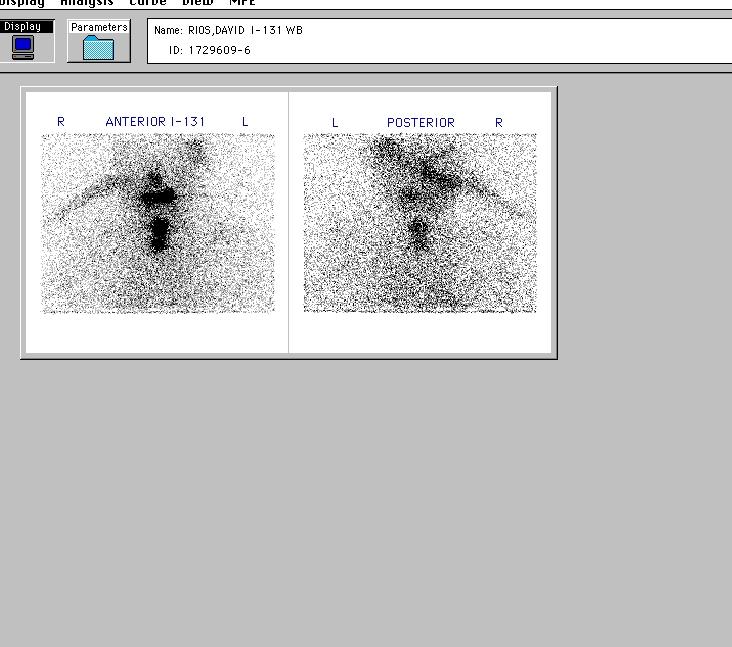
17 Diagnostic whole body 123 I scan Ø Proof of elevated TSH ü How high should it be? ü Withdrawal of thyroid hormone ü rhtsh Ø Measurement of Tg when TSH is stimulated Ø Low iodine diet Ø Which radionuclide of iodine? MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
18 How high should TSH be? Ø 25 mu/l Ø 30 mu/l Ø 50 mu/l Ø In one of our published reports the mean TSH value was 121 mu/l ATA Management Guidelines: TSH > 30 mu/l Rating B MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
19 Withdrawal of thyroid hormone vs. rhtsh ü 4-6 week delay before testing and treatment ü Physical symptoms and signs of hypothyroidism ü Psychological symptoms of hypothyroidism ü 2 week delay for testing and treatment ü No signs and symptoms of hypothyroidism MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
20 Thyroglobulin Ø Tg values depend on amount of thyroid tissue present Ø Tg levels increase with increase in TSH Ø About 25% of patients with papillary cancer have antibodies to Tg ü Antibodies alter validity of measurement ü Antibodies probably benefit prognosis ATA recommendation: Tg measured every 6-12 months using IRMA (same laboratory with antibody assay) Rating A MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology

21 Day 13 of low iodine diet Christmas card from patient, presented with permission ATA recommendation: Lowiodine diet for 1-2 weeks Rating B Courtesy of Dr McDougall
22
23 123 I/ 131 I: false positive scans Carlisle, Lu and McDougall Nucl Med Comm 2003;24: Shapiro et al in Thyroid Cancer edited by Wartofsky and Van Nostrand Humana Press 2006, Chap 16 Unusual sites of Iodine uptake Tissues that have NIS receptor Secretion and excretion of iodine Other pathologies Breast Thymus Salivary glands Courtesy of Dr McDougall
24 123 I/ 131 I: false positive scans Unusual sites of Iodine uptake Tissues with NIS receptor Secretion and excretion of iodine Other pathologies Saliva Milk Gastric fluid Bile/stool Sweat Courtesy of Dr McDougall
25
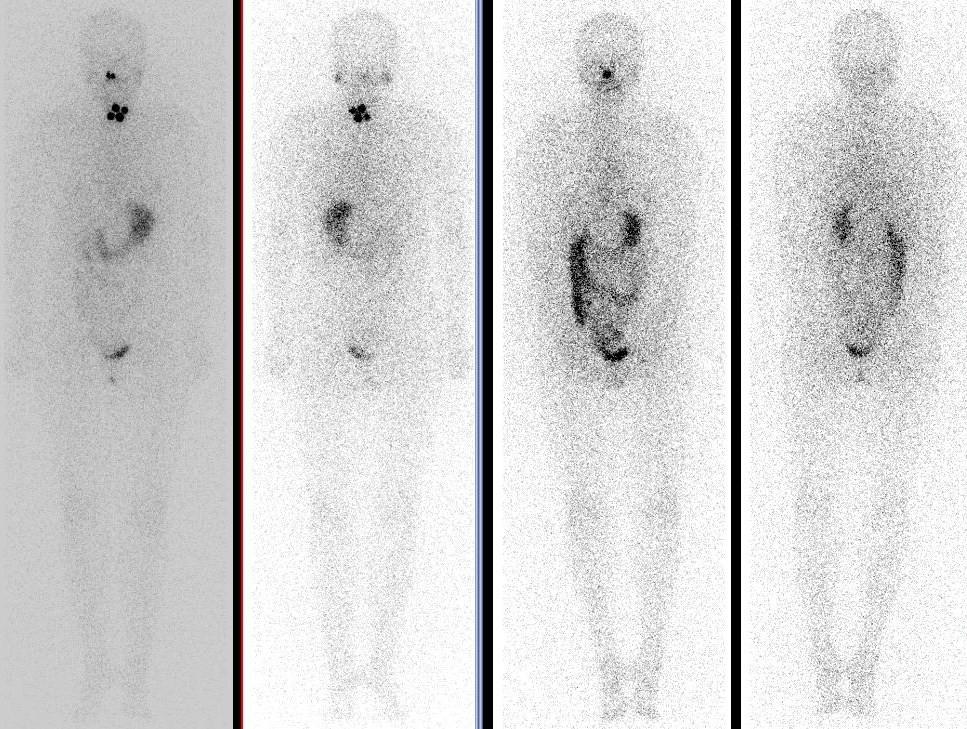
26 Pre-therapy Post-therapy
27
28
29
30



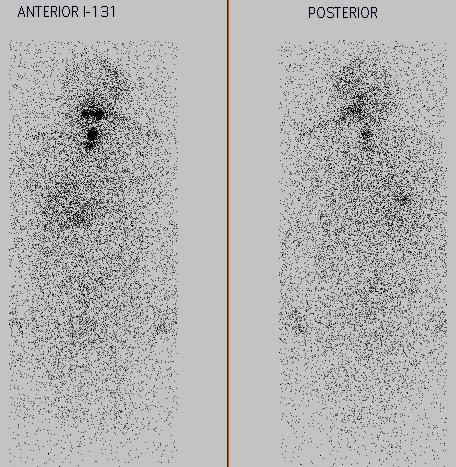
31 131 I trapping in thymus is uncommon, but not rare! Davidson and McDougall Nucl Med Comm 2000;27:
32 123 I/ 131 I: false negative scans
33
34


35 124 I PET/CT in DTC
36
37 Ø 52 women, 17 men; years old (average: 46) Ø 124 I PET/CT and a whole body scan were done, before and after 131 I ablation, respectively Ø 124 I PET/CT and 131 I WBS matched in 58/67 patients (86.6%) Ø 124 I PET/CT detected more disease than 131 I WBS in 5/67 patients (7.5%), mainly lymph node involvement Ø 131 I WBS detected more disease than 124 I PET/CT in 4/67 patients (4.9%), including lymph nodes and disseminated 131 I-avid lung metastases MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
38 Ø 39 women, 31 men; years old (average: 50) Ø 124 I PET/CT and a whole body scan were done, before and after 131 I ablation, respectively Ø Quantitative data consisted of absolute lung 124 I activity concentrations and lung-to-background (L/B) 124 I uptake ratios Ø Only 1/7 patients with disseminated lung metastases on the 131 I WBS had visible disseminated lung uptake on the 124 I PET/CT Ø L/B ratios overlapped between the subjects with/without 124 I uptake in disseminated lung metastases to an extent that an unequivocal diagnosis based solely on this criterion was impossible in some patients MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
39 Ø Some differentiated thyroid cancers lose the ability to trap iodine Ø How would you determine extent of disease in this situation? MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology


40 Normal thyroid: little or no uptake of 18 F FDG MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology


41 Diffusely increased uptake in the thyroid MIPS Diffuse uptake most likely chronic lymphocytic thyroiditis 18 F FDG PET in 1,102 healthy subjects Diffuse uptake in the thyroid in 36 patients 33 women 27 positive thyroid antibodies Ultrasound consistent with chronic thyroiditis or with Graves disease if the patient is thyrotoxic Molecular Imaging Program at Stanford Yasuda et al. Radiology 1998;207:775-8 Stanford University School of Medicine Department of Radiology

