Renal Cell Carcinoma: Navigating a Maze of Choices
|
|
|
- Morris Norton
- 5 years ago
- Views:
Transcription


1 Renal Cell Carcinoma: Navigating a Maze of Choices Sumanta Kumar Pal, M.D. Associate Professor Department of Medical Oncology & Experimental Therapeutics Co-Director, Kidney Cancer Program City of Hope Comprehensive Cancer Center August 11, 2018
2 Disclosures Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Aveo, Eisai, Roche, Pfizer, Novartis, Exelixis, Ipsen, BMS, Astellas speakers bureau: Genentech The speaker will directly disclosure the use of products for which are not labeled (e.g., off label use) or if the product is still investigational.
3 Debates in RCC Therapy Is HD IL-2 appropriate for everyone? Sunitinib or sorafenib? Everolimus or sorafenib? Cabozantinib, nivolumab or lenvatinib/ everolimus? Goals of therapy: 1. Live longer (ideally with a cure!) 2. Live better First Line Debate Temsirolimus for poor risk? Axitinib or everolimus? Nivo/ipi or cabozantinib or bev/atezo? Second Line Debate
4 A Banner Year for Immunotherapy in RCC ESMO 2017: Nivolumab/Ipilimumab vs Sunitinib Primary Analysis SITC 2017: Nivolumab/Ipilimumab vs Sunitinib Subset Analysis GUCS 2018: Bevacizumab/Atezolizumab vs Sunitinib Primary Analysis
5 CheckMate 214: Study design Treatment-naïve advanced or metastatic clear-cell RCC Measurable disease KPS 70% Tumor tissue available for PD-L1 testing Patients Randomize 1:1 Stratified by IMDC prognostic score (0 vs 1 2 vs 3 6) Region (US vs Canada/Europe vs Rest of World) Treatment Arm A 3 mg/kg nivolumab IV + 1 mg/kg ipilimumab IV Q3W for four doses, then 3 mg/kg nivolumab IV Q2W Arm B 50 mg sunitinib orally once daily for 4 weeks (6-week cycles) Treatment until progression or unacceptable toxicity Escudier et al ESMO 2017
6 Overall Survival (Probability) Co-primary endpoint OS: IMDC intermediate/poor risk Median OS, months (95% CI) NIVO + IPI NR (28.2 NE) No. at Risk NIVO + IPI SUN 0 Outcome 3 6 NIVO + IPI N = N = 847 SUN N = 422 Confirmed ORR, a % (95% CI) 42 (37 47) 27 (22 31) Confirmed BOR, a % Complete response Partial response Stable disease Progressive disease Unable to determine/not reported 9 b P < b SUN 26.0 (22.1 NE) Hazard ratio (99.8% CI), 0.63 ( ) P < Months Escudier et al ESMO 2017
7 Exploratory endpoint ORR and PFS: IMDC favorable risk N = 249 a Outcome NIVO + IPI N = 125 SUN N = 124 Confirmed ORR, b % (95% CI) 29 (21 38) 52 (43 61) P = PFS, c median (95% CI), months 15.3 ( ) 25.1 (20.9 NE) HR (99.1% CI) 2.18 ( ) P < Escudier et al ESMO 2017
8 Patient disposition: All treated patients NIVO + IPI N = 547 SUN N = 535 Treatment discontinuation, % Reasons for treatment discontinuation, % Disease progression Study drug toxicity Adverse event unrelated to study drug Other Median duration of therapy (95% CI), months 7.9 ( ) 7.8 ( ) Median doses received (range), no. Nivolumab Ipilimumab 14 (1 63) 4 (1 4) NA NA Median daily dose (range), mg/day NA 31 (14 50) In the NIVO + IPI arm, 79% of patients received all four doses of IPI Median follow-up was 25.2 months Escudier et al ESMO 2017
9 Secondary endpoint Treatment-related adverse events: All treated patients NIVO + IPI N = 547 SUN N = 535 Event, % Any grade Grade 3 5 Any grade Grade 3 5 a Treatment-related adverse events in 25% of patients Fatigue Pruritus 28 <1 9 0 Diarrhea Nausea 60% of patients treated with NIVO 20 + IPI required 2 systemic 38 1 Hypothyroidism corticosteroids for an 16 adverse <1 event 25 <1 Decreased appetite Dysgeusia <1 Stomatitis Hypertension 2 < Mucosal inflammation Palmar-plantar erythrodysesthesia syndrome Treatment-related AEs leading to discontinuation, % Treatment-related deaths n = 7 b n = 4 c a Two patients had grade 5 cardiac arrest. b Pneumonitis, immune mediated bronchitis, lower GI hemorrhage, hemophagocytic syndrome, sudden death, liver toxicity, lung infection. c Cardiac arrest (n = 2), heart failure, multiple organ failure Escudier et al ESMO 2017
10 Progression-Free Survival (Probability) Exploratory endpoint PFS by PD-L1 expression: IMDC intermediate/poor risk PD-L1 <1% (n = 562) PD-L1 1% (n = 214) Median PFS, months (95% CI) Median PFS, months (95% CI) NIVO + IPI 11.0 ( ) SUN 10.4 ( ) HR (95% CI) 1.00 ( ) P = NIVO + IPI 22.8 (9.4 NE) SUN 5.9 ( ) HR (95% CI) 0.48 ( ) P = No. at Risk NIVO SUN Months Months
11 Overall Survival (Probability) Motzer et al SITC OS by tumor PD-L1 expression: IMDC intermediate/poor risk PD-L1 <1% (n = 562) PD-L1 1% (n = 214) Median OS (95% CI), months NIVO + IPI NR (28.2 NE) SUN NR (24.0 NE) HR (95% CI), 0.73 ( ) P = Median OS (95% CI), months NIVO + IPI SUN NR (NE NE) 19.6 (14.8 NE) HR (95% CI), 0.45 ( ) P < No. at Risk Months NIVO + IPI SUN Months
12 A Banner Year for Immunotherapy in RCC ESMO 2017: Nivolumab/Ipilimumab vs Sunitinib Primary Analysis SITC 2017: Nivolumab/Ipilimumab vs Sunitinib Subset Analysis GUCS 2018: Bevacizumab/Atezolizumab vs Sunitinib Primary Analysis
13 Study Design Key Eligibility: Treatment-naive advanced or metastatic RCC Clear cell and/or sarcomatoid histology KPS 70 Tumor tissue available for PD-L1 staining Stratification: MSKCC risk score Liver metastases PD-L1 IC IHC status (< 1% vs 1%) a N = 915 R 1:1 Atezolizumab 1200 mg IV q3w b + Bevacizumab 15 mg/kg IV q3w b Sunitinib 50 mg/day orally (4 wk on, 2 wk off) a 1% IC: 40% prevalence using SP142 IHC assay; b No dose reduction for atezolizumab or bevacizumab. Presented by: Dr. Robert Motzer 13
14 PFS (PD-L1+ & ITT) Co-Primary Endpoint Median PFS, mo (95% CI) Atezo + Bev 11.2 (8.9, 15.0) Sunitinib 7.7 (6.8, 9.7) HR, 0.74 (95% CI: 0.57, 0.96) P = 0.02 Median PFS, mo (95% CI) Atezo + Bev 11.2 (9.6, 13.3) Sunitinib 8.4 (7.5, 9.7) HR, 0.83 (95% CI: 0.70, 0.97) Consistent PFS results in PD-L1+ & ITT population by investigator review. PFS assessed by investigators. Minimum follow-up, 12 mo. Median follow-up, 15 mo. Presented by: Dr. Robert Motzer 14
