Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017
|
|
|
- Frank Short
- 6 years ago
- Views:
Transcription

1 Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017 Dr AJ Terblanche Paediatric Gastroenterology and Hepatology Unit, SBAH Paediatric Transplant Unit Wits Donald Gordon Medical Centre
2 DISCLOSURES No financial disclosures

3 Disclosure: Paediatric perspective





4 Disclosure: liver transplant experience Paediatric liver transplant immunosuppression (consent obtained for use of photos)

5 Experience local
6 Transplant Immunosuppression in 2017 Hepatobiliary Liver Transplant Symposium 2017 Dr AJ Terblanche Paediatric Gastroenterology and Hepatology Unit, SBAH Paediatric Transplant Unit Wits Donald Gordon Medical Centre
7
8
9
10 Solid organ transplantation Medical field most dramatic developments last decade with advances Surgical technique Graft preservation Critical care management

11 Solid organ transplantation Increased understanding of the immune response Improved immunosuppression management Improved outcomes and long-term survival
12 Goal transplant immunosuppression Prevent Allograft rejection Immune mediated graft injury By Altering / inhibit the normal host immune response to foreign antigen
13 Ideal transplant immunosuppression Create allograft-specific nonresponse Maintain immunocompetence against other potential pathogens and conditions

14 Ideal transplant immunosuppression Desired level of immunosuppression a balance Prevention acute rejection Excess immunosuppression increased risk infection malignancy drug-specific toxicities
15 Current strategies varies Different centers Organ transplant types Protocols Combination of drugs Organ-specific planned tapering of medication and doses over time Active surveillance emerging viral infections / other signs over-immunosuppression
16 Historical Perspective

17 Era of solid organ transplantation Early 20 th century xenotransplantation attempted World War I skin allografts were implemented to treat injured Theory immune mediated rejection developed


18 Peter Medawar Serial full-thickness skin allografts in cattle rejected more vigorously Grafts between monozygotic twins promptly thrived and tolerated ALLOGRAFT REJECTION IMMUNOLOGIC PHENOMENON WITH THE CLASSIC IMMUNE PROPERTIES SENSITIZATION MEMORY AND TOLERANCE CONCEPT PILLARS TRANSPLANTATION SCIENCE
19 1954 Kidney transplant 1960 s Liver, heart, pancreas transplants 1980 s Lung and intestinal transplants 1963 Paediatric liver transplant 1984 Paediatric heart transplant Success limited surgical technique and lack of adequate immunosuppression
20 1930 s Immunosuppression by total body irradiation 1970 s Steroids and Azathioprine Outcome dismal 15% one year survival liver transplant 1980 s Cyclosporin Transplantation clinical reality One year survival 80% 1990 s Surge availability new agents Tacrolimus Refinement protocols to prevent and treat long term rejection Variability different regimens centers Aim standardize care and achieve excellent graft and patient survival
21 Pharmacology of Immunosuppression
22 Paediatric perspective Significant developments immunosuppression management past 60 years Use new agents limited lack pharmacokinetic data Children as vulnerable population often excluded from studies of new regimens due to safety concerns
23 Important challenges medication Medications must be dispensed in liquid form Find compounding pharmacies Pertinent pay attention to exact medication concentrations, as compounded suspensions vary (1mg/ml vs 0.5 mg/ml) Remember volume rather than concentration
24 Important challenges medication Suspensions unpalatable, toddlers refuse to take Nasoenteric, percutaneous gastric tube placement Consistent administration, trough levels may change switch suspension / pill Interaction nutrition, medication, supplements significant Certain suspensions refrigerated Travel etc Suspensions shaken before administration
25 Important challenges medication Some medications may clog feeding tubes routine flushing Suspension more expensive than pill form often not covered medical aids add financial burden
26 Important challenges medication Young patients dependent caregiver administration All individuals involved educated Information not transmitted visits Parental anxiety and family instability risks errors Adverse drug reactions significant morbidity and mortality children Exponential risk multiple medications Pharmacodynamics / Pharmacokinetics Dedicated transplant pharmacist

27 Pharmacokinetics substantially different Metabolize drugs more rapidly - increased hepatic enzyme activity Changes in hepatic blood flow, which generally decrease with age, may affect drug extraction and clearance Differences body surface area Shortened bowel length, decreased area drug absorption Slower gastric emptying <6m Slower intestinal transit time <12y
28 Differences particularly important paediatric transplant recipient Tacrolimus dosages 2-5x higher to achieve same levels in adults Partial liver graft from adult donor: pharmacokinetic pattern of tacrolimus retains the characteristics of the age of the donor, not the recipient
29 Variations gastric ph alters absorption Gastric environment Neutral neonate Acid production adult levels 3y Co-administration antacids common Chelation coadministration Milk Antacids Iron supplements
30 Absorption further altered Co-administration prokinetic agents Variations cytochrome P450 enzyme activity Immaturity pancreatic and biliary function Intestinal microbiome Presence of food alter rate/extent of absorption Tacro/MMF empty stomach, GIT S/E with food consistent administration with / without food Challenge toddlers!

31 Water 70% body mass newborn Adult levels 55-60% around 1-2 years First few months Extracellular fluid intracellular fluid Affect drug distribution and lower plasma levels drug administered on weight basis Drug distribution
32 Pharmacodynamics Bone marrow suppression Nephrotoxicity Avoid nephrotoxic drugs, adjusted doses QTc prolongation ECG Bone disease Ca, Vit D levels, supplement GIT disturbances Separate administration times other drugs GIT effect Photosensitivity Tacro, Bactrim, voriconazole Skin protection and avoidance long direct sunlight exposure
33 Pharmacodynamics Neuropsychological deficits and lower cognitive function mild functional impairment 79% after LT Pre-existing deficits Prolonged exposure developing paediatric brain immunosuppression

34 N X Minor Major E I tremor encephalopathy U C R I headache seizures O T T Y insomnia polyneuropathy O parasthesia Speech disorder

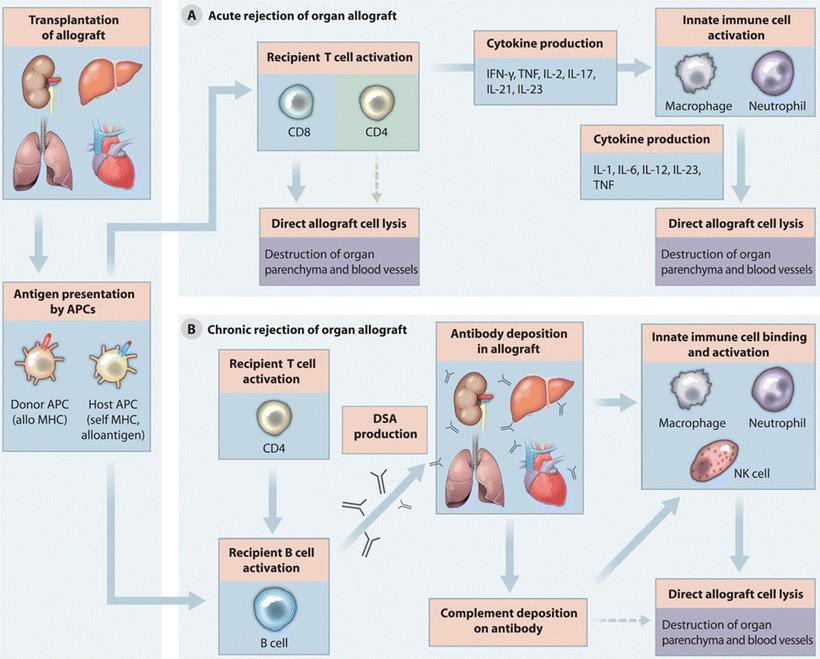
35 Host immune response: Graft foreign Destructive T-lymphocyte mediated immune response