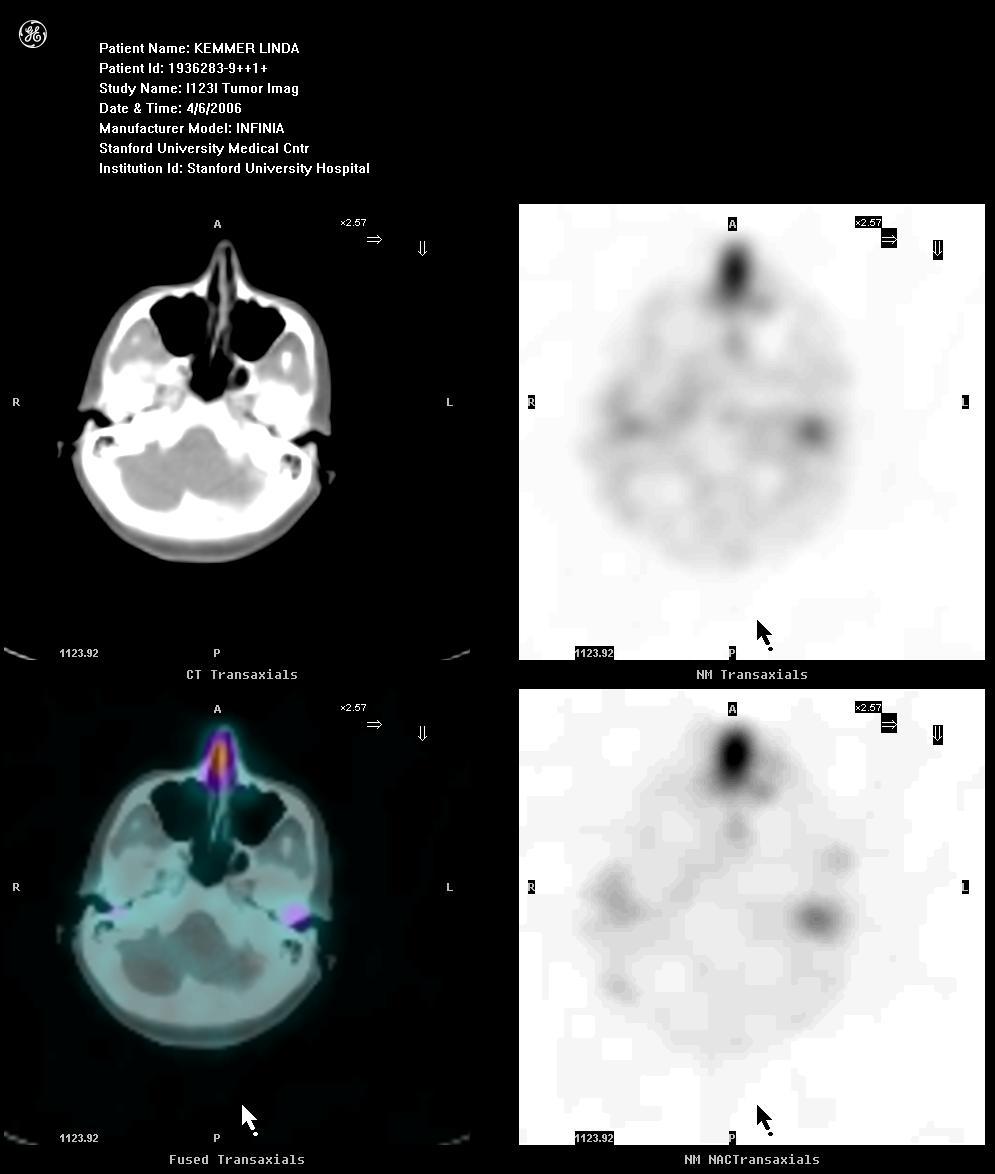
42 123 I scan positive; Tg 1,000 ng/ml PET very positive; surgery and XRT

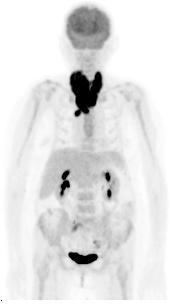
43 63-year-old woman with follicular thyroid cancer. Whole body 123 I scintiscan is negative. FDG PET/CT shows multiple lung metastases.
, mediastinal lymph nodes")
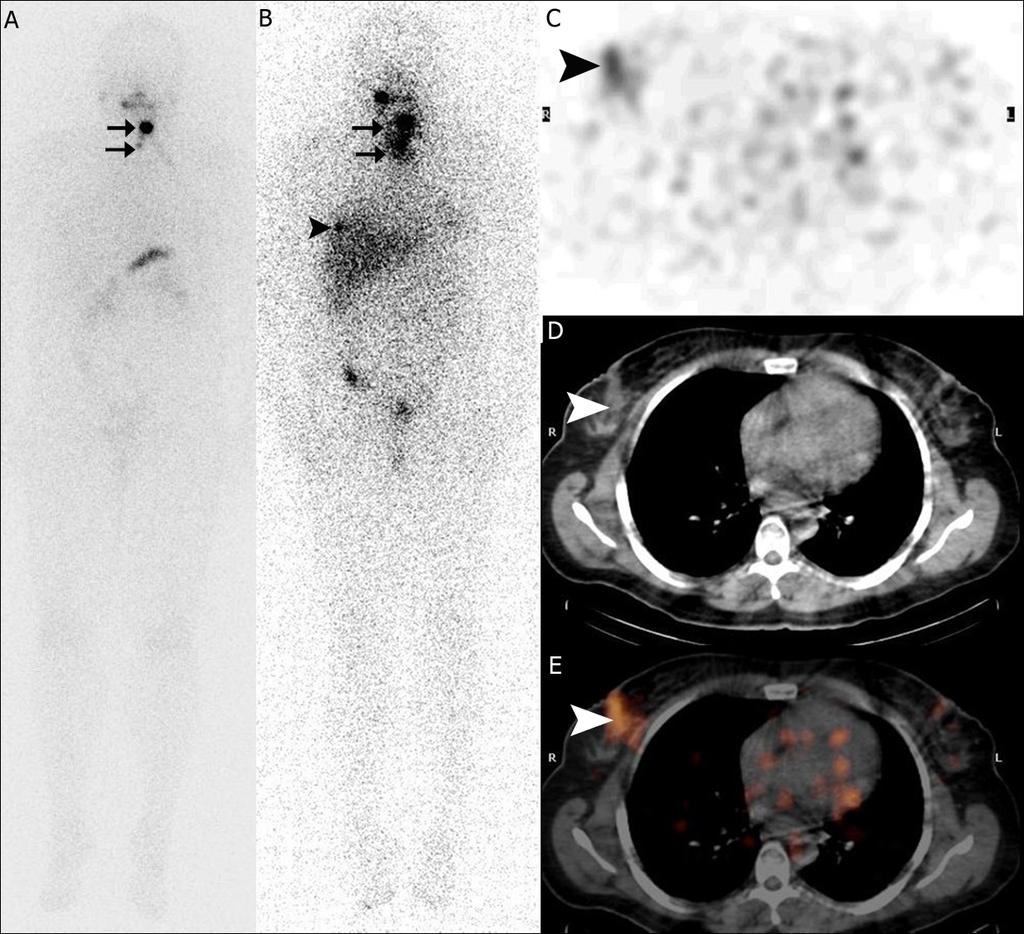
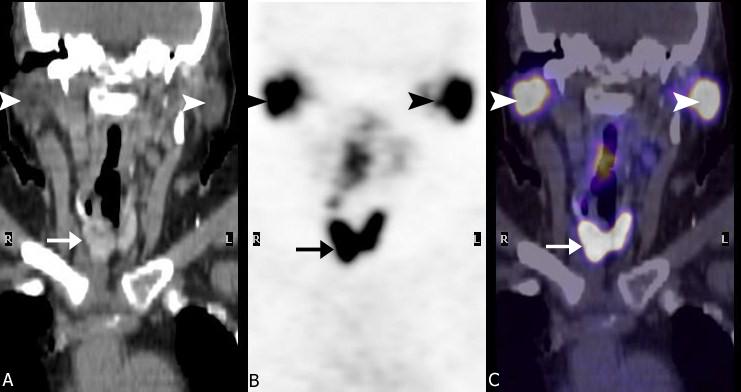
44 57-year-old man with papillary thyroid cancer. 123 I scintigraphy and FDG PET/CT show lesions in the thyroid bed (arrows), mediastinal lymph nodes (black arrowheads) and the left hip (white arrowheads).

