Waldenström s Macroglobulinemia: Treatment Approach
|
|
|
- Noah Harmon
- 5 years ago
- Views:
Transcription



1 Waldenström s Macroglobulinemia: Treatment Approach Steve Treon MD, PhD Bing Center for Waldenstrom s Macroglobulinemia Dana Farber Cancer Institute Harvard Medical School
2 Primary Therapy of WM with Rituximab Regimen ORR VGPR/CR TTP (mo) Rituximab x % 0-5% 13 Rituximab x % 5-10% Rituximab/thalidomide 70% 10% 30 Rituximab/cyclophosphamide i.e. CHOP-R, CVP-R, CPR, CDR Rituximab/nucleoside analogues i.e. FR, FCR, CDA-R Rituximab/Proteasome Inhibitor i.e. BDR, VR, CaRD 70-80% 20-25% % 20-30% % 20-40% Rituximab/bendamustine 90% 30-40% 69 Reviewed in Dimopoulos et al, Blood 2014; 124(9): ; Treon et al, Blood 2015; How I Treat WM
3 WM centric toxicities with commonly used therapies Agent WM Toxicities Rituximab IgM flare (40-60%)-> Hyperiscosity crisis, Aggravation of IgM related PN, CAGG, Cryos. Hypogammaglobulinemia-> infections, IVIG Intolerance (10-15%) Fludarabine Hypogammaglobulinemia-> infections, IVIG Transformation, AML/MDS (15%) Bendamustine Prolonged neutropenia, thrombocytopenia (especially after fludarabine) AML/MDS (5-8%) Bortezomib Grade 2+3 Peripheral neuropathy (60-70%); High discontinuation (20-60%)






4 Pro-Survival Signaling Driven by Mutated MYD88 in Waldenström's Macroglobulinemia MYD88 mutations 95-97% WM TLRs/IL-1R Ibrutinib IL-6R IL-6 IL-6 IL-6 IBTK del6q21-25 MYD88 BTK BTK IRAK4 IRAK1 TRAF6 PLCγ PKC HCK PIK3R2 PI3K gp-130 Ibrutinib Acalabrutinib BGB-3111 SNS-062 TAK1 NEMO IKKα IKKβ MEK MAPKs ERK AKT mtor HCK IL-6 Degradation TNFAIP3 HIVEP2 NFKB growth survival Yang et al, Blood 2013 Yang et al, Blood 2016 Hunter et al, Blood 2014 Hunter et al, JCO 2017 Guerrera et al, Haematologica 2018

5 Mutations in CXCR4 permit ongoing pro-survival signaling by CXCL12, the ligand for CXCR4 receptor. CXCR4 receptor remains up with mutation CXCL12 CXCR4 Bone Marrow Stroma WM Cell CXCR4 mutations in 30-40% WM Drug resistance