36 Goal immunosuppression Inhibit the antigeninduced T-lymphocyte activation and cytokine production to interrupt allo-major histocompatibility complex recognition or to block effector responses
37 Accomplish while preserving immunocompetence to maintain adequate host response to infections
38 Immunosuppressive protocols Induction, maintenance, treatment of rejection Combination of medications Induction immunosuppression Used varying frequency different organs Given at time of transplant to rapidly create a state of immunologic unresponsiveness of the recipient to donor antigens
39 Induction immunosuppression
40
41 Acute rejection Still occurs in significant number of patients Studies of Pediatric Liver Transplantation (SPLIT) registry 1902 patients AR most often first 3 months (45%) 59% at 24 months Less rejection age < 6m and LRD grafts No evidence less rejection episodes better HLA compatibility liver transplant recipients same protocols Tacrolimus vs cyclosporin less rejection episodes at 6 months, final time of follow up no significance difference
42 Acute rejection treatment Short course high-dose steroids Bolus several days with rapid taper to baseline therapy successful 75-80% SPLIT registry: steroid resistant rejection 11% Uncommon Problematic to treat Poly- and monoclonal antibodies, increased risk infection and PTLD Refractory / recurrent rejection anti-lymphocytic therapy with poly/monoclonal antibody therapy can be successful Bilirubin >10mg/dl successful control resistant rejection unlikely Late acute rejection different prognosis associated low levels immunosuppression and non-adherance Response to steroids suboptimal Increased risk chronic rejection
43 Immunosuppressive agents

44 Induction agents Polyclonal antibodies Monoclonal antibodies Antithymocyte globulin Muronomab- CD3 Basiliximab Daclizumab Alemtuzumab
45 ATG (Thymoglobulin) Rabbit polyclonal antibody directed against human lymphocytes Potent modulator immune response 3 Hypotheses mechanism of action Classic complement mediated cell lysis CD2, CD3, CD4, CD8, CD11a, CD25, CD40, CD54 Uptake opsonized T cells by RES Modulation essential surface receptors on lymphocytes that remain in circulation but function is blocked Create profound lymphocyte depletion (actual or functional)
46 ATG (Thymoglobulin) Uses Induction agent at time of transplant Suppress host immune system Allow use CNI several days after transplant CNI side effects exacerbated hemodynamic changes around Tx minimized Steroid resistant rejection Steroid sparing protocols
47 Symptoms ATG administration Incidence and severity varied Related cytokine release IL1, IL6, TNF Cytokine storm Fever, chills, diarrhoea, serum sickness, seizures, anaphylaxis Dose dependent thrombocytopaenia and leucopenia CMV prophylaxis CVP chemical phlebitis
48 Muronomab CD3 (Orthoclone OKT-3) Liver transplantation Cytokine release syndrome CD3 pos T cells fall 60% to <5% 24-48h Voluntarily withdrawn decreased utilization Basiliximab (Simulect) and daclizumab (Zenepax) Humanized antibody IL-2 receptor Target proliferative T-cell response Prevent rejection pediatric Tx patients Do not trigger cytokine release syndrome, better tolerated Basiliximab induction reduced acute rejection rate after paediatric liver transplant Rate steroid refractive and chronic rejection remained the same Alemtuzumab target CD52 surface protein Most recent effective monoclonal Ab adult liver Tx Not widely implemented paediatric use
49 Maintenance of Immunosuppression
50 Corticosteroids First anti-rejection drugs used SOT Used varying degrees in most immunosuppressive regimens
51 Mechanism of action Suppress antibody production Suppress cytokine synthesis (IL-1,2,6, IFN-Υ) Bind glucocorticoid receptors in cytoplasm, translocate to the nucleus, decreased proliferation of T cells and B cells
52 Corticosteroids Compromise important role SOT: Effective prevention and treatment acute rejection Well-known adverse effects children SPLIT study 23% 10 year survivors liver transplant impaired linear growth Paediatric programs Steroid withdrawal Steroid minimization Steroid free immunosuppressive protocols
53 Corticosteroids

54 Other adverse effects Increased infection rates Osteoporosis Metabolic derangements Glucose intolerance Weight gain Psychiatric disturbances
55 Long term steroid therapy Avoided Current practice of steroid withdrawal variable 3 m, start weaning at 3m or at 12m Steroid-free immunosuppressive protocols adults promising Most benefit low risk rejection, high risk DM / HT Large multicenter trials children lacking Clearest contraindication weaning AIH

56 Calcineurin inhibitors (CNI) Cyclosporine and Tacrolimus Backbone immunosuppression past 4 decades Dramatically improved transplant survival 1980 s
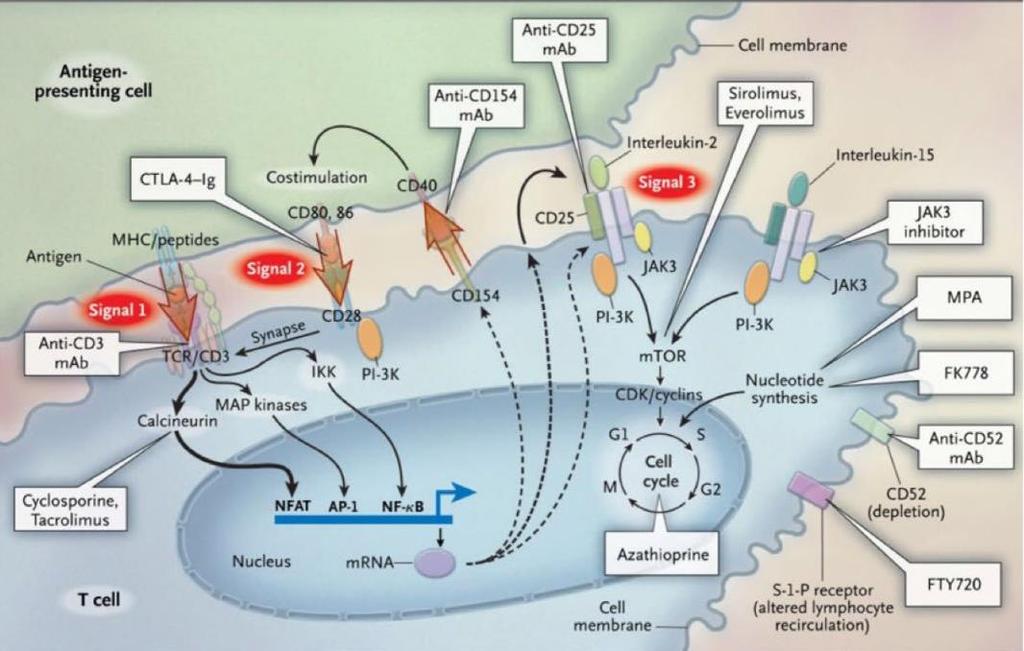
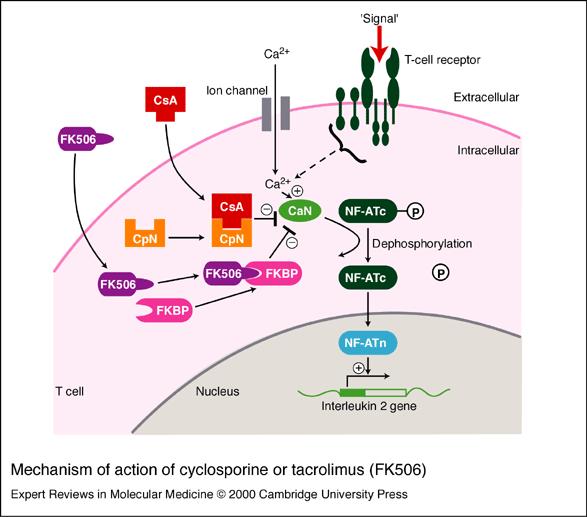
57 Mechanism of immunological action Complex with intracellular proteins Cyclosporin cyclophilin Tacrolimus tacrolimus binding protein FKBP12 Inhibit calcineurin enzyme to dephosphorylate nuclear regulatory elements Interfere with production and release IL-2 IL-2 required T-cell activation and proliferation Tacrolimus 100x more potent
58
59 Cyclosporine mainstay immunosuppression 1983 Tacrolimus following decade rescue therapy Equal controlled trials patient / graft survival Tacrolimus more effective preventing acute and steroid-resistant rejection
60 Benefits Tacrolimus primary immunosuppression Superior efficacy in preventing acute and steroid resistant rejection Freedom long-term steroid use Allow steroid withdrawal within 1y without adverse effects Single agent Cyclosporin in combination MMF / AZA
61 Tacrolimus primary immunosuppressive agent paediatric SOT
")
62 Both metabolized liver cytochrome P4503A(CYP3A) system
63 Differences metabolism Tacrolimus absorption, unlike cyclosporin, not dependent on bile more effective cholestasis, draining biliary tube should not affect levels Both bind to plastic (gastrostomy tubes, feeding tubes, plastic cutlery) influence levels Diarrhoea reduce cyclosporine levels, increase tacrolimus levels frequent levels to avoid toxicity
64 Side effects CNIs Nephrotoxicity Neurotoxicity Infection Gastrointestinal disturbances Tacrolimus: hyperglycemia, DM but lower incidence hyperkalemia, hypercholesterolaemia and hypertension Renal impairment most serious complication both limit use other nephrotoxic agents
65
66 Mycophenolate mofetil (MMF) Converted in liver to active metabolite mycophenolic acid (MPA) Selectively inhibits ionosine monophosphate dehydrogenase inhibits synthesis guanosine (purine nucleosides) T and B lymphocytes uniquely dependent on for proliferation Selectively inhibits T- and B-cell proliferation and thus antibody formation
67 MMF Pharmacokinetics does not vary with age Effectively reduce incidence rejection adults Incorporated in paediatric regimens as CNI sparing agent Co-agent Tacrolimus pre-existing renal impairment GIT side effects: cramping, vomiting, diarrhoea, pancytopaenia Start low dose and increase if no side effects
68 Sirolimus Macrolide antibiotic produced by Streptomyces species isolated Easter Island 1975 Originally anti-tumor agent Bind mtor receptor, intracellular regulator of protein kinases Inhibit IL-2 production and B and T cell activation and proliferation
69 Sirolimus Initially rescue therapy CNI failure Subsequently primary immunosuppression Associated poor wound healing and hepatic artery thrombosis liver transplant recipients recent studies no significant differences cohorts Not used first several months post transplant Anti-tumor proliferative activity role hepatic tumors
70 Sirolimus Extensively metabolized liver cytochrome P4503A system Extremely long half life 62h MULTIPLE DRUG INTERACTIONS toxicity Side effects reversible Bone marrow suppression Hyperlipidaemia Athralgia Oral ulcers Interstitial pneumonitis Diarrhoea
71 Everolimus Sirolimus derivative, mtor inhibitor Rescue therapy rejection and renal insufficiency paediatric kidney, heart, liver Tx Retrospective cohort 301 paediatric kidney transplant patients decreased 3y incidence CMV disease high risk donor + recipient pt: possible direct antiviral effects through mtor inhibition Paediatric heart transplant pt everolimus and MMF improvement GFR without increased rejection Safety trials needed paediatrics
72

73 Operational tolerance Acceptance of an allograft by a recipient in the absence of maintenance immunosuppression Long sought paediatric SOT decades immunosuppression Liver relatively immunologically permissive majority studies liver allograft recipients
74 < 18y age Parental LRD allograft >4y Stable allograft function 6m No features rejection / significant fibrosis on protocol liver biopsy

 off")
75 Gradual withdrawal 36w Frequent labs Protocol biopsies 4-8 w, 2y, 4y 12/20 (60%) off medications 1 year
76 Remained tolerant without increased graft fibrosis 5y off immunosuppression

77 Decreased hypertension, Increased GFR Similar incidence post transplant metabolic syndrome
78 Operational tolerance is possible Highly selected group of paediatric recipients Gradual withdrawal immunosuppression Ongoing studies Identification biomarkers to refine the process Immunophenotypes of circulating blood Peripheral blood signatures of tolerance Operational tolerance possibility beyond liver transplantation
79
80 Future directions Increasing awareness long-term effects of immunosuppression changes management New approaches induction, maintenance and rejection considered widely Paediatric late losses all related to immunosuppression Over treating: infection and malignancy Under treating: acute and chronic rejection
81 Future directions New induction therapies should strive to enough immunosuppression to control rejection and protect graft, without added risks of unnecessary immunosuppression like infection and toxicity Ultimate goal: induce donor-specific operational tolerance and allow eventual freedom from immunosuppression and long term toxicities
82 Disclosure: liver transplant experience Thank you
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Immunosuppressants. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Immunosuppressants Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Immunosuppressive Agents Very useful in minimizing the occurrence of exaggerated or inappropriate
Liver Transplant Immunosuppression
 Liver Transplant Immunosuppression Michael Daily, MD, MS, FACS Surgical Director, Kidney and Pancreas Transplantation University of Kentucky Medical Center Disclosures No financial disclosures I will be
Liver Transplant Immunosuppression Michael Daily, MD, MS, FACS Surgical Director, Kidney and Pancreas Transplantation University of Kentucky Medical Center Disclosures No financial disclosures I will be
Controversies in Renal Transplantation. The Controversial Questions. Patrick M. Klem, PharmD, BCPS University of Colorado Hospital
 Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
Controversies in Renal Transplantation Patrick M. Klem, PharmD, BCPS University of Colorado Hospital The Controversial Questions Are newer immunosuppressants improving patient outcomes? Are corticosteroids
9/30/ DISCLOSURES. + First: Why immunosuppress? Transplant Immunosuppression and Prophylaxis
 Transplant Immunosuppression and Prophylaxis Sarah Fitz, APN, MSN, ACNP-BC Loyola University Medical Center DISCLOSURES I am not being paid by any entity to endorse a specific product. Any mention of brand
Transplant Immunosuppression and Prophylaxis Sarah Fitz, APN, MSN, ACNP-BC Loyola University Medical Center DISCLOSURES I am not being paid by any entity to endorse a specific product. Any mention of brand
European Risk Management Plan. Measures impairment. Retreatment after Discontinuation
 European Risk Management Plan Table 6.1.4-1: Safety Concern 55024.1 Summary of Risk Minimization Measures Routine Risk Minimization Measures Additional Risk Minimization Measures impairment. Retreatment
European Risk Management Plan Table 6.1.4-1: Safety Concern 55024.1 Summary of Risk Minimization Measures Routine Risk Minimization Measures Additional Risk Minimization Measures impairment. Retreatment
Literature Review: Transplantation July 2010-June 2011
 Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
Literature Review: Transplantation July 2010-June 2011 James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Kidney Transplant Top 10 List: July Kidney
Tolerance Induction in Transplantation
 Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Tolerance Induction in Transplantation Reza F. Saidi, MD, FACS, FICS Assistant Professor of Surgery Division of Organ Transplantation Department of Surgery University of Massachusetts Medical School Percent
Intruduction PSI MODE OF ACTION AND PHARMACOKINETICS
 Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
Multidisciplinary Insights on Clinical Guidance for the Use of Proliferation Signal Inhibitors in Heart Transplantation Andreas Zuckermann, MD et al. Department of Cardio-Thoracic Surgery, Medical University
OBJECTIVES. Phases of Transplantation and Immunosuppression
 Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Transplant and Immunosuppression: Texas Transplant Center April 29, 2017 Regina L. Ramirez, Pharm.D., BCPS PGY1 Pharmacy Residency Program Director Clinical Practice Specialist Solid Organ Transplant and
Aljoša Kandus Renal Transplant Center, Department of Nephrology, University Medical Center Ljubljana, Slovenia
 Aljoša Kandus Renal Transplant Center, Department of Nephrology, University Medical Center Ljubljana, Slovenia Immunosuppression in kidney transplantation Aljoša Kandus Renal Transplant Center, Department
Aljoša Kandus Renal Transplant Center, Department of Nephrology, University Medical Center Ljubljana, Slovenia Immunosuppression in kidney transplantation Aljoša Kandus Renal Transplant Center, Department
Immunosuppressant medicines have allowed patients
 48 Clinical Pharmacist February 2010 Vol 2 Patients who tolerate a transplanted organ without the need for pharmacological intervention are few and far between. Several immunosuppressants can be used to
48 Clinical Pharmacist February 2010 Vol 2 Patients who tolerate a transplanted organ without the need for pharmacological intervention are few and far between. Several immunosuppressants can be used to
Post Transplant Immunosuppression: Consideration for Primary Care. Sameh Abul-Ezz, M.D., Dr.P.H.
 Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Post Transplant Immunosuppression: Consideration for Primary Care Sameh Abul-Ezz, M.D., Dr.P.H. Objectives Discuss the commonly used immunosuppressive medications and what you need to know to care for
Medications in the Solid Organ Transplant Recipient
 Medications in the Solid Organ Transplant Recipient Monica Morgan, PharmD Transplant Pharmacist UT Southwestern Medical Center Solid Organ Transplant Program Objectives To describe the typical medications
Medications in the Solid Organ Transplant Recipient Monica Morgan, PharmD Transplant Pharmacist UT Southwestern Medical Center Solid Organ Transplant Program Objectives To describe the typical medications
Transplant Hepatology
 Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
Transplant Hepatology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified
For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847)
") For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847) 317-5405 Lauren McDonnell GolinHarris (312) 729-4233 ASTELLAS RECEIVES FDA APPROVAL FOR USE OF PROGRAF (TACROLIMUS) IN CONJUNCTION WITH
For Immediate Release Contacts: Jenny Keeney Astellas US LLC (847) 317-5405 Lauren McDonnell GolinHarris (312) 729-4233 ASTELLAS RECEIVES FDA APPROVAL FOR USE OF PROGRAF (TACROLIMUS) IN CONJUNCTION WITH
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 30 November 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 30 November 2011 NULOJIX 250 mg, powder for concentrate for solution for infusion B/1 (CIP code: 580 415-7) B/2 (CIP
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 30 November 2011 NULOJIX 250 mg, powder for concentrate for solution for infusion B/1 (CIP code: 580 415-7) B/2 (CIP
Better than Google- Click on Immunosuppression Renal Transplant. David Landsberg Oct
 Better than Google- Click on Immunosuppression Renal Transplant David Landsberg Oct 3 2008 OUTLINE History of Immunosuppression Trends in Immunosupression FK vs CYA Steroid Minimization CNI Avoidance Sirolimus
Better than Google- Click on Immunosuppression Renal Transplant David Landsberg Oct 3 2008 OUTLINE History of Immunosuppression Trends in Immunosupression FK vs CYA Steroid Minimization CNI Avoidance Sirolimus
Immunosuppression: evolution in practice and trends,
 American Journal of Transplantation 25; 5 (Part 2): 874 886 Blackwell Munksgaard Blackwell Munksgaard 25 Immunosuppression: evolution in practice and trends, 1993 23 Ron Shapiro a,, James B. Young b, Edgar
American Journal of Transplantation 25; 5 (Part 2): 874 886 Blackwell Munksgaard Blackwell Munksgaard 25 Immunosuppression: evolution in practice and trends, 1993 23 Ron Shapiro a,, James B. Young b, Edgar
Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial
: a randomised trial") Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial Journal club Feb 2014 Background and Rationale Despite substantial
Alemtuzumab-based induction treatment versus basiliximab based induction treatment in kidney transplantation (the 3C Study): a randomised trial Journal club Feb 2014 Background and Rationale Despite substantial
Long term liver transplant management
 Long term liver transplant management Dr Bill Griffiths Cambridge Liver Unit Royal College of Physicians 5.7.17 Success of Liver Transplantation Current survival, 1 st elective transplant: 1 yr survival
Long term liver transplant management Dr Bill Griffiths Cambridge Liver Unit Royal College of Physicians 5.7.17 Success of Liver Transplantation Current survival, 1 st elective transplant: 1 yr survival
Nephrology Grand Rounds
 Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
Nephrology Grand Rounds PTLD in Kidney Transplantation Charles Le University of Colorado 6/15/12 Objectives Background Pathogenesis Epidemiology and Clinical Manifestation Incidence Risk Factors CNS Lymphoma
Immunosuppressive therapy for graft-versus-host disease. Mohamad Mohty Institut Paoli-Calmettes, Marseille
 Immunosuppressive therapy for graft-versus-host disease Mohamad Mohty Institut Paoli-Calmettes, Marseille Survival according to GVHD grade (Joint SFGM-TC, DFCI and IBMTR data; N=607) Cahn et al., Blood
Immunosuppressive therapy for graft-versus-host disease Mohamad Mohty Institut Paoli-Calmettes, Marseille Survival according to GVHD grade (Joint SFGM-TC, DFCI and IBMTR data; N=607) Cahn et al., Blood
Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant
 SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/29755 holds various files of this Leiden University dissertation. Author: Moes, Dirk Jan Alie Roelof Title: Optimizing immunosuppression with mtor inhibitors
Cover Page The handle http://hdl.handle.net/1887/29755 holds various files of this Leiden University dissertation. Author: Moes, Dirk Jan Alie Roelof Title: Optimizing immunosuppression with mtor inhibitors
1. Discuss the basic pathophysiology of end-stage liver and kidney failure.
 TRANSPLANT SURGERY ROTATION (PGY1, 2) A. Medical Knowledge Goal: The resident will achieve a detailed knowledge of the evaluation and treatment of a variety of disease processes. The resident will be exposed
TRANSPLANT SURGERY ROTATION (PGY1, 2) A. Medical Knowledge Goal: The resident will achieve a detailed knowledge of the evaluation and treatment of a variety of disease processes. The resident will be exposed
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
TRANSPLANT IMMUNOLOGY. Shiv Pillai Ragon Institute of MGH, MIT and Harvard
 TRANSPLANT IMMUNOLOGY Shiv Pillai Ragon Institute of MGH, MIT and Harvard Outline MHC / HLA Direct vs indirect allorecognition Alloreactive cells: where do they come from? Rejection and Immunosuppression
TRANSPLANT IMMUNOLOGY Shiv Pillai Ragon Institute of MGH, MIT and Harvard Outline MHC / HLA Direct vs indirect allorecognition Alloreactive cells: where do they come from? Rejection and Immunosuppression
It s just not that into you:
 CSHP Clinical Symposium - It s just not that into you: The no-excuses truth to understanding rejection and transplant pharmacology Erica D. Greanya, PharmD Clinical Pharmacy Specialist Solid Organ Transplantation
CSHP Clinical Symposium - It s just not that into you: The no-excuses truth to understanding rejection and transplant pharmacology Erica D. Greanya, PharmD Clinical Pharmacy Specialist Solid Organ Transplantation
Emerging Drug List EVEROLIMUS
 Generic (Trade Name): Manufacturer: Everolimus (Certican ) Novartis Pharmaceuticals NO. 57 MAY 2004 Indication: Current Regulatory Status: Description: Current Treatment: Cost: Evidence: For use with cyclosporine
Generic (Trade Name): Manufacturer: Everolimus (Certican ) Novartis Pharmaceuticals NO. 57 MAY 2004 Indication: Current Regulatory Status: Description: Current Treatment: Cost: Evidence: For use with cyclosporine
REACH Risk Evaluation to Achieve Cardiovascular Health
 Dyslipidemia and transplantation History: An 8-year-old boy presented with generalized edema and hypertension. A renal biopsy confirmed a diagnosis of focal segmental glomerulosclerosis (FSGS). After his
Dyslipidemia and transplantation History: An 8-year-old boy presented with generalized edema and hypertension. A renal biopsy confirmed a diagnosis of focal segmental glomerulosclerosis (FSGS). After his
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
By the way, I have a transplant..
 By the way, I have a transplant.. Transplant patient for non-transplant surgery David Elliott No relevant disclosures Organ donation in Australia - 2017 Survival rates following organ donation have increased
By the way, I have a transplant.. Transplant patient for non-transplant surgery David Elliott No relevant disclosures Organ donation in Australia - 2017 Survival rates following organ donation have increased
Certified Clinical Transplant Nurse (CCTN) * Detailed Content Outline
 * Detailed Content Outline") I. PRETRANSPLANTATION CARE 9 11 3 23 A. Evaluate End-Stage Organ Failure 1 1 1 3 1. History and physical assessment 2. Vital signs and / or hemodynamic parameters 3. Lab values 4. Diagnostic tests B. Monitor
I. PRETRANSPLANTATION CARE 9 11 3 23 A. Evaluate End-Stage Organ Failure 1 1 1 3 1. History and physical assessment 2. Vital signs and / or hemodynamic parameters 3. Lab values 4. Diagnostic tests B. Monitor
Immunosuppressive therapy in liver transplantation
 Journal of Hepatology 39 (2003) 664 678 Short Reviews on Liver Transplantation Associate Editor: Didier Samuel Immunosuppressive therapy in liver transplantation Filomena Conti 1, Emmanuel Morelon 2, Yvon
Journal of Hepatology 39 (2003) 664 678 Short Reviews on Liver Transplantation Associate Editor: Didier Samuel Immunosuppressive therapy in liver transplantation Filomena Conti 1, Emmanuel Morelon 2, Yvon
American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc.
: S1 S157 Wiley Periodicals Inc.") American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc. 2009 The Authors Journal compilation 2009 The American Society of Transplantation and the American Society of Transplant
American Journal of Transplantation 2009; 9 (Suppl 3): S1 S157 Wiley Periodicals Inc. 2009 The Authors Journal compilation 2009 The American Society of Transplantation and the American Society of Transplant
What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham
 What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham SYMPHONY Study Ekberg et al. NEJM 2008 Excluded: DCD kidneys; CIT>30hours;
What is the Best Induction Immunosuppression Regimen in Kidney Transplantation? Richard Borrows: Queen Elizabeth Hospital Birmingham SYMPHONY Study Ekberg et al. NEJM 2008 Excluded: DCD kidneys; CIT>30hours;
CAMPATH INDUCTION IN RENAL TRANSPLANTATION. by Kakit Edmond Chan. Thesis is submitted for the degree of MD [Res] of Imperial College London
![CAMPATH INDUCTION IN RENAL TRANSPLANTATION. by Kakit Edmond Chan. Thesis is submitted for the degree of MD [Res] of Imperial College London](/thumbs/80/80968355.jpg "CAMPATH INDUCTION IN RENAL TRANSPLANTATION. by Kakit Edmond Chan. Thesis is submitted for the degree of MD [Res] of Imperial College London") CAMPATH INDUCTION IN RENAL TRANSPLANTATION by Kakit Edmond Chan Thesis is submitted for the degree of MD [Res] of Imperial College London Department of Medicine Imperial College London kkchan 1 Abstract
CAMPATH INDUCTION IN RENAL TRANSPLANTATION by Kakit Edmond Chan Thesis is submitted for the degree of MD [Res] of Imperial College London Department of Medicine Imperial College London kkchan 1 Abstract
This study is currently recruiting participants.
 A Two Part, Phase 1/2, Safety, PK and PD Study of TOL101, an Anti-TCR Monoclonal Antibody for Prophylaxis of Acute Organ Rejection in Patients Receiving Renal Transplantation This study is currently recruiting
A Two Part, Phase 1/2, Safety, PK and PD Study of TOL101, an Anti-TCR Monoclonal Antibody for Prophylaxis of Acute Organ Rejection in Patients Receiving Renal Transplantation This study is currently recruiting
SELECTED ABSTRACTS. All (n) % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%
 % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%") SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
TDM. Measurement techniques used to determine cyclosporine level include:
 TDM Lecture 15: Cyclosporine. Cyclosporine is a cyclic polypeptide medication with immunosuppressant effect. It has the ability to block the production of interleukin-2 and other cytokines by T-lymphocytes.
TDM Lecture 15: Cyclosporine. Cyclosporine is a cyclic polypeptide medication with immunosuppressant effect. It has the ability to block the production of interleukin-2 and other cytokines by T-lymphocytes.
Mycophenolate Mofetil (MMF)
") SCG: For Transplant patients The following guidelines are designed to provide information relating to mycophenolate mofetil and to outline the responsibilities of the primary and secondary care teams in
SCG: For Transplant patients The following guidelines are designed to provide information relating to mycophenolate mofetil and to outline the responsibilities of the primary and secondary care teams in
Literature Review Transplantation
 Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
PUO in the Immunocompromised Host: CMV and beyond
 PUO in the Immunocompromised Host: CMV and beyond PUO in the immunocompromised host: role of viral infections Nature of host defect T cell defects Underlying disease Treatment Nature of clinical presentation
PUO in the Immunocompromised Host: CMV and beyond PUO in the immunocompromised host: role of viral infections Nature of host defect T cell defects Underlying disease Treatment Nature of clinical presentation
Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP
 Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP Pancreas transplant recipients are usually under age 50. The majority of pancreas transplants are performed on diabetics, who are generally
Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP Pancreas transplant recipients are usually under age 50. The majority of pancreas transplants are performed on diabetics, who are generally
Liver Transplant: What s Different? Brian Lin, MD, FACEP Emergency Medicine, Kaiser Permanente, San Francisco UCSF Clinical Assistant Professor
 Liver Transplant: What s Different? Brian Lin, MD, FACEP Emergency Medicine, Kaiser Permanente, San Francisco UCSF Clinical Assistant Professor No Disclosures. Background 45 years 1998-2008: 90,830 transplants
Liver Transplant: What s Different? Brian Lin, MD, FACEP Emergency Medicine, Kaiser Permanente, San Francisco UCSF Clinical Assistant Professor No Disclosures. Background 45 years 1998-2008: 90,830 transplants
ASSESSMENT OF THE PAEDIATRIC NEEDS IMMUNOLOGY DISCLAIMER
 European Medicines Agency Evaluation of Medicines for Human Use London, September 2006 Doc. Ref.: EMEA/381922/2006 ASSESSMENT OF THE PAEDIATRIC NEEDS IMMUNOLOGY DISCLAIMER The Paediatric Working Party
European Medicines Agency Evaluation of Medicines for Human Use London, September 2006 Doc. Ref.: EMEA/381922/2006 ASSESSMENT OF THE PAEDIATRIC NEEDS IMMUNOLOGY DISCLAIMER The Paediatric Working Party
Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ
 Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ Art of Good Cooking Good Ingredient Good donor + OK recipient Good technique Good team Good timing Good
Post Operative Management in Heart Transplant นพ พ ชร อ องจร ต ศ ลยศาสตร ห วใจและทรวงอก จ ฬาลงกรณ Art of Good Cooking Good Ingredient Good donor + OK recipient Good technique Good team Good timing Good
Innovation In Transplantation:
 Innovation In Transplantation: Improving outcomes Thomas C. Pearson Department of Surgery Emory Transplant Center CHOA Symposium October 22, 2016 Disclosures Belatacept preclinical and clinical trial were
Innovation In Transplantation: Improving outcomes Thomas C. Pearson Department of Surgery Emory Transplant Center CHOA Symposium October 22, 2016 Disclosures Belatacept preclinical and clinical trial were
FIT Board Review Corner March 2016
 FIT Board Review Corner March 2016 Welcome to the FIT Board Review Corner, prepared by Sarah Spriet, DO, and Tammy Peng, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
FIT Board Review Corner March 2016 Welcome to the FIT Board Review Corner, prepared by Sarah Spriet, DO, and Tammy Peng, MD, senior and junior representatives of ACAAI's Fellows-In-Training (FITs) to the
Transplantation simplified. Dr Jasna Macanovic Consultant Nephrologist Wessex Renal and Transplant Services Portsmouth, UK
 Transplantation simplified Dr Jasna Macanovic Consultant Nephrologist Wessex Renal and Transplant Services Portsmouth, UK HISTORY The first successful kidney transplant was performed in 1954 between identical
Transplantation simplified Dr Jasna Macanovic Consultant Nephrologist Wessex Renal and Transplant Services Portsmouth, UK HISTORY The first successful kidney transplant was performed in 1954 between identical
Belatacept: An Update of Ongoing Clinical Trials
 Belatacept: An Update of Ongoing Clinical Trials Michael D. Rizzari, MD University of Wisconsin Madison School of Medicine and Public Health, Madison, Wisconsin Abstract Belatacept is a fusion protein
Belatacept: An Update of Ongoing Clinical Trials Michael D. Rizzari, MD University of Wisconsin Madison School of Medicine and Public Health, Madison, Wisconsin Abstract Belatacept is a fusion protein
Immunopharmacology: Immunosuppression in Organ Transplanation
 Immunopharmacology: Immunosuppression in Organ Transplanation Prof D. A. Joyce Pharm 3320/3321 Organ Transplants, Australia Organ Donors (2013) Kidney 630 Liver 248 Heart 77 Lung 167 Pancreas 33 Bone Marrow
Immunopharmacology: Immunosuppression in Organ Transplanation Prof D. A. Joyce Pharm 3320/3321 Organ Transplants, Australia Organ Donors (2013) Kidney 630 Liver 248 Heart 77 Lung 167 Pancreas 33 Bone Marrow
BK Virus (BKV) Management Guideline: July 2017
 Management Guideline: July 2017") BK Virus (BKV) Management Guideline: July 2017 BK virus has up to a 60-80% seroprevalence rate in adults due to a primary oral or respiratory exposure in childhood. In the immumocompromised renal transplant
BK Virus (BKV) Management Guideline: July 2017 BK virus has up to a 60-80% seroprevalence rate in adults due to a primary oral or respiratory exposure in childhood. In the immumocompromised renal transplant
The common premise for immunosuppressive
 therapy update Current trends in immunosuppressive therapies for renal transplant recipients The common premise for immunosuppressive therapies in kidney transplantation is to use multiple agents to work
therapy update Current trends in immunosuppressive therapies for renal transplant recipients The common premise for immunosuppressive therapies in kidney transplantation is to use multiple agents to work
Transplantation. Immunology Unit College of Medicine King Saud University
 Transplantation Immunology Unit College of Medicine King Saud University Objectives To understand the diversity among human leukocyte antigens (HLA) or major histocompatibility complex (MHC) To know the
Transplantation Immunology Unit College of Medicine King Saud University Objectives To understand the diversity among human leukocyte antigens (HLA) or major histocompatibility complex (MHC) To know the
Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents
 BUMC Proceedings 1999;12:110-112 Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents CHERYLE GURK-TURNER, RPH Department of Pharmacy Services, BUMC wo mouse/human
BUMC Proceedings 1999;12:110-112 Pharmacology notes Interleukin-2 receptor-blocking monoclonal antibodies: evaluation of 2 new agents CHERYLE GURK-TURNER, RPH Department of Pharmacy Services, BUMC wo mouse/human
Fellows Conference 01/21/2016
 Fellows Conference 01/21/2016 Outline Basics of transplantation Benefits of transplantation Immunosuppressive medications Anatomy of Renal Transplantation Recipient Selection General medical condition.
Fellows Conference 01/21/2016 Outline Basics of transplantation Benefits of transplantation Immunosuppressive medications Anatomy of Renal Transplantation Recipient Selection General medical condition.
PanGraf Tacrolimus Capsules 0.5 / 1.0 / 5.0
 For the use of a Nephrologist / Transplant Surgeon or a Hospital or a Laboratory only PanGraf Tacrolimus Capsules 0.5 / 1.0 / 5.0 DESCRIPTION Tacrolimus is a macrolide lactone with potent immunosuppressive
For the use of a Nephrologist / Transplant Surgeon or a Hospital or a Laboratory only PanGraf Tacrolimus Capsules 0.5 / 1.0 / 5.0 DESCRIPTION Tacrolimus is a macrolide lactone with potent immunosuppressive
Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function
 ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
ArtIcle Efficacy and Safety of Thymoglobulin and Basiliximab in Kidney Transplant Patients at High Risk for Acute Rejection and Delayed Graft Function Guodong Chen, 1 Jingli Gu, 2 Jiang Qiu, 1 Changxi
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: TACROLIMUS Protocol number: CV 43
 UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: TACROLIMUS Protocol number: CV 43") Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: TACROLIMUS Protocol number: CV 43 Indications: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION IN ADULTS.
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: TACROLIMUS Protocol number: CV 43 Indications: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION IN ADULTS.
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Transplantation in Australia and New Zealand
 Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Chronic Kidney Disease & Transplantation. Paediatrics : 2004 FRACP
 Chronic Kidney Disease & Transplantation Paediatrics : 2004 FRACP ANZDATA Registry Mode of First Treatment - Paediatric 14 12 10 8 6 4 2 0 0-4 y 5-9 y 10-14 y 15-19 y Hospital CAPD Hospital HD Hospital
Chronic Kidney Disease & Transplantation Paediatrics : 2004 FRACP ANZDATA Registry Mode of First Treatment - Paediatric 14 12 10 8 6 4 2 0 0-4 y 5-9 y 10-14 y 15-19 y Hospital CAPD Hospital HD Hospital
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15
 UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15") Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: MYCOPHENOLATE MOFETIL/SODIUM Protocol number: CV 15 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION
Immunosuppression for pediatric cardiac transplantation in the modern era
 Ž. Progress in Pediatric Cardiology 11 2000 115 129 Immunosuppression for pediatric cardiac transplantation in the modern era Bill A. Pietra, Mark M. Boucek Department of Pediatrics, Uni ersity of Colorado
Ž. Progress in Pediatric Cardiology 11 2000 115 129 Immunosuppression for pediatric cardiac transplantation in the modern era Bill A. Pietra, Mark M. Boucek Department of Pediatrics, Uni ersity of Colorado
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies
 Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Post-Transplant Monitoring for the Development of Anti-Donor HLA Antibodies Lorita M Rebellato, Ph.D., D (ABHI) Associate Professor Department of Pathology The Brody School of Medicine at ECU Scientific
Date: 23 June Context and policy issues:
 Title: Basiliximab for Immunosuppression During a Calcineurin Inhibitor Holiday in Renal Transplant Patients with Acute Renal Dysfunction: Guidelines for Use and a Clinical and Cost-Effectiveness Review
Title: Basiliximab for Immunosuppression During a Calcineurin Inhibitor Holiday in Renal Transplant Patients with Acute Renal Dysfunction: Guidelines for Use and a Clinical and Cost-Effectiveness Review
Immunopathology of T cell mediated rejection
 Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Immunopathology of T cell mediated rejection Ibrahim Batal MD Columbia University College of Physicians & Surgeons New York, NY, USA Overview Pathophysiology and grading of TCMR TCMR is still a significant
Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta482
 Immunosuppressive e therapy for kidney transplant in children and young people Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta482 NICE 2018. All rights reserved. Subject
Immunosuppressive e therapy for kidney transplant in children and young people Technology appraisal guidance Published: 11 October 2017 nice.org.uk/guidance/ta482 NICE 2018. All rights reserved. Subject
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham
 Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
Victims of success: Do we still need clinical trials? Robert S. Gaston, MD CTI Clinical Trials and Consulting University of Alabama at Birmingham Disclosure Employee: CTI Clinical Trials and Consulting
Solid Organ Transplantation
 LOGO Solid Organ Transplantation Dr. Mohammad Taraz Clinical Pharmacist June 2011 2 Introduction Solid organ transplantation is a well accepted therapeutic option for patients with end-stage kidney, liver,
LOGO Solid Organ Transplantation Dr. Mohammad Taraz Clinical Pharmacist June 2011 2 Introduction Solid organ transplantation is a well accepted therapeutic option for patients with end-stage kidney, liver,
Strategies for Desensitization
 Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Image: Bruce Wetzel - Harry Schaefer, Wikimedia Commons
 Image: Bruce Wetzel - Harry Schaefer, Wikimedia Commons Martin lversen Section of Lung Transplantation Rigshospitalet Copenhagen Denmark martin.iversen@dadlnet.dk Immunosuppression for the non-transplant
Image: Bruce Wetzel - Harry Schaefer, Wikimedia Commons Martin lversen Section of Lung Transplantation Rigshospitalet Copenhagen Denmark martin.iversen@dadlnet.dk Immunosuppression for the non-transplant
Transplantation Immunology
 Transplantation Immunology Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation Children s Hospital New York Presbyterian
Transplantation Immunology Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation Children s Hospital New York Presbyterian
Transplantation Immunology
 Transplantation Immunology MHC Restricted Allograft Rejection Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation
Transplantation Immunology MHC Restricted Allograft Rejection Mitchell S. Cairo, MD Professor of Pediatrics, Medicine and Pathology Chief, Division, Pediatric Hematology & Blood & Marrow Transplantation
Serologic Markers CONVENTIONAL ANTIBODIES ANTIBODIES UNCONVENTIONAL. AIH Type I
 Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Autoimmune Hepatitis By Thomas Frazier Objective What we need to know about AIH Diagnosis Treatment Difficulties in both Liver transplantation concerns AASLD Guidelines: Hepatology. 2010 Jun;51(6):2193-213.
Clinical decisions regarding immunosuppressive
 PHARMACOLOGIC THERAPIES AND RATIONALES * Stuart D. Russell, MD ABSTRACT This article reviews evidence related to the use of induction therapy and longer-term combination immunosuppressive drug regimens
PHARMACOLOGIC THERAPIES AND RATIONALES * Stuart D. Russell, MD ABSTRACT This article reviews evidence related to the use of induction therapy and longer-term combination immunosuppressive drug regimens
Potential Catalysts in Therapeutics
 LIVER TRANSPLANTATION 20:S22 S31, 2014 SUPPLEMENT Potential Catalysts in Therapeutics Bruce A. Luxon Division of Gastroenterology-Hepatology, University of Iowa, Iowa City, IA Received July 23, 2014; accepted
LIVER TRANSPLANTATION 20:S22 S31, 2014 SUPPLEMENT Potential Catalysts in Therapeutics Bruce A. Luxon Division of Gastroenterology-Hepatology, University of Iowa, Iowa City, IA Received July 23, 2014; accepted
IMMUNOSUPPRESSIVE THERAPY Overview. Desensitization
 IMMUNOSUPPRESSIVE THERAPY Overview Two types of immune responses to allografts: Cellular response: foreign antigen recognition activate antigen-specific lymphocytes (T-cells) o Key mediator: T-cells o
IMMUNOSUPPRESSIVE THERAPY Overview Two types of immune responses to allografts: Cellular response: foreign antigen recognition activate antigen-specific lymphocytes (T-cells) o Key mediator: T-cells o
Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration Rate
 Case Reports in Transplantation, Article ID 190516, 4 pages http://dx.doi.org/10.1155/2014/190516 Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration
Case Reports in Transplantation, Article ID 190516, 4 pages http://dx.doi.org/10.1155/2014/190516 Case Report Beneficial Effect of Conversion to Belatacept in Kidney-Transplant Patients with a Low Glomerular-Filtration
Autoimmune Hepatitis. What Drug and for How Long? Hepatology Day May 30 th, 2015
 Autoimmune Hepatitis What Drug and for How Long? Rajaa Chatila, MD Associate Professor of Medicine Director, Internal Medicine Residency Program Lebanese American University Hepatology Day May 30 th, 2015
Autoimmune Hepatitis What Drug and for How Long? Rajaa Chatila, MD Associate Professor of Medicine Director, Internal Medicine Residency Program Lebanese American University Hepatology Day May 30 th, 2015
Proton Pump Inhibitors do not Interact with the Immunosuppressant Enteric-Coated Mycophenolate Sodium
 Proton Pump Inhibitors do not Interact with the Immunosuppressant Enteric-Coated Mycophenolate Sodium S. Kofler, C. Wolf, Z. Sisic, J. Behr, M. Vogeser, M. Shipkova, B. Meiser, G. Steinbeck, B. Reichart,
Proton Pump Inhibitors do not Interact with the Immunosuppressant Enteric-Coated Mycophenolate Sodium S. Kofler, C. Wolf, Z. Sisic, J. Behr, M. Vogeser, M. Shipkova, B. Meiser, G. Steinbeck, B. Reichart,
Overview of Immunosuppression in Renal Transplantation
 Chapter 10 Overview of Immunosuppression in Renal Transplantation M. Ghanta, J. Dreier, R. Jacob and I. Lee Additional information is available at the end of the chapter http://dx.doi.org/10.5772/54865
Chapter 10 Overview of Immunosuppression in Renal Transplantation M. Ghanta, J. Dreier, R. Jacob and I. Lee Additional information is available at the end of the chapter http://dx.doi.org/10.5772/54865
Heart Transplantation ACC Middle East Conference Dubai UAE October 21, 2017
 Heart Transplantation ACC Middle East Conference Dubai UAE October 21, 2017 Randall C Starling MD MPH FACC FAHA FESC FHFSA Professor of Medicine Kaufman Center for Heart Failure Department of Cardiovascular
Heart Transplantation ACC Middle East Conference Dubai UAE October 21, 2017 Randall C Starling MD MPH FACC FAHA FESC FHFSA Professor of Medicine Kaufman Center for Heart Failure Department of Cardiovascular
Chapter 22: Hematological Complications
 Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Islet Cell Allo-Transplantation. Disclosure. Objectives
 Islet Cell Allo-Transplantation Gregory P. Forlenza, MD MCR Assistant Professor Barbara Davis Center University of Colorado Denver Special thanks to Melena Bellin, MD at The University of Minnesota who
Islet Cell Allo-Transplantation Gregory P. Forlenza, MD MCR Assistant Professor Barbara Davis Center University of Colorado Denver Special thanks to Melena Bellin, MD at The University of Minnesota who
Ryszard Grenda: Steroid-Free Pediatric Transplantation. Early Steroid Withdrawal in Pediatric Renal Transplantation
 Trends in Transplant. 2011;5:115-20 Ryszard Grenda: Steroid-Free Pediatric Transplantation Early Steroid Withdrawal in Pediatric Renal Transplantation Ryszard Grenda Department of Nephrology, Kidney Transplantation
Trends in Transplant. 2011;5:115-20 Ryszard Grenda: Steroid-Free Pediatric Transplantation Early Steroid Withdrawal in Pediatric Renal Transplantation Ryszard Grenda Department of Nephrology, Kidney Transplantation
Progress in Pediatric Kidney Transplantation
 Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
Novel Therapies in Autoimmune Hepatitis
 Novel Therapies in Autoimmune Hepatitis Paul W. Rassam,MD Ass. Clinical Professor of Medicine Div. of Gastroenterology and Hepatology St George Hospital University Medical Center University of Balamand
Novel Therapies in Autoimmune Hepatitis Paul W. Rassam,MD Ass. Clinical Professor of Medicine Div. of Gastroenterology and Hepatology St George Hospital University Medical Center University of Balamand
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
Induction Immunosuppression With Rabbit Antithymocyte Globulin in Pediatric Liver Transplantation
 LIVER TRANSPLANTATION 12:1210-1214, 2006 ORIGINAL ARTICLE Induction Immunosuppression With Rabbit Antithymocyte Globulin in Pediatric Liver Transplantation Ashesh Shah, 1 Avinash Agarwal, 1 Richard Mangus,
LIVER TRANSPLANTATION 12:1210-1214, 2006 ORIGINAL ARTICLE Induction Immunosuppression With Rabbit Antithymocyte Globulin in Pediatric Liver Transplantation Ashesh Shah, 1 Avinash Agarwal, 1 Richard Mangus,
2/28/2017. Adult Heart Transplants Donor and Recipient Characteristics UNOS, Retransplant VCM. Other /2015 (N = 24,474)
") 1 46% 2% 3% 4% 0% 2% 2% CHD HCM ICM NICM RCM 49% 3% 3% 3% 1% 3% 3% Retransplant VCM 42% Other 35% 1/1982 6/2015 1/2009 6/2015 2016 JHLT. 2016 Oct; 35(10): 1149-1205 UNOS, 2017 Adult Heart Transplants Donor
1 46% 2% 3% 4% 0% 2% 2% CHD HCM ICM NICM RCM 49% 3% 3% 3% 1% 3% 3% Retransplant VCM 42% Other 35% 1/1982 6/2015 1/2009 6/2015 2016 JHLT. 2016 Oct; 35(10): 1149-1205 UNOS, 2017 Adult Heart Transplants Donor
Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center
 Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center Disclosure Research Funding from BMS. Learning Objectives -Define belatacept-resistant rejection
Belatacept: An Opportunity to Personalize Immunosuppression? Andrew Adams MD/PhD Emory Transplant Center Disclosure Research Funding from BMS. Learning Objectives -Define belatacept-resistant rejection
Acute GVHD. ESH-EBMT 2009 Latimer A. Devergie
 Acute GVHD ESH-EBMT 2009 Latimer A. Devergie Acute GVHD Activated Donor T cells damage host epithelial cells after an inflammatory cascade that begins after the preparative regimen GVHD is the major barrier
Acute GVHD ESH-EBMT 2009 Latimer A. Devergie Acute GVHD Activated Donor T cells damage host epithelial cells after an inflammatory cascade that begins after the preparative regimen GVHD is the major barrier
Pediatric Kidney Transplantation
 Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Increased Early Rejection Rate after Conversion from Tacrolimus in Kidney and Pancreas Transplantation
 Increased Early Rejection Rate after Conversion from Tacrolimus in Kidney and Pancreas Transplantation Gary W Barone 1, Beverley L Ketel 1, Sameh R Abul-Ezz 2, Meredith L Lightfoot 1 1 Department of Surgery
Increased Early Rejection Rate after Conversion from Tacrolimus in Kidney and Pancreas Transplantation Gary W Barone 1, Beverley L Ketel 1, Sameh R Abul-Ezz 2, Meredith L Lightfoot 1 1 Department of Surgery
clevelandclinic.org/transplant
 carolyn spiotta Pancreas/Kidney Transplant Recipient I feel so fortunate and thankful that I have received a second chance at life. Carolyn Spiotta, 44, Pittsburgh. Carolyn needed a new pancreas and kidney
carolyn spiotta Pancreas/Kidney Transplant Recipient I feel so fortunate and thankful that I have received a second chance at life. Carolyn Spiotta, 44, Pittsburgh. Carolyn needed a new pancreas and kidney
Rabbit Antithymocyte Globulin (Thymoglobulin Ò )
") REVIEW ARTICLE Drugs 2010; 70 (6): 691-732 0012-6667/10/0006-0691/$55.55/0 ª 2010 Adis Data Information BV. All rights reserved. Rabbit Antithymocyte Globulin (Thymoglobulin Ò ) 25 Years and New Frontiers
REVIEW ARTICLE Drugs 2010; 70 (6): 691-732 0012-6667/10/0006-0691/$55.55/0 ª 2010 Adis Data Information BV. All rights reserved. Rabbit Antithymocyte Globulin (Thymoglobulin Ò ) 25 Years and New Frontiers