An outer surface protein C (OspC) peptide derived from Borrelia burgdorferi sensu. strico as a target for the serodiagnosis of early Lyme disease.
|
|
|
- Holly Garrett
- 5 years ago
- Views:
Transcription
1 CVI Accepts, published online ahead of print on 30 January 2013 Clin. Vaccine Immunol. doi: /cvi Copyright 2013, American Society for Microbiology. All Rights Reserved An outer surface protein C (OspC) peptide derived from Borrelia burgdorferi sensu strico as a target for the serodiagnosis of early Lyme disease Paul M. Arnaboldi, Ph.D 1,2., Rudra Seedarnee, M.S. 2, Mariya Sambir, M.S. 1,2, Steven M. Callister, Ph.D. 3, Josephine A. Imparato 1, and Raymond J. Dattwyler, M.D 1,2,4,# Running Title: A diagnostic OspC peptide for Lyme disease 1 -Biopeptides Corp, East Setauket, New York, 11733, USA 2 -Department of Microbiology, New York Medical College, Valhalla, New York, 10595, USA 3 -Gundersen Lutheran Medical Center, La Crosse, Wisconsin, 54601, USA 4 -Department of Medicine, New York Medical College, Valhalla, New York, 10595, USA # -Correspondence should be addressed to Raymond J. Dattwyler, M.D., raymond_dattwyler@nymc.edu 18 1
2 19 Abstract Current serodiagnostic assays for Lyme disease are inadequate at detecting early infection due to poor sensitivity and non-specificity that arise from the use of whole bacteria or bacterial proteins as assay targets; both targets contain epitopes that are cross-reactive with epitopes found in antigens of other bacteria species. Tests utilizing peptides that containing individual epitopes highly-specific for Borrelia burgdorferi as diagnostic targets are an attractive alternative to current assays. Using an overlapping peptide library, we mapped linear epitopes in OspC, a critical virulence factor of B. burgdorferi required for mammalian infection, and confirmed the results by ELISA. We identified a highly conserved 20-amino acid peptide epitope, OspC1. Via ELISA, OspC1 detected specific IgM and/or IgG in 60 out of 98 serum samples (62.1%) obtained from patients with erythema migrans (early Lyme disease) at the time of their initial presentation. By comparison, the commercially available OspC peptide, PepC10, detected antibody in only 48 of 98 serum samples (49.0%). In addition, OspC1 generated fewer false positive results among negative healthy and disease (rheumatoid arthritis and RPR+) control populations compared to PepC10. Both highly specific and more sensitive than currently available OspC peptides, OspC1 could have value as a component of a multi-peptide Lyme disease serological assay with significantly improved capabilities for the diagnosis of early infection Key Words: Lyme disease; immunodiagnostic assays; Borrelia burgdorferi; OspC; serological assay 41 2
3 42 Introduction Lyme disease is the most common tick-transmitted disease in North America and Europe. The disease is caused by spirochetes of the genus Borrelia (including burgdorferi, garinii, and afzelli), which are transmitted to humans through the bite of infected Ixodes ticks (1, 2). Early disease is typified by the characteristic skin lesion erythema migrans (EM) that occurs in the majority of infected patients, as well as more nonspecific symptoms that can include low grade fever, headache, muscle and joint aches, and swollen regional lymph nodes. Though early disease is easily cured with an appropriate short course of antibiotics, if allowed to persist, disease progression can lead to permanent neurological and/or musculoskeletal damage (1-3, 3-8). Early intervention is therefore critical to disease outcome. Unlike most bacterial diseases where the presence of the pathogen can be defined microbiologically by direct observation, culture, or PCR, Lyme disease is defined indirectly (9-12). EM is the classic marker of early infection, and is considered pathognomonic in endemic areas (9). However, not all patients infected with B. burgdorferi develop EM (9), and even if present, it is fleeting and may be gone by the time patient seeks medical attention. In the absence of EM, diagnosis of Lyme disease is based on the serological detection of antibodies against whole Borrelia and/or Borrelia proteins (10). Current CDC guidelines for the serodiagnosis of Lyme disease mandate a twotier analysis for improved accuracy, as current IgM and IgG serological assays lack sufficient specificity and/or are insensitive for the detection of antibody present at the time that many patients with early Lyme disease seek initial medical care (13-19). The first tier assay is an ELISA, typically utilizing lysates of whole-borrelia as the target, 3
4 which if positive or equivocal, is followed by a western blot containing several whole Borrelia proteins (9, 10, 20, 21). Some of the whole protein antigens present in both whole cell ELISAs and in western blot assays contain epitopes that are cross-reactive with epitopes found in antigens of other bacteria (9). Because of the need to maintain a reasonable balance between specificity and sensitivity, current laboratory tests fail to serodiagnose early Lyme disease approximately 50% of the time (1, 4, 10, 20, 22). Clearly, new approaches are needed to develop better diagnostics. Peptides containing specific epitopes represent a logical alternative to whole-protein antigens as targets in diagnostics as it allows for the elimination of cross-reactive epitopes, retaining only those highly specific for Borrelia. An ELISA (IR6) using a peptide derived from the VlsE protein of Borrelia has demonstrated greater specificity in the detection of Lyme disease than whole cell ELISAs, and has been approved for use by the FDA (19, 23). However, C6, the peptide derived from VlsE, does not bind IgM particularly well, is derived from an antigen that is expressed only after infection is established (less than 1% of bacteria in the tick express VlsE, and transcription of the gene is suppressed prior to transmission of the bacteria), and the IR6 region of VlsE from which the peptide is derived has shown a greater degree of variability than originally thought (19, 23-26). Though a significant improvement, in terms of specificity, compared to the whole cell ELISA test (27), these concerns have precluded the use of the C6 assay as a standalone diagnostic test for early Lyme disease. These limitations could be addressed by combining multiple peptide-epitopes into a single assay (28). Thus, the identification of further epitopes is of paramount importance to the advancement of Lyme disease serodiagnostics. 4
5 OspC is a Borrelia surface protein required for transmission of the bacteria from the midgut of tick into the human host (29). It is a protein of significant diagnostic value because it is required for entry into the mammalian host, and therefore, will always present during infection and is expressed during the initiation of infection. However, the OspC protein is not highly conserved, containing numerous subtypes that have significant sequence variability. Furthermore, some previous studies using whole recombinant OspC as a serodiagnostic for Lyme disease demonstrated a high level of cross-reactivity within negative disease control samples (30, 31), though cross-reactivity was not often seen in normal control serum (30-34). In the present study we mapped linear epitopes within the OspC protein to identify highly-conserved regions lacking cross-reactivity with antigens from other bacteria. We have generated an antigenic peptide (OspC1) that binds to antibody from early Lyme disease patients with high specificity. OspC1 outperformed a previously identified peptide antigen from OspC (PepC10) in an ELISA-based immunoassay, and is a potential target for inclusion into a sensitive multi-peptide serological assay for the diagnosis of early Lyme disease. 5
6 103 Materials and Methods Serum: 98 serum samples were obtained with consent, under IRB approval, from patients with erythema migrans (early Lyme disease) at their initial presentation to the Lyme disease clinic at Westchester Medical Center in Westchester, NY (n=48) or Gundersen-Lutheran Medical Center in La Crosse, WI (n=50). 20 serum samples were obtained from patients with Lyme arthritis (late Lyme disease) upon first clinical presentation at Gundersen-Lutheran Medical Center in La Crosse, WI with swollen joints (n=20). Both areas are highly endemic for Lyme disease. 48 sera from healthy individuals residing in a non-endemic region for Lyme disease (New Mexico) were purchased from Creative Testing Solutions (Tempe, AZ). 87 disease-control sera obtained from patients with Rheumatoid arthritis (RA) (n=48) or a positive Rapid Plasma Reagin (RPR+) test result (n-=39) were purchased from Bioreclamation, LLC (Westbury, NY). 34 of 39 RPR+ sera were also confirmed positive for IgG against Treponema pallidum by ELISA (Abnova, Walnut, CA). Both the RA and the RPR+ control sera were collected in a region endemic for Lyme disease (southern New York State). Peptides: Epitope mapping was performed by ProImmune, Inc. (Oxford, UK) using their proprietary ProArray Ultra peptide microarray technology. In brief, overlapping peptide libraries generated from the sequence for OspC type K (accession # AAB86554), and consisting of 15-mer peptides overlapping by 10 AA, were exposed to multiple dilutions of eight individual sera containing antibodies against B. burgdorferi sensu stricto, as determined by western blot ( Viramed Biotech AG, Planegg, Germany). Positive binding of serum was detected using a fluorochrome-labeled anti-human 6
7 secondary antibody and the data were reported as dimensionless units of the average fluorescence signal intensity (FSI) for replicate spots of each peptide. A positive signal was required to be at least 4x the FSI of the negative assay control. Peptides chosen for further analysis were produced by Lifetein, Inc. (South Plainfield, NJ), and were a minimum of 90% purity. Sequence alignment of different OspC types was performed using CLC Workbench (Figures 1 and S1). The following sequences for each OspC type were identified previously (14, 35, 36), {B. burgdorferi strain, OspC type, Accession#}: {B31, A, CAA49306}; {PBRe, B, CAA57242}; {OC3, C, AAB86545}; {CA- 11.2A, D, AAA22956}; {N40, E, CAA58545}; {B. pacificus, F, AAC45538}; {OC8, G, AAB86550}; {LDS79, H, ABK41060}; {OC9, H, AAB86551}; {HB19, I, AAC43297}; {MIL, J, AAB81899}; {OC10, J, AAB86553}; {OC12, K, AAB86554}; {LDP74, K, ABK41058}; {T255, L, CAA57244}; {B356, M, AAN37936}; {2591, M, AAN16057}; {26815, N, AAB37006}; {CS5, U, ABD95831}. When a complete sequence was not available for an OspC type multiple sequences (if available) for that type were presented showing the presence or absence of the peptide of interest. ELISA: 96-well Maxisorp (Nunc, Rochester, NY) plates were coated with 10 µg/ml of peptide in 0.1 M sodium carbonate buffer, ph 9.4 for 1h at room temperature. After 1h, 1% BSA in PBS(blocking buffer) was added to each well and incubated overnight at 4 C. The next morning plates were washed 3x with 0.05% Tween-20 in PBS using an automated plate washer (Molecular Devices, Sunnyvale, CA). Serum samples diluted 1:100 in blocking buffer were added in triplicate and incubated at room temperature for 2h. The plates were washed again and HRP-labeled goat anti-human IgM (μ-chain specific) or HRP-labeled goat anti-human IgG (γ-chain specific) (Southern Biotech, 7
8 Birmingham, AL) diluted 1:5000 in blocking buffer was added to each well for 1h at room temperature. The plates were washed and developed with TMB substrate (KPL, Gaithersburg, Maryland) for 30 min at room temperature. The reaction was stopped by addition of 2N sulfuric acid, and absorbance was read at 450nm and 570nm (Molecular Devices) Data Analysis: The sensitivity and specificity of each peptide was determined for both IgM and IgG by comparing results from Lyme patients with results from negative controls via ROC analysis using Prism 6.0 (Graphpad, La Jolla, CA). Cut-off values used for comparing sensitivity and specificity between the two peptides were 3 SD from the mean of healthy controls as the cut-off (limit of detection). Statistical analysis of categorical data presented in tables and the text was performed using a Fisher s exact test with a two-tailed p value using Prism 6.0 (Graphpad). Downloaded from on July 17, 2018 by guest 8
9 161 Results Eight serum samples from Lyme disease patients were chosen for the initial epitope mapping based upon a high titer of anti-borrelia antibodies as determined by the detection of 9-10 out of 10 bands on a commercially available Lyme disease diagnostic western blot strip test (5 of 10 bands is the minimum requirement for a sample to be considered positive). Epitope mapping was performed by ProImmune, Inc. using their proprietary ProArray Ultra peptide microarray technology. A partial sequence for OspC type K (B. burgdorferi OC12, accession # AAB86554) was expressed as an overlapping peptide library consisting of a total of 37 peptides (Table I), each 15 amino acids (AA) in length overlapping by 10AA (offset by 5AA). OspC type K was used for the epitope mapping because it has been associated with disseminated disease (37). In addition to lacking the first 10AA, the partial sequence does not contain the final 10AA, which correspond to the commercially available OspC peptide, PepC10. Of the 37 peptides assessed, only 3 were observed to bind more than 50% of the eight serum samples used in the epitope mapping. These were peptide 1, peptide 18, and peptide 30; in addition, 3 of 5 samples that bound peptide 1 also bound peptide 2 indicating that the epitope found in peptide 1 might extended into peptide 2. Herein these peptides will be referred to as OspC1 (peptide 1 + 2, MTLFLFISCNNSGKDGNTSA), OspC18 (peptide 18, TLLAGAYTISKLITQ), and OspC30 (peptide 30, AKKAILITDAAKDKG). Serum binding was confirmed in subsequent ELISAs where the 3 peptides were incubated with an additional 30 sera from high titer Lyme disease patients (8-10 of 10 bands on western blot strip assay), and 20 negative sera from healthy individuals (Fig 1a + b). Initially, 10 Lyme disease 9
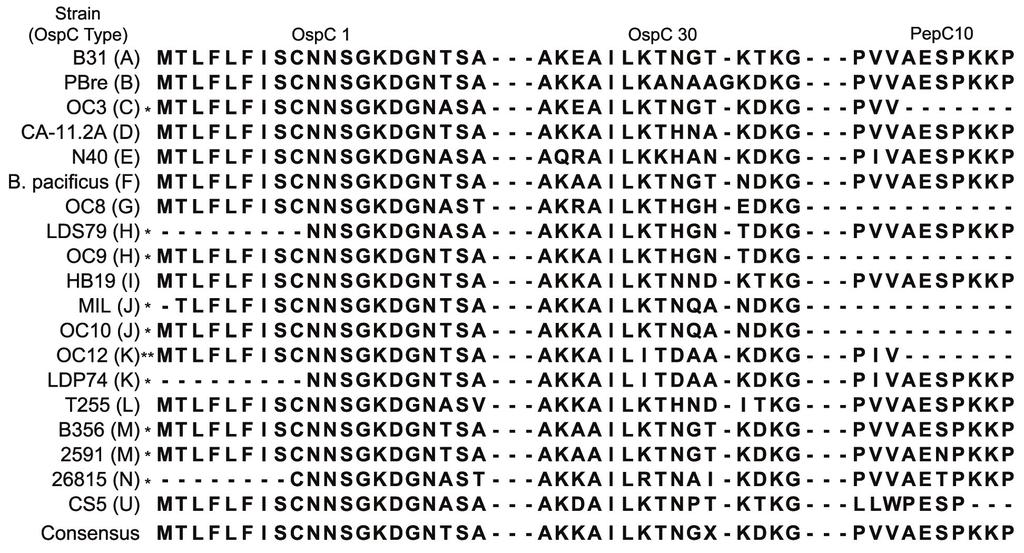
10 and 10 healthy control sera were titrated on peptide coated plates to determine an optimal dilution for further study (Fig 1a), and then peptide binding was confirmed at a single serum dilution of 1:100 (Fig 1b) using an additional 20 sera from Lyme disease patients and 10 sera from healthy controls. OspC18 bound serum antibodies from Lyme patients and normal individuals equivalently (Fig 1a +b), indicating that the epitope contained in the peptide was cross-reactive and not specific for Borrelia. OspC18 was not used in further analyses. The mean absorbance of serum antibody binding to both OspC1 and OspC30 was significantly higher in Lyme disease patients compared to normal individuals; however, OspC1 appeared to detect more individual Lyme samples than did OspC30 (Fig. 1b). A limitation in the use of OspC in a diagnostic assay is the inherent variability found within the protein. Many OspC types (allelic variants) have been described in the literature (14, 35, 36), some having been associated with a greater propensity for dissemination of the bacteria from the site of initial infection following the tick bite. While the association of OspC type and disseminated disease is beyond the scope of this study, to be effective within the constraints of a diagnostic assay, an epitope must be highly conserved. Thus, we aligned the sequences of 15 different OspC types, assessing the AA variability in the epitopes OspC1 and OspC30 and comparing it to the degree of sequence variability found within the commercially available PepC10 sequence (PVVAESPKKP). Complete single sequences were not available for OspC types C, G, H, J, K, M, and U; when possible, multiple different sequences from the same OspC type were aligned to demonstrate the presence or absence of each epitope. As demonstrated in Figure 2, the sequence for OspC1 is both present and 10
11 highly conserved in all of OspC types analyzed, being identical to the consensus sequence generated by alignment of the different OspC proteins. This is similar to PepC10 that is also highly conserved and identical to the aligned consensus sequence, though this peptide does appear to be absent in OspC type U and type J. Complete sequences containing the c-terminal portion (where PepC10 is located) of OspC type C, and type G were not available, so it is unclear if PepC10 is fully present in those types. On the other hand, OspC30 is poorly conserved among the different OspC types; the sequence identified in the epitope mapping was highly divergent from the consensus sequence generated by alignment of that position within the different OspC types. Indeed, a subsequent epitope mapping of OspC type A did not identify the analogous region for OspC 30 as an epitope (data not shown). The high degree of conservation in both OspC1 and PepC10 may be due to their placement, respectively, in the n-terminal and c-terminal portions of the protein, as the highest degree of variation among the different OspC types falls in the middle of the protein (Figure S1). OspC 30 was not used in further analyses. To assess the potential of OspC1 in a diagnostic assay for early Lyme disease, we screened the peptide against a large panel of serum obtained from patients with EM at the time of their initial diagnosis, and compared the results to those obtained with PepC10. As EM develops anywhere from 3 to 30 days after tick bite (with the average being 7 days), the level of anti-borrelia antibody within this patient population can vary greatly. Early disease is marked by elevated IgM antibodies against Borrelia. As the disease progresses, and the immune response evolves, the IgM response diminishes and is replaced with IgG. Dependent upon when a patient seeks medical attention they 11
12 may present with IgM, IgG or a mixture of both. As a result we independently assayed for IgM and IgG against OspC1 and PepC10 (Fig 3). Sera from healthy individuals collected in a non-endemic region for Lyme disease (the American southwest) were used as a negative control and to set the limits of detection. In addition, sera from patients with RA or a positive RPR test were used as negative disease controls in this assay. RA is an autoimmune inflammatory disease marked by elevated serum antibody levels and joint destruction, which can also occur in Lyme disease. The RPR test is a first-tier screening test for syphilis, an infectious disease caused by the related spirochete Treponema pallidum, and was used as a negative control for cross-reactive antibody generated by infection with a related spirochete. Serum from 48 healthy donors was used to establish the limits of detection for the ELISA. The mean absorbance for OspC1 binding of IgM (0.316 ± 0.187) and IgG (0.139 ±.051) and PepC10 binding of IgM (0.335 ± 0.187) and IgG (0.125 ± 0.101) was determined. Samples were considered positive if the mean absorbance of three replicate wells was greater than 3SD from the mean of the healthy controls, equivocal if it was between 2SD and 3SD from the mean of healthy controls, or negative if it was less than 2SD from the mean of the healthy controls. IgG bound to PepC10 in four of 48 serum samples in the healthy control population with high absorbance levels. In two of these four samples IgG binding occurred at absorbance values more than 3SD from the mean of the population. These two samples were treated as outliers, and while not removed from the analysis, they were not included in the calculation of cutoff values. All four high binding samples were not positive for IgM binding to PepC10 or binding of either isotype to OspC1, and were subsequently treated as bonafide false positives. All false positive 12
