Solid Organ Transplantation
|
|
|
- Edwin Pitts
- 6 years ago
- Views:
Transcription
1 Solid Organ Transplantation Ronald H. Kerman, PhD Professor of Surgery Director, Histocompatibility and Immune Evaluation Laboratory Division of Immunology & Organ Transplantation The University of Texas Medical School at Houston
2 Solid Organ Transplantation Blood Transfusions in 1600s Animal to humans: incompatible Again in the 1800s: incompatible Karl Landsteiner work begun in Led to description of ABO, M, N, Rh compatible/incompatible transfusions. Nobel Prize in Medicine
3 In the year 1491, Pope Innocent VIII, had an apoplectic stroke and fell into a kind of somnolence, which was sometimes so profound that the whole court believed him to be dead. All means to awaken the Pope s exhausted vitality were tried in vain. Finally, a physician proposed to use a new instrument to exchange the blood of a young person with that of the Pope. Hitherto this experiment had only been done on animals. Accordingly, the blood of the decrepit old pontiff was passed into the veins of a youth, whose blood was transferred into the veins of the old man. The experiment was tried three times at the cost of the lives of three boys (and 36 units of blood). The Pope also died and the physician quickly disappeared! -Vallari
4 Historical Efforts in Transplantation Chinese: Second century B.C. Cosmas and Damian: A.D. Casparo Tagliacozzi: A. Carrel, C. Guthrie: vascular anastomosis using a fine continuous suture technique, penetrating all vessel layers, resulted in tissue and organ transplants. For this vascular anastomosis procedure, Carrel won the Nobel Prize in Medicine, 1912.

5 Cosmas and Damian

6 Gasparo Tagliacozzi
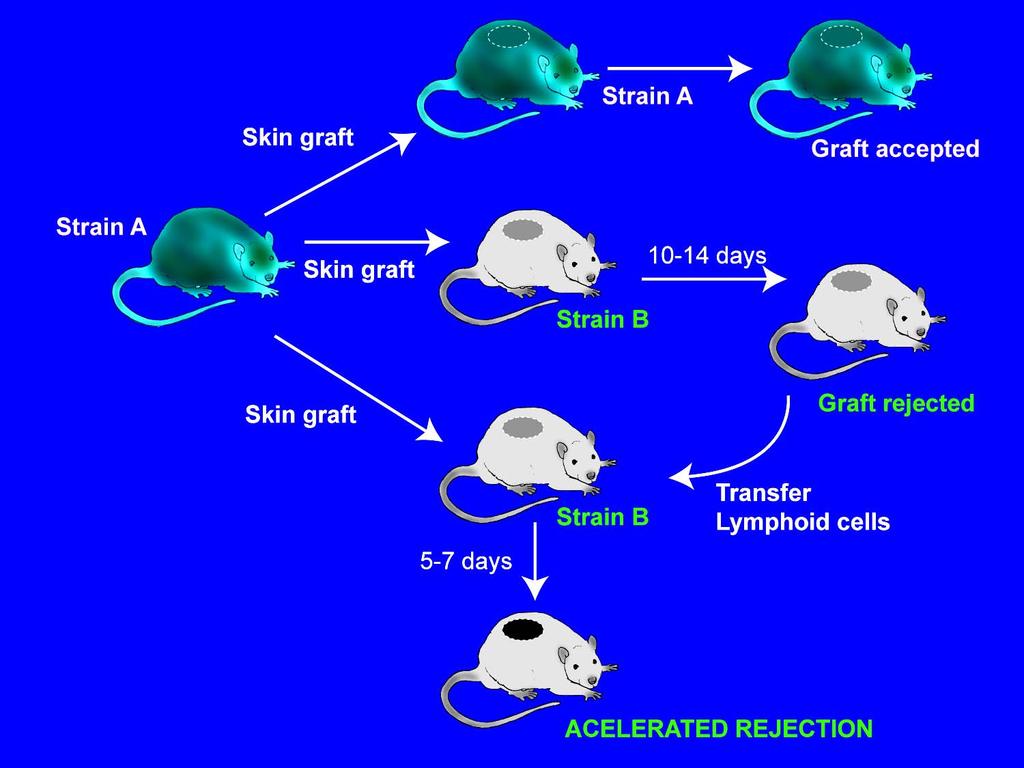
7 Solid Organ Transplantation Arguments Re: Cellular vs. Humoral Immunity Ray Owen: Dizygotic twin cattle sharing same circulation in utero became red cell chimeras and were unable to respond immunologically to one another s antigens. Burnet: Neonatal antigen exposure may lead to antigen unresponsiveness (tolerance) whereas after this neonatal time period antigen exposure leads to immune response. Nobel Prize in Medicine, Holman (1924) demonstrated that a single donor s skin graft applied to a burn patient rejected more rapidly with the second application.
8 Historical Efforts in Transplantation First human kidney transplanted unsuccessfully in 1933 by Voronoy into the groin of a patient in the Ukraine. During WW II, Peter Medawar, a zoologist interested in skin grafting and Thomas Gibson, a plastic surgeon, demonstrated that a second set of skin grafts from a parent to a burned child was rejected more rapidly than the first set. Gibson concluded that allografts were of no immediate clinical use. For Medawar it was evidence that allograft rejection was a major, unexplained, immunological phenomenon.
9 12-08
10 Solid Organ Transplantation During World War II Medawar re-examined this second-set phenomenon and established that rejection of foreign skin grafts followed all the rules of immune specificity. Billingham, Brent and Medawar described neonatal tolerance in mice. Won Nobel Prize in Medicine, Peter Gorer: described genetically determined antigens present in host tissue elicited immune response and destruction (rejection). George Snell: inbred mice, tumors, immune response, MHC, histocompatibility antigens. This work led to human MHC, HLA A, B, C, DR, DQ, DP antigens. Benaceraff, Dausset and Snell Nobel Prize in Medicine, 1980.
11 Historical Efforts in Transplantation 1945 saw the development of dialysis machines Kolff in Holland and Alwell in Sweden. 1945, Hufnagel et al joined the vessel of a cadaveric kidney to the brachial vessels of a comatose workman suffering from acute renal failure from septicemia the patient recovered. December 23, 1954 saw the first succesful kidney transplant between monosygotic twins. This validated the surgical technique and that without rejection normal health could be restored. The surgeon, Joseph Murray, won the Nobel Prize in Medicine.
