VAGINITIS/CERVICITIS/ TRICHOMONIASIS. Susan Tuddenham, MD, MPH Division of Infectious Diseases Johns Hopkins
|
|
|
- Christopher Blake
- 6 years ago
- Views:
Transcription
1 VAGINITIS/CERVICITIS/ TRICHOMONIASIS Susan Tuddenham, MD, MPH Division of Infectious Diseases Johns Hopkins
2 Vaginitis
3 Case A: Alyssa : a 17 yo female runaway, on the streets for 6 mos living with her new boyfriend 10 days of funny vaginal discharge and mild abdominal pain Has never had an STD, has sex only with her boyfriend, she doesn t think he has any symptoms or STDs. Engages in oral, vaginal and anal sex Not using birth control, LMP 6-8 weeks ago Only engaged in injection drug use once, shared boyfriend s needle.
4 Even before you examine her, what is on your differential diagnosis list? Funny Vaginal Discharge Cervicitis/Urethritis: Chlamydia Gonorrhea (Mycoplasma genitalium) Vaginitis: Bacterial Vaginosis Trichomonas Candidiasis Other things to consider Sites of infection HIV HCV Pregnancy Co-morbidities Drug use Abuse Psychiatric issues PID

5 Examination reveals
6 Vaginitis/Vaginal Infection Most women will have one during lifetime Symptoms: discharge, itching/irritation or odor Etiology: Bacterial Vaginosis (40-45%) Trichomonas (15-20%) Vulvovaginal candidiasis (20-25%)
7 Clinical, economic issues Over six million health care visits each year are attributed to vaginitis Over one billion dollars are spent annually for the care and treatment of vaginitis
8 Back to Alyssa On exam she has a vaginal discharge. Pregnancy test is POSITIVE. Wet prep of vaginal secretions shows ph of 6.0 Clue cells +Whiff test Motile trichomonads No yeast What can you diagnose her with based on the wet prep?
9 Diagnostic Criteria DDx of Vaginal Syndrome Infections Normal Bacterial vaginosis Candida vulvovaginitis Vaginal ph >4.5 > 4.5 (usually) Discharge Amine odor (KOH whiff test) Microscopic exam Main patient complaints White, clear, flocculent Absent Lactobacilli None Thin, homogeneous, white, gray, adherent, often increased Present (fishy) Clue cells, coccoid bacteria, no WBCs Discharge, bad odor, White, curdy, cottage Cheese like, sometimes increased Absent Mycelia, budding yeast, pseudohyphae with KOH Itching/burnin g, discharge Trichomonas vaginitis >4.5 Yellow, green, frothy adherent, increased Present (fishy but not always) Trichomonads, WBCs >10/hpf Frothy discharge, bad odor, vulvar
10 Normal Vaginal Discharge Normal vaginal discharge is clear to white, odorless, and of high viscosity. Lactic acid helps to maintain a normal vaginal ph of 3.0 to 4.5. Acidic environment and other host immune factors inhibit the overgrowth of bacteria. Stratified squamous epithelial cells produce glycogen, due to estrogen stimulation nourish lactobacilli.
 ph, Bacteriocins, competitive binding Immunomodulatory effects? L. crispatus")
11 The Vaginal Microbiota (VMB) Communities of bacteria inhabiting the vagina Healthy VMB Lactobacillus species lactic acid acidify the vagina L. crispatus, L. jensenii, L. gasseri, L. iners Protect against pathogens (STIs, E.coli) ph, Bacteriocins, competitive binding Immunomodulatory effects? L. crispatus

12 Bacterial Vaginosis In some women, lactobacilli replaced by an overgrowth of a variety of gram negatives/anaerobes Gardnerella vaginalis, Prevotella, Mobiluncus etc BV associated with Inc risk acquisition TV, HSV, GC, CT Inc risk acquisition & transmission of HIV Inc risk preterm birth, chorioamnionitis. G. vaginalis


13 Bacterial Vaginosis Clinical Features % asymptomatic Malodorous, thin adherent vaginal discharge, ph>4.7, clue cells >20% of epithelial cells, positive amine or Whiff test Amsel's criteria- 3 out of the above 4 Nugent s criteria- quantifies the different bacteria present on gram stained vaginal fluid sample


14 Vaginitis Curriculum Wet Prep: Common Characteristics RBCs Saline: 40X objective Clue cells PMN Sperm RBCs Artifact Squamous epithelial cell Source: Seattle STD/HIV Prevention Training Center at the University of Washington
15 Epidemiology of BV Most common dx for women coming in to STD clinics Many women asymptomatic. In study of 14-49yo US women: BV prevalence: African-American 51%, Mexican Americans 32%, Caucasian 23%. Sexually associated (inc risk with inc # sexual partners and lack of barrier protection), but thus far insufficient evidence to treat partners. Douching? +/-
16 BV treatment Recommended for women with symptoms BV Adults/ adolescents RECOMMENDED REGIMENS DOSE/ROUTE Metronidazole 500 mg orally twice a day for 7 days or Metronidazole gel 0.75%, one full applicator (5g) intravaginally qd x 5 d or Clindamycin cream one full applicator (5g) intravaginally qhs x 7 d ALTERNATIVE REGIMENS: To be used if medical contraindication to recommended regimen Tinidazole 2 g po qd x 2 d or Tinidazole 1 g po qd x 5 d or Clindamycin 300 mg po bid x 7 d or Clindamycin ovules 100 mg intravaginally qhs x 3 d (Note: no studies support the addition of any available lactobacillus formulations or probiotic as an adjunctive or replacement therapy in women with BV.) Refrain from sex or use condoms during treatment; douching may increase relapse
 vs. placebo Previous European data suggested not inferior to flagyl. Not better than placebo for women with >=4 recurrances per year.")
17 Breaking news a new treatment for BV Secnidazole-2g po X1 Modified intent-to-treat population, with clinical outcome responder rates of 53.3% (57/107) vs 19.3% (11/57; P <.001) vs. placebo Previous European data suggested not inferior to flagyl. Not better than placebo for women with >=4 recurrances per year. Mix with pudding/applesauce
18 BV and Pregnancy Screening: Not recommended to screen in pregnancy Treatment of pregnant women: same as non-pregnant NO association between metronidazole during pregnancy and teratogenic or mutagenic effects in newborns Vaginal clindamycin also safe
19 High Rates of BV Recurrence BV frequently persists/recurs after antibiotic treatment 30% of women have symptomatic recurrence within days, and 70% within 9 months Why? Suspected causative factors include: failure to eliminate BV-associated organisms re-inoculation with organisms from an outside source i.e. sex partner or fomite (but thusfar efforts to treat partner have not been shown to improve response to therapy, relapse or recurrence.) persistence of risk factors i.e. intrauterine device, douching, lubricants failure to re-colonize lactobacilli or bacteria which sufficiently produce lactic acid,? microbial community important? failure of lactobacilli to fully acidify the vagina presence of bacteriophages that destroy lactobacilli Fredricks, Curr Infect Dis Rep, 2005; Marrazzo, J Infect Dis, 2002 and J Infect Dis, 2006; Bradshaw, J Infect Dis, 2006
20 Persistent or recurrent BV Limited data regarding management Try different recommended treatment regimen If this fails: Metronidazole gel twice weekly for 4-6 months reduced recurrences, but BV may recur when suppressive therapy is stopped (Sobel JD. Am J OB Gyn 2006;194: ) an oral nitroimidazole followed by intravaginal boric acid and suppressive metronidazole gel twice weekly for 4-6 months for those women in remission (Reichman O. Sex Transm Dis 2009;36:732-34) Monthly oral metronidazole administered with fluconazole has also been evaluated as suppressive therapy which reduced the incidence of BV and promoted colonization with normal vaginal flora (McClelland RS J Infect Dis 2008;197: ) Awaiting more data Vitamin D deficiencies; contraceptives and BV risk L. crispatus vaginal capsule (LACTIN-V) for BV prevention
 in non-lactobacillus women Detectable mucosal tenofovir was lower in non- Lactobacillus women In vitro, G.")
21 Can BV affect the efficacy of PrEP in women? Klatt et al. Science Vaginal tenofovir gel decreased HIV incidence by 61% (p=0.013) in Lactobacillus dominated women but only 18% (p=0.644) in non-lactobacillus women Detectable mucosal tenofovir was lower in non- Lactobacillus women In vitro, G. vaginalis and other BV associated bacteria appeared to metabolize tenofovir.

22 But Heffron et al. Lancet 2017 No difference in women on oral PrEP in PrEP efficacy based on vaginal microbiota.

23 Trichomoniasis Most common non-viral STI. Transmission is almost exclusively sexual Up to 85% asymptomatic
24 Trichomonas Epidemiology NAAT prevalence of TV, CT, and GC infections among 7593 U.S. women age 18 89, by age group Ginocchio CC Journal of clinical microbiology. Aug 2012
25 Trichomonas Prevalence: 50%-60% in female prison inmates & commercial sex workers Approx 20% of females at STD clinics 18-50% of women with vaginal complaints 10-43% in HIV+ women, recent study at HIV clinic: 17.4% of women tested were positive via NAAT. (Muzny et al. STD 2016) Increases risk for HIV acquisition. Screening recommended for HIV+ women (proposed interval: at least annually) Associated with inc risk of preterm birth and other adverse pregnancy outcomes and PID in HIV infected women Consider screening in those at high risk for infection or negative sequelae new or multiple partners, history of STDs exchange sex for payment, use injection drugs pregnant

26 Trichomonas Maximum growth at ph Motile at high ph Less prominent signs & symptoms at low ph Kills and ingests lactobacilli Clinical Features In men, urethritis, epididymitis, or prostatis OR asymptomatic In women,ranges from asymptomatic to severe vaginitis Purulent vaginal discharge Abnormal vaginal bleeding/post coital bleeding Vulvar edema, erythema Dysparenuia, pruritis
27 Diagnosis ph is usually >5 Examine saline wet prep of fresh vaginal fluid for motile trich - sensitivity is about 51-65% Culture on Diamond medium was gold standard: sensitivity 75-96% NAATs is >95% sensitive and > 95% specific Several assays are FDA-cleared for vaginal, endocervical or urine specimens from women with or without symptoms and for urine or urethral swabs (preferred) from men if lab is CLIA certified to run the test CLIA waved Point of care tests for women: OSOM Trich Rapid test (10 minutes with 82-95% sensitivity and >97% specificity and self-testing is option) Affirm VP III (45 minutes, with sensitivity 63% and specificity 99% No for Pap tests: too many false negatives and false positives
28 Treatment Metronidazole 2 g PO in a single dose OR Tinidazole 2 g PO in a single dose Alternate regimens Metronidazole 500 mg PO BID for 7 days No alcohol (24 hours MTZ; 72 hours TNZ); Metronidazole gel is not recommended (less efficacious); Tinidazole is not recommended in pregnancy (animal studies) Retest 3 mo after treatment (for HIV pos and neg women)
29 T vaginalis and HIV infection Women with HIV infection should receive screening at entry to care and annually if sexually active associated with PID (Moodley 2002) Treatment reduces genital HIV shedding (Kissinger 2009, Anderson 2012) Longer treatment course better in women metronidazole 500mg BID x7d (vs. 2g )-less TV at TOC/3 mo RR 0.46, CI: (Kissinger, 2010) Potential factors- BV infection, arv, changes in vaginal ecology No data to recommend extended treatment in men HIV + women should get Flagyl 500mg po BID X 7d
30 Treatment for Persistent or Recurrent Trichomoniasis Metronidazole 500 mg PO BID for 7 days If this regimen fails: Metronidazole 2 g PO for 7 days Tinidazole 2 g PO for 7 days OR If this regimen fails, do susceptibility tests May need to consider 2-3g po tinidazole X14 days plus intravaginal tinidazole,?intravaginal boric acid?
31 Management Sex partner management- all contacts should be treated Note: Patients should be counseled to refrain from sexual intercourse until all partners have been treated and symptoms have subsided.
32 Candidiasis Curriculum Epidemiology Epidemiology- VVC Affects most females during lifetime Most cases caused by C. albicans (85%- 90%) Second most common cause of vaginitis Estimated cost: $1 billion annually in the U.S.
33 Vulvovaginal Candidiasis (VVC) Inflammatory vaginitis and, if vulvar area is involved, vulvitis Etiology: C. albicans 80-92%, C. glabrata Candida is normal flora of the vagina 20% women are colonized with Candida
34 Classification of VVC Uncomplicated- sporadic or infrequent, mild to moderate, likely to be C. albicans, non-immunocompromised host Complicated- recurrent, severe, nonalbicans species, uncontrolled diabetes, debilitation, pregnancy, other immune suppression
35 Risk Factors oral contraceptive users pregnancy antibiotic use steroid use uncontrolled diabetes prior history of candida infections
36 Clinical Manifestations Pruritis vaginal irritation, vaginal discharge vulvar edema/excoriation dysuria, dysparenuia fissures

37 Candidiasis Curriculum Clinical Manifestations Vulvovaginal Candidiasis Source: Health Canada, Sexual Health and STI Section, Clinical Slide Gallery
38 Diagnosis Diagnosis: clinical exam, ph <4.5 (ph can be high with co-infections with TV or BV), KOH prep budding yeast and/or pseudo-hyphae, 50% may have negative microscopy, culture is gold standard

39 Candidiasis Curriculum Diagnosis PMNs and Yeast Pseudohyphae Saline: 40X objective Yeast pseudohyphae PMNs Squamous epithelial cells Yeast buds Source: Seattle STD/HIV Prevention Training Center at the University of Washington
40 Treatment Uncomplicated- OTC (butaconazole, clotrimazole, miconazole 3,7 day regimens) Single dose butaconazole available Other azoles- terconazole (non-otc) Oral agent- fluconazole 150 mg po once
41 Management Severe: 7 14 days of topical azole or 150 mg of fluconazole in two sequential oral doses (second dose 72 hours after initial dose) Complicated-recurrent VVC: ( 4 or more episodes in a year), 7-14 days of topical azole or 100-mg, 150-mg, or 200-mg oral dose of fluconazole every third day for a total of 3 doses [day 1, 4, and 7]) Maintenance: Oral fluconazole (i.e., 100-mg, 150-mg, or 200-mg dose) weekly for 6 months is the first line maintenance regimen. If this regimen is not feasible, topical treatments used intermittently can also be considered
42 Management Pregnancy: only topicals recommended. Immunocompromised may need 7-14 day regimen.
43 Back to Alyssa Pregnancy test +, has vaginal discharge. Wet prep of vaginal secretions shows ph of 6.0 Clue cells +Whiff test Motile trichomonads No yeast She has BV and Trichomonas!
44 But wait...
45 CERVICITIS
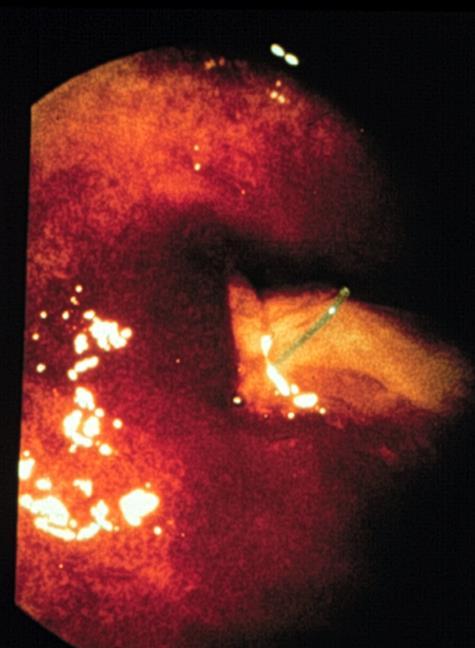
46 Definitions Endocervicitis- also known as mucopurulent cervicitis(mpc) Inflammation of the cervical epithelium Yellow/Green exudate visible in the endocervical canal OR yellow exudate on the endocervical swab Other features- edema/erythema of the zone of ectopy

47 Mucopurulent Cervical Discharge (Positive swab test) Diagnosis Source:Seattle STD/HIV Prevention Training Center at the University of Washington/ Claire E. Stevens and Ronald E. Roddy 47
48 Definitions Purulent discharge Easily induced cervical bleeding
49 Endocervicitis Etiology C. trachomatis, N. gonorrhea, HSV Others: Mycoplasma genitalium? No infectious etiology is identified in a significant number of these cases.
50 Ectocervicitis Etiology Ectocervicitis- T.vaginalis, HSV, Candida, CMV Non-infectious: trauma (chemical or mechanical), neoplasia.
51 Epidemiology Percentage distribution of the causes of MPC No infection- 38% CT- 15% GC- 8% HSV- 6% Multiple etiologies- 1-5%
52 Diagnosis Clinical- very difficult, utilized where there are no lab facilities or if patient is high risk Clues for clinical diagnosis- friability of cervix, mucopus in endocervical canal, change in color of endocervical swab
53 Diagnosis Nucleic acid tests- DNA detection e.g genprobes, DNA amplification e.g PCR/LCR (NAAT) for Chlamydia, Gonorrhea Higher sensitivity and specificity, compared to culture PCR/LCR- sens/spec up to 98-99%
54 Treatment Empiric tx for women at increased risk, esp if there are concerns re: followup Inc risk:aged <25 years, new sex partner, a sex partner with concurrent, partners, or a sex partner who has a sexually transmitted infection). All partners (last 60 days) should be evaluated and treated.
55 Empiric Treatment Treat for gonorrhea and chlamydia Ceftriaxone 250mg IV X1 Plus Azithromycin 1g po X1 (consider tx CT alone if community prevalence low) Persistent cervicitis: Further testing, Treatment for Mycoplasma genitalium with Moxifloxacin? (400 mg daily x 7, 10 or 14 days)
56 What should Alyssa be treated with? Doxycycline 100mg po BID for 7 days Flagyl 500mg po BID for 7 days plus Ceftriaxone 250mg IM X1 plus Azithromycin 1g po X1 Benzathine penicillin G IM X1 plus flagyl 500mg po BID for 7 days plus ceftriaxone 250mg IM X 1 plus doxycycline 100mg po BID for 7 days
57 The rest of Alyssa s test results Oral NG/CT NAT: positive for gonorrhea Rectal NG/CT NAT: negative Vaginal NG/CT NAT: positive for gonorrhea HCV ab: Positive HIV ab: Negative
58 Candidiasis Curriculum Prevention Patient Counseling and Education Nature of the disease Normal vs. abnormal vaginal discharge, signs and symptoms Transmission Issues- importance of partner evaluation and treatment Risk reduction Avoid douching, avoid unnecessary antibiotic use, complete course of treatment, abstain from sex until treatment is complete 58
59 Trichomoniasis Curriculum Prevention Risk Reduction The clinician should: Assess patient s potential for behavior change Discuss individualized risk-reduction plans with the patient Discuss prevention strategies such as monogamy, use of condoms, and limiting the number of sex partners Latex condoms, when used consistently and correctly, can reduce risk 59
60 Thank You! Susan Tuddenham
Learning Objectives VAGINITIS. Normal Vaginal Discharge. Learning Objectives
 Learning Objectives VAGINITIS Mychelle Y. Farmer, M.D. BCHD, STD-HIV Training Center Baltimore, Maryland Describe the characteristics of normal vaginal discharge. Understand the epidemiology and the common
Learning Objectives VAGINITIS Mychelle Y. Farmer, M.D. BCHD, STD-HIV Training Center Baltimore, Maryland Describe the characteristics of normal vaginal discharge. Understand the epidemiology and the common
Complex Vaginitis Cases: Applying New Diagnostic Methods to Enhance Patient Outcomes ReachMD Page 1 of 5
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
VAGINITIS What Makes a Good Vagina Go Bad?
 VAGINITIS What Makes a Good Vagina Go Bad? The 23 rd Annual Charleston Advanced Practice Registered Nurses Conference Judith T. Burgis, M.D. Professor and Chair Palmetto Health/USC Medical Group February
VAGINITIS What Makes a Good Vagina Go Bad? The 23 rd Annual Charleston Advanced Practice Registered Nurses Conference Judith T. Burgis, M.D. Professor and Chair Palmetto Health/USC Medical Group February
**Florida licensees, please note: This exercise is NOT intended to fulfill your state education requirement for molecular pathology.
 EDUCATIONAL COMMENTARY VAGINAL INFECTIONS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Earn
EDUCATIONAL COMMENTARY VAGINAL INFECTIONS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Earn
Vaginitis. Differential Diagnosis (con t) Vaginitis: Differential Diagnosis
 Vaginitis: Differential Diagnosis") 3:15 4:00 PM Case Studies in Vaginitis SPEAKER Martin A. Quan, MD Vaginitis one of the most common gynecologic disorders 10 million office visits/ year and 7 % visits to gynecologists 1 % antibiotics prescribed
3:15 4:00 PM Case Studies in Vaginitis SPEAKER Martin A. Quan, MD Vaginitis one of the most common gynecologic disorders 10 million office visits/ year and 7 % visits to gynecologists 1 % antibiotics prescribed
Dr Lilianne Scholtz (MBBCh)
") Dr Lilianne Scholtz (MBBCh) I have a discharge. It s itchy and it burns. My urine burns too. Diagnosis based on symptoms alone is accurate in ~34 % of women because symptoms are very non-specific Sobel
Dr Lilianne Scholtz (MBBCh) I have a discharge. It s itchy and it burns. My urine burns too. Diagnosis based on symptoms alone is accurate in ~34 % of women because symptoms are very non-specific Sobel
Vaginitis. Vaginitis: Differential Diagnosis. Differential Diagnosis (con t) Useful historical items. Infectious vaginitis 60 %
 Useful historical items. Infectious vaginitis 60 %") Presenter Disclosure Information 4:45 5:30 pm Case Studies in Vaginitis SPEAKER Martin Quan, MD The following relationships exist related to this presentation: Martin A. Quan, MD: No financial relationships
Presenter Disclosure Information 4:45 5:30 pm Case Studies in Vaginitis SPEAKER Martin Quan, MD The following relationships exist related to this presentation: Martin A. Quan, MD: No financial relationships
Microscopy Competency/Training For Clinic-Based Providers
 Microscopy Competency/Training For Clinic-Based Providers OSBHCN October 11, 2013 Diane Avenoso, MPH, MT(ASCP)SBB, CQA(ASQ) Clinical Laboratory Inspector/Compliance Specialist OHA, Oregon State Public
Microscopy Competency/Training For Clinic-Based Providers OSBHCN October 11, 2013 Diane Avenoso, MPH, MT(ASCP)SBB, CQA(ASQ) Clinical Laboratory Inspector/Compliance Specialist OHA, Oregon State Public
Vaginitis. Is vaginal discharge ever normal? Women with vaginal discharge. Vaginal symptoms are very common. Patient with chronic vaginal discharge
 Vaginitis Is the wet prep out of the building? No disclosures related to this topic Images are cited with permissions Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Health
Vaginitis Is the wet prep out of the building? No disclosures related to this topic Images are cited with permissions Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Health
Diagnosis of Vaginitis
 Vaginitis:, Bacterial Vaginosis, Candida, and Trichomonas Joy E. Zeh Family Nurse Practitioner Virginia Commonwealth University HIV/AIDS Center jzeh@vcu.edu Slides and self-study module available at www2a.cdc.gov/std/training
Vaginitis:, Bacterial Vaginosis, Candida, and Trichomonas Joy E. Zeh Family Nurse Practitioner Virginia Commonwealth University HIV/AIDS Center jzeh@vcu.edu Slides and self-study module available at www2a.cdc.gov/std/training
VAGINITIS: IT S NOT JUST YEAST. Index of this slide set VULVOVAGINITIS DAVID J. BOES, D.O., FACOOG MSU-COM SCS BOOT CAMP, 2018
 VAGINITIS: IT S NOT JUST YEAST DAVID J. BOES, D.O., FACOOG MSU-COM SCS BOOT CAMP, 2018 Index of this slide set Slide # 1-14: General aspects of Vaginitis Slide # 15-35: Trichomoniasis Slide # 36-59 Bacterial
VAGINITIS: IT S NOT JUST YEAST DAVID J. BOES, D.O., FACOOG MSU-COM SCS BOOT CAMP, 2018 Index of this slide set Slide # 1-14: General aspects of Vaginitis Slide # 15-35: Trichomoniasis Slide # 36-59 Bacterial
An All Too Familiar Story
 All that itches is not yeast Michele Ambor Hutz NP An All Too Familiar Story A patient presents to her provider complaining of frequent yeast infections. The provider prescribes treatment without an exam
All that itches is not yeast Michele Ambor Hutz NP An All Too Familiar Story A patient presents to her provider complaining of frequent yeast infections. The provider prescribes treatment without an exam
Vaginitis Do I have to look?
 Vaginitis Do I have to look? { Josette D Amato, D.O. Assistant Professor Department of Obstetrics & Gynecology Wright State University Boonshoft School of Medicine Pre-test Amsel s Diagnostic Criteria
Vaginitis Do I have to look? { Josette D Amato, D.O. Assistant Professor Department of Obstetrics & Gynecology Wright State University Boonshoft School of Medicine Pre-test Amsel s Diagnostic Criteria
Vaginitis. Background. Vaginal Environment. Vaginitis. This is a PDF version of the following document:
 National STD Curriculum PDF created November 12, 2018, 6:30 pm Vaginitis This is a PDF version of the following document: Disease Type 2: Syndrome-Based Diseases Disease 7: Vaginitis You can always find
National STD Curriculum PDF created November 12, 2018, 6:30 pm Vaginitis This is a PDF version of the following document: Disease Type 2: Syndrome-Based Diseases Disease 7: Vaginitis You can always find
Clinical Policy: Diagnosis of Vaginitis Reference Number: CP.MP.97
 Clinical Policy: Reference Number: CP.MP.97 Effective Date: 06/16 Last Review Date: 06/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Clinical Policy: Reference Number: CP.MP.97 Effective Date: 06/16 Last Review Date: 06/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Vaginitis. Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
 2:45 3:30pm Case Studies in Vaginitis SPEAKER Martin A. Quan, MD Presenter Disclosure Information The following relationships exist related to this presentation: Martin A. Quan, MD has no financial relationships
2:45 3:30pm Case Studies in Vaginitis SPEAKER Martin A. Quan, MD Presenter Disclosure Information The following relationships exist related to this presentation: Martin A. Quan, MD has no financial relationships
Clinical Policy: Diagnosis of Vaginitis Reference Number: CP.MP.97
 Clinical Policy: Reference Number: CP.MP.97 Effective Date: 06/16 Last Review Date: 06/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Clinical Policy: Reference Number: CP.MP.97 Effective Date: 06/16 Last Review Date: 06/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Investigation and Management of Vaginal Discharge in Adult Women
 Investigation and Management of Vaginal Discharge in Adult Women SUMMARY POINTS A detailed history, including sexual history, should be taken to explore potential causes and guide investigation and management.
Investigation and Management of Vaginal Discharge in Adult Women SUMMARY POINTS A detailed history, including sexual history, should be taken to explore potential causes and guide investigation and management.
Bacterial Vaginosis & VVC: How Can We Improve Current Diagnosis Methods?
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/womens-health-update/bacterial-vaginosis-vvc-how-can-we-improvecurrent-diagnosis-methods/10413/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/womens-health-update/bacterial-vaginosis-vvc-how-can-we-improvecurrent-diagnosis-methods/10413/
Vaginitis and STIs Causes, Work-up, Treatment
 Vaginitis and STIs Causes, Work-up, Treatment E.J. Mayeaux, Jr., M.D., FAAFP Professor of Family Medicine Professor of Obstetrics/Gynecology Louisiana State University Health Sciences Center Shreveport,
Vaginitis and STIs Causes, Work-up, Treatment E.J. Mayeaux, Jr., M.D., FAAFP Professor of Family Medicine Professor of Obstetrics/Gynecology Louisiana State University Health Sciences Center Shreveport,
Vaginal Discharge Syndromes
 Vaginal Discharge Syndromes Kees Rietmeijer, MD, PhD Colorado School of Public Health University of Colorado Denver Update on Sexually Transmitted Infections Harare, May 3, 2012 Cervical Anatomy and Terminology
Vaginal Discharge Syndromes Kees Rietmeijer, MD, PhD Colorado School of Public Health University of Colorado Denver Update on Sexually Transmitted Infections Harare, May 3, 2012 Cervical Anatomy and Terminology
Sexually Transmitted Disease Treatment Tables
 Sexually Transmitted Disease Treatment Tables Federal Bureau of Prisons Clinical Practice Guidelines June 2011 Clinical guidelines are made available to the public for informational purposes only. The
Sexually Transmitted Disease Treatment Tables Federal Bureau of Prisons Clinical Practice Guidelines June 2011 Clinical guidelines are made available to the public for informational purposes only. The
Overview of Wet Preps and Gram stains. Lorna Rabe Central Lab Magee-Womens Research Institute Pittsburgh, Pa
 Overview of Wet Preps and Gram stains Lorna Rabe Central Lab Magee-Womens Research Institute Pittsburgh, Pa Vaginal Flora A secondary objective of the 035 study is to assess the effectiveness of BufferGel
Overview of Wet Preps and Gram stains Lorna Rabe Central Lab Magee-Womens Research Institute Pittsburgh, Pa Vaginal Flora A secondary objective of the 035 study is to assess the effectiveness of BufferGel
Sexually Transmitted Infections in the Adolescent Population. Abraham Lichtmacher MD FACOG Chief of Women s Services Lovelace Health System
 Sexually Transmitted Infections in the Adolescent Population Abraham Lichtmacher MD FACOG Chief of Women s Services Lovelace Health System STI in the Adolescent High school students nationwide, 34.2% were
Sexually Transmitted Infections in the Adolescent Population Abraham Lichtmacher MD FACOG Chief of Women s Services Lovelace Health System STI in the Adolescent High school students nationwide, 34.2% were
What s New. Vaginal Discharge Protocol. History
 What s New Information has been added on interpreting vaginal scoring system and AV scores. Vaginal Discharge Protocol History Low risk STI PLUS Typical BV or VVC history AND No symptoms of PID High risk
What s New Information has been added on interpreting vaginal scoring system and AV scores. Vaginal Discharge Protocol History Low risk STI PLUS Typical BV or VVC history AND No symptoms of PID High risk
Answers to those burning questions -
 Answers to those burning questions - Ann Avery MD Infectious Diseases Physician-MetroHealth Medical Center Assistant Professor- Case Western Reserve University SOM Medical Director -Cleveland Department
Answers to those burning questions - Ann Avery MD Infectious Diseases Physician-MetroHealth Medical Center Assistant Professor- Case Western Reserve University SOM Medical Director -Cleveland Department
Burdensome Vaginal Infections: Best Diagnostic Practices for Driving Better Patient Outcomes
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Her Diagnosis Matters: What Can You Do to Prevent Misdiagnosis of Vaginitis?
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-industry-feature/her-diagnosis-matters-what-can-you-do-toprevent-misdiagnosis-of-vaginitis/9603/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/medical-industry-feature/her-diagnosis-matters-what-can-you-do-toprevent-misdiagnosis-of-vaginitis/9603/
Corporate Medical Policy
 Corporate Medical Policy Multitarget Polymerase Chain Reaction Testing for Diagnosis of File Name: Origination: Last CAP Review: Next CAP Review: Last Review: multitarget_polymerase_chain_reaction_testing_for_diagnosis_of_bacterial_vaginosis
Corporate Medical Policy Multitarget Polymerase Chain Reaction Testing for Diagnosis of File Name: Origination: Last CAP Review: Next CAP Review: Last Review: multitarget_polymerase_chain_reaction_testing_for_diagnosis_of_bacterial_vaginosis
Case Study 1. Cervical Cancer Screening and Sexually Transmitted Infections Case Studies
 Case Study 1 Cervical Cancer Screening and Sexually Transmitted Infections Case Studies Joyce, a 32 year old returning veteran, comes in for a Well Woman visit. She has a history of an abnormal Pap before
Case Study 1 Cervical Cancer Screening and Sexually Transmitted Infections Case Studies Joyce, a 32 year old returning veteran, comes in for a Well Woman visit. She has a history of an abnormal Pap before
Natural and Holistic Medicine Approach in Evaluation and Treatment of Vaginal and Urinary Tract Health
 Natural and Holistic Medicine Approach in Evaluation and Treatment of Vaginal and Urinary Tract Health By Dr. Michael John Badanek, BS, DC, CNS, CTTP, DACBN, DCBCN, MSGR./CHEV While the gut has an estimated
Natural and Holistic Medicine Approach in Evaluation and Treatment of Vaginal and Urinary Tract Health By Dr. Michael John Badanek, BS, DC, CNS, CTTP, DACBN, DCBCN, MSGR./CHEV While the gut has an estimated
The V The word the you cannot say on TV SHELAGH LARSON, WHNP, NCMP UNIVERSITY OF NORTH TEXAS HEALTH SCIENCE CENTER
 The V The word the you cannot say on TV SHELAGH LARSON, WHNP, NCMP UNIVERSITY OF NORTH TEXAS HEALTH SCIENCE CENTER Celebrity Vaginas???????? Parts Vulva Vestibule Vagina vagina is a specific internal
The V The word the you cannot say on TV SHELAGH LARSON, WHNP, NCMP UNIVERSITY OF NORTH TEXAS HEALTH SCIENCE CENTER Celebrity Vaginas???????? Parts Vulva Vestibule Vagina vagina is a specific internal
STI S: GONORRHEA, CHLYMADIA
 VAGINITIS IT S NOT JUST YEAST DAVID J. BOES, D.O., FACOOG SEPTEMBER, 2010 VAGINITIS LEARNING OBJECTIVES LEARNING OBJECTIVES Become familiar with EVALUATION & MANAGEMENT of the 3 most common vaginal infections
VAGINITIS IT S NOT JUST YEAST DAVID J. BOES, D.O., FACOOG SEPTEMBER, 2010 VAGINITIS LEARNING OBJECTIVES LEARNING OBJECTIVES Become familiar with EVALUATION & MANAGEMENT of the 3 most common vaginal infections
4/3/2017 DIAGNOSIS AND THERAPY OF RECURRENT VULVOVAGINAL SYMPTOMS BACTERIAL VAGINOSIS EPIDEMIOLOGY OBJECTIVES
 DIAGNOSIS AND THERAPY OF RECURRENT VULVOVAGINAL SYMPTOMS KELLY HODGES, MD (NO DISCLOSURES) OBJECTIVES REVIEW THE TWO MOST COMMON CAUSES OF RECURRENT ABNORMAL DISCHARGE (CANDIDA AND BV) REVIEW THE MOST
DIAGNOSIS AND THERAPY OF RECURRENT VULVOVAGINAL SYMPTOMS KELLY HODGES, MD (NO DISCLOSURES) OBJECTIVES REVIEW THE TWO MOST COMMON CAUSES OF RECURRENT ABNORMAL DISCHARGE (CANDIDA AND BV) REVIEW THE MOST
Nothing to disclose.
 Update on Diagnosis and Treatment Lisa Winston, MD University of California, San Francisco/ Zuckerberg San Francisco General Nothing to disclose. 1 This talk will be a little depressing Rising incidence
Update on Diagnosis and Treatment Lisa Winston, MD University of California, San Francisco/ Zuckerberg San Francisco General Nothing to disclose. 1 This talk will be a little depressing Rising incidence
Company. Relationship. Content Area. Glaxo Smith Kline. Speaker. Over Active Bladder, Herpes
 Conflict of Interest Disclosure R. Mimi Secor, MS, NP, FAANP I disclose the following financial relationships with commercial entities that produce health care-related products or services relevant to
Conflict of Interest Disclosure R. Mimi Secor, MS, NP, FAANP I disclose the following financial relationships with commercial entities that produce health care-related products or services relevant to
CLINICAL MANAGEMENT OF STDS
 CLINICAL MANAGEMENT OF STDS Diana Torres-Burgos MD, MPH NYC STD/HIV Prevention Training Center STD/HIV Update Conference Grand Rapids, MI 3/11/2014 Outline Essential components of STD care management Sexual
CLINICAL MANAGEMENT OF STDS Diana Torres-Burgos MD, MPH NYC STD/HIV Prevention Training Center STD/HIV Update Conference Grand Rapids, MI 3/11/2014 Outline Essential components of STD care management Sexual
Vaginitis. Antibiotics Changes in hormone levels due to pregnancy, breastfeeding, or menopause Douching Spermicides Sexual intercourse Infection
 WOMENCARE A Healthy Woman is a Powerful Woman (407) 898-1500 Vaginitis Vaginitis is an inflammation of a woman s vagina. It is one of the most common reasons why women see their health care providers.
WOMENCARE A Healthy Woman is a Powerful Woman (407) 898-1500 Vaginitis Vaginitis is an inflammation of a woman s vagina. It is one of the most common reasons why women see their health care providers.
TRICHOMONAS VAGINALIS
 TRICHOMONAS VAGINALIS What s New: There are no changes to this guideline. Introduction Trichomonas vaginalis (TV) is a flagellated protozoan that is a parasite of the genital tract. Due to site specificity,
TRICHOMONAS VAGINALIS What s New: There are no changes to this guideline. Introduction Trichomonas vaginalis (TV) is a flagellated protozoan that is a parasite of the genital tract. Due to site specificity,
Who's There? Changing concepts of vaginal microbiota
 Who's There? Changing concepts of vaginal microbiota Healthy vaginal ecosystem: H 2 O 2 -producing lactobacilli E.J. Baron, Ph.D., D(ABMM), F(AAM), F(IDSA) Prof. Emerita Pathology, Stanford University
Who's There? Changing concepts of vaginal microbiota Healthy vaginal ecosystem: H 2 O 2 -producing lactobacilli E.J. Baron, Ph.D., D(ABMM), F(AAM), F(IDSA) Prof. Emerita Pathology, Stanford University
Advances in STI diagnostics. Dr Paddy Horner Consultant Senior Lecturer University of Bristol
 Advances in STI diagnostics Dr Paddy Horner Consultant Senior Lecturer University of Bristol Advances in STI diagnostics Rapid expansion in on-line STI testing Outstripping NHS expert advice Increasing
Advances in STI diagnostics Dr Paddy Horner Consultant Senior Lecturer University of Bristol Advances in STI diagnostics Rapid expansion in on-line STI testing Outstripping NHS expert advice Increasing
Behaviors Associated with Changes in The Vaginal Microbiome
 Behaviors Associated with Changes in The Vaginal Microbiome Jeanne Marrazzo, MD, MPH UAB Division of Infectious Diseases MTN Annual Meeting March 2017 Discussion: The Healthy Vaginal Microbiome! What defines
Behaviors Associated with Changes in The Vaginal Microbiome Jeanne Marrazzo, MD, MPH UAB Division of Infectious Diseases MTN Annual Meeting March 2017 Discussion: The Healthy Vaginal Microbiome! What defines
Update on Sexually Transmitted Infections among Persons Living with HIV
 Update on Sexually Transmitted Infections among Persons Living with HIV Stephen A. Berry, MD PhD Assistant Professor of Medicine Johns Hopkins University Division of Infectious Diseases Abbreviations and
Update on Sexually Transmitted Infections among Persons Living with HIV Stephen A. Berry, MD PhD Assistant Professor of Medicine Johns Hopkins University Division of Infectious Diseases Abbreviations and
Genital Tract Infections in Women. Michael S. Policar, MD, MPH UCSF School of Medicine
 Genital Tract Infections in Women Michael S. Policar, MD, MPH UCSF School of Medicine www.policarlectures.com Value of STI Screening and Testing Benefits Detect infection Patient treatment Partner treatment
Genital Tract Infections in Women Michael S. Policar, MD, MPH UCSF School of Medicine www.policarlectures.com Value of STI Screening and Testing Benefits Detect infection Patient treatment Partner treatment
SEXUALLY TRANSMITTED INFECTIONS IN ST LOUIS
 SEXUALLY TRANSMITTED INFECTIONS IN ST LOUIS Sarah Garwood MD, Assistant Professor of Pediatrics, Washington University Elizabeth Fox MD, Pediatric Resident, St Louis Children s Hospital STDS IN ADOLESCENTS
SEXUALLY TRANSMITTED INFECTIONS IN ST LOUIS Sarah Garwood MD, Assistant Professor of Pediatrics, Washington University Elizabeth Fox MD, Pediatric Resident, St Louis Children s Hospital STDS IN ADOLESCENTS
BD Affirm VPIII Microbial Identification Test
 BD Affirm VPIII Microbial Identification Test VAGINAL INFECTIONS: The power of DNA technology for better patient care Diagnose and treat vaginitis/vaginosis patients correctly the first time Vaginitis
BD Affirm VPIII Microbial Identification Test VAGINAL INFECTIONS: The power of DNA technology for better patient care Diagnose and treat vaginitis/vaginosis patients correctly the first time Vaginitis
BD Affirm VPIII Microbial Identification Test VAGINAL INFECTIONS:
 BD Affirm VPIII Microbial Identification Test VAGINAL INFECTIONS: The power of DNA technology for better patient care Accurate test results on three pathogens with DNA technology The BD Affirm VPIII Microbial
BD Affirm VPIII Microbial Identification Test VAGINAL INFECTIONS: The power of DNA technology for better patient care Accurate test results on three pathogens with DNA technology The BD Affirm VPIII Microbial
STIs in Primary Care. Dr Eleanor Draeger 19 th January 2016
 STIs in Primary Care Dr Eleanor Draeger 19 th January 2016 Poli=cs! 2012! Health and Social Care act! Sexual Health commissioning moved to local authority! 2015! 200 million cuts to public health! 40%
STIs in Primary Care Dr Eleanor Draeger 19 th January 2016 Poli=cs! 2012! Health and Social Care act! Sexual Health commissioning moved to local authority! 2015! 200 million cuts to public health! 40%
Chapter 11. Sexually Transmitted Diseases
 Chapter 11. Sexually Transmitted Diseases General Guidelines Persons identified as having one sexually transmitted disease (STD) are at risk for others and should be screened as appropriate. Partners of
Chapter 11. Sexually Transmitted Diseases General Guidelines Persons identified as having one sexually transmitted disease (STD) are at risk for others and should be screened as appropriate. Partners of
Chlamydia, Gardenerella, and Ureaplasma
 Chlamydia, Gardenerella, and Ureaplasma Dr. Hala Al Daghsitani Chlamydia trachomatis is a Gram negative with LPS, obligate intracellular life cycle, associated with sexually transmitted disease (STD).
Chlamydia, Gardenerella, and Ureaplasma Dr. Hala Al Daghsitani Chlamydia trachomatis is a Gram negative with LPS, obligate intracellular life cycle, associated with sexually transmitted disease (STD).
Sexual consequencies of STIs:Chicken or egg. Dr Philip Kell Sexual Medicine Consultant UK
 Sexual consequencies of STIs:Chicken or egg Dr Philip Kell Sexual Medicine Consultant UK Obrigado por me terem convidado para falar na bela cidade de São Paulo Subjects to be covered HIV Chlamydia/Gonorrhoea
Sexual consequencies of STIs:Chicken or egg Dr Philip Kell Sexual Medicine Consultant UK Obrigado por me terem convidado para falar na bela cidade de São Paulo Subjects to be covered HIV Chlamydia/Gonorrhoea
FEMININE INTIMATE CARE
 FEMININE INTIMATE CARE The role of the pharmacist Dr Trudy Smith Vaginal Health Vagina sensitive area Just like GIT, also contain flora Vaginal flora Maintain healthy ph (4.5) Lactobacilli (aerobic) Automatic
FEMININE INTIMATE CARE The role of the pharmacist Dr Trudy Smith Vaginal Health Vagina sensitive area Just like GIT, also contain flora Vaginal flora Maintain healthy ph (4.5) Lactobacilli (aerobic) Automatic
Sexually Transmitted Diseases. Summary of CDC Treatment Guidelines
 DC 2015 Sexually Transmitted Diseases Summary of CDC Treatment Guidelines These summary guidelines reflect the June 2015 update to the 2010 CDC Guidelines for Treatment of Sexually Transmitted Diseases.
DC 2015 Sexually Transmitted Diseases Summary of CDC Treatment Guidelines These summary guidelines reflect the June 2015 update to the 2010 CDC Guidelines for Treatment of Sexually Transmitted Diseases.
GYNAZOLE 1 (butoconazole nitrate) vaginal cream 2%
 vaginal cream 2%") GYNAZOLE 1 (butoconazole nitrate) vaginal cream 2% Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
GYNAZOLE 1 (butoconazole nitrate) vaginal cream 2% Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
Clinical Prevention Behavioral Prevention Counseling
 38 th National Conference on Pediatric Health Care March 16-19, 2017 Disclosures Sexually Transmitted Infections: Update on Screening, Testing and Treatment Guidelines Brenda Cassidy, DNP, RN, CPNP Assistant
38 th National Conference on Pediatric Health Care March 16-19, 2017 Disclosures Sexually Transmitted Infections: Update on Screening, Testing and Treatment Guidelines Brenda Cassidy, DNP, RN, CPNP Assistant
Dr John Short. Obstetrician and Gynaecologist Christchurch Women s Hospital Oxford Women's Health Christchurch. 8:55-9:20 Infections in Gynaecology
 Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital Oxford Women's Health Christchurch 8:55-9:20 Infections in Gynaecology Infections in Gynaecology John Short Gynaecologist Oxford
Dr John Short Obstetrician and Gynaecologist Christchurch Women s Hospital Oxford Women's Health Christchurch 8:55-9:20 Infections in Gynaecology Infections in Gynaecology John Short Gynaecologist Oxford
EDUCATIONAL COMMENTARY - CLUE CELL MORPHOLOGY: DIAGNOSTIC CONSIDERATIONS
 EDUCATIONAL COMMENTARY - CLUE CELL MORPHOLOGY: DIAGNOSTIC CONSIDERATIONS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE
EDUCATIONAL COMMENTARY - CLUE CELL MORPHOLOGY: DIAGNOSTIC CONSIDERATIONS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE
Clinical Cases from the STD Clinical Consultation Network
 Clinical Cases from the STD Clinical Consultation Network Christine Johnston STD TCG April 24, 2017 Last Updated: uwptc@uw.edu uwptc.org 206-685-9850 STD Clinical Consultation Network (STDCCN) Developed
Clinical Cases from the STD Clinical Consultation Network Christine Johnston STD TCG April 24, 2017 Last Updated: uwptc@uw.edu uwptc.org 206-685-9850 STD Clinical Consultation Network (STDCCN) Developed
LABORATORY DIAGNOSIS SEXUALLY TRANSMITTED DISEASES
 LABORATORY DIAGNOSIS SEXUALLY TRANSMITTED DISEASES LABORATORY MEDICINE COURSE 2004 CLINICAL MICROBIOLOGY SERVICE STD EPIDEMIC- USA TIP OF THE ICEBERG INCIDENCE DISCHARGE Chlamydia - 4 million Gonorrhea
LABORATORY DIAGNOSIS SEXUALLY TRANSMITTED DISEASES LABORATORY MEDICINE COURSE 2004 CLINICAL MICROBIOLOGY SERVICE STD EPIDEMIC- USA TIP OF THE ICEBERG INCIDENCE DISCHARGE Chlamydia - 4 million Gonorrhea
Ackers, JP (2003) Trichomonas. In: The Oxford Textbook of Medicine. Oxford University Press, Oxford, 1:783-4.
 Trichomonas. In: The Oxford Textbook of Medicine. Oxford University Press, Oxford, 1:783-4.") Ackers, JP (2003) Trichomonas. In: The Oxford Textbook of Medicine. Oxford University Press, Oxford, 1:783-4. Downloaded from: http://researchonline.lshtm.ac.uk/15085/ DOI: Usage Guidelines Please refer
Ackers, JP (2003) Trichomonas. In: The Oxford Textbook of Medicine. Oxford University Press, Oxford, 1:783-4. Downloaded from: http://researchonline.lshtm.ac.uk/15085/ DOI: Usage Guidelines Please refer
Genital Chlamydia and Gonorrhea Epidemiology, Diagnosis, and Management. William M. Geisler M.D., M.P.H. University of Alabama at Birmingham
 Genital Chlamydia and Gonorrhea Epidemiology, Diagnosis, and Management William M. Geisler M.D., M.P.H. University of Alabama at Birmingham Chlamydia and Gonorrhea Current Epidemiology Chlamydia Epidemiology
Genital Chlamydia and Gonorrhea Epidemiology, Diagnosis, and Management William M. Geisler M.D., M.P.H. University of Alabama at Birmingham Chlamydia and Gonorrhea Current Epidemiology Chlamydia Epidemiology
The V The word the you cannot say on TV
 The V The word the you cannot say on TV SHELAGH LARSON, WHNP, NCMP UNIVERSITY OF NORTH TEXAS HEALTH SCIENCE CENTER 1 Celebrity Vaginas???????? Parts Vulva Vestibule Vagina vagina is a specific internal
The V The word the you cannot say on TV SHELAGH LARSON, WHNP, NCMP UNIVERSITY OF NORTH TEXAS HEALTH SCIENCE CENTER 1 Celebrity Vaginas???????? Parts Vulva Vestibule Vagina vagina is a specific internal
Sexually transmitted infections (in women)
") Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
Sexually transmitted infections (in women) Timothy Kremer, MD Assistant Professor, Department of Obstetrics and Gynecology University of North Texas Health Science Center Last official CDC guidelines:
Outline. Trichomoniasis: Testing and Treatment Update. What s in a name? From the Greek: trichos, hair monas, unit, single
 Trichomoniasis: Testing and Treatment Update Arlene C. Sena, MD, MPH Medical Director, Durham County Health Department Associate Professor, University of North Carolina Infectious Diseases Outline Epidemiology
Trichomoniasis: Testing and Treatment Update Arlene C. Sena, MD, MPH Medical Director, Durham County Health Department Associate Professor, University of North Carolina Infectious Diseases Outline Epidemiology
Cervical Cancer Screening and Sexually Transmitted Infections
 Cervical Cancer Screening and Sexually Transmitted Infections Primary author: Catherine Staropoli, MD VA Maryland Healthcare System Contributors: Kathleen McIntyre Seltman, MD VA Pittsburgh Healthcare
Cervical Cancer Screening and Sexually Transmitted Infections Primary author: Catherine Staropoli, MD VA Maryland Healthcare System Contributors: Kathleen McIntyre Seltman, MD VA Pittsburgh Healthcare
The (likely) New 2010 CDC STD Treatment Guidelines Guideline Development Process. Overview
 New 2010 CDC STD Treatment Guidelines Guideline Development Process. Overview") The (likely) New 2010 CDC STD Treatment Guidelines http://www.cdc.gov/std/treatment Deborah Cohan, MD, MPH University of California, San Francisco San Francisco General Hospital cohand@obgyn.ucsf.edu I
The (likely) New 2010 CDC STD Treatment Guidelines http://www.cdc.gov/std/treatment Deborah Cohan, MD, MPH University of California, San Francisco San Francisco General Hospital cohand@obgyn.ucsf.edu I
Evidence Based Commentary
 Evidence Based Commentary EBC Topic 2: 1 st Sept 2009 to 31 st Aug 2010 Faculty candidate number: ExM00643 Date completed: 26 th August 2010 Word Count: 1995 This Evidence Based Commentary is submitted
Evidence Based Commentary EBC Topic 2: 1 st Sept 2009 to 31 st Aug 2010 Faculty candidate number: ExM00643 Date completed: 26 th August 2010 Word Count: 1995 This Evidence Based Commentary is submitted
Disclosures. STD Screening for Women. Chlamydia & Gonorrhea. I have no disclosures or conflicts of interest to report.
 Disclosures Management of STIs: Challenges in Practice I have no disclosures or conflicts of interest to report. Alison O. Marshall, MSN, FNP-C Associate Professor of Practice & Director of the Family
Disclosures Management of STIs: Challenges in Practice I have no disclosures or conflicts of interest to report. Alison O. Marshall, MSN, FNP-C Associate Professor of Practice & Director of the Family
Elevating the Standard of Care for Women s Health: The BD MAX Vaginal Panel and Management of Vaginal Infections
 Elevating the Standard of Care for Women s Health: The BD MAX Vaginal Panel and Management of Vaginal Infections AUTHORS: Diane Kawa, PhD; Sonia Paradis, MSc; Judy H. Yu, PhD; Megan LeJeune BD Life Sciences-
Elevating the Standard of Care for Women s Health: The BD MAX Vaginal Panel and Management of Vaginal Infections AUTHORS: Diane Kawa, PhD; Sonia Paradis, MSc; Judy H. Yu, PhD; Megan LeJeune BD Life Sciences-
ORIGINAL ARTICLE. MICROBIOLOGICAL PROFILE OF VAGINAL SWABS. Sevitha Bhat, Nilica Devi, Shalini Shenoy
 MICROBIOLOGICAL PROFILE OF VAGINAL SWABS. Sevitha Bhat, Nilica Devi, Shalini Shenoy 1. Assistant Professor, Department of Microbiology, Kasturba Medical College, Mangalore. 2. MSc Student, Department of
MICROBIOLOGICAL PROFILE OF VAGINAL SWABS. Sevitha Bhat, Nilica Devi, Shalini Shenoy 1. Assistant Professor, Department of Microbiology, Kasturba Medical College, Mangalore. 2. MSc Student, Department of
Alberta Treatment Guidelines for Sexually Transmitted Infections (STI) in Adolescents and Adults 2008
 in Adolescents and Adults 2008") Alberta Treatment Guidelines for Sexually Transmitted Infections (STI) in Adolescents and Adults 2008 General for STI Given the current rise in all STI in Alberta, it is appropriate to assess for risk
Alberta Treatment Guidelines for Sexually Transmitted Infections (STI) in Adolescents and Adults 2008 General for STI Given the current rise in all STI in Alberta, it is appropriate to assess for risk
Expert Tips for Diagnosis and Management of Bacterial Vaginosis
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/miscellaneous/whats-new-bacterial-vaginosis/expert-tips-for-diagnosismanagement-of-bacterial-vaginosis/9894/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/miscellaneous/whats-new-bacterial-vaginosis/expert-tips-for-diagnosismanagement-of-bacterial-vaginosis/9894/
Differences in Vaginal Bacterial Communities of Women in North America: Implications for disease diagnosis and prevention
 Differences in Vaginal Bacterial Communities of Women in North America: Implications for disease diagnosis and prevention Larry J. Forney, Pawel Gajer, Christopher J. Williams, Maria G. Schneider, Stacey
Differences in Vaginal Bacterial Communities of Women in North America: Implications for disease diagnosis and prevention Larry J. Forney, Pawel Gajer, Christopher J. Williams, Maria G. Schneider, Stacey
Speaker Disclosures. What is the differential diagnosis? A Typical Case. Recurrent Vaginitis Syndromes: Etiologies
 Persistent Vaginitis: Practical Approaches to Care Speaker Disclosures Research funding: Cepheid, Viamet, GenProbe, BioHelix Scientific advisor: Merck, Astra-Zeneca 1919 2014 Jeanne Marrazzo, MD, MPH University
Persistent Vaginitis: Practical Approaches to Care Speaker Disclosures Research funding: Cepheid, Viamet, GenProbe, BioHelix Scientific advisor: Merck, Astra-Zeneca 1919 2014 Jeanne Marrazzo, MD, MPH University
The objectives of this presentation are; to increase awareness of the issue of antimicrobial resistant gonorrhea, and to inform primary care and
 1 Antimicrobial resistant gonorrhea is an emerging public health threat that needs to be addressed. Neisseria gonorrhoeae is able to develop resistance to antimicrobials quickly. Effective antibiotic stewardship
1 Antimicrobial resistant gonorrhea is an emerging public health threat that needs to be addressed. Neisseria gonorrhoeae is able to develop resistance to antimicrobials quickly. Effective antibiotic stewardship
Acute and Recurrent Bacterial Vaginosis
 Acute and Recurrent Bacterial Vaginosis Claire E. Hull, MHS, PA-C, Alison R. McLellan, MMS, PA-C Bacterial vaginosis (BV) is the most common cause of vaginal discharge in women of reproductive age. Although
Acute and Recurrent Bacterial Vaginosis Claire E. Hull, MHS, PA-C, Alison R. McLellan, MMS, PA-C Bacterial vaginosis (BV) is the most common cause of vaginal discharge in women of reproductive age. Although
Setting The setting was primary care. The economic study was carried out in the USA.
 "Shotgun" versus sequential testing: cost-effectiveness of diagnostic strategies for vaginitis Carr P L, Rothberg M B, Friedman R H, Felsenstein D, Pliskin J S Record Status This is a critical abstract
"Shotgun" versus sequential testing: cost-effectiveness of diagnostic strategies for vaginitis Carr P L, Rothberg M B, Friedman R H, Felsenstein D, Pliskin J S Record Status This is a critical abstract
Gynaecology. Pelvic inflammatory disesase
 Gynaecology د.شيماءعبداألميرالجميلي Pelvic inflammatory disesase Pelvic inflammatory disease (PID) is usually the result of infection ascending from the endocervix causing endometritis, salpingitis, parametritis,
Gynaecology د.شيماءعبداألميرالجميلي Pelvic inflammatory disesase Pelvic inflammatory disease (PID) is usually the result of infection ascending from the endocervix causing endometritis, salpingitis, parametritis,
Trichomoniasis allergic flagyl
 Trichomoniasis allergic flagyl The Borg System is 100 % Trichomoniasis allergic flagyl Dec 1, 2004. Because metronidazole is the only agent that is used to treat T. vaginalis infection, potential management
Trichomoniasis allergic flagyl The Borg System is 100 % Trichomoniasis allergic flagyl Dec 1, 2004. Because metronidazole is the only agent that is used to treat T. vaginalis infection, potential management
Vulvovaginal Candidiasis
 Vulvovaginal Candidiasis Hope K. Haefner, MD Michigan Medicine Ann Arb, MI USA Make Your Selection 1 Your Diagnosis Is? A. Candida albicans infection B. Non albicans Candida infection C. Gonrhea D. None
Vulvovaginal Candidiasis Hope K. Haefner, MD Michigan Medicine Ann Arb, MI USA Make Your Selection 1 Your Diagnosis Is? A. Candida albicans infection B. Non albicans Candida infection C. Gonrhea D. None
Stephanie. STD Diagnosis and Treatment. STD Screening for Women. Physical Exam. Cervix with discharge from os
 STD Diagnosis and Treatment Ina Park, MD, MS STD Control Branch, California Department of Public Health California STD/HIV Prevention Training Center Stephanie 23 year-old female presents for contraception,
STD Diagnosis and Treatment Ina Park, MD, MS STD Control Branch, California Department of Public Health California STD/HIV Prevention Training Center Stephanie 23 year-old female presents for contraception,
Types of vaginal yeast
 Types of vaginal yeast You should seek medical care any time if you have pain. Although vaginal infections may cause unpleasant itching, they should not cause pain. Call for an appointment with your healthcare
Types of vaginal yeast You should seek medical care any time if you have pain. Although vaginal infections may cause unpleasant itching, they should not cause pain. Call for an appointment with your healthcare
Fred Hutchinson Cancer Research Center, 2 University of Washington, 3. University of Nairobi, 4 University of Alabama at Birmingham
 Impact of periodic presumptive treatment for bacterial vaginosis on the vaginal microbiome among women participating in the Preventing Vaginal Infections trial Jennifer E. Balkus, PhD 1,2,, Sujatha Srinivasan,
Impact of periodic presumptive treatment for bacterial vaginosis on the vaginal microbiome among women participating in the Preventing Vaginal Infections trial Jennifer E. Balkus, PhD 1,2,, Sujatha Srinivasan,
Vaginal Microbial Ecology: an introduction. The Importance of Understanding Normal Vaginal Communities
 Vaginal Microbial cology: an introduction Larry J. Forney, Ph.D. Department of Biological Sciences Initiative for Bioinformatics and volutionary Studies University of Idaho The Importance of Understanding
Vaginal Microbial cology: an introduction Larry J. Forney, Ph.D. Department of Biological Sciences Initiative for Bioinformatics and volutionary Studies University of Idaho The Importance of Understanding
Multitarget Polymerase Chain Reaction Testing for Diagnosis of Bacterial Vaginosis
 Multitarget Polymerase Chain Reaction Testing for Diagnosis of Bacterial Vaginosis Policy Number: 2.04.127 Last Review: 12/2018 Origination: 12/2014 Next Review: 12/2019 Policy Blue Cross and Blue Shield
Multitarget Polymerase Chain Reaction Testing for Diagnosis of Bacterial Vaginosis Policy Number: 2.04.127 Last Review: 12/2018 Origination: 12/2014 Next Review: 12/2019 Policy Blue Cross and Blue Shield
Chlamydia Curriculum. Chlamydia. Chlamydia trachomatis
 Chlamydia Chlamydia trachomatis 1 Learning Objectives Upon completion of this content, the learner will be able to: 1. Describe the epidemiology of chlamydial infection in the U.S. 2. Describe the pathogenesis
Chlamydia Chlamydia trachomatis 1 Learning Objectives Upon completion of this content, the learner will be able to: 1. Describe the epidemiology of chlamydial infection in the U.S. 2. Describe the pathogenesis
SYNDROMIC CASE MANAGEMENT OF RTIs Advantages, Limitations, Optimization
 WHO COLLABORATING CENTRE FOR RESEARCH IN HUMAN REPRODUCTION Hôpitaux Universitaires de Genève SYNDROMIC CASE MANAGEMENT OF RTIs Advantages, Limitations, Optimization Dr SALONEY NAZEER Department of Gynaecology
WHO COLLABORATING CENTRE FOR RESEARCH IN HUMAN REPRODUCTION Hôpitaux Universitaires de Genève SYNDROMIC CASE MANAGEMENT OF RTIs Advantages, Limitations, Optimization Dr SALONEY NAZEER Department of Gynaecology
Sexually Transmitted Infections. Kim Dawson October 2010
 Sexually Transmitted Infections Kim Dawson October 2010 Objectives: You will learn about: Sexually Transmitted Infections (STI s). How they are transferred. High risk behavior. The most common STI s. How
Sexually Transmitted Infections Kim Dawson October 2010 Objectives: You will learn about: Sexually Transmitted Infections (STI s). How they are transferred. High risk behavior. The most common STI s. How
Edward W. Hook, III, M.D.
 Challenging Cases Edward W. Hook III M.D. Professor and Director Division of Infectious Diseases University of Alabama at Birmingham And PI, Alabama/North Carolina STD PTC Edward W. Hook, III, M.D. Grant/Research
Challenging Cases Edward W. Hook III M.D. Professor and Director Division of Infectious Diseases University of Alabama at Birmingham And PI, Alabama/North Carolina STD PTC Edward W. Hook, III, M.D. Grant/Research
CANDIDIASIS (WOMEN) Single Episode. Clinical Features. Diagnosis. Management
 Single Episode. Clinical Features. Diagnosis. Management") CANDIDIASIS (WOMEN) What s new: Section on Management of Vulvovaginal Non-Albicans Candida Infection in Adults approved by GGC antimicrobial team Routine candida sensitivity testing has been discontinued,
CANDIDIASIS (WOMEN) What s new: Section on Management of Vulvovaginal Non-Albicans Candida Infection in Adults approved by GGC antimicrobial team Routine candida sensitivity testing has been discontinued,
INTRAUTERINE DEVICES AND INFECTIONS. Tips for Evaluation and Management
 INTRAUTERINE DEVICES AND INFECTIONS Tips for Evaluation and Management Objectives At the end of this presentation, the participant should be able to: 1. Diagnose infection after IUD placement 2. Provide
INTRAUTERINE DEVICES AND INFECTIONS Tips for Evaluation and Management Objectives At the end of this presentation, the participant should be able to: 1. Diagnose infection after IUD placement 2. Provide
X-Treme Primary Care: HPV and STIs. Arti Barnes MD MPH Clinical Director South Central AIDS Education and Training Centers
 X-Treme Primary Care: HPV and STIs Arti Barnes MD MPH Clinical Director South Central AIDS Education and Training Centers Learning Objectives Review recommendations for HPV related cancer screening in
X-Treme Primary Care: HPV and STIs Arti Barnes MD MPH Clinical Director South Central AIDS Education and Training Centers Learning Objectives Review recommendations for HPV related cancer screening in
Study to Evaluate Targeted Management and Syndromic Management in Women Presenting with Abnormal Vaginal Discharge
 DOI 10.1007/s13224-016-0879-x ORIGINAL ARTICLE Study to Evaluate Targeted Management and Syndromic Management in Women Presenting with Abnormal Vaginal Discharge Veena Meena 1 Charu Lata Bansal 2 Received:
DOI 10.1007/s13224-016-0879-x ORIGINAL ARTICLE Study to Evaluate Targeted Management and Syndromic Management in Women Presenting with Abnormal Vaginal Discharge Veena Meena 1 Charu Lata Bansal 2 Received:
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES
 ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
ALASKA NATIVE MEDICAL CENTER SEXUALLY TRANSMITTED DISEASE SCREENING AND TREATMENT GUIDELINES A. Screening Page Chlamydia and Gonorrhea 1 HIV 1 Syphilis 1 Genital Herpes 2 Hepatitis A 2 Hepatitis B 2 Hepatitis
MP Multitarget Polymerase Chain Reaction Testing for Diagnosis of Bacterial Vaginosis
 Medical Policy MP 2.04.127 BCBSA Ref. Policy: 2.04.127 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Medicine Related Policies 2.04.10 Identification of Microorganisms Using Nucleic Acid
Medical Policy MP 2.04.127 BCBSA Ref. Policy: 2.04.127 Last Review: 07/25/2018 Effective Date: 07/25/2018 Section: Medicine Related Policies 2.04.10 Identification of Microorganisms Using Nucleic Acid
Parasitology. The genus Trichomonas
 Parasitology Lecture: 2 د. هيفاء The genus Trichomonas -These are common flagellates of the tropical areas,. -They exist only in trophozoite stage. -They are pear-shaped body and measures 10-12 microns
Parasitology Lecture: 2 د. هيفاء The genus Trichomonas -These are common flagellates of the tropical areas,. -They exist only in trophozoite stage. -They are pear-shaped body and measures 10-12 microns
Population attributable fraction of genital inflammation and ulceration in HIV risk among discordant couples, Zambia,
 Population attributable fraction of genital inflammation and ulceration in HIV risk among discordant couples, Zambia, 1994-2012 10 th International Workshop on HIV Transmission Kristin M. Wall, PhD kmwall@emory.edu
Population attributable fraction of genital inflammation and ulceration in HIV risk among discordant couples, Zambia, 1994-2012 10 th International Workshop on HIV Transmission Kristin M. Wall, PhD kmwall@emory.edu
What's the problem? - click where appropriate.
 STI Tool v 1.9 @ 16/11/2017 What's the problem? - click where appropriate. Male problems: screening urethral symptoms proctitis in gay men lumps or swellings ulcers or sores skin rash and/or itch Female
STI Tool v 1.9 @ 16/11/2017 What's the problem? - click where appropriate. Male problems: screening urethral symptoms proctitis in gay men lumps or swellings ulcers or sores skin rash and/or itch Female