13 control samples were evaluated with commercially available Lyme disease diagnostic western blot strip tests to determine if the serum was obtained from an individual with previously undiagnosed Lyme disease. All negative controls included in this evaluation were negative for Lyme via western blot strips Positive binding of serum IgM to OspC1 was detected in almost half (47 of 97) of early Lyme disease patient sera (Figure 2a, Table II), while significantly fewer sera positive for IgG (24 of 98) were found (Figure 2b, Table II, p=0.006). This was expected, as IgM is the predominant antibody isotype found during early infection. However, some of the samples were only positive for either IgM or IgG; the total number of patient sera considered unequivocally positive (detecting either serum IgM or IgG) for Lyme disease via binding of OspC1 was greater than 60% (60 of 98, 62.9%) (Table II). If samples found to be equivocal were included in that rate, OspC1 positively detected Lyme disease more than 75% of the time (75 of 98, 76.5%, Table II, total antibody positive + equivocal). By comparison, PepC10 positively detected serum IgM antibodies in fewer early Lyme patient serum samples compared to OspC1 (40 of 97 vs. 47 of 97, respectively, no significant difference (NS)) (Table II), and also had a higher rate of false positives for IgM binding within negative disease control populations (Table II). As with OspC1, PepC10 detected significantly fewer IgG positive sera compared to IgM (16 of 98 vs. 40 of 97, respectively, p<0.001), but detected a lower number of IgG positive early Lyme patient sera compared to OspC1 (16 of 98 vs. 24 of 98, respectively, NS). Fewer total positive sera (binding either IgM or IgG) were detected by PepC10 (48 of 98, 49.0%) compared to OspC1 (60 of 98, 62.9%, Table II Total Ab, NS). This difference was also maintained when the number of equivocal samples was 13
14 included (OspC1-75 of 98, 76.5% vs. PepC10-64 of 98, 65.3%, NS). OspC1 detected a higher number of IgG false positives within the negative disease control patient population (Table II and Fig 3). However, PepC10 demonstrated more variability in serum IgG binding within the negative healthy control population compared to OspC1, (PepC10 =0.125±0.100, CV=0.80 vs. OspC1=0.139±0.049, CV=0.35, mean±sd), with the detection of 4 false positives within the normal control sera incubated with PepC10 compared to no false positives in the normal control sera incubated with OspC1 (Figure 3b). This resulted in incrementally higher cut-off values for the detection of IgG antibodies by PepC10 compared to OspC1, as a result of larger SD values (Figure 3b), which in turn resulted in lower rates of both true and false positives. Thus, counterintuitively, the higher degree of nonspecificity demonstrated by PepC10 following incubation with normal control serum resulted in the detection of fewer false positives in other negative control populations. Late Lyme disease sera were obtained from patients with Lyme disease upon first presentation with swollen joints. OspC1 positively detected IgM in 3 of 20 (15%) and IgG in 5 of 20 (25%) patients with late Lyme disease. Unlike with early Lyme disease, all unequivocally positive sera detected only IgM or IgG; thus, OspC1 detected late Lyme disease in a total of 8 of 20 samples (40%). On the other hand, PepC10 detected IgM in only 2 of 20 (10%) and IgG in only 2 of 20 (10%) samples for a total detection of Lyme disease in 4 of 20 (20%) samples The sensitivity and specificity of both peptides for identifying positive samples was determined by ROC analysis using 3SD from the mean of healthy controls as a cutoff. When comparing detection of Lyme disease in patient sera to healthy controls, 14
15 OspC1 demonstrated a specificity of % and sensitivity of 41.24% for IgM detection and a specificity of 97.92% and sensitivity of 24.92% for IgG detection. This is compared to PepC10 which demonstrated a specificity/sensitivity of % and 29.90% for IgM, and 91.67% and 17.35% for IgG, respectively. Thus, both peptides were highly specific for the detection of Lyme disease, indicating that when a positive value is returned it is highly likely that it is a true positive. When these values were recalculated comparing Lyme patient sera with all negative controls, OspC1 demonstrated a specificity/sensitivity of 98.52% and 41.24% for IgM and 92.59% and 24.49% for IgG, respectively. In comparison PepC10 demonstrated a specificity/sensitivity of 99.26% and 29.90% for IgM and 94.81% and 17.35% for IgG, respectively. Thus, with respect to both healthy and disease controls, both peptides are highly specific. However, OspC1 had a marginally higher sensitivity than PepC10 (41.24% vs % for IgM and 24.49% vs % for IgG). Overall, the area under the curve (AUC) for both peptides was similar (OspC1 IgM AUC= vs. PepC10 IgM AUC=0.7406, NS, and OspC 1 IgG AUC= vs. PepC10 IgG AUC=0.7573, NS). 15
16 315 Discussion The inefficiency of current whole-cell and whole-protein based serological assays for Lyme disease diagnosis mandates the need for improved technologies. Though erythema migrans develops in a large majority, it does not develop in all cases of Lyme disease and may be gone by the time a patient seeks medical care (9). Improved laboratory diagnostics are critical for the diagnosis of early Lyme disease in the absence of EM and other indeterminate cases. Peptide based diagnostics, where cross-reactive epitopes can be excluded, are an attractive alternative to currently available assays. The IR6 assay, based on a peptide (C6) from the 6 th conserved region of the VlsE protein of B. burgdorferi, demonstrates that a peptide target can significantly improve both sensitivity and specificity compared to whole protein/cell based assays. A recent report by Wormser, et. al. (27) provides evidence suggesting that the IR6 assay has both the specificity and sensitivity to function as a stand-alone diagnostic assay for Lyme disease. In that study, the authors compared C6 to a standard two-tier assay against a large panel of Lyme disease patient and negative control sera and found that C6 had a much higher sensitivity than the standard two-tier assay while demonstrating a near similar level of specificity. However, as the authors noted, the patient population was derived from a single hyper-endemic area; therefore it is unclear if similar results would be obtained using sera from different geographical locations. Furthermore, the individual second tier western blot utilized in the study has been demonstrated to be less sensitive than other comparable kits, suggesting that the use of a more sensitive second tier assay could alter the results. The use of a single epitope increases the likelihood of generating false-negatives, as there is only a single antibody binding site, 16
17 and a relatively small variation in the AA sequence at that site would decrease the ability of such an assay to detect infection. C6, which is more variable than originally recognized, is at risk for this limitation (19, 23, 24). Despite the recent results, it is unlikely that the current paradigm will be changed in favor of the single peptide IR6 assay. However, these results strongly support the further development of peptidebased assays. The logical solution is to create a multi-peptide assay, which would retain specificity while increasing sensitivity through the inclusion of multiple antibody binding sites (through multiple peptides), limiting the impact of sequence variability within any one epitope. An elegant analysis by Barbour, et.al. demonstrated that an effective diagnostic serological assay for the detection of early Borrelia infection would require a minimum of five distinct antigens to attain an appropriate level of both specificity and sensitivity that would be unaffected by antigenic variation (28). In the present study, we performed epitope mapping of OspC, a principal virulence factor for B. burgdorferi that is expressed at the initiation of infection, making it an ideal target for a diagnostic assay. We identified 3 potential epitopes for further analysis. Previous studies utilizing OspC as a serodiagnostic peptide for Lyme disease demonstrated substantial cross-reactivity with negative disease controls indicating the presence of cross-reactive epitopes within the protein (30, 31). PepC10 is a commercially available, conserved peptide from the c-terminal region of OspC that, when initially described, demonstrated a similar level of sensitivity and specificity with respect to healthy controls and a slightly reduced cross-reactivity to negative disease control sera compared to the whole OspC protein (30). Given the amount of previous data generated on the serodiagnostic capabilities and limitations of recombinant OspC 17
18 protein (30-34), as well as the significant sequence variability associated with the different OspC types, we instead chose to draw comparisons in our study to the more efficacious peptide, PepC10, rather than whole OspC protein. Of the three peptideepitopes identified, OspC1, a 20AA peptide from the N-terminal region of OspC, was the only peptide that was both highly conserved among the different OspC types (Figure 2) and capable of distinguishing between individual Lyme disease patient sera and healthy control sera (Figure 1 + Table II). OspC30 did bind to some Lyme patient serum samples during the initial screening process; however, as this sequence was found to be poorly conserved among the different OspC types, it was not included for further analysis because of the high likelihood that the peptide would be unable to consistently detect serum antibody in large patient populations from different geographical areas. In subsequent analyses, OspC1 was found to be highly effective at detecting the presence of IgM and/or IgG antibodies in serum obtained from patients diagnosed with early Lyme disease at the time of initial diagnosis, outperforming the commercially available peptide, PepC10 (Fig. 3 and Table II). OspC1 was also more effective at detecting late Lyme disease than PepC10 (Fig. 3 and Table II). Much of the higher observed efficacy of OspC1 compared to PepC10 lay in reduced variability among negative healthy and diseased patient controls, resulting in lower cutoff values. Indeed, ROC analysis revealed that the specificity of both peptides for the positive detection of Lyme disease was very high, though ultimately both peptides functioned similarly in the assay (comparable AUC). As expected, however, the sensitivity of both peptides was lower than desirable, highlighting the need for multi-peptide assay development (28). The observed sensitivity of OspC1 in binding IgM in our study mirrors the level of sensitivity 18