12
13 Transplant Considerations: ABO compatibility Matching for HLA Pre-sensitization
14 Histocompatibility Systems: 1) ABO Red blood cells 2) HLA White blood cells and most body cells Histo (tissue) Compatibility
15 Blood Transfusion Success Donor: Recipient: Yes A A No Yes No B AB O
16 Human MHC Gene Locus
17 Methodologies to Evaluate HLA Serologic typing: HLA B7 vs B51 2) HLA-DNA (PCR Typing) use of PCR methodology to increase nucleotide sequences and sequence-specific oligonucleotide probes (SSOP), to identify DNA-genomic subtypes
18 Sequence-specific Primer (PCR-SSP) The SSP utilizes DNA primers that are specific for individual or similar groups of Class II alleles. The primers are used with PCR to amplify relevant genomic DNA.
19 Sequence-specific Oligonucleotide Probes (PCR-SSOP) Uses locus-specific or group-specific primers to amplify the desired genomic DNA. This is followed by application of a labeled oligonucleotide probe that binds to an allele-specific sequence.
20 Phenotype A32, A33, B65 (W6), B-, CW5, DR1, DR17, All positive antigens by tissue typing Genotype (A32, B65 (W6), CW8, DR1) (A33, B-, CW5, DR17) Antigens on same chromosomes Haplotype A32, B65 (W6), CW8, DR1 Antigens on single chromosome
21 Possible Haplotype Distributions Father Mother (A2, B8, DR1) (A23, B44, DR3) (A1, B51, DR4) (A3, B7, DR5) HLA identical siblings (A2, B8, DR1) (A1, B51, DR4) (A2, B8, DR1) (A1, B51, DR4) Haplo-identical siblings (A2, B8, DR1) (A1, B51, DR4) (A2, B8, DR1) (A3, B7, DR5) Totally mismatched siblings (A2, B8, DR1) (A1, B51, DR4) (A23, B44, DR3) (A3, B7, DR5)
22 % Graft Survival
23 Significance of HLA-A, -B and -DR Typing for AZA+Pred-treated Cadaveric Renal Transplant Recipients Patient HLA mismatches <2A, B, 0-1 DR <2A, B, 2 DR >2A, B, 0-1 DR >2A, B, 2 DR One-year Graft Survival 73% (29/40) 44% (7/16) 54% (21/39) 38% (6/16) P - < <0.05
24 Effect of HLA-B or -DR-mismatches
25 One-year Graft Survival for HLA-identical Sibling, Parental and Cadaveric Donor Transplants

26 Effect of HLA-A B and DR Mismatching on Graft Survival
27 Donor-recipient HLA incompatibility can result in an immune response, rejection and possible graft loss. Immunosuppressants may obviate the impact of HLA-matching for both short and long-term graft outcome.
28 Key Terms: Autograft: a graft or transplant from one area to another on the same individual. Isograft: a graft or cells from one individual to another who is syngeneic (genetically identical) to the donor. Allograft: graft or transplant from one individual to an MHC-disparate individual of the same species. Xenograft: graft between a donor and a recipient from different species.
29 Types of solid organ transplants: Kidney Liver Heart Lung Pancreas Intestine Deceased donors (D-D): formerly cadaveric donors (CAD) Living donors: Living related donors (LRD) Living unrelated donors (LURD)
30 Transplant Considerations ABO compatibility Matching for HLA Pre-sensitization
31 Allograft Rejection Type: Hyperacute Accelerated Acute Chronic Time: 0-48 hrs 5-7 days Early/delayed >60 days Immune Non-immune Mediated by: Abs Abs/cells Cells/Abs Abs/cells Trauma
32 HLA Ab Sensitization Pregnancy Blood transfusions Failed allograft Some types of bacterial infections
33 HLA Antigen Expression in the Kidney Vasculature Glomerulus Tubules Interstitium Arteries Cap. Endo Mesan Epi Prox Dist. Dendritic Class I /+ 0/ Class II /
34 Why Pre-transplant Crossmatches are Performed Crossmatch: Positive Rejection 24 No Rejection 6 Negative P = 8.18 x Patel & Terasaki, NEJM; 280:735, 1969
35 Detection of Antibody to Donor (HLA) Antigens Antibody screen Crossmatch
36 Serum Screening Screen sera for reactivity vs target cells by cytotoxicity/fluorescence readouts. Since a patient s Ab response could fluctuate, serum evaluations must be done at several time points. Use the most informative sera when performing the recipient vs donor crossmatch (historically most reactive, current and pretransplant sera).
37 Variation in Lymphocytotoxic Abs
38 PRA Panel Reactive Antibody Percent Reactive Antibody
39 Serum Screening Procedure
40 Panel-reactive Antibody (PRA) Peak : (Historical past) 90 : Current (Recent) 40
41 Determination of % PRA NIH-CDC AHG-CDC Flow cytometry Membrane-dependent Assays
42 Complement-dependent Cytotoxicity NIH Assay
 Assay")
43 Anti-human Globulin (Enhancement) Assay

44 Flow Cytometry Assay NIH - CDC Negative AHG CDC Negative Now measuring binding of IgG (absent C )
45 Abs by Different Methodologies Type: CDC AHG-CDC Flow Positive Negative
46 The Cell Surface Is a Jungle HLA
47 The Cell Surface Is a Jungle HLA Non-HLA Non-HLA
48 Membrane-dependent Assays NIH-CDC AHG-CDC Flow cytometry Detection of membrane receptors may not be related to HLA!
49 Membrane-independent Assays ELISA-determined IgG HLA Abs vs MHC-I (pooled platelets) ELISA-determined IgG HLA Abs vs MHC-I/II (PBL cultures) Flow bead PRA-determined IgG HLA vs I/II (soluble HLA I/II antigens on microbeads measured by cytometry)
50 Flow PRA I and Flow PRA II
51 Correlation of Pre-transplant Abs Detected by Flow PRA with Biopsy-documented Cardiac Rejection Tambur et al, Transplantation; 70:1055, 2000
52 Crossmatch Recipient serum + Donor cells = RXN
53 The purpose of the crossmatch is to detect clinically relevant IgG anti-donor antibodies to prevent hyperacute, accelerated or chronic rejection.
54 Detection of Donor-Reactive Antibodies NIH-CDC AHG-CDC Flow cytometry
55 Cadaveric Renal Allograft Survival Among 1 o CsA-Pred Recipients at 12 months NIH AHG Neg. Neg. Pos. n=166 81% (134/166) n=151 n=15 82% 67% (124/151) (10/15) P<0.01 Kerman et al, Transplantation; 51:316, 1991
56 Cadaveric Renal Allograft Survival Among 1 o CsA-Pred Recipients at 12 months AHG Pos. Neg. DTE-AHG Pos. n=15 67% (10/15) n=12 n=3 83% 0% (10/12) (0/3) P<0.01 Kerman et al, Transplantation; 51:316, 1991
57 Neg-NIH Extended XM: FCXM Study T-FCXM T-FCXM Pos. Neg. n=148 75% n=693 82% P<0.01 Ogura et al, Transplantation; 56:294, 1993
58 Now we can identify HLA Abs. Also we can identify the HLA Ab specificity that is anti-hla 1 or HLA B5. Therefore, we can drop the term PRA and refer to the specific HLA Ab specificity in patient sera and it s strength.