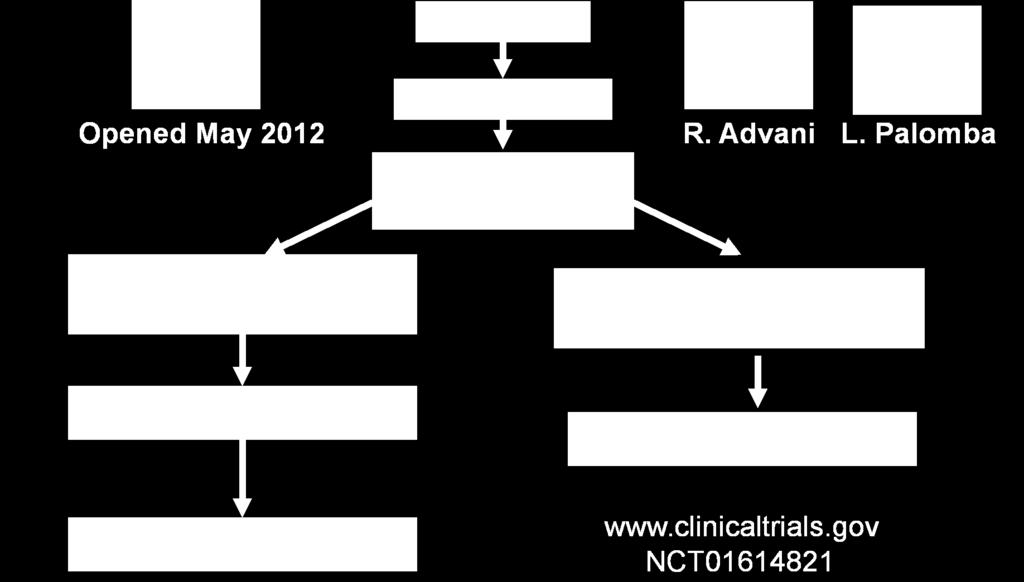


6 Multicenter study of Ibrutinib in Relapsed/Refractory WM (>1 prior therapy) NCT MYD88, CXCR4 Mutation Status
7 Responses to ibrutinib are impacted by MYD88 (L265P and non-l265p) and CXCR4 mutations. ALL MYD88 Mut CXCR4 WT MYD88 Mut CXCR4 Mut MYD88 WT CXCR4 WT N= * P-value ORR 91% 100% 85.7% 60% Major (>PR) 78% 97% 67% 0% <0.001 VGPR 29% 44% 10% 0% Time to Minor Response (mos.) Time to Major response (mos.) N/A 0.05 *2 patients at initial reporting with major responses were discovered subsequently to have MYD88 mutated disease (S243N, L265P). One patient at initial reporting was subsequently found to CXCR4 mutated disease upon genotyping of CD19- selected WM cells. Treon et al, EHA 2018
.")
8 Ibrutinib in Previously O Treated WM: Updated PFS All patients MYD88 and CXCR4 Status MYD88 MUTATED ONLY BOTH MYD88 AND CXCR4 MUTATED NO MYD88 OR CXCR4 MUTATIONS 5 year PFS: 60% (95% CI 46-71%). Treon et al, EHA 2018
 and in >5% IGG of immunoglobulins patients: Neutropenia (22%); Thrombocytopenia (14%), Pneumonia (9%);")
9 Original Study Ibrutinib Related Adverse Events in previously treated WM patients Toxicities >1 patient; N=63 22% (No change) 14% (No change) 5% to 11% with longer follow-up 2% to 8% with longer follow-up Number of Subjects with Toxicity Update on Adverse No impact Events on (Grade IGA >2) and in >5% IGG of immunoglobulins patients: Neutropenia (22%); Thrombocytopenia (14%), Pneumonia (9%); GERD (8%); Hypertension (8%); anemia (6%); and skin infection (5%). Seven patients (11%) had atrial arrhythmia [Grade 1 (n=1); Grade 2 (n=5); Grade 3 (n=1)], and 6 continued ibrutinib following medical management. Treon et al, EHA 2018



10 Ibrutinib Monotherapy in Symptomatic Treatment Naive WM R MYD88, CXCR4 Mutation Status NCT Treon et al, JCO 2018
11 Time to and depth of response to ibrutinib are impacted by CXCR4 mutations. All Patients MYD88 MUT CXCR4 WT MYD88 MUT CXCR4 MUT P-value N= N/A Overall Response Rate-no. (%) Major Response Rateno. (%) Categorical responses Minor responses-no. (%) Partial responses-no. (%) Very good partial responses-no. (%) 30 (100%) 16 (100%) 14 (100%) (83%) 15 (94%) 10 (71%) (17%) 1 (6%) 4 (29%) (63%) 10 (63%) 9 (64%) (20%) 5 (31%) 1 (7%) 0.18 Median time to response (months) Minor response ( Minor response) Major response ( Partial response) Data cutoff: Jan. 22, Median f/u: 14.6 (range months) Treon et al, JCO 2018
12 Adverse Events (>5%) Event or Total Grade 2 Grade 3 Grade 4 Abnormality Grades 2-4 Arthralgia 2 (7%) 0 (0%) 0 (0%) 2 (7%) Atrial fibrillation 3 (10%) 0 (0%) 0 (0%) 3 (10%) Bruising 2 (7%) 0 (0%) 0 (0%) 2 (7%) Hypertension 2 (7%) 2 (7%) 0 (0%) 4 (13%) Neutropenia 2 (7%) 0 (0%) 0 (0%) 2 (7%) Upper respiratory infection Urinary tract infection 2 (7%) 0 (0%) 0 (0%) 2 (7%) 2 (7%) 0 (0%) 0 (0%) 2 (7%) Minimal hematological toxicity Median serum IgA levels decreased from 62 to 39 mg/dl; p=0.04 Median serum IgG levels declined from 563 to 462; p=0.003 Afib medically managed in 2 patients who continue on treatment; cardiac ablation for one patient with left atrial enlargement off treatment. Treon et al, JCO 2018

13 O Ibrutinib Monotherapy in Frontline WM: PFS 18 mo: PFS 92%; All patients alive. PD patients were both CXCR4 mutated. Data cutoff: Jan. 22, 2018 Median f/u: 14.6 (range months) Treon et al, JCO 2018

14 Ibrutinib (560 mg/day) induced response in a WM patient with Bing Neel Syndrome Mason et al, BJH 2016
15 Acalabrutinib (ACP-196) in Treatment Naïve and Previously Treated WM Owen et al, ASCO 2018; EHA 2018

16 Acalabrutinib in WM Atrial fibrillation occurred in 3 pts (1 Gr 3). Bleeding events occurred in 57% of pts; 4 events were Gr 3/4: There were 5 Gr 5 events: pneumonia, glioblastoma multiforme, esophageal carcinoma, myocardial ischemia, and intracranial hematoma. Owen et al, ASCO 2018; EHA 2018

17 Zanubrutinib in WM Phase I/II Data 51 patients out of 67 evaluable for efficacy Genotyping unknown for many patients 91% PFS at 1 year Trotman et al, EHA 2018

18 Zanubrutinib in WM Trotman et al, EHA 2018
")

19 innovate Study in WM Treatment Naïve + Previously Treated 45 centers in 9 countries 1:1 Randomization N = 150 ARM A: ibrutinib 420mg + Rituximab 375mg/m 2 x 8 infusions (weeks 1,2,3,4,17,18,19, and 20) ARM B: Placebo + Rituximab 375mg/m 2 x 8 infusions (weeks 1,2,3,4,17,18,19, and 20) N=31 ARM C: ibrutinib 420mg Subjects considered refractory to prior rituximab ABC patients genotyped for MYD88 and CXCR4
20 Responses in Innovate AB Study: Update Best Response (%) Overall ORR 95% Major 79% ORR 48% 3 1 Major 29 33% Ibrutinib Placebo -RTX -RTX MYD88 L265P /CXCR4 WT MYD88 L265P /CXCR4 WHIM MYD88 WT /CXCR4 WT ORR 100% Major 94% ORR 46% 6 Major 23 29% Ibrutinib Placebo -RTX -RTX ORR 96% Major 73% ORR 57% Ibrutinib Placebo -RTX -RTX Major 48% ORR 91% 27 36?? Major 64% ORR 56% Ibrutinib Placebo -RTX -RTX Major 33% CR VGPR PR MR Median time to PR, months (range) 2 (1 28) 6 (2 26) 2 (1 28) 5 (2 17) 3 (1 19) 11 (4 18) 6 (1 17) 6 (5 26) Median time to MR, months (range) 1 (1 18) 3 (1 24) 1 (1 18) 3 (1 24) a Following modified 6th IWWM Response Criteria (NCCN 2014); required two consecutive assessments. 1 (1 11) 3 (1 8) 2 (1-17) 3 (2 17) Busket et al, ASH 2018

21 Progression-Free Survival Benefit With Ibrutinib- RTX Independent of MYD88/CXCR4 Genotype Progression-Free Survival (%) MYD88 L265P /CXCR4 WT MYD88 WT /CXCR4 WT MYD88 L265P /CXCR4 WHIM MYD88 WT /CXCR4 WT MYD88 L265P /CXCR4 WT MYD88 L265P /CXCR4 WHIM Ibrutinib-RTX Placebo-RTX Improved PFS across all genotypes with ibrutinib-rtx 36-month PFS rates MYD88 L265P /CXCR4 W T : 84% vs 29% MYD88 L265P /CXCR4 W HIM : 64% vs 26% MYD88 WT /CXCR4 WT : 82% vs 44% Months Innovate AB Data: Busket et al, ASH 2018.



22 Phase I/II Trial of Ulocuplumab and Ibrutinib in CXCR4 mutated patients with symptomatic WM Schema Ibrutinib Until PD or Intolerance Weekly Ulo 4 weeks Biweekly Ulo 20 weeks STOP Dose Level Ibrutinib Ulocuplumab Cycle 1 Ulocuplumab Cycles 2-6 Level 1 Starting dose 420mg PO DQ 400 mg weekly 800 mg every other week Level 2 420mg PO DQ 800 mg weekly 1200 mg every other week Level 3 420mg PO DQ 800 mg weekly 1600 mg every other week ClinicalTrials.gov Identifier: NCT032

23 Venetoclax (ABT-199) impacted by CXCR4 mutation Cao et al, BJH 2015
24 Phase II Study of Venetoclax in Previously Treated WM Selected inclusion criteria: Clinicopathological diagnosis of WM Serum IgM >2 x ULN Previously treated Age 18 years Good performance Normal organ and marrow function Screening Informed Consent and Registration Venetoclax 200 mg PO QD Selected exclusion criteria: Serious medical condition Concurrent anticancer agent Known CNS lymphoma Active HIV, HBV, HCV infection Lactating or pregnant women Progressive Disease or Unacceptable Toxicity 800 mg PO QD SD or Response Continue for 2 years Stop ABT-199 Event Monitoring NCT Castillo et al. EHA 2018
25 Phase II Study of Venetoclax in Previously Treated WM Baseline characteristics Characteristic Number (%) Age, years 66 (39-80) Male sex 17 (57%) Previous treatments 2 (1-10) Prior BTK inhibitors 15 (50%) MYD88 L265P 30 (100%) CXCR4 mutations 16 (53%) Serum IgM level (mg/dl) 3,543 (642-7,970) Hemoglobin level (g/dl) 10.6 ( ) Platelet count (K/ul) 222 (7-445) Lymphadenopathy 9 (30%) Splenomegaly 6 (20%) Castillo et al. EHA 2018
26 Phase II Study of Venetoclax in Previously Treated WM Response No prior ibrutinib (n=15) Prior ibrutinib (n=15) Overall 14 (93%) 12 (80%) Major 13 (87%) 9 (60%) Very good 4 (27%) 1 (7%) Partial 9 (60%) 8 (53%) Minor 1 (7%) 3 (20%) Stable 1 (7%) 3 (20%) CXCR4 WT (n=14) CXCR4 MUT (n=16) 12 (86%) 14 (87%) 9 (86%) 13 (63%) 4 (29%) 1 (7%) 8 (57%) 9 (56%) 0 (0%) 4 (25%) 2 (14%) 2 (13%) Median follow-up: 11 months 1 patient had progressive disease at 9 months (MYD88, CXCR4, TP53) Castillo et al. EHA 2018


27 Phase II Study of Venetoclax in Previously Treated WM Laboratory TLS (n=1). No IgM flare. No deaths. Castillo et al. EHA 2018

")
28 Ibrutinib and Venetoclax in Treatment Naïve WM 24 months Ibrutinib 420 mg/day x 4 weeks Ibrutinib 420 mg/day Add Venetoclax 100 mg/day week mg/day week mg/day weeks 7,8 Ibrutinib 420 mg/day And Venetoclax 400 mg/day Observation 4 weeks 4 weeks 22 months Follow to PD or off study Jorge Castillo, PI (DFCI)
29 Approach to Frontline Therapy of Symptomatic WM Hyperviscosity, Severe Cryos, CAGG, PN Plasmapheresis MYD88 Mutated/No CXCR4 mutation No bulky disease, no contraindications Ibrutinib (if available) Bulky disease Benda-R +Ibrutinib and Rituximab Amyloidosis Bortezomib/Dex/Rituximab (BDR) IgM Peripheral Neuropathy Rituximab + Alkylator MYD88 Mutated/CXCR4 mutation +Ibrutinib and Rituximab Same caveats as above If immediate response needed, either BDR or Benda-R MYD88 Wild-Type non-l265p MYD88 mutations BDR > Benda-R Hunter et al, JCO 2017; LeBlond IWWM10 Hold Rituximab until IgM <4000 mg/dl or empiric pheresis is performed. Consider Maintenance Rituximab Consider Ofatumumab if R intolerant.
30 Salvage Therapy of Symptomatic WM Consider repeat primary therapy if response >2 years MYD88 Mutated/No CXCR4 mutation Same caveats as primary therapy MYD88 Mutated/CXCR4 mutation Same caveats as primary therapy If immediate response needed, either BDR or Benda-R MYD88 Wild-Type Same caveats as primary therapy non-l265p MYD88 mutations Hunter et al, JCO Venetoclax for pts previously exposed to IB Everolimus >2 prior therapies Nucleoside analogues (non-asct candidates) ASCT in multiple relapses, chemosensitive disease
Waldenström s Macroglobulinemia Biology and Management
 Waldenström s Macroglobulinemia Biology and Management Steven P. Treon, MD, MA, MS, PhD, FRCP, FACP Professor of Medicine, Harvard Medical School Director, Bing Center for WM Dana Farber Cancer Institute
Waldenström s Macroglobulinemia Biology and Management Steven P. Treon, MD, MA, MS, PhD, FRCP, FACP Professor of Medicine, Harvard Medical School Director, Bing Center for WM Dana Farber Cancer Institute
Advances in Waldenström s Macroglobulinemia
 Advances in Waldenström s Macroglobulinemia Steven. Treon, MD, hd Dana-Farber/Brigham and Women s Cancer Center Massachusetts General Hospital Cancer Center Waldenström s Macroglobulinemia first described
Advances in Waldenström s Macroglobulinemia Steven. Treon, MD, hd Dana-Farber/Brigham and Women s Cancer Center Massachusetts General Hospital Cancer Center Waldenström s Macroglobulinemia first described
New Insights into the Biology and Therapy of Waldenström s Macroglobulinemia. Steven P. Treon, MD, MA, MS, PhD Professor of Medicine
 New Insights into the Biology and Therapy of Waldenström s Macroglobulinemia Steven P. Treon, MD, MA, MS, PhD Professor of Medicine Waldenström s Macroglobulinemia first described by Jan Gosta Waldenström
New Insights into the Biology and Therapy of Waldenström s Macroglobulinemia Steven P. Treon, MD, MA, MS, PhD Professor of Medicine Waldenström s Macroglobulinemia first described by Jan Gosta Waldenström
Novel treatment options for Waldenstrom Macroglobulinemia
 Novel treatment options for Waldenstrom Macroglobulinemia Irene Ghobrial, MD Associate Professor of Medicine Harvard Medical School Dana Farber Cancer Institute Boston, MA Ghobrial et al, Lancet Oncol
Novel treatment options for Waldenstrom Macroglobulinemia Irene Ghobrial, MD Associate Professor of Medicine Harvard Medical School Dana Farber Cancer Institute Boston, MA Ghobrial et al, Lancet Oncol
Frontline treatment options in Waldenström Macroglobulinemia. Jorge J. Castillo, MD Assistant Professor of Medicine Harvard Medical School
 Frontline treatment options in Waldenström Macroglobulinemia Jorge J. Castillo, MD Assistant Professor of Medicine Harvard Medical School Disclosures Consulting Otsuka Pharmaceuticals Biogen IDEC Alexion
Frontline treatment options in Waldenström Macroglobulinemia Jorge J. Castillo, MD Assistant Professor of Medicine Harvard Medical School Disclosures Consulting Otsuka Pharmaceuticals Biogen IDEC Alexion
WM GENOMICS AND TREATMENT OPTIONS
 WM GENOMICS AND TREATMENT OPTIONS BY STEVEN P. TREON MD, PhD, FRCP Dr. Steven Treon is a Professor of Medicine at Harvard Medical School, Director of the Bing Center for Waldenstrom s Macroglobulinemia
WM GENOMICS AND TREATMENT OPTIONS BY STEVEN P. TREON MD, PhD, FRCP Dr. Steven Treon is a Professor of Medicine at Harvard Medical School, Director of the Bing Center for Waldenstrom s Macroglobulinemia
Macroglobulinemia di Waldenstrom Terapia Alessandra Tedeschi Divisione di Ematologia ASST Grande Ospedale Metropoliano Niguarda Milano
 Milano 21 Aprile 2018 Macroglobulinemia di Waldenstrom Terapia Alessandra Tedeschi Divisione di Ematologia ASST Grande Ospedale Metropoliano Niguarda Milano Management of WM patient Ø IgM monoclonal gammopathy
Milano 21 Aprile 2018 Macroglobulinemia di Waldenstrom Terapia Alessandra Tedeschi Divisione di Ematologia ASST Grande Ospedale Metropoliano Niguarda Milano Management of WM patient Ø IgM monoclonal gammopathy
Current Treatment Options for WM
 Current Treatment Options for WM Shuo Ma, MD, PhD Northwestern University and Robert H. Lurie Comprehensive Cancer Center Waldenström s Macroglobulinemia Described by Jan Waldenström in 1944 Low grade
Current Treatment Options for WM Shuo Ma, MD, PhD Northwestern University and Robert H. Lurie Comprehensive Cancer Center Waldenström s Macroglobulinemia Described by Jan Waldenström in 1944 Low grade
Update on Waldenström Macroglobulinemia (WM)
") Update on Waldenström Macroglobulinemia (WM) Stephen M. Ansell, MD, PhD Professor of Medicine Division of Hematology Mayo Clinic Rochester, MN Update on Waldenström Macroglobulinemia (WM) Disclosures Stephen
Update on Waldenström Macroglobulinemia (WM) Stephen M. Ansell, MD, PhD Professor of Medicine Division of Hematology Mayo Clinic Rochester, MN Update on Waldenström Macroglobulinemia (WM) Disclosures Stephen
Traditional Therapies for Waldenstrom s Macroglobulinemia. Christine Chen Princess Margaret Cancer Centre Toronto, Canada May 2014
 Traditional Therapies for Waldenstrom s Macroglobulinemia Christine Chen Princess Margaret Cancer Centre Toronto, Canada May 2014 Jeff Atlin (1953-2014) Standard treatment options Single drug therapies
Traditional Therapies for Waldenstrom s Macroglobulinemia Christine Chen Princess Margaret Cancer Centre Toronto, Canada May 2014 Jeff Atlin (1953-2014) Standard treatment options Single drug therapies
Steven P. Treon Dana-Farber Cancer Institute Harvard Medical School
 Steven P. Treon Dana-Farber Cancer Institute Harvard Medical School 1 Jan Gosta Waldenstrom Described Macroglobulinemia in 1943 2 nd Intl Workshop on Waldenstrom s Macroglobulinemia Athens 2002 WM Treatment
Steven P. Treon Dana-Farber Cancer Institute Harvard Medical School 1 Jan Gosta Waldenstrom Described Macroglobulinemia in 1943 2 nd Intl Workshop on Waldenstrom s Macroglobulinemia Athens 2002 WM Treatment
Cyclophosphamide, bortezomib and dexamethasone (CyBorD) combination in Waldenstrom Macroglobulinemia
 combination in Waldenstrom Macroglobulinemia") Cyclophosphamide, bortezomib and dexamethasone (CyBorD) combination in Waldenstrom Macroglobulinemia Houry Leblebjian, PharmD, Kimberly Noonan, NP, Claudia Paba-Prada, MD, Steven P. Treon, MD, Jorge J.
Cyclophosphamide, bortezomib and dexamethasone (CyBorD) combination in Waldenstrom Macroglobulinemia Houry Leblebjian, PharmD, Kimberly Noonan, NP, Claudia Paba-Prada, MD, Steven P. Treon, MD, Jorge J.
Waldenström s macroglobulinemia: Genetic Basis and Therapy.
 Waldenström s macroglobulinemia: Genetic Basis and Therapy. Steve Treon MD, MA, PhD Dana Farber Cancer Institute Harvard Medical School Boston, Massachusetts, United States Waldenström s Macroglobulinemia
Waldenström s macroglobulinemia: Genetic Basis and Therapy. Steve Treon MD, MA, PhD Dana Farber Cancer Institute Harvard Medical School Boston, Massachusetts, United States Waldenström s Macroglobulinemia
Treatment of Waldenström s Macroglobulinemia Mayo Consensus
 Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Waldenstrom s Macroglobulinemia
 Waldenstrom s Macroglobulinemia : Targeted Therapies/ Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called
Waldenstrom s Macroglobulinemia : Targeted Therapies/ Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called
Waldenstrom s Macroglobulinemia
 Waldenstrom s Macroglobulinemia : Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called a B-lymphocyte or B-cell,
Waldenstrom s Macroglobulinemia : Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called a B-lymphocyte or B-cell,
Impact of ibrutinib dose intensity on patient outcomes in previously treated Waldenström macroglobulinemia
 Published Ahead of Print on May 17, 2018, as doi:10.3324/haematol.2018.191999. Copyright 2018 Ferrata Storti Foundation. Impact of ibrutinib dose intensity on patient outcomes in previously treated Waldenström
Published Ahead of Print on May 17, 2018, as doi:10.3324/haematol.2018.191999. Copyright 2018 Ferrata Storti Foundation. Impact of ibrutinib dose intensity on patient outcomes in previously treated Waldenström
Ibrutinib discontinuation in Waldenstr om macroglobulinemia: Etiologies, outcomes, and IgM rebound
 Received: 11 October 2017 Revised: 20 December 2017 Accepted: 21 December 2017 DOI: 10.1002/ajh.25023 RESEARCH ARTICLE Ibrutinib discontinuation in Waldenstr om macroglobulinemia: Etiologies, outcomes,
Received: 11 October 2017 Revised: 20 December 2017 Accepted: 21 December 2017 DOI: 10.1002/ajh.25023 RESEARCH ARTICLE Ibrutinib discontinuation in Waldenstr om macroglobulinemia: Etiologies, outcomes,
Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111)
 and Zanubrutinib (BGB-3111)") Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111) Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia
Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111) Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia
BTK Inhibitors and BCL2 Antagonists
 BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
Prospective, multicenter clinical trial of everolimus as primary therapy in Waldenstrom Macroglobulinemia (WMCTG ).
.") Prospective, multicenter clinical trial of everolimus as primary therapy in Waldenstrom Macroglobulinemia (WMCTG 09-214). Steven P. Treon 1, Kirsten Meid 1, Christina Tripsas 1, Leonard Heffner 2, Herbert
Prospective, multicenter clinical trial of everolimus as primary therapy in Waldenstrom Macroglobulinemia (WMCTG 09-214). Steven P. Treon 1, Kirsten Meid 1, Christina Tripsas 1, Leonard Heffner 2, Herbert
Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia
 Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia Edward Libby M.D. Associate Professor, University of Washington Department of Medicine, Division of Medical Oncology Fred Hutchinson
Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia Edward Libby M.D. Associate Professor, University of Washington Department of Medicine, Division of Medical Oncology Fred Hutchinson
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia
 Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
I Need Treatment First-Line WM Treatments & Side Effects IWMF Educational Forum Grapevine, TX 5/1/2015
 I Need Treatment First-Line WM Treatments & Side Effects IWMF Educational Forum Grapevine, TX 5/1/2015 Larry Anderson, MD, PhD Plasma Cell Disorder and Stem Cell Transplant Specialist UT Southwestern Medical
I Need Treatment First-Line WM Treatments & Side Effects IWMF Educational Forum Grapevine, TX 5/1/2015 Larry Anderson, MD, PhD Plasma Cell Disorder and Stem Cell Transplant Specialist UT Southwestern Medical
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Waldenstrom s Macroglobulinemia (WM) Treatment Options for Recurrent WM- What Are My Choices?
 Treatment Options for Recurrent WM- What Are My Choices?") Waldenstrom s Macroglobulinemia (WM) Treatment Options for Recurrent WM- What Are My Choices? IWMF Patient Education Forum June, 2016 Jeffrey V. Matous, MD Very Important Points The nature of WM is that
Waldenstrom s Macroglobulinemia (WM) Treatment Options for Recurrent WM- What Are My Choices? IWMF Patient Education Forum June, 2016 Jeffrey V. Matous, MD Very Important Points The nature of WM is that
Ibrutinib Withdrawal Symptoms in Patients with Waldenström Macroglobulinemia
 Published Ahead of Print on February 22, 2018, as doi:10.3324/haematol.2017.186908. Copyright 2018 Ferrata Storti Foundation. Ibrutinib Withdrawal Symptoms in Patients with Waldenström Macroglobulinemia
Published Ahead of Print on February 22, 2018, as doi:10.3324/haematol.2017.186908. Copyright 2018 Ferrata Storti Foundation. Ibrutinib Withdrawal Symptoms in Patients with Waldenström Macroglobulinemia
Background. Approved by FDA and EMEA for CLL and allows for treatment without chemotherapy in all lines of therapy
 Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Management of CLL in the Targeted Therapy Era
 Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients
 MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November
MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November
Waldenstrom s Macroglobulinemia
 Waldenstrom s Macroglobulinemia : Monoclonal Antibodies Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called
Waldenstrom s Macroglobulinemia : Monoclonal Antibodies Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called
CLL what do I need to know as an Internist in Taimur Sher MD Associate Professor of Medicine Mayo Clinic
 CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
The Map of Current Treatment Options for Waldenström Macroglobulinemia
 The Map of Current Treatment Options for Waldenström Macroglobulinemia Craig Reeder Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida DISCLOSURES Relevant Financial Relationship(s)
The Map of Current Treatment Options for Waldenström Macroglobulinemia Craig Reeder Mayo Clinic Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida DISCLOSURES Relevant Financial Relationship(s)
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia
 Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Toward personalized treatment in Waldenström macroglobulinemia
 INDOLENT LYMPHOMA: HOW UNDERSTANDING DISEASE BIOLOGY IS INFLUENCING CLINICAL DECISION-MAKING Toward personalized treatment in Waldenström macroglobulinemia Jorge J. Castillo and Steven P. Treon Bing Center
INDOLENT LYMPHOMA: HOW UNDERSTANDING DISEASE BIOLOGY IS INFLUENCING CLINICAL DECISION-MAKING Toward personalized treatment in Waldenström macroglobulinemia Jorge J. Castillo and Steven P. Treon Bing Center
MANTLE CELL LYMPHOMA MTOR-INHIBITION
 MANTLE CELL LYMPHOMA MTOR-INHIBITION Rome, 23. March 2017 Prof. Dr. med. Georg Heß III. Med. Klinik Universitäres Centrum für Tumorerkrankungen Universitätsmedizin der Johannes Gutenberg-Universität Mainz
MANTLE CELL LYMPHOMA MTOR-INHIBITION Rome, 23. March 2017 Prof. Dr. med. Georg Heß III. Med. Klinik Universitäres Centrum für Tumorerkrankungen Universitätsmedizin der Johannes Gutenberg-Universität Mainz
BR is an established treatment regimen for CLL in the front-line and R/R settings
 Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Treatment Landscape in R/R DLBCL Novel Targets and Strategies. Wyndham H. Wilson, M.D., Ph.D. Senior Investigator
 Treatment Landscape in R/R DLBCL Novel Targets and Strategies Wyndham H. Wilson, M.D., Ph.D. Senior Investigator Gene-expression profiling of DLBCL subtypes Roschewski, M. et al. (2013) Nat. Rev. Clin.
Treatment Landscape in R/R DLBCL Novel Targets and Strategies Wyndham H. Wilson, M.D., Ph.D. Senior Investigator Gene-expression profiling of DLBCL subtypes Roschewski, M. et al. (2013) Nat. Rev. Clin.
Treatment Nodal Marginal Zone Lymphoma
 Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
CLL: Future Therapies. Dr. Anca Prica
 CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
MANTLE CELL LYMPHOMA
 MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
Overview on clinical trials in Waldenstrom s macroglobulinemia
 trom s Overview on clinical trials in Waldenstrom s macroglobulinemia Waldenstrom s macroglobulinemia is characterized by lymphoplasmocytic cells accumulation predominantly in bone marrow, secreting immunoglobulin
trom s Overview on clinical trials in Waldenstrom s macroglobulinemia Waldenstrom s macroglobulinemia is characterized by lymphoplasmocytic cells accumulation predominantly in bone marrow, secreting immunoglobulin
Management of 17p Deleted CLL Patients in the Era of Targeted Therapy
 Management of 17p Deleted CLL Patients in the Era of Targeted Therapy Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November 11,
Management of 17p Deleted CLL Patients in the Era of Targeted Therapy Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November 11,
Managing patients with relapsed follicular lymphoma. Case
 Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies
 December 10, 2013 Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies -- Clinical Presentation in Waldenstrom's Macroglobulinemia Deemed "Best of ASH" -- NEW ORLEANS, Dec. 10,
December 10, 2013 Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies -- Clinical Presentation in Waldenstrom's Macroglobulinemia Deemed "Best of ASH" -- NEW ORLEANS, Dec. 10,
Disclosures. I receive honoraria and research funding from Beigene, Janssen and AbbVie.
 Improved depth of response with increased follow-up in phase 1 trial of patients with Waldenström macroglobulinemia (WM) treated with oral Bruton tyrosine kinase (BTK) inhibitor zanubrutinib (BGB-3111)
Improved depth of response with increased follow-up in phase 1 trial of patients with Waldenström macroglobulinemia (WM) treated with oral Bruton tyrosine kinase (BTK) inhibitor zanubrutinib (BGB-3111)
Pomalidomide (CC4047) Plus Low-Dose Dexamethasone as Therapy for Relapsed Multiple Myeloma. Lacy MQ et al. J Clin Oncol 2009;27(30):
 Plus Low-Dose Dexamethasone as Therapy for Relapsed Multiple Myeloma. Lacy MQ et al. J Clin Oncol 2009;27(30):") Pomalidomide (CC4047) Plus Low-Dose Dexamethasone as Therapy for Relapsed Multiple Myeloma Lacy MQ et al. J Clin Oncol 2009;27(30):5008-14. Introduction A curative therapy for multiple myeloma (MM) does
Pomalidomide (CC4047) Plus Low-Dose Dexamethasone as Therapy for Relapsed Multiple Myeloma Lacy MQ et al. J Clin Oncol 2009;27(30):5008-14. Introduction A curative therapy for multiple myeloma (MM) does
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents
 Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Highlights in chronic lymphocytic leukemia
 Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant
 Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Chronic Lymphocytic Leukemia: State of the Art
 14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Dimopoulos MA, Tedeschi A, Trotman J, et al. Phase 3 trial
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Dimopoulos MA, Tedeschi A, Trotman J, et al. Phase 3 trial
Multiple Myeloma Updates 2007
 Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Phase 3 Trial of Ibrutinib plus Rituximab in Waldenström s Macroglobulinemia
 Original Article Phase 3 Trial of Ibrutinib plus Rituximab in Waldenström s Macroglobulinemia M.A. Dimopoulos, A. Tedeschi, J. Trotman, R. García Sanz, D. Macdonald, V. Leblond, B. Mahe, C. Herbaux, C.
Original Article Phase 3 Trial of Ibrutinib plus Rituximab in Waldenström s Macroglobulinemia M.A. Dimopoulos, A. Tedeschi, J. Trotman, R. García Sanz, D. Macdonald, V. Leblond, B. Mahe, C. Herbaux, C.
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES
 How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
Dana-Farber Cancer Institute, Boston, MA, USA; 2. H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, USA; 3
 The investigational agent MLN9708, an oral proteasome inhibitor, in patients with relapsed and/or refractory multiple myeloma (MM): results from the expansion cohorts of a phase 1 dose-escalation study
The investigational agent MLN9708, an oral proteasome inhibitor, in patients with relapsed and/or refractory multiple myeloma (MM): results from the expansion cohorts of a phase 1 dose-escalation study
Leukemia. Roland B. Walter, MD PhD MS. Fred Hutchinson Cancer Research Center University of Washington
 Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
BENDAMUSTINE + RITUXIMAB IN CLL
 BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
The case for maintenance rituximab in FL
 New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
Update: New Treatment Modalities
 ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
To Maintain or Not to Maintain? Immunomodulators vs PIs Yes: Proteasome Inhibitors
 To Maintain or Not to Maintain? Immunomodulators vs PIs Yes: Proteasome Inhibitors James Berenson, MD Institute for Myeloma and Bone Cancer Research West Hollywood, CA Financial Disclosures Takeda, Celgene
To Maintain or Not to Maintain? Immunomodulators vs PIs Yes: Proteasome Inhibitors James Berenson, MD Institute for Myeloma and Bone Cancer Research West Hollywood, CA Financial Disclosures Takeda, Celgene
State of the Art Treatment for Relapsed Mantle Cell Lymphoma
 Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
Winship Cancer Institute of Emory University State of the Art Treatment for Relapsed Mantle Cell Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor, BMT Program Emory University- Winship Cancer Institute
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
Novel Treatment Advances and Approaches in Management of Relapsed/Refractory Multiple Myeloma
 Novel Treatment Advances and Approaches in Management of Relapsed/Refractory Multiple Myeloma Ravi Vij, MD MBA Professor of Medicine Washington University School of Medicine Section of Stem Cell Transplant
Novel Treatment Advances and Approaches in Management of Relapsed/Refractory Multiple Myeloma Ravi Vij, MD MBA Professor of Medicine Washington University School of Medicine Section of Stem Cell Transplant
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
ICML Updates on BTK Inhibitor BGB-3111 and its Clinical Development Plan. June 16, 2017
 ICML Updates on BTK Inhibitor BGB-3111 and its Clinical Development Plan June 16, 2017 Forward Looking Statements Certain statements contained in this presentation, other than statements of fact that are
ICML Updates on BTK Inhibitor BGB-3111 and its Clinical Development Plan June 16, 2017 Forward Looking Statements Certain statements contained in this presentation, other than statements of fact that are
Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD
: Refresher Course for Hematologists Ekarat Rattarittamrong, MD") Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang-Mai University Outline
Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang-Mai University Outline
Methods: Studies included in the analysis
 Efficacy and safety of long-term ixazomib maintenance therapy in patients with newly diagnosed multiple myeloma not undergoing transplant: An integrated analysis of four phase 1/2 studies Meletios A. Dimopoulos,
Efficacy and safety of long-term ixazomib maintenance therapy in patients with newly diagnosed multiple myeloma not undergoing transplant: An integrated analysis of four phase 1/2 studies Meletios A. Dimopoulos,
FCR and BR: When to use, how to use?
 FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
Atrial fibrillation associated with Ibrutinib in Waldenström s macroglobulinemia.
 Atrial fibrillation associated with Ibrutinib in Waldenström s macroglobulinemia. Joshua N. Gustine 1, Kirsten Meid 1, Toni E. Dubeau 1, Steven P. Treon 1,2, and Jorge J. Castillo 1,2. 1 Bing Center for
Atrial fibrillation associated with Ibrutinib in Waldenström s macroglobulinemia. Joshua N. Gustine 1, Kirsten Meid 1, Toni E. Dubeau 1, Steven P. Treon 1,2, and Jorge J. Castillo 1,2. 1 Bing Center for
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
How to Integrate the New Drugs into the Management of Multiple Myeloma
 How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
Front-line treatment in young. Role of maintenance therapy. Rome 2017 Prof Le Gouill S.
 Front-line treatment in young patients with MCL: Role of maintenance therapy Rome 2017 Prof Le Gouill S. Is there a need for maintenance for young MCL patients? Is there a need for maintenance for young
Front-line treatment in young patients with MCL: Role of maintenance therapy Rome 2017 Prof Le Gouill S. Is there a need for maintenance for young MCL patients? Is there a need for maintenance for young
CLL: disease specific biology and current treatment. Dr. Nathalie Johnson
 CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
Smoldering Myeloma: Leave them alone!
 Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
POST ICML Indolent lymphomas relapse treatment
 POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
MYD88, CXCR4 and the Genetics of WM
 MYD88, CXCR4 and the Genetics of WM Zachary Hunter Bing Center for WM Dana-Farber Cancer Institute Harvard Medical School Bing Center for WM Research at the Dana-Farber Cancer Institute Harvard Medical
MYD88, CXCR4 and the Genetics of WM Zachary Hunter Bing Center for WM Dana-Farber Cancer Institute Harvard Medical School Bing Center for WM Research at the Dana-Farber Cancer Institute Harvard Medical
US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA
 FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA") US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA Accelerated approval of Bruton tyrosine kinase (BTK) inhibitor in MCL marks AstraZeneca
US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA Accelerated approval of Bruton tyrosine kinase (BTK) inhibitor in MCL marks AstraZeneca
Update on Management of CLL. Presenter Disclosure Information. Chronic Lymphocytic Leukemia. Audience Response Question?
 Welcome to Master Class for Oncologists New York, NY May 14, 2010 Session 5: 4:20 PM - 5:00 PM Update on Management of CLL John C. Byrd, MD D Warren Brown Professor of Leukemia Research Professor of Medicine
Welcome to Master Class for Oncologists New York, NY May 14, 2010 Session 5: 4:20 PM - 5:00 PM Update on Management of CLL John C. Byrd, MD D Warren Brown Professor of Leukemia Research Professor of Medicine
Ibrutinib in Previously Treated Waldenström s Macroglobulinemia
 The new england journal of medicine Original Article Ibrutinib in Previously Treated Waldenström s Macroglobulinemia Steven P. Treon, M.D., Ph.D, Christina K. Tripsas, M.A., Kirsten Meid, M.P.H., Diane
The new england journal of medicine Original Article Ibrutinib in Previously Treated Waldenström s Macroglobulinemia Steven P. Treon, M.D., Ph.D, Christina K. Tripsas, M.A., Kirsten Meid, M.P.H., Diane
Nuove opportunità di cura. Stefano Sacchi, Modena
 Nuove opportunità di cura Stefano Sacchi, Modena Antiangiogenesis therapies The goal is to target the blood supply that feeds tumors. Vorinostat (suberoylanilide hydroxamic acid - SAHA) TOPIC SEARCH:
Nuove opportunità di cura Stefano Sacchi, Modena Antiangiogenesis therapies The goal is to target the blood supply that feeds tumors. Vorinostat (suberoylanilide hydroxamic acid - SAHA) TOPIC SEARCH:
CME Information LEARNING OBJECTIVES
 CME Information LEARNING OBJECTIVES Identify patients with MM who have undergone autologous stem cell transplant and would benefit from maintenance lenalidomide. Counsel older patients (age 65 or older)
CME Information LEARNING OBJECTIVES Identify patients with MM who have undergone autologous stem cell transplant and would benefit from maintenance lenalidomide. Counsel older patients (age 65 or older)
Myeloma update ASH 2014
 Myeloma update ASH 2014 Updates in Newly Diagnosed Multiple Myeloma FIRST: effect of age on lenalidomide/dexamethasone vs MPT in transplantation-ineligible pts Phase III: MPT-T vs MPR-R in transplantation-ineligible
Myeloma update ASH 2014 Updates in Newly Diagnosed Multiple Myeloma FIRST: effect of age on lenalidomide/dexamethasone vs MPT in transplantation-ineligible pts Phase III: MPT-T vs MPR-R in transplantation-ineligible
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced CLL and NHL
, ublituximab, and ibrutinib in patients with advanced CLL and NHL") Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Advances in CLL 2016
 Advances in CLL 2016 The Geoffrey P. Herzig Memorial Symposium, Louisville, KY Kanti R. Rai, MD Northwell-Hofstra School of Medicine Long Island Jewish Medical Center New Hyde Park, NY Disclosures Member
Advances in CLL 2016 The Geoffrey P. Herzig Memorial Symposium, Louisville, KY Kanti R. Rai, MD Northwell-Hofstra School of Medicine Long Island Jewish Medical Center New Hyde Park, NY Disclosures Member
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
CLL & SLL: Current Management & Treatment. Dr. Peter Anglin
 CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
Management of Patients With Relapsed Chronic Lymphocytic Leukemia
 Management of Patients With Relapsed Chronic Lymphocytic Leukemia Polina Shindiapina, MD, PhD, and Farrukh T. Awan, MD Abstract The management of chronic lymphocytic leukemia (CLL) has improved significantly
Management of Patients With Relapsed Chronic Lymphocytic Leukemia Polina Shindiapina, MD, PhD, and Farrukh T. Awan, MD Abstract The management of chronic lymphocytic leukemia (CLL) has improved significantly
Clinical Overview: MRD in CLL. Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel
 Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
State of the art: CAR-T cell therapy in lymphoma
 State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division
 Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division University of Virginia Cancer Center The Clinical Continuum of CLL Early asymptomatic
Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division University of Virginia Cancer Center The Clinical Continuum of CLL Early asymptomatic