45 123 I scan positive; Tg >3,000 ng/ml PET very positive; surgery and XRT
46 Ø 18 F FDG PET/CT is commonly used when there is discordance between elevated Tg and negative 123 I wholebody scans (WBS) Ø When used in combination, 18 F FDG PET/CT and 123 I WBS may result in tumor foci being missed in as few as 7% of cases, suggesting a complementary role for the two imaging modalities MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology

47 Ø 14 women & 7 men, years old (average: 50 ± 16) Ø All patients had papillary cancer MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
48 Serum Tg levels were ng/ml (average: 4.5 ng/ml) in the patients with negative PET scans (white) and ng/ml (average: 16.8 ng/ml) in the patients with positive scans (black) P: 0.029


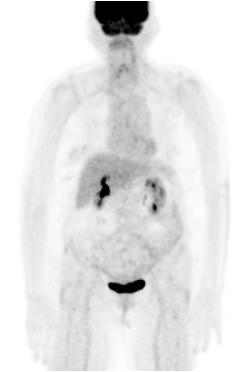
49 Local thyroid cancer recurrence, as well as pulmonary metastases in a 75-year old woman with Tg=36 ng/ml.
50 Ø The sensitivity and specificity of 18 F FDG PET for disease detection in this cohort were 88.2% (95% CI: ) and 75% (95 % CI: ), respectively Ø Detectable levels of Tg, even in the presence of a negative 123 I WBS or anatomic imaging, should prompt imaging with 18 F FDG PET/CT Ø Tg values less than 10 ng/ml can produce both positive and negative PET scans, while levels higher than 10 ng/ml appear to correlate with successful tumor identification on PET scans MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
51 Ø 44 women & 32 men, years old (average: 51.1±18.1) Ø 68 patients had papillary and 8 had follicular cancer Ø 98 PET/CT scans were analyzed (59 patients had 1 scan, 12 patients had 2 scans and 5 patients had 3 scans) MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
52 Sensitivities and specificities of PET/CT in differentiated thyroid cancer Sensitivity % (95% CI) Specificity % (95% CI) Based on patients (n=76) 88.6 ( ) 89.3 ( ) Lesions in thyroid bed 87.5 ( ) 96.5 ( ) Metastases (overall) 88.9 ( ) 94.3 ( ) Lymph nodes metastases 87.7 ( ) 97.1 ( ) Other metastases 88.9 ( ) 96.4 ( ) MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
53 Positive PET/CT Negative PET/CT Tg ng/ml mean (range) 1203 (0.5-28,357) 9.7 ( ) SUV max (thyroid bed) 10.8 (2.5-32) SUV max (metastases) 7.53 ( ) P value: TSH miu/l mean (range) in 73 scans 51 (< ) 32 ( ) ü Tg levels ranged ng/ml (average: 9.72) in pts with negative PET/CT and ,357 ng/ml (average: 1203) for those with positive PET/CT scans (P value: ) ü TSH values ranged miu/l (average: 32.21) in pts with negative PET/CT and miu/l (average: 51.22) in pts with positive scans (P value: MIPS 0.258) Stanford University Molecular Imaging Program at Stanford School of Medicine Department of Radiology
 in 63 patients (52 PTC and 11 FTC) Ø rhtsh-pet was significantly more sensitive than basal")
 and tended to be more sensitive for the detection of involved organs (94 vs. 79%; P = 0.")