59 Immunosuppressive Drugs to Prevent Allograft Rejection At the present time there is no clinical protocol to induce tolerance to allografts. Therefore, all patients require daily treatment (for a life-time) with immunosuppressive agents to inhibit rejection. All the immunosuppressive agents used in clinical practice have drawbacks relating either to toxicity and side effects or to the failure to provide sufficient immunosuppression. On one hand, excessive immunosuppression can lead to development of opportunistic infections and neoplasia. On the other hand, inadequate immunosuppression allows the recipient to mount the immune response, causing allograft rejection.
60 Immunosuppressives: Azathioprine (Imuran ) Steroids Cyclosporine (Neoral) Tacrolimus (Prograf ) Sirolimus (Rapamune ) Mycophenolate mofetil (Cellcept) Anti-lymphocyte preparations: Thymoglobulin (anti-t, B, NK, etc.) Anti-CD3 (OKT3 ), anti-cd20 (Rituximab) Anti-CD54 (Campath)
61 Azathioprine (AZA): AZA (Burroughs-Wellcome, NC) is an S-imidazole derivative of 6-mercaptopurine which inhibits de novo DNA synthesis. Although AZA inhibits the primary immune responses, it has little effect upon the secondary responses. AZA was the first immunosuppressive drug successfully used in organ transplantation. Today AZA is only used clinically in combination with other immunosuppressive drugs. Corticosteroids: Corticosteroids are used in patients treated with AZA, CsA or TAC as a mandatory addition to produce an effective immunosuppression in transplant patients. Corticosteroids used in clinical transplantation allow physicians to lower the doses of other immunosuppressive drugs.
62 Cyclosporine (CsA): CsA (Sandimmune; Novartis Pharmaceuticals; Switzerland) a cyclic polypeptide produced by Tolypocladium inflatum fungi is very effective immunosuppressant for preventing allograft rejection. CsA has a selective (but reversible) inhibitory effect on T helper lymphocytes by blocking the production of IL-2, IFN-γ, IL-4 and other cytokines. In particular, in the cytoplasm CsA binds to immunophilin (CyPA) and CsA-CyPA complex blocks the function of enzyme calcineurin (CaN). In effect, CaN fails to dephosphorylate the cytoplasmic compound of the nuclear factor of activated T cell (NF-ATc), thereby preventing IL-2 (or other cytokine) gene transcription.
63 Tacrolimus (TAC- FK506): TAC (Fujisawa Pharmaceuticals, Japan), a macrolide, is produced by Streptomyces tsukubaensis. TAC forms a complex with FK binding protein (FK-BP), and the TAC/FK-BP complex blocks calcinuerin function preventing IL-2 (and other cytokine) gene transcription. Tacrolimus is presently used for kidney, heart, liver, lungs and pancreas transplantation.
64 Sirolimus (SRL): SRL (Rapamycin; Wyeth-Ayerst, Princeton, NJ) is a macrolide antibiotic produced by Streptomvces hygroscopicus. SRL molecule binds to the FK-BP and to the mammalian target of rapamycin (mtor). In contrast to CsA and FK506, SRL does not block cytokine production but instead inhibits cytokine signal transduction. for example IL-2 cytokine/il-2 receptor. Interestingly, SRL is particularly effective when used in combination with CsA or TAC by producing a potent synergistic immunosuppressive interaction. At present, the SRL/TAC as well as SRL/TAC combinations are used in clinical therapy.
65 Biological Products Used for Immunosuppression: In addition to drugs, polyclonal sera are prepared by immunization of animals with human lymphocytes to produce anti-lymphocyte serum (ALS). ALS is used to treat the incidence of rejection or as induction therapy shortly after transplantation (Thymoglobulin). Furthermore, murine monoclonal antibodies (MAb) directed to CD3 molecules (Orthoclone, OKT3) are licensed for use in clinical organ transplantation. The OKT3 MAb reacts with one of the CD3 molecules expressed on T cells and blocks their function. Treatment with OKT3 MAb inhibits allograft rejection, by lowering the number of circulating T lymphocytes. However, both these antibodies may induce potent immune responses, thereby limiting the duration of treatments.
66 To Transplant or Not to Transplant? HLA Ab (-); FCXM (-) Tx HLA Ab (+); FCXM (-) Tx (? ) HLA Ab (-); FCXM (+)? HLA Ab (+); FCXM (+) high-risk for rejection and graft loss
Transplantation. Immunology Unit College of Medicine King Saud University
 Transplantation Immunology Unit College of Medicine King Saud University Objectives To understand the diversity among human leukocyte antigens (HLA) or major histocompatibility complex (MHC) To know the
Transplantation Immunology Unit College of Medicine King Saud University Objectives To understand the diversity among human leukocyte antigens (HLA) or major histocompatibility complex (MHC) To know the
Desensitization in Kidney Transplant. James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver
 Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Dr. Yi-chi M. Kong August 8, 2001 Benjamini. Ch. 19, Pgs Page 1 of 10 TRANSPLANTATION
 Benjamini. Ch. 19, Pgs 379-399 Page 1 of 10 TRANSPLANTATION I. KINDS OF GRAFTS II. RELATIONSHIPS BETWEEN DONOR AND RECIPIENT Benjamini. Ch. 19, Pgs 379-399 Page 2 of 10 II.GRAFT REJECTION IS IMMUNOLOGIC
Benjamini. Ch. 19, Pgs 379-399 Page 1 of 10 TRANSPLANTATION I. KINDS OF GRAFTS II. RELATIONSHIPS BETWEEN DONOR AND RECIPIENT Benjamini. Ch. 19, Pgs 379-399 Page 2 of 10 II.GRAFT REJECTION IS IMMUNOLOGIC
Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation
 AACC Professional Course BETH ISRAEL DEACONESS MEDICAL CENTER HARVARD MEDICAL SCHOOL Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation J. Ryan
AACC Professional Course BETH ISRAEL DEACONESS MEDICAL CENTER HARVARD MEDICAL SCHOOL Transplant Applications of Solid phase Immunoassays Anti HLA antibody testing in solid organ transplantation J. Ryan
FIT Board Review Corner March 2016
 FIT Board Review Corner March 2016 Welcome to the FIT Board Review Corner, prepared by Sarah Spriet, DO, and Tammy Peng, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
FIT Board Review Corner March 2016 Welcome to the FIT Board Review Corner, prepared by Sarah Spriet, DO, and Tammy Peng, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
TRANSPLANT IMMUNOLOGY. Shiv Pillai Ragon Institute of MGH, MIT and Harvard
 TRANSPLANT IMMUNOLOGY Shiv Pillai Ragon Institute of MGH, MIT and Harvard Outline MHC / HLA Direct vs indirect allorecognition Alloreactive cells: where do they come from? Rejection and Immunosuppression
TRANSPLANT IMMUNOLOGY Shiv Pillai Ragon Institute of MGH, MIT and Harvard Outline MHC / HLA Direct vs indirect allorecognition Alloreactive cells: where do they come from? Rejection and Immunosuppression
10/18/2012. A primer in HLA: The who, what, how and why. What?
