ICML Updates on BTK Inhibitor BGB-3111 and its Clinical Development Plan. June 16, 2017
|
|
|
- Gerard Stephens
- 6 years ago
- Views:
Transcription
1 ICML Updates on BTK Inhibitor BGB-3111 and its Clinical Development Plan June 16, 2017
2 Forward Looking Statements Certain statements contained in this presentation, other than statements of fact that are independently verifiable at the date hereof, may constitute forward-looking statements. Examples of such forward-looking statements include those regarding investigational drug candidates and clinical trials and the status and related results thereto, as well those regarding continuing and further development efforts. Such statements, based as they are on the current analysis and expectations of management, inherently involve numerous risks and uncertainties, known and unknown, many of which are beyond BeiGene s control. Such risks include but are not limited to: the impact of general economic conditions, general conditions in the pharmaceutical industries, changes in the global and regional regulatory environments in the jurisdictions in which BeiGene does business, market volatility, fluctuations in costs and changes to the competitive environment. Consequently, actual future results may differ materially from the anticipated results expressed in the forward-looking statements. In the case of forward-looking statements regarding investigational drug candidates and continuing further development efforts, specific risks which could cause actual results to differ materially from BeiGene s current analysis and expectations include: failure to demonstrate the safety, tolerability and efficacy of our drug candidates, final and quality controlled verification of data and the related analyses, the expense and uncertainty of obtaining regulatory approval, including from the FDA, CFDA and EMA, and the possibility of having to conduct additional clinical trials. Further, even if regulatory approval is obtained, pharmaceutical products are generally subject to: stringent on-going governmental regulation, challenges in gaining market acceptance and competition. These statements are also subject to a number of material risks and uncertainties that are described in BeiGene s filings with the Securities and Exchange Commission. The reader should not place undue reliance on any forward-looking statements included in this presentation. These statements speak only as of the date made, and BeiGene is under no obligation and disavows any obligation to update or revise such statements as a result of any event, circumstances or otherwise, unless required by applicable legislation or regulation. 2
3 Agenda Pipeline Overview and Summary 14-ICML Presentations Abstract # 059: Bruton s Tyrosine Kinase (BTK) Inhibitor BGB-3111 Demonstrates High Very Good Partial Response (VGPR) Rate in Patients with Waldenström Macroglobulinemia (WM) Abstract # 237: High Overall Response Rate With the BTK Inhibitor BGB-3111 in Patients With Chronic Lymphocytic Leukemia / Small Lymphocytic Lymphoma: an Update on Safety and Activity Abstract # 103: Safety and Activity of the Highly Specific BTK Inhibitor, BGB-3111 Plus Obinutuzumab in Patients with Follicular Lymphoma and Chronic Lymphocytic Leukemia BGB-3111 Clinical Development Plan Q&A 3
4 BeiGene Pipeline: Lead Asset in Global Phase III Additional Global Pivotal Programs Expected to Start in 2017 Global Clinical Pipeline Status Small Molecule Antibody Program Molecular Target Commercial Rights Preclinical Dose Escalation Dose Expansion Registrational Trials Potential Differentiation BGB-3111 BTK Worldwide Deeper target suppression enabled by improved selectivity and exposure BGB-A317 PD-1 Worldwide Fc receptor binding has been engineered out BGB-290 PARP Worldwide 1 strong DNA trapping and Significant brain penetration, high selectivity BGB-283 RAF Dimer Worldwide 1 Inhibits monomer and dimer forms of RAF; potential activity in RAS In total, over 1,200 patients and healthy adults 2 enrolled across 4 programs including combination trials 1 Limited collaboration with Merck KGaA; 2 As of May 31,

5 Two Assets in Pivotal Trials in China Additional Pivotal Trials Expected to Start in China in 2017 Clinical Pipeline Status in China Small Molecule Antibody Program Molecular Target Preclinical CTA Approval Dose Confirmation/ Expansion Registrational Trials BGB-3111 BTK BGB-A317 PD-1 BGB-290 PARP BGB-283 RAF Dimer 5

6 Combinations in Development Broad Internal Portfolio Provides Advantages in Combination Therapy External Combo Internal Combo Combination Mechanism of Action Planning for Combination Dose Escalation Dose Expansion Registrational Trials Differentiation BGB Gazyva BTK + CD20 BGB-A317 + BGB-290 PD-1 + PARP No interference with CD20 antibody activity due to BTK selectivity Good tolerability due to PARP selectivity BGB-A317 + BGB-3111 PD-1 + BTK Good tolerability due to BTK selectivity Combination Potential We believe we have the only wholly owned PD-1 and BTK inhibitor combination in clinical testing We believe we are one of a small number of companies with internal combinations of PD-1 + PARP inhibitors Potential for RAF dimer / PD-1 inhibitor combination based on internal data Broad preclinical programs target multiple points in the immunity cycle 6
7 ICML Update on BGB-3111 and Summary WM monotherapy data: improving VGPR rate (43% vs. 34% at ASH) in a larger number of patients (42 vs. 32 evaluable) further supports ongoing global head-to-head Phase III trial CLL monotherapy data: continued high ORR (94%) in a larger number of patients (66 vs 46 evaluable at ASH); CRs emerging despite relatively short follow-up; low discontinuation rate due to AE or progression Initiating 1L CLL trial vs. BR to address the large population of previously untreated patients who are not eligible for intensive chemo-immunotherapy (FCR) Combination data with Gazyva: strong early signal in FL (high ORR and CR after a short follow-up) supports expedited development in FL where there is an unmet need as well as a large opportunity for which a BTK inhibitor has not been approved Continue to show excellent safety and tolerability profile; very low rate of discontinuation Nearly 500 patients dosed in BGB-3111 clinical program 7
8
9 BGB-3111 Background Bruton s Tyrosine Kinase (BTK), is a critical signaling component of the B- cell receptor, and mediates proliferation, cellular homing, and stromal adhesion in a variety of B cell malignancies Ibrutinib, the first generation BTK inhibitor, is currently approved in the following diseases/ treatment settings: CLL/SLL: Survival advantage over ofatumumab (relapsed/ refractory setting) and chlorambucil (treatment-naïve setting) Waldenstrom s macroglobulinemia (WM): single-arm trial (n=63) with major RR 73%, VGPR 15%, 3-year EFS 69% Mantle cell lymphoma and marginal zone lymphoma Ibrutinib remains under development, but not yet approved, in other B cell malignancy subtypes, including FL and DLBCL BGB-3111 is a potent and specific BTK inhibitor, designed to minimize off target inhibition of TEC- and EGFR-family kinases Favorable pharmacokinetic properties designed to maximize plasma exposure and tissue-independent BTK occupancy 9
10 BGB-3111: Kinase Selectivity Relative to Ibrutinib Targets Highly selective inhibition of BTK relative to similar tyrosine kinases Assays Ibrutinib IC 50 (nm) BGB-3111 IC 50 (nm) Ratio (BGB-3111:Ibrutinib) BTK BTK-pY223 Cellular Assay Rec-1 Proliferation BTK Occupation Cellular Assay BTK Biochemical Assay EGFR ITK p-egfr HTRF Cellular Assay A431 Proliferation 323 3, ITK Occupancy Cellular Assay 189 3, p-plc γ1 Cellular Assay 77 3, IL-2 Production Cellular Assay 260 2, ITK Biochemical Assay JAK3 JAK3 Biochemical Assay HER2 HER2 Biochemical Assay TEC TEC Biochemical Assay
 Time post-dose (hours) 40 mg QD 80 mg QD 160 mg QD 320 mg QD 560 mg PBMC 700 600 500 400 300 200 100")

11 Pharmacokinetics of BGB-3111, Ibrutinib and Acalabrutinib^ (Fig A) and BTK Occupancy for BGB-3111 in Peripheral Blood and Lymph Node (Fig B) A. Plasma Concentration (ng/ml) B BGB Time post-dose (hours) Time post-dose (hours) 40 mg QD 80 mg QD 160 mg QD 320 mg QD 560 mg PBMC Ibrutinib Adapted from Advani, et al, J Clin Oncol, % Time post-dose (hours) 100 mg Lymph Node Acalabrutinib Adapted from Byrd et al., NEJM, 2016 BTK Occupancy, % 100% 80% 60% 40% 20% 0% CLL MCL FL DLBCL MZL WM mg QD mg BID 4 ^ Cross-trial comparison 1 Tam CS, et al. Blood. 2015;126: Advani RH, et al. J Clin Oncol. 2013;31: Byrd, et al. NEJM. 2016;374: Tam, et al. ASH 2016 (Abstracts 642 and 1216) 11
12 Bruton s Tyrosine Kinase (BTK) Inhibitor BGB-3111 Demonstrates High Very Good Partial Response (VGPR) Rate in Patients with Waldenström Macroglobulinemia (WM) Judith Trotman, 1,2 Stephen Opat, 3,4 Paula Marlton, 5 David Gottlieb, 6 David Simpson, 7 Gavin Cull, 8 David Ritchie, 9,10 Emma Verner, 1 Sumita Ratnasingam, 3 Mary Ann Anderson, 10,11 Peter Wood, 5 Lai Wang, 12 Ling Xue, 12 Eric Hedrick, 12 Jane Huang, 12 James Hilger, 12 John F. Seymour, 9,10 Andrew W. Roberts, 10,11 Constantine S. Tam 9,10,13 1 Concord Repatriation General Hospital, Concord, Australia; 2 University of Sydney, Concord, Australia; 3 Monash Health, Clayton, Victoria, Australia; 4 Monash University, Clayton, Victoria, Australia; 5 Princess Alexandra Hospital and University of Queensland, Brisbane, Australia; 6 Westmead Hospital, Westmead, Australia; 7 North Shore Hospital, Auckland, New Zealand; 8 Sir Charles Gairdner Hospital, Perth, Western Australia, Australia; 9 Peter MacCallum Cancer Center, East Melbourne, Victoria, Australia; 10 University of Melbourne, Parkville, Victoria, Australia; 11 Melbourne Health, Parkville, Victoria, Australia; 12 Beigene (Beijing) Company Ltd, Beijing, China and Emeryville, CA; 13 St Vincent s Hospital, Fitzroy, Victoria, Australia
13 WM: Patient Characteristics Characteristic Total (N = 48) Age, years, median (range) 66 (44-87) ECOG Performance Status, n (%) (29) 34 (71) Follow-up, months, median (range) 10.6 ( ) Prior Treatment Status, n (%) Treatment-naïve Relapsed/refractory Number of prior therapies, median (range) Prior rituximab (% R/R pts) Genotype MYD88 L265P / CXCR4 WT MYD88 L265P / CXCR4 WHIM MYD88 WT Unavailable 10 (21) 38 (79) 1 (1-8) 28 (74%) 21 (43.8) 5 (10.4) 5 (10.4) 17 (35.4) 13
14 WM: Most Frequent Adverse Events (> 10%) Independent of Causality (Safety Population: N = 48) Adverse Event All Grade Grade 3-4 n (pts) % n (pts) % Petechiae/purpura/contusion 17 35% 0 0% Upper respiratory tract infection 15 31% 0 0% Constipation 12 25% 0 0% Diarrhea 9 19% 1 2% Epistaxis 9 19% 0 0% Nausea 8 17% 0 0% Cough 7 15% 0 0% Anemia 7 15% 4 8% Headache 7 15% 1 2% Neutropenia 6 13% 4 8% Rash 6 13% 0 0% 14
15 WM: Overview of Adverse Events Event All Cause n (pts) % Patients with at least one AE Grade % Patients with at least one SAE 18 38% Events leading to treatment discontinuation 3 6% SAE pos. related to BGB-3111: haemothorax, atrial fib, colitis, febrile neutropenia, headache (all n=1) Bronchiectasis, adenocarcinoma of pylori, and prostate adenocarcinoma (all n=1) AE of Special Interest All Grade Grade 3-4 n (pts) % n (pts) % Diarrhea 9 19% 1 2% Serious hemorrhage 1 2% 1 2% Atrial fibrillation 3 6% 0 0 Def serious hemorrhage: grade 3, or CNS hemorrhage of any grade. 15
16 WM: Efficacy Summary (n = 42) Total Median follow-up (range) 12.3 months ( ) Best Response (n = 42) CR VGPR PR MR SD IgM reduction (median, %) Hemoglobin change (median) Lymphadenopathy reduction by CT (n, range) 0 18 (43%) 14 (33%) 6 (14%) 4 (10%) 90% ORR 32.7 g/l to 6.1 g/l (81.3%) g/l to 142 g/l 45.5% (median) (16, 18.2%-81.4%) A VGPR and a PR (along with two minor responses) were observed in the 5 patients with MYD88 wildtype status. Overall response rate. * Major response rate. 76% MRR* 16
17 WM: Progression-Free Survival 91.7% Survival Month 4 patients have discontinued treatment to date, 1 with progressive disease and 3 with adverse events: exacerbation of bronchiectasis (n=1), prostate adenocarcinoma (n=1), and gastric carcinoma (n=1) 17
18 Conclusions BGB-3111, a highly selective oral BTK inhibitor achieves high plasma concentrations and complete BTK occupancy in blood and lymph nodes BGB-3111 is very well tolerated To date: No treatment discontinuation due to BGB-3111 related toxicity One AE-related death (due to pre-existing bronchiectasis, while in VGPR) Highly active in WM Overall response rate 90%, with 43% VGPR 18
19 High Overall Response Rate With the BTK Inhibitor BGB-3111 in Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma: an Update on Safety and Activity John F. Seymour 1,2, Stephen Opat 3,4, Gavin Cull 5, Judith Trotman 6,7, David Gottlieb 8,9, David Simpson 10, Paula Marlton 11, Mary Ann Anderson 1,12, Matthew Ku 13, David S. Ritchie 12,14,15, Sumita Ratnasingam 16, Bradley Augustson 17, Won Seog Kim 18, Lai Wang 19, Ling Xue 19, James Hilger 19, Jane Huang 19, Eric Hedrick 19, Andrew W. Roberts 14,20,21, and Constantine S. Tam 1,22,23 1 University of Melbourne, Parkville, Australia; 2 Department of Haematology, Peter MacCallum Cancer Centre, Melbourne, Australia; 3 School of Clinical Sciences at Monash Health, Faculty of Medicine, Nursing & Dentistry, Monash University, Melbourne, Australia; 4 Monash Haematology, Monash Health, Clayton, Australia; 5 Department of Haematology, Sir Charles Gairdner Hospital, Perth, Australia; 6 Department of Hematology, Concord Repatriation General Hospital, Concord, New South Wales, Australia; 7 University of Sydney, Concord, Australia; 8 Blood and Marrow Transplant Service, Westmead Hospital, Sydney, Australia; 9 Sydney Medical School, University of Sydney, Sydney, Australia; 10 North Shore Hospital, Auckland, New Zealand; 11 Princess Alexandra Hospital, University of Queensland School of Medicine, Brisbane, Australia; 12 Department of Clinical Haematology and Bone Marrow Transplantation, The Royal Melbourne Hospital, Parkville, Australia; 13 Austin Health, Melbourne, Australia; 14 University of Melbourne, Melbourne, Australia; 15 Peter MacCallum Cancer Centre, Melbourne, Australia; 16 Department of Haematology, Monash Medical Centre, Monash Health, Melbourne, Australia; 17 Sir Charles Gairdner Hospital, Perth, Australia; 18 Division of Hematology-Oncology Samsung Medical Center, Seoul, Korea; 19 Beigene (Beijing) Company Ltd, Beijing, China; 20 Royal Melbourne Hospital, Melbourne, Australia; 21 Walter and Eliza Hall Institute of Medical Research, Royal Melbourne Hospital, Melbourne, Australia; 22 Peter MacCallum Cancer Centre, Melbourne, Australia; 23 St. Vincent's Hospital, Melbourne, Australia
20 CLL/ SLL: Patient Characteristics Characteristic Total (N = 69) Age, years, median (range) 68 (24-87) ECOG Performance Status, (%) Follow-up, months, median (range) 34 (49) 33 (48) 2 (3) 10.3 ( ) Prior treatment status Treatment-naïve, n (%) Relapsed/refractory, n (%) Number of prior therapies, median (range) 18 (26) 51 (74) 2 (1-7) Bulky disease*, n (%) 4 (6) Molecular risk factors, n (%) del17p/p53mut (n = 51) 11q- (n = 44) IgHV unmutated (n = 16) ECOG, Eastern Cooperative Oncology Group; LN, lesion. 20 (39) 14 (32) 11 (69) * Any lymph node >10 cm in maximum diameter. 20
21 CLL/SLL: Most Frequent Adverse Events (> 10%) Independent of Causality (N = 69) Adverse Event All Grade Grade 3-4 n (pts) % (N = 69) n (pts) % (N = 69) Petechiae/purpura/contusion 32 46% 1 1% Fatigue 20 29% 0 0% Upper respiratory tract infection 19 28% 0 0% Cough 16 23% 0 0% Diarrhea 15 22% 0 0% Headache 13 19% 0 0% Hematuria 10 15% 0 0% Nausea 9 13% 0 0% Rash 9 13% 0 0% Arthralgia 8 12% 0 0% Muscle spasms 8 12% 0 0% Urinary tract infection 8 12% 0 0% pts, patients. 21
22 CLL/SLL: Adverse Events of Special Interest SAE n (pts) % (N = 69) Grade Led to Treatment Discontinuation Purpura (subcutaneous hemorrhage) Y 1 1% G3 0 Diarrhea Y 1 1% G2 0 Atrial fibrillation N 1 1% G2 0 A total of 18 SAEs were experienced by 13 patients SAE s not listed above (1 each) were also reported: CLL, delirium, febrile neutropenia, Invasive ductal breast carcinoma, lower respiratory tract infection, pleural effusion, renal colic, sepsis, splenectomy, splenomegaly, painful swelling in right neck, cardiac failure, coronary artery stenosis, ventricular extrasystole, pneumonia, and hemorrhoidal infection 22
23 CLL/SLL: Events Leading to Permanent Treatment Discontinuation Event n (pts) % (N = 69) Adverse event (Pleural effusion) 1* 1% Hodgkin s Transformation 1 1% * Taken off study prior to first response assessment. No patients have progressed with a C481S mutation 23
24 CLL/SLL: Response Response Treatment Naive (n = 16) Relapsed/Refractory (n = 50) Total (n = 66) Median follow-up, mo (range) 7.6 ( ) 14.0 ( ) 10.5 ( ) Best Response ORR CR* PR PR-L SD D/C prior to assessment 16 (100%) 1 (6%) 13 (81%) 2 (13%) (92%) 1 (2%) 41 (82%) 4 (8%) 3 (6%) 1 (2%) 62 (94%) 2 (3%) 54 (82%) 6(9%) 3 (5%) 1 (2%) CR, complete response; D/C, discontinuation; ORR, overall response rate; PR, partial response; PR-L, partial response with lymphocytosis; SD, stable disease. The ORR in patients with del17p and/or 11q- (n = 22) was 96% * Most patients in this series have yet to reach the protocol-defined marrow reassessment time point for CR assessment 24
25 CLL/SLL: Progression-Free Survival 25
26 Conclusions (CLL/ SLL Phase 1 Update) BGB-3111 is highly active in CLL/SLL Very high rate (94%) of durable response, independent of poor-risk features With a median follow-up of 10.3 months, only one patient has experienced disease progression (Hodgkin s transformation) BGB-3111 is safe and well tolerated in CLL/SLL Only one patient with adverse event-related treatment discontinuation Very low incidence of serious diarrhea (1%), and serious bleeding (1%) and atrial fibrillation (1%) These updated results support Phase 3 trials of BGB-3111 in a broad population of CLL/SLL patients 26
27 Safety and Activity of the Highly Specific BTK Inhibitor, BGB-3111 Plus Obinutuzumab in Patients with Follicular Lymphoma and Chronic Lymphocytic Leukemia Constantine S. Tam, 1,2,3 Hang Quach, 1,2 Andrew Nicol, 4 Xavier Badoux, 5 Hannah Rose, 6 Henry Miles Prince, 7 Michael F. Leahy, 8 Richard Eek, 9 Nicholas Wickham, 10 Sushrut Patil, 11 Jane Huang, 12 Xiaoping Zhang, 12 Lai Wang, 13 Eric Hedrick, 12 William Novotny, 12 Ian Flinn 14 1 St. Vincent's Hospital, Melbourne, Australia; 2 University of Melbourne, Parkville, Australia; 3 Peter MacCallum Cancer Centre, Melbourne, Australia; 4 Brisbane Clinic for Lymphoma, Myeloma, and Leukaemia, Brisbane, Australia; 5 St. George Hospital, Australia 6 University Hospital Geelong, Australia; 7 St. Frances Xavier Cabrini Hospital, Australia; 8 Royal Perth Hospital, Australia; 9 Border Medical Oncology Research Unit, Australia; 10 Ashford Cancer Centre Research, Australia; 11 The Alfred Hospital, Australia; 12 BeiGene USA, Cambridge, MA, USA; 13 BeiGene Company Ltd, Beijing, China; and 14 Tennessee Oncology, PLLC, Nashville, TN, USA.


28 BGB-3111 Does Not Impair Rituximab-Induced ADCC Published preclinical data suggest that off-target effects of ibrutinib may be detrimental to CD20 mab-induced ADCC and the activity of the combination In a human MCL xenograft model, the combination of BGB-3111 and CD20 antibody demonstrated improved anti-tumor activity as compared to monotherapies and combination of ibrutinib and CD20 antibody 1 Li N, et al. Cancer Res. 2015;75:2597 [abstract]. 28
29 BGB-3111+Obinutuzumab: Patient and Disease Characteristics Characteristic CLL/SLL (n = 45) FL (n = 17) Age, years, median (range) 68 (38-82) 56 (41-86) ECOG Performance Status, (%) Follow-up, months, median (range) Prior Treatment Status Treatment-naïve, n (%) Relapsed/refractory, n (%) Number of prior therapies, median (range) 19 (42.2) 25 (55.6) 1 (2.2) 6.5 ( ) 20 (44.4) 25 (55.6) 1 (1-4) 14 (82.4) 2 (11.8) 1 (5.9) 7.9 ( ) 0 17 (100) 3 (1-7) Bulky Disease*,n (%) 0 2 (11.8) Molecular Risk Factors, n (%) del17p/p53mut (n = 37) 11q- (n = 37) IGHV unmutated (n = 37) Complex karyotype (n = 37) * Any lymph node >10 cm in maximum diameter. 6 (16.2) 6 (16.2) 19 (51.4) 7 (18.9) N/A N/A N/A N/A 29
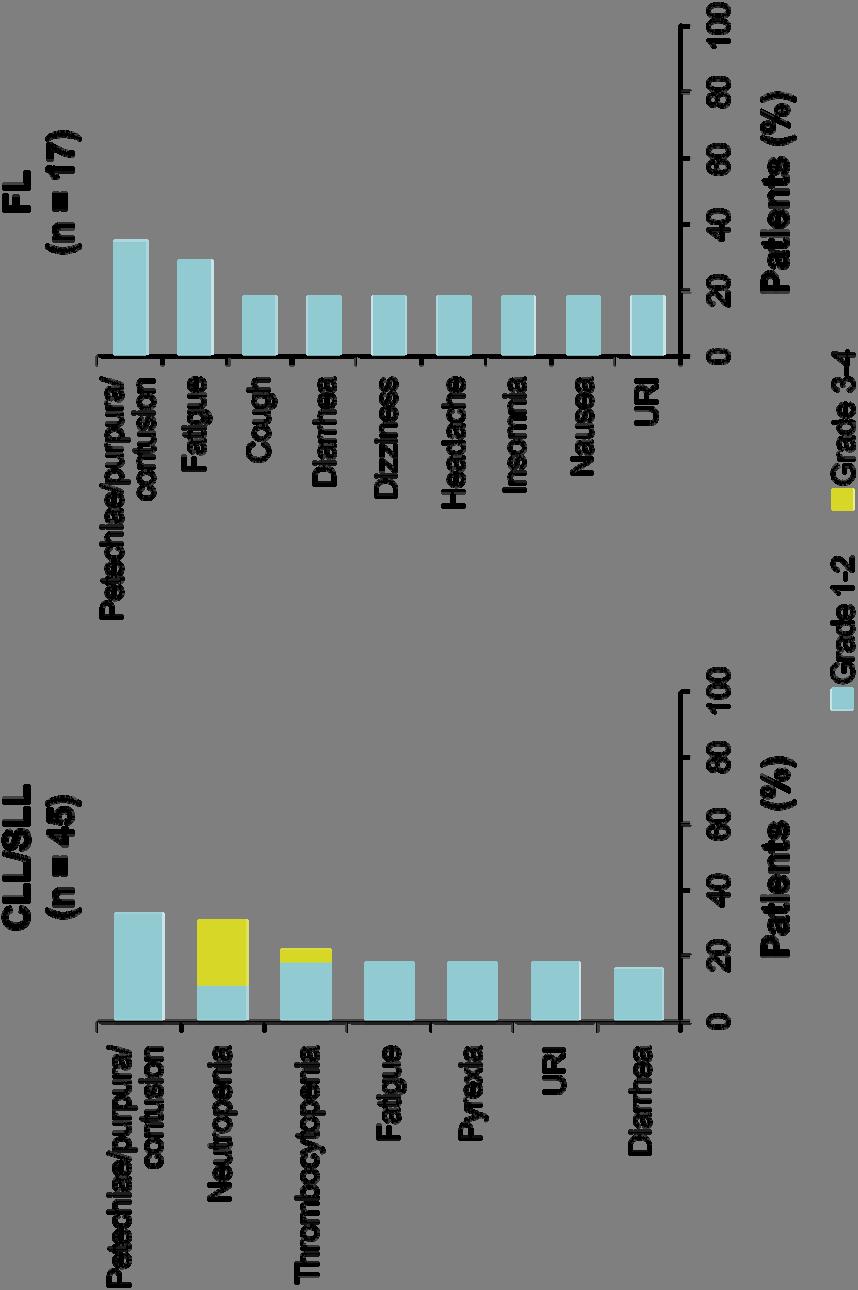
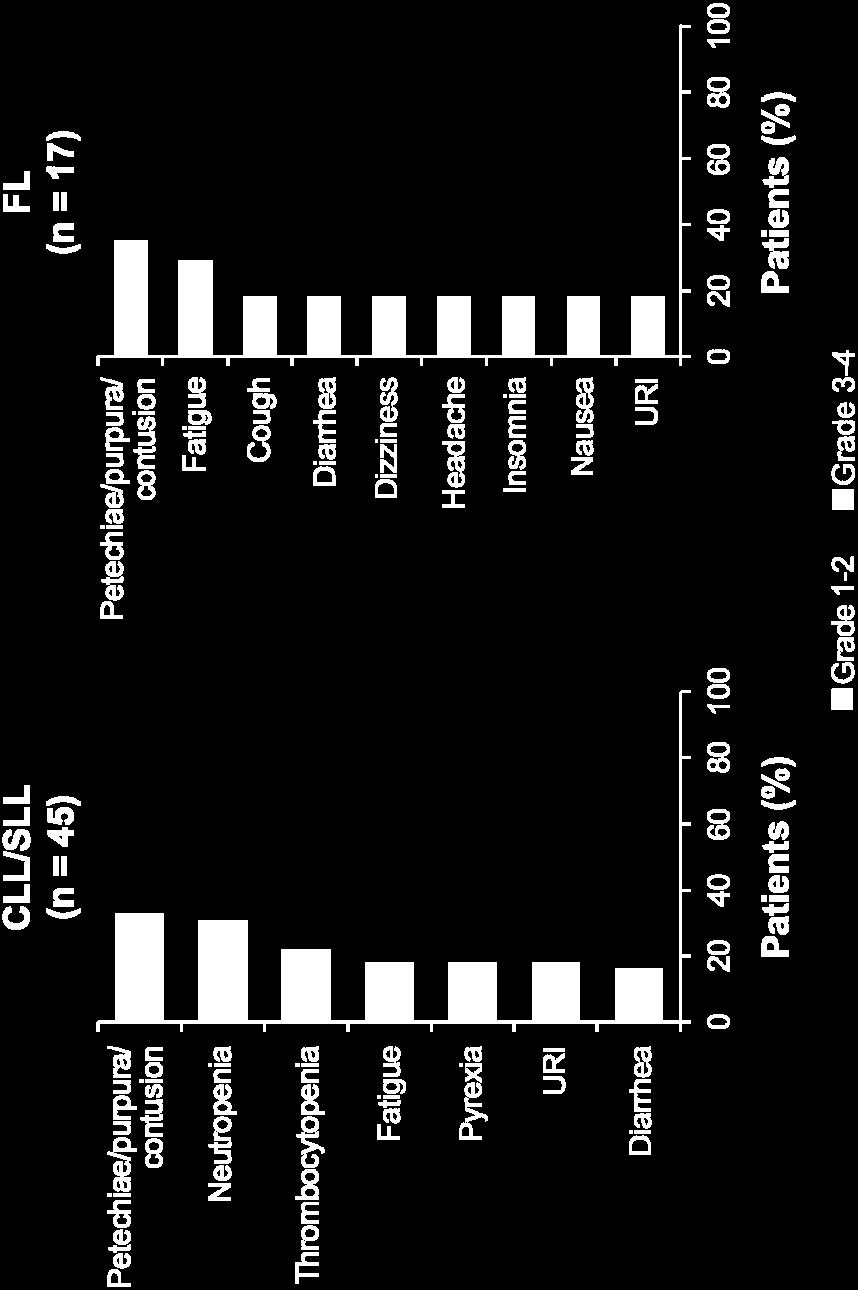
30 BGB-3111+Obinutuzumab: Most Common Adverse Events (Regardless of Causality) 30
31 BGB-3111+Obintuzumab: Adverse Events Event, n (%) CLL/ SLL (n = 45) FL (n = 17) Patients with at least one AE Grade 3 19 (42.2) 4 (23.5) Patients with at least one SAE 11 (24.4) 4 (23.5) Events leading to treatment discontinuation 1 (2.2)* 0 * Patient with a history of squamous cell carcinoma discontinued due to squamous cell carcinoma AE of Special Interest, n (%) CLL/SLL (n = 45) FL (n = 17) All Grade Grade 3-4 All Grade Grade 3-4 Diarrhea 7 (15.6) 0 3 (17.6) 0 Serious hemorrhage* Atrial fibrillation Infusion-related reactions 11 (24.4) 1 (2.2) 1 (5.9) 0 * >Grade 3 hemorrhage, or central nervous system hemorrhage of any grade. 31
32 BGB-3111+Obinutuzumab: Disease Response Follow-up and Response Median follow-up, mo (range) TN CLL/SLL R/R CLL/SLL FL (n = 18) (n = 25) (n = 15) 7.0 ( ) 8.0 ( ) 6.2 ( ) Best Response ORR 16 (88.9) 23 (92.0) 11 (73.3) CR 4 (22.2) 4 (16.0) 5 (33.3) PR 12 (66.7) 19 (76.0) 6 (40.0) PR-L 0 0 N/A SD 2 (11.1) 1 (4.0) 2 (13.3) PD 0 1 (4.0) 2 (13.3) As of 31 March 2017, all responses (CLL and FL) are ongoing (range 3-12 months) 32
33 Conclusions The potent and selective BTK inhibitor BGB-3111 and the anti-cd20 antibody obinutuzumab are safe and well-tolerated when given in combination in patients with CLL/SLL and FL The combination of BGB-3111 and obinutuzumab is highly active in CLL/SLL and FL Early CR rate in CLL/SLL is favorable compared to the expected rate with BTK-inhibitors or anti-cd20 antibodies alone Both the frequency and depth of response in FL (overall and complete response rates) are favorable compared to reported data with BTKinhibitors or anti-cd20 antibodies alone BeiGene is planning late-stage trials of this combination in FL 33
34
35 BGB-3111 Near-Term Development Strategy Current data suggest potential best-in-class attributes Response depth, response durability, and tolerability as a monotherapy Preliminary evidence of augmented activity in combination with obinutuzumab BeiGene s overall global plan is to develop BGB-3111 broadly, pursuing approvals in multiple indications and broadly-defined patient populations Near-term development considerations WM: maturing monotherapy data continue to support ongoing Phase 3 trial vs. ibrutinib. CLL: The data from the updated Phase 1 monotherapy experience supports approvaldirected development in a broad initial treatment CLL population. FL: Unmet medical need exists (failed at least 2 prior lines of therapy and progression within one year of last treatment). Initial efficacy results with BGB-3111+obinutuzumab combination support an expedited development trial in this unmet need population, plus a confirmatory study in a broader (earlier line) FL population.
36 BGB-3111 Phase 3 Study Design in WM MYD88 WT (n~15-20) BGB mg po bid to progression Assess for CR/VGPR, MRR rates and safety R/R WM or TN WM inappropriate for chemoimmunotherapy Age 18y Indication for treatment per IWWM ECOG 0-2 No prior BTK inhibitor MYD88 mutated N=150 Randomize 1:1 BGB mg BID to progression N=75 Ibrutinib 420mg QD to progression N=75 Primary Endpoint CR/VGPR rate Secondary Endpoint MRR (>PR) PFS Duration of response Symptom resolution Stratification factors at randomization: CXCR4 status (WHIM vs WT) No. of lines of prior therapy (0 vs. 1-3 vs. >3) 36
37 BGB-3111 in WM: ICML update continues to support the ongoing global head-to-head pivotal trial With a median follow-up of 12.3mo, VGPR of 43% compares very favorably to VGPR of 13-16% of ibrutinib with longer follow up^ BGB-3111 (IWWM 2016) BGB-3111 (ASH 2016) Responses occurred across mutation statuses including patients with MYD88 wild-type background Global pivotal trial enrolling well with the opportunity to establish superiority over SOC Estimated 22,500 new cases worldwide each year BGB-3111 (14-ICML) Ibrutinib (Treon) Ibrutinib (PCYC-1127) n Follow-up (med) 8.0 mo 9.6 mo 12.3 mo 19.1 mo* 17.1 mo VGPR 33% 34% VGPR 43% VGPR 16% VGPR 13% VGPR Genotype N=31* MYD88 L265P /CXCR4 WT (n = 22) MYD88 L265P /CXCR4 WHIM (n = 4) MYD88 WT (n = 5) Best Response VGPR PR MR SD 11 (50%) 1 (25%) 1 (20%) 7 (32%) 2 (50%) 1 (20%) 2 (9%) 1 (25%) 2 (40%) 2 (9%) 0 1 (20%) Notes: ^ Cross-trial comparison; * Not reported, treatment duration being 19.1 mo; Genotyping results available for 31 patients Source: Tam et al., IWWM, 2016; Tam et al., ASH, 2016; Trotman et al., 14-ICML, 2017; Treon et al., NEJM, 2015; Dimopoulos et al., EHA, 2016; Fonseca, et al., Br J Haematol,
38 BGB-3111 Phase 3 Study Design in Treatment-Naïve CLL del17p or p53 mutation (n~47) BGB mg BID to progression Assess for response and safety Previously Untreated CLL/SLL Indication for treatment per iwcll Unsuitable for treatment with FCR ECOG 0-2 No prior BTK inhibitor No del17p or p53 mutation (n=420) Randomize 1:1 BGB mg BID to progression N=210 Bendamustine + Rituximab N=210* Primary Endpoint PFS Secondary Endpoints ORR Duration of response OS Patient-reported outcomes *crossover allowed at progression 38
39 BGB-3111 for CLL: positioned for broad opportunity in 1L CLL ICML update maintains high responses in larger dataset in all treatment settings Response TN (n = 16) R/R (n = 50) Total (n = 66) Median follow-up, mo (range) 7.6 ( ) 14.0 ( ) 10.5 ( ) ORR 16 (100%) 46 (92%) 62 (94%) Very low rate of discontinuation (3%) due to any event, 1 AE and 1 PD out of 69 patients with a median follow-up of 10.5 mo Plan to initiate pivotal trial in CLL front line against BR, considered most broadly applicable standard-of-care Estimated 191,000 new cases of CLL and 61,000 deaths worldwide; 20,110 new cases and 4,660 deaths in the U.S. each year BR is frequently used as a SOC for healthy, elderly patients, representing the largest segment of CLL CLL Patient Subtypes and SOC Del17p Ibr >65 yo, comorbidity Chl / RTX or Chl / Ob >65 yo, healthy BR <65 yo, healthy FCR or FR or BR 39
40 BGB-3111 Phase 2 Pivotal Study Design in Relapsed or Refractory Follicular Lymphoma BGB Obinutuzumab N=140 Relapsed or refractory FL At least 2 prior lines of therapy Progression within 12 months of last treatment or refractory to last treatment N=210 2:1 Randomisation Stratification factors: number of prior lines of therapy (2-3 and > 3) Study Endpoints: Primary ORR Secondary Duration of Response PFS OS Time-to-response Obinutuzumab* N=70 *option to add BGB-3111 after 12 months if no response 40
41 BGB-3111 for FL: Potential Rapid Entry into a Large Market Segment by Addressing a High Unmet Medical Need FL represents a significant market Significant unmet medical need: patients failed at least 2 prior lines of therapy and progression within one year of last treatment BGB-3111/ obinutuzumab combination highly active in a treatment setting where ibrutinib is not yet approved Early frequency and depth of responses in FL (73% ORR and 33% CR) compares favorably to reported data with BTK inhibitors or anti-cd20 antibodies alone^ BGB-3111 & Obinutuzumab Significant Market (FL) 1,2 Accounts for ~35% of NHLs, one of the most common forms Estimated 140,000 new cases worldwide each year Estimated 25,000 new cases in the U.S. each year ~50% of blockbuster drug Rituximab oncology revenue reported to come from FL Ibrutinib 3 Obinutuzumab 4 Idelalisib 5 n Population Prior alkylator and CD20, mixed Rituxansensitive and -refractory Prior alkylator and CD20, last response <12 months Mixed Rituxansensitive and - refractory Alkylator and Rituxanrefractory relapse Follow-up (med) 7.9 mo 27.7 mo 33.7 mo NR ORR 73% 21% 50% 54% CR 33% 11% 18% 6% Notes: ^ cross-trial comparison Source: Tam et al., 14-ICML, 1 SEER, 2 GLOBOCAN; 3 Gopal, et al ASH 2016; 4 Salles, et al J Clin Oncol 2013; 5 Gopal, et al N Engl J Med
42 BGB-3111 Near-Term Development Plan Global Monotherapy Global Combination China Current Phase 1 CLL, WM, MCL, DLBCL, FL, MZL, HCL, RT Phase vs ibrutinib 1L WM Phase 1b GA101 CLL, FL, DLBCL, NHL Phase 1b A317 FL, DLBCL+, 1 CNS lymphoma Phase 1 B-cell Malignancies Phase 2 Mono in RR MCL Phase 2 Mono in RR CLL/SLL Future Proof of Concept Trial Registrational Trial Phase vs BR 1L CLL Phase G vs G R/R FL Phase 3 Confirmatory Trial in Earlier-line treatment of FL Phase 2 Monotherapy RR WM Phase 2 Monotherapy RR DLBCL Phase vs chlorambucil in 1L CLL/SLL Phase 1b rituximab 42
43 BGB-3111 Clinical Development Summary Expanding program with close to 500 patients treated to date 2017 Phase 3/ Registrational Programs China- accelerated programs in relapsed/ refractory CLL and MCL On track for filing Best-in-class Phase 3 Trial in Waldenstrom macroglobulinemia Superiority comparison (VGPR) with ibrutinib First-in-class registrational opportunity in follicular lymphoma (in combination with obinutuzumab)* Phase 3 trial in broad first-line CLL population* Broad Phase 2/ proof-of-concept program ongoing, including: BGB-3111/ BGB-A317 (anti-pd1) combination DLBCL (including molecular characterization studies) Other B cell malignancies (MCL, MZL, etc.) * Designs of registrational trials in FL and CLL have been discussed with US and EU regulatory authorities 43
44 BeiGene Near-term Milestones Event BGB-3111 (BTK Inhibitor) Present data from the combination study with BGB-A317 at a medical conference Present additional data from the dose-expansion phase of the Phase I monotherapy study Present data from the China Phase I study Expected Timing BGB-A317 (PD-1 Antibody) Present data from the Phase Ia/Ib study in patients with advanced hepatocellular carcinoma at the ESMO 18 th World Congress on Gastrointestinal Cancer Present additional clinical combination data Present data from the dose-expansion phase of the ongoing Phase I trials June 28-July 1, BGB-290 (PARP Inhibitor) Present updated Phase I monotherapy study data 2017 Initiate additional registrational trials globally and in China with our portfolio compounds in

45
46 Appendix 46
47 BGB-3111 Phase 1 Trial Design DOSE ESCALATION Dose Enrolled (WM) 40 mg QD 4 (1) 80 mg QD 5 (2) 160 mg QD 6 (1) 320 mg QD 6 (0) 160 mg BID 4 (0) Eligibility: 1 prior therapy (relapsed cohorts only) No available higher priority treatment ECOG 0-2 ANC >1,000/µl, PLT >50,000/µl RP2D 320 mg 320 BIDmg QD or 160 mg BID Population Relapsed/Refractory Relapsed/Refractory DOSE EXPANSION RP2D Dose BID or QD BID Disease MCL, MZL, FL, GCB DLBCL, WM Non-GCB DLBCL Planned (WM enrolled) 40 (2) Relapsed/Refractory BID CLL/SLL 70 Relapsed/Refractory BID WM 20 (20) Relapsed/Refractory QD CLL/SLL 20 Relapsed/Refractory or Treatment-naïve 40 BID or QD WM 50 (22) Relapsed/Refractory BID or QD MCL 20 Treatment-naive BID or QD CLL/SLL 20 Treatment-naive BID or QD MCL 20 Relapsed/Refractory BID or QD HCL 10 Relapsed/Refractory BID inhl 40 Relapsed/Refractory BID Richter Transform. 15 NCT Relapsed/Refractory from prior btk-i BID WM 15 47
48 WM: Patient Disposition Enrolled/Safety Population N = 48 (38 R/R,10 TN) Not Evaluable for Efficacy < 12 weeks follow-up (n = 2) IgM < 500 mg/dl (n = 3) IgM inaccurate due to cryoprotein (n = 1) Efficacy Population n = 42 (33 R/R, 9 TN) As of March 31, 2017 On Study Treatment n = 44 (1/44 has PD but remains on study drug due to clinical benefit Off Study PD: n = 1 AE: n = 3 48
49 WM: Modified IWWM Response Criteria Category Complete Response (CR) Very Good Partial Response (VGPR) Partial Response (PR) Minor Response (MR) Criteria Normal serum IgM values Disappearance of monoclonal protein by immunofixation No histological evidence of bone marrow involvement Complete resolution of lymphadenopathy/splenomegaly (if present at baseline) 90% reduction of serum IgM from baseline or normal IgM values Reduction in lymphadenopathy/splenomegaly (if present at baseline) 50% reduction of serum IgM from baseline Reduction in lymphadenopathy/splenomegaly (if present at baseline) At least 25% but <50% reduction of serum IgM from baseline Stable Disease (SD) Not meeting criteria for CR, VGPR, PR, MR, or progressive disease Progressive Disease (PD) At least one of the following: Confirmed 25% increase in serum IgM and total increase of 500 mg/dl from nadir (on treatment) New lymph nodes >1.5 cm, or 50% increase from nadir in SPD of >1 node, or 50% increase in longest diameter of previously identified node >1 cm in short axis New splenomegaly or 50% increase from nadir in enlargement New extranodal disease New or recurrent involvement in bone marrow New symptomatic disease Owen RG, et al. Br J Haematol. 2013;160:
 IgM HgB 39 38 36")

50 WM: Decreased IgM and Improved Hemoglobin Levels over time At risk (n) IgM HgB
51 WM: Response Rate By MYD88 Mutation Status Preliminary Results (n = 31*) Genotype N=31* Best Response VGPR PR MR SD MYD88 L265P /CXCR4 WT (n = 22) 11 (50%) 7 (32%) 2 (9%) 2 (9%) MYD88 L265P /CXCR4 WHIM (n = 4) 1 (25%) 2 (50%) 1 (25%) 0 MYD88 WT (n = 5) 1 (20%) 1 (20%) 2 (40%) 1 (20%) * Patients evaluable for response with mutation data 51
52 WM: Efficacy by Prior Treatment Treatment-naive N=9 Relasped/refractory N=33 Total N=42 Median follow-up (range) 9.3 months ( ) 15.5 months ( ) 12.3 months ( ) Best Response CR VGPR PR MR SD 0 2 (22%) 5 (56%) 2 (22% (49%) 9 (27%) 4 (12%) 4 (12%) 0 18 (43%) 90% 76% 14 (33%) ORR MRR* 6 (14%) 4 (10%) * Major response rate. Overall response rate. 52
53 WM: Intrapatient Dose Escalation S401: Initial dose 40mg QD S101: Initial dose 80mg QD Increase to 80mg QD Increase to 160mg QD Increase to 160mg QD Increase to 160mg BID 53
54 WM: IWWM Response Over Time on Treatment: 21 patients on study >12 months 100% 80% 19% Response Rate 60% 40% 76% 57% 57% 23% VGPR PR MR SD 20% 0% 10% 10% 14% 14% Cycle 3 (n = 21) Cycle 6 (n = 21) 10% 10% Cycle >= 12 (n = 21) 54
55 CLL/ SLL: Patient Disposition Enrolled/Safety Population N = 69 (18 TN, 51 R/R) Dose escalation (n = 4) Dose expansion (n = 65) < 12 weeks of follow-up n = 3 (2 TN, 1 R/R) Efficacy Population n = 66 (16 TN, 50 R/R) Currently on Study Treatment n = 67 As of March 31, 2017 Off study n = 2 (1 AE, 1 Hodgkins Transformation) AE, adverse event; CLL/SLL, chronic lymphocytic leukemia/small lymphocytic lymphoma; R/R, relapsed/refractory; TN, treatment naïve. 55
56 CLL: Kinetics of ALC and SPD Response 56

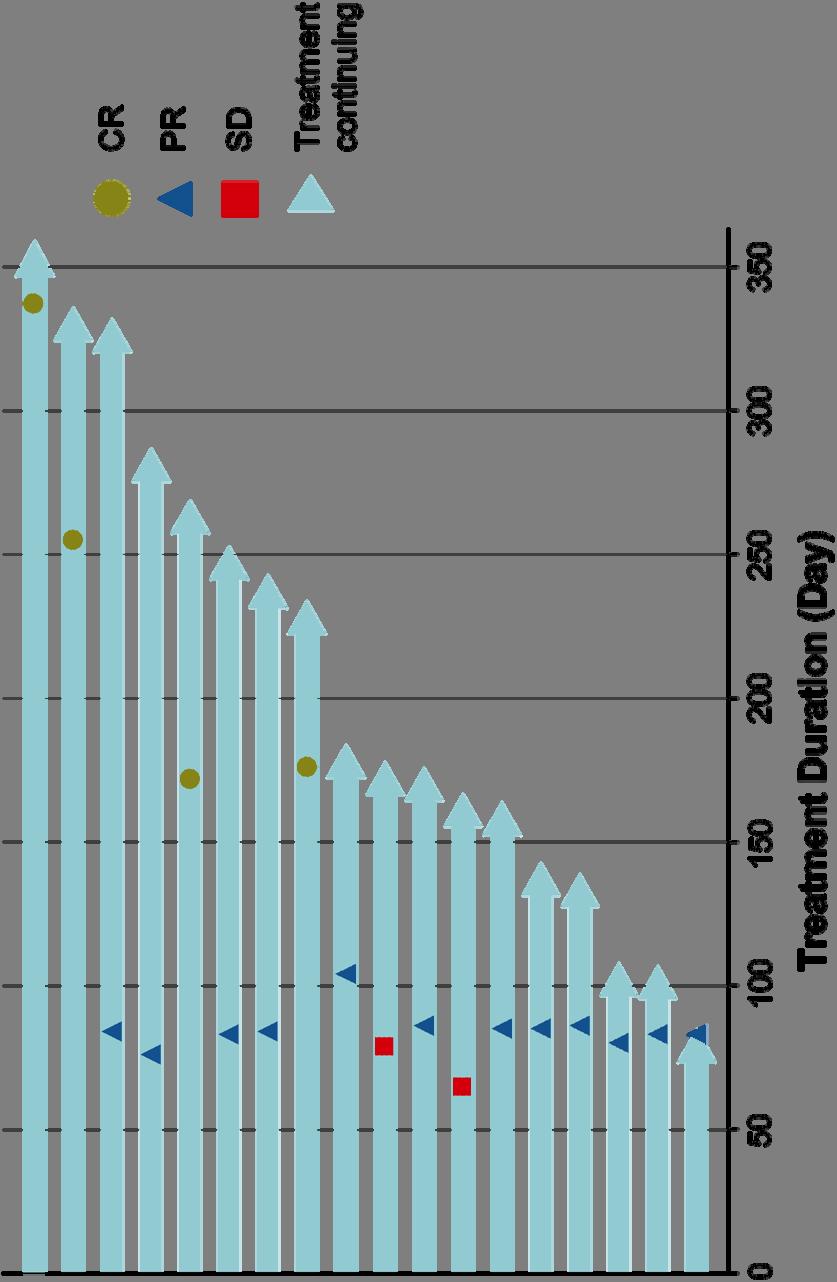
57 BGB-3111+Obinutuzumab in R/R CLL/SLL: Duration of Treatment 57
58 Study Design: BGB-3111 in Combination with Obinutuzumab Cohort BGB-3111* (D1-28/28-day cycles) DOSE ESCALATION Obinutuzumab Patients Dosed 1a 320 mg QD Cycle 1 D2: 100 mg Cycle 1 D3: 900 mg Cycle 1 D9 and D16: 1000 mg Cycles 2-6 D1: 1000 mg 1b 160 mg BID 5 4 * BGB-3111 treatment continued until progression, death, or unacceptable toxicity. Cohort -1a and -1b will be opened if 2 or more DLTs are observed in Cohorts 1a and 1b. Eligibility: WHO defined B cell lymphoid malignancy 1 prior therapy (relapsed cohorts only) No available higher priority treatment ECOG 0-2 ANC >1,000/µl, platelets >40,000/µl Adequate renal and hepatic function No significant cardiac disease Growth factor/transfusion allowed. Anti-coagulation allowed. DOSE EXPANSION Pop Disease Planned TN CLL/SLL 20 R/R CLL 20 R/R non-gcb DLBCL 20 R/R FL, MCL, MZL, and WM 20 R/R FL 40 NCT
59 BGB-3111+Obinutuzumab: CLL/SLL Patient Disposition As of March 31,
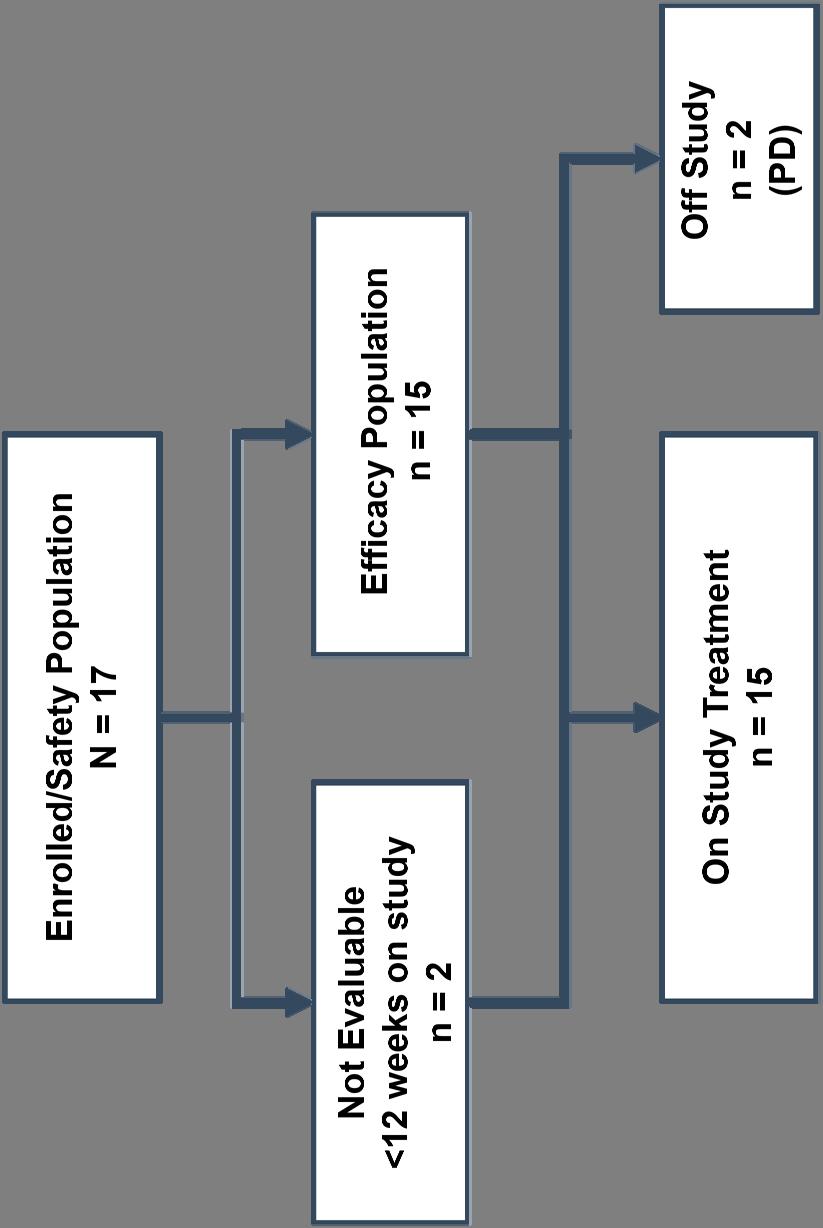
60 BGB-3111+Obinuzumab: FL Patient Disposition As of March 31,
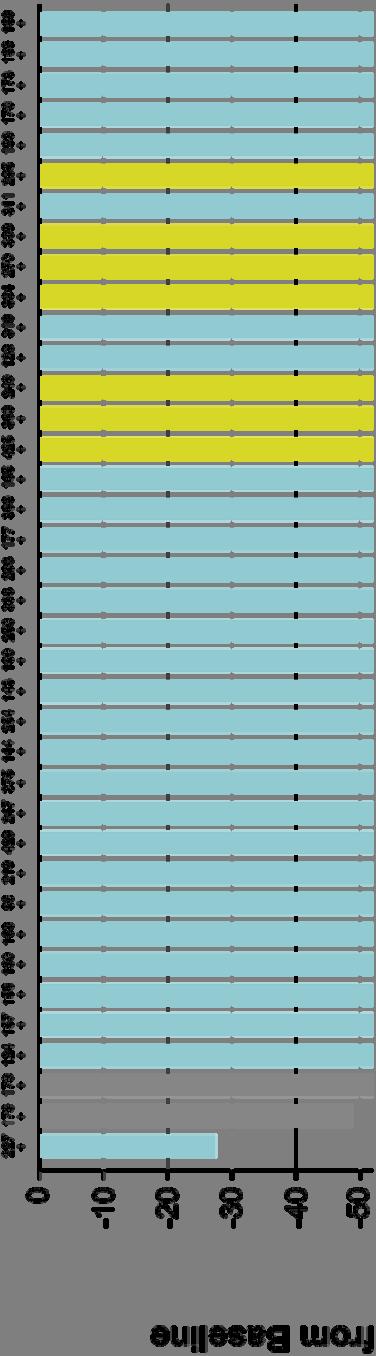
61 BGB-3111+Obinuzumab in CLL/SLL: Maximum Improvement in SPD 61

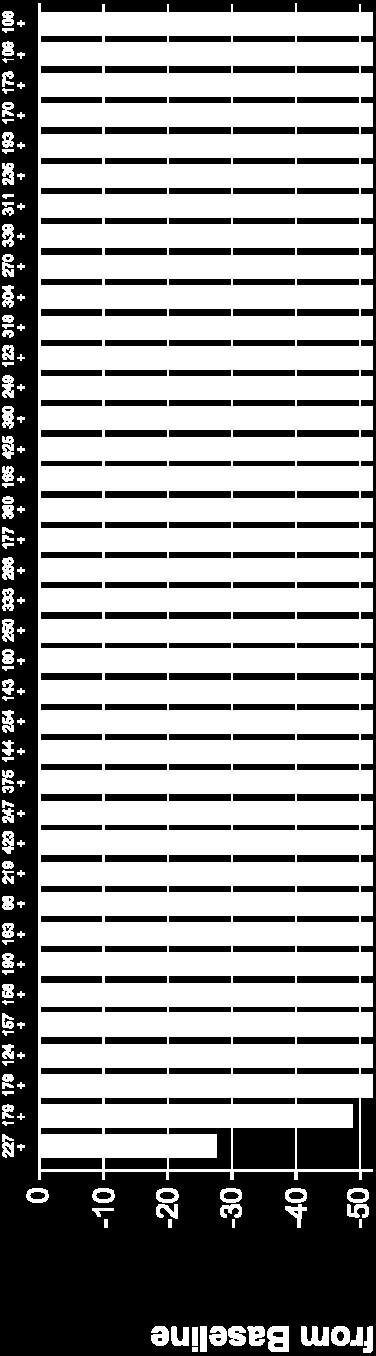
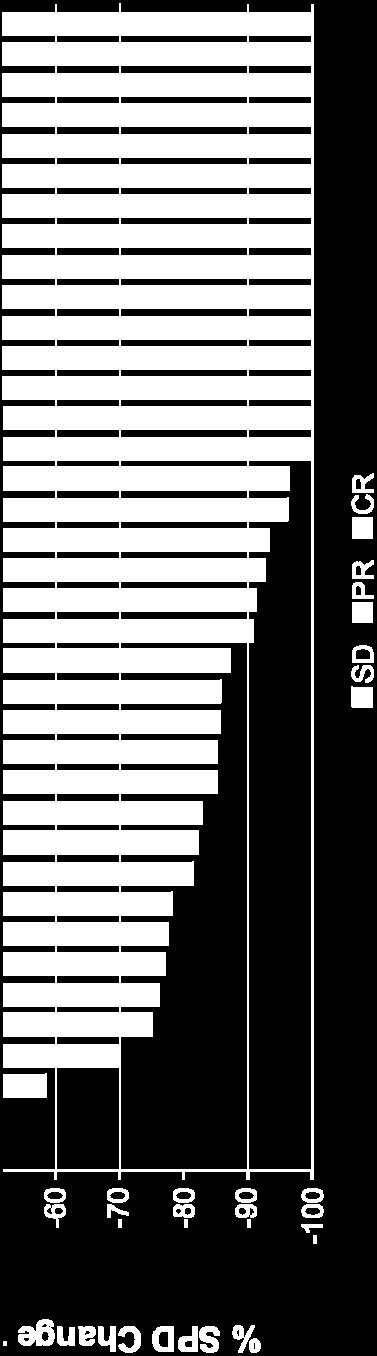
62 BGB-3111+Obinuzumab in FL: Maximum Improvement in SPD 62

63 BGB-3111+Obinutuzumab in TN CLL/SLL: Duration of Treatment 63

64 BGB-3111+Obinutuzumab in FL: Duration of Treatment 64

65 BGB-3111+Obinutuzumab in CLL/SLL: Progression-Free Survival 65

66 BGB-3111+Obinutuzumab in FL: Progression-Free Survival 66
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia
 Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
Constan'ne S Tam Victorian Comprehensive Cancer Center Melbourne, Australia BGB-3111: Kinase Selec.vity Rela.ve to Ibru.nib Equipotent against BTK compared to ibru.nib Higher selec.vity vs EGFR, ITK, JAK3,
Disclosures. I receive honoraria and research funding from Beigene, Janssen and AbbVie.
 Improved depth of response with increased follow-up in phase 1 trial of patients with Waldenström macroglobulinemia (WM) treated with oral Bruton tyrosine kinase (BTK) inhibitor zanubrutinib (BGB-3111)
Improved depth of response with increased follow-up in phase 1 trial of patients with Waldenström macroglobulinemia (WM) treated with oral Bruton tyrosine kinase (BTK) inhibitor zanubrutinib (BGB-3111)
Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111)
 and Zanubrutinib (BGB-3111)") Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111) Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia
Second Generation BTK Inhibitors Acalabrutinib (ACP-196) and Zanubrutinib (BGB-3111) Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia
BTK Inhibitors and BCL2 Antagonists
 BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
BTK Inhibitors and BCL2 Antagonists Constantine (Con) S. Tam Director of Haematology, St Vincent s Hospital Melbourne; Lead for Chronic Lymphocytic Leukemia and Indolent Lymphoma, Peter MacCallum Cancer
Building a Fully Integrated Biopharmaceutical Company. June 2014
 Building a Fully Integrated Biopharmaceutical Company June 2014 Forward-Looking Statements This presentation contains forward-looking statements within the meaning of The Private Securities Litigation
Building a Fully Integrated Biopharmaceutical Company June 2014 Forward-Looking Statements This presentation contains forward-looking statements within the meaning of The Private Securities Litigation
Background. Approved by FDA and EMEA for CLL and allows for treatment without chemotherapy in all lines of therapy
 Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
BR is an established treatment regimen for CLL in the front-line and R/R settings
 Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia
, a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia") Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia Susan M. O Brien 1, Manish R. Patel 2,3, Brad Kahl 4, Steven Horwitz 5,
Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia Susan M. O Brien 1, Manish R. Patel 2,3, Brad Kahl 4, Steven Horwitz 5,
ASH POSTER: LYMRIT UPDATE
 ASH POSTER: LYMRIT 37-01 UPDATE DECEMBER 2018 EDUARDO BRAVO, CEO LISA ROJKJAER, MD, CMO Nordic Nanovector ASA Kjelsåsveien 168 B, 0884 Oslo, Norway www.nordicnanovector.com IR contact: ir@nordicnanovector.com
ASH POSTER: LYMRIT 37-01 UPDATE DECEMBER 2018 EDUARDO BRAVO, CEO LISA ROJKJAER, MD, CMO Nordic Nanovector ASA Kjelsåsveien 168 B, 0884 Oslo, Norway www.nordicnanovector.com IR contact: ir@nordicnanovector.com
NASDAQ: TGTX. 33 rd Annual JP Morgan Healthcare Conference
 NASDAQ: TGTX 33 rd Annual JP Morgan Healthcare Conference January 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities
NASDAQ: TGTX 33 rd Annual JP Morgan Healthcare Conference January 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities
NASDAQ: TGTX Jefferies Healthcare Conference June 2015
 NASDAQ: TGTX Jefferies Healthcare Conference June 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
NASDAQ: TGTX Jefferies Healthcare Conference June 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia
 Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Janssen Hematologic Malignancy Portfolio
 Janssen Hematologic Malignancy Portfolio Recorded Webcast: Update for Analysts and Investors January 216 Oncology 1 Safe Harbor Statement This webcast contains "forward-looking statements" as defined in
Janssen Hematologic Malignancy Portfolio Recorded Webcast: Update for Analysts and Investors January 216 Oncology 1 Safe Harbor Statement This webcast contains "forward-looking statements" as defined in
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Pharmacyclics Reports Updated Clinical Results from its Phase IA Trial of its First in Human BTK- Inhibitor PCI-32765
 Contact: Ramses Erdtmann Vice President of Finance Phone: 408-215-3325 Pharmacyclics Reports Updated Clinical Results from its Phase IA Trial of its First in Human BTK- Inhibitor PCI-32765 Company to Host
Contact: Ramses Erdtmann Vice President of Finance Phone: 408-215-3325 Pharmacyclics Reports Updated Clinical Results from its Phase IA Trial of its First in Human BTK- Inhibitor PCI-32765 Company to Host
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
NASDAQ: TGTX. J.P. Morgan Healthcare Conference January 2017
 NASDAQ: TGTX J.P. Morgan Healthcare Conference January 2017 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
NASDAQ: TGTX J.P. Morgan Healthcare Conference January 2017 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia
 Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia Edward Libby M.D. Associate Professor, University of Washington Department of Medicine, Division of Medical Oncology Fred Hutchinson
Clinical Trial News on the Treatment of Waldenstrom s Macroglobulinemia Edward Libby M.D. Associate Professor, University of Washington Department of Medicine, Division of Medical Oncology Fred Hutchinson
POST ICML Indolent lymphomas relapse treatment
 POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced CLL and NHL
, ublituximab, and ibrutinib in patients with advanced CLL and NHL") Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Highlights in chronic lymphocytic leukemia
 Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Management of CLL in the Targeted Therapy Era
 Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
Management of CLL in the Targeted Therapy Era Jennifer A. Woyach, MD The Ohio State University The Ohio State University Comprehensive Cancer Center Arthur G. James Cancer Hospital and Richard J. Solove
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
Department of Medicine, Division of Hematology-Oncology, Weill Cornell Medical College, New York, NY 3
 The Bruton s Tyrosine Kinase (BTK) Inhibitor Ibrutinib (PCI-32765) is Highly Active and Tolerable in Treatment Naïve (TN) Chronic Lymphocytic Leukemia (CLL) Patients: Interim Results of a Phase Ib/II Study
The Bruton s Tyrosine Kinase (BTK) Inhibitor Ibrutinib (PCI-32765) is Highly Active and Tolerable in Treatment Naïve (TN) Chronic Lymphocytic Leukemia (CLL) Patients: Interim Results of a Phase Ib/II Study
REWRITING CANCER TREATMENT THROUGH EPIGENETIC MEDICINES
 REWRITING CANCER TREATMENT THROUGH EPIGENETIC MEDICINES May 18, 2017 Molecularly Defined Solid Tumor Program Update FORWARD-LOOKING STATEMENTS Any statements in this press release about future expectations,
REWRITING CANCER TREATMENT THROUGH EPIGENETIC MEDICINES May 18, 2017 Molecularly Defined Solid Tumor Program Update FORWARD-LOOKING STATEMENTS Any statements in this press release about future expectations,
Chronic Lymphocytic Leukemia Update. Learning Objectives
 Chronic Lymphocytic Leukemia Update Ashley Morris Engemann, PharmD, BCOP, CPP Clinical Associate Adult Stem Cell Transplant Program Duke University Medical Center August 8, 2015 Learning Objectives Recommend
Chronic Lymphocytic Leukemia Update Ashley Morris Engemann, PharmD, BCOP, CPP Clinical Associate Adult Stem Cell Transplant Program Duke University Medical Center August 8, 2015 Learning Objectives Recommend
ACALABRUTINIB IN MCL
 ACALABRUTINIB IN MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK BRUTON S TYROSINE KINASE (BTK): A CRITICAL KINASE
ACALABRUTINIB IN MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK BRUTON S TYROSINE KINASE (BTK): A CRITICAL KINASE
CLL & SLL: Current Management & Treatment. Dr. Peter Anglin
 CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
CLL & SLL: Current Management & Treatment Dr. Peter Anglin Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of blood cell B lymphocyte Lymphocytic Cancer of white blood
Media Inquiries: Satu Glawe Phone: Bernadette King Phone:
 Media Inquiries: Satu Glawe Phone: +49-172-294-6264 Bernadette King Phone: 1-215-778-3027 Investor Relations: Christopher DelOrefice Phone: 1-732-524-2955 Lesley Fishman Phone: 1-732-524-3922 U.S. Medical
Media Inquiries: Satu Glawe Phone: +49-172-294-6264 Bernadette King Phone: 1-215-778-3027 Investor Relations: Christopher DelOrefice Phone: 1-732-524-2955 Lesley Fishman Phone: 1-732-524-3922 U.S. Medical
CLL: disease specific biology and current treatment. Dr. Nathalie Johnson
 CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
TarGeting B-Cell Diseases
 TarGeting B-Cell Diseases Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements
TarGeting B-Cell Diseases Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. These statements
Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division
 Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division University of Virginia Cancer Center The Clinical Continuum of CLL Early asymptomatic
Raising the Bar in CLL Michael E. Williams, MD, ScM Byrd S. Leavell Professor of Medicine Chief, Hematology/Oncology Division University of Virginia Cancer Center The Clinical Continuum of CLL Early asymptomatic
Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies
 December 10, 2013 Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies -- Clinical Presentation in Waldenstrom's Macroglobulinemia Deemed "Best of ASH" -- NEW ORLEANS, Dec. 10,
December 10, 2013 Pharmacyclics Announces Data Presentations for Ibrutinib in B-Cell Malignancies -- Clinical Presentation in Waldenstrom's Macroglobulinemia Deemed "Best of ASH" -- NEW ORLEANS, Dec. 10,
BTKi in MCL. Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK
 BTKi in MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK 2 Table of Various Treatment for R/R MCL Treatment Study or
BTKi in MCL Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth UK 2 Table of Various Treatment for R/R MCL Treatment Study or
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
DELIVERING NEXT-GENERATION RADIO-IMMUNOTHERAPIES FOR LYMPHOMA PATIENTS
 DELIVERING NEXT-GENERATION RADIO-IMMUNOTHERAPIES FOR LYMPHOMA PATIENTS DNB SME CONFERENCE 4 TH APRIL, 2019 EDUARDO BRAVO, CEO Nordic Nanovector ASA Kjelsåsveien 168 B, 0884 Oslo, Norway www.nordicnanovector.com
DELIVERING NEXT-GENERATION RADIO-IMMUNOTHERAPIES FOR LYMPHOMA PATIENTS DNB SME CONFERENCE 4 TH APRIL, 2019 EDUARDO BRAVO, CEO Nordic Nanovector ASA Kjelsåsveien 168 B, 0884 Oslo, Norway www.nordicnanovector.com
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib
PCI-32765DBL1002. Janssen Research & Development, Raritan, NJ, USA; 9 Janssen Research & Development, Belgrade, Serbia; 10
 Phase 1b Study Combining Ibrutinib With Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone (R-CHOP) in Patients With CD20-Positive B-Cell Non-Hodgkin Lymphoma (NHL) Anas Younes, 1 Ian
Phase 1b Study Combining Ibrutinib With Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone (R-CHOP) in Patients With CD20-Positive B-Cell Non-Hodgkin Lymphoma (NHL) Anas Younes, 1 Ian
Waldenström s Macroglobulinemia: Treatment Approach
 Waldenström s Macroglobulinemia: Treatment Approach Steve Treon MD, PhD Bing Center for Waldenstrom s Macroglobulinemia Dana Farber Cancer Institute Harvard Medical School Primary Therapy of WM with Rituximab
Waldenström s Macroglobulinemia: Treatment Approach Steve Treon MD, PhD Bing Center for Waldenstrom s Macroglobulinemia Dana Farber Cancer Institute Harvard Medical School Primary Therapy of WM with Rituximab
Update: New Treatment Modalities
 ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
Venetoclax in MCL. Prof. Le Gouill Nantes Medical University, France
 Venetoclax in MCL Prof. Le Gouill Nantes Medical University, France Evasion of Apoptosis, or Cell Death, is 1. Resisting Cell Death 2. Sustained angiogenesis for growth and survival (primarily solid tumors)
Venetoclax in MCL Prof. Le Gouill Nantes Medical University, France Evasion of Apoptosis, or Cell Death, is 1. Resisting Cell Death 2. Sustained angiogenesis for growth and survival (primarily solid tumors)
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL
 Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth
 Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth") VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD
: Refresher Course for Hematologists Ekarat Rattarittamrong, MD") Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang-Mai University Outline
Chronic Lymphocytic Leukemia (CLL): Refresher Course for Hematologists Ekarat Rattarittamrong, MD Division of Hematology Department of Internal Medicine Faculty of Medicine Chiang-Mai University Outline
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
Advances in CLL 2016
 Advances in CLL 2016 The Geoffrey P. Herzig Memorial Symposium, Louisville, KY Kanti R. Rai, MD Northwell-Hofstra School of Medicine Long Island Jewish Medical Center New Hyde Park, NY Disclosures Member
Advances in CLL 2016 The Geoffrey P. Herzig Memorial Symposium, Louisville, KY Kanti R. Rai, MD Northwell-Hofstra School of Medicine Long Island Jewish Medical Center New Hyde Park, NY Disclosures Member
US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA
 FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA") US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA Accelerated approval of Bruton tyrosine kinase (BTK) inhibitor in MCL marks AstraZeneca
US FDA APPROVES ASTRAZENECA S CALQUENCE (acalabrutinib) FOR ADULT PATIENTS WITH PREVIOUSLY-TREATED MANTLE CELL LYMPHOMA Accelerated approval of Bruton tyrosine kinase (BTK) inhibitor in MCL marks AstraZeneca
ICML BETALUTIN LYMRIT STUDY UPDATE JUNE 14 TH, 2017
 ICML 2017 - BETALUTIN LYMRIT 37-01 STUDY UPDATE JUNE 14 TH, 2017 Disclaimer This presentation may contain certain forward-looking statements and forecasts based on uncertainty, since they relate to events
ICML 2017 - BETALUTIN LYMRIT 37-01 STUDY UPDATE JUNE 14 TH, 2017 Disclaimer This presentation may contain certain forward-looking statements and forecasts based on uncertainty, since they relate to events
CLL: future therapies. Dr. Nathalie Johnson
 CLL: future therapies Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck Outline Treatment of relapsed
CLL: future therapies Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck Outline Treatment of relapsed
CLL - venetoclax. Peter Hillmen St James s University Hospital Leeds 10 th May 2016
 CLL - venetoclax Peter Hillmen peter.hillmen@nhs.net St James s University Hospital Leeds 10 th May 2016 Pathophysiology of CLL: Proliferation vs Apoptosis Proliferation Apoptosis Ki-67 Expression Bcl-2
CLL - venetoclax Peter Hillmen peter.hillmen@nhs.net St James s University Hospital Leeds 10 th May 2016 Pathophysiology of CLL: Proliferation vs Apoptosis Proliferation Apoptosis Ki-67 Expression Bcl-2
CLL: Future Therapies. Dr. Anca Prica
 CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
CLL: Future Therapies Dr. Anca Prica Treatment Options: Improved by Decade 1960 1970 1980 1990 2000 2017 5% CR 5% CR Chemo Alkylator chlorambucil or cyclophosphamide 25% CR Chemo Purine analogues Fludarabine
Leukemia. Roland B. Walter, MD PhD MS. Fred Hutchinson Cancer Research Center University of Washington
 Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Leukemia Roland B. Walter, MD PhD MS Fred Hutchinson Cancer Research Center University of Washington Discussed Abstracts Confirmatory open-label, single-arm, multicenter phase 2 study of the BiTE antibody
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Building a Leading Oncology Franchise
 ASDAQ: MEIP Building a Leading Oncology Franchise 17th Annual eedham Healthcare Conference March 27, 2018 Forward-Looking Statements This presentation contains, and our officers and representatives may
ASDAQ: MEIP Building a Leading Oncology Franchise 17th Annual eedham Healthcare Conference March 27, 2018 Forward-Looking Statements This presentation contains, and our officers and representatives may
Corporate Presentation June Curis, Inc All Rights Reserved
 Corporate Presentation June 2018 Curis, Inc. 2018 All Rights Reserved Forward Looking Statements This presentation contains certain forward-looking statements about Curis, Inc. ( we, us, or the Company
Corporate Presentation June 2018 Curis, Inc. 2018 All Rights Reserved Forward Looking Statements This presentation contains certain forward-looking statements about Curis, Inc. ( we, us, or the Company
Management of 17p Deleted CLL Patients in the Era of Targeted Therapy
 Management of 17p Deleted CLL Patients in the Era of Targeted Therapy Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November 11,
Management of 17p Deleted CLL Patients in the Era of Targeted Therapy Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November 11,
Treatment Nodal Marginal Zone Lymphoma
 Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Chronic Lymphocytic Leukemia: State of the Art
 14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
14th Annual INDY Hematology Review March 2017 Chronic Lymphocytic Leukemia: State of the Art Adrian Wiestner, MD/PhD Bethesda, MD awiestner@hotmail.com Disclosures Grant/research support: Pharmacyclics
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
FCR and BR: When to use, how to use?
 FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
FCR and BR: When to use, how to use? Mitchell R. Smith, M.D., Ph.D. Director of Lymphoid Malignancy Program Taussig Cancer Institute Cleveland Clinic, Cleveland, OH DEBATE ISSUE 2013: Which is the optimal
Clinical Overview: MRD in CLL. Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel
 Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
Clinical Overview: MRD in CLL Dr. Matthias Ritgen UKSH, Medizinische Klinik II, Campus Kiel m.ritgen@med2.uni-kiel.de Remission in CLL Clinical criteria (NCI->WHO) Lymphadenopathy Splenomegaly Hepatomegaly
Chronic lymphocytic Leukemia
 Chronic lymphocytic Leukemia after IwCLL, ICML and EHA 2017 Ann Janssens, MD, PhD Hematology, UZ Leuven Brussels, 14 september 2017 Front line treatment CLL Active or progressive disease No active or progressive
Chronic lymphocytic Leukemia after IwCLL, ICML and EHA 2017 Ann Janssens, MD, PhD Hematology, UZ Leuven Brussels, 14 september 2017 Front line treatment CLL Active or progressive disease No active or progressive
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
International Conference on Malignant Lymphoma (ICML) June 14-17, 2017
 June 14-17, 2017") International Conference on Malignant Lymphoma (ICML) June 14-17, 2017 INTERIM REPORT FROM A PHASE 2 MULTICENTER STUDY OF TAZEMETOSTAT, AN EZH2 INHIBITOR: CLINICAL ACTIVITY AND FAVORABLE SAFETY IN PATIENTS
International Conference on Malignant Lymphoma (ICML) June 14-17, 2017 INTERIM REPORT FROM A PHASE 2 MULTICENTER STUDY OF TAZEMETOSTAT, AN EZH2 INHIBITOR: CLINICAL ACTIVITY AND FAVORABLE SAFETY IN PATIENTS
Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto)
 and Dr. Matt Cheung (Staff Hematologist, University of Toronto)") CLL Updated March 2017 by Doreen Ezeife Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto) DISCLAIMER: The following
CLL Updated March 2017 by Doreen Ezeife Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff Hematologist, University of Toronto) DISCLAIMER: The following
CONTRAINDICATIONS None (4)
") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use IMBRUVICA safely and effectively. See full prescribing information for IMBRUVICA. PRC-498 IMBRUVICA
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use IMBRUVICA safely and effectively. See full prescribing information for IMBRUVICA. PRC-498 IMBRUVICA
Corporate Presentation. Curis, Inc All Rights Reserved
 Corporate Presentation Curis, Inc. 2018 All Rights Reserved Forward Looking Statements This presentation contains certain forward-looking statements about Curis, Inc. ( we, us, or the Company ) within
Corporate Presentation Curis, Inc. 2018 All Rights Reserved Forward Looking Statements This presentation contains certain forward-looking statements about Curis, Inc. ( we, us, or the Company ) within
We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT
 We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT Danielle M. Brander, MD Duke University Division of Hematologic Malignancies & Cell Therapy CLL & Indolent
We Can Cure Chronic Lymphocytic Leukemia with Current / Soon to be Approved Agents: CON ARGUMENT Danielle M. Brander, MD Duke University Division of Hematologic Malignancies & Cell Therapy CLL & Indolent
BENDAMUSTINE + RITUXIMAB IN CLL
 BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
BENDAMUSTINE + RITUXIMAB IN CLL Barbara Eichhorst Bologna 13. November 2017 CONFLICT OF INTERESTS 1. Advisory Boards Janssen, Gilead, Roche, Abbvie, GSK 2. Honoraria Roche, GSK, Gilead, Janssen, Abbvie,
MMAE disrupts cell division and triggers apoptosis. Pola binds to cell surface antigen CD79b. Pola is internalized; linker cleaves, releasing MMAE
 Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Imbruvica. Imbruvica (ibrutinib) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.41 Subject: Imbruvica Page: 1 of 5 Last Review Date: June 22, 2017 Imbruvica Description Imbruvica
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.41 Subject: Imbruvica Page: 1 of 5 Last Review Date: June 22, 2017 Imbruvica Description Imbruvica
Building a Leading Oncology Franchise
 Building a Leading Oncology Franchise January 2019 NASDAQ: MEIP Forward-Looking Statements This presentation contains, and our officers and representatives may from time to time make, statements that are
Building a Leading Oncology Franchise January 2019 NASDAQ: MEIP Forward-Looking Statements This presentation contains, and our officers and representatives may from time to time make, statements that are
MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients
 MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November
MRD Negativity as an Outcome in CLL: Ongoing Challenges with Del 17p Patients Jennifer R Brown, MD PhD Director, CLL Center Dana-Farber Cancer Institute Associate Professor Harvard Medical School November
*Jagiellonian University, Kraków, Poland
 Single-Agent MOR208 in Relapsed or Refractory (R-R) Non-Hodgkin s Lymphoma (NHL): Results from Diffuse Large B-Cell Lymphoma (DLBCL) and Indolent NHL Subgroups of a Phase IIa Study Wojciech Jurczak, *
Single-Agent MOR208 in Relapsed or Refractory (R-R) Non-Hodgkin s Lymphoma (NHL): Results from Diffuse Large B-Cell Lymphoma (DLBCL) and Indolent NHL Subgroups of a Phase IIa Study Wojciech Jurczak, *
Mathias J Rummel, MD, PhD
 I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
B Kahl 1, M Hamadani 2, P Caimi 3, E Reid 4, K Havenith 5, S He 6, JM Feingold 6, O O Connor 7
 First Clinical Results of ADCT-42, a Novel Pyrrolobenzodiazepine-Based Antibody Drug Conjugate (ADC), in Relapsed/Refractory B-cell Lineage Non-Hodgkin Lymphoma B Kahl 1, M Hamadani 2, P Caimi 3, E Reid
First Clinical Results of ADCT-42, a Novel Pyrrolobenzodiazepine-Based Antibody Drug Conjugate (ADC), in Relapsed/Refractory B-cell Lineage Non-Hodgkin Lymphoma B Kahl 1, M Hamadani 2, P Caimi 3, E Reid
CHMP recommends EU approval of Roche s Gazyvaro for people with previously treated follicular lymphoma
 Media Release Basel, 29 April 2016 CHMP recommends EU approval of Roche s Gazyvaro for people with previously treated follicular lymphoma In the pivotal study, treatment with Gazyvaro plus bendamustine
Media Release Basel, 29 April 2016 CHMP recommends EU approval of Roche s Gazyvaro for people with previously treated follicular lymphoma In the pivotal study, treatment with Gazyvaro plus bendamustine
Update on Waldenström Macroglobulinemia (WM)
") Update on Waldenström Macroglobulinemia (WM) Stephen M. Ansell, MD, PhD Professor of Medicine Division of Hematology Mayo Clinic Rochester, MN Update on Waldenström Macroglobulinemia (WM) Disclosures Stephen
Update on Waldenström Macroglobulinemia (WM) Stephen M. Ansell, MD, PhD Professor of Medicine Division of Hematology Mayo Clinic Rochester, MN Update on Waldenström Macroglobulinemia (WM) Disclosures Stephen
Disclosures WOJCIECH JURCZAK
 Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
CLL what do I need to know as an Internist in Taimur Sher MD Associate Professor of Medicine Mayo Clinic
 CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
CLL what do I need to know as an Internist in 218 Taimur Sher MD Associate Professor of Medicine Mayo Clinic Case 1 7 y/o white male for yearly medical evaluation Doing well and healthy Past medical history
Betalutin, a novel CD37-targeted radioimmunotherapy for NHL. Arne Kolstad Oslo University Hospital 2 October 2018
 Betalutin, a novel CD37-targeted radioimmunotherapy for NHL Arne Kolstad Oslo University Hospital 2 October 2018 Disclosures of: Arne Kolstad Company name Research support Employee Consultant Stockholder
Betalutin, a novel CD37-targeted radioimmunotherapy for NHL Arne Kolstad Oslo University Hospital 2 October 2018 Disclosures of: Arne Kolstad Company name Research support Employee Consultant Stockholder
Company Overview. April Rewriting cancer treatment NASDAQ: EPZM
 Company Overview NASDAQ: EPZM Rewriting cancer treatment Forward Looking Statements This presentation contains forward-looking statements within the meaning of The Private Securities Litigation Reform
Company Overview NASDAQ: EPZM Rewriting cancer treatment Forward Looking Statements This presentation contains forward-looking statements within the meaning of The Private Securities Litigation Reform
Media Release. Basel, 7 November 2013
 Media Release Basel, November 2013 Roche s Gazyva helped people with one of the most common forms of blood cancer live significantly longer without their disease worsening compared to MabThera/Rituxan
Media Release Basel, November 2013 Roche s Gazyva helped people with one of the most common forms of blood cancer live significantly longer without their disease worsening compared to MabThera/Rituxan
Novel treatment options for Waldenstrom Macroglobulinemia
 Novel treatment options for Waldenstrom Macroglobulinemia Irene Ghobrial, MD Associate Professor of Medicine Harvard Medical School Dana Farber Cancer Institute Boston, MA Ghobrial et al, Lancet Oncol
Novel treatment options for Waldenstrom Macroglobulinemia Irene Ghobrial, MD Associate Professor of Medicine Harvard Medical School Dana Farber Cancer Institute Boston, MA Ghobrial et al, Lancet Oncol
7 Recruiting Carfilzomib, Rituximab and Dexamethasone in Waldenstrom's Macroglobulinemia Condition: Waldenstrom's Macroglobulinemia
 1 Recruiting Questionnaire and Tissue Banking For Multiple Myeloma, Waldenstrom and Related Disorders Conditions: Multiple Myeloma; Waldenstrom's ; Smoldering Multiple Myeloma; Lymphoblastic Lymphoma Intervention:
1 Recruiting Questionnaire and Tissue Banking For Multiple Myeloma, Waldenstrom and Related Disorders Conditions: Multiple Myeloma; Waldenstrom's ; Smoldering Multiple Myeloma; Lymphoblastic Lymphoma Intervention:
ArQule Jefferies Global Healthcare Conference June 2015
 ArQule Jefferies Global Healthcare Conference June 2015 1 ArQule Corporate Update Safe Harbor This presentation and other statements by ArQule may contain forward-looking statements within the meaning
ArQule Jefferies Global Healthcare Conference June 2015 1 ArQule Corporate Update Safe Harbor This presentation and other statements by ArQule may contain forward-looking statements within the meaning
eastern cooperative oncology group Michael Williams, Fangxin Hong, Brad Kahl, Randy Gascoyne, Lynne Wagner, John Krauss, Sandra Horning
 Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Brad S Kahl, MD. Tracks 1-21
 I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
CORPORATE PRESENTATION
 CORPORATE PRESENTATION June 2017 FORWARD LOOKING SAFE HARBOR STATEMENT This presentation contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995.
CORPORATE PRESENTATION June 2017 FORWARD LOOKING SAFE HARBOR STATEMENT This presentation contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995.
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014
![[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014](/thumbs/73/68853651.jpg "[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014") [ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
State of the art: CAR-T cell therapy in lymphoma
 State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
Managing patients with relapsed follicular lymphoma. Case
 Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Bcl-2 inhibition in NHL. Jonathan W. Friedberg M.D., M.M.Sc.
 Bcl-2 inhibition in NHL Jonathan W. Friedberg M.D., M.M.Sc. BCL-2, BH3 and apoptosis: Rational therapeutic targets in NHL Antiapoptotic proteins, prevent activation of Bax and Bak, thus inhibiting apoptosis.
Bcl-2 inhibition in NHL Jonathan W. Friedberg M.D., M.M.Sc. BCL-2, BH3 and apoptosis: Rational therapeutic targets in NHL Antiapoptotic proteins, prevent activation of Bax and Bak, thus inhibiting apoptosis.
Corporate Presentation. July 30, 2018
 Corporate Presentation July 30, 2018 Disclosures Certain statements contained in this presentation and in the accompanying oral presentation, other than statements of fact that are independently verifiable
Corporate Presentation July 30, 2018 Disclosures Certain statements contained in this presentation and in the accompanying oral presentation, other than statements of fact that are independently verifiable
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag