Parathyroid Disease Scenarios for the Practicing Clinician. Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix
|
|
|
- Cecily Walton
- 5 years ago
- Views:
Transcription
1 Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix
2 Clinical Scenario-1 73 year man (BK) with hypercalcemia on routine labs Concerned about insomnia, fatigue, memory loss, polyuria, nocturia Denied other symptoms related to hypercalcemia No family history of hypercalcemia/hyperparathyroidism No medications that could cause hypercalcemia PMHx: Hepatitis B, CAD, HTN, HLD, chronic anemia, Barrett s eshophagitis PSHx: Inguinal hernia, cataract, prostatectomy
3 Clinical Scenario-1 Physical exam: Vitals: 6 feet, 207 lbs, BMI 28, BP 140/74, HR 84/min General: Overweight gentleman Neck: No goiter, no clinically palpable nodules/neck mass CVS: Rhythm is normal, no murmurs RS: No wheezing. Chest clear to auscultation Musculoskeletal: No kyphoscoliosis Abd: Soft, non tender, no organomegaly
4 Clinical Scenario-1
5 Clinical Scenario-1 What is the diagnosis? Mild, asymptomatic PTH-mediated hypercalcemia? What is the next step in management?
6 Clinical Scenario-1 DXA scan Lumbar 1.26 gm/cm 2 T-score 0.2 Femoral 1.10 gm/cm 2 T-score 0.0


7 Clinical Scenario-1 What next? With negative Sestamibi scan, would you refer patient to surgeon?


8 What next? Clinical Scenario-1 ULTRASOUND Right paratracheal density measuring 13 x 10 mm with teardrop hypoechoic shape and vascular branching pattern compatible with parathyroid adenoma
9 Clinical Scenario-1 Indications for surgery in primary hyperparathyroidism Serum Calcium 1 mg/dl > upper limit of normal T-score less than -2.5 at lumbar spine, total hip, femoral neck or distal 1/3 radius Vertebral fracture 24 hour urine calcium > 400 mg/day and increased stone risk by biochemical stone risk analysis Presence of nephrolithiasis, nephrocalcinosis Age < 50 years of age John P. Bilezikian, Maria Luisa Brandi, Richard Eastell, Shonni J. Silverberg, Robert Udelsman, Claudio Marcocci, and John T. Potts Jr
10 Clinical Scenario-1 On Oct 13 th 2015, patient underwent focused parathyroid exploration with parathyroidectomy of right lower parathyroid adenoma.
11 Pathology Clinical Scenario-1
12 Clinical Scenario-1 6 Month Labs Jan 2016 Total calcium ( mg/dl) 9.7 Ionized calcium ( mg/dl) 5.18 Intact PTH (15-65 pg/ml) 35
13
14 Clinical Scenario-2 73 year woman (MB) was diagnosed with Waldenstroms Macroglobulinemia (WM) and lymphoplasmacytic lymphoma in March 2006 Treated with plasmapheresis Progressed to non-hodgkin B-cell lymphoma IVIG Rx for neuropathy (hands, vocal cords, forehead) In remission until 2014 Relapse of WM in October 2014 Presented to us for evaluation in early 2015 for management of hypercalcemia