 A primer in HLA: The who, what, how and why What? 1 First recognized in mice during 1930 s and 1940 s. Mouse (murine) experiments with tumors Independent observations were made in humans with leukoagglutinating
A primer in HLA: The who, what, how and why What? 1 First recognized in mice during 1930 s and 1940 s. Mouse (murine) experiments with tumors Independent observations were made in humans with leukoagglutinating
Tolerance Induction in Transplantation
 Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Virtual Crossmatch in Kidney Transplantation
 Virtual Crossmatch in Kidney Transplantation Shiva Samavat Associate Professor of Nephrology Labbafinejad Hospital SBMU 2018.11.21 All transplant candidates are screened to determine the degree of humoral
Virtual Crossmatch in Kidney Transplantation Shiva Samavat Associate Professor of Nephrology Labbafinejad Hospital SBMU 2018.11.21 All transplant candidates are screened to determine the degree of humoral
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Basel - 6 September J.-M. Tiercy National Reference Laboratory for Histocompatibility (LNRH) University Hospital Geneva
 University Hospital Geneva") Basel - 6 eptember 2012 J.-M. Tiercy National Reference Laboratory for Histocompatibility (LNRH) University Hospital Geneva Outline the HLA system is (a) complex anti-hla immunisation and alloreactivity
Basel - 6 eptember 2012 J.-M. Tiercy National Reference Laboratory for Histocompatibility (LNRH) University Hospital Geneva Outline the HLA system is (a) complex anti-hla immunisation and alloreactivity
Robert B. Colvin, M.D. Department of Pathology Massachusetts General Hospital Harvard Medical School
 Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Robert B. Colvin Transplantation: Friendly organs in a hostile environment Robert B. Colvin,
Harvard-MIT Division of Health Sciences and Technology HST.035: Principle and Practice of Human Pathology Dr. Robert B. Colvin Transplantation: Friendly organs in a hostile environment Robert B. Colvin,
- Transplantation: removing an organ from donor and gives it to a recipient. - Graft: transplanted organ.
 Immunology Lecture num. (21) Transplantation - Transplantation: removing an organ from donor and gives it to a recipient. - Graft: transplanted organ. Types of Graft (4 types): Auto Graft - From a person
Immunology Lecture num. (21) Transplantation - Transplantation: removing an organ from donor and gives it to a recipient. - Graft: transplanted organ. Types of Graft (4 types): Auto Graft - From a person
1. Discuss the basic pathophysiology of end-stage liver and kidney failure.
 TRANSPLANT SURGERY ROTATION (PGY1, 2) A. Medical Knowledge Goal: The resident will achieve a detailed knowledge of the evaluation and treatment of a variety of disease processes. The resident will be exposed
TRANSPLANT SURGERY ROTATION (PGY1, 2) A. Medical Knowledge Goal: The resident will achieve a detailed knowledge of the evaluation and treatment of a variety of disease processes. The resident will be exposed
Transplant Overview. Timothy J. Schroeder President and CEO CTI Clinical Trial and Consulting Services November 10, 2005
 Transplant Overview Timothy J. Schroeder President and CEO CTI Clinical Trial and Consulting Services November 10, 2005 CTI Clinical Trial and Consulting Services Drug Development Company focused in key
Transplant Overview Timothy J. Schroeder President and CEO CTI Clinical Trial and Consulting Services November 10, 2005 CTI Clinical Trial and Consulting Services Drug Development Company focused in key
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials
 The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation
 Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation Stephen J Tomlanovich MD Objectives of this Talk Define the sensitized patient Describe the scope of the problem for a
Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation Stephen J Tomlanovich MD Objectives of this Talk Define the sensitized patient Describe the scope of the problem for a
Autoimmunity & Transplantation. Dr. Aws Alshamsan Department of Pharmaceu5cs Office: AA87 Tel:
 Autoimmunity & Transplantation Dr. Aws Alshamsan Department of Pharmaceu5cs Office: AA87 Tel: 4677363 aalshamsan@ksu.edu.sa Learning Objectives By the end of this lecture you will be able to: 1 Recognize
Autoimmunity & Transplantation Dr. Aws Alshamsan Department of Pharmaceu5cs Office: AA87 Tel: 4677363 aalshamsan@ksu.edu.sa Learning Objectives By the end of this lecture you will be able to: 1 Recognize
IMMUNOBIOLOGY OF TRANSPLANTATION. Wasim Dar
 IMMUNOBIOLOGY OF TRANSPLANTATION Wasim Dar Immunobiology of Transplantation Overview Transplantation: A complex immunologic process Contributions Innate Immunity Adaptive immunity T Cells B Cells HLA Consequences
IMMUNOBIOLOGY OF TRANSPLANTATION Wasim Dar Immunobiology of Transplantation Overview Transplantation: A complex immunologic process Contributions Innate Immunity Adaptive immunity T Cells B Cells HLA Consequences
Immunology. Anas Abu-Humaidan M.D. Ph.D. Transplant immunology+ Secondary immune deficiency
 Immunology Anas Abu-Humaidan M.D. Ph.D. Transplant immunology+ Secondary immune deficiency Transplant Immunology Transplantation is the process of moving cells, tissues or organs from one site to another
Immunology Anas Abu-Humaidan M.D. Ph.D. Transplant immunology+ Secondary immune deficiency Transplant Immunology Transplantation is the process of moving cells, tissues or organs from one site to another
Transplantation in Australia and New Zealand
 Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Intruduction PSI MODE OF ACTION AND PHARMACOKINETICS
 Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
The Lecture s topics
 The Lecture s topics Blood groups -ABO system *Transfusion reaction -Rhesus factor *Hemolytic disease of newborn Blood transfusion and Tissue transplant The ABO System Discovered in 1901 by Dr. Karl Landsteiner
The Lecture s topics Blood groups -ABO system *Transfusion reaction -Rhesus factor *Hemolytic disease of newborn Blood transfusion and Tissue transplant The ABO System Discovered in 1901 by Dr. Karl Landsteiner
Immunosuppressants. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
This study is currently recruiting participants.
