Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children s Hospital
|
|
|
- Leo Stephens
- 5 years ago
- Views:
Transcription
1 Attention Deficit Hyperactivity Disorder: an update on biological risk factors and a pharmacological treatment approach Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children s Hospital
2 Outline of presentation 1. ADHD: definition 2. ADHD: Key biological risk factors 3. A model for intervention 4. A medication approach (Australian perspective)


3
4 1. ADHD: definition Diagnostic nosology-some comments: DSM-IV definition of a mental disorder- A mental disorder is conceptualized as a clinically significant behavioural pattern that occurs in an individual and is associated with impairment in one or more areas of functioning
5 1. ADHD: definition Diagnostic nosology-some comments in children and adolescentsimpairment is developmentally inappropriate, judged relative to children of the same age, gender and IQ in social, academic, occupational or other important areas of functioning multi-informant reports required
6 1. ADHD: definition Attention Deficit Hyperactivity Disorder (ADHD) DSM-IV CRITERIA -six or more symptoms, at least six months duration, maladaptive/inconsistent with developmental level -inattention dimension and/or hyperactivity-impulsivity dimension -evident in at least two settings -onset before seven years of age -impairment in social, academic, occupational functioning -symptoms not due to a PDD, Psychotic, Mood, or Anxiety Disorder
7 1. ADHD: definition TYPES of ADHD -combined type -predominantly inattentive type -predominantly hyperactive-impulsive type
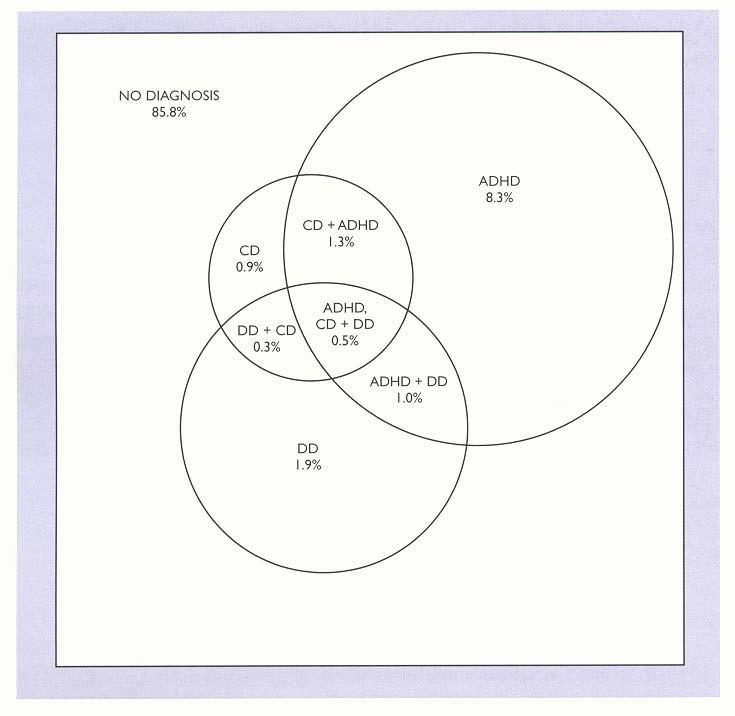
8 1. ADHD: definition Key comorbid conditions: -tic disorders -oppositional defiant disorder/conduct disorder -anxiety and/or depressive disorders -language learning disorders (spelling/reading/arithmetic/writing) -speech and language disorders (articulation/grammar) -developmental coordination disorder
9
10 1. ADHD: definition Common possible developmental pathways: all associated with educational, social, occupational under-achievement, alcohol/ substance abuse/dependence disorders, altered adult personality childhood adolescence adulthood ADHD-CT ADHD-IA ADHD-IA ADHD-CT Depressive d Depressive d ADHD-CT Conduct d ASPD
11 Healthy ADHD ADHD 2. ADHD: Key biological risk factors d = 1.0 d =0.5 Biological risk factors Psychosocial risk factors
12 2. ADHD: Key biological risk factors Genetics: -heritability estimates 65%-90% phenotypic variance in population Studies OR -DAT1 10-repeat allele, N= DRD4 7-repeat allele, N= Taq1 polymorphism DBH, N= SNAP-25 gene N= HT1B N=3 1.44
13 2. ADHD: Key biological risk factors - Cognitive deficits in ADHD are associated with these key candidate genes: Healthy children: DAT1 3 VNTR 10-repeat allele DAT1 intron 8 VNTR 3-repeat allele R spatial inattention DAT1 3 UTR VNTR 10-repeat allele (η 2 =.07/.08/.08) - this 10/3DAT1 haplotype ADHD (OR 2.58)
14 2. ADHD: Key biological risk factors Neuroimaging -structural MRI: prefrontal cortex, basal ganglia, medial temporal and inferior parietal lobes (global 3% decrease) primarily white matter (d=.45 cf.28 gray matter) developmental trajectories independent of medication treatment
 Castellanos et al.")
15 Total cerebral growth curves 1100 Controls > ADHD p<.003 m L Age (y) Castellanos et al., JAMA 2002 NV Males ADHD Males NV Females ADHD Females
16 2. ADHD: Key biological risk factors Neuroimaging -functional MRI: prefrontal cortex, basal ganglia, medial temporal and inferior parietal lobes bilateral task dependent decrease in activation post-puberty - midline activation - compensatory? pre-puberty - not evident

17 Regions under-activated in ADHD Silk, Vance, et al., Br J Psychiatry, 2005

18 Regions over-activated in ADHD Silk, Vance, et al., Br J Psychiatry, 2005

19 Vance et al., Mol. Psychiatry 2007
20 2. ADHD: Key biological risk factors Cognitive neuroscience response inhibition tasks (eg STOP tasks) working memory tasks (eg n-back; VSWM tasks) deficits in both implicating PFC-striatal and PFC-striatal-parietal neural networks investigated as markers for medication response in children with ADHD
21 2. ADHD: Key biological risk factors Cognitive neuroscience working memory (Mehta et al., 2000) PET VSWM task 10 healthy adult males 2 sessions 2W apart MPD 40mg or placebo with scanning 90+ minutes later rcbf -left DLPFC, left SMA, left PPC associated with improved VSWM performance
22 2. ADHD: Key biological risk factors Cognitive neuroscience selective attention/working memory (Bush et al., 2008) fmri MSIT 21 adults ADHD RCT 6 weeks OROs-MPD or placebo damcc associated with improved performance
23 2.ADHD: Key biological risk factors Behavioural z-composite score e composit 2.5 r 2 = Behavioural z- score Cognitive z-composite score r 2 = Cognitive z-composite score Composite z-scores ADHD children in the low dose and high dose Condition (dex. 2.5mg/ 7.5mg) (Mollica et al., Human Psychopharmacology 2004)
24 2. ADHD: Key biological risk factors Summary - biological factors important - small effect: candidate genes - medium effect: candidate genes- CogNS measures; brain structural/functional changes - large effect: CogNS constructs - developmental stage-independent deficits - compensatory changes post-puberty - medication changes non-specific currently
25
26


27
28 3. A model for intervention -assessment and treatment focuses on delineation of risk factors and resilience factors-biologically (eg, executive function deficits; good arousal regulation) psychologically (eg, externalise blame; balanced critical self-reflection) and socially (eg, hostile critical interpersonal environment; confiding, nurturing consistent interpersonal environment) -monitoring of these risk and resilience factors and their response to treatment through developmental phases
29 3. A model for intervention -a practical approach [A] psychological and social treatment approach implemented for 4-6 weeks (may take 6 months of new habit formation before sustained behavioural change) key elements are the interpersonal and the intra-individual milieu interpersonal: positive reinforcement, response cost, token economy, contingency planning (turn taking, active listening, active ignoring, empathy skills, etc), making and keeping friends intra-individual: controlled breathing, muscle biofeedback, guided visual imagery
30 3. A model for intervention - a practical approach [B] key other vulnerabilities addressed vision, hearing, specific verbal and/or visuospatial learning difficulties, developmental coordination difficulties, speech and language difficulties
31 3. A model for intervention a practical approach [C] medication use to facilitate availability of the young person to learn from the psychological and social interventions through better arousal regulation better mood regulation better executive functioning
32 3. A model for intervention Summary - medication can aid a child s ability to invest in a psychosocial treatment program and learn from this program - can take 6 months of practice before new habits are formed - biological and psychosocial treatments maximize resilience and minimize risk factors through shared effects on the brain and the mind
33 4. A medication approach (Australian perspective) - stimulant medication is the first line treatment short-acting forms: methylphenidate, dexamphetamine long-acting forms: OROS-methylphenidate, LA-methylphenidate clear and substantial evidence for methylphenidate efficacy up to a dose of 60mg daily for treatments periods of approximately 12 months methylphenidate and dexamphetamine similar efficacy and adverse effects profile although individual preferences manifest