15 Objective Response Rate Secondary Endpoint Confirmed ORR, % 95% CI Atezo + Bev n = % (35, 50) PD-L1+ Sunitinib n = % (28, 42) Complete response 9% 4% Partial response 34% 30% PD-L1+ Median DOR, mo (95% CI) Ongoing Responders, n (%) Atezo + Bev NR (12.4, NR) 49 (65%) Sunitinib 12.9 (9.8, NR) 34 (53%) Higher CR rates than associated with VEGF-TKIs. Stable disease 32% 35% Progressive disease 19% 21% Not evaluable a 7% 10% NR, not reached. a Including patients with no post-baseline tumor assessment. ORR assessed by investigators in patients with measurable disease at baseline. Minimum follow-up, 12 mo. Median follow-up, 15 mo. Presented by: Dr. Robert Motzer 15


16 Treatment-related AEs > 5% difference between arms and 20% frequency in either arm Atezo + Bev Sunitinib Secondary Endpoint Diarrhea PPE Hypertension Fatigue Nausea Dysgeusia Decreased appetite Mucosal inflammation Stomatitis Asthenia Discontinuation rate due to AEs lower with bev/atezo; 16% of patients required steroids. Vomiting Proteinuria All-grade AEs Grade 3-4 AEs All-grade AEs Grade 3-4 AEs 60% 50% 40% 30% 20% 10% 0 10% 20% 30% 40% 50% 60% PPE, palmar-plantar erythrodysesthesia. Presented by: Dr. Robert Motzer 16
17 PFS and ORR by IRC Secondary Endpoint Median PFS, mo (95% CI) Stratified HR (95% CI) Confirmed ORR, % (95% CI) Atezo + Bev n = (6.9, 12.5) 36% (29, 44) PD-L1+ PD-L1- a ITT 0.93 (0.72, 1.21) Sunitinib n = (6.1, 11.1) 33% (26, 40) Atezo + Bev n = (8.3, 13.3) 32% (26, 37) 0.84 (0.67, 1.04) Sunitinib n = 277 b 8.4 (7.4, 10.1) 30% (25, 36) Atezo + Bev n = (8.3, 11.5) 33% (29, 38) 0.88 (0.74, 1.04) Sunitinib n = (7.0, 9.7) 31% (27, 36) CR rate 15% 8% 8% 6% 11% 7% IRC and INV assessment of PFS benefit was generally consistent in the ITT population; however, results differed from INV assessment in patients with PD-L1+ disease Investigators, IRC reviewers and the sponsor were blinded to PD-L1 status a PD-L1 negative tumors had a PD-L1 IC IHC expression < 1%. b n = 276 for ORR. Presented by: Dr. Robert Motzer 17
18 Overall Survival in ITT & PD-L1+ Co-Primary Endpoint Atezo + Bev Sunitinib ITT Median OS, mo (95% CI) Not reached Not reached HR, 0.81 (95% CI: 0.63, 1.03) P = 0.09 PD-L1+ Median OS, mo (95% CI) Atezo + Bev Not reached Sunitinib 23.3 (21.3, NR) HR, 0.68 (95% CI: 0.46, 1.00) OS data are immature; 29% of patients had an OS event at data cutoff OS data are immature; 30% of patients had an OS event at data cutoff Minimum follow-up, 12 mo. Median of follow-up, 15 mo. Event/patient ratio: 27% for atezo + bev, 31% for sunitinib. The OS analysis did not pass the P value boundary of alpha = at the first interim analysis. Presented by: Dr. Robert Motzer 18

19 Immotion151 vs CheckMate214 CheckMate214 Immotion151 Duration of doublet therapy Toxicity Benefit across risk strata Mature OS data Impressive CR rate Impressive CR rate OS trend PFS EP positive

20 Immotion151 vs CheckMate214 CheckMate214 Immotion151
 8.6 mo 43 Sunitinib (N=78) 5.3 mo 49 HR=0.48 (95% CI: 0.31-0.74), p=0.")
 Data cutoff : PFS, Sep 15, 2016; OS,")
 HR=0.80 (95% CI: 0.53-1.")
