arguably the greatest risk to human health comes in the form of antibiotic-resistant bacteria. We live in a bacterial world where we will never be
|
|
|
- Lewis Welch
- 5 years ago
- Views:
Transcription
1
2 arguably the greatest risk to human health comes in the form of antibiotic-resistant bacteria. We live in a bacterial world where we will never be able to stay ahead of the mutation curve. A test of our resilience is how far behind the curve we allow ourselves to fail. World Economic Forum, 2013
3 First, do no harm
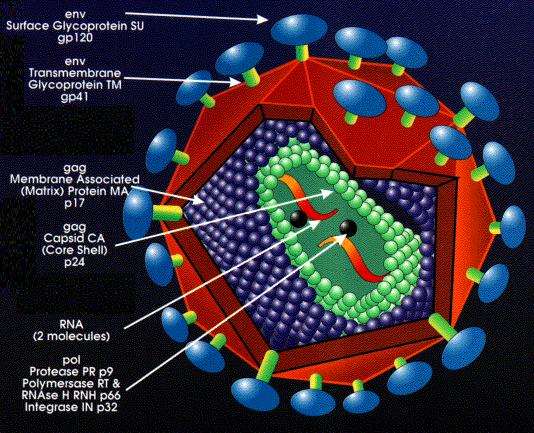
4 HIV
5 Review of 162 HIV pts hospitalized at Cleveland Clinic in % errors in prescriptions for ARV 65% of these errors not corrected by discharge E.Neuner. Abstract #36170, ID Week, San Diego 2012 Postulated reasons Complexity of regimens Unfamiliarity re HIV Rx by hospital MD s Shift of therapy to outpatient setting
6 ART should be offered regardless of CD4 count ART is recommended to persons during acute phase of primary HIV infection regardless of symptoms ART should be started as soon as possible in pts with opportunistic infections TB and Cryptococcus can be exceptions * JAMA. 2012; 308(4):
7 ART should be offered regardless of CD4 count There is a steady decrease in AIDS-free survival as CD4 threshold for initiation of Rx decreased. The higher the CD4 achieved after ART, the greater the survival benefit ART reduces likelihood of HIV transmission Cohen MS, et al. N Engl J Med 2011;365:
8
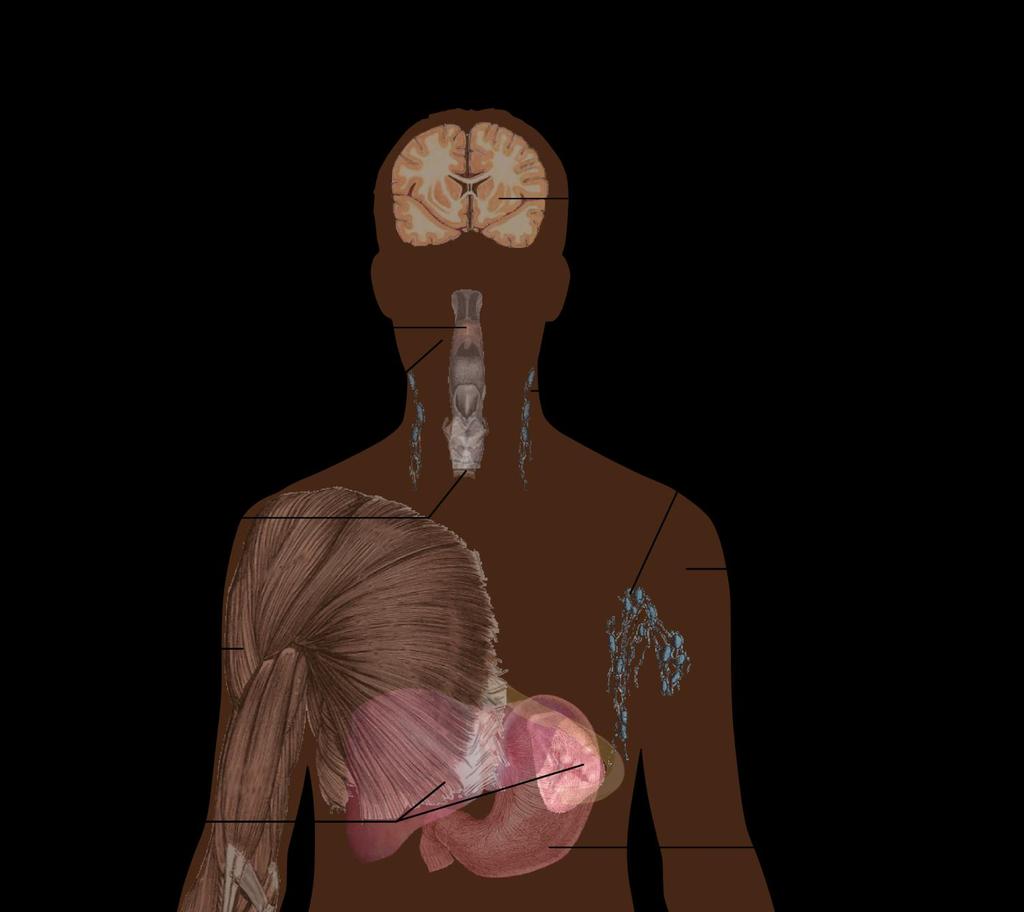
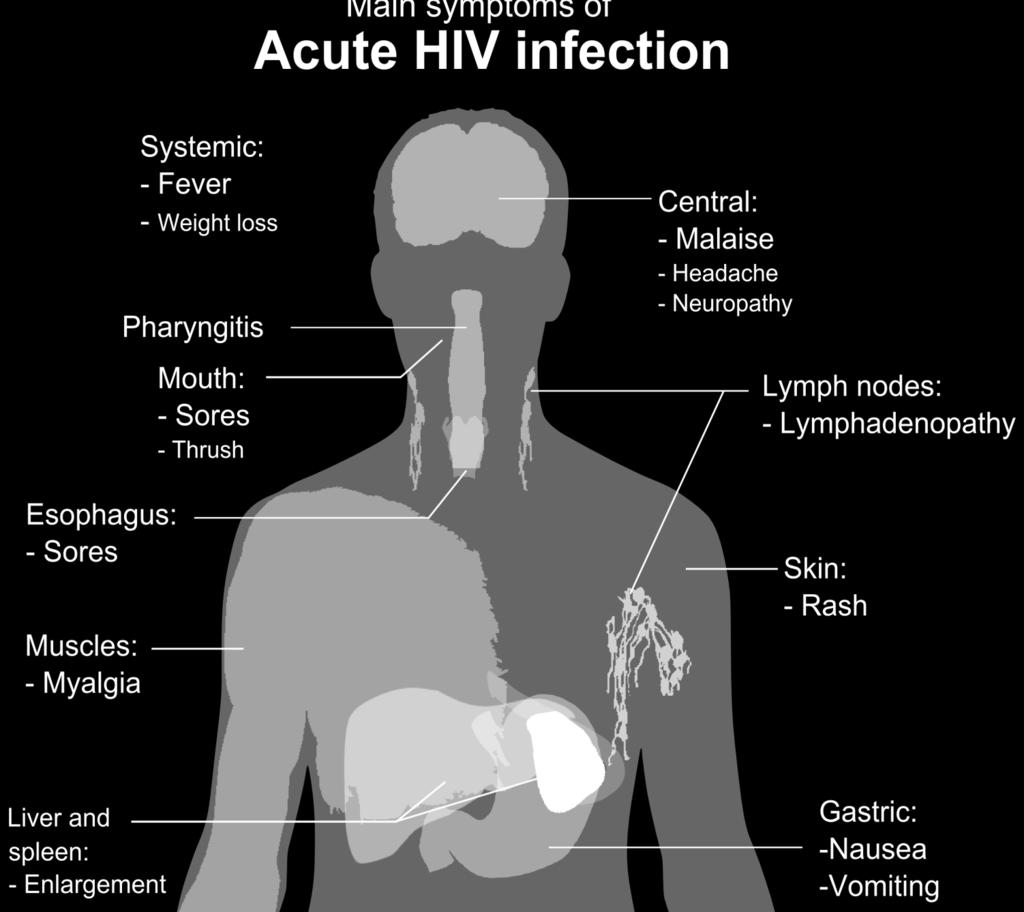
9 ART is recommended to persons during acute phase of primary HIV infection regardless of symptoms. Early Rx associated with: Conserved lymphocyte function Lowered cell-associated HIV DNA Reduction in viral set point Delayed rate of CD4 cell decline Theoretical decline in transmission because of high viral load in newly infected individuals
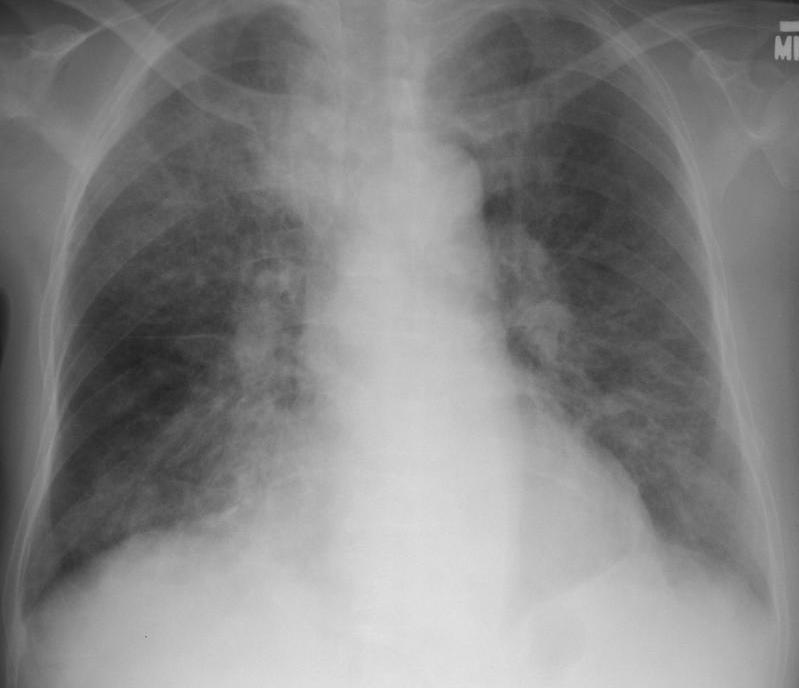
10 Pneumocystis
11 ART should be started as soon as possible in pts with opportunistic infections Usually start within 2 weeks of diagnosis Cryptococcal meningitis is less certain because of association of increased mortality with early Rx In TB, may delay ART Rx when CD4 > 50 to avoid immune reconstitution syndrome
12
13 What to start Prior to Rx should check genotype susceptibility Always treat with multiple agents (usually minimum of 3) Convenience of regimen is important as compliance is key to good outcome Specialist involvement improves patient outcomes

14
15
16 The desire to take medicine is perhaps the greatest factor which distinguishes man from animals. Sir William Osler
17 Indications for screening for ASB in adults includes: Pregnancy Prior to urologic procedures where mucosal bleeding is anticipated. No other adults with ASB should be treated CID. 2005;40:643-54
18 Screening for or treatment of ASB is not recommended for the following: Presence of pyuria Nonpregnant women Diabetic women Elderly persons, whether or not institutionalized Spinal cord injuries Catheterized patients Renal or other solid organ transplant
19 The Role of Asymptomatic Bacteruria in Young Women With Recurrent Urinary Tract Infections: To Treat or Not to Treat? 673 young women with ASB 312 not treated, 361 treated 13.1% not treated had recurrence at 12 mos 46.8% treated group had recurrence at 12 mos Cai T. Clin Infect Dis. 2012;55:

20 Table 2. Prevalence of asymptomatic bacteriuria in selected populations. Population Prevalence, % Healthy, premenopausal women Pregnant women Postmenopausal women aged years Diabetic patients Women Men Elderly persons in the community Women Men Elderly persons in a long-term care facility Women Men Patients with spinal cord injuries Intermittent catheter use Sphincterotomy and condom catheter in place 57 Patients undergoing hemodialysis 28 Patients with indwelling catheter use Short-term 9 23 Long-term 100
21 Patients in nursing homes are frequently evaluated for lethargy/stupor These patients frequently have ASB In the absence of fever and/or leukocytosis, the depressed mental status is seldom due to UTI. (Dr. Pontzer s observations unpublished) Many other factors, including dehydration, medications and metabolic factors are common causes
22 The downside for treatment of ASB include: C. diff C. diff C. diff Colonization/infection with multidrug-resistant bacteria in both the index patient and those patients surrounding him/her. Other adverse drug reactions
23 If your patient is afebrile and hemodynamically stable, recommend in most cases refrain from antibiotic treatment for ASB
24
25
26 246 pts with CDI reviewed 141 received non-cdi ABX Rx during and/or shortly after their CDI Rx totaling 445 courses 77% received at least 1 unnecessary ABX dose 26% of ABX Rx was totally unnecessary Leading indications for unnecessary Rx were putative UTI or pneumonia Shaughnessy MK, et al. Infect Control Hosp Epidemiol 2013;34:





27 HIGH RISK Cephalosporins 3 rd & 4 th gen MEDIUM RISK LOW or NO RISK ß-lactam Narrow spectrum Sulfonamides Tigecycline Quinolones Carbapenems Vancomycin Clindamycin TMP/SMX Metronidazole Broad Spectrum Penicillins Tetracyclines Macrolides Linezolid & Daptomycin Nitrofurantoin
28 Discontinue the inciting antibiotic therapy Mild disease po metronidazole 500 mg tid or vanco 125 mg qid for days Moderately severe disease po vancomycin with or without IV metronidazole Cohen SH, et al. Infect Control Hospit Epidiemol. 2010; 31:

29 Fulminant disease po vanco (500 mg qid) &/or intraluminal vanco (500 mg 3-4 x day) with IV metronidazole (500 mg q 8h) WBC Criteria for subtotal colectomy: age >65 with a >50,000 and/or lactate > 5 mmol/l Right-sided colonic lavage as substitute for subtotal colectomy may be viable option* IVIG reported effective in some case reports Controlled studies remain to be done *Lamontagne et al. Ann Surg. 2007;245:267
30 Fidaxomicin Narrower spectrum than vanco or metronidazole Less disruption of colonic flora Lower recurrence (10% v 28%) with non NAP1 strains No difference with NAP1 strains Expensive ~$3000 per course Louie et al. N Engl J Med. 2011;364:422

31 No antimicrobial agent is clearly superior for the initial cure of C. difficile infection Dimitri, DM. et al. Ann Intern Med 2011;155:
32 My current favorite po vancomycin pulse taper regimen: Week 1: 125 mg po qid Week 2: 125 mg po bid Week 3: 125 mg po daily Week 4-7: 125 mg po every other day
33 Fecal transplant following 4 days po vanco vs. po vancomycin 500 mg po qid X 14 days 81% cure with transplant 2 of 3 who failed were cured with 2 nd transplant 27% cure with standard vanco Rx Donor screening included risk factor questionnaire, parasites, C. diff, pathogenic bacteria, HIV, hepatitis A,B,C, CMV, EBV, Syphilis, serologies for Strongyloides & Amoeba Nood, E. et al. N Engl J Med 2013;368:407-15

34 Synthetic stool RePOOPulate Mixture of 33 different intestinal bacteria isolated in pure culture Treated 2 patients who had failed at least 3 courses of Rx for hypervirulent CDI Both were asymptomatic at 6 month follow-up Eliminates concern for disease transmission Eliminates yuk factor Petrof, E O, et al. Microbiome 2013; 1: 3
35
36 S. aureus
37 20-40 % mortality Leading cause of both community and hospital acquired bacteremia Complications include endocarditis, osteomyelitis, discitis, joint infection, endopthalmitis and many others Recurrence of bacteremia is common Sexton, D. et al. Treatment of Staphylococcus aureus bacteremia in adults UpToDate Jan 2013
38 Endocarditis frequency 25-32% TEE often indicated since presence of vegetation can impact management Occasional exceptions may include rapid clearance of bacteremia in the presence of a removable focus (i.e. vascular catheter) TTE is inadequate for ruling out IE
39 Vancomycin Dose must be adjusted based upon patient mass and creatinine clearance Follow trough vanco levels For sepsis target ug/ml Should be obtained at steady state Consider shift to another agent if MIC is > 2 ug/ml Change to beta-lactam if organism is MSSA Superiority supported by multiple studies
40 Daptomycin (Cubicin ) Effective against most MRSA & MSSA Not indicated for pneumonia Monitor CPK weekly Linezolid (Zyvox ) Effective against most MSSA & MRSA Lack of cidality suboptimal for endocarditis Not FDA approved for SAB
 and community acquired pneumonia (not MRSA) Overuse may well lead to resistance Q 12 hr dose may be suboptimal for")
41 Ceftaroline (Teflaro ) 5 th generation cephalosporin Active against MRSA It is bactericidal Not FDA approved for bacteremia/sepsis Only for SSI (MRSA and MSSA) and community acquired pneumonia (not MRSA) Overuse may well lead to resistance Q 12 hr dose may be suboptimal for sepsis
42 Removable focus Retaining an IV foreign body greatly reduces probability for cure ideally remove infected devices Presence of cardiac devices decrease cure rate Chamis AL, et al. Circulation 2001; 104:1029
43 Patients who have a removable focus may be treated with a 14 day course of IV ABX Rx if all of the following are present: Blood cultures clear within 4 days of onset Rx No valvular abnormalities No indwelling devices: prosthetic joints, heart valves or vascular grafts No evidence for metastatic infection
44 All others should receive 4-6 wks IV ABX Rx Multiple studies conclude that patients with SAB have improved outcomes with an ID consult Forsblom E, et al. CID 2013;56:527 Jenkins TC, et al. CID 2008; 46:1000 Honda H, et al. Am J Med 2010;123:631 Lahey T, et al. Medicine 2009; 88: 263

45
46
Asyntomatic bacteriuria, Urinary Tract Infection
 Asyntomatic bacteriuria, Urinary Tract Infection C. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asyntomatic Bacteriuria in Adults (2005) Pyuria accompanying asymptomatic
Asyntomatic bacteriuria, Urinary Tract Infection C. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asyntomatic Bacteriuria in Adults (2005) Pyuria accompanying asymptomatic
MICHIGAN MEDICINE GUIDELINES FOR TREATMENT OF URINARY TRACT INFECTIONS IN ADULTS
 When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
Clostridium difficile Infection (CDI) Management Guideline
 Management Guideline") Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Updated Clostridium difficile Treatment Guidelines
 Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
Clostridium difficile Infection: Diagnosis and Management
 Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
1/21/2016. Overview. Significance
 Asymptomatic Bacteriuria: Myths, Magic and Management Christopher Ohl MD Professor of Medicine, Section on Infectious Diseases Wake Forest School of Medicine, Winston Salem, NC Slide credits to Katie Wallace,
Asymptomatic Bacteriuria: Myths, Magic and Management Christopher Ohl MD Professor of Medicine, Section on Infectious Diseases Wake Forest School of Medicine, Winston Salem, NC Slide credits to Katie Wallace,
Stony Brook Adult Clostridium difficile Management Guidelines. Discontinue all unnecessary antibiotics
 Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013
 Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Clostridium Difficile Associated Disease. Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011
 Clostridium Difficile Associated Disease Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011 Introduction Which of the following is more common in community hospitals in the Southeast
Clostridium Difficile Associated Disease Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011 Introduction Which of the following is more common in community hospitals in the Southeast
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
UTI IN ELDERLY. Zeinab Naderpour
 UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Methicillin-Resistant Staphylococcus aureus (MRSA) S urveillance Report 2008 Background Methods
 S urveillance Report 2008 Background Methods") Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
ABSTRACT PURPOSE METHODS
 ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
EMPIRICAL TREATMENT OF SELECT INFECTIONS ADULT GUIDELINES. Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection
 URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
9/18/2018. Clostridium Difficile: Updates on Diagnosis and Treatment. Clostridium difficile Infection (CDI) Clostridium difficile Infection (CDI)
 Clostridium difficile Infection (CDI)") Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
All POOPed out: fecal microbiota transplant in C. difficile
 All POOPed out: fecal microbiota transplant in C. difficile SUSAN M. KELLIE, MD, MPH PROFESSOR OF INTERNAL MEDICINE DIVISION OF INFECTIOUS DISEASES UNIVERSITY OF NEW MEXICO SCHOOL OF MEDICINE HOSPITAL
All POOPed out: fecal microbiota transplant in C. difficile SUSAN M. KELLIE, MD, MPH PROFESSOR OF INTERNAL MEDICINE DIVISION OF INFECTIOUS DISEASES UNIVERSITY OF NEW MEXICO SCHOOL OF MEDICINE HOSPITAL
Urinary Tract Infections
 Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Nursing Infectious Diseases Topics. David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle
 Nursing Infectious Diseases Topics David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Clostridium difficile Free Access Via Web Source: Cohen SH,
Nursing Infectious Diseases Topics David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Clostridium difficile Free Access Via Web Source: Cohen SH,
Clostridium Difficile colitismore
 Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH
 The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
! Macrolide antibacterial. Fidaxomicin (Dificid ) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
 package labeling. Optimer Pharmaceuticals, Inc. May 2011.") Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Consideration of some other specific indications: Bacteremia
 European Medicines Agency Workshop on Antibacterials, London 7-8 February 2011 Consideration of some other specific indications: Bacteremia Harald Seifert Institut für Medizinische Mikrobiologie, Immunologie
European Medicines Agency Workshop on Antibacterials, London 7-8 February 2011 Consideration of some other specific indications: Bacteremia Harald Seifert Institut für Medizinische Mikrobiologie, Immunologie
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE
 ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
Case 1. Which of the following would be next appropriate investigation/s regarding the pts diarrhoea?
 Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acinetobacter baumannii, carbapenem-resistant, 497 498 Adolescents, urinary tract infections in, 520 521 Aminoglycosides, for UTIs and
Index Note: Page numbers of article titles are in boldface type. A Acinetobacter baumannii, carbapenem-resistant, 497 498 Adolescents, urinary tract infections in, 520 521 Aminoglycosides, for UTIs and
Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure
 Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure Brian S. Zuckerbraun, MD, FACS Henry T. Bahnson Professor of Surgery University of Pittsburgh Chief, Trauma
Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure Brian S. Zuckerbraun, MD, FACS Henry T. Bahnson Professor of Surgery University of Pittsburgh Chief, Trauma
CLOSTRIDIUM DIFICILE. Negin N Blattman Infectious Diseases Phoenix VA Healthcare System
 CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
ASK THE ID SPECIALIST
 ASK THE ID SPECIALIST Raymond E. Pontzer, MD, FACP Chief, Infectious Diseases UPMC St. Margaret Hospital Interim Medical Director of Infection Prevention for UPMC I have no conflict of interest with any
ASK THE ID SPECIALIST Raymond E. Pontzer, MD, FACP Chief, Infectious Diseases UPMC St. Margaret Hospital Interim Medical Director of Infection Prevention for UPMC I have no conflict of interest with any
Update on Clostridium difficile infection.
 Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
Hospital-wide Impact of Mandatory Infectious Disease Consultation on Staphylococcus aureus Septicemia
 Hospital-wide Impact of Mandatory Infectious Disease Consultation on Staphylococcus aureus Septicemia Amanda Guth 1 Amy Slenker MD 1,2 1 Department of Infectious Diseases, Lehigh Valley Health Network
Hospital-wide Impact of Mandatory Infectious Disease Consultation on Staphylococcus aureus Septicemia Amanda Guth 1 Amy Slenker MD 1,2 1 Department of Infectious Diseases, Lehigh Valley Health Network
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE
 EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018
 Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
What s New for Clostridium difficile John Lynch MD MPH Harborview Medical Center University of Washington
 What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
URINARY TRACT INFECTIONS
 URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
! MQ is a 44 year old woman that I first saw in Sept ! In MVA in Jan 2003 requiring spinal surgery
 Case MQ is a 44 year old woman that I first saw in Sept 2006 UPDATE ON CLOSTRIDIUM DIFFICILE DISEASE Richard A. Jacobs, M.D.,PhD In MVA in Jan 2003 requiring spinal surgery Subsequently developed fecal
Case MQ is a 44 year old woman that I first saw in Sept 2006 UPDATE ON CLOSTRIDIUM DIFFICILE DISEASE Richard A. Jacobs, M.D.,PhD In MVA in Jan 2003 requiring spinal surgery Subsequently developed fecal
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Infections Amenable to OPAT. (Nabin Shrestha + Ajay Mathur)
") 3 Infections Amenable to OPAT (Nabin Shrestha + Ajay Mathur) Decisions regarding outpatient treatment of infections vary with the institution, the prescribing physician, the individual patient s condition
3 Infections Amenable to OPAT (Nabin Shrestha + Ajay Mathur) Decisions regarding outpatient treatment of infections vary with the institution, the prescribing physician, the individual patient s condition
CATHETER-ASSOCIATED URINARY TRACT INFECTIONS
 CATHETER-ASSOCIATED URINARY TRACT INFECTIONS Hamid Emadi M.D Associate professor of Infectious diseases Department Tehran university of medical science The most common nosocomial infection The urinary
CATHETER-ASSOCIATED URINARY TRACT INFECTIONS Hamid Emadi M.D Associate professor of Infectious diseases Department Tehran university of medical science The most common nosocomial infection The urinary
Update in diagnosis and management of UTIs
 Update in diagnosis and management of UTIs I have no disclosures Brian S. Schwartz, MD UCSF, Division of Infectious Diseases Lecture outline Challenges in cystitis Complicated UTI/pyelonephritis Asymptomatic
Update in diagnosis and management of UTIs I have no disclosures Brian S. Schwartz, MD UCSF, Division of Infectious Diseases Lecture outline Challenges in cystitis Complicated UTI/pyelonephritis Asymptomatic
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate
 Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Clostridiodes Difficile Colitis: Update on Guidelines. Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018
 Clostridiodes Difficile Colitis: Update on Guidelines Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018 Outline Overview of CDI Diagnosis of C Difficile- updates Infection Prevention
Clostridiodes Difficile Colitis: Update on Guidelines Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018 Outline Overview of CDI Diagnosis of C Difficile- updates Infection Prevention
Star Articles in Review
 Star Articles in Review CDDW/CASL Meeting Toronto, February 10, 2014 Christina M. Surawicz, MD MACG Professor of Medicine Division of Gastroenterology Department of Medicine University of Washington Disclosure
Star Articles in Review CDDW/CASL Meeting Toronto, February 10, 2014 Christina M. Surawicz, MD MACG Professor of Medicine Division of Gastroenterology Department of Medicine University of Washington Disclosure
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine
 Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
Brice Taylor Assistant Professor Division of Pulmonary and Critical Care Medicine Discuss advances in predicting prognosis Understand dwhat we know (and don t know) about the Microbiology Recognize important
What s new in Infectious Diseases. Petronella Adomako, MD Infectious Disease Specialist Mckay-Dee Hospital
 What s new in Infectious Diseases Petronella Adomako, MD Infectious Disease Specialist Mckay-Dee Hospital None Disclosures Objectives New information in infectious diseases. New diseases and outbreaks.
What s new in Infectious Diseases Petronella Adomako, MD Infectious Disease Specialist Mckay-Dee Hospital None Disclosures Objectives New information in infectious diseases. New diseases and outbreaks.
Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association
 Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association Els Vandecasteele, Jan De Waele, Dominique Vandijck, Stijn Blot, Dirk
Antimicrobial prophylaxis in liver transplant A multicenter survey endorsed by the European Liver and Intestine Transplant Association Els Vandecasteele, Jan De Waele, Dominique Vandijck, Stijn Blot, Dirk
Treatment of febrile neutropenia in patients with neoplasia
 Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
Treatment of febrile neutropenia in patients with neoplasia George Samonis MD, PhD Medical Oncologist Infectious Diseases Specialist Professor of Medicine The University of Crete, Heraklion,, Crete, Greece
C. difficile: When to Do Fecal Microbiota Transplant (FMT)
") C. difficile: When to Do Fecal Microbiota Transplant (FMT) Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
C. difficile: When to Do Fecal Microbiota Transplant (FMT) Lawrence J. Brandt, MD, MACG Emeritus Chief, Gastroenterology Montefiore Medical Center Professor of Medicine and Surgery Albert Einstein College
Modern approach to Clostridium Difficile Infection
 Modern approach to Clostridium Difficile Infection Pseudomembranous Colitis: Principles for diagnosis and treatment Aggelos Stefos Internist, Infectious diseases Specialist Department of Medicine and Research
Modern approach to Clostridium Difficile Infection Pseudomembranous Colitis: Principles for diagnosis and treatment Aggelos Stefos Internist, Infectious diseases Specialist Department of Medicine and Research
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program
 Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Clostridium difficile: Can you smell the new updates?
 Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
Fecal transplantation as a treatment option for recurrent Clostridium difficile infection
 Fecal transplantation as a treatment option for recurrent Clostridium difficile infection Josbert Keller Department of Gastroenterology Haga Teaching Hospital, The Hague Case: 81 yrs, CVA, recurrent UTI,
Fecal transplantation as a treatment option for recurrent Clostridium difficile infection Josbert Keller Department of Gastroenterology Haga Teaching Hospital, The Hague Case: 81 yrs, CVA, recurrent UTI,
Infectious Disease in the Critically Ill Patient
 Infectious Disease in the Critically Ill Patient Heather L. Evans, MD MS FACS Director of Surgical Infectious Disease Harborview Medical Center Asst. Professor UW Department of Surgery New Antibiotics:
Infectious Disease in the Critically Ill Patient Heather L. Evans, MD MS FACS Director of Surgical Infectious Disease Harborview Medical Center Asst. Professor UW Department of Surgery New Antibiotics:
Probiotics for Primary Prevention of Clostridium difficile Infection
 Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS
 PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS SITI HIR HURAIZAH MD TAHIR Bpharm (UKM), MSc (Clinical Microbiology) (UoN) CLINICAL PHARMACIST HOSPITAL MELAKA WHY STUDY PHARMACOKINETICS (PK) AND PHARMACODYNAMICS
PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS SITI HIR HURAIZAH MD TAHIR Bpharm (UKM), MSc (Clinical Microbiology) (UoN) CLINICAL PHARMACIST HOSPITAL MELAKA WHY STUDY PHARMACOKINETICS (PK) AND PHARMACODYNAMICS
Terapia dell infezione da Clostridium difficile. Massimo Coen I Div Mal Inf AO L Sacco
 Terapia dell infezione da Clostridium difficile Massimo Coen I Div Mal Inf AO L Sacco Disease Severity Mild CDI 3 5 BM/day WBC 15,000/mm 3 Defining CDI Disease Severity Mild abdominal pain due to CDI Moderate
Terapia dell infezione da Clostridium difficile Massimo Coen I Div Mal Inf AO L Sacco Disease Severity Mild CDI 3 5 BM/day WBC 15,000/mm 3 Defining CDI Disease Severity Mild abdominal pain due to CDI Moderate
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Outline. Cryptococcosis Pneumocystosis Diarrhea. Case Histories: HIV Related- Opportunistic Infections in 2015
 AU Edited: 05/06/15 Case Histories: HIV Related- Opportunistic Infections in 2015 Henry Masur, MD Clinical Professor of Medicine George Washington University School of Medicine Bethesda, Maryland Washington,
AU Edited: 05/06/15 Case Histories: HIV Related- Opportunistic Infections in 2015 Henry Masur, MD Clinical Professor of Medicine George Washington University School of Medicine Bethesda, Maryland Washington,
No Need to Agonize! Tips for the Diagnosis and Treatment of Complicated UTIs
 ASCENSION TEXAS No Need to Agonize! Tips for the Diagnosis and Treatment of Complicated UTIs Austin Area Society of Health-System Pharmacists April 26, 2018 Amy Carr, PharmD PGY-2 Infectious Diseases Pharmacy
ASCENSION TEXAS No Need to Agonize! Tips for the Diagnosis and Treatment of Complicated UTIs Austin Area Society of Health-System Pharmacists April 26, 2018 Amy Carr, PharmD PGY-2 Infectious Diseases Pharmacy
Treatment Regimens for Bacterial Urinary Tract Infections. Characteristic Pathogen. E. coli, S.saprophyticus P.mirabilis, K.
 HEALTHSPAN URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12, 4-14 Key Stakeholders: IM, Urology, Next Review:
HEALTHSPAN URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12, 4-14 Key Stakeholders: IM, Urology, Next Review:
TMP/SMZ DS Ciprofloxacin Norfloxacin Ofloxacin Cefadroxil * 30 Amoxicilin 86* 19 25
 Evidence-Based Evaluation and Treatment of UTI UTI Prevalence Leslee L. Subak, MD Associate Professor Obstetrics, Gynecology & RS Epidemiology & Biostatistics University of California, San Francisco 50%
Evidence-Based Evaluation and Treatment of UTI UTI Prevalence Leslee L. Subak, MD Associate Professor Obstetrics, Gynecology & RS Epidemiology & Biostatistics University of California, San Francisco 50%
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
Infective Endocarditis Empirical therapy Antibiotic Guidelines. Contents
 Infective Endocarditis Empirical therapy Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Group Additional author(s): as above Authors Division: Division of Clinical
Infective Endocarditis Empirical therapy Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Group Additional author(s): as above Authors Division: Division of Clinical
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH)
") Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
Rochester Patient Safety C. difficile Prevention Collaborative: Long Term Care Antimicrobial Stewardship (funded by NYSDOH) Clinical Practice Guideline* for the Diagnosis and Management of Acute Bacterial
What's New in Infectious Diseases Pharmacotherapy?
 Disclosure What's New in Infectious Diseases Pharmacotherapy? Nothing to Disclose Douglas Slain, Pharm.D., BCPS, FCCP, FASHP Associate Professor Infectious Diseases Clinical Specialist West Virginia University
Disclosure What's New in Infectious Diseases Pharmacotherapy? Nothing to Disclose Douglas Slain, Pharm.D., BCPS, FCCP, FASHP Associate Professor Infectious Diseases Clinical Specialist West Virginia University
Updates to pharmacological management in the prevention of recurrent Clostridium difficile
 Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Preventing & Controlling the Spread of Infection
 Preventing & Controlling the Spread of Infection Contributors: Alice Pong M.D., Hospital Epidemiologist Chris Abe, R.N., Senior Director Ancillary and Support Services Objectives Review the magnitude of
Preventing & Controlling the Spread of Infection Contributors: Alice Pong M.D., Hospital Epidemiologist Chris Abe, R.N., Senior Director Ancillary and Support Services Objectives Review the magnitude of
Patient Safety Summit 2014
 Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
CLINICAL USE OF GLYCOPEPTIDES. Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel
 CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
CLINICAL USE OF GLYCOPEPTIDES Herbert Spapen Intensive Care Department University Hospital Vrije Universiteit Brussel Glycopeptides Natural Vancomycin introduced in 1958 Teicoplanin introduced in Europe
Infections In Cirrhotic patients. Dr Abid Suddle Institute of Liver Studies King s College Hospital
 Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
Infections In Cirrhotic patients Dr Abid Suddle Institute of Liver Studies King s College Hospital Infection in cirrhotic patients Leading cause morbidity/mortality Common: 30-40% of hospitalised cirrhotic
OHSU URGE OVERKILL - UTIS GRAEME FORREST, MBBS, FIDSA ASSOCIATE PROFESSOR OF MEDICINE VA PORTLAND HEALTHCARE SYSTEM AND OHSU
 URGE OVERKILL - UTIS GRAEME FORREST, MBBS, FIDSA ASSOCIATE PROFESSOR OF MEDICINE VA PORTLAND HEALTHCARE SYSTEM AND DISCLOSURES NOTHING TO DISCLOSE THE INFORMATION PRESENTED IS MY MINE AND NOT A RECOMMENDATION
URGE OVERKILL - UTIS GRAEME FORREST, MBBS, FIDSA ASSOCIATE PROFESSOR OF MEDICINE VA PORTLAND HEALTHCARE SYSTEM AND DISCLOSURES NOTHING TO DISCLOSE THE INFORMATION PRESENTED IS MY MINE AND NOT A RECOMMENDATION
Cubicin A Guide to Dosing
 Cubicin A Guide to Dosing Cubicin (Daptomycin) powder for solution for injection or infusion Indications (see SmPC) 1 : Cubicin is indicated for the treatment of the following infections (see sections
Cubicin A Guide to Dosing Cubicin (Daptomycin) powder for solution for injection or infusion Indications (see SmPC) 1 : Cubicin is indicated for the treatment of the following infections (see sections
Development of Drugs for Bacteremia
 Development of Drugs for Bacteremia Charles Knirsch, MD, MPH VP, Clinical Research Pfizer Inc 1 Bacteremia Guidance Issues EMA guidance suggests that bacteremia is not a primary diagnosis but represents
Development of Drugs for Bacteremia Charles Knirsch, MD, MPH VP, Clinical Research Pfizer Inc 1 Bacteremia Guidance Issues EMA guidance suggests that bacteremia is not a primary diagnosis but represents
Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured
 9 million visits/year! Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured Interpretation of the culture result has been controversial-
9 million visits/year! Customary urine test is the dip stick and the mid-stream culture of voided urine. Up to 77% of cystitis cases are cultured Interpretation of the culture result has been controversial-
PATIENT DEMOGRAPHICS. Surname. Given name. Pacific Islander (non-maori) ADMISSION DETAILS
 ADMISSION DETAILS") Reviewer / hospital Date review started PATIENT DEMOGRAPHICS MRN DOB Sex Patient sticky label if available, else enter details here Surname Post-code Given name Australian Aborigine / TSI Middle Eastern
Reviewer / hospital Date review started PATIENT DEMOGRAPHICS MRN DOB Sex Patient sticky label if available, else enter details here Surname Post-code Given name Australian Aborigine / TSI Middle Eastern
D DAVID PUBLISHING. 1. Introduction. Kathryn Koliha 1, Julie Falk 1, Rachana Patel 1 and Karen Kier 2
 Journal of Pharmacy and Pharmacology 5 (2017) 607-615 doi: 10.17265/2328-2150/2017.09.001 D DAVID PUBLISHING Comparative Evaluation of Pharmacist-Managed Vancomycin Dosing in a Community Hospital Following
Journal of Pharmacy and Pharmacology 5 (2017) 607-615 doi: 10.17265/2328-2150/2017.09.001 D DAVID PUBLISHING Comparative Evaluation of Pharmacist-Managed Vancomycin Dosing in a Community Hospital Following
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review
 Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal catastrophes in ICU, 1017 1044. See also specific types, e.g., Abdominal compartment syndrome treatment of, 1032 1037 antimicrobial,
Index Note: Page numbers of article titles are in boldface type. A Abdominal catastrophes in ICU, 1017 1044. See also specific types, e.g., Abdominal compartment syndrome treatment of, 1032 1037 antimicrobial,
Urinary Tract Infections: From Simple to Complex. Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014
 Urinary Tract Infections: From Simple to Complex Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014 Learning Objectives Develop empiric antimicrobial treatment
Urinary Tract Infections: From Simple to Complex Adriane N Irwin, MS, PharmD, BCACP Clinical Assistant Professor Ambulatory Care October 25, 2014 Learning Objectives Develop empiric antimicrobial treatment
Investigators Meeting
 Outcomes of Urinary Tract Infection Management by Pharmacists (R x OUTMAP) Investigators Meeting June 11, 2017 Overview 1. Introductions and Opening Remarks 2. Epidemiology and Definitions 3. UTI Assessment
Outcomes of Urinary Tract Infection Management by Pharmacists (R x OUTMAP) Investigators Meeting June 11, 2017 Overview 1. Introductions and Opening Remarks 2. Epidemiology and Definitions 3. UTI Assessment
Antibiotic Consumption in the Community in Ireland REPORT FOR First Half of 2013
 Antibiotic Consumption in the Community in Ireland REPORT FOR First Half of 2013 1 Summary: Community Antibiotic Use The rate for Quarter 1 of 2013 (1 st January to 31 st March) was 27.4 Defined Daily
Antibiotic Consumption in the Community in Ireland REPORT FOR First Half of 2013 1 Summary: Community Antibiotic Use The rate for Quarter 1 of 2013 (1 st January to 31 st March) was 27.4 Defined Daily
Responders as percent of overall members in each category: Practice: Adult 537 (51% of 1063 members) 23 (59% of 39 members)
 23 (59% of 39 members)") Infectious Diseases Society of America Emerging Infections Network Report for Query: Antibiotic Allergies and Infectious Disease Practice Overall response rate: 744/1411 (52.7%) physicians responded from
Infectious Diseases Society of America Emerging Infections Network Report for Query: Antibiotic Allergies and Infectious Disease Practice Overall response rate: 744/1411 (52.7%) physicians responded from
Long-Term Care Updates
 Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA
 The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA Franklin D. Lowy, MD Columbia University College of Physicians & Surgeons New York, NY Topics to Be Covered Background Some
The Curious Intersection of HIV and Staphylococcus aureus with a Focus on MRSA Franklin D. Lowy, MD Columbia University College of Physicians & Surgeons New York, NY Topics to Be Covered Background Some
NEW DEVELOPMENTS AND CHALLENGING CASES IN HOSPITAL INFECTIOUS DISEASES
 Lisa G. Winston, MD Professor, University of California, San Francisco Vice Chief, Inpatient Medical Services and Hospital Epidemiologist, San Francisco General Hospital NEW DEVELOPMENTS AND CHALLENGING
Lisa G. Winston, MD Professor, University of California, San Francisco Vice Chief, Inpatient Medical Services and Hospital Epidemiologist, San Francisco General Hospital NEW DEVELOPMENTS AND CHALLENGING
Renal Unit. Catheter Related Bacteraemia Guidelines
 Renal Unit Policy Manager Drew Henderson Policy Group Renal Unit Policy Established 21/01/2014 Policy Review Period/Expiry 21/01/2015 Last Updated 21/01/2014 This policy does apply to Medical/Dental Staff
Renal Unit Policy Manager Drew Henderson Policy Group Renal Unit Policy Established 21/01/2014 Policy Review Period/Expiry 21/01/2015 Last Updated 21/01/2014 This policy does apply to Medical/Dental Staff
Daptomycin in Clinical Practice. Paolo Grossi
 Clinica delle Malattie Infettive e Tropicali Università degli Studi dell Insubria Ospedale di Circolo e Fondazione Macchi, Varese Second Opinion Infettivologica Centro Nazionale Trapianti, ISS, Roma Daptomycin
Clinica delle Malattie Infettive e Tropicali Università degli Studi dell Insubria Ospedale di Circolo e Fondazione Macchi, Varese Second Opinion Infettivologica Centro Nazionale Trapianti, ISS, Roma Daptomycin
December 3, 2015 Severe Sepsis and Septic Shock Antibiotic Guide
 Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Severe Sepsis and Septic Shock Antibiotic Guide Surviving Sepsis: The choice of empirical antimicrobial therapy depends on complex issues related to the patient s history, including drug intolerances,
Warren S Joseph, DPM, FIDSA Roxborough Memorial Hospital Philadelphia, PA. Special Thanks to: Mark A Kosinski, DPM, FIDSA
 Warren S Joseph, DPM, FIDSA Roxborough Memorial Hospital Philadelphia, PA Special Thanks to: Mark A Kosinski, DPM, FIDSA Speaking on surgical prophylaxis is an exercise in futility since, frankly, none
Warren S Joseph, DPM, FIDSA Roxborough Memorial Hospital Philadelphia, PA Special Thanks to: Mark A Kosinski, DPM, FIDSA Speaking on surgical prophylaxis is an exercise in futility since, frankly, none
Staphylococcal Bacteremia
 Staphylococcal Bacteremia Henry F. Chambers, M.D. Professor of Medicine, UCSF Chief of Infectious Diseases San Francisco General Hospital Case 1 38 y/o man, new CHF, alcoholic cardiomyopathy, Hct = 13
Staphylococcal Bacteremia Henry F. Chambers, M.D. Professor of Medicine, UCSF Chief of Infectious Diseases San Francisco General Hospital Case 1 38 y/o man, new CHF, alcoholic cardiomyopathy, Hct = 13
Nicola Petrosillo Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani, IRCCS Roma. L infezione da C difficile grave o complicata
 Nicola Petrosillo Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani, IRCCS Roma L infezione da C difficile grave o complicata Bagdasarian N et al. JAMA 2015; 313: 398-408 European Society
Nicola Petrosillo Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani, IRCCS Roma L infezione da C difficile grave o complicata Bagdasarian N et al. JAMA 2015; 313: 398-408 European Society
KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE)
") KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12 Key Stakeholders: IM, Urology, Next
KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12 Key Stakeholders: IM, Urology, Next
Responders as percent of overall members in each category: Region: New England 50 (57% of 87 members) 46 (57% of 81 members) 21 (55% of 38 members)
 46 (57% of 81 members) 21 (55% of 38 members)") Infectious Diseases Society of America Emerging Infections Network Report for Query: Recurrent C. difficile Infections (CDI) Overall response rate: 621/1212 (51.2%) physicians responded from 09/26/12 to
Infectious Diseases Society of America Emerging Infections Network Report for Query: Recurrent C. difficile Infections (CDI) Overall response rate: 621/1212 (51.2%) physicians responded from 09/26/12 to
Antimicrobial Stewardship and Urinary Tract Infections
 Antimicrobial Stewardship and Urinary Tract Infections Samantha Loutzeheiser, PharmD, BCPS Andrea Pallotta, PharmD, BCPS (AQ-ID), AAHIVP Cleveland Clinic Medina Hospital Cleveland Clinic Main Campus Objectives
Antimicrobial Stewardship and Urinary Tract Infections Samantha Loutzeheiser, PharmD, BCPS Andrea Pallotta, PharmD, BCPS (AQ-ID), AAHIVP Cleveland Clinic Medina Hospital Cleveland Clinic Main Campus Objectives
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Top Curbside Consult Questions in Inpatient ID
 Top Curbside Consult Questions in Inpatient ID Management of the Hospitalized Patient October 2014 Jennifer Babik, MD, PhD Assistant Clinical Professor Division of Infectious Diseases, UCSF Disclosures
Top Curbside Consult Questions in Inpatient ID Management of the Hospitalized Patient October 2014 Jennifer Babik, MD, PhD Assistant Clinical Professor Division of Infectious Diseases, UCSF Disclosures
declara&ons Clostridium difficile infec&on. Time to wake up and smell the..., um, nevermind. OK, next slide please. Bruce Dalton, BScPhm. PharmD.
 Clostridium difficile infec&on. Time to wake up and smell the..., um, nevermind. OK, next slide please. Bruce Dalton, BScPhm. PharmD. declara&ons No financial disclosures Personal acquaintance, co- worker,
Clostridium difficile infec&on. Time to wake up and smell the..., um, nevermind. OK, next slide please. Bruce Dalton, BScPhm. PharmD. declara&ons No financial disclosures Personal acquaintance, co- worker,
ESCMID Online Lecture Library. by author
 Hospital Universitario Virgen Macarena, Seville New drugs against MRSA and VRE L. Eduardo López Cortés Seville, 8th July Tedizolid Oxazolidinone Ceftaroline // Ceftobiprole 5 th gen cephalosporin Overview
Hospital Universitario Virgen Macarena, Seville New drugs against MRSA and VRE L. Eduardo López Cortés Seville, 8th July Tedizolid Oxazolidinone Ceftaroline // Ceftobiprole 5 th gen cephalosporin Overview
Clostridium difficile infections: Drug treatment re-evaluated
 Clostridium difficile infections: Drug treatment re-evaluated Kimberly D. Leuthner, PharmD University Medical Center of Southern Nevada August 11, 2016 Random Fact: The human body has 10 13 human cells
Clostridium difficile infections: Drug treatment re-evaluated Kimberly D. Leuthner, PharmD University Medical Center of Southern Nevada August 11, 2016 Random Fact: The human body has 10 13 human cells