19 demonstrated for full length recombinant OspC in multiple previous studies, which was between 40 and 45% (30-33, 38). The initial study describing the efficacy of PepC10, also demonstrated that PepC10 performed at least as well as full-length recombinant OspC in the detection of Lyme antibodies (30). This indicates that OspC peptides have the capacity to function in serological assays as well as full-length protein, but with superior specificity. We assessed the ability of OspC1 and PepC10 to function in concert for the detection of Lyme disease (data not shown); however, the use of both peptides together resulted in an increased background staining in healthy control serum, which in turn lead to an increased cut-off and did not enhance the ability of the assay to identify Lyme disease compared to the individual peptides. As a target for a serological diagnostic assay, OspC1 has a number of desirable attributes: it is derived from a principal virulence factor that is required for mammalian infection, it is expressed very early in infection increasing the likelihood of an immune response being mounted against it, it is highly conserved among different OspC genotypes, and it identified a significant majority of patients with early disease. Our data suggest that OspC1 should be considered a viable candidate for testing in a multipeptide diagnostic assay. An assay containing 5 or more specific peptide antigens, derived from multiple B. burgdorferi proteins, would markedly improve upon currently available technologies in both specificity and sensitivity (28), and represent a potentially viable standalone laboratory test for all phases of Lyme disease diagnosis, especially early disease. 19
20 405 Acknowledgments: Conflict of Interest Statement: R.J.D. is a shareholder in Biopeptides, Corp. P.M.A. and M.S. have research appointments with Biopeptides, Corp. The peptides OspC1 and OspC30 are protected under U.S. provisional patent application No. 61/705,344, filed by Biopeptides, Corp., and could serve as a future source of funding. S.M.C., R.S., and J.A.I. have no conflicts. This work was supported by the National Institute of Allergy and Infectious Disease grants R44 AI and R43 AI The authors would like to thank Dr. Mary Petzke, Ph.D. for providing some of the Lyme disease patient serum samples and Dr. Fred Moy, Ph.D. for his assistance with statistical analyses. Downloaded from on July 17, 2018 by guest 20
21 416 References Stanek, G., Wormser, G.P., Gray, J., and Strle, F. (2012) Lyme borreliosis. The Lancet. 379, Steere, A.C. (2001) Lyme disease. N.Engl.J.Med. 345, Dattwyler, R.J. (2010) A commentary on the treatment of early lyme disease. Clin.Infect.Dis. 50, Coyle, P.K., and Schutzer, S.E. (2002) Neurologic aspects of Lyme disease. Med.Clin.North Am. 86, Steere, A.C., Schoen, R.T., and Taylor, E. (1987) The clinical evolution of Lyme arthritis. Ann.Intern.Med. 107, Nardelli, D.T., Callister, S.M., and Schell, R.F. (2008) Lyme arthritis: current concepts and a change in paradigm. Clin.Vaccine Immunol. 15, Halperin, J.J. (2009) Nervous system lyme disease: diagnosis and treatment. Rev.Neurol.Dis. 6, Raveche, E.S., Schutzer, S.E., Fernandes, H., Bateman, H., McCarthy, B.A., Nickell, S.P., and Cunningham, M.W. (2005) Evidence of Borrelia autoimmunity-induced component of Lyme carditis and arthritis. J.Clin.Microbiol. 43, Centers for Disease Control and Prevention (CDC) (1995) Recommendations for test performance and interpretation from the Second National Conference on Serologic Diagnosis of Lyme Disease. MMWR Morb.Mortal.Wkly.Rep. 44,
22 Aguero-Rosenfeld, M.E., Wang, G., Schwartz, I., and Wormser, G.P. (2005) Diagnosis of lyme borreliosis. Clin.Microbiol.Rev. 18, Porwancher, R. (1999) A Reanalysis of IgM Western Blot Criteria for the Diagnosis of Early Lyme Disease. Journal of Infectious Diseases. 179, Seriburi, V., Ndukwe, N., Chang, Z., Cox, M.E., and Wormser, G.P. (2012) High frequency of false positive IgM immunoblots for Borrelia burgdorferi in Clinical Practice. Clinical Microbiology and Infection. 18, Gomes-Solecki, M.J., Wormser, G.P., Persing, D.H., Berger, B.W., Glass, J.D., Yang, X., and Dattwyler, R.J. (2001) A first-tier rapid assay for the serodiagnosis of Borrelia burgdorferi infection. Arch.Intern.Med. 161, Wang, I., Dykhuizen, D.E., Qiu, W., Dunn, J.J., Bosler, E.M., and Luft, B.J. (1999) Genetic Diversity of ospc in a Local Population of Borrelia burgdorferi sensu stricto. Genetics. 151, Porwancher, R. (2003) Improving the Specificity of Recombinant Immunoassays for Lyme Disease. Journal of Clinical Microbiology. 41, Branda, J.A., Aguero-Rosenfeld, M.E., Ferraro, M.J., Johnson, B.J.B., Wormser, G.P., and Steere, A.C. (2010) 2-Tiered Antibody Testing for Early and Late Lyme Disease Using Only an Immunoglobulin G Blot with the Addition of a VlsE Band as the Second-Tier Test. Clinical Infectious Diseases. 50,
23 Branda, J.A., Linskey, K., Kim, Y.A., Steere, A.C., and Ferraro, M.J. (2011) Two- Tiered Antibody Testing for Lyme Disease With Use of 2 Enzyme Immunoassays, a Whole-Cell Sonicate Enzyme Immunoassay Followed by a VlsE C6 Peptide Enzyme Immunoassay. Clinical Infectious Diseases. 53, Barbour, A.G., and Travinsky, B. (2010) Evolution and distribution of the ospc Gene, a transferable serotype determinant of Borrelia burgdorferi. MBio. 1, e Bacon, R.M., Biggerstaff, B.J., Schriefer, M.E., Gilmore, R.D.,Jr, Philipp, M.T., Steere, A.C., Wormser, G.P., Marques, A.R., and Johnson, B.J. (2003) Serodiagnosis of Lyme disease by kinetic enzyme-linked immunosorbent assay using recombinant VlsE1 or peptide antigens of Borrelia burgdorferi compared with 2-tiered testing using whole-cell lysates. J.Infect.Dis. 187, Johnson, B.J.B., Robbins, K.E., Bailey, R.E., Cao, B., Sviat, S.L., Craven, R.B., Mayer, L.W., and Dennis, D.T. (1996) Serodiagnosis of Lyme Disease: Accuracy of a Two-Step Approach Using a Flagella-Based ELISA and Immunoblotting. Journal of Infectious Diseases. 174, Anonymous (1997) Case definitions for infectious conditions under public health surveillance. Centers for Disease Control and Prevention. MMWR Recomm Rep. 46, Nowakowski, J., Schwartz, I., Liveris, D., Wang, G., Aguero-Rosenfeld, M.E., Girao, G., McKenna, D., Nadelman, R.B., Cavaliere, L.F., Wormser, G.P., and Lyme Disease Study Group (2001) Laboratory diagnostic techniques for patients with early Lyme 23
24 disease associated with erythema migrans: a comparison of different techniques. Clin.Infect.Dis. 33, Liang, F.T., Steere, A.C., Marques, A.R., Johnson, B.J., Miller, J.N., and Philipp, M.T. (1999) Sensitive and specific serodiagnosis of Lyme disease by enzyme-linked immunosorbent assay with a peptide based on an immunodominant conserved region of Borrelia burgdorferi vlse. J.Clin.Microbiol. 37, Gomes-Solecki, M.J., Meirelles, L., Glass, J., and Dattwyler, R.J. (2007) Epitope length, genospecies dependency, and serum panel effect in the IR6 enzyme-linked immunosorbent assay for detection of antibodies to Borrelia burgdorferi. Clin.Vaccine Immunol. 14, Ohnishi, J., Schneider, B., Messer, W.B., Piesman, J., and de Silva, A.M. (2003) Genetic Variation at the vlse Locus of Borrelia burgdorferi within Ticks and Mice over the Course of a Single Transmission Cycle. Journal of Bacteriology. 185, Bykowski, T., Woodman, M.E., Cooley, A.E., Brissette, C.A., Wallich, R., Brade, V., Kraiczy, P., and Stevenson, B. (2008) Borrelia burgdorferi complement regulatoracquiring surface proteins (BbCRASPs): Expression patterns during the mammal-tick infection cycle. Int.J.Med.Microbiol. 298 Suppl 1, Wormser, G.P., Schriefer, M., Aguero-Rosenfeld, M.E., Levin, A., Steere, A.C., Nadelman, R.B., Nowakowski, J., Marques, A., Johnson, B.J.B., and Dumler, J.S. Single-tier testing with the C6 peptide ELISA kit compared with two-tier testing for Lyme disease. Diagn.Microbiol.Infect.Dis. 24
25 Barbour, A.G., Jasinskas, A., Kayala, M.A., Davies, D.H., Steere, A.C., Baldi, P., and Felgner, P.L. (2008) A genome-wide proteome array reveals a limited set of immunogens in natural infections of humans and white-footed mice with Borrelia burgdorferi. Infect.Immun. 76, Tilly, K., Krum, J.G., Bestor, A., Jewett, M.W., Grimm, D., Bueschel, D., Byram, R., Dorward, D., VanRaden, M.J., Stewart, P., and Rosa, P. (June 2006) Borrelia burgdorferi OspC Protein Required Exclusively in a Crucial Early Stage of Mammalian Infection. Infection and Immunity. 74, Mathiesen, M.J., Christiansen, M., Hansen, K., Holm, A., Åsbrink, E., and Theisen, M. (1998) Peptide-Based OspC Enzyme-Linked Immunosorbent Assay for Serodiagnosis of Lyme Borreliosis. Journal of Clinical Microbiology. 36, Panelius, J., Lahdenne, P., Heikkilla, T., Peltomaa, M., Oksi, J., and Seppala, I. (2002) Recombinant OspC from Borrelia burgdorferi sensu stricto, B. afzelii and B. garinii in the serodiagnosis of Lyme borreliosis. Journal of Medical Microbiology. 51, Magnarelli, L.A., Fikrig, E., Padula, S.J., Anderson, J.F., and Flavell, R.A. (1996) Use of recombinant antigens of Borrelia burgdorferi in serologic tests for diagnosis of lyme borreliosis. Journal of Clinical Microbiology. 34, Gerber, M.A., Shapiro, E.D., Bell, G.L., Sampieri, A., and Padula, S.J. (1995) Recombinant Outer Surface Protein C Elisa For The Diagnosis Of Early Lyme Disease. Journal of Infectious Diseases. 171,
26 Kaiser, R., and Rauer, S. (1999) Advantage of recombinant borrelial proteins for serodiagnosis of neuroborreliosis. Journal of Medical Microbiology. 48, Earnhart, C.G., and Marconi, R.T. (May 2007) OspC Phylogenetic Analyses Support the Feasibility of a Broadly Protective Polyvalent Chimeric Lyme Disease Vaccine. Clinical and Vaccine Immunology. 14, Jauris-Heipke, S., Liegl, G., Preac-Mursic, V., Rössler, D., Schwab, E., Soutschek, E., Will, G., and Wilske, B. (1995) Molecular analysis of genes encoding outer surface protein C (OspC) of Borrelia burgdorferi sensu lato: relationship to ospa genotype and evidence of lateral gene exchange of ospc. Journal of Clinical Microbiology. 33, Earnhart, C.G., Buckles, E.L., Dumler, J.S., and Marconi, R.T. (December 2005) Demonstration of OspC Type Diversity in Invasive Human Lyme Disease Isolates and Identification of Previously Uncharacterized Epitopes That Define the Specificity of the OspC Murine Antibody Response. Infection and Immunity. 73, Magnarelli, L.A., Ijdo, J.W., Padula, S.J., Flavell, R.A., and Fikrig, E. (2000) Serologic diagnosis of Lyme borreliosis by using enzyme-linked immunosorbent assays with recombinant antigens. J.Clin.Microbiol. 38,
27 537 Figure Legends: Figure 1: IgG and IgM antibodies specific for OspC peptides in serum from patients with Lyme disease. Serum from patients with Lyme disease was confirmed to be positive for anti-borrelia antibodies using commercially available western blot strips prior to incubation with OspC peptides (10μg/ml) in an ELISA. Antibody binding was detected using a polyclonal HRP-labeled goat anti-human IgG and IgM (γ and μ chain specific) antibody. Upper panels show a dose titration of Lyme disease patient sera (n=10) and healthy control serum (normal sera, n=10) on OspC-peptide coated 96-well plates. Data are reported as mean absorbance ± SD. Lower panels depict binding of serum from Lyme disease patients and healthy controls (normal sera) at a single dilution of 1:100. Data are reported as absorbance at 450nm, the line represents mean ± SD. OspC 1 (Lyme n=20, normal n=10), OspC 18 (Lyme n=20 and normal n=10), OspC 30 (Lyme n=17, normal n=10). Patient samples depicted in the upper panels are different from those used in the lower panels. *p<0.05 by Mann-Whitney test. Figure 2: Amino acid sequence alignment of different OspC types depicting the regions corresponding to OspC1, OspC 30, and PepC10. Sequences were aligned using CLC workbench and were trimmed to show only the regions corresponding to the peptides of interest. In several instances complete sequences for the OspC types containing all three peptides were not available. When possible, multiple partial sequences for that OspC type were aligned depicting the presence or absence of a particular peptide sequence. *=partial sequence. **= partial sequence used for epitope mapping. 27
28 Figure 3: Comparison of OspC1 and PepC10 in the detection of IgM and IgG antibodies in serum from patients with early Lyme disease. Serum from patients with early Lyme disease (erythema migrans+), healthy controls, patients with rheumatoid arthritis (RA), RPR+ patients, or patients with Lyme Arthritis (late Lyme disease) were incubated on OspC1 or PepC10 coated (10μg/ml) plates in an ELISA. Serum IgM (a) and IgG (b) was detected using HRP-labeled goat anti-μ or anti-γ chain antibodies, respectively. The dashed line represents 3SD from the mean of healthy controls incubated with OspC1; the dotted line represents 3SD from the mean of healthy controls incubated with PepC10. The lines overlap in a. The y-axis in b is segmented to show the data more clearly. Data are reported as absorbance at 450nm. Lyme (n=98), Normal (n=48), RA (n=48), RPR+ (n=39), Late Lyme (n=20). Downloaded from on July 17, 2018 by guest 28
29
30
31
32 Table I: Borrelia burgdorferi OC12 OspC (type K) a Peptide # Pos. in Protein Sequence Peptide Sequence Peptide # Pos. in Protein Sequence Peptide Sequence MTLFLFISCNNSGKD KLITQKLDGLKNSEK FISCNNSGKDGNTSA KLDGLKNSEKLKEKI NSGKDGNTSANSADE KNSEKLKEKIENAKK GNTSANSADESVKGP LKEKIENAKKCSEDF NSADESVKGPNLTEI ENAKKCSEDFTKKLE SVKGPNLTEISKKIT CSEDFTKKLEGEHAQ NLTEISKKITESNAV TKKLEGEHAQLGIEN SKKITESNAVVLAVK GEHAQLGIENVTDEN ESNAVVLAVKEIETL LGIENVTDENAKKAI VLAVKEIETLLASID VTDENAKKAILITDA EIETLLASIDELATK AKKAILITDAAKDKG LASIDELATKAIGKK LITDAAKDKGAAELE ELATKAIGKKIQQNG AKDKGAAELEKLFKA AIGKKIQQNGGLAVE AAELEKLFKAVENLA IQQNGGLAVEAGHNG KLFKAVENLAKAAKE GLAVEAGHNGTLLAG VENLAKAAKEMLANS AGHNGTLLAGAYTIS KAAKEMLANSVKELT TLLAGAYTISKLITQ EMLANSVKELTSPIV AYTISKLITQKLDGL a Partial Sequence; Accession #AAB86554
33 Table II: OspC1 and PepC10 serum IgM and IgG binding Lyme Healthy RA RPR+ Late Lyme e OspC1 PepC10 OspC1 PepC10 OspC1 PepC10 OspC1 PepC10 OspC1 PepC10 IgM Positive a 48.5% 41.2% 0% 0% 2.0% 12.5% 10.3% 20.5% 15% 10% (47/97) (40/97) (0/48) (0/48) (1/48) (6/48) (4/39) (8/39) (3/20) (2/20) Equivocal b 8.2% 13.4% 2% 6.2% 6.2% 2.0% 12.8% 7.7% 10% 0% (8/97) (13/97) (1/48) (3/48) (3/48) (1/48) (5/39) (3/39) (2/20) (0/20) Negative c 43.3% (42/97) IgG Positive a 24.5% (24/98) Equivocal b 16.3% (16/98) Negative c 59.2% (58/98) 45.4% (44/97) 16.3% (16/98) 11.2% (11/98) 72.5% (71/98) 98% (47/48) 2.0% (1/48) 4.2% (2/48) 93.8% (45/48) 93.8% (45/48) 8.3% (4/48) 0% (0/48) 91.7% (44/48) 91.8% (44/48) 12.5% (6/48) 6.2% (3/48) 81.3% (39/48) 85.5% (41/48) 2.0% (1/48) 4.2% (2/48) 93.8% (45/48) 76.9% (30/39) 7.7% (3/39) 17.9% (7/39) 74.4% (29/39) 71.8% (28/39) 5.1% (2/39) 0% (0/39) 94.9% (37/39) 75% (15/20) 25% (5/20) 20% (4/20) 55% (11/20) 90% (18/20) 10% (2/20) 15% (3/20) 75% (15/20) Downloaded from Total Ab d Positive a 62.1% (60/98) Equivocal b 15.3% (15/98) Negative c 23.5% (23/98) 49.0% (48/98) 16.3% (16/98) 34.7% (34/98) 2.0% (1/48) 6.3% (3/48) 92.7% (44/48) 8.3% (4/48) 6.3% (3/48) 85.4% (41/48) 14.6% (7/48) 8.3% (4/48) 77.1% (37/48) 14.6% (7/48) 6.3% (3/48) 79.1% (38/48) 15.4% (6/39) 20.5% (8/39) 64.1% (25/39) 20.5% (8/39) 7.7% (3/39) 71.8% (28/39) 40% (8/20) 20% (4/20) 40% (8/20) 20% (4/20) 15% (3/20) 65% (13/20) on July 17, 2018 by guest a -More than 3 SD from mean of healthy controls b -Between 2 SD and 3 SD from mean of healthy controls c -Less than 2 SD from the mean of the health controls d -Total number of serum samples containing either IgM or IgG antibody binding to OspC1 or PepC10 e -Late Lyme = Lyme arthritis
LU:research Institutional Repository of Lund University
 LU:research Institutional Repository of Lund University This is an author produced version of a paper published in European journal of clinical microbiology & infectious diseases: official publication
LU:research Institutional Repository of Lund University This is an author produced version of a paper published in European journal of clinical microbiology & infectious diseases: official publication
MAJOR ARTICLE. John A. Branda, 1 Katy Linskey, 1 Yeowon A. Kim, 1 Allen C. Steere, 2 and Mary Jane Ferraro 1,2
 MAJOR ARTICLE Two-Tiered Antibody Testing for Lyme Disease With Use of 2 Enzyme Immunoassays, a Whole-Cell Sonicate Enzyme Immunoassay Followed by a VlsE C6 Peptide Enzyme Immunoassay John A. Branda, 1
MAJOR ARTICLE Two-Tiered Antibody Testing for Lyme Disease With Use of 2 Enzyme Immunoassays, a Whole-Cell Sonicate Enzyme Immunoassay Followed by a VlsE C6 Peptide Enzyme Immunoassay John A. Branda, 1
STATEMENT FOR MANAGING LYME DISEASE IN NOVA SCOTIA
 INFECTIOUS DISEASES EXPERT GROUP (IDEG) DEPARTMENT OF HEALTH AND WELLNESS STATEMENT FOR MANAGING LYME DISEASE IN NOVA SCOTIA Executive Summary: In 2016, the Public Health Agency of Canada (PHAC) modified
INFECTIOUS DISEASES EXPERT GROUP (IDEG) DEPARTMENT OF HEALTH AND WELLNESS STATEMENT FOR MANAGING LYME DISEASE IN NOVA SCOTIA Executive Summary: In 2016, the Public Health Agency of Canada (PHAC) modified
Lyme Disease. Abstract Lyme disease is a vector borne infection primarily transmitted by Ixodes ticks and. Special Issue
 Special Issue Lyme Disease Min Geol Lee, M.DYoung Hun Cho, M.D. Department of Dermatology Yonsei University College of Medicine, Severance Hospital Email : mglee@yumc.yonsei.ac.krsalute@yumc.yonsei.ac.kr
Special Issue Lyme Disease Min Geol Lee, M.DYoung Hun Cho, M.D. Department of Dermatology Yonsei University College of Medicine, Severance Hospital Email : mglee@yumc.yonsei.ac.krsalute@yumc.yonsei.ac.kr
Infectious Diseases Expert Group (IDEG) Department of Health and Wellness. Statement for Managing Lyme Disease in Nova Scotia
 Department of Health and Wellness. Statement for Managing Lyme Disease in Nova Scotia") Infectious Diseases Expert Group (IDEG) Department of Health and Wellness Statement for Managing Lyme Disease in Nova Scotia 2018 Executive Summary: In 2016, the Public Health Agency of Canada (PHAC) modified
Infectious Diseases Expert Group (IDEG) Department of Health and Wellness Statement for Managing Lyme Disease in Nova Scotia 2018 Executive Summary: In 2016, the Public Health Agency of Canada (PHAC) modified
Title: Revisiting the Lyme Disease Serodiagnostic Algorithm: The Momentum Gathers
 JCM Accepted Manuscript Posted Online 13 June 2018 J. Clin. Microbiol. doi:10.1128/jcm.00749-18 Copyright 2018 American Society for Microbiology. All Rights Reserved. 1 Title: Revisiting the Lyme Disease
JCM Accepted Manuscript Posted Online 13 June 2018 J. Clin. Microbiol. doi:10.1128/jcm.00749-18 Copyright 2018 American Society for Microbiology. All Rights Reserved. 1 Title: Revisiting the Lyme Disease
Persistence of Immunoglobulin M or Immunoglobulin G Antibody Responses to Borrelia burgdorferi Years after Active Lyme Disease
 MAJOR ARTICLE Persistence of Immunoglobulin M or Immunoglobulin G Antibody Responses to Borrelia burgdorferi 10 20 Years after Active Lyme Disease Robert A. Kalish, 1 Gail McHugh, 1 John Granquist, 1 Barry
MAJOR ARTICLE Persistence of Immunoglobulin M or Immunoglobulin G Antibody Responses to Borrelia burgdorferi 10 20 Years after Active Lyme Disease Robert A. Kalish, 1 Gail McHugh, 1 John Granquist, 1 Barry
Anti-Borrelia burgdorferi Antibody Profile in Post-Lyme Disease Syndrome
 CLINICAL AND VACCINE IMMUNOLOGY, May 2011, p. 767 771 Vol. 18, No. 5 1556-6811/11/$12.00 doi:10.1128/cvi.00002-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Anti-Borrelia burgdorferi
CLINICAL AND VACCINE IMMUNOLOGY, May 2011, p. 767 771 Vol. 18, No. 5 1556-6811/11/$12.00 doi:10.1128/cvi.00002-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Anti-Borrelia burgdorferi
SUPPLEMENTARY INFORMATION. Microfluidics-based point-of-care test for serodiagnosis of Lyme Disease
 SUPPLEMENTARY INFORMATION Microfluidics-based point-of-care test for serodiagnosis of Lyme Disease Samiksha Nayak 1, Archana Sridhara 1, Rita Melo 2, Luciana Richer 3, Natalie H. Chee 1, Jiyoon Kim 1,
SUPPLEMENTARY INFORMATION Microfluidics-based point-of-care test for serodiagnosis of Lyme Disease Samiksha Nayak 1, Archana Sridhara 1, Rita Melo 2, Luciana Richer 3, Natalie H. Chee 1, Jiyoon Kim 1,
Department of Medical Microbiology, University Hospital Maastricht, Maastricht, The Netherlands
 ORIGINAL ARTICLE 10.1111/j.1469-0691.2006.01448.x Comparison of five different immunoassays for the detection of Borrelia burgdorferi IgM and IgG antibodies A. Smismans, V. J. Goossens, E. Nulens and C.
ORIGINAL ARTICLE 10.1111/j.1469-0691.2006.01448.x Comparison of five different immunoassays for the detection of Borrelia burgdorferi IgM and IgG antibodies A. Smismans, V. J. Goossens, E. Nulens and C.
Received 7 March 2002/Returned for modification 21 June 2002/Accepted 10 July 2002
 CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Nov. 2002, p. 1348 1355 Vol. 9, No. 6 1071-412X/02/$04.00 0 DOI: 10.1128/CDLI.9.6.1348 1355.2002 Copyright 2002, American Society for Microbiology. All Rights
CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Nov. 2002, p. 1348 1355 Vol. 9, No. 6 1071-412X/02/$04.00 0 DOI: 10.1128/CDLI.9.6.1348 1355.2002 Copyright 2002, American Society for Microbiology. All Rights
Prospective Study of Serologic Tests for Lyme Disease
 MAJOR ARTICLE Prospective Study of Serologic Tests for Lyme Disease Allen C. Steere, Gail McHugh, Nitin Damle, and Vijay K. Sikand Center for Immunology and Inflammatory Diseases, Division of Rheumatology,
MAJOR ARTICLE Prospective Study of Serologic Tests for Lyme Disease Allen C. Steere, Gail McHugh, Nitin Damle, and Vijay K. Sikand Center for Immunology and Inflammatory Diseases, Division of Rheumatology,
Fatigue, persistence after Lyme borreliosis 196, 197 Francisella tularensis, see Tularemia
 Subject Index Acrodermatitis chronica atrophicans (ACA) antibiotic therapy 121, 122 Borrelia induction 13 clinical characteristics 64, 65, 82 diagnosis 65, 66 differential diagnosis 66 etiology 62 frequency
Subject Index Acrodermatitis chronica atrophicans (ACA) antibiotic therapy 121, 122 Borrelia induction 13 clinical characteristics 64, 65, 82 diagnosis 65, 66 differential diagnosis 66 etiology 62 frequency
BlueBLOT-LINE Borrelia. Test Characteristics. Antibody Response
 BlueDiver Instrument IMMUNOBLOT KITS FOR DIAGNOSIS OF LYME BORRELIOSIS INFECTIOUS SEROLOGY IN NEW AUTOMATED SYSTEM FOR THE ANALYSIS AND EVALUATION OF IMMUNOBLOTS BlueDiver Instrument, Immunoblot Software
BlueDiver Instrument IMMUNOBLOT KITS FOR DIAGNOSIS OF LYME BORRELIOSIS INFECTIOUS SEROLOGY IN NEW AUTOMATED SYSTEM FOR THE ANALYSIS AND EVALUATION OF IMMUNOBLOTS BlueDiver Instrument, Immunoblot Software
Q fever. Lyme disease LDA Conference Anja Garritsen 1. Lyme Disease Diagnostics. Today s presentation
 Today s presentation Lyme Disease Diagnostics What can we use now What do we need for the future? Anja Garritsen, Innatoss Laboratories, NL Innatoss Diagnostics for Lyme Disease The present Diagnostic
Today s presentation Lyme Disease Diagnostics What can we use now What do we need for the future? Anja Garritsen, Innatoss Laboratories, NL Innatoss Diagnostics for Lyme Disease The present Diagnostic
Peter J. Weina, PhD, MD, FACP, FIDSA. Colonel, Medical Corps, US Army Deputy Commander Walter Reed Army Institute of Research
 Peter J. Weina, PhD, MD, FACP, FIDSA Colonel, Medical Corps, US Army Deputy Commander Walter Reed Army Institute of Research Background Most common vector-borne disease in U.S. First described in Lyme,
Peter J. Weina, PhD, MD, FACP, FIDSA Colonel, Medical Corps, US Army Deputy Commander Walter Reed Army Institute of Research Background Most common vector-borne disease in U.S. First described in Lyme,
1 of 12 23/11/ :25
 1 of 12 23/11/2008 09:25 And The Bands Played On - Western blot serological test for Lyme disease http://www.geocities.com/hotsprings/oasis/6455/western-blot.txt ************************************************************************
1 of 12 23/11/2008 09:25 And The Bands Played On - Western blot serological test for Lyme disease http://www.geocities.com/hotsprings/oasis/6455/western-blot.txt ************************************************************************
Biodiversity of Borrelia burgdorferi Strains in Tissues of Lyme Disease Patients
 Biodiversity of Borrelia burgdorferi Strains in Tissues of Lyme Disease Patients Dustin Brisson 1 *, Nilofer Baxamusa 2, Ira Schwartz 3, Gary P. Wormser 2 1 Biology Department, University of Pennsylvania,
Biodiversity of Borrelia burgdorferi Strains in Tissues of Lyme Disease Patients Dustin Brisson 1 *, Nilofer Baxamusa 2, Ira Schwartz 3, Gary P. Wormser 2 1 Biology Department, University of Pennsylvania,
Comparative evaluation of three different ELISA methods for the diagnosis of early culture-confirmed Lyme disease in Italy
 Journal of Medical Microbiology (2005), 54, 361 367 DOI 10.1099/jmm.0.45853-0 Comparative evaluation of three different ELISA methods for the diagnosis of early culture-confirmed Lyme disease in Italy
Journal of Medical Microbiology (2005), 54, 361 367 DOI 10.1099/jmm.0.45853-0 Comparative evaluation of three different ELISA methods for the diagnosis of early culture-confirmed Lyme disease in Italy
Interpretation Criteria for Standardized Western Blots for Three European Species of Borrelia burgdorferi Sensu Lato
 JOURNAL OF CLINICAL MICROBIOLOGY, June 1997, p. 1433 1444 Vol. 35, No. 6 0095-1137/97/$04.00 0 Copyright 1997, American Society for Microbiology Interpretation Criteria for Standardized Western Blots for
JOURNAL OF CLINICAL MICROBIOLOGY, June 1997, p. 1433 1444 Vol. 35, No. 6 0095-1137/97/$04.00 0 Copyright 1997, American Society for Microbiology Interpretation Criteria for Standardized Western Blots for
Two-Year Evaluation of Borrelia burgdorferi Culture and Supplemental Tests for Definitive Diagnosis of Lyme Disease
 JOURNAL OF CLINICAL MICROBIOLOGY, Oct. 2005, p. 5080 5084 Vol. 43, No. 10 0095-1137/05/$08.00 0 doi:10.1128/jcm.43.10.5080 5084.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved.
JOURNAL OF CLINICAL MICROBIOLOGY, Oct. 2005, p. 5080 5084 Vol. 43, No. 10 0095-1137/05/$08.00 0 doi:10.1128/jcm.43.10.5080 5084.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved.
Laboratory Diagnostics:
 Laboratory Diagnostics: Utility of Different Test Systems Klaus-Peter Hunfeld, MD, MPH Institute for Laboratory Medicine, Microbiology & Infection Control, Northwest Medical Centre, Frankfurt/Main, Germany
Laboratory Diagnostics: Utility of Different Test Systems Klaus-Peter Hunfeld, MD, MPH Institute for Laboratory Medicine, Microbiology & Infection Control, Northwest Medical Centre, Frankfurt/Main, Germany
Anti-Borrelia burgdorferi antibody profile in post-lyme disease syndrome
 CVI Accepts, published online ahead of print on 16 March 2011 Clin. Vaccine Immunol. doi:10.1128/cvi.00002-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
CVI Accepts, published online ahead of print on 16 March 2011 Clin. Vaccine Immunol. doi:10.1128/cvi.00002-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
False-negative serology in patients with neuroborreliosis and the value of employing of different borrelial strains in serological assays
 J. Med. Microbiol. Ð Vol. 49 2000), 911±915 # 2000 The Pathological Society of Great Britain and Ireland ISSN 0022-2615 IMMUNOLOGICAL RESPONSE TO INFECTION False-negative serology in patients with neuroborreliosis
J. Med. Microbiol. Ð Vol. 49 2000), 911±915 # 2000 The Pathological Society of Great Britain and Ireland ISSN 0022-2615 IMMUNOLOGICAL RESPONSE TO INFECTION False-negative serology in patients with neuroborreliosis
Animal Health Diagnostic Center. Lyme Disease Multiplex Testing for Dogs. Background on Lyme disease and Lyme diagnostics in dogs
 Animal Health Diagnostic Center Lyme Disease Multiplex Testing for Dogs Background on Lyme disease and Lyme diagnostics in dogs Lyme disease is induced by the spirochete B. burgdorferi. Spirochetes are
Animal Health Diagnostic Center Lyme Disease Multiplex Testing for Dogs Background on Lyme disease and Lyme diagnostics in dogs Lyme disease is induced by the spirochete B. burgdorferi. Spirochetes are
Update on Lyme Disease Surveillance in Wisconsin for Providers and Laboratories
 Update on Lyme Disease Surveillance in Wisconsin for Providers and Laboratories Christopher Steward Division of Public Health Wisconsin Department of Health Services 04/10/14 Protecting and promoting the
Update on Lyme Disease Surveillance in Wisconsin for Providers and Laboratories Christopher Steward Division of Public Health Wisconsin Department of Health Services 04/10/14 Protecting and promoting the
Explanation of the Lyme Disease Western Blot
 1 of 5 09/05/2008 16:30 From: BCLyme Newsgroups: sci.med.diseases.lyme Subject: Helpful info for understanding the LD Western blot test NNTP-Posting-Host: ladder05.news.aol.com X-Admin: news@aol.com Date:
1 of 5 09/05/2008 16:30 From: BCLyme Newsgroups: sci.med.diseases.lyme Subject: Helpful info for understanding the LD Western blot test NNTP-Posting-Host: ladder05.news.aol.com X-Admin: news@aol.com Date:
Received 22 November 2004/Returned for modification 14 January 2005/Accepted 17 April 2005
 JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 2005, p. 3602 3609 Vol. 43, No. 8 0095-1137/05/$08.00 0 doi:10.1128/jcm.43.8.3602 3609.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved.
JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 2005, p. 3602 3609 Vol. 43, No. 8 0095-1137/05/$08.00 0 doi:10.1128/jcm.43.8.3602 3609.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved.
ELISA Range. VIROTECH Diagnostics GmbH. Lot independent. Reagent. System. IgG-Conjugate. Substrate. IgM-Conjugate. Washing Solution.
 Quelle: www.fotolia.com ELISA Range IgG-Conjugate IgM-Conjugate IgA-Conjugate Lot independent Reagent System Stop Solution Substrate Washing Solution Serum Dilution Dilution Buffer Incubation Time Cerebrospinal
Quelle: www.fotolia.com ELISA Range IgG-Conjugate IgM-Conjugate IgA-Conjugate Lot independent Reagent System Stop Solution Substrate Washing Solution Serum Dilution Dilution Buffer Incubation Time Cerebrospinal
Corporate Medical Policy
 Corporate Medical Policy Intravenous Antibiotic Therapy for Lyme Disease File Name: intravenous_antibiotic_therapy_for_lyme_disease Origination: 3/2006 Last CAP Review: 2/2017 Next CAP Review: 2/2018 Last
Corporate Medical Policy Intravenous Antibiotic Therapy for Lyme Disease File Name: intravenous_antibiotic_therapy_for_lyme_disease Origination: 3/2006 Last CAP Review: 2/2017 Next CAP Review: 2/2018 Last
C 6 Test as an Indicator of Therapy Outcome for Patients with Localized or Disseminated Lyme Borreliosis
 JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2003, p. 4955 4960 Vol. 41, No. 11 0095-1137/03/$08.00 0 DOI: 10.1128/JCM.41.11.4955 4960.2003 Copyright 2003, American Society for Microbiology. All Rights Reserved.
JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2003, p. 4955 4960 Vol. 41, No. 11 0095-1137/03/$08.00 0 DOI: 10.1128/JCM.41.11.4955 4960.2003 Copyright 2003, American Society for Microbiology. All Rights Reserved.
Detection of Multiple Reactive Protein Species by Immunoblotting after Recombinant Outer Surface Protein A Lyme Disease Vaccination
 42 Detection of Multiple Reactive Protein Species by Immunoblotting after Recombinant Outer Surface Protein A Lyme Disease Vaccination Philip J. Molloy, 1,2 Victor P. Berardi, 2 David H. Persing, 2,3,a
42 Detection of Multiple Reactive Protein Species by Immunoblotting after Recombinant Outer Surface Protein A Lyme Disease Vaccination Philip J. Molloy, 1,2 Victor P. Berardi, 2 David H. Persing, 2,3,a
Antibody Profiling of Borrelia burgdorferi Infection in Horses
 CLINICAL AND VACCINE IMMUNOLOGY, Sept. 2011, p. 1562 1567 Vol. 18, No. 9 1556-6811/11/$12.00 doi:10.1128/cvi.05123-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Antibody Profiling
CLINICAL AND VACCINE IMMUNOLOGY, Sept. 2011, p. 1562 1567 Vol. 18, No. 9 1556-6811/11/$12.00 doi:10.1128/cvi.05123-11 Copyright 2011, American Society for Microbiology. All Rights Reserved. Antibody Profiling
NOTES. Received 4 November 2005/Returned for modification 30 December 2005/Accepted 2 February 2006
 CLINICAL AND VACCINE IMMUNOLOGY, Apr. 2006, p. 525 529 Vol. 13, No. 4 1556-6811/06/$08.00 0 doi:10.1128/cvi.13.4.525 529.2006 Copyright 2006, American Society for Microbiology. All Rights Reserved. NOTES
CLINICAL AND VACCINE IMMUNOLOGY, Apr. 2006, p. 525 529 Vol. 13, No. 4 1556-6811/06/$08.00 0 doi:10.1128/cvi.13.4.525 529.2006 Copyright 2006, American Society for Microbiology. All Rights Reserved. NOTES
Serodiagnosis of Lyme Borreliosis by Borrelia burgdorferi Sensu Stricto, B. garinii, and B. afzelii Western Blots (Immunoblots)
") JOURNAL OF CLINICAL MICROBIOLOGY, July 1996, p. 1732 1738 Vol. 34, No. 7 0095-1137/96/$04.00 0 Copyright 1996, American Society for Microbiology Serodiagnosis of Lyme Borreliosis by Borrelia burgdorferi
JOURNAL OF CLINICAL MICROBIOLOGY, July 1996, p. 1732 1738 Vol. 34, No. 7 0095-1137/96/$04.00 0 Copyright 1996, American Society for Microbiology Serodiagnosis of Lyme Borreliosis by Borrelia burgdorferi
Serodiagnosis in Early Lyme Disease
 JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1993, p. 3090-3095 Vol. 31, No. 12 0095-1137/93/123090-06$02.00/0 Copyright 0) 1993, American Society for Microbiology Serodiagnosis in Early Lyme Disease MARIA E.
JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1993, p. 3090-3095 Vol. 31, No. 12 0095-1137/93/123090-06$02.00/0 Copyright 0) 1993, American Society for Microbiology Serodiagnosis in Early Lyme Disease MARIA E.
Panel # Panel CPT Code Price 2010 AUTOIMMUNE PROFILE - BASIC 99.00
 2010 AUTOIMMUNE PROFILE - BASIC 99.00 Anti-Nuclear Antibody (ANA) 86038 33.00 Rheumatoid Factor 86431 33.00 C1Q Immune Complex 86332 33.00 2011 AUTOIMMUNE PROFILE (COMPREHENSIVE) 210.00 Anti-Nuclear Antibody
2010 AUTOIMMUNE PROFILE - BASIC 99.00 Anti-Nuclear Antibody (ANA) 86038 33.00 Rheumatoid Factor 86431 33.00 C1Q Immune Complex 86332 33.00 2011 AUTOIMMUNE PROFILE (COMPREHENSIVE) 210.00 Anti-Nuclear Antibody
Comparison of Different Strains of Borrelia burgdorferi Sensu Lato Used as Antigens in Enzyme-Linked Immunosorbent Assays
 JOURNAL OF CLINICAL MICROBIOLOGY, May 1994, p. 1154-1158 Vol. 32, No. 5 0095-1 137/94/$04.00+0 Copyright C) 1994, American Society for Microbiology Comparison of Different Strains of Borrelia burgdorferi
JOURNAL OF CLINICAL MICROBIOLOGY, May 1994, p. 1154-1158 Vol. 32, No. 5 0095-1 137/94/$04.00+0 Copyright C) 1994, American Society for Microbiology Comparison of Different Strains of Borrelia burgdorferi
Humoral Immune Responses in Patients with Lyme Neuroborreliosis
 CLINICAL AND VACCINE IMMUNOLOGY, Apr. 2010, p. 645 650 Vol. 17, No. 4 1556-6811/10/$12.00 doi:10.1128/cvi.00341-09 Copyright 2010, American Society for Microbiology. All Rights Reserved. Humoral Immune
CLINICAL AND VACCINE IMMUNOLOGY, Apr. 2010, p. 645 650 Vol. 17, No. 4 1556-6811/10/$12.00 doi:10.1128/cvi.00341-09 Copyright 2010, American Society for Microbiology. All Rights Reserved. Humoral Immune
Identifying false-positive syphilis antibody results using a semi-quantitative
 CVI Accepts, published online ahead of print on 20 April 2011 Clin. Vaccine Immunol. doi:10.1128/cvi.05066-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
CVI Accepts, published online ahead of print on 20 April 2011 Clin. Vaccine Immunol. doi:10.1128/cvi.05066-11 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
Technical Bulletin No. 121
 CPAL Central Pennsylvania Alliance Laboratory Technical Bulletin No. 121 January 31, 2014 Lyme Blot, IgG and IgM - Now Performed at CPAL Contact: J. Matthew Groeller, 717.851.1416 Operations Manager, Clinical
CPAL Central Pennsylvania Alliance Laboratory Technical Bulletin No. 121 January 31, 2014 Lyme Blot, IgG and IgM - Now Performed at CPAL Contact: J. Matthew Groeller, 717.851.1416 Operations Manager, Clinical
Immunoblot Interpretation Criteria for Serodiagnosis of Early Lyme Disease
 JOURNAL OF CLINICAL MICROBIOLOGY, Feb. 1995, p. 419 427 Vol. 33, No. 2 0095-1137/95/$04.00 0 Copyright 1995, American Society for Microbiology Immunoblot Interpretation Criteria for Serodiagnosis of Early
JOURNAL OF CLINICAL MICROBIOLOGY, Feb. 1995, p. 419 427 Vol. 33, No. 2 0095-1137/95/$04.00 0 Copyright 1995, American Society for Microbiology Immunoblot Interpretation Criteria for Serodiagnosis of Early
JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1999, p Vol. 37, No. 12. Copyright 1999, American Society for Microbiology. All Rights Reserved.
 JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1999, p. 3990 3996 Vol. 37, 12 0095-1137/99/$04.00 0 Copyright 1999, American Society for Microbiology. All Rights Reserved. Sensitive and Specific Serodiagnosis
JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1999, p. 3990 3996 Vol. 37, 12 0095-1137/99/$04.00 0 Copyright 1999, American Society for Microbiology. All Rights Reserved. Sensitive and Specific Serodiagnosis
Lyme Neuroborreliosis
 Lyme Neuroborreliosis Presenter: Elitza S. Theel, Ph.D., D(ABMM) Director of Infectious Diseases Serology Co-Director, Vector-Borne Diseases Service Line Department of Laboratory Medicine and Pathology
Lyme Neuroborreliosis Presenter: Elitza S. Theel, Ph.D., D(ABMM) Director of Infectious Diseases Serology Co-Director, Vector-Borne Diseases Service Line Department of Laboratory Medicine and Pathology
Introduction ORIGINAL ARTICLE
 Eur J Clin Microbiol Infect Dis (2017) 36:2137 2146 DOI 10.1007/s10096-017-3037-1 ORIGINAL ARTICLE Disagreement between the results from three commercial tests for the detection of Borrelia-specific serum
Eur J Clin Microbiol Infect Dis (2017) 36:2137 2146 DOI 10.1007/s10096-017-3037-1 ORIGINAL ARTICLE Disagreement between the results from three commercial tests for the detection of Borrelia-specific serum
Characterization of a Borrelia burgdorferi VlsE Invariable Region Useful in Canine Lyme Disease Serodiagnosis by Enzyme-Linked Immunosorbent Assay
 JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2000, p. 4160 4166 Vol. 38, No. 11 0095-1137/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Characterization of a Borrelia burgdorferi
JOURNAL OF CLINICAL MICROBIOLOGY, Nov. 2000, p. 4160 4166 Vol. 38, No. 11 0095-1137/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Characterization of a Borrelia burgdorferi
Serodiagnosis of Early Lyme Disease
 JOURNAL OF CLINICAL MICROBIOLOGY, July 1994, p. 1733-1738 0095-1137/94/$04.00+0 Copyright 1994, American Society for Microbiology Vol. 32, No. 7 Use of Recombinant OspC from Borrelia burgdorferi for Serodiagnosis
JOURNAL OF CLINICAL MICROBIOLOGY, July 1994, p. 1733-1738 0095-1137/94/$04.00+0 Copyright 1994, American Society for Microbiology Vol. 32, No. 7 Use of Recombinant OspC from Borrelia burgdorferi for Serodiagnosis
Received 12 August 1996/Returned for modification 15 October 1996/Accepted 4 November 1996
 JOURNAL OF CLINICAL MICROBIOLOGY, Mar. 1997, p. 537 543 Vol. 35, No. 3 0095-1137/97/$04.00 0 Copyright 1997, American Society for Microbiology Interlaboratory Comparison of Test Results for Detection of
JOURNAL OF CLINICAL MICROBIOLOGY, Mar. 1997, p. 537 543 Vol. 35, No. 3 0095-1137/97/$04.00 0 Copyright 1997, American Society for Microbiology Interlaboratory Comparison of Test Results for Detection of
Clinical and Laboratory Investigations. Dermatology 2008;216: DOI: /
 Clinical and Laboratory Investigations DOI: 10.1159/000111505 Received: March 5, 2007 Accepted: June 28, 2007 Immunoblot Analysis of the Seroreactivity to Recombinant Borrelia burgdorferi sensu lato Antigens,
Clinical and Laboratory Investigations DOI: 10.1159/000111505 Received: March 5, 2007 Accepted: June 28, 2007 Immunoblot Analysis of the Seroreactivity to Recombinant Borrelia burgdorferi sensu lato Antigens,
Evaluation of two commercially available rapid diagnostic tests for Lyme borreliosis
 DOI 10.1007/s10096-014-2217-5 ARTICLE Evaluation of two commercially available rapid diagnostic tests for Lyme borreliosis P. W. Smit & S. Kurkela & M. Kuusi & O. Vapalahti Received: 26 June 2014 /Accepted:
DOI 10.1007/s10096-014-2217-5 ARTICLE Evaluation of two commercially available rapid diagnostic tests for Lyme borreliosis P. W. Smit & S. Kurkela & M. Kuusi & O. Vapalahti Received: 26 June 2014 /Accepted:
Viramed Biotech AG Borrelia B31 IgG ViraStripe
 - 1 - Viramed Biotech AG Borrelia B31 IgG ViraStripe A line blot serologic assay for the detection of IgG-specific antibodies against Borrelia burgdorferi in human serum The Borrelia B31 IgG ViraStripe
- 1 - Viramed Biotech AG Borrelia B31 IgG ViraStripe A line blot serologic assay for the detection of IgG-specific antibodies against Borrelia burgdorferi in human serum The Borrelia B31 IgG ViraStripe
A European Multicenter Study of Immunoblotting in Serodiagnosis of Lyme Borreliosis
 JOURNAL OF CLINICAL MICROBIOLOGY, June 2000, p. 2097 2102 Vol. 38, No. 6 0095-1137/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. A European Multicenter Study of Immunoblotting
JOURNAL OF CLINICAL MICROBIOLOGY, June 2000, p. 2097 2102 Vol. 38, No. 6 0095-1137/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. A European Multicenter Study of Immunoblotting
Borrelia B31 ViraChip IgG Test Kit
 Borrelia B31 ViraChip IgG Test Kit Intended Use: The Viramed Biotech AG Borrelia B31 ViraChip IgG Test Kit is an in vitro qualitative protein microarray assay for the detection of IgG antibodies to Borrelia
Borrelia B31 ViraChip IgG Test Kit Intended Use: The Viramed Biotech AG Borrelia B31 ViraChip IgG Test Kit is an in vitro qualitative protein microarray assay for the detection of IgG antibodies to Borrelia
Received 23 November 1998/Returned for modification 8 March 1999/Accepted 6 April 1999
 JOURNAL OF CLINICAL MICROBIOLOGY, July 1999, p. 2241 2247 Vol. 37, No. 7 0095-1137/99/$04.00 0 Copyright 1999, American Society for Microbiology. All Rights Reserved. Validity of Interpretation Criteria
JOURNAL OF CLINICAL MICROBIOLOGY, July 1999, p. 2241 2247 Vol. 37, No. 7 0095-1137/99/$04.00 0 Copyright 1999, American Society for Microbiology. All Rights Reserved. Validity of Interpretation Criteria
Treponema-Specific Tests for Serodiagnosis of Syphilis: Comparative Evaluation of Seven Assays
 JOURNAL OF CLINICAL MICROBIOLOGY, Apr. 2011, p. 1313 1317 Vol. 49, No. 4 0095-1137/11/$12.00 doi:10.1128/jcm.02555-10 Copyright 2011, American Society for Microbiology. All Rights Reserved. Treponema-Specific
JOURNAL OF CLINICAL MICROBIOLOGY, Apr. 2011, p. 1313 1317 Vol. 49, No. 4 0095-1137/11/$12.00 doi:10.1128/jcm.02555-10 Copyright 2011, American Society for Microbiology. All Rights Reserved. Treponema-Specific
BBK07, a Dominant In Vivo Antigen of Borrelia burgdorferi, Is a Potential Marker for Serodiagnosis of Lyme Disease
 CLINICAL AND VACCINE IMMUNOLOGY, Nov. 2009, p. 1569 1575 Vol. 16, No. 11 1556-6811/09/$12.00 doi:10.1128/cvi.00301-09 Copyright 2009, American Society for Microbiology. All Rights Reserved. BBK07, a Dominant
CLINICAL AND VACCINE IMMUNOLOGY, Nov. 2009, p. 1569 1575 Vol. 16, No. 11 1556-6811/09/$12.00 doi:10.1128/cvi.00301-09 Copyright 2009, American Society for Microbiology. All Rights Reserved. BBK07, a Dominant
Lyme disease Overview
 Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 21 Lyme Disease Learning Objectives 1. Describe the agent and vector of Lyme Disease 2. Identify the geographic and temporal patterns
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 21 Lyme Disease Learning Objectives 1. Describe the agent and vector of Lyme Disease 2. Identify the geographic and temporal patterns
Lyme Disease. By Farrah Jangda
 Lyme Disease By Farrah Jangda Disease Name: Lyme Disease Lyme disease is a common tick-borne bacterial infection transmitted from the bite of a tick in United States and Europe (2). It is caused by the
Lyme Disease By Farrah Jangda Disease Name: Lyme Disease Lyme disease is a common tick-borne bacterial infection transmitted from the bite of a tick in United States and Europe (2). It is caused by the
Lyme disease Overview
 Infectious Disease Epidemiology BMTRY 713 (A. Selassie, Dr.PH) Lecture 22 Lyme Disease Learning Objectives 1. Describe the agent and vector of Lyme Disease 2. Identify the geographic and temporal patterns
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, Dr.PH) Lecture 22 Lyme Disease Learning Objectives 1. Describe the agent and vector of Lyme Disease 2. Identify the geographic and temporal patterns
Seroprevalence of Babesia microti in Individuals with Lyme Disease. Sabino R. Curcio, M.S, MLS(ASCP)
") Seroprevalence of Babesia microti in Individuals with Lyme Disease Sabino R. Curcio, M.S, MLS(ASCP) Lyme Disease Most common vectorborne illness in the United States Caused by the tick-transmitted spirochete
Seroprevalence of Babesia microti in Individuals with Lyme Disease Sabino R. Curcio, M.S, MLS(ASCP) Lyme Disease Most common vectorborne illness in the United States Caused by the tick-transmitted spirochete
MP Intravenous Antibiotic Therapy and Associated Diagnostic Testing for Lyme Disease. Related Policies None
 Medical Policy BCBSA Ref. Policy: 5.01.08 Last Review: 10/18/2018 Effective Date: 10/18/2018 Section: Prescription Drug Related Policies None DISCLAIMER Our medical policies are designed for informational
Medical Policy BCBSA Ref. Policy: 5.01.08 Last Review: 10/18/2018 Effective Date: 10/18/2018 Section: Prescription Drug Related Policies None DISCLAIMER Our medical policies are designed for informational
Intravenous Antibiotic Therapy and Associated Diagnostic Testing for Lyme Disease
 Intravenous Antibiotic Therapy and Associated Diagnostic Testing for Lyme Disease Policy Number: 5.01.08 Last Review: 01/2018 Origination: 1/2009 Next Review: 01/2019 Policy Blue Cross and Blue Shield
Intravenous Antibiotic Therapy and Associated Diagnostic Testing for Lyme Disease Policy Number: 5.01.08 Last Review: 01/2018 Origination: 1/2009 Next Review: 01/2019 Policy Blue Cross and Blue Shield
Reinfection in Patients with Lyme Disease
 CLINICAL PRACTICE Ellie J. C. Goldstein, Section Editor INVITED ARTICLE Reinfection in Patients with Lyme Disease Robert B. Nadelman and Gary P. Wormser Division of Infectious Diseases, Department of Medicine,
CLINICAL PRACTICE Ellie J. C. Goldstein, Section Editor INVITED ARTICLE Reinfection in Patients with Lyme Disease Robert B. Nadelman and Gary P. Wormser Division of Infectious Diseases, Department of Medicine,
LYME DISEASE Last revised May 30, 2012
 Wisconsin Department of Health Services Division of Public Health Communicable Disease Surveillance Guideline LYME DISEASE Last revised May 30, 2012 I. IDENTIFICATION A. CLINICAL DESCRIPTION: A multi-systemic
Wisconsin Department of Health Services Division of Public Health Communicable Disease Surveillance Guideline LYME DISEASE Last revised May 30, 2012 I. IDENTIFICATION A. CLINICAL DESCRIPTION: A multi-systemic
A bs tr ac t. n engl j med 367;20 nejm.org november 15,
 The new england journal of medicine established in 1812 november 15, 2012 vol. 367 no. 20 Differentiation of Reinfection from Relapse in Recurrent Lyme Disease Robert B. Nadelman, M.D., Klára Hanincová,
The new england journal of medicine established in 1812 november 15, 2012 vol. 367 no. 20 Differentiation of Reinfection from Relapse in Recurrent Lyme Disease Robert B. Nadelman, M.D., Klára Hanincová,
JOURNAL OF CLINICAL MICROBIOLOGY, Apr. 2000, p Vol. 38, No. 4. Copyright 2000, American Society for Microbiology. All Rights Reserved.
 JOURNAL OF CLINICAL MICROBIOLOGY, Apr. 2000, p. 1569 1574 Vol. 38, No. 4 0095-1137/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Borrelia burgdorferi B31 Erp Proteins
JOURNAL OF CLINICAL MICROBIOLOGY, Apr. 2000, p. 1569 1574 Vol. 38, No. 4 0095-1137/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Borrelia burgdorferi B31 Erp Proteins
Supplementary Figure 1. ALVAC-protein vaccines and macaque immunization. (A) Maximum likelihood
 Maximum likelihood") Supplementary Figure 1. ALVAC-protein vaccines and macaque immunization. (A) Maximum likelihood tree illustrating CRF01_AE gp120 protein sequence relationships between 107 Envs sampled in the RV144 trial
Supplementary Figure 1. ALVAC-protein vaccines and macaque immunization. (A) Maximum likelihood tree illustrating CRF01_AE gp120 protein sequence relationships between 107 Envs sampled in the RV144 trial
b Ospea ale Ciuile di Gemona, Gemona, Italy
 ELSEVIER FEMS Immunology and Medical Microbiology 14 (1996) 159-166 /f~d~blf~ogy MICROBIOLOGY AND Abstract IgM and IgG significant reactivity to Borrelia