21 Probability of PFS Choueiri et al ESMO 2017 PFS per IRC and Overall Survival Median PFS No. of Events Cabozantinib (N=79) 8.6 mo 43 Sunitinib (N=78) 5.3 mo 49 HR=0.48 (95% CI: ), p= (2-sided) Subgroup Analyses of PFS per IRC No. at risk Cabozantinib Sunitinib Time Since Randomization (Months) Data cutoff : PFS, Sep 15, 2016; OS, July 1, 2017; IRC, Independent Review Committee; IMDC, International Metastatic RCC Database Consortium. Favors cabozantinib Favors sunitinib Overall Survival (OS) HR=0.80 (95% CI: ); p=0.29 (2-sided) Median OS: Cabozantinib 26.6 mo, Sunitinib 21.2 mo 21
22 Algorithm incorporating emerging first-line options Treatment First-Line Second-Line Good risk Bevacizumab/Atezolizumab Cabozantinib Cabozantinib* Nivolumab Intermediate/Poor-risk CHMP ruled against Bevacizumab/Atezolizumab approval of nivolumab/ipilimumab! Cabozantinib Nivolumab/Ipilimumab Cabozantinib* Nivolumab * For special populations (e.g., bony metastatic disease)
23 Beyond the current debate Is HD IL-2 appropriate for everyone? Sunitinib or sorafenib? Everolimus or sorafenib? Cabozantinib, nivolumab or lenvatinib/ everolimus? TKI + PD-1/-L1 Ab? First Line Debate Temsirolimus for poor risk? Axitinib or everolimus? Nivo/ipi or cabozantinib or bev/atezo? Second Line Debate
24 Does biology matter? Agent Immunomodulatory Properties Sunitinib Reduces peripheral MDSCs, reverses type 1 T-cell suppression, decreases Tregs Pazopanib Prompts evolution of MDSC subtype; non-responders have elevated MDSCs Axitinib Biology may matter, but we will have clinical data regardless. Induces differentiation of monocytic MDSCs toward an antigen-presenting phenotype Cabozantinib Induces tumor cell death via CXCR4-dependent neutrophil recruitment Bevacizumab Decreases peripheral Tregs 1 Ko et al CCR 2009; 2 Pal et al J Urol 2015; 3 Du Four et al Oncoimmunol 2015; 1 Patnaik et al Cancer Disc 2017; 3 Thomas et al Cancer Immunol Immunother 2017
25 % Progression Free % Progression Free % Progression Free Objective of combination therapy TKI IO TKI + IO? Time Time Time

26 Axitinib + Pembrolizumab * Stable disease or partial response not confirmed, or no follow-up scans available. ORR=objective response rate Presented by: Michael B Atkins, MD 26
 Median PFS 20.9 months (95% CI 15.")
27 Axitinib + Pembrolizumab Median time to response was 2.8 months (range ) Median duration of tumor response was 18.6 months (95% CI 15.1 not reached) Median PFS 20.9 months (95% CI 15.4 NE) Median OS NR CI=confidence interval; PD=progressive disease Presented by: Michael B Atkins, MD 27

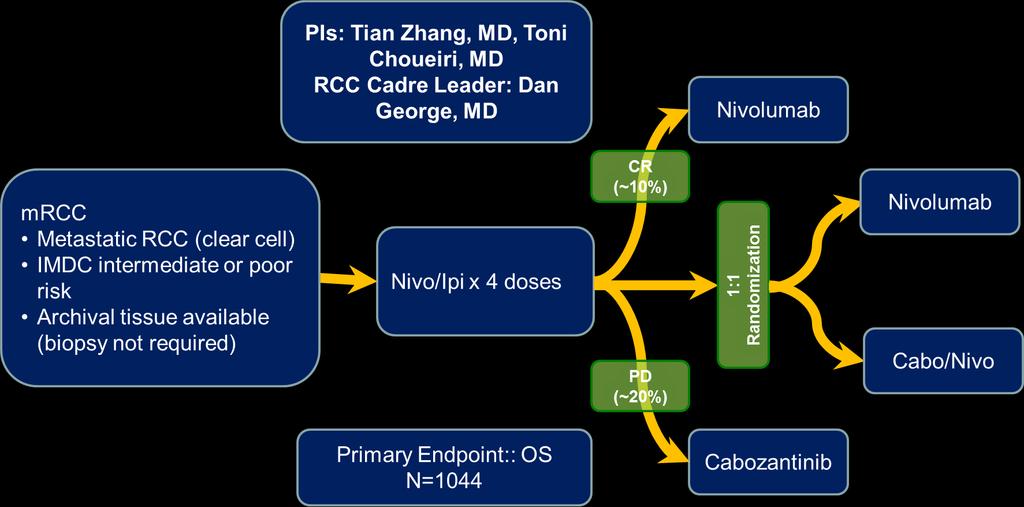
28 Cabozantinib/Nivolumab +/- Ipilimumab Presented by: Dr. Rosa Nadal (PI: Dr. Andrea Apolo) 28