54 Ø 38 women, 25 men; years old (average: 52) Ø PET/CT was performed before (basal PET) and h after rhtsh administration (rhtsh-pet) in 63 patients (52 PTC and 11 FTC) Ø rhtsh-pet was significantly more sensitive than basal PET for the detection of lesions (95 vs. 81%; P = 0.001) and tended to be more sensitive for the detection of involved organs (94 vs. 79%; P = 0.054) Ø However, basal PET and rhtsh-pet did not have significantly different sensitivity for detecting patients with any lesions (49 vs. 54%; P = 0.42) Ø Treatment changes due to true positive lesions occurred in 6% of cases MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology

55 Imaging MTC
56 Ø When MTC is diagnosed by fine needle aspiration biopsy, ultrasonography, CT and/or MRI scanning of the neck are indicated to look for cervical lymph node involvement Ø 123 I MIBG, 111 In Octreotide, and 99m Tc DMSA-V were investigated for evaluation of MTC and are currently used in detection of metastatic/recurrent disease Ø 18 F FDG PET detects more lesions than 99m Tc DMSA-V and 111 In Octreotide, as well as bone scintigraphy combined with morphologic imaging such as ultrasound, CT, or MRI MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology

57 Ø 7 women & 6 men, years old (average: 48 ± 13) Ø All patients had histologic diagnosis of MTC Ø The PET scan request was triggered by rising levels of calcitonin and negative anatomical imaging studies MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology
58 The calcitonin levels ranged from 52 to 5090 pg/ml (average: 1996 pg/ml) in patients with negative PET scans (black) and from 132 to 9500 pg/ml (average: 3757 pg/ml) in patients with positive studies (gray) P: 0.26

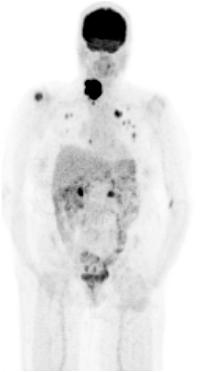
59 Whole body FDG PET of a 49-year old female with MTC recurrence in the thyroid bed and superior mediastinum. Her calcitonin levels prior to the PET examination were 9500 pg/ml.

60 Negative scan of a 42-year old female with calcitonin levels of 5090 pg/ml.
")

61 FDG PET scan of a 62-year old male with recurrent cervical (arrows) and hepatic disease (arrowheads), and calcitonin levels of 5290 pg/ml.
62 Ø The lesions were located in superior mediastinum (4), cervical lymph nodes (3), thyroid bed (2), lung (1) and liver (1) Ø The sensitivity and specificity of F-18 FDG PET for recurrence/residual disease detection in this cohort were 85.7% (95% CI: ) and 83.3 % (95 % CI: ), respectively Ø An overlap of measured calcitonin levels in patients with positive/negative scans was noted MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology

63 Imaging ATC

64 PET in anaplastic thyroid cancer Ø To stage disease Ø To define local extent of cancer Ø To evaluate response to therapy
65
66

67 Focal uptake of 18 FDG Scan done for non thyroidal cancer ü Incidentaloma ü Metaboloma Approximately 40-50% chance of thyroid cancer, usually papillary BUT Metastasis to thyroid can occur

68 THANK YOU!
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Thyroid Cancer. With 51 Figures and 30 Tables. Springer
 H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer
 Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
Strategies for detection of recurrent disease in longterm follow-up of differentiated thyroid cancer A rational approach to longterm follow-up based on dynamic risk assessment. World Congress on Thyroid
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Tumour Markers. For these reasons, only a handful of tumour markers are commonly used by most doctors.
 Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans
 131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
131-I Therapy Planning in Thyroid Cancer: The role of diagnostic radioiodine scans Anca M. Avram, M.D. Associate Professor of Radiology Department of Nuclear Medicine University of Michigan Ann Arbor,
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Thyroid Cancer (Carcinoma)
") Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Nuclear Medicine in Oncology
 Radiopharmaceuticals Nuclear Medicine in Oncology Practice Pharmaceutical Radionuc lide Function Tumor type Diphosphonates Tc-99m Osteoblast Bone tumor & metast. Ga-citrate Ga-67 Fe-analogue Bronchogenous
Radiopharmaceuticals Nuclear Medicine in Oncology Practice Pharmaceutical Radionuc lide Function Tumor type Diphosphonates Tc-99m Osteoblast Bone tumor & metast. Ga-citrate Ga-67 Fe-analogue Bronchogenous
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer
 Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Disseminated bone
Case 4: Disseminated bone metastases from differentiated follicular thyroid cancer Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Disseminated bone
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Outcomes Report: Accountability Measures and Quality Improvements
 Outcomes Report: Accountability Measures and Quality Improvements The s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures. Because we are an accredited
Outcomes Report: Accountability Measures and Quality Improvements The s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures. Because we are an accredited
What you need to know about Thyroid Cancer
 What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
What you need to know about Thyroid Cancer This booklet has been designed to help you to learn more about your thyroid cancer. It covers the most important areas and answers some of the frequently asked
Anca M. Avram, M.D. Professor of Radiology
 Thyroid Cancer Theranostics: the case for pre-treatment diagnostic staging 131-I scans for 131-I therapy planning Anca M. Avram, M.D. Professor of Radiology Department of Nuclear Medicine University of
Thyroid Cancer Theranostics: the case for pre-treatment diagnostic staging 131-I scans for 131-I therapy planning Anca M. Avram, M.D. Professor of Radiology Department of Nuclear Medicine University of
Outcomes Report: Accountability Measures and Quality Improvements
 Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
F NaF PET/CT in the Evaluation of Skeletal Malignancy
 F NaF PET/CT in the Evaluation of Skeletal Malignancy Andrei Iagaru, MD September 26, 2013 School of of Medicine Ø Introduction Ø F NaF PET/CT in Primary Bone Cancers Ø F NaF PET/CT in Bone Metastases
F NaF PET/CT in the Evaluation of Skeletal Malignancy Andrei Iagaru, MD September 26, 2013 School of of Medicine Ø Introduction Ø F NaF PET/CT in Primary Bone Cancers Ø F NaF PET/CT in Bone Metastases
Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma.
 ORIGINAL ARTICLE Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma. Md. Sayedur Rahman Miah, Md. Reajul Islam, Tanjim Siddika Institute of Nuclear Medicine & Allied Sciences,
ORIGINAL ARTICLE Thyroid remnant volume and Radioiodine ablation in Differentiated thyroid carcinoma. Md. Sayedur Rahman Miah, Md. Reajul Islam, Tanjim Siddika Institute of Nuclear Medicine & Allied Sciences,
Thyroid Cancer: Overview And Peculiar Aspects In Philippines Nemencio A. Nicodemus Jr., MD
 16 April 2016, Manila, Philippines Thyroid Cancer: Overview And Peculiar Aspects In Philippines Nemencio A. Nicodemus Jr., MD IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Learning
16 April 2016, Manila, Philippines Thyroid Cancer: Overview And Peculiar Aspects In Philippines Nemencio A. Nicodemus Jr., MD IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Learning
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Cancer A Superficial Introduction
 Cancer A Superficial Introduction Gabor Fichtinger, Queen s University Cancer some definitions Medical term: malignant neoplasm Class of diseases in which a group of cells display: uncontrolled growth
Cancer A Superficial Introduction Gabor Fichtinger, Queen s University Cancer some definitions Medical term: malignant neoplasm Class of diseases in which a group of cells display: uncontrolled growth
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS Advances in Medical and Surgical Management of Thyroid Cancer January 23-24, 2015 I-131 ABLATION AND ADJUVANT THERAPY OF THYROID CANCER 2015 Leonard Wartofsky,
Dr Sneha Shah Tata Memorial Hospital, Mumbai.
 Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Imaging in Thyroid Cancer
 Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
Imaging in Thyroid Cancer Susan J. Mandel MD MPH University of Pennsylvania School of Medicine Philadelphia, PA I-123 Ultrasound Background Radioiodine ablation of thyroid remnants after surgery is a generally
MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site
 POLICY: PG0364 ORIGINAL EFFECTIVE: 04/22/16 LAST REVIEW: 07/26/18 MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site GUIDELINES This policy does not certify benefits or authorization