34 4. A medication approach (Australian perspective) - Stimulant medication benefits decrease core symptoms of ADHD decrease aggression increase quality of social interactions increase compliance - Stimulant medication indications ADHD diagnosis and psychosocial interventions insufficient
35 4. A medication approach (Australian perspective) - Stimulant medication adverse effects initial insomnia, appetite suppression nervousness, restlessness, dysphoria, easy crying, agitation, depressive symptoms, stomach ache headache, dizziness, rash, motor tics, mannerisms in overdose: delirium, sweating, tremor, twitching, vomiting
36 4. A medication approach (Australian perspective) - Stimulant medication adverse effects growth retardation (MTA 3y f/u: 2cm /2.7kg ) weight loss epileptic seizures psychotic episodes abuse potential not adverse effects but careful monitoring needed in vulnerable patients
37 Different efficacy between short-acting and long-acting forms of methylphenidate 50% 40% *P<0.05 **P=0.001 completed improvement rate (SNAP-IV) 30% 20% 10% 0% methylphenidate Tid methylphenidate Bid OROS-methylphenidate Steele et al. Can J Clin Pharmacol 2006; 13:e50-62.
38 Stimulant medication benefits: OROS-methylphenidate improve Cognition Note: CPT=Continuous Performance Test; RT=response time; MFFT=Matching Familiar Figure Test; VFT=Verbal Fluency Test; TMT=Trail Making Test;CTT=Color Trail Test; CTT Index=(time to completion of Trail B time to completion of Trail A)/ time to completion of Trail A; SD=standard deviation. ***p<0.001, **p<0.01, *p<0.05, baseline to end of study change. Lee et al., Prog Neuropsychopharmacol Biol Psychiatry. 2007; 30:

39 Outcome of CONCERTA vs Atomoxetine Kemner et al. Advances in Therapy 2005; 22:
40 OROS-methylphenidate effect on growth Absolute height (cm) Absolute weight (kg) Treatment time (month) Treatment time (month) Spencer et al., J.AM.ACAD.CHILD ADOLESC. PSYCHIATRY 2006; 45:
41 4. A medication approach (Australian perspective) - Atomoxetine is the second line treatment specific potent noradrenaline re-uptake inhibitor indicated when stimulant medication ineffective, associated with significant adverse effects common adverse effects: nausea, drowsiness, initial insomnia, appetite suppression
42 4. A medication approach (Australian perspective) - Imipramine is a third line treatment tricyclic compound similar to atomoxetine (a phenylpropanolamine derivative) but with less specific noradrenaline effect and significant cardiac adverse effects - Clonidine is a third line treatment central α-2 noradrenergric agonist significant effect; primarily hyperactivity/impulsiveness significant drowsiness, hypotensive and cardiac adverse effects gradual withdrawal because of rebound hypertension and tics
43 4. A medication approach (Australian perspective) - Neuroleptic medication is a third line treatment atypical neuroleptic medication: eg risperidone / aripiprazole low doses (up to risperidone 1.5mg daily equivalent) severe aggression, affective lability, PDD, ID typical neuroleptic medication: eg pericyazine - thioridazine equivalent (now withdrawn) third line treatments only used with careful monitoring and involvement in a treatment-resistant unit
44 4. A medication approach (Australian perspective) Conclusion - start low, go slow, finish slow, although ensure optimal doses are used - medication facilitates each child s ability to learn in the classroom, playground and home environment: new habits can take 6 months to evolve - Comprehensively assess and treat with approved medication and/or psychosocial treatments all comorbid conditions
Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children s Hospital
 Assessment and treatment of ADHD in children and adolescents In Australia: an overview Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children
Assessment and treatment of ADHD in children and adolescents In Australia: an overview Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children
Attention Deficit Hyperactivity Disorder: an overview of current advances in the field
 Attention Deficit Hyperactivity Disorder: an overview of current advances in the field Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children
Attention Deficit Hyperactivity Disorder: an overview of current advances in the field Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children
Disruptive behaviour disorders Oppositional defiant disorder (ODD) / Conduct disorder (CD)
 / Conduct disorder (CD)") Disruptive behaviour disorders Oppositional defiant disorder (ODD) / Conduct disorder (CD) Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal
Disruptive behaviour disorders Oppositional defiant disorder (ODD) / Conduct disorder (CD) Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal
Attention deficit hyperactivity disorder (ADHD), Conduct disorder biological treatments
, Conduct disorder biological treatments") Attention deficit hyperactivity disorder (ADHD), Conduct disorder biological treatments Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal
Attention deficit hyperactivity disorder (ADHD), Conduct disorder biological treatments Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal
Depressive disorders in young people: what is going on and what can we do about it? Lecture 1
 Depressive disorders in young people: what is going on and what can we do about it? Lecture 1 Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne
Depressive disorders in young people: what is going on and what can we do about it? Lecture 1 Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne
 Passport control a bit carried away. appreciated the advice forgot to talk to the manager, next thing I know my fmri thankfully, when aroused things back to normal Inattentive impaired children and adolescents:
Passport control a bit carried away. appreciated the advice forgot to talk to the manager, next thing I know my fmri thankfully, when aroused things back to normal Inattentive impaired children and adolescents:
Depressive disorders and ADHD
 Depressive disorders and ADHD Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children s Hospital avance@unimelb.edu.au www.rch.org.au/acpu
Depressive disorders and ADHD Professor Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children s Hospital avance@unimelb.edu.au www.rch.org.au/acpu
Week 2: Disorders of Childhood
 Week 2: Disorders of Childhood What are neurodevelopmental disorders? A group of conditions with onset in the developmental period Disorders of the brain The disorders manifest early in development, often
Week 2: Disorders of Childhood What are neurodevelopmental disorders? A group of conditions with onset in the developmental period Disorders of the brain The disorders manifest early in development, often
Biological Risk Factors
 Biological Risk Factors Ms Angelina Crea Provisional Psychologist Academic Child Psychiatry Unit Royal Children s Hospital Professor Alasdair Vance Head Academic Child Psychiatry Department of Paediatrics
Biological Risk Factors Ms Angelina Crea Provisional Psychologist Academic Child Psychiatry Unit Royal Children s Hospital Professor Alasdair Vance Head Academic Child Psychiatry Department of Paediatrics
MRCPsych Pharmacology of ADHD treatment. Dr Xanthe Barkla, Consultant Child and Adolescent Psychiatrist
 MRCPsych Pharmacology of ADHD treatment Dr Xanthe Barkla, Consultant Child and Adolescent Psychiatrist 04 01 17 Curriculum mapping MRCPsych Paper A(ii) covers clinical psychopharmacology MRCPsych Syllabus:
MRCPsych Pharmacology of ADHD treatment Dr Xanthe Barkla, Consultant Child and Adolescent Psychiatrist 04 01 17 Curriculum mapping MRCPsych Paper A(ii) covers clinical psychopharmacology MRCPsych Syllabus:
Robust cognitive neuroscience constructs and comorbidity: can they help?
 Robust cognitive neuroscience constructs and comorbidity: can they help? A/Professor Alasdair Vance Consultant Child and Adolescent Psychiatrist Head, Academic Child Psychiatry Department of Paediatrics
Robust cognitive neuroscience constructs and comorbidity: can they help? A/Professor Alasdair Vance Consultant Child and Adolescent Psychiatrist Head, Academic Child Psychiatry Department of Paediatrics
ADHD Explanation 5: Medications used in ADHD
 ADHD Explanation 5: Medications The aim of treatment is efficient functioning and achieving goals in life It is most important to find the dose of medications that works best As children grow they may
ADHD Explanation 5: Medications The aim of treatment is efficient functioning and achieving goals in life It is most important to find the dose of medications that works best As children grow they may
Translational Clinical Science
 Translational Clinical Science Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children s Hospital Outline of Presentation 1. Translational Clinical
Translational Clinical Science Alasdair Vance Head, Academic Child Psychiatry Department of Paediatrics University of Melbourne Royal Children s Hospital Outline of Presentation 1. Translational Clinical
Role of ADHD medication in children with autism spectrum disorder. Pieter Hoekstra University of Groningen, Netherlands
 Role of ADHD medication in children with autism spectrum disorder Pieter Hoekstra University of Groningen, Netherlands Symptoms of ADHD are highly prevalent in children with ASD Two independent chart reviews
Role of ADHD medication in children with autism spectrum disorder Pieter Hoekstra University of Groningen, Netherlands Symptoms of ADHD are highly prevalent in children with ASD Two independent chart reviews
Challenging Behaviours in Childhood
 Challenging Behaviours in Childhood A/Professor Alasdair Vance Consultant Child and Adolescent Psychiatrist Department of Paediatrics University of Melbourne Royal Children s Hospital Email: avance@unimelb.edu.au
Challenging Behaviours in Childhood A/Professor Alasdair Vance Consultant Child and Adolescent Psychiatrist Department of Paediatrics University of Melbourne Royal Children s Hospital Email: avance@unimelb.edu.au
Psychopharmacology of ADHD. Copyright 2006 Neuroscience Education Institute. All rights reserved.
 Psychopharmacology of ADHD Persistence (Predicted Value) Persistence of ADHD Into Adulthood 90 80 70 60 50 40 30 20 10 0 NA 10 15 20 25 30 Age at Follow-Up Syndromatic Persistence Symptomatic Persistence
Psychopharmacology of ADHD Persistence (Predicted Value) Persistence of ADHD Into Adulthood 90 80 70 60 50 40 30 20 10 0 NA 10 15 20 25 30 Age at Follow-Up Syndromatic Persistence Symptomatic Persistence
ADHD Part II: Managing Comorbities
 ADHD Part II: Managing Comorbities Brett Johnson, MD Staff Psychiatrist Rady Children s Behavioral Crisis Center Assistant Clinical Professor (Voluntary), UCSD January 26, 2011 Financial Disclosure I have
ADHD Part II: Managing Comorbities Brett Johnson, MD Staff Psychiatrist Rady Children s Behavioral Crisis Center Assistant Clinical Professor (Voluntary), UCSD January 26, 2011 Financial Disclosure I have
3/19/2018. Cynthia King, MD Associate Professor of Psychiatry UNMSOM. Autism Spectrum Disorder
 Cynthia King, MD Associate Professor of Psychiatry UNMSOM Autism Spectrum Disorder 1 Identify three behavioral health concerns in ASD Identify three common families of medication that may be supportive
Cynthia King, MD Associate Professor of Psychiatry UNMSOM Autism Spectrum Disorder 1 Identify three behavioral health concerns in ASD Identify three common families of medication that may be supportive
3/19/2018. Cynthia King, MD Associate Professor of Psychiatry UNMSOM
 Cynthia King, MD Associate Professor of Psychiatry UNMSOM 1 2 Autism Spectrum Disorder 3 Identify three behavioral health concerns in ASD Identify three common families of medication that may be supportive
Cynthia King, MD Associate Professor of Psychiatry UNMSOM 1 2 Autism Spectrum Disorder 3 Identify three behavioral health concerns in ASD Identify three common families of medication that may be supportive
Prevalence of Comorbidity and Pattern Drug Use among Children with Attention-deficit hyperactivity disorder: A Single Center in Thailand
 The 25th Federation Of Asian Pharmaceutical Association (FAPA) Congress 2014 Kota Kinabalu, Sabah, Malaysia 9th - 12th October, 2014 Prevalence of Comorbidity and Pattern Drug Use among Children with Attention-deficit
The 25th Federation Of Asian Pharmaceutical Association (FAPA) Congress 2014 Kota Kinabalu, Sabah, Malaysia 9th - 12th October, 2014 Prevalence of Comorbidity and Pattern Drug Use among Children with Attention-deficit
Attention Deficit Hyperactivity Disorder State of the Art. Christopher Okiishi, MD
 Attention Deficit Hyperactivity Disorder State of the Art Christopher Okiishi, MD What is ADHD? Three subtypes: Inattentive (under diagnosed, esp. in girls) Hyperactive Impulsive Combined Impairments must
Attention Deficit Hyperactivity Disorder State of the Art Christopher Okiishi, MD What is ADHD? Three subtypes: Inattentive (under diagnosed, esp. in girls) Hyperactive Impulsive Combined Impairments must
PRACTICE PARAMETERS FOR THE ASSESSMENT AND TREATMENT OF CHILDREN WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER
 PRACTICE PARAMETERS FOR THE ASSESSMENT AND TREATMENT OF CHILDREN WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER Attention-Deficit / Hyperactivity Disorder (ADHD). (2017, August 31). Retrieved April 06,
PRACTICE PARAMETERS FOR THE ASSESSMENT AND TREATMENT OF CHILDREN WITH ATTENTION DEFICIT HYPERACTIVITY DISORDER Attention-Deficit / Hyperactivity Disorder (ADHD). (2017, August 31). Retrieved April 06,
Alpha-2 Agonists. Antipsychotics
 Table 5: Randomized Controlled Trials of Psychotropic Medications in Children and Adolescents with ASD Agent Study Target Symptoms Dose Demographics Significant Side Clonidine Guanfacine Jaselskis et al.,
Table 5: Randomized Controlled Trials of Psychotropic Medications in Children and Adolescents with ASD Agent Study Target Symptoms Dose Demographics Significant Side Clonidine Guanfacine Jaselskis et al.,
ADHD in the Preschool Aged Child
 ADHD in the Preschool Aged Child (PATS) 11/2/2013 Stephen Meister MD, MHA, FAAP The Edmund N Ervin Pediatric Center (PATS) National Institute of Mental Health study First papers published in 2006 after
ADHD in the Preschool Aged Child (PATS) 11/2/2013 Stephen Meister MD, MHA, FAAP The Edmund N Ervin Pediatric Center (PATS) National Institute of Mental Health study First papers published in 2006 after
6/22/2012. Co-morbidity - when two or more conditions occur together. The two conditions may or may not be causally related.
 Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
Autism Spectrum Disorders and Co-existing Mental Health Issues By Dr. Karen Berkman Objective To present an overview of common psychiatric conditions that occur in persons with autism spectrum disorders
4/2/13 COMMON CLASSES OF MEDICATIONS. Child & Adolescent Behavioral Medicine & Medication Therapies. Behavioral Medicine & Medication Therapies
 Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Child & Adolescent Behavioral Medicine & Medication Therapies Brian J Cowles, PharmD Associate Professor of Pharmacy Practice Albany College of Pharmacy & Health Sciences; Vermont Campus Behavioral Medicine
Attention-Deficit/Hyperactivity Disorder Nathan J. Blum, M.D.
 ADHD in Preschool Children Preschool ADHD: When Should We Diagnose it & How Should We Treat it? Professor of Pediatrics Diagnosis of ADHD in Preschool Children: Impact of DSM-IV Is Preschool ADHD Associated
ADHD in Preschool Children Preschool ADHD: When Should We Diagnose it & How Should We Treat it? Professor of Pediatrics Diagnosis of ADHD in Preschool Children: Impact of DSM-IV Is Preschool ADHD Associated
Practical care of the Child with ADHD Kristina Hingre MD
 Practical care of the Child with ADHD Kristina Hingre MD Objectives Know the DSM 5 Criteria for diagnosis of ADHD Identify 4 Comorbidities of ADHD Be familiar with the common ADHD medications and Side
Practical care of the Child with ADHD Kristina Hingre MD Objectives Know the DSM 5 Criteria for diagnosis of ADHD Identify 4 Comorbidities of ADHD Be familiar with the common ADHD medications and Side
OH, Adolescents and Attention Deficit Hyperactivity Disorder (ADHD) How do you deal with them? Presented By: Todd Twogood MD, FAAP
 How do you deal with them? Presented By: Todd Twogood MD, FAAP") OH, Adolescents and Attention Deficit Hyperactivity Disorder (ADHD) How do you deal with them? Presented By: Todd Twogood MD, FAAP Teenagers Time of Transformation Allergy to Parents The Real Self Looks
OH, Adolescents and Attention Deficit Hyperactivity Disorder (ADHD) How do you deal with them? Presented By: Todd Twogood MD, FAAP Teenagers Time of Transformation Allergy to Parents The Real Self Looks
Contents Definition and History of ADHD Causative Factors
 1 Definition and History of ADHD................... 1 Brain Damage Syndromes........................ 1 Alternative Terms for ADHD...................... 2 Evolution of Present Concept of ADHD................
1 Definition and History of ADHD................... 1 Brain Damage Syndromes........................ 1 Alternative Terms for ADHD...................... 2 Evolution of Present Concept of ADHD................
ADHD Training for General Practitioners
 ADHD Training for General Practitioners Learning Objectives Understand the stigma surrounding ADHD and develop ability to challenge stigma. Understand your role in the ADHD pathway. Understand what you
ADHD Training for General Practitioners Learning Objectives Understand the stigma surrounding ADHD and develop ability to challenge stigma. Understand your role in the ADHD pathway. Understand what you
Citation for published version (APA): Jónsdóttir, S. (2006). ADHD and its relationship to comorbidity and gender. s.n.
: Jónsdóttir, S. (2006). ADHD and its relationship to comorbidity and gender. s.n.") University of Groningen ADHD and its relationship to comorbidity and gender Jónsdóttir, Sólveig IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite
University of Groningen ADHD and its relationship to comorbidity and gender Jónsdóttir, Sólveig IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite
Medications for Anxiety & Behavior in Williams Syndrome. Disclosure of Potential Conflicts. None 9/22/2016. Evaluation
 Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Medications for Anxiety & Behavior in Williams Syndrome Christopher J. McDougle, M.D. Director, Lurie Center for Autism Professor of Psychiatry and Pediatrics Massachusetts General Hospital and MassGeneral
Attention Deficit Hyperactivity Disorder (ADHD) BY MARK FABER M.D.
 BY MARK FABER M.D.") Attention Deficit Hyperactivity Disorder (ADHD) BY MARK FABER M.D. PREVALENCE & STATISTICS 6-8% of all children have ADHD (CDC Statistical Data) Age of onset: 7 years old (Prior DSM-IV) 12 years old (Current
Attention Deficit Hyperactivity Disorder (ADHD) BY MARK FABER M.D. PREVALENCE & STATISTICS 6-8% of all children have ADHD (CDC Statistical Data) Age of onset: 7 years old (Prior DSM-IV) 12 years old (Current
Medications in Autism: What We Know and Don't Know
 Medications in Autism: What We Know and Don't Know Jeremy Veenstra-VanderWeele, M.D. Mortimer D. Sackler, M.D., Associate Professor Center for Autism and the Developing Brain Sackler Institute for Developmental
Medications in Autism: What We Know and Don't Know Jeremy Veenstra-VanderWeele, M.D. Mortimer D. Sackler, M.D., Associate Professor Center for Autism and the Developing Brain Sackler Institute for Developmental
Pharmacological interventions for children with Disruptive Behaviour Disorders or Conduct Disorder or Oppositional Defiant Disorder
 updated 2012 Pharmacological interventions for children with Disruptive Behaviour Disorders or Conduct Disorder or Oppositional Defiant Disorder Q8: What is the effectiveness, safety and role of pharmacological
updated 2012 Pharmacological interventions for children with Disruptive Behaviour Disorders or Conduct Disorder or Oppositional Defiant Disorder Q8: What is the effectiveness, safety and role of pharmacological
What are the most common signs of ADHD? And what are the most common medication interventions?
 What are the most common signs of ADHD? And what are the most common medication interventions? Bennett Gertz, MD, FAAP Developmental Behavioral Pediatrician Children s Developmental Health Services Albertina
What are the most common signs of ADHD? And what are the most common medication interventions? Bennett Gertz, MD, FAAP Developmental Behavioral Pediatrician Children s Developmental Health Services Albertina
5/16/2018. Pediatric Attention Deficit Hyperactivity Disorder: Do you get it?
 Pediatric Attention Deficit Hyperactivity Disorder: Do you get it? Mashelle Jansen, DNP, FNP BC Clinical Assistant Professor SUNY Upstate Medical University ADHD is a Commonly diagnosed Childhood Neurodevelopmental
Pediatric Attention Deficit Hyperactivity Disorder: Do you get it? Mashelle Jansen, DNP, FNP BC Clinical Assistant Professor SUNY Upstate Medical University ADHD is a Commonly diagnosed Childhood Neurodevelopmental
Pediatric Psychopharmacology
 Pediatric Psychopharmacology General issues to consider. Pharmacokinetic differences Availability of Clinical Data Psychiatric Disorders can be common in childhood. Early intervention may prevent disorders
Pediatric Psychopharmacology General issues to consider. Pharmacokinetic differences Availability of Clinical Data Psychiatric Disorders can be common in childhood. Early intervention may prevent disorders
Update on the Treatment of ADHD 2019
 Update on the Treatment of ADHD 2019 James H. Beard, Jr., M.D, FAAP Developmental-Behavioral Pediatrician Division of Developmental Pediatrics The Rights of ADHD The right diagnosis of ADHD and co morbidities
Update on the Treatment of ADHD 2019 James H. Beard, Jr., M.D, FAAP Developmental-Behavioral Pediatrician Division of Developmental Pediatrics The Rights of ADHD The right diagnosis of ADHD and co morbidities
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XIV, 2012 INDEX
 A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
Pharmacotherapy of Adult ADHD
 Pharmacotherapy of Adult ADHD Thomas J. Spencer, MD Massachusetts General Hospital Harvard Medical School Disclosures Dr. Spencer receives research support from Royalties and Licensing fees on copyrighted
Pharmacotherapy of Adult ADHD Thomas J. Spencer, MD Massachusetts General Hospital Harvard Medical School Disclosures Dr. Spencer receives research support from Royalties and Licensing fees on copyrighted
Other Disorders Myers for AP Module 69
 1 Other s Myers for AP Module 69 Describe the general characteristics of somatic symptom disorders. How does culture influence people s expression of physical complaints? Compare the symptoms of conversion
1 Other s Myers for AP Module 69 Describe the general characteristics of somatic symptom disorders. How does culture influence people s expression of physical complaints? Compare the symptoms of conversion
Treating Disruptive Behavior Disorders in Children and Teens. A Review of the Research for Parents and Caregivers
 Treating Disruptive Behavior Disorders in Children and Teens A Review of the Research for Parents and Caregivers e Is This Information Right for Me? This information is for you if: A health care professional*
Treating Disruptive Behavior Disorders in Children and Teens A Review of the Research for Parents and Caregivers e Is This Information Right for Me? This information is for you if: A health care professional*
Update on First Psychotic Episodes in Childhood and Adolescence. Cheryl Corcoran, MD Assistant Professor of Psychiatry Columbia University
 Update on First Psychotic Episodes in Childhood and Adolescence Cheryl Corcoran, MD Assistant Professor of Psychiatry Columbia University Childhood-Onset Psychosis 8% of psychiatrically referred youth
Update on First Psychotic Episodes in Childhood and Adolescence Cheryl Corcoran, MD Assistant Professor of Psychiatry Columbia University Childhood-Onset Psychosis 8% of psychiatrically referred youth
Learning, to help them learn Seminar on Learning Disability and ADHD 25th June 2017 Country Inn & Suites, Patto Plaza, Panaji
 Learning, to help them learn Seminar on Learning Disability and ADHD 25th June 2017 Country Inn & Suites, Patto Plaza, Panaji Medical Management of ADHD www.antarman.goadoctor.co.in Community Management
Learning, to help them learn Seminar on Learning Disability and ADHD 25th June 2017 Country Inn & Suites, Patto Plaza, Panaji Medical Management of ADHD www.antarman.goadoctor.co.in Community Management
Perspective Truth on ADHD & Medications. Thomas L. Matthews, M.D. Associate Dean of Student Affairs Professor of Psychiatry
 Perspective Truth on ADHD & Medications Thomas L. Matthews, M.D. Associate Dean of Student Affairs Professor of Psychiatry Disclosures National Institute of Health ADHD and Aggression Study Co- Investigator
Perspective Truth on ADHD & Medications Thomas L. Matthews, M.D. Associate Dean of Student Affairs Professor of Psychiatry Disclosures National Institute of Health ADHD and Aggression Study Co- Investigator
Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder,
 Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder, Journal of the Academy of Child and Adolescent Psychiatry, 1997 Primary Authors: Jon McClellan MD
Practice Parameter for the Assessment and Treatment of Children and Adolescents with Bipolar Disorder, Journal of the Academy of Child and Adolescent Psychiatry, 1997 Primary Authors: Jon McClellan MD
DRUGS FOR ADHD: ADOLESCENTS TO ADULTS
 DRUGS FOR ADHD: ADOLESCENTS TO ADULTS DISCLOSURE Natasha Rodney-Cail, Pharmacist, Drug Evaluation Unit Has no conflicts of interest Dr. James Chandler, MD, FRCPC Has no conflicts of interest STEVEN Age
DRUGS FOR ADHD: ADOLESCENTS TO ADULTS DISCLOSURE Natasha Rodney-Cail, Pharmacist, Drug Evaluation Unit Has no conflicts of interest Dr. James Chandler, MD, FRCPC Has no conflicts of interest STEVEN Age
Psychiatric Medications. Positive and negative effects in the classroom
 Psychiatric Medications Positive and negative effects in the classroom Teaching the Medicated Child Beverly Bryant, M.D. Hattiesburg Clinic 9/17/14 Introduction According to the National Survey of Children
Psychiatric Medications Positive and negative effects in the classroom Teaching the Medicated Child Beverly Bryant, M.D. Hattiesburg Clinic 9/17/14 Introduction According to the National Survey of Children
Attention Deficit Hyperactivity Disorder A Neuro-Anatomical Approach to diagnosis and treatment
 Attention Deficit Hyperactivity Disorder A Neuro-Anatomical Approach to diagnosis and treatment Damon Lipinski, Ph.D. Clinical Psychologist Center for Pediatric Neuropsychology What is Attention? Different
Attention Deficit Hyperactivity Disorder A Neuro-Anatomical Approach to diagnosis and treatment Damon Lipinski, Ph.D. Clinical Psychologist Center for Pediatric Neuropsychology What is Attention? Different
Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder
 Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder Hannah Sauer, PharmD PGY1 Pediatric Pharmacy Resident Mayo Clinic 2015 MFMER slide-1 Objectives
Piecing the Puzzle Together: Pharmacologic Approaches to Behavioral Management in Autism Spectrum Disorder Hannah Sauer, PharmD PGY1 Pediatric Pharmacy Resident Mayo Clinic 2015 MFMER slide-1 Objectives
GOALS FOR THE PSCYHIATRY CLERKSHIP
 GOALS FOR THE PSCYHIATRY CLERKSHIP GOALS - The aim of the core psychiatry clerkship is to expose students to patients with mental illness and to prepare them to provide psychiatric care at a basic level.
GOALS FOR THE PSCYHIATRY CLERKSHIP GOALS - The aim of the core psychiatry clerkship is to expose students to patients with mental illness and to prepare them to provide psychiatric care at a basic level.
About ADHD in children, adolescents and adults
 About ADHD in children, adolescents and adults About ADHD ADHD is not a new disease. ADHD and other disorders with similar symptoms have been described for more than a century. Although ADHD may seem more
About ADHD in children, adolescents and adults About ADHD ADHD is not a new disease. ADHD and other disorders with similar symptoms have been described for more than a century. Although ADHD may seem more
Pharmacological management of behavioural problems in children with acquired brain injury. A/Professor A Vance
 Pharmacological management of behavioural problems in children with acquired brain injury Outline of presentation 1. The key types of acquired brain injury behavioural problems 2. A useful clinical model
Pharmacological management of behavioural problems in children with acquired brain injury Outline of presentation 1. The key types of acquired brain injury behavioural problems 2. A useful clinical model
Adult ADHD. 1. Overview of ADHD 4. Principles for managing ADHD. 2. Common features of ADHD in adults. 3. General approaches to managing ADHD
 Adult ADHD 1. Overview of ADHD 4. Principles for managing ADHD 2. Common features of ADHD in adults 3. General approaches to managing ADHD Definition The name... 1. Overview of ADHD Definition Attention
Adult ADHD 1. Overview of ADHD 4. Principles for managing ADHD 2. Common features of ADHD in adults 3. General approaches to managing ADHD Definition The name... 1. Overview of ADHD Definition Attention
IRONSHORE TO PRESENT THREE POSTERS AT THE 2019 ANNUAL AMERICAN PROFESSIONAL SOCIETY OF ADHD AND RELATED DISORDERS (APSARD) MEETING
 MEETING") FOR IMMEDIATE RELEASE IRONSHORE TO PRESENT THREE POSTERS AT THE 2019 ANNUAL AMERICAN PROFESSIONAL SOCIETY OF ADHD AND RELATED DISORDERS (APSARD) MEETING George Town, Cayman Islands January 10, 2019 Ironshore
FOR IMMEDIATE RELEASE IRONSHORE TO PRESENT THREE POSTERS AT THE 2019 ANNUAL AMERICAN PROFESSIONAL SOCIETY OF ADHD AND RELATED DISORDERS (APSARD) MEETING George Town, Cayman Islands January 10, 2019 Ironshore
ADHD Assessment and Treatment in Primary Care
 ADHD Assessment and Treatment in Primary Care Matthew Tolliver, Ph.D., Assistant Professor, ETSU Pediatrics Dr. David Wood, Professor and Chair, ETSU Pediatrics ADHD in Teenagers We have no financial disclosures.
ADHD Assessment and Treatment in Primary Care Matthew Tolliver, Ph.D., Assistant Professor, ETSU Pediatrics Dr. David Wood, Professor and Chair, ETSU Pediatrics ADHD in Teenagers We have no financial disclosures.
11/2/2016 INSIDE THE MIND OF A CHILD PSYCHIATRIST: PROBLEM BEHAVIORS IN CHILDREN WITH AUTISM FACULTY DISCLOSURE
 FACULTY DISCLOSURE INSIDE THE MIND OF A CHILD PSYCHIATRIST: PROBLEM BEHAVIORS IN CHILDREN WITH AUTISM KristinDawson, MD Assistant Professor University of Kentucky No commercial conflicts of Interest Salary
FACULTY DISCLOSURE INSIDE THE MIND OF A CHILD PSYCHIATRIST: PROBLEM BEHAVIORS IN CHILDREN WITH AUTISM KristinDawson, MD Assistant Professor University of Kentucky No commercial conflicts of Interest Salary
March 10, Group 1 presentation 2. Personality and emotional development, and Gender (pwr. pnt. slides from Mar. 3, 2010) 4.
 4.") March 10,2010 1. Group 1 presentation 2. Personality and emotional development, and Gender (pwr. pnt. slides from Mar. 3, 2010) 3. Self-regulation 4. ADHD-DVD The Development of Self-regulation Self-regulation
March 10,2010 1. Group 1 presentation 2. Personality and emotional development, and Gender (pwr. pnt. slides from Mar. 3, 2010) 3. Self-regulation 4. ADHD-DVD The Development of Self-regulation Self-regulation
The Use of ADHD Medication in the Pediatric Population
 The Use of ADHD Medication in the Pediatric Population Shirin Madzhidova, PharmD Pediatric Pharmacotherapy Fellow Nova Southeastern University Objectives Discuss the importance of treatment with medications
The Use of ADHD Medication in the Pediatric Population Shirin Madzhidova, PharmD Pediatric Pharmacotherapy Fellow Nova Southeastern University Objectives Discuss the importance of treatment with medications
What About Health 3: Challenging Behaviors
 The title of this presentation is What About Health. I m. In this presentation I will discuss a number of health and mental health issues related to children with ASD. 1 Now I am going to switch to discussing
The title of this presentation is What About Health. I m. In this presentation I will discuss a number of health and mental health issues related to children with ASD. 1 Now I am going to switch to discussing
Attention Deficit Hyperactivity Disorder
 AMS-MOH CLINICAL PRACTICE GUIDELINES 1/2014 Attention Deficit Hyperactivity Disorder Academy of Medicine, Singapore College of Paediatrics and Child Health, Singapore College of Family Physicians Singapore
AMS-MOH CLINICAL PRACTICE GUIDELINES 1/2014 Attention Deficit Hyperactivity Disorder Academy of Medicine, Singapore College of Paediatrics and Child Health, Singapore College of Family Physicians Singapore
The relationship between ADHD and substance use disorder: Evidence based treatment and clinical implications
 Society for the Study of Addiction, York The relationship between ADHD and substance use disorder: Evidence based treatment and clinical implications November 12.th 2010 Soren Dalsgaard, MD, PhD, associate
Society for the Study of Addiction, York The relationship between ADHD and substance use disorder: Evidence based treatment and clinical implications November 12.th 2010 Soren Dalsgaard, MD, PhD, associate
Pharmacotherapy of ADHD with Non-Stimulants
 Pharmacotherapy of ADHD with Non-Stimulants Timothy E. Wilens, M.D. Chief, Division of Child and Adolescent Psychiatry, (Co)Director of Center for Addiction Medicine, Massachusetts General Hospital Massachusetts
Pharmacotherapy of ADHD with Non-Stimulants Timothy E. Wilens, M.D. Chief, Division of Child and Adolescent Psychiatry, (Co)Director of Center for Addiction Medicine, Massachusetts General Hospital Massachusetts
GM ADHD Strategic Clinical Network. Training for Specialist ADHD Teams
 GM ADHD Strategic Clinical Network Training for Specialist ADHD Teams Learning Objectives Understand the stigma surrounding ADHD and develop ability to challenge stigma.. DSM-5 classification of ADHD ADHD
GM ADHD Strategic Clinical Network Training for Specialist ADHD Teams Learning Objectives Understand the stigma surrounding ADHD and develop ability to challenge stigma.. DSM-5 classification of ADHD ADHD
2013 Virtual AD/HD Conference 1
 Medication for & Coexisting Conditions Part 2 Dr. Kenny Handelman Child, Adolescent & Adult Psychiatrist Halton Healthcare Adjunct Professor of Psychiatry, University of Western Ontario www.drkenny.com
Medication for & Coexisting Conditions Part 2 Dr. Kenny Handelman Child, Adolescent & Adult Psychiatrist Halton Healthcare Adjunct Professor of Psychiatry, University of Western Ontario www.drkenny.com
Index. Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) b-adrenergic blockers
 b-adrenergic blockers") Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Note: Page numbers of article titles are in boldface type. A ADHD. See Attention-deficit/hyperactivity disorder (ADHD) a-adrenergic blockers for PTSD, 798 b-adrenergic blockers for PTSD, 798 Adrenergic
Humberto Nagera M.D. Director, The Carter-Jenkins Center Psychoanalyst, Children, Adolescents and Adults Professor of Psychiatry at USF Professor
 The Carter Jenkins Center presents 1 Humberto Nagera M.D. Director, The Carter-Jenkins Center Psychoanalyst, Children, Adolescents and Adults Professor of Psychiatry at USF Professor Emeritus of Psychiatry
The Carter Jenkins Center presents 1 Humberto Nagera M.D. Director, The Carter-Jenkins Center Psychoanalyst, Children, Adolescents and Adults Professor of Psychiatry at USF Professor Emeritus of Psychiatry
Index. B Behavioral training for children with ASD, 99 Behavior modification, 5 Brain tumors, 72 Bronfenbrenner s ecological systems Theory, 137
 A ABA training behavior modification techniques, 101, 106 UCLA model, 103 Acute Lymphoblastic Leukemia (ALL), 71, 78 Acute pain, 49, 51, 56 Adherence to diabetes regimens, 34 American Cancer Society, 71
A ABA training behavior modification techniques, 101, 106 UCLA model, 103 Acute Lymphoblastic Leukemia (ALL), 71, 78 Acute pain, 49, 51, 56 Adherence to diabetes regimens, 34 American Cancer Society, 71
Behavioural Disorders
 Behavioural Disorders BEH Hyperkinetic disorder / attention deficit hyperactivity disorder (ADHD) Behavioural disorders is an umbrella term that includes more specific disorders, such as hyperkinetic disorder
Behavioural Disorders BEH Hyperkinetic disorder / attention deficit hyperactivity disorder (ADHD) Behavioural disorders is an umbrella term that includes more specific disorders, such as hyperkinetic disorder
Scottish Medicines Consortium
 Scottish Medicines Consortium atomoxetine capsules 10 mg to 60 mg (Strattera ) (153/05) Eli Lilly and Company Ltd No. 4 February 2005 The Scottish Medicines Consortium has completed its assessment of the
Scottish Medicines Consortium atomoxetine capsules 10 mg to 60 mg (Strattera ) (153/05) Eli Lilly and Company Ltd No. 4 February 2005 The Scottish Medicines Consortium has completed its assessment of the
The Neurobiology of Attention
 The Neurobiology of Attention by Nadia Fike, MD/PhD Pediatric Neurology Center for Neurosciences Disclosures Nadia Fike, MD/PhD No relevant financial or nonfinancial relationships to disclose. Objectives
The Neurobiology of Attention by Nadia Fike, MD/PhD Pediatric Neurology Center for Neurosciences Disclosures Nadia Fike, MD/PhD No relevant financial or nonfinancial relationships to disclose. Objectives
Ippeita Dan on behalf of RISTEX ADHD Diagnosis Consortium Chuo University, Tokyo, Japan
 Functional near-infrared spectroscopy on the go for clinical application along with recent technical development for enhancing its potential With emphasis on neuropharmacological assessment on children
Functional near-infrared spectroscopy on the go for clinical application along with recent technical development for enhancing its potential With emphasis on neuropharmacological assessment on children
Issue date September 2010 (Reviewed October 2013) Clinicians from Andrew Lang Centre, Mental. Specialist Pharmacist & Formulary Pharmacist
 Clinicians from Andrew Lang Centre, Mental. Specialist Pharmacist & Formulary Pharmacist") Title Document Type Issue no Shared care guidelines in the Treatment of Attention Deficit/ Hyperactivity Disorders Shared Care Guidelines and Information for GPs Clinical Governance Support Team Use Issue
Title Document Type Issue no Shared care guidelines in the Treatment of Attention Deficit/ Hyperactivity Disorders Shared Care Guidelines and Information for GPs Clinical Governance Support Team Use Issue
Gender Sensitive Factors in Girls Delinquency
 Gender Sensitive Factors in Girls Delinquency Diana Fishbein, Ph.D. Research Triangle Institute Transdisciplinary Behavioral Science Program Shari Miller-Johnson, Ph.D. Duke University Center for Child
Gender Sensitive Factors in Girls Delinquency Diana Fishbein, Ph.D. Research Triangle Institute Transdisciplinary Behavioral Science Program Shari Miller-Johnson, Ph.D. Duke University Center for Child
Summary of risk management plan for Methylphenidate modifiedrelease hard capsules (methylphenidate)
") Part VI: Summary of the risk management plan Summary of risk management plan for Methylphenidate modifiedrelease hard capsules (methylphenidate) This is a summary of the risk management plan (RMP) for
Part VI: Summary of the risk management plan Summary of risk management plan for Methylphenidate modifiedrelease hard capsules (methylphenidate) This is a summary of the risk management plan (RMP) for
Correlates of Tic Disorders. Hyperactivity / motor restlessness Inattentiveness Anxiety Aggression Other
 Tourette Disorder Rarely present in pure form No two individuals with TD are the same Often associated with other symptoms, which may be more disabling than the tics themselves Treatments need to target
Tourette Disorder Rarely present in pure form No two individuals with TD are the same Often associated with other symptoms, which may be more disabling than the tics themselves Treatments need to target
Indications for Medications. John Wermager, MD May 2, 2017
 Indications for Medications John Wermager, MD May 2, 2017 First and foremost, accurate diagnosis is imperative for good treatment. It may also guide a person to go down the medication route sooner, depending
Indications for Medications John Wermager, MD May 2, 2017 First and foremost, accurate diagnosis is imperative for good treatment. It may also guide a person to go down the medication route sooner, depending
Clinical assessment of ADHD. The size of a clinic s problem. Diagnosis: detecting the disorder. ADHD has several components
 Assessment is more than recognition Clinical assessment of ADHD Eric Taylor Department of Child & Adolescent Psychiatry Institute of Psychiatry-Kings College London Detecting the disorder Contextual assessment
Assessment is more than recognition Clinical assessment of ADHD Eric Taylor Department of Child & Adolescent Psychiatry Institute of Psychiatry-Kings College London Detecting the disorder Contextual assessment
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
Adult ADHD for GPs. Maria Mazfari Associate Nurse Consultant Adult ADHD Tina Profitt Clinical Nurse Specialist Adult ADHD
 Adult ADHD for GPs Maria Mazfari Associate Nurse Consultant Adult ADHD Tina Profitt Clinical Nurse Specialist Adult ADHD I m a Believer.. Are You? What is ADHD? ADHD is a valid clinical condition defined
Adult ADHD for GPs Maria Mazfari Associate Nurse Consultant Adult ADHD Tina Profitt Clinical Nurse Specialist Adult ADHD I m a Believer.. Are You? What is ADHD? ADHD is a valid clinical condition defined
ADHD DIAGNOSIS AND MANAGEMENT
 ADHD DIAGNOSIS AND MANAGEMENT Cesar Ochoa, MD Head, Developmental-Behavioral Pediatrics Rush University Medical Center Medical Director, Rush Neurobehavioral Center April 28,2017 LEARNING OBJECTIVES 1.
ADHD DIAGNOSIS AND MANAGEMENT Cesar Ochoa, MD Head, Developmental-Behavioral Pediatrics Rush University Medical Center Medical Director, Rush Neurobehavioral Center April 28,2017 LEARNING OBJECTIVES 1.
ADHD DIAGNOSIS AND MANAGEMENT LEARNING OBJECTIVES CASE 4/28/2017
 ADHD DIAGNOSIS AND MANAGEMENT Cesar Ochoa, MD Head, Developmental-Behavioral Pediatrics Rush University Medical Center Medical Director, Rush Neurobehavioral Center April 28,2017 LEARNING OBJECTIVES 1.
ADHD DIAGNOSIS AND MANAGEMENT Cesar Ochoa, MD Head, Developmental-Behavioral Pediatrics Rush University Medical Center Medical Director, Rush Neurobehavioral Center April 28,2017 LEARNING OBJECTIVES 1.
Cognitive Rehabilitation with Current Research and Transition of Care
 Cognitive Rehabilitation with Current Research and Transition of Care Mike Dichiaro, MD Pediatric Rehabilitation Medicine Carin Rowan, MPT Pediatric Physical Therapy Financial Disclosures No relevant financial
Cognitive Rehabilitation with Current Research and Transition of Care Mike Dichiaro, MD Pediatric Rehabilitation Medicine Carin Rowan, MPT Pediatric Physical Therapy Financial Disclosures No relevant financial
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
Drug Class Review Pharmacologic Treatments for Attention Deficit Hyperactivity Disorder
 Drug Class Review Pharmacologic Treatments for Attention Deficit Hyperactivity Disorder Final Report Update 3 September 2009 Update 2: November 2007 Update 1: May 2006 Original Report: September 2005 The
Drug Class Review Pharmacologic Treatments for Attention Deficit Hyperactivity Disorder Final Report Update 3 September 2009 Update 2: November 2007 Update 1: May 2006 Original Report: September 2005 The
Trea%ng ADHD. Primary Empirically Based Treatments: ü Psychos%mulants. ü Behavioral/Con%ngency Management. ü Parent Training
 Trea%ng ADHD Primary Empirically Based Treatments: ü Psychos%mulants ü Behavioral/Con%ngency Management ü Parent Training DSM-IV CLINICAL MODEL OF ADHD Biological Influences, e.g., genetics NEUROBIOLOGICAL
Trea%ng ADHD Primary Empirically Based Treatments: ü Psychos%mulants ü Behavioral/Con%ngency Management ü Parent Training DSM-IV CLINICAL MODEL OF ADHD Biological Influences, e.g., genetics NEUROBIOLOGICAL
SHARED PRESCRIBING GUIDELINE
 working in partnership with Kingston Richmond Wandsworth SHARED PRESCRIBING GUIDELINE Sutton & Merton Methylphenidate, Dexamfetamine and Atomoxetine for Attention Deficit Hyperactivity Disorder in patients
working in partnership with Kingston Richmond Wandsworth SHARED PRESCRIBING GUIDELINE Sutton & Merton Methylphenidate, Dexamfetamine and Atomoxetine for Attention Deficit Hyperactivity Disorder in patients
4. Definition, clinical diagnosis and diagnostic criteria
 4. Definition, clinical diagnosis and diagnostic criteria 4.1. Definition Major depression is a mood disorder consisting of a set of symptoms, which include a predominance of the affective type (pathological
4. Definition, clinical diagnosis and diagnostic criteria 4.1. Definition Major depression is a mood disorder consisting of a set of symptoms, which include a predominance of the affective type (pathological
Challenging ASD Cases November 11, Melanie Penner, MD, MSc, Mohammad Zubairi, MD, MEd,
 Challenging ASD Cases November 11, 2017 Melanie Penner, MD, MSc, FRCPC @drmelpenner Mohammad Zubairi, MD, MEd, FRCPC @md_mszubairi Learning Objectives By the end of this workshop, participants will: 1)
Challenging ASD Cases November 11, 2017 Melanie Penner, MD, MSc, FRCPC @drmelpenner Mohammad Zubairi, MD, MEd, FRCPC @md_mszubairi Learning Objectives By the end of this workshop, participants will: 1)
28 th Annual Learning Symposium
 Friday, January 6, 8 Breakout Session 8 th Annual Learning Symposium ADHD & Medication Steven Pliszka, M.D. Presented by: Steven Pliszka, M.D. Dielmann Distinguished Professor and Chair Department of Psychiatry,
Friday, January 6, 8 Breakout Session 8 th Annual Learning Symposium ADHD & Medication Steven Pliszka, M.D. Presented by: Steven Pliszka, M.D. Dielmann Distinguished Professor and Chair Department of Psychiatry,
Attention Deficit/Hyperactivity Disorder (ADHD)
") Disclaimers Attention Deficit/Hyperactivity Disorder (ADHD) Paul Glasier, Ph.D. Licensed Psychologist I have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
Disclaimers Attention Deficit/Hyperactivity Disorder (ADHD) Paul Glasier, Ph.D. Licensed Psychologist I have no relevant financial relationships with the manufacturers(s) of any commercial products(s)
SUPPORT INFORMATION ADVOCACY
 THE ASSESSMENT OF ADHD ADHD: Assessment and Diagnosis in Psychology ADHD in children is characterised by developmentally inappropriate overactivity, distractibility, inattention, and impulsive behaviour.
THE ASSESSMENT OF ADHD ADHD: Assessment and Diagnosis in Psychology ADHD in children is characterised by developmentally inappropriate overactivity, distractibility, inattention, and impulsive behaviour.
The Brain on ADHD. Ms. Komas. Introduction to Healthcare Careers
 The Brain on ADHD Ms. Komas Introduction to Healthcare Careers Ms. Komas Period 9/2/2016 Komas 1 HOOK: Attention Deficit Hyperactivity Disorder (ADHD) plagues between 5% and 7% of children and less than
The Brain on ADHD Ms. Komas Introduction to Healthcare Careers Ms. Komas Period 9/2/2016 Komas 1 HOOK: Attention Deficit Hyperactivity Disorder (ADHD) plagues between 5% and 7% of children and less than
Treatment for Co-Occurring Attention Deficit/Hyperactivity Disorder and Autism Spectrum Disorder
 Neurotherapeutics DOI 10.1007/s13311-012-0126-9 REVIEW Treatment for Co-Occurring Attention Deficit/Hyperactivity Disorder and Autism Spectrum Disorder Naomi Ornstein Davis Scott H. Kollins # The American
Neurotherapeutics DOI 10.1007/s13311-012-0126-9 REVIEW Treatment for Co-Occurring Attention Deficit/Hyperactivity Disorder and Autism Spectrum Disorder Naomi Ornstein Davis Scott H. Kollins # The American
Attention Deficit Hyperactivity Disorder Overview and New Perspectives
 1st Annual Regional Psychiatry Conference Psychiatry for the Non-Psychiatrist Attention Deficit Hyperactivity Disorder Overview and New Perspectives Thomas B. Henry, MD Board Certified Child & Adolescent
1st Annual Regional Psychiatry Conference Psychiatry for the Non-Psychiatrist Attention Deficit Hyperactivity Disorder Overview and New Perspectives Thomas B. Henry, MD Board Certified Child & Adolescent
I. Diagnostic Considerations (Assessment)...Page 1. II. Diagnostic Criteria and Consideration - General...Page 1
...Page 1. II. Diagnostic Criteria and Consideration - General...Page 1") SUTTER PHYSICIANS ALLIANCE (SPA) 2800 L Street, 7 th Floor Sacramento, CA 95816 SPA PCP Treatment & Referral Guideline Attention Deficit/Hyperactivity Disorder in Children and Adolescents Developed March
SUTTER PHYSICIANS ALLIANCE (SPA) 2800 L Street, 7 th Floor Sacramento, CA 95816 SPA PCP Treatment & Referral Guideline Attention Deficit/Hyperactivity Disorder in Children and Adolescents Developed March
An Overview on the Use of Psychotropic Medications
 An Overview on the Use of Psychotropic Medications Marilyn B. Benoit, M.D. Chief Clinical Officer SVP, Clinical & Professional Affairs Classes of Medications Antidepressants Anti-anxiety Mood stabilizers
An Overview on the Use of Psychotropic Medications Marilyn B. Benoit, M.D. Chief Clinical Officer SVP, Clinical & Professional Affairs Classes of Medications Antidepressants Anti-anxiety Mood stabilizers