29 Tivozanib + Nivolumab Presented by: Dr. Bernard Escudier 29

30 The current landscape Motzer et al ASCO GU 2018; Lee et al ESMO 2017; Choueiri et al ASCO 2017; Atkins et al ASCO GU 2018; Nadal et al ASCO GU 2018
 after prior platinum-based therapy, or RCC (clear cell, non-clear cell) with or without prior systemic")
31 Define Recommend Dose Understanding activity of PD-L1 inhibitors in rare subtypes Cabozantinib with Atezolizumab Dose Expansion RCC with clear cell histology who have not received prior systemic anticancer therapy Dose escalation UC (including renal pelvis, ureter, bladder, urethra) after prior platinum-based therapy, or RCC (clear cell, non-clear cell) with or without prior systemic anticancer therapy UC with progression on or after platinumcontaining chemotherapy UC not eligible for cisplatin-based chemo and no prior platinum-based chemotherapy UC eligible for cisplatin-based chemotherapy with no prior platinum-based chemotherapy We need you! Dose Escalation in ncrcc Planned NCT : A Phase 1b Dose-Escalation Study of Cabozantinib (XL184) Administered in Combination With Atezolizumab to Subjects With Locally Advanced or Metastatic Solid Tumors
32 Phase III Assessments of VEGF + CPI Combinations in RCC Control Sunitinib Sunitinib Sunitinib Sunitinib Sunitinib Sunitinib Comparator Nivolumab/Ipilimumab Bevacizumab + Atezolizumab Axitinib + Pembrolizumab Lenvatinib + Everolimus vs Lenvatinib/Pembrolizumab Axitinib + Avelumab Cabozantinib/Nivolumab
33 Sunitinib Nivolumab Could increasing crossover from sunitinib to nivolumab blunt OS? Margin of benefit in OS ~20% of patients on control arm crossed over from sunitinib to nivolumab in Immotion151 Time
34 Forthcoming Phase III Trials
35 Beyond the current debate Is HD IL-2 appropriate for everyone? Sunitinib or sorafenib? Everolimus or sorafenib? Cabozantinib, nivolumab or lenvatinib/ everolimus? TKI + PD-1/-L1 Ab? First Line Debate Temsirolimus for poor risk? Axitinib or everolimus? Nivo/ipi or cabozantinib or bev/atezo? Second Line Debate Future Debates: Will adjuvant therapy change the preferred upfront regimen?
36 My Take on Adjuvant Therapy with VEGF inhibitors S-TRAC shows benefit in DFS balanced with duration of treatment Favors Adjuvant Therapy Favors Observation PROTECT and ASSURE fail to meet primary endpoint No study shows a compelling signal of OS benefit Motzer et al J Clin Oncol 35, 2017 (suppl; abstr 4507)
 Key Eligibility (n=664) High risk OR limited metastasis s/p metastasectomy s/p nephrectomy 12 weeks No evidence of residual disease")
 PD-L1 (IC0 vs IC1/2/3) Region (US/Canada vs ROW) Atezolizumab 1200 mg IV q3wk x 16 cycles Placebo q3wk x 16 cycles We need you!")
37 1:1 Randomization Adjuvant Immunotherapy for RCC? Atezolizumab Adjuvant (An SUO-CTC Trial) Key Eligibility (n=664) High risk OR limited metastasis s/p metastasectomy s/p nephrectomy 12 weeks No evidence of residual disease Clear cell or sarcomatoid histology Stratification Factors Disease stage (T2/T3a vs. T3b/c/T4/N+ vs metastasectomy) PD-L1 (IC0 vs IC1/2/3) Region (US/Canada vs ROW) Atezolizumab 1200 mg IV q3wk x 16 cycles Placebo q3wk x 16 cycles We need you! NCT : A Phase III, Open-Label, Multicenter, Randomized Study of Atezolizumab (Anti-PD-L1 Antibody) Versus Observation as Adjuvant Therapy in Patients With High-Risk Muscle-Invasive Urothelial Carcinoma After Surgical Resection
38 Beyond the current debate Is HD IL-2 appropriate for everyone? Sunitinib or sorafenib? Everolimus or sorafenib? Cabozantinib, nivolumab or lenvatinib/ everolimus? TKI + PD-1/-L1 Ab? First Line Debate Temsirolimus for poor risk? Axitinib or everolimus? Nivo/ipi or cabozantinib or bev/atezo? Second Line Debate Future Debates: 1. Role for VEGF or IO alone? 2. Non clear cell disease? 3. Focus on optimizing VEGF-directed therapy?

39 KEYNOTE-427: A role for CPI monotherapy? McDermott et al ASCO 2018

40 KEYNOTE-427: A role for CPI monotherapy? McDermott et al ASCO 2018
 Translational PI: B.")



41 SWOG 1500 for mprcc PI: S. Pal (City of Hope) Translational PI: B. Shuch (Yale) BISQFP funding for genomic characterization Requires 41 pts/arm 164 pts total Assuming 10% ineligibility 180 pts total We need you! NCT : A Randomized, Phase II Efficacy Assessment of Multiple MET Kinase Inhibitors (Cabozantinib [NSC #761968], Crizotinib [NSC #749005], Savolitinib [NSC #785348], and Sunitinib [NSC #736511]) in Metastatic Papillary Renal Carcinoma (PAPMET)

 Prior PD-1/PD-L1 treatment (yes,")
42 HOPE 218: An FDA Mandated Study (PI: Pal) N = 306 Key Inclusion Criteria Advanced clear cell RCC Progression on/after 1 prior VEGF-targeted treatment Prior PD-1/PD-L1 inhibitor treatment is allowed Measurable disease KPS 70 R 1:1 Lenvatinib 18 mg qd + Everolimus 5 mg qd Lenvatinib 14 mg qd + Everolimus 5 mg qd Heng (Calgary) Puente (Spain) On Cycle 2 Day 1: Lenvatinib will be escalated to 18 mg qd if no intolerable G2 or G3/G4 AEs or SAEs are observed in the first 28 days Stratification by: MSKCC prognostic groups (favorable, intermediate and poor risk) Prior PD-1/PD-L1 treatment (yes, no) 42
 Ravi Salgia, MD (Chair,Medical Oncology) GU Fellows: Paulo")
43 Thank you! City of Hope / Beckman Research Institute Tanya Dorff, MD (Head, GU Medical Oncology) Ravi Salgia, MD (Chair,Medical Oncology) GU Fellows: Paulo Bergerot, MD; Cris Bergerot, PsyD; Nazli Dizman, MD; Jacob Adashek; Meghan Salgia Feel free to or call me for trials!
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
NEXT GENERATION DRUGS IN KIDNEY CANCER. Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden
 NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Immunotherapy for the Treatment of Kidney and Bladder Cancer
 Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY FOR THE RIGHT PATIENT
 Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA. Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA
 UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
Integrating novel therapy in advanced renal cell carcinoma
 Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Atezolizumab Adjuvant Study: Medical Oncologist Perspective. Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center
 Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
I Kid(ney) You Not: Updates on Renal Cell Carcinoma
 You Not: Updates on Renal Cell Carcinoma") Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients
 A Phase II Study of With or Without Bevacizumab vs in Untreated Metastatic Renal Cell Carcinoma Patients David McDermott, 1 Michael Atkins, 2 Robert Motzer, 3 Brian Rini, 4 Bernard Escudier, 5 Lawrence
A Phase II Study of With or Without Bevacizumab vs in Untreated Metastatic Renal Cell Carcinoma Patients David McDermott, 1 Michael Atkins, 2 Robert Motzer, 3 Brian Rini, 4 Bernard Escudier, 5 Lawrence
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Innovaciones en el tratamiento del ca ncer renal. Enrique Grande
 Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients
 A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients Viktor Grünwald, 1 David McDermott, 2 Michael Atkins, 3 Robert Motzer, 4
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients Viktor Grünwald, 1 David McDermott, 2 Michael Atkins, 3 Robert Motzer, 4
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea
 Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Metastatic renal cancer (mrcc): Evidence-based treatment
: Evidence-based treatment") Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Medical Management of Renal Cell Carcinoma
 Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial
: Results of a phase I trial") Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
Checkpointinhibitoren in der Uro-Onkologie. Carsten Grüllich
 Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Renal Cell Cancer: Present and Future. Bernard Escudier, Gustave Roussy
 Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request Disclosures
Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request Disclosures
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game?
 Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care
 vs standard of care") A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
Sequencing of therapies in mrcc. Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC
 Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
New strategies and future of target therapy in advanced kidney cancer
 New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Linee guida terapeutiche oncologiche. Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona
 Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
The Therapeutic Landscape in Advanced Renal Cell Carcinoma
 The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
ESMO Madrid, Spain Associate Professor Brian Costello Division of Medical Oncology, Genitourinary Tumour Group, Mayo Clinic, USA
 ESMO 2017 - Madrid, Spain Associate Professor Brian Costello Division of Medical Oncology, Genitourinary Tumour Group, Mayo Clinic, USA HIGHLIGHTS ON RENAL CELL CARCINOMA CHECKMATE 214: EFFICACY AND SAFETY
ESMO 2017 - Madrid, Spain Associate Professor Brian Costello Division of Medical Oncology, Genitourinary Tumour Group, Mayo Clinic, USA HIGHLIGHTS ON RENAL CELL CARCINOMA CHECKMATE 214: EFFICACY AND SAFETY
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
Second - Line Debate: Axitinib
 Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Tratamiento adyuvante y neoadyuvante del cáncer renal en Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet.
 Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Treatment Algorithm and Therapy Management in mrcc. Manuela Schmidinger Medical University of Vienna Austria
 Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Why was HOPE 205 a Positive After Years of Negative Studies?
 Why was HOPE 205 a Positive After Years of Negative Studies? Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Why do we pursue combinations?
Why was HOPE 205 a Positive After Years of Negative Studies? Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Why do we pursue combinations?
Alternativas de Futuro en Cáncer Renal Enrique Grande
 Alternativas de Futuro en Cáncer Renal Enrique Grande Hospital Ramón y Cajal de Madrid The ncreasingly Challenging Field of mrcc Sorafenib (US 2005, EU 2006) 3,4 Sunitinib (US & EU 2006) 3,4 Early 1940s:
Alternativas de Futuro en Cáncer Renal Enrique Grande Hospital Ramón y Cajal de Madrid The ncreasingly Challenging Field of mrcc Sorafenib (US 2005, EU 2006) 3,4 Sunitinib (US & EU 2006) 3,4 Early 1940s:
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Media Release. Basel, 6 th February 2018
 Media Release Basel, 6 th February 2018 Phase III IMmotion151 study showed Roche's TECENTRIQ (atezolizumab) and Avastin (bevacizumab) reduced the risk of disease worsening or death by 26 percent in certain
Media Release Basel, 6 th February 2018 Phase III IMmotion151 study showed Roche's TECENTRIQ (atezolizumab) and Avastin (bevacizumab) reduced the risk of disease worsening or death by 26 percent in certain
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Kidney Cancer. Version February 6, NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines )
") NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Kidney Cancer Overall management of Kidney Cancer from diagnosis through recurrence is described in the full NCCN Guidelines for Kidney
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Kidney Cancer Overall management of Kidney Cancer from diagnosis through recurrence is described in the full NCCN Guidelines for Kidney
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapy for Genitourinary Cancers
 Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Advances in the Treatment of Renal Cell Carcinoma
 Advances in the Treatment of Renal Cell Carcinoma Developed in collaboration Learning Objectives Upon completion, participants should be able to: Identify patients with metastatic renal cell carcinoma
Advances in the Treatment of Renal Cell Carcinoma Developed in collaboration Learning Objectives Upon completion, participants should be able to: Identify patients with metastatic renal cell carcinoma
A Review in the Treatment Options for Renal Cell Cancer
 A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO
 REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Urothelial Cancers- New Strategies. Sandy Srinivas.MD Stanford University
 Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
17th ESO-ESMO Masterclass Clinical Oncology
 Metastatic Renal Cell Cancer: Evidence Based Treatment Manuela Schmidinger Medical University of Vienna, Austria Disclosures Honoraria for lectures or advisory boards from: Pfizer, Roche, BMS, Novartis,
Metastatic Renal Cell Cancer: Evidence Based Treatment Manuela Schmidinger Medical University of Vienna, Austria Disclosures Honoraria for lectures or advisory boards from: Pfizer, Roche, BMS, Novartis,
Brain mets under I.O.
 Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia
 Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia New target, new agent (James Brugarolas) Atezolizumab + Bevacizumab and PD-L1
Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia New target, new agent (James Brugarolas) Atezolizumab + Bevacizumab and PD-L1
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy for Kidney Cancer: Finally Center-Stage? Nizar M. Tannir, MD, FACP Professor and Deputy Chair GU Medical Oncology
 Immunotherapy for Kidney Cancer: Finally Center-Stage? Nizar M. Tannir, MD, FACP Professor and Deputy Chair GU Medical Oncology 2013: Breakthrough of the Year December 20, 2013 Why immunotherapy? Immune
Immunotherapy for Kidney Cancer: Finally Center-Stage? Nizar M. Tannir, MD, FACP Professor and Deputy Chair GU Medical Oncology 2013: Breakthrough of the Year December 20, 2013 Why immunotherapy? Immune
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Immunoterapia di 1 linea Evidenze e Prospettive Future
 Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
Will All Adjuvant Therapy Trials Be Negative in RCC?
 Will All Adjuvant Therapy Trials Be Negative in RCC? Tim Eisen Eleventh European International Kidney Cancer Symposium 29-30 April 2016 Crowne Plaza Barcelona Fira Center, Barcelona, Spain Tim Eisen -
Will All Adjuvant Therapy Trials Be Negative in RCC? Tim Eisen Eleventh European International Kidney Cancer Symposium 29-30 April 2016 Crowne Plaza Barcelona Fira Center, Barcelona, Spain Tim Eisen -
Carcinoma de Tiroide: Teràpies Diana
 Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Immunotherapy in GU Cancers. Dr Ravindran Kanesvaran Medical Oncologist National Cancer Centre Singapore
 Immunotherapy in GU Cancers Dr Ravindran Kanesvaran Medical Oncologist National Cancer Centre Singapore 1 Disclosures Speaker Bureau: Pfizer, J&J, Sanofi, Novartis, MSD Advisory Board/ Consultant: GSK,
Immunotherapy in GU Cancers Dr Ravindran Kanesvaran Medical Oncologist National Cancer Centre Singapore 1 Disclosures Speaker Bureau: Pfizer, J&J, Sanofi, Novartis, MSD Advisory Board/ Consultant: GSK,
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Media Release. Basel, 21 July 2017
 Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Second-line treatment for advanced NSCLC
 UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
Management of High Risk Renal Cell Carcinoma
 Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma
 for Metastatic Renal Cell Carcinoma") pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations
 Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration