Current aspects of renal diseases in HIV infection. Eric DAUGAS Service de Néphrologie Hôpital Bichat Paris France
|
|
|
- Marjorie Thomas
- 5 years ago
- Views:
Transcription
1 Current aspects of renal diseases in HIV infection Eric DAUGAS Service de Néphrologie Hôpital Bichat Paris France
2 1996 = HAART highly active antiretroviral therapy combination of three antiretroviral agents two RTI + one PI or three RTIs
3 Schwartz et al, JASN, 2005
4 EPIDEMIOLOGY of renal diseases in HIV infected patients
5 HIV is a CKD risk factor Gardner et al. J Acquir Immune Defic Syndr. 2003
6 High prevalence of CKD n Proteinuria % Stage 3-5 CKD Szczech LA, Kidney Int, (w) 32 Gupta SK, Clin Nephrol, Overton E, CROI % Fernando SK, Am J Med Sci %
7 CKD is associated with uncontrolled HIV Proteinuria Viral load CD4 200 mm 3 Afro-american HCV Renal failure CD4 200 mm 3 Viral load Hypertension Hypoalbuminemia Szczech LA, Kidney Int, 2002
8 CKD = 3 rd death risk factor in this study Gardner et al. J Acquir Immune Defic Syndr. 2003
9 Acute renal failure Prospective data from 754 patients between 2000 and 2002 incidence = 5.9 %/year #100 x Population générale Risk factors <200 T4/mm 3 Detectable viral load AIDS HCV Franceschini et al. Kidney Int, 2005
10 Modifications of renal diseases profile in HAART era
11 New profile of kidney diseases in HAART era Improved control of HIV Control of HIV-related renal diseases Prolonged life with a continuous exposure to HIV and to therapies Immune reconstitution
12 Proportion % HIV-related Directly due to HIV (group 1) HIVAN TMA Immune complexe GN Related to immune deficiency (group 2) Infiltrative interstitial nephritis (Lymphomas, DILS ) Infectious interstitial nephritis Infectious GN Amyloidosis? Unrelated to HIV context (group 4) Diabetic nephropathy, Vascular nephropathy HCV-related Related to HAART (group 3) Direct nephrotoxicity Indirectly: IRIS pre-haart era HAART era 1996 Time





13 HIVAN: HIV-Associated Nephropathy Kimmel, Barisoni and Kopp; Ann Intern Med; 2003
14 Beneficial effect of Zidovudine on HIVAN course in pre-haart era Cook P.P, J Am Soc Nephrol 1990 Michel C., Nephron 1992 Ifudu O., Am J Nephrol 1995 Kimmel P.L, Am J Kidney Dis 1996



15 HIVAN and HAART Dialysis Proteinuria 10 g/d Creatinine 132 µmol/l Proteinuria #1g/d Wali et al; Lancet 1998





16 HIVAN and HAART Creatinine 557 µmol/l Proteinuria 17 g/d Creatinine 124 µmol/l Protenuria 1.5 g/d Winston et al; NEJM 2001

17 HIVAN/HAART in African American No ART NRT alone HAART Lucas et al, AIDS, 2004
18 HIVAN/HAART in African American Schwartz et al, JASN, 2005
19 HIVAN / HAART in Paris HIVAN on histology patients in pre- HAART era Mean creatinine 496µmol/L versus 33 patients HAART Mean creatinine 592µmol/L renal survival rate ,5 1 3 follow-up (year) Laradi et al, JASN 1998 and Burckle et al; Am Soc Nephrol; 2002
20 Guidelines for HIVAN treatment Gupta SK et al. Clin Infect Dis 2005
21 Immune glomerulonephritis Caucasians Numerous nosologic entities IgA nephritis: 8% prevalence in Beaufils et al NDT 1995 Eluted immune complex including IgA anti-hiv: Kimmel et al, NEJM 1992 Treatment with HAART????
22 Thrombotic microangiopathy Decreased incidence in HAART era Gervasoni et al, Clin Infect Dis, 2002 Becker et al, Clin Infect Dis, 2004 Direct and indirect effect of HIV containment by HAART
23 Renal toxicity of HAART


24 Indinavir Renal and urological disorders related to crystalluria Daudon M et al Lancet May 3;349(9061):1294-5
25 Indinavir (Crixivan ) Clinical manifestations Renal colic /Flank pain / Dysuria/ Gross hematuria Urolithiasis / radiolucent calculi Renal parenchymal defect / Papillary necrosis Crystalluria / Leukocyturia / Microhematuria / Mild proteinuria Acute renal failure / Chronic renal failure Hypertension Discontinuation in 33% of patients Histological findings Tubulointerstitial nephritis with indinavir crystals in tubules
26 Recommendations of the HIV Medicine Association of the Infectious Diseases Society of America Patients receiving indinavir should drink at least 1.5 L of water daily to prevent stone formation. Periodic monitoring of renal function and pyuria should be performed during the first 6 months of indinavir therapy and biannually thereafter, although routine screening for crystalluria is not warranted unless there is a suspicion of nephrolithiasis. Indinavir need not be withheld from patients with reduced renal function. In patients who develop indinavir nephrolithiasis, it would be reasonable to restart indinavir therapy once rehydration is achieved. Patients who develop indinavir-induced hypertension, pyuria, rhabdomyolysis, or renal insufficiency (acute or chronic) should permanently discontinue use of this drug. Gupta SK et al. Clin Infect Dis 2005 Jun 1;40(11):
27 Renal toxicity of antiproteases Atazanavir (Reyataz ) Indinavir (Crixivan ) Interstitial nephritis, urolithiasis Cristalluria, renal colic, AKI and CKD Nelfinavir (Viracept ) Ritonavir (Norvir ) Urolithiasis, renal colic AKI Daugas E et al., Kidney International, 2005 Izzedine H et al. AIDS, 2007
28 Nucleotide reverse transcriptase inhibitors: tenofovir Dose dependent nephrotoxicity Exacerbated by advanced HIV disease, reduced GFR, no dosage adaptation to reduced GFR concurrent ritonavir or ddi, other nephrotoxic 5 to 12 months after starting tenofovir
29 Tenofovir (Viread Truvada ) Proximal and distal tubular cells dysfunction Total or partial Fanconi s syndrome Earlier manifestations: Glucosuria and hypophosphatemia Nephrogenic diabetes insipidus Acute renal failure One case including nephritic syndrome Discontinuation Total or (rarely) partial reversibility several months after discontinuation Verhelst et al Am J Kidney Dis 2002

30 Rare in patient without prior kidney disease Gallant JE et al; JAMA Jul 14;292(2):


31
32 Recommendations of the HIV Medicine Association of the Infectious Diseases Society of America Patients receiving tenofovir who have a GFR <90 ml/min per 1.73 m2, patients receiving other medications eliminated via renal secretion (e.g., adefovir, acyclovir, ganciclovir, or cidofovir), patients with other comorbid diseases (e.g., diabetes or hypertension), or patients receiving ritonavir-boosted protease inhibitor regimens should be monitored at least biannually for measurements of renal function, serum phosphorus, and urine analysis for proteinuria and glycosuria. Dosage adaptation to reduced GFR. Gupta SK et al. Clin Infect Dis 2005 Jun 1;40(11):
33 Renal IRIS Differential diagnosis of HAART renal toxicity
34 Immune restoration inflammatory syndrome (IRIS) Patient with severe immune deficiency Silent spread of infectious agent HAART initiation Immune restoration Paradoxical inflammatory response
35 IRIS Up to 1/3 of patients coinfected with Mycobacterium tuberculosis, MAC or Cryptococcus neoformans Time between HAART and IRIS: #6-7 weeks Risk factors male gender long duration and deep immunodeficiency first introduction of HAART short delay between treatment of opportunistic infection and HAART marked increase of CD4 T cell count and reduction of HIV RNA level Shelburne SA et al ; AIDS, 2005;19:399
36 IRIS: infectious agents and clinical manifestations Wide spectrum of pathogens General manifestations Visceral manifestations (hepatitis, pneumonitis, encephalitis, lymphadenopathies, splenomegaly..) Life threatening in most severe cases Management: continuation of HAART and antiinfectious treatment, addition of antiinflammatory therapy: steroid therapy Hirsch HH et al, Clin Infect Dis 2004;38:1159-
37 References Jehle et al Daugas et al Daugas et al Izzedine et al Salliot et al Initial CD4-cell count (/mm 3 ) Initial RNA viral load (copies/ml) 1,247,786 56, ,850 <750, ,504 Infectious agent TB TB MAC TB TB Time from OI treatment to HAART (days) Time from HAART to IRIS (days) CD4-cell count (/mm 3 ) RNA viral load (copies/ml) < Creatinine level (µmol/l) Others IRIS-related symptoms Worsening of pulmonary infiltrate Fever, abdominal lymphadenopathie s, salpingitis, ascitis Fever, weight loss, severe cholestasis Erythematous skin lesions, lymphadenopathy, splenomegaly, cholestasis None Kidney biopsy Granulomatous interstitial nephritis Interstitial nephritis Liver biopsy: extensive granulomatous inflammation Granulomatous interstitial nephritis Granulomatous interstitial nephritis Steroid therapy (1 mg/kg/day) duration (months) NA 6 Outcome Healthy with normal renal f ti Healthy with normal renal f ti Healthy Healthy with normal renal f ti Healthy with normal renal f ti
38 Case report 51-year-old Chinese man No previous medical history Disseminated tuberculosis revealed HIV-1 CD4 cell 80/mm3 RNA viral load 177,504 copies/ml GFR 92 ml/min/ 1.73 m 2 (creatinine: 62 µmol/l)
39 Serum creatinine level (µmol/l) RNA viral load (copies/ml) Creatinine level (µmmol/l) CD4-cell count (/mm 3 ) Time Time (months) (months) Antituberculosis therapy HAART including tenofovir
40 Serum creatinine level (µmol/l) RNA viral load (copies/ml) Creatinine level (µmmol/l) CD4-cell count (/mm 3 ) Acute renal failure with tubulointerstitial nephropathy syndrome Time Time (months) (months) Antituberculosis therapy HAART including tenofovir
41 Serum creatinine level (µmol/l) RNA viral load (copies/ml) Creatinine level (µmmol/l) CD4-cell count (/mm 3 ) Acute renal failure with tubulointerstitial nephropathy syndrome Tenofovir toxicity? IRIS? Time Time (months) (months) Antituberculosis therapy HAART including tenofovir
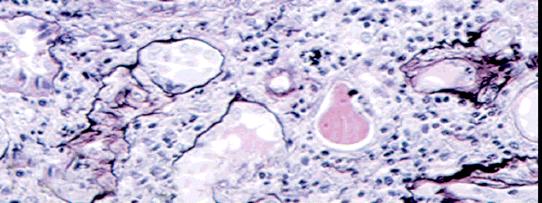
42 Serum creatinine level (µmol/l) RNA viral load (copies/ml) Creatinine level (µmmol/l) CD4-cell count (/mm 3 ) Acute renal failure with tubulointerstitial nephropathy syndrome Tenofovir toxicity? IRIS? Time Time (months) (months) Antituberculosis therapy HAART including tenofovir Renal biopsy

43 J Vérine, Hôpital Saint-Louis, Paris
44 Serum creatinine level (µmol/l) RNA viral load (copies/ml) Creatinine level (µmmol/l) CD4-cell count (/mm 3 ) Time (months) Antituberculosis therapy HAART including tenofovir
45 Serum creatinine level (µmol/l) RNA viral load (copies/ml) Creatinine level (µmmol/l) CD4-cell count (/mm 3 ) Time (months) Antituberculosis therapy HAART including tenofovir Prednisone
46 However HAART is beneficial
47 The Strategies for Management of Antiretroviral Therapy (SMART) trial 5472 patients, HIV, >350 CD4+/mm 3 Open randomized controlled trial Continuous HAART «viral suppression group» Episodic HAART if CD4<250/mm 3 until > 350/mm 3 «drug conservation group» SMART study group, NEJM, 2006
48 After a mean followup of 16 months SMART study group, NEJM, 2006
49 After 16 months (instead of 6 years) enrollment was stopped because of a safety risk in the drug conservation group SMART study group, NEJM, 2006
50 Conclusion
51 Main treatment strategy for CKD is HAART HAART at all stages including stage 5 HAART as early as possible
52 HIV: yet a more severe renal threat than diabetes in black patients in HAART era Choi et al, Kidney Int, 2007
53 Thank you
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER
: 30 YEARS LATER") HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. HIV and the Kidney. Leah Haseley, MD. Presentation prepared by: LH NW AETC ECHO June 2012
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
HIV and Renal Disease
 HIV and Renal Disease THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 8, 2012 Disclosure: No conflicts of interest Disclaimer: This presentation may contain information on off-label or investigational uses
HIV and Renal Disease THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 8, 2012 Disclosure: No conflicts of interest Disclaimer: This presentation may contain information on off-label or investigational uses
COMPETING INTEREST OF FINANCIAL VALUE
 BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
Kidney Disease in HIV. Kidney Disease in HIV: An Update for Ryan White Providers
 Kidney Disease in HIV: An Update for Ryan White Providers Christina M. Wyatt, MD Assistant Professor Mount Sinai School of Medicine New York, New York FORMATTED: 11/16/2015 Learning Objectives After attending
Kidney Disease in HIV: An Update for Ryan White Providers Christina M. Wyatt, MD Assistant Professor Mount Sinai School of Medicine New York, New York FORMATTED: 11/16/2015 Learning Objectives After attending
X H I V / A I D S J o h n s H o p k i n s / B r a z i l April 11-13, 2012 Sofitel Rio de Janeiro Copacabana, Brazil
 HIV and the Kidney Mohamed G. Atta, MD, MPH X H I V / A I D S J o h n s H o p k i n s / B r a z i l April 11-13, 2012 Sofitel Rio de Janeiro Copacabana, Brazil Objectives Multivariate hazard ratios for
HIV and the Kidney Mohamed G. Atta, MD, MPH X H I V / A I D S J o h n s H o p k i n s / B r a z i l April 11-13, 2012 Sofitel Rio de Janeiro Copacabana, Brazil Objectives Multivariate hazard ratios for
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Differences in Calculated Glomerular Filtration Rates (GFR) in Efavirenz (EFV) or Tenofovir (TDF)-treated Adults in ESS40006
 in Efavirenz (EFV) or Tenofovir (TDF)-treated Adults in ESS40006") 13th Conference on Retroviruses and Opportunistic Infections Denver, CO, USA. February 5-9, 2006 Poster Number 777 Differences in Calculated Glomerular Filtration Rates (GFR) in Efavirenz (EFV) or Tenofovir
13th Conference on Retroviruses and Opportunistic Infections Denver, CO, USA. February 5-9, 2006 Poster Number 777 Differences in Calculated Glomerular Filtration Rates (GFR) in Efavirenz (EFV) or Tenofovir
Incidence and etiology of acute renal failure among ambulatory HIV-infected patients
 Kidney International, Vol. 67 (2005), pp. 1526 1531 Incidence and etiology of acute renal failure among ambulatory HIV-infected patients NORA FRANCESCHINI, SONIA NAPRAVNIK, JOSEPH J. ERON, JR., LYNDA A.
Kidney International, Vol. 67 (2005), pp. 1526 1531 Incidence and etiology of acute renal failure among ambulatory HIV-infected patients NORA FRANCESCHINI, SONIA NAPRAVNIK, JOSEPH J. ERON, JR., LYNDA A.
TDF Renal Dysfunction
 TDF Renal Dysfunction Sarala Naicker MBChB, FRCP, PhD Division of Nephrology Dept of Internal Medicine University of the Witwatersrand Johannesburg South Africa SA HIV Clinician Society Conference Cape
TDF Renal Dysfunction Sarala Naicker MBChB, FRCP, PhD Division of Nephrology Dept of Internal Medicine University of the Witwatersrand Johannesburg South Africa SA HIV Clinician Society Conference Cape
Renal safety of tenofovir containing antiretroviral regimen in a Singapore cohort
 Chua et al. AIDS Research and Therapy 2012, 9:19 SHORT REPORT Open Access Renal safety of tenofovir containing antiretroviral regimen in a Singapore cohort Arlene C Chua 1*, Ryan M Llorin 1, Kelvin Lai
Chua et al. AIDS Research and Therapy 2012, 9:19 SHORT REPORT Open Access Renal safety of tenofovir containing antiretroviral regimen in a Singapore cohort Arlene C Chua 1*, Ryan M Llorin 1, Kelvin Lai
IDSA GUIDELINES EXECUTIVE SUMMARY
 IDSA GUIDELINES Guidelines for the Management of Chronic Kidney Disease in HIV-Infected Patients: Recommendations of the HIV Medicine Association of the Infectious Diseases Society of America Samir K.
IDSA GUIDELINES Guidelines for the Management of Chronic Kidney Disease in HIV-Infected Patients: Recommendations of the HIV Medicine Association of the Infectious Diseases Society of America Samir K.
Dr Michael Rayment Chelsea and Westminster Hospital, London
 17 TH ANNUAL CONFERENCE OF THE BRITISH HIV ASSOCIATION (BHIVA) Dr Michael Rayment Chelsea and Westminster Hospital, London 6-8 April 2011, Bournemouth International Centre A decade of renal biopsies in
17 TH ANNUAL CONFERENCE OF THE BRITISH HIV ASSOCIATION (BHIVA) Dr Michael Rayment Chelsea and Westminster Hospital, London 6-8 April 2011, Bournemouth International Centre A decade of renal biopsies in
Descovy. (emtricitabine, tenofovir alafenamide) New Product Slideshow
 New Product Slideshow") Descovy (emtricitabine, tenofovir alafenamide) New Product Slideshow Introduction Brand name: Descovy Generic name: Emtricitabine, tenofovir alafenamide (TAF) Pharmacological class: Nucleoside analog reverse
Descovy (emtricitabine, tenofovir alafenamide) New Product Slideshow Introduction Brand name: Descovy Generic name: Emtricitabine, tenofovir alafenamide (TAF) Pharmacological class: Nucleoside analog reverse
Safety Profile of Viread and Truvada. Ian McGowan, MD PhD FRCP Cape Town MTN Regional Meeting September, 2008
 Safety Profile of Viread and Truvada Ian McGowan, MD PhD FRCP Cape Town MTN Regional Meeting September, 2008 Overview Safety assessment in drug development Physiology 101 Renal Bone Liver Safety profile
Safety Profile of Viread and Truvada Ian McGowan, MD PhD FRCP Cape Town MTN Regional Meeting September, 2008 Overview Safety assessment in drug development Physiology 101 Renal Bone Liver Safety profile
Antiretroviral Dosing in Renal Impairment
 Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
Protease Inhibitors (PIs) Atazanavir Reyataz hard capsules 300 mg once daily taken with ritonavir 100 mg once daily No dosage adjustment is needed for atazanavir in renal impairment Atazanavir use in haemodialysis
1950 CID 2009:49 (15 December) HIV/AIDS. Received 17 April 2009; accepted 31 July 2009; electronically published 13 November 2009.
 HIV/AIDS. Received 17 April 2009; accepted 31 July 2009; electronically published 13 November 2009.") HIV/AIDS BRIEF REPORT Long-Term Evolution and Determinants of Renal Function in HIV-Infected Patients Who Began Receiving Combination Antiretroviral Therapy in 1997 1999, ANRS CO8 APROCO-COPILOTE Catherine
HIV/AIDS BRIEF REPORT Long-Term Evolution and Determinants of Renal Function in HIV-Infected Patients Who Began Receiving Combination Antiretroviral Therapy in 1997 1999, ANRS CO8 APROCO-COPILOTE Catherine
IN PRACTICE Kidney Biopsy in HIV: Beyond HIV-Associated Nephropathy
 IN PRACTICE Kidney Biopsy in HIV: Beyond HIV-Associated Nephropathy 1 2 1 Derek M. Fine, MD, Mark A. Perazella, MD, Gregory M. Lucas, MD, PhD, and Mohamed G. Atta, MD, MPH 1 INDEX WORDS: Human immunodeficiency
IN PRACTICE Kidney Biopsy in HIV: Beyond HIV-Associated Nephropathy 1 2 1 Derek M. Fine, MD, Mark A. Perazella, MD, Gregory M. Lucas, MD, PhD, and Mohamed G. Atta, MD, MPH 1 INDEX WORDS: Human immunodeficiency
Year 2002 Paper two: Questions supplied by Jo 1
 Year 2002 Paper two: Questions supplied by Jo 1 Question 9 A 37 year old man with known human immunodeficiency virus (HIV) infection for 10 years presents with severe renal colic for which he has no prior
Year 2002 Paper two: Questions supplied by Jo 1 Question 9 A 37 year old man with known human immunodeficiency virus (HIV) infection for 10 years presents with severe renal colic for which he has no prior
Lithium toxicity. Dr Aude Servais Service de Néphrologie adulte Hôpital Necker, Paris
 Lithium toxicity Dr Aude Servais Service de Néphrologie adulte Hôpital Necker, Paris Lithium Use of lithium salts as salt substitutes but recall from the marketplace in 1949 Efficient in the treatment
Lithium toxicity Dr Aude Servais Service de Néphrologie adulte Hôpital Necker, Paris Lithium Use of lithium salts as salt substitutes but recall from the marketplace in 1949 Efficient in the treatment
Immune Reconstitution Inflammatory Syndrome. Dr. Lesego Mawela
 Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Immune Reconstitution Inflammatory Syndrome Dr. Lesego Mawela TOPICS FOR DISCUSSION IRIS Case Epidermiology Pathogenesis of IRIS Risk factors for IRIS Epidemiology of IRIS Health system burden of IRIS
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Renal Transporters- pathophysiology of drug - induced renal disorders. Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November
 Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Immune Reconstitution Inflammatory Syndrome - IRIS
 Immune Reconstitution Inflammatory Syndrome - IRIS Douglas G. Fish, MD Head, Division of HIV Medicine Albany Medical College Cali, Colombia March 25, 2010 I-Tech: Thank you International Training and
Immune Reconstitution Inflammatory Syndrome - IRIS Douglas G. Fish, MD Head, Division of HIV Medicine Albany Medical College Cali, Colombia March 25, 2010 I-Tech: Thank you International Training and
Fanconi-like syndrome and rhabdomyolysis in a person with HIV infection. on highly active antiretroviral treatment including tenofovir
 1 Letter to the Editor Fanconi-like syndrome and rhabdomyolysis in a person with HIV infection on highly active antiretroviral treatment including tenofovir The nucleotide analogue, tenofovir disoproxil
1 Letter to the Editor Fanconi-like syndrome and rhabdomyolysis in a person with HIV infection on highly active antiretroviral treatment including tenofovir The nucleotide analogue, tenofovir disoproxil
Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers
 Training Guide for Healthcare Providers") Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers About emtricitabine/tenofovir disoproxil fumarate for HIV-1 PrEP
Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) Training Guide for Healthcare Providers About emtricitabine/tenofovir disoproxil fumarate for HIV-1 PrEP
Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP)
") Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) For Healthcare Providers About Emtricitabine/Tenofovir Disoproxil
Important Safety Information About Emtricitabine/Tenofovir Disoproxil Fumarate 200 mg/300 mg for HIV-1 Pre-exposure Prophylaxis (PrEP) For Healthcare Providers About Emtricitabine/Tenofovir Disoproxil
CLINICAL PEARLS OF NEW HIV MEDICATIONS PHARMACIST OBJECTIVES TECHNICIAN OBJECTIVES. At the end of this presentation pharmacists will be able to:
 CLINICAL PEARLS OF NEW HIV MEDICATIONS Cindy Lou Zoellner, PharmD, BCPS Added Qualifications in Infectious Diseases Senior Clinical Pharmacy Specialist in HIV Parkland Health & Hospital System Volunteer
CLINICAL PEARLS OF NEW HIV MEDICATIONS Cindy Lou Zoellner, PharmD, BCPS Added Qualifications in Infectious Diseases Senior Clinical Pharmacy Specialist in HIV Parkland Health & Hospital System Volunteer
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Slide #1 Case Presentation: Kidney Disease
 Slide #1 Case Presentation: Kidney Disease Christina Wyatt, MD Mount Sinai, New York Slide #2 Disclosures Investigator-initiated research support Gilead Sciences Honoraria for internal education Bristol
Slide #1 Case Presentation: Kidney Disease Christina Wyatt, MD Mount Sinai, New York Slide #2 Disclosures Investigator-initiated research support Gilead Sciences Honoraria for internal education Bristol
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort
 Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Outcomes of HIV-positive. Patients with Renal Insufficiency. on treatment with HAART at. Charlotte Maxeke Johannesburg.
 Outcomes of HIV-positive Patients with Renal Insufficiency on treatment with HAART at Charlotte Maxeke Johannesburg Academic Hospital Sadaf Rahmanian MBBCH (Wits) FCP (SA) Student number 0002443A Date
Outcomes of HIV-positive Patients with Renal Insufficiency on treatment with HAART at Charlotte Maxeke Johannesburg Academic Hospital Sadaf Rahmanian MBBCH (Wits) FCP (SA) Student number 0002443A Date
Glomerular filtration rates in HIV-infected patients treated with and without tenofovir: a prospective, observational study
 Journal of Antimicrobial Chemotherapy Advance Access published December 17, 2008 Journal of Antimicrobial Chemotherapy doi:10.1093/jac/dkn499 Glomerular filtration rates in HIV-infected patients treated
Journal of Antimicrobial Chemotherapy Advance Access published December 17, 2008 Journal of Antimicrobial Chemotherapy doi:10.1093/jac/dkn499 Glomerular filtration rates in HIV-infected patients treated
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Important Safety Information About TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication. For Healthcare Providers
 Indication. For Healthcare Providers") Important Safety Information About TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication For Healthcare Providers About TRUVADA for a PrEP Indication INDICATION AND PRESCRIBING CONSIDERATIONS TRUVADA,
Important Safety Information About TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication For Healthcare Providers About TRUVADA for a PrEP Indication INDICATION AND PRESCRIBING CONSIDERATIONS TRUVADA,
TB Intensive Tyler, Texas December 2-4, Tuberculosis and HIV Co-Infection. Lisa Y. Armitige, MD, PhD. December 4, 2008.
 TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
A Study on Estimated Glomerular Filtration Rate As A Predictor of Renal Dysfunction Among Adult Hiv Patients on Highly Active Antiretroviral Therapy
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 10 Ver. IX (Oct. 2017), PP 28-34 www.iosrjournals.org A Study on Estimated Glomerular Filtration
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 10 Ver. IX (Oct. 2017), PP 28-34 www.iosrjournals.org A Study on Estimated Glomerular Filtration
Elements for a public summary
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology The human immunodeficiency virus type 1 (HIV-1) is the primary cause of the acquired immunodeficiency syndrome (AIDS), which is
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology The human immunodeficiency virus type 1 (HIV-1) is the primary cause of the acquired immunodeficiency syndrome (AIDS), which is
Didactic Series. HIV-Associated Renal Disease. Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 10/9/14
 Didactic Series HIV-Associated Renal Disease Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 10/9/14 ACCREDITATION STATEMENT: University of California, San Diego
Didactic Series HIV-Associated Renal Disease Christian B. Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic 10/9/14 ACCREDITATION STATEMENT: University of California, San Diego
HIV basics. Katya Calvo Medical Director of Antimicrobial Stewardship
 HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV 101: Overview of the Physiologic Impact of HIV and Its Diagnosis Part 2: Immunologic Impact of HIV and its Effects on the Body
 HIV 101: Overview of the Physiologic Impact of HIV and Its Diagnosis Part 2: Immunologic Impact of HIV and its Effects on the Body Melissa Badowski, PharmD, BCPS, AAHIVP Clinical Assistant Professor University
HIV 101: Overview of the Physiologic Impact of HIV and Its Diagnosis Part 2: Immunologic Impact of HIV and its Effects on the Body Melissa Badowski, PharmD, BCPS, AAHIVP Clinical Assistant Professor University
104 MMWR December 17, 2004
 104 MMWR December 17, 2004 TABLE 8. Substantial pharmacokinetic drug-drug interactions for drugs used in the treatment of opportunistic Drugs Interacting with Mechanism/effects Recommendations Acyclovir
104 MMWR December 17, 2004 TABLE 8. Substantial pharmacokinetic drug-drug interactions for drugs used in the treatment of opportunistic Drugs Interacting with Mechanism/effects Recommendations Acyclovir
Stribild, a Single Tablet Regimen for the Treatment of HIV Disease
 Comb Prod Ther (2013) 3:1 8 DOI 10.1007/s13556-013-0001-y REVIEW Stribild, a Single Tablet Regimen for the Treatment of HIV Disease Cynthia Brinson To view enhanced content go to www.combitherapy-open.com
Comb Prod Ther (2013) 3:1 8 DOI 10.1007/s13556-013-0001-y REVIEW Stribild, a Single Tablet Regimen for the Treatment of HIV Disease Cynthia Brinson To view enhanced content go to www.combitherapy-open.com
HIGHLIGHTS OF PRESCRIBING INFORMATION
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use VIREAD safely and effectively. See full prescribing information for VIREAD. VIREAD (tenofovir disoproxil
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use VIREAD safely and effectively. See full prescribing information for VIREAD. VIREAD (tenofovir disoproxil
Alterations of Renal and Urinary Tract Function
 Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
1. Disorders of glomerular filtration
 RENAL DISEASES 1. Disorders of glomerular filtration 2. Nephrotic syndrome 3. Disorders of tubular transport 4. Oliguria and polyuria 5. Nephrolithiasis 6. Disturbances of renal blood flow 7. Acute renal
RENAL DISEASES 1. Disorders of glomerular filtration 2. Nephrotic syndrome 3. Disorders of tubular transport 4. Oliguria and polyuria 5. Nephrolithiasis 6. Disturbances of renal blood flow 7. Acute renal
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
HIGHLIGHTS OF PRESCRIBING INFORMATION
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use VIREAD safely and effectively. See full prescribing information for VIREAD. VIREAD (tenofovir disoproxil
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use VIREAD safely and effectively. See full prescribing information for VIREAD. VIREAD (tenofovir disoproxil
Impact of Tenofovir on Renal Function in HIV-Infected, Antiretroviral-Naive Patients
 CLINICAL SCIENCE Impact of Tenofovir on Renal Function in HIV-Infected, Antiretroviral-Naive Patients Michael Horberg, MD,* Beth Tang, MA, William Towner, MD, Michael Silverberg, PhD,* Susan Bersoff-Matcha,
CLINICAL SCIENCE Impact of Tenofovir on Renal Function in HIV-Infected, Antiretroviral-Naive Patients Michael Horberg, MD,* Beth Tang, MA, William Towner, MD, Michael Silverberg, PhD,* Susan Bersoff-Matcha,
THE HIV LIFE CYCLE. Understanding How Antiretroviral Medications Work
 THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
THE HIV LIFE CYCLE Understanding How Antiretroviral Medications Work DEFINITIONS Host: The animal or cell that another organism lives in. In HIV human CD4 T-cells are the host for HIV. Nucleus: The core
TB/HIV Co-Infection. Tuberculosis and HIV
 TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
Elements for summary tables in the EPAR
 VI.1 Elements for summary tables in the EPAR VI.1.1 Summary table of Safety concerns The following risks are defined with the EU reference product: Table 2. Summary of safety concerns Important identified
VI.1 Elements for summary tables in the EPAR VI.1.1 Summary table of Safety concerns The following risks are defined with the EU reference product: Table 2. Summary of safety concerns Important identified
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
The impact of antiretroviral drugs on renal function
 The impact of antiretroviral drugs on renal function Professor Bruce Hendry Renal Medicine King s College London King s College Hospital NHS Foundation Trust 1 DISCLOSURES: BRUCE HENDRY I have received
The impact of antiretroviral drugs on renal function Professor Bruce Hendry Renal Medicine King s College London King s College Hospital NHS Foundation Trust 1 DISCLOSURES: BRUCE HENDRY I have received
Summary of the risk management plan (RMP) for Evotaz (atazanavir/cobicistat)
 for Evotaz (atazanavir/cobicistat)") EMA/391330/2015 Summary of the risk management plan (RMP) for Evotaz (atazanavir/cobicistat) This is a summary of the risk management plan (RMP) for Evotaz, which details the measures to be taken in order
EMA/391330/2015 Summary of the risk management plan (RMP) for Evotaz (atazanavir/cobicistat) This is a summary of the risk management plan (RMP) for Evotaz, which details the measures to be taken in order
Central Nervous System Immune Reconstitution Disease: Pathology
 Central Nervous System Immune Reconstitution Disease: Pathology F.Gray, H.Adle-Biassette, F.Héran, G. Pialoux, A.Moulignier, APHP Hôpital Lariboisière Université Paris VII Introduction of HAART, which
Central Nervous System Immune Reconstitution Disease: Pathology F.Gray, H.Adle-Biassette, F.Héran, G. Pialoux, A.Moulignier, APHP Hôpital Lariboisière Université Paris VII Introduction of HAART, which
POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta
 Anjali Gupta") POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta PIGN One of the oldest recognized renal diseases. Now less commonly seen in industrialized nations, but in the underprivileged world, the burden remains
POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta PIGN One of the oldest recognized renal diseases. Now less commonly seen in industrialized nations, but in the underprivileged world, the burden remains
AIDS at 30 Epidemiology and Clinical Epidemiology and Management MID 37
 AIDS at 30 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Adults and children
AIDS at 30 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Adults and children
TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication. Training Guide for Healthcare Providers
 Indication. Training Guide for Healthcare Providers") TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication Training Guide for Healthcare Providers About TRUVADA for a PrEP indication to reduce the risk of sexually acquired HIV-1 infection in high-risk
TRUVADA for a Pre-exposure Prophylaxis (PrEP) Indication Training Guide for Healthcare Providers About TRUVADA for a PrEP indication to reduce the risk of sexually acquired HIV-1 infection in high-risk
Changes in Renal Function Associated with Tenofovir Disoproxil Fumarate Treatment, Compared with Nucleoside Reverse-Transcriptase Inhibitor Treatment
 HIV/AIDS BRIEF REPORT Changes in Renal Function Associated with Tenofovir Disoproxil Fumarate Treatment, Compared with Nucleoside Reverse-Transcriptase Inhibitor Treatment Joel E. Gallant, Michelle A.
HIV/AIDS BRIEF REPORT Changes in Renal Function Associated with Tenofovir Disoproxil Fumarate Treatment, Compared with Nucleoside Reverse-Transcriptase Inhibitor Treatment Joel E. Gallant, Michelle A.
HIGHLIGHTS OF PRESCRIBING INFORMATION
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use VIREAD safely and effectively. See full prescribing information for VIREAD. VIREAD (tenofovir disoproxil
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use VIREAD safely and effectively. See full prescribing information for VIREAD. VIREAD (tenofovir disoproxil
PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN
 PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN Summary of Risk Management Plan for REZOLSTA This is a summary of the risk management plan (RMP) for REZOLSTA. The RMP details important risks of REZOLSTA,
PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN Summary of Risk Management Plan for REZOLSTA This is a summary of the risk management plan (RMP) for REZOLSTA. The RMP details important risks of REZOLSTA,
TDF .*.* -** mg, ++,* -** mg HAART TDF HAART CMV +, +* +, +, -* ,**/ 2. BAL,**/ 3 / Pneumocystis jiroveci PCR ST +, +* 2. Kaposi HIV + + X HIV-RNA +,.
 ,**3 The Japanese Society for AIDS Research The Journal of AIDS Research TDF, +,, -. + -. : ST TDF HAART + : /0 HAART ST TDF, -TC, EFV TDF ++ Creat. -. +. mg/dl, BUN 0- mg/dl HAART TDF Creat. /*/. mgdl
,**3 The Japanese Society for AIDS Research The Journal of AIDS Research TDF, +,, -. + -. : ST TDF HAART + : /0 HAART ST TDF, -TC, EFV TDF ++ Creat. -. +. mg/dl, BUN 0- mg/dl HAART TDF Creat. /*/. mgdl
HIV Related Kidney Disease in Jamaican Children
 HIV Related Kidney Disease in Jamaican Children Professor Russell Pierre Faculty of Medical Sciences The University of the West Indies, Mona, Jamaica 3rd Jamaican Paediatric Nephrology Conference 2018
HIV Related Kidney Disease in Jamaican Children Professor Russell Pierre Faculty of Medical Sciences The University of the West Indies, Mona, Jamaica 3rd Jamaican Paediatric Nephrology Conference 2018
Emtricitabine / Tenofovir disoproxil Stada 200 mg/245 mg film-coated tablets , Version 1.3 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN
 Emtricitabine / Tenofovir disoproxil Stada 200 mg/245 mg film-coated tablets 30.5.2016, Version 1.3 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN VI.2 Elements for a public summary Emtricitabine / Tenofovir
Emtricitabine / Tenofovir disoproxil Stada 200 mg/245 mg film-coated tablets 30.5.2016, Version 1.3 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN VI.2 Elements for a public summary Emtricitabine / Tenofovir
Recent developments in HIV and the kidney Frank A. Post a and Stephen G. Holt b
 Recent developments in HIV and the kidney Frank A. Post a and Stephen G. Holt b a Department of HIV/GU Medicine, King s College London, London and b Brighton and Sussex University Hospitals NHS Trust,
Recent developments in HIV and the kidney Frank A. Post a and Stephen G. Holt b a Department of HIV/GU Medicine, King s College London, London and b Brighton and Sussex University Hospitals NHS Trust,
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Lecture 7. The Urinary System
 Lecture 7 The Urinary System Copyright 2006 Thomson Delmar Learning The Urinary System The urinary system removes wastes from the body The urinary system also maintains homeostasis or a constant internal
Lecture 7 The Urinary System Copyright 2006 Thomson Delmar Learning The Urinary System The urinary system removes wastes from the body The urinary system also maintains homeostasis or a constant internal
The Annotated Bibliography of the UCSF HIV Solid Organ Transplantation Project. ARV Dosing in End Stage Renal Disease
 The Annotated Bibliography of the UCSF HIV Solid Organ Transplantation Project ARV Dosing in End Stage Renal Disease 1. Jayasekara, D., Aweeka, F. T., Rodriguez, R., Kalayjian, R. C., Humphreys, M. H.,
The Annotated Bibliography of the UCSF HIV Solid Organ Transplantation Project ARV Dosing in End Stage Renal Disease 1. Jayasekara, D., Aweeka, F. T., Rodriguez, R., Kalayjian, R. C., Humphreys, M. H.,
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
EU-Risk Management Plan for Emtricitabine/Tenofovir (NL/H/3635/001/DC and NL/H/3636/001/DC) V1.3
 V1.3") VI.2 Elements for a public summary 200 mg/245 mg film-coated tablets VI.2.1 Overview of disease epidemiology HIV-1 infection In this decade, the global prevalence of HIV-1 infection stabilized
VI.2 Elements for a public summary 200 mg/245 mg film-coated tablets VI.2.1 Overview of disease epidemiology HIV-1 infection In this decade, the global prevalence of HIV-1 infection stabilized
Supplementary Data. Supplementary Table S2. Antiretroviral Therapies Taken with Ledipasvir/Sofosbuvir
 Supplementary Data Statistical Analysis Due to the limited number of patients with acute kidney injury and concern for model overfitting, covariates included in multivariable logistic regression analyses
Supplementary Data Statistical Analysis Due to the limited number of patients with acute kidney injury and concern for model overfitting, covariates included in multivariable logistic regression analyses
Changing spectrum of renal disease in HIV
 Available online at www.ijmrhs.com ISSN No: 239-5886 International Journal of Medical Research & Health Sciences, 206, 5, 2:3-35 Changing spectrum of renal disease in HIV R. Sunil, R. Sandeep 2, V. Mahesh
Available online at www.ijmrhs.com ISSN No: 239-5886 International Journal of Medical Research & Health Sciences, 206, 5, 2:3-35 Changing spectrum of renal disease in HIV R. Sunil, R. Sandeep 2, V. Mahesh
Darunavir STADA 400, 600 and 800 mg film-coated tablets , Version 1.1 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN
 Darunavir STADA 400, 600 and 800 mg film-coated tablets 7.9.2016, Version 1.1 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Human
Darunavir STADA 400, 600 and 800 mg film-coated tablets 7.9.2016, Version 1.1 PUBLIC SUMMARY OF THE RISK MANAGEMENT PLAN VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Human
Nothing to disclose.
 Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
Lisa G. Winston, MD University of California, San Francisco San Francisco General Hospital HIV UPDATE FOR THE PRIMARY CARE PROVIDER Nothing to disclose. 1 Outline Epidemiology Screening / testing for HIV
What we will cover. HIV in Case 1. HIV drugs frequently cause drug reactions. What is the most likely diagnosis
 HIV in 2009 Susan Hopkins Consultant in Infectious Diseases & Microbiology Royal Free Hampstead NHS Trust What we will cover Not Opportunistic Infections Important adverse events Important points to consider
HIV in 2009 Susan Hopkins Consultant in Infectious Diseases & Microbiology Royal Free Hampstead NHS Trust What we will cover Not Opportunistic Infections Important adverse events Important points to consider
Pathogenesis of IgA Nephropathy. Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS
 Pathogenesis of IgA Nephropathy Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS History Immunoglobin A nephropathy was first described by Berger and Hinglais in 1968 in Paris
Pathogenesis of IgA Nephropathy Shokoufeh Savaj MD Associate Professor of Medicine Firoozgar hospital- IUMS History Immunoglobin A nephropathy was first described by Berger and Hinglais in 1968 in Paris
Summary of treatment benefits
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Human immunodeficiency virus (HIV) attacks the cells of the immune system, the body's natural defense against germs and other
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Human immunodeficiency virus (HIV) attacks the cells of the immune system, the body's natural defense against germs and other
Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease
 Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease Assist Prof. Somnuek Sungkanuparph Division of Infectious Diseases Faculty of Medicine Ramathibodi Hospital Mahidol
Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease Assist Prof. Somnuek Sungkanuparph Division of Infectious Diseases Faculty of Medicine Ramathibodi Hospital Mahidol
Options for HBV treatments in case of TDF toxicity
 Options for HBV treatments in case of TDF toxicity Pr Corinne Isnard Bagnis Pitie Salpetriere Hospital corinne.bagnis@psl.aphp.fr Honorarium from Novartis BMS Gilead Abbvie GSK Roche Research funding BMS
Options for HBV treatments in case of TDF toxicity Pr Corinne Isnard Bagnis Pitie Salpetriere Hospital corinne.bagnis@psl.aphp.fr Honorarium from Novartis BMS Gilead Abbvie GSK Roche Research funding BMS
Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD
 Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J. Regional Chest Clinic New Jersey State TB Physician Advisory Board Cooper Univ. Hospital EIP Program TB and HIV
Approach to Co-infection with TB and HIV: 2011 Henry Fraimow, MD Consultant, Southern N.J. Regional Chest Clinic New Jersey State TB Physician Advisory Board Cooper Univ. Hospital EIP Program TB and HIV
0.14 ( 0.053%) UNAIDS 10% (94) ( ) (73-94/6 ) 8,920
 UNAIDS 10% (94) ( ) (73-94/6 ) 8,920") 0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
Tenofovir plasma exposures and Creatinine Clearance changes in 1st line Regimen of African patients in Cameroon and Senegal: ANRS12115 DAYANA study
 Abstract O_03 Tenofovir plasma exposures and Creatinine Clearance changes in 1st line Regimen of African patients in Cameroon and Senegal: ANRS12115 DAYANA study M.P. Lê Pharmacy Resident Clinical Pharmacology
Abstract O_03 Tenofovir plasma exposures and Creatinine Clearance changes in 1st line Regimen of African patients in Cameroon and Senegal: ANRS12115 DAYANA study M.P. Lê Pharmacy Resident Clinical Pharmacology
This is the author s version of a work that was submitted/accepted for publication in the following source:
 This is the author s version of a work that was submitted/accepted for publication in the following source: Kelly, Mark D., Gibson, Abby, Bartlett, Harry, Rowling, Diane, & Patten, John (2013) Tenofovir-associated
This is the author s version of a work that was submitted/accepted for publication in the following source: Kelly, Mark D., Gibson, Abby, Bartlett, Harry, Rowling, Diane, & Patten, John (2013) Tenofovir-associated
AIDS at 25. Epidemiology and Clinical Management MID 37
 AIDS at 25 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Regional HIV and
AIDS at 25 Epidemiology and Clinical Management Blood HIV Transmission transfusion injection drug use Sexual Intercourse heterosexual male to male Perinatal intrapartum breast feeding Regional HIV and
Tenofovir nephrotoxicity: acute tubular necrosis with distinctive clinical, pathological, and mitochondrial abnormalities
 http://www.kidney-international.org & 2010 International Society of Nephrology see commentary on page 1060 Tenofovir nephrotoxicity: acute tubular necrosis with distinctive clinical, pathological, and
http://www.kidney-international.org & 2010 International Society of Nephrology see commentary on page 1060 Tenofovir nephrotoxicity: acute tubular necrosis with distinctive clinical, pathological, and
NIH Public Access Author Manuscript Curr Infect Dis Rep. Author manuscript; available in PMC 2010 November 1.
 NIH Public Access Author Manuscript Published in final edited form as: Curr Infect Dis Rep. 2009 November ; 11(6): 479 485. HIV and the Kidney Leslie A. Bruggeman 1, Charles Bark 2, and Robert C. Kalayjian
NIH Public Access Author Manuscript Published in final edited form as: Curr Infect Dis Rep. 2009 November ; 11(6): 479 485. HIV and the Kidney Leslie A. Bruggeman 1, Charles Bark 2, and Robert C. Kalayjian
Renal safety of tenofovir in HIV-infected patients who switch from stavudine or zidovudine to tenofovir
 Original Article Vol. 29 No. 3 Renal safety of tenofovir:- Wiwattanathum P & Sungkanuparph S. 113 Renal safety of tenofovir in HIV-infected patients who switch from stavudine or zidovudine to tenofovir
Original Article Vol. 29 No. 3 Renal safety of tenofovir:- Wiwattanathum P & Sungkanuparph S. 113 Renal safety of tenofovir in HIV-infected patients who switch from stavudine or zidovudine to tenofovir
The ART of Antiretroviral Therapy in Critically-ill Patients with HIV
 The ART of Antiretroviral Therapy in Critically-ill Patients with HIV Tyler Finocchio, PharmD, BCPS PGY2 Critical Care Pharmacy Resident Avera McKennan Hospital & University Health Center February 10 th,
The ART of Antiretroviral Therapy in Critically-ill Patients with HIV Tyler Finocchio, PharmD, BCPS PGY2 Critical Care Pharmacy Resident Avera McKennan Hospital & University Health Center February 10 th,
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
When to start: guidelines comparison
 The editorial staff When to start: guidelines comparison The optimal time to begin antiretroviral therapy remains a critical question for the HIV field, and consensus about the appropriate CD4+ cell count
The editorial staff When to start: guidelines comparison The optimal time to begin antiretroviral therapy remains a critical question for the HIV field, and consensus about the appropriate CD4+ cell count
Supplemental Digital Content 1. Combination antiretroviral therapy regimens utilized in each study
 Supplemental Digital Content 1. Combination antiretroviral therapy regimens utilized in each study Study Almeida 2011 Auld 2011 Bassett 2012 Bastard 2012 Boulle 2008 (a) Boulle 2008 (b) Boulle 2010 Breen
Supplemental Digital Content 1. Combination antiretroviral therapy regimens utilized in each study Study Almeida 2011 Auld 2011 Bassett 2012 Bastard 2012 Boulle 2008 (a) Boulle 2008 (b) Boulle 2010 Breen
TDF containing ART: Efficacy and Safety. Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia
 TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
The Hospitalized HIV+ Patient
 The Hospitalized HIV+ Patient Danny Toub MD dannyt@srheathcenters.org October 8, 2012 Santa Rosa Family Medicine Residency List 3 ways of risk-stratifying known or suspected HIV+ inpatients Perform differential
The Hospitalized HIV+ Patient Danny Toub MD dannyt@srheathcenters.org October 8, 2012 Santa Rosa Family Medicine Residency List 3 ways of risk-stratifying known or suspected HIV+ inpatients Perform differential