15 Clinical Scenario-2 Current symptoms: fatigue, constipation/diarrhea, nausea, abdominal cramps, shortness of breath Denied kidney stones, fractures Mother has osteoporosis Currently taking Vitamin D 5000 IU BID When she has a cold, she takes 30,000 IU BID for 2 days and reports that her cold gets better
16 Clinical Scenario-2 Jan 4th 2015 Total calcium ( mg/dl) 15.7 IgM ( mg/dl) 3155 IgG 266 Beta 2 microglobulin 12.1 Hemoglobin 10.2 Treated with IV fluids, calcitonin, diuretics, plasmapheresis
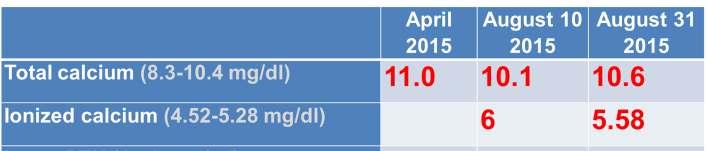
17 Clinical Scenario-2 Jan 9th 2015 Jan 22nd 2015 Total calcium ( mg/dl) Intact PTH (15-65 pg/ml) OH Vitamin D ( ng/ml) 96 1,25-OH Vitamin D (18-72 pg/ml) 179 Creatinine, Serum ( mg/dl) 1.85
18 Clinical Scenario-2 Diagnosis: Non PTH-mediated hypercalcemia Hypercalcemia due to vitamin D toxicity and increased 1,25 dihydroxy vitamin D
19 Clinical scenario-2 Feb 2015 Total calcium ( mg/dl) 13.1 Intact PTH (15-65 pg/ml) 9 25-OH Vitamin D ( ng/ml) 66 1,25-OH Vitamin D (18-72 pg/ml) >200 Creatinine, Serum ( mg/dl) 1.14 IgM ( mg/dl) 3000
20 Clinical Scenario-2 What next? Non PTH-mediated hypercalcemia Hypercalcemia due to continued high level of 1,25 dihydroxy vitamin D STEROIDS: Patient refused
21 Clinical Scenario-2 What next? Oncologist treated patient with IBRUTINIB Total calcium ( mg/dl) 9.6 Intact PTH (15-65 pg/ml) OH Vitamin D ( ng/ml) 50 1,25-OH Vitamin D (18-72 pg/ml) 60 April 2015 Creatinine, Serum ( mg/dl) 1.1 IgM ( mg/dl) 693
22 Summary Clinical Scenario-2 Non PTH-mediated hypercalcemia Hypercalcemia due to increased level of 1,25 dihydroxy vitamin D due to lymphoma After Rx with Ibrutinib, calcium normalized, IgM levels improved, lymphoma was better controlled




23
24 Clinical Scenario-3 65 year old woman (ML) was found to have serum calcium level of 15 mg/dl in routine evaluation and referred to an endocrinologist for evaluation She was recently diagnosed with stage 1 invasive ductal breast cancer Symptoms of hypercalcemia: GERD, osteoporosis. Patient denied other symptoms of hypercalcemia. No family history of hypercalcemia/hyperparathyroidism Patient was taking hydrochlorothiazide
25 Clinical Scenario-3 PMHx: Anxiety, HTN, obesity PSHx: Cholecystectomy, TAH with BSO, resection of colon polyp Social Hx: Single, no hx of tobacco, recreational drug use. Drinks wine 5 times/week. One child.
26 Physical exam: Clinical Scenario-3 General: Obese lady Neck: No goiter, no clinically palpable nodules, neck masses CVS: Rhythm is normal, no murmurs RS: No wheezing, chest clear to auscultation Musculoskeletal: No kyphoscoliosis Abd: Soft, non tender, no organomegaly

27 Clinical Scenario-3


28 Clinical scenario-3 DXA done in 2015 Lumbar 0.84 gm/cm 2 T-score -2.9 Femoral gm/cm 2 T-score -2.0
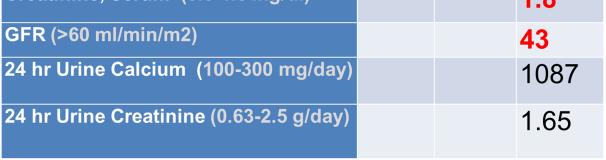
29 Clinical scenario-3 What is the diagnosis? Severe, symptomatic PTH-mediated hypercalcemia What is the next step in management?

30 Sestamibi scan Clinical scenario-3

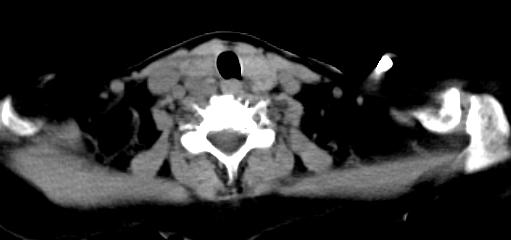
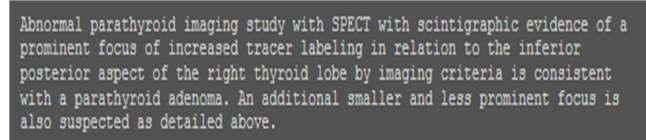
31 Clinical scenario-3


32 Clinical scenario-3 ULTRASOUND of thyroid/parathyroid glands
33 Clinical scenario-3 In July 2016, patient underwent focused parathyroidectomy with excision of right inferior parathyroid adenoma that was located in retroesophageal area. Date Baseline PTH (12-88 pg/ml) PTH in 10 minutes Calcium ( mg/dl)

34 Clinical scenario-3 14,700 mg adenoma (normal parathyroid weight 30 mg)


35 Thank You
Endocrinologist - Surgeon: Critical Collaboration with Case-Based Conversations
 Endocrinologist - Surgeon: Critical Collaboration with Case-Based Conversations Chairs: Jeffrey Garber MD and Mira Milas MD W32: Pre-Congress Session II Endocrinologists and Surgeons Mira Milas MD Banner-U
Endocrinologist - Surgeon: Critical Collaboration with Case-Based Conversations Chairs: Jeffrey Garber MD and Mira Milas MD W32: Pre-Congress Session II Endocrinologists and Surgeons Mira Milas MD Banner-U
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
76 year-old female presents with muscle cramps. Jess Hwang 12/6/12
 76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
4/20/2015. The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy. Learning Objectives
 Testing During Surgical Parathyroidectomy. Learning Objectives") The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Primary Hyperparathyroidism
 Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP
 Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
Targeted Issues in Endocrinology Joshua S. Coren, DO, MBA, FACOFP Endocrine in 25 Minutes Joshua S. Coren, D.O., MBA, FACOFP Vice Chair and Associate Professor, Family Medicine Rowan University School
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
Thyroid and Parathyroid Disease. RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010
 Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Case study Group 2 presentation
 Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
CASE-BASED SMALL GROUP DISCUSSION. MHD II Session VII. Friday, March 28, 2014 STUDENT COPY
 CASE-BASED SMALL GROUP DISCUSSION MHD II Session VII Friday, March 28, 2014 STUDENT COPY Helpful resources ACP Medicine available online through Loyola Health Science Library Endocrinology and Metabolism
CASE-BASED SMALL GROUP DISCUSSION MHD II Session VII Friday, March 28, 2014 STUDENT COPY Helpful resources ACP Medicine available online through Loyola Health Science Library Endocrinology and Metabolism
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Talking to patients with osteoporosis about initiating therapy
 Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
38 year old Male with Ankylosing Spondylitis. Olesya Krivospitskaya, MD April,
 38 year old Male with Ankylosing Spondylitis Olesya Krivospitskaya, MD April, 11 2013 HPI (Letter from the patient): Diagnosed with Ankylosing Spondylitis and prescribed a Sulfa drug to help with my back
38 year old Male with Ankylosing Spondylitis Olesya Krivospitskaya, MD April, 11 2013 HPI (Letter from the patient): Diagnosed with Ankylosing Spondylitis and prescribed a Sulfa drug to help with my back
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine
 Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
Shon E. Meek, M.D., Ph.D. Assistant Professor of Medicine meek.shon@mayo.edu 2016 MFMER 3561772-1 Update on Vitamin D Shon Meek MD, PhD 20 th Annual Endocrine Update January 30-Feb 3, 2017 Disclosure Relevant
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand
 International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
Minimally invasive parathyroidectomy
 Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
Since the advent of multichannel serum chemistry
 ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
ONLINE EXCLUSIVE Padmaja Sanapureddy, MD; Vishnu Vardhan Garla, MD; Mallikarjuna Reddy Pabbidi, DVM, PhD Department of Primary Care and Medicine, G.V. (Sonny) Montgomery VA Medical Center, Jackson, Miss
Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma
 ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
ISPUB.COM The Internet Journal of Internal Medicine Volume 6 Number 2 Radiographic Appearance Of Primary Hyperparathyroidism With Atypical Parathyroid Adenoma P George, N Philip, B Pawar Citation P George,
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Cases in Endocrinology
 Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Vijaya Chockalingam, MD Faculty Endocrinologist Banner University Medical Group-Phoenix April 19th 2016
 Vijaya Chockalingam, MD Faculty Endocrinologist Banner University Medical Group-Phoenix April 19th 2016 Osteoporosis- Review of 2 cases Case: C.T. H & P 86 year old consulted for management of osteoporosis
Vijaya Chockalingam, MD Faculty Endocrinologist Banner University Medical Group-Phoenix April 19th 2016 Osteoporosis- Review of 2 cases Case: C.T. H & P 86 year old consulted for management of osteoporosis
When the level of calcium in the blood falls too low, the parathyroid glands secrete just enough PTH to restore the blood calcium level.
 Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
PRIMARY HYPERPARATHYROIDISM WITH RICKETS. KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College
 PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
PRIMARY HYPERPARATHYROIDISM WITH RICKETS KRITHIKA.P Dr.L.N.Padmasani Unit 1 Sri Ramachandra Medical College Presenting Complaints v 17 year old developmentally normal adolescent boy, first of a twin pregnancy,
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Hypercalcemia. Brian Rose, M.D. Bozeman Health June 6, 2018
 Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Hypercalcemia Brian Rose, M.D. Bozeman Health June 6, 2018 Hypercalcemia Diagnosis PTH Mediated Primary Hyperparathyroidism Lithium Familial Hypocalciuric Hypercalcemia Non PTH mediated Malignancy Humoral
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Diagnosis and Treatment of Primary Hyperparathyroidism. Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic
 Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic Disclosure Nothing to Disclose Primary HPT Autonomous secretion of
Hyperparathyroidism (primary): diagnosis, assessment and initial management
: diagnosis, assessment and initial management") National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
Rajesh Jain MD Endorama
 50 F with history of duodenal switch presenting for low BMD Rajesh Jain MD Endorama HPI 50 F presenting with low BMD referred by PCP She has a history of malnutrition following duodenal switch procedure
50 F with history of duodenal switch presenting for low BMD Rajesh Jain MD Endorama HPI 50 F presenting with low BMD referred by PCP She has a history of malnutrition following duodenal switch procedure
The most current assessment of this problem can be found in the Apex note dated
 Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Acute renal failure and unknown cause hypercalcemia (case report)
") Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
Acute renal failure and unknown cause hypercalcemia (case report) Clinic for hemodialysis CCU Sarajevo ... What is hypercalcemia??? ... What is hypercalcemia??? The definition of hypercalcemia is having
GASTROENTEROLOGY PATIENT QUESTIONNAIRE - PLEASE PRINT
 GASTROENTEROLOGY PATIENT QUESTIONNAIRE - PLEASE PRINT Full name: Date: Telephone Number: Age: Address: Email address: CHIEF COMPLAINTS(List the problems about which you came to see the doctor) 1) 2) 3)
GASTROENTEROLOGY PATIENT QUESTIONNAIRE - PLEASE PRINT Full name: Date: Telephone Number: Age: Address: Email address: CHIEF COMPLAINTS(List the problems about which you came to see the doctor) 1) 2) 3)
Challenges in the Management of Primary HPTH. Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH
 Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
HPI joint pain/arthritis serum calcium 11.5 PTH 147pg/ml
 HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
2 Year old Girl with Severe Hypercalcemia. March 7, 2013 Matt Wise, MD All ages
 2 Year old Girl with Severe Hypercalcemia March 7, 2013 Matt Wise, MD All ages HPI 2y3m caucasian girl presents to OSH ER with 1 day of fever to 102, vomiting, increased tiredness Several weeks of excess
2 Year old Girl with Severe Hypercalcemia March 7, 2013 Matt Wise, MD All ages HPI 2y3m caucasian girl presents to OSH ER with 1 day of fever to 102, vomiting, increased tiredness Several weeks of excess
Treatment of Waldenström s Macroglobulinemia Mayo Consensus
 Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
UPDATES ON PRIMARY HYPERPARATHYROIDISM. Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY
 UPDATES ON PRIMARY HYPERPARATHYROIDISM Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY Disclosures Speaker (Honorarium): Shire Off-label use of estrogen, raloxifene
UPDATES ON PRIMARY HYPERPARATHYROIDISM Natalie E. Cusano, MD, MS Director, Bone Metabolism Program Lenox Hill Hospital New York, NY Disclosures Speaker (Honorarium): Shire Off-label use of estrogen, raloxifene
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
73 year-old Female with Hypercalcemia
 73 year-old Female with Hypercalcemia Katie O Sullivan, M.D. Fellow, Adult/Pediatric Endocrinology University of Chicago Thursday, December 19 th, 2013 Chief Complaint 73 year-old female who presents for
73 year-old Female with Hypercalcemia Katie O Sullivan, M.D. Fellow, Adult/Pediatric Endocrinology University of Chicago Thursday, December 19 th, 2013 Chief Complaint 73 year-old female who presents for
AMSER Rad Path Case of the Month: December 2018
 AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
MHD II, Session X, STUDENT Copy Page 1 ENDOCRINOLOGY CASE-BASED SMALL GROUP DISCUSSION SESSION X MHD II. April 2, 2015 STUDENT COPY
 MHD II, Session X, STUDENT Copy Page 1 ENDOCRINOLOGY CASE-BASED SMALL GROUP DISCUSSION SESSION X MHD II April 2, 2015 STUDENT COPY MHD II, Session X, STUDENT Copy Page 2 CASE 1 History: A 35 year-old woman
MHD II, Session X, STUDENT Copy Page 1 ENDOCRINOLOGY CASE-BASED SMALL GROUP DISCUSSION SESSION X MHD II April 2, 2015 STUDENT COPY MHD II, Session X, STUDENT Copy Page 2 CASE 1 History: A 35 year-old woman
J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health
 J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health Patient Clinical Information Questionnaire 1.0 Date of Questionnaire Completion; / / 2.0 Patient Data 2.1 Name:
J. Van Lier Ribbink, M.D., F.A.C.S. Center for Endocrine and Pancreas Surgery at Honor Health Patient Clinical Information Questionnaire 1.0 Date of Questionnaire Completion; / / 2.0 Patient Data 2.1 Name:
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
301 S. Westfield Rd., Suite 250 Madison, WI See inside for information about our Endocrine Surgery Referral Program
 301 S. Westfield Rd., Suite 250 Madison, WI 53717 See inside for information about our Endocrine Surgery Referral Program December 2017 Dear Colleague, Thank you for referring your patient(s) to UW Health
301 S. Westfield Rd., Suite 250 Madison, WI 53717 See inside for information about our Endocrine Surgery Referral Program December 2017 Dear Colleague, Thank you for referring your patient(s) to UW Health
PTH > 60pg/ml PRIMARY HYPERPARATHYROIDISM. Introduction Biochemical Diagnosis. Normal Parathyroid. Parathyroid Glands
 next speaker: Declan Neeson Belfast/UK SPECT/CT scanning and parathyroid surgery in Southern Trust, N. Ireland D Neeson M Korda, G Gray, C Leonard, M Fawzy, R Lambon Parathyroid Glands PRIMARY HYPERPARATHYROIDISM
next speaker: Declan Neeson Belfast/UK SPECT/CT scanning and parathyroid surgery in Southern Trust, N. Ireland D Neeson M Korda, G Gray, C Leonard, M Fawzy, R Lambon Parathyroid Glands PRIMARY HYPERPARATHYROIDISM
Patient Interview Form
 Patient Interview Form Patient Information First Name: Last Name: Date of Birth: Age: Email Personal: Race Select one or more Referring Physician White Black or African Asian American Indian Native Hawaiian
Patient Interview Form Patient Information First Name: Last Name: Date of Birth: Age: Email Personal: Race Select one or more Referring Physician White Black or African Asian American Indian Native Hawaiian
Parathyroidectomy. Surgery for Parathyroid Problems
 Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century
 Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century John P. Bilezikian, John T. Potts, Jr., Ghada El-Hajj Fuleihan, Michael Kleerekoper, Robert
Summary Statement from a Workshop on Asymptomatic Primary Hyperparathyroidism: A Perspective for the 21st Century John P. Bilezikian, John T. Potts, Jr., Ghada El-Hajj Fuleihan, Michael Kleerekoper, Robert
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Patient History Form
 Patient History Form Advanced Directive Care Plan? Yes No Name: Birth date: / / Address: Age: Sex: F M STREET DAY YEAR Telephone: Home ( ) CITY STATE DAY YEAR MARITAL STATUS: Divorced Separated Alive/Age
Patient History Form Advanced Directive Care Plan? Yes No Name: Birth date: / / Address: Age: Sex: F M STREET DAY YEAR Telephone: Home ( ) CITY STATE DAY YEAR MARITAL STATUS: Divorced Separated Alive/Age
Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease?
 Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
Elena Castellano, Roberto Attanasio, Laura Gianotti, Flora Cesario, Francesco Tassone, and Giorgio Borretta
 ORIGINAL ARTICLE Forearm DXA Increases the Rate of Patients With Asymptomatic Primary Hyperparathyroidism Meeting Surgical Criteria Elena Castellano, Roberto Attanasio, Laura Gianotti, Flora Cesario, Francesco
ORIGINAL ARTICLE Forearm DXA Increases the Rate of Patients With Asymptomatic Primary Hyperparathyroidism Meeting Surgical Criteria Elena Castellano, Roberto Attanasio, Laura Gianotti, Flora Cesario, Francesco
Calcium and Parathyroid Disorders
 Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
Calcium and Parathyroid Disorders Hussain Mahmud, MD Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism University of Pittsburgh Butler Memorial Hospital November
28 yo F w/esrd with a facial deformity
 28 yo F w/esrd with a facial deformity Jess Hwang Endocrinology fellow 1/30/14 History of renal failure-- 2005 Woke up blind one day At the hospital she was told she was 4 months pregnant Diagnosed with
28 yo F w/esrd with a facial deformity Jess Hwang Endocrinology fellow 1/30/14 History of renal failure-- 2005 Woke up blind one day At the hospital she was told she was 4 months pregnant Diagnosed with
Primary Hyperparathyroidism
 November 2002 Primary Hyperparathyroidism Lori Coburn, Harvard Medical School Year III Hyperparathyroidism An increase in parathyroid hormone (PTH) production Divided into Primary, Secondary and Tertiary
November 2002 Primary Hyperparathyroidism Lori Coburn, Harvard Medical School Year III Hyperparathyroidism An increase in parathyroid hormone (PTH) production Divided into Primary, Secondary and Tertiary
Calcium Nephrolithiasis and Bone Health. Noah S. Schenkman, MD
 Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Parathyroid Imaging What is best
 Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
MHD II, Session 9, STUDENT Copy Page 1 ENDOCRINOLOGY CASE-BASED SMALL GROUP DISCUSSION SESSION 9 MHD II. March 29, 2017 STUDENT COPY
 MHD II, Session 9, STUDENT Copy Page 1 ENDOCRINOLOGY CASE-BASED SMALL GROUP DISCUSSION SESSION 9 MHD II March 29, 2017 STUDENT COPY MHD II, Session 9, STUDENT Copy Page 2 CASE 1 History: A 57-year-old
MHD II, Session 9, STUDENT Copy Page 1 ENDOCRINOLOGY CASE-BASED SMALL GROUP DISCUSSION SESSION 9 MHD II March 29, 2017 STUDENT COPY MHD II, Session 9, STUDENT Copy Page 2 CASE 1 History: A 57-year-old
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
PLAS/RECON SURGERY PATIENT HEALTH HISTORY
 PLAS/RECON SURGERY PATIENT HEALTH HISTORY Chief Complaint - Please describe the problem that brings you into the office today: Allergies 1. Do you have any allergies? if so, please list To Medications?
PLAS/RECON SURGERY PATIENT HEALTH HISTORY Chief Complaint - Please describe the problem that brings you into the office today: Allergies 1. Do you have any allergies? if so, please list To Medications?