POLICY: PG0364 ORIGINAL EFFECTIVE: 04/22/16 LAST REVIEW: 07/26/18 MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site GUIDELINES This policy does not certify benefits or authorization
THYROID CANCER IN CHILDREN
 THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
THYROID CANCER IN CHILDREN Isabel ROCA, Montserrat NEGRE Joan CASTELL HU VALL HEBRON BARCELONA EPIDEMIOLOGY ADULTS males 1,2-2,6 cases /100.000 females 2,0-3,8 cases /100.000 0,02-0,3 / 100.000 children
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
AN INTRODUCTION TO NUCLEAR MEDICINE
 AN INTRODUCTION TO NUCLEAR MEDICINE WITH RESPECT TO THYROID DISORDERS By: B.Shafiei MD Nuclear Physician Taleghani Medical Center Radioactive: An element with Unstable Nucleus (Excess Energy), can achieve
AN INTRODUCTION TO NUCLEAR MEDICINE WITH RESPECT TO THYROID DISORDERS By: B.Shafiei MD Nuclear Physician Taleghani Medical Center Radioactive: An element with Unstable Nucleus (Excess Energy), can achieve
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Preoperative Evaluation
 Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Preoperative Evaluation Lateral compartment lymph nodes are easier to detect and are amenable to FNA Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
Epidemiology in Texas 2006 Annual Report. Cancer
 Epidemiology in Texas 2006 Annual Report Cancer Epidemiology in Texas 2006 Annual Report Page 94 Cancer Incidence and Mortality in Texas, 2000-2004 The Texas Department of State Health Services Texas Cancer
Epidemiology in Texas 2006 Annual Report Cancer Epidemiology in Texas 2006 Annual Report Page 94 Cancer Incidence and Mortality in Texas, 2000-2004 The Texas Department of State Health Services Texas Cancer
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
How good are we at finding nodules? Thyroid Nodules Thyroid Cancer Epidemiology Initial management Long-term follow up Disease-free status
 New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
New Perspectives in Thyroid Cancer Jennifer Sipos, MD Assistant Professor of Medicine Division of Endocrinology The Ohio State University Outline Thyroid Nodules Thyroid Cancer Epidemiology Initial management
Ryan Niederkohr, M.D. Slides are not to be reproduced without permission of author
 Ryan Niederkohr, M.D. CMS: PET/CT CPT CODES 78814 Limited Area (e.g., head/neck only; chest only) 78815 78816 Regional (skull base to mid-thighs) True Whole Body (skull vertex to feet) SELECTING FIELD
Ryan Niederkohr, M.D. CMS: PET/CT CPT CODES 78814 Limited Area (e.g., head/neck only; chest only) 78815 78816 Regional (skull base to mid-thighs) True Whole Body (skull vertex to feet) SELECTING FIELD
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
New Visions in PET: Surgical Decision Making and PET/CT
 New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
Oncology 101. Cancer Basics
 Oncology 101 Cancer Basics What Will You Learn? What is Cancer and How Does It Develop? Cancer Diagnosis and Staging Cancer Treatment What is Cancer? Cancer is a group of more than 100 different diseases
Oncology 101 Cancer Basics What Will You Learn? What is Cancer and How Does It Develop? Cancer Diagnosis and Staging Cancer Treatment What is Cancer? Cancer is a group of more than 100 different diseases
Subject: PET Scan With or Without CT Attenuation. Original Effective Date: 11/7/2017. Policy Number: MCR: 610. Revision Date(s): Review Date:
: Review Date:") Subject: PET Scan With or Without CT Attenuation Policy Number: MCR: 610 Revision Date(s): MHW Original Effective Date: 11/7/2017 Review Date: DISCLAIMER This Molina Clinical Review (MCR) is intended to
Subject: PET Scan With or Without CT Attenuation Policy Number: MCR: 610 Revision Date(s): MHW Original Effective Date: 11/7/2017 Review Date: DISCLAIMER This Molina Clinical Review (MCR) is intended to
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Hybrid Imaging SPECT/CT PET/CT PET/MRI. SNMMI Southwest Chapter Aaron C. Jessop, MD
 Hybrid Imaging SPECT/CT PET/CT PET/MRI SNMMI Southwest Chapter 2014 Aaron C. Jessop, MD Assistant Professor, Department of Nuclear Medicine UT MD Anderson Cancer Center, Houston, Texas Complimentary role
Hybrid Imaging SPECT/CT PET/CT PET/MRI SNMMI Southwest Chapter 2014 Aaron C. Jessop, MD Assistant Professor, Department of Nuclear Medicine UT MD Anderson Cancer Center, Houston, Texas Complimentary role
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art
 Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Work Up & Evaluation of Thyroid Nodules In 2013: State of The Art BC Surgical Oncology Network, Fall Update Todd McMullen MD PhD FRCSC FACS Endocrine Surgeon Divisions of General Surgery and Oncology Director,
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Case-Based Discussion of Thyroid Cancer Therapy
 Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Case-Based Discussion of Thyroid Cancer Therapy Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology The Ohio State University Co-Leader, Molecular Biology
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
1. Protocol Summary Summary of Trial Design. IoN
 1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
Bioengineering and World Health. Lecture Twelve
 Bioengineering and World Health Lecture Twelve Four Questions What are the major health problems worldwide? Who pays to solve problems in health care? How can technology solve health care problems? How
Bioengineering and World Health Lecture Twelve Four Questions What are the major health problems worldwide? Who pays to solve problems in health care? How can technology solve health care problems? How
Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers
 Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers Samuel M. Lesko, MD, MPH Medical Director Karen Ryczak, RN Surveillance Coordinator December 2014 334 Jefferson Avenue, Scranton,
Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers Samuel M. Lesko, MD, MPH Medical Director Karen Ryczak, RN Surveillance Coordinator December 2014 334 Jefferson Avenue, Scranton,
Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional
 study: An IRB approved study with funding to Rochester Regional") October 20 th 2018 Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional Health from Veracyte Review ultrasound
October 20 th 2018 Principal Site Investigator ENHANCE (Evaluation of Thyroid FNA Genomic Signature) study: An IRB approved study with funding to Rochester Regional Health from Veracyte Review ultrasound
Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers
 Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers Samuel M. Lesko, MD, MPH Medical Director Karen Ryczak, RN Surveillance Coordinator November 2018 334 Jefferson Avenue, Scranton,
Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers Samuel M. Lesko, MD, MPH Medical Director Karen Ryczak, RN Surveillance Coordinator November 2018 334 Jefferson Avenue, Scranton,
Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers
 Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers Samuel M. Lesko, MD, MPH Medical Director Karen Ryczak, RN Surveillance Coordinator December 2017 334 Jefferson Avenue, Scranton,
Cancer in Northeastern Pennsylvania: Incidence and Mortality of Common Cancers Samuel M. Lesko, MD, MPH Medical Director Karen Ryczak, RN Surveillance Coordinator December 2017 334 Jefferson Avenue, Scranton,
FDG PET/CT in the Detection of Pancreatic Metastasis in a Patient with Follicular Thyroid Carcinoma and Negative I-131 Whole Body Scan Findings
 CASE REPORT FDG PET/CT in the Detection of Pancreatic Metastasis in a Patient with Follicular Thyroid Carcinoma and Negative I-131 Whole Body Scan Findings Hae Jung Na 1, Bo Hyun Kim 1,2, Ji Ryang Kim
CASE REPORT FDG PET/CT in the Detection of Pancreatic Metastasis in a Patient with Follicular Thyroid Carcinoma and Negative I-131 Whole Body Scan Findings Hae Jung Na 1, Bo Hyun Kim 1,2, Ji Ryang Kim
Thyroid Neoplasm. ORL-Head and neck Surgery 2014
 In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
In The Name of God Thyroid Neoplasm ORL-Head and neck Surgery 2014 Malignant Neoplasm By age 90, virtually everyone has nodules Estimates of cancer prevalence at autopsy 4% to 36% Why these lesions are
Cancer in Estonia 2014
 Cancer in Estonia 2014 Estonian Cancer Registry (ECR) is a population-based registry that collects data on all cancer cases in Estonia. More information about ECR is available at the webpage of National
Cancer in Estonia 2014 Estonian Cancer Registry (ECR) is a population-based registry that collects data on all cancer cases in Estonia. More information about ECR is available at the webpage of National
Cancer Program Report 2014
 Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis
 1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Reference No: Author(s) Approval date: October committee. September Operational Date: Review:
 Approval date: October committee. September Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) guidelines for Thyroid cancer Dr Fionnuala Houghton Consultant Clinical Oncologist & Dr Lois Mulholland Consultant Clinical Oncologist
Thermo Scientific B R A H M S Biomarkers Tumor Marker Assays. Excellent precision. Confident cancer monitoring
 Thermo Scientific B R A H M S Biomarkers Tumor Marker Assays Excellent precision Confident cancer monitoring Thermo Scientific B R A H M S Biomarkers Tumor Markers Parameter Clinical Interest Product Technology
Thermo Scientific B R A H M S Biomarkers Tumor Marker Assays Excellent precision Confident cancer monitoring Thermo Scientific B R A H M S Biomarkers Tumor Markers Parameter Clinical Interest Product Technology
Biochemistry of Carcinogenesis. Lecture # 35 Alexander N. Koval
 Biochemistry of Carcinogenesis Lecture # 35 Alexander N. Koval What is Cancer? The term "cancer" refers to a group of diseases in which cells grow and spread unrestrained throughout the body. It is difficult
Biochemistry of Carcinogenesis Lecture # 35 Alexander N. Koval What is Cancer? The term "cancer" refers to a group of diseases in which cells grow and spread unrestrained throughout the body. It is difficult
Thyroid Ultrasonography: clinical and radiological correlations
 Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Case 5: Thyroid cancer in 42 yr-old woman with Graves disease
 Case 5: Thyroid cancer in 42 yr-old woman with Graves disease Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Thyroid cancer in 42 yr-old woman with
Case 5: Thyroid cancer in 42 yr-old woman with Graves disease Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Thyroid cancer in 42 yr-old woman with
B Berry, J. 25 see also suspensory ligament of Berry biopsy see fine-needle aspiration biopsy (FNAB); open wedge biopsy
; open wedge biopsy") 174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
174 Index Index Page numbers in italics refer to illustrations A abscess 80, 137 adenoma 61 parathyroid 18, 18 19, 62, 84 differential diagnosis 84, 84, 85, 85 thyroid 63 follicular 62, 63, 64 macrofollicular
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Carcinoma of thyroid - clinical presentation and outcome
 Med. J. Malaysia Vol. 46 No. 3 September 1991 Carcinoma of thyroid - clinical presentation and outcome K. Sothy, MBBS M. Mafauzy, MBBS, MRCP, M.Med. Sci. W.B. Wan Mohamad, MD, MRCP B.E. Mustaffa, MBBS,
Med. J. Malaysia Vol. 46 No. 3 September 1991 Carcinoma of thyroid - clinical presentation and outcome K. Sothy, MBBS M. Mafauzy, MBBS, MRCP, M.Med. Sci. W.B. Wan Mohamad, MD, MRCP B.E. Mustaffa, MBBS,
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.