 A Two Part, Phase 1/2, Safety, PK and PD Study of TOL101, an Anti-TCR Monoclonal Antibody for Prophylaxis of Acute Organ Rejection in Patients Receiving Renal Transplantation This study is currently recruiting
A Two Part, Phase 1/2, Safety, PK and PD Study of TOL101, an Anti-TCR Monoclonal Antibody for Prophylaxis of Acute Organ Rejection in Patients Receiving Renal Transplantation This study is currently recruiting
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
IMMUNOGENETICS AND TRANSPLANTATION
 IMMUNOGENETICS AND TRANSPLANTATION WHAT S THE MHC GOT TO DO WITH TRANSPLANTATION? We have learned that the molecules of Class I and II MHC are involved in presenting antigenic peptides to the receptors
IMMUNOGENETICS AND TRANSPLANTATION WHAT S THE MHC GOT TO DO WITH TRANSPLANTATION? We have learned that the molecules of Class I and II MHC are involved in presenting antigenic peptides to the receptors
The Human Major Histocompatibility Complex
 The Human Major Histocompatibility Complex 1 Location and Organization of the HLA Complex on Chromosome 6 NEJM 343(10):702-9 2 Inheritance of the HLA Complex Haplotype Inheritance (Family Study) 3 Structure
The Human Major Histocompatibility Complex 1 Location and Organization of the HLA Complex on Chromosome 6 NEJM 343(10):702-9 2 Inheritance of the HLA Complex Haplotype Inheritance (Family Study) 3 Structure
The MHC and Transplantation Brendan Clark. Transplant Immunology, St James s University Hospital, Leeds, UK
 The MHC and Transplantation Brendan Clark Transplant Immunology, St James s University Hospital, Leeds, UK Blood Groups Immunofluorescent staining has revealed blood group substance in the cell membranes
The MHC and Transplantation Brendan Clark Transplant Immunology, St James s University Hospital, Leeds, UK Blood Groups Immunofluorescent staining has revealed blood group substance in the cell membranes
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
Strategies for Desensitization
 Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
IMMUNOGENETICS AND INTRODUCTION TO TRANSPLANTATION
 IMMUNOGENETICS AND INTRODUCTION TO TRANSPLANTATION WHAT S THE MHC GOT TO DO WITH TRANSPLANTATION? We have learned that Class I and II MHC are involved in presenting antigenic peptides to the receptors
IMMUNOGENETICS AND INTRODUCTION TO TRANSPLANTATION WHAT S THE MHC GOT TO DO WITH TRANSPLANTATION? We have learned that Class I and II MHC are involved in presenting antigenic peptides to the receptors
Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation. Doctoral Thesis. Dr. Petra Gombos
 Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation Doctoral Thesis Dr. Petra Gombos Semmelweis University Doctoral School of Pathology Supervisor: Dr. Róbert Langer, Ph.D. Consultant:
Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation Doctoral Thesis Dr. Petra Gombos Semmelweis University Doctoral School of Pathology Supervisor: Dr. Róbert Langer, Ph.D. Consultant:
Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant
 SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS
 APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
6/19/2012. Who is in the room today? What is your level of understanding of Donor Antigens and Candidate Unacceptables in KPD?
 6/19/212 KPD Webinar Series: Part 3 Demystifying the OPTN Kidney Paired Donation Pilot Program Unacceptable HLA antigens: The key to finding a compatible donor for your patient M. Sue Leffell, Ph.D. J.
6/19/212 KPD Webinar Series: Part 3 Demystifying the OPTN Kidney Paired Donation Pilot Program Unacceptable HLA antigens: The key to finding a compatible donor for your patient M. Sue Leffell, Ph.D. J.
Histocompatibility antigens
 Histocompatibility antigens Tuesday 09 November 2010 Telegraph UK Livers grown in the laboratory could eventually solve organ transplant shortage. Made-to-measure organs for transplantation are a step
Histocompatibility antigens Tuesday 09 November 2010 Telegraph UK Livers grown in the laboratory could eventually solve organ transplant shortage. Made-to-measure organs for transplantation are a step
XIV. HLA AND TRANSPLANTATION MEDICINE
 XIV. HLA AND TRANSPLANTATION MEDICINE A. Introduction 1. The HLA system includes a complex array of genes and their molecular products that are involved in immune regulation and cellular differentiation.
XIV. HLA AND TRANSPLANTATION MEDICINE A. Introduction 1. The HLA system includes a complex array of genes and their molecular products that are involved in immune regulation and cellular differentiation.
Histocompatibility Evaluations for HSCT at JHMI. M. Sue Leffell, PhD. Professor of Medicine Laboratory Director
 Histocompatibility Evaluations for HSCT at JHMI M. Sue Leffell, PhD Professor of Medicine Laboratory Director JHMI Patient Population Adults Peds NMDP data >20,000 HSCT JHMI HSCT Protocols Bone marrow
Histocompatibility Evaluations for HSCT at JHMI M. Sue Leffell, PhD Professor of Medicine Laboratory Director JHMI Patient Population Adults Peds NMDP data >20,000 HSCT JHMI HSCT Protocols Bone marrow
Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT. 4th April 2014
 Solid Organ Transplantation How the Lab Contributes to Improved Patient Outcomes Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT 4th April 2014 Solid Organ Transplantation
Solid Organ Transplantation How the Lab Contributes to Improved Patient Outcomes Mary Keogan, on Mary behalf Keogan of all in NHISSOT On behalf of all in NHISSOT 4th April 2014 Solid Organ Transplantation
Significance of the MHC
 CHAPTER 7 Major Histocompatibility Complex (MHC) What is is MHC? HLA H-2 Minor histocompatibility antigens Peter Gorer & George Sneell (1940) Significance of the MHC role in immune response role in organ
CHAPTER 7 Major Histocompatibility Complex (MHC) What is is MHC? HLA H-2 Minor histocompatibility antigens Peter Gorer & George Sneell (1940) Significance of the MHC role in immune response role in organ
Transplantation Immunology
 Transplantation Immunology Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation Children s Hospital New York Presbyterian
Transplantation Immunology Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation Children s Hospital New York Presbyterian
Transplantation Immunology
 Transplantation Immunology MHC Restricted Allograft Rejection Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation
Transplantation Immunology MHC Restricted Allograft Rejection Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation
Completing the CIBMTR Confirmation of HLA Typing Form (Form 2005)
") Completing the CIBMTR Confirmation of HLA Typing Form (Form 2005) Stephen Spellman Research Manager NMDP Scientific Services Maria Brown Scientific Services Specialist Data Management Conference 2007 1
Completing the CIBMTR Confirmation of HLA Typing Form (Form 2005) Stephen Spellman Research Manager NMDP Scientific Services Maria Brown Scientific Services Specialist Data Management Conference 2007 1
HLA and more. Ilias I.N. Doxiadis. Geneva 03/04/2012.
 www.ebmt.org HLA and more Ilias I.N. Doxiadis Geneva 03/04/2012 HLA and more HLA and more / Doxiadis 2 Topic of the day Compatibility testing is a type of testing used to ensure compatibility of the system/application/website
www.ebmt.org HLA and more Ilias I.N. Doxiadis Geneva 03/04/2012 HLA and more HLA and more / Doxiadis 2 Topic of the day Compatibility testing is a type of testing used to ensure compatibility of the system/application/website
Innovation In Transplantation:
 Innovation In Transplantation: Improving outcomes Thomas C. Pearson Department of Surgery Emory Transplant Center CHOA Symposium October 22, 2016 Disclosures Belatacept preclinical and clinical trial were
Innovation In Transplantation: Improving outcomes Thomas C. Pearson Department of Surgery Emory Transplant Center CHOA Symposium October 22, 2016 Disclosures Belatacept preclinical and clinical trial were
Immunity. Acquired immunity differs from innate immunity in specificity & memory from 1 st exposure
 Immunity (1) Non specific (innate) immunity (2) Specific (acquired) immunity Characters: (1) Non specific: does not need special recognition of the foreign cell. (2) Innate: does not need previous exposure.
Immunity (1) Non specific (innate) immunity (2) Specific (acquired) immunity Characters: (1) Non specific: does not need special recognition of the foreign cell. (2) Innate: does not need previous exposure.
Controversies in Renal Transplantation. The Controversial Questions. Patrick M. Klem, PharmD, BCPS University of Colorado Hospital
 Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
The role of HLA in Allogeneic Hematopoietic Stem Cell Transplantation and Platelet Refractoriness.
 The role of HLA in Allogeneic Hematopoietic Stem Cell Transplantation and Platelet Refractoriness. Robert Liwski, MD, PhD, FRCPC Medical Director HLA Typing Laboratory Department of Pathology Dalhousie
The role of HLA in Allogeneic Hematopoietic Stem Cell Transplantation and Platelet Refractoriness. Robert Liwski, MD, PhD, FRCPC Medical Director HLA Typing Laboratory Department of Pathology Dalhousie
Post Transplant Immunosuppression: Consideration for Primary Care. Sameh Abul-Ezz, M.D., Dr.P.H.
 Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
The Acceptable Mismatch program of Eurotransplant.
 The Acceptable Mismatch program of Eurotransplant. Frans Claas Leiden University Medical Center Eurotransplant Reference Laboratory Leiden, the Netherlands. Hinterzarten, December 7, 2013 Main problem
The Acceptable Mismatch program of Eurotransplant. Frans Claas Leiden University Medical Center Eurotransplant Reference Laboratory Leiden, the Netherlands. Hinterzarten, December 7, 2013 Main problem
Solid Organ Transplantation 1. Chapter 55. Solid Organ Transplant, Self-Assessment Questions
 Solid Organ Transplantation 1 Chapter 55. Solid Organ Transplant, Self-Assessment Questions Questions 1 to 9 are related to the following case: A 38-year-old white man is scheduled to receive a living-unrelated
Solid Organ Transplantation 1 Chapter 55. Solid Organ Transplant, Self-Assessment Questions Questions 1 to 9 are related to the following case: A 38-year-old white man is scheduled to receive a living-unrelated
What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham
 What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham SYMPHONY Study Ekberg et al. NEJM 2008 Excluded: DCD kidneys; CIT>30hours;
What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham SYMPHONY Study Ekberg et al. NEJM 2008 Excluded: DCD kidneys; CIT>30hours;
Immunosuppression: evolution in practice and trends,
 American Journal of Transplantation 25; 5 (Part 2): 874 886 Blackwell Munksgaard Blackwell Munksgaard 25 Immunosuppression: evolution in practice and trends, 1993 23 Ron Shapiro a,, James B. Young b, Edgar
American Journal of Transplantation 25; 5 (Part 2): 874 886 Blackwell Munksgaard Blackwell Munksgaard 25 Immunosuppression: evolution in practice and trends, 1993 23 Ron Shapiro a,, James B. Young b, Edgar
Liver Transplant Immunosuppression
 Liver Transplant Immunosuppression Michael Daily, MD, MS, FACS Surgical Director, Kidney and Pancreas Transplantation University of Kentucky Medical Center Disclosures No financial disclosures I will be
Liver Transplant Immunosuppression Michael Daily, MD, MS, FACS Surgical Director, Kidney and Pancreas Transplantation University of Kentucky Medical Center Disclosures No financial disclosures I will be
Glossary. Anesthesiologist A doctor who puts you or parts of your body to sleep during surgery.
 1-Glossary Glossary Acute rejection A type of rejection that occurs when immune cells from your body attack the transplanted organ(s). Acute rejection may occur at any time after a transplant. But it usually
1-Glossary Glossary Acute rejection A type of rejection that occurs when immune cells from your body attack the transplanted organ(s). Acute rejection may occur at any time after a transplant. But it usually
Renal Transplant. Tony Chacon. Program Head BCIT Nephrology Nursing Program.
 Renal Transplant Tony Chacon Program Head BCIT Nephrology Nursing Program Email: tony_chacon@bcit.ca Summary of CNA Renal Transplant Competencies Potential contraindications to renal transplant. Assessment/selection
Renal Transplant Tony Chacon Program Head BCIT Nephrology Nursing Program Email: tony_chacon@bcit.ca Summary of CNA Renal Transplant Competencies Potential contraindications to renal transplant. Assessment/selection
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant
 James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
ABO INCOMPATILIBITY AND TRANSPLANTATION
 ABO INCOMPATILIBITY AND TRANSPLANTATION Aleksandar Mijovic Consultant Haematologist/Senior Lecturer King s College Hospital/NHS Blood and Transplant London, UK RTC Edu Meeting May 2017 ABO antigens Expressed
ABO INCOMPATILIBITY AND TRANSPLANTATION Aleksandar Mijovic Consultant Haematologist/Senior Lecturer King s College Hospital/NHS Blood and Transplant London, UK RTC Edu Meeting May 2017 ABO antigens Expressed
Transfusion support in Transplantation
 Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Chapter 10. Histocompatibility Testing
 Chapter 10 Histocompatibility Testing Chapter 10 Histocompatibility Testing Table of Contents 10.1 General... 3 10.1.1 Registration of renal transplant patients...3 10.1.2 Material for histocompatibility
Chapter 10 Histocompatibility Testing Chapter 10 Histocompatibility Testing Table of Contents 10.1 General... 3 10.1.1 Registration of renal transplant patients...3 10.1.2 Material for histocompatibility
GUIDELINES ON RENAL TRANSPLANTATION
 46 GUIDELINES ON RENAL TRANSPLANTATION T. Kälbe (chairman), M. Lucan, G. Nicita, R. Sells, F.J. Burgos Revilla, M. Wiesel Introduction The number of patients registered as starting end-stage renal disease
46 GUIDELINES ON RENAL TRANSPLANTATION T. Kälbe (chairman), M. Lucan, G. Nicita, R. Sells, F.J. Burgos Revilla, M. Wiesel Introduction The number of patients registered as starting end-stage renal disease
Better than Google- Click on Immunosuppression Renal Transplant. David Landsberg Oct
 Better than Google- Click on Immunosuppression Renal Transplant David Landsberg Oct 3 2008 OUTLINE History of Immunosuppression Trends in Immunosupression FK vs CYA Steroid Minimization CNI Avoidance Sirolimus
Better than Google- Click on Immunosuppression Renal Transplant David Landsberg Oct 3 2008 OUTLINE History of Immunosuppression Trends in Immunosupression FK vs CYA Steroid Minimization CNI Avoidance Sirolimus
CHAPTER 10 BLOOD GROUPS: ABO AND Rh
 CHAPTER 10 BLOOD GROUPS: ABO AND Rh The success of human blood transfusions requires compatibility for the two major blood group antigen systems, namely ABO and Rh. The ABO system is defined by two red
CHAPTER 10 BLOOD GROUPS: ABO AND Rh The success of human blood transfusions requires compatibility for the two major blood group antigen systems, namely ABO and Rh. The ABO system is defined by two red
Increased Early Rejection Rate after Conversion from Tacrolimus in Kidney and Pancreas Transplantation
 Increased Early Rejection Rate after Conversion from Tacrolimus in Kidney and Pancreas Transplantation Gary W Barone 1, Beverley L Ketel 1, Sameh R Abul-Ezz 2, Meredith L Lightfoot 1 1 Department of Surgery
Increased Early Rejection Rate after Conversion from Tacrolimus in Kidney and Pancreas Transplantation Gary W Barone 1, Beverley L Ketel 1, Sameh R Abul-Ezz 2, Meredith L Lightfoot 1 1 Department of Surgery
Should red cells be matched for transfusions to patients listed for renal transplantation?
 Should red cells be matched for transfusions to patients listed for renal transplantation? Dr M.Willicombe Imperial College Renal and Transplant Centre, Hammersmith Hospital Should red cells be matched
Should red cells be matched for transfusions to patients listed for renal transplantation? Dr M.Willicombe Imperial College Renal and Transplant Centre, Hammersmith Hospital Should red cells be matched
Co-dominance. Dr.Shivani Gupta, Department of Zoology, PGGCG-11, Chandigarh
 Co-dominance Dr.Shivani Gupta, Department of Zoology, PGGCG-11, Chandigarh Blood groups and Rhesus factor History of Blood Groups and Blood Transfusions Experiments with blood transfusions have been carried
Co-dominance Dr.Shivani Gupta, Department of Zoology, PGGCG-11, Chandigarh Blood groups and Rhesus factor History of Blood Groups and Blood Transfusions Experiments with blood transfusions have been carried
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
SELECTED ABSTRACTS. All (n) % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%
 % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%") SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
Clinical impact of de-novo HLA antibodies in pancreas and islet transplantation
 Clinical impact of de-novo HLA antibodies in pancreas and islet transplantation David Turner, PhD, FRCPath Lead for H&I Services, Scottish National Blood Transfusion Service Treatment of Type I DM Insulin
Clinical impact of de-novo HLA antibodies in pancreas and islet transplantation David Turner, PhD, FRCPath Lead for H&I Services, Scottish National Blood Transfusion Service Treatment of Type I DM Insulin
Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly Sensitized Renal Transplanted Patients
 BioMed Research International Volume 2013, Article ID 738404, 5 pages http://dx.doi.org/10.1155/2013/738404 Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly
BioMed Research International Volume 2013, Article ID 738404, 5 pages http://dx.doi.org/10.1155/2013/738404 Clinical Study Different Impact of Pretransplant Anti-HLA Antibodies Detected by Luminex in Highly
2017 BANFF-SCT Joint Scientific Meeting. BARCELONA March 2017
 2017 BANFF-SCT Joint Scientific Meeting BARCELONA 27-31 March 2017 Adriana Zeevi PhD (D) ABHI Professor of Pathology, Surgery and Immunology Director of Histocompatibility Laboratory University of Pittsburgh
2017 BANFF-SCT Joint Scientific Meeting BARCELONA 27-31 March 2017 Adriana Zeevi PhD (D) ABHI Professor of Pathology, Surgery and Immunology Director of Histocompatibility Laboratory University of Pittsburgh
SEVENTH EDITION CHAPTER
 Judy Owen Jenni Punt Sharon Stranford Kuby Immunology SEVENTH EDITION CHAPTER 16 Tolerance, Autoimmunity, and Transplantation Copyright 2013 by W. H. Freeman and Company Immune tolerance: history * Some
Judy Owen Jenni Punt Sharon Stranford Kuby Immunology SEVENTH EDITION CHAPTER 16 Tolerance, Autoimmunity, and Transplantation Copyright 2013 by W. H. Freeman and Company Immune tolerance: history * Some
Steroid Minimization: Great Idea or Silly Move?
 Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
25/10/2017. Clinical Relevance of the HLA System in Blood Transfusion. Outline of talk. Major Histocompatibility Complex
 Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
Clinical Relevance of the HLA System in Blood Transfusion Dr Colin J Brown PhD FRCPath. October 2017 Outline of talk HLA genes, structure and function HLA and immune complications of transfusion TA-GVHD
Overview. Evaluation of Potential Kidney Transplant Recipients. Projected Years of Life in Patients with ESRD
 Evaluation of Potential Kidney Transplant Recipients Donald E. Hricik MD Professor of Medicine and Chief, Division of Nephrology and Hypertension University Hospitals Case Medical Center Conflict of Interest
Evaluation of Potential Kidney Transplant Recipients Donald E. Hricik MD Professor of Medicine and Chief, Division of Nephrology and Hypertension University Hospitals Case Medical Center Conflict of Interest
Chapter 19. Blood Types
 Chapter 19 Blood Types What is an antigen? Antigens are glycoprotein and glycolipid molecules which are part of the plasma membrane (i.e. part of the glycocalyx) These molecules maybe imbedded into the
Chapter 19 Blood Types What is an antigen? Antigens are glycoprotein and glycolipid molecules which are part of the plasma membrane (i.e. part of the glycocalyx) These molecules maybe imbedded into the
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham
 Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
IMMUNOSUPPRESSIVE THERAPY Overview. Desensitization
 IMMUNOSUPPRESSIVE THERAPY Overview Two types of immune responses to allografts: Cellular response: foreign antigen recognition activate antigen-specific lymphocytes (T-cells) o Key mediator: T-cells o
IMMUNOSUPPRESSIVE THERAPY Overview Two types of immune responses to allografts: Cellular response: foreign antigen recognition activate antigen-specific lymphocytes (T-cells) o Key mediator: T-cells o
Solid Organ Transplant
 Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
Management of platelet refractory patients, why does your patient keep on bleeding? Dr Colin Brown, H&I Dept, NHSBT Colindale
 Management of platelet refractory patients, why does your patient keep on bleeding? Dr Colin Brown, H&I Dept, NHSBT Colindale Pooled Platelets (Buffy Coat Derived) Adult dose from 4 ABO-identical donors
Management of platelet refractory patients, why does your patient keep on bleeding? Dr Colin Brown, H&I Dept, NHSBT Colindale Pooled Platelets (Buffy Coat Derived) Adult dose from 4 ABO-identical donors
Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation
 Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation Doctoral Dissertation Dr. Petra Gombos Semmelweis University Doctoral School of Pathology Supervisor: Consultant: Official
Evaluation of Two New Antibody Detection Techniques in Kidney Transplantation Doctoral Dissertation Dr. Petra Gombos Semmelweis University Doctoral School of Pathology Supervisor: Consultant: Official
23/10/2017. Panel Reactive Antibodies and Crossmatch by Flow Cytometry. Antibodies against. Renal transplantation. Antibody mediated rejection (AMR)
") Renal transplantation Panel Reactive Antibodies and Crossmatch by Flow Cytometry Katherina Psarra Immunology Histocompatibility Dept Evangelismos Hospital Athens, Greece In spite of the enormous progress
Renal transplantation Panel Reactive Antibodies and Crossmatch by Flow Cytometry Katherina Psarra Immunology Histocompatibility Dept Evangelismos Hospital Athens, Greece In spite of the enormous progress
A Tolerance Approach to the Transplantation of Vascularized Tissues
 A Tolerance Approach to the Transplantation of Vascularized Tissues The 9th New Jersey Symposium on Biomaterials Science and Regenerative Medicine October 29-31, 2008 David H. Sachs, M.D. Harvard Medical
A Tolerance Approach to the Transplantation of Vascularized Tissues The 9th New Jersey Symposium on Biomaterials Science and Regenerative Medicine October 29-31, 2008 David H. Sachs, M.D. Harvard Medical
Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017
 Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017 Dr AJ Terblanche Paediatric Gastroenterology and Hepatology Unit, SBAH Paediatric Transplant Unit Wits Donald Gordon Medical
Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017 Dr AJ Terblanche Paediatric Gastroenterology and Hepatology Unit, SBAH Paediatric Transplant Unit Wits Donald Gordon Medical
Nephrology Grand Rounds
 Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
NONSPECIFIC Starts in the blood by
 BASIC IMMUNOLOGY and ORGAN TRANSPLANTATION Ahmed Mahmoud,MD Host defense against infection is 1- nonspecific or 2- specific (immune system) NONSPECIFIC Starts in the blood by 1) leucocytes phagocytosis
BASIC IMMUNOLOGY and ORGAN TRANSPLANTATION Ahmed Mahmoud,MD Host defense against infection is 1- nonspecific or 2- specific (immune system) NONSPECIFIC Starts in the blood by 1) leucocytes phagocytosis
the HLA complex Hanna Mustaniemi,
 the HLA complex Hanna Mustaniemi, 28.11.2007 The Major Histocompatibility Complex Major histocompatibility complex (MHC) is a gene region found in nearly all vertebrates encodes proteins with important
the HLA complex Hanna Mustaniemi, 28.11.2007 The Major Histocompatibility Complex Major histocompatibility complex (MHC) is a gene region found in nearly all vertebrates encodes proteins with important
Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents
 BUMC Proceedings 1999;12:110-112 Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents CHERYLE GURK-TURNER, RPH Department of Pharmacy Services, BUMC wo mouse/human
BUMC Proceedings 1999;12:110-112 Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents CHERYLE GURK-TURNER, RPH Department of Pharmacy Services, BUMC wo mouse/human
Highly Sensitized Patient Registry: Update and Successes
 Highly Sensitized Patient Registry: Update and Successes Dr. Olwyn Johnston Medical Director Kidney and Pancreas Transplant Program Vancouver General Hospital Conflict of Interest Transplant Nephrologist
Highly Sensitized Patient Registry: Update and Successes Dr. Olwyn Johnston Medical Director Kidney and Pancreas Transplant Program Vancouver General Hospital Conflict of Interest Transplant Nephrologist
Significance of the MHC
 CHAPTER 8 Major Histocompatibility Complex (MHC) What is is MHC? HLA H-2 Minor histocompatibility antigens Peter Gorer & George Sneell (1940) Significance of the MHC role in immune response role in organ
CHAPTER 8 Major Histocompatibility Complex (MHC) What is is MHC? HLA H-2 Minor histocompatibility antigens Peter Gorer & George Sneell (1940) Significance of the MHC role in immune response role in organ
Renal Pathology- Transplantation. Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic
 Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Renal Pathology- Transplantation Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Kidney has a limited number of tissue reactions by which the kidney
Organ transplantation in Bulgaria
 Cell Tissue Banking (28) 9:337 342 DOI 1.17/s1561-7-935-2 Organ transplantation in Bulgaria Elissaveta Naumova Æ Petar Panchev Æ Pencho J. Simeonov Æ Anastassia Mihaylova Æ Kalina Penkova Æ Petia Boneva
Cell Tissue Banking (28) 9:337 342 DOI 1.17/s1561-7-935-2 Organ transplantation in Bulgaria Elissaveta Naumova Æ Petar Panchev Æ Pencho J. Simeonov Æ Anastassia Mihaylova Æ Kalina Penkova Æ Petia Boneva
Kidney Transplantation
 Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Transplantation Yesterday, Today and Tomorrow
 http://www.bioline.org.br/js 20 Rahima Dawood Traveling Fellow Lecture, Mombasa Kenya December 2007. Transplantation Yesterday, Today and Tomorrow Ali Bakran Consultant Transplant and Vascular Surgeon
http://www.bioline.org.br/js 20 Rahima Dawood Traveling Fellow Lecture, Mombasa Kenya December 2007. Transplantation Yesterday, Today and Tomorrow Ali Bakran Consultant Transplant and Vascular Surgeon