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
Patient Name: Date of Birth: Date of Visit (Today s Date): Date of Injury (if applicable): Occupation: Right or Left Handed: Referring Provider:
: Date of Injury (if applicable): Occupation: Right or Left Handed: Referring Provider:") New Patient History & Intake Form Patient Information Patient Name: Date of Birth: Date of Visit (Today s Date): Date of Injury (if applicable): Occupation: Right or Left Handed: Referring Provider: Preferred
New Patient History & Intake Form Patient Information Patient Name: Date of Birth: Date of Visit (Today s Date): Date of Injury (if applicable): Occupation: Right or Left Handed: Referring Provider: Preferred
2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT)
") 2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT) Scott M. Wilhelm, MD, FACS Associate Professor and Section Head Endocrine Surgery University Hospitals-Cleveland
2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT) Scott M. Wilhelm, MD, FACS Associate Professor and Section Head Endocrine Surgery University Hospitals-Cleveland
REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care. Reddy Urgent Care Pre-Employment Physical Form
 REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care 132 Franklin Springs St. 1061 Dowdy Road STE 100 280 General Daniels Ave. Royston, GA 30662 Athens, GA 30606 Danielsville, GA 30633
REDDY & ASSOCIATES LLC D/B/A Reddy Medical Group D/B/A Reddy Urgent Care 132 Franklin Springs St. 1061 Dowdy Road STE 100 280 General Daniels Ave. Royston, GA 30662 Athens, GA 30606 Danielsville, GA 30633
Case 4 Generalised bone pain
 Case 4 Generalised bone pain C A 34- year- old woman presented complaining of multifocal pain in her chest and legs. The pain was intermittent, was aggravated by weight bearing. Initially was alleviated
Case 4 Generalised bone pain C A 34- year- old woman presented complaining of multifocal pain in her chest and legs. The pain was intermittent, was aggravated by weight bearing. Initially was alleviated
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
CONCORD INTERNAL MEDICINE VITAMIN D/CALCIUM/MAGNESIUM PROTOCOL. Revised April 8, 2012
 CONCORD INTERNAL MEDICINE VITAMIN D/CALCIUM/MAGNESIUM PROTOCOL Douglas G. Kelling, Jr., ND C. Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised April 8, 2012 The information contained in this
CONCORD INTERNAL MEDICINE VITAMIN D/CALCIUM/MAGNESIUM PROTOCOL Douglas G. Kelling, Jr., ND C. Gismondi-Eagan, MD, FACP George C. Monroe, III, MD Revised April 8, 2012 The information contained in this
Original Research Article
 Medrech ISSN No. 2394-3971 Original Research Article TYPE 2 DIABETES WITH RECURRENT OSTEOPOROTIC FRACTURES, OR CUSHING S SYNDROME? Blertina Dyrmishi¹*; Taulant Olldashi²; Prof Asc Thanas Fureraj 3 ; Prof
Medrech ISSN No. 2394-3971 Original Research Article TYPE 2 DIABETES WITH RECURRENT OSTEOPOROTIC FRACTURES, OR CUSHING S SYNDROME? Blertina Dyrmishi¹*; Taulant Olldashi²; Prof Asc Thanas Fureraj 3 ; Prof
New Patient Form. Patient Demographics. Emergency Information. Employment Information. Page 1 of 7. Family Health Chiropractic Care
 Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Page 1 of 7 Patient Demographics First Name* Last Name* Date Of Birth* Home Phone* Mobile Phone Phone Gender* Email Preferred Communication Street Address 1* Street Addresss 2 Zip* City* State* Emergency
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease
 Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor
 Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
DATE OF BIRTH: MELANOMA INTAKE
 MELANOMA INTAKE GENERAL INFORMATION How was your first diagnosed? (Check the diagnosis that describes your condition.) Melanoma Merkel Cell Carcinoma Squamous Cell Carcinoma Basal Cell Carcinoma Other
MELANOMA INTAKE GENERAL INFORMATION How was your first diagnosed? (Check the diagnosis that describes your condition.) Melanoma Merkel Cell Carcinoma Squamous Cell Carcinoma Basal Cell Carcinoma Other
All Other Medications, Dose Times per day Reason for taking the medication. Phone #
 Patient Name: Date of Birth: _ Medical Record Number: Mailing Address: PO Box 29086 Thornton, CO 80229 Phone: 720.215.0700 Fax: 877.332.3131 Allergies Do you have Allergies Yes No If yes, please complete
Patient Name: Date of Birth: _ Medical Record Number: Mailing Address: PO Box 29086 Thornton, CO 80229 Phone: 720.215.0700 Fax: 877.332.3131 Allergies Do you have Allergies Yes No If yes, please complete
Hypercalcemia may be detected incidentally. Practice CMAJ. Primary hyperparathyroidism. Primer. Key points. The case. What causes hypercalcemia?
 CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
CMAJ Practice Primer Primary hyperparathyroidism Hafsah Al-Azem HBSc, Aliya Khan MD The case A 17-year-old man presented at the clinic with thirst, lethargy and fatigue that had been ongoing for several
Patient Name Date of Birth Age. Other phone ( ) . Other
 . Other") GASTROINTESTINAL & MINIMALLY INVASIVE SURGERY HEALTH HISTORY QUESTIONNAIRE Date Patient Name _ Date of Birth Age Daytime phone ( ) Other phone ( ) Email How did you hear about us? My doctor Yellow pages
GASTROINTESTINAL & MINIMALLY INVASIVE SURGERY HEALTH HISTORY QUESTIONNAIRE Date Patient Name _ Date of Birth Age Daytime phone ( ) Other phone ( ) Email How did you hear about us? My doctor Yellow pages
Screening tests. When you need them and when you don t
 Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
PATIENT INFORMATION Last Name: First Name: Middle: Date of Birth: EMERGENCY CONTACT INFORMATION PRIMARY INSURANCE INFORMATION
 PATIENT INFORMATION Last Name: First Name: Middle: Date of Birth: Gender: SSN: Race: Marital Status: Address Line: City: State: Zip Code: Home Phone: Work Phone: Email Address: Cell Phone: Primary Care
PATIENT INFORMATION Last Name: First Name: Middle: Date of Birth: Gender: SSN: Race: Marital Status: Address Line: City: State: Zip Code: Home Phone: Work Phone: Email Address: Cell Phone: Primary Care
Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary Referral Population
 Pierreux Jan, Bravenboer Bert. Normocalcemic Primary Hyperparathyroidism: A Horm Metab Res 2018; 00: 00 00 Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary
Pierreux Jan, Bravenboer Bert. Normocalcemic Primary Hyperparathyroidism: A Horm Metab Res 2018; 00: 00 00 Normocalcemic Primary Hyperparathyroidism: A Comparison with the Hypercalcemic Form in a Tertiary
Calcium Conundrums. California Chapter AACE. September 2015
 Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA www.endocrinesurgery.ucla.edu
Calcium Conundrums California Chapter AACE September 2015 Michael W. Yeh, MD Chief, Section of Endocrine Surgery Associate Professor of Surgery and Medicine David Geffen School of Medicine at UCLA www.endocrinesurgery.ucla.edu
Primary hyperparathyroidism
 How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
Primary Hyperparathyroidism, 2018: A Comprehensive Update
 Primary Hyperparathyroidism, 2018: A Comprehensive Update John P. Bilezikian, MD, PhD(hon) Silberberg Professor of Medicine Vice-Chair for International Education and Research Chief, Division of Endocrinology,
Primary Hyperparathyroidism, 2018: A Comprehensive Update John P. Bilezikian, MD, PhD(hon) Silberberg Professor of Medicine Vice-Chair for International Education and Research Chief, Division of Endocrinology,
NEUROSURGERY PATIENT INTAKE FORM
 NEUROSURGERY PATIENT INTAKE FORM Surgical Movement Disorders Center Name: DOB: / / Age: Gender: Male Female (circle one) Height: feet inches Weight: lbs What is the main reason for your visit? Are there
NEUROSURGERY PATIENT INTAKE FORM Surgical Movement Disorders Center Name: DOB: / / Age: Gender: Male Female (circle one) Height: feet inches Weight: lbs What is the main reason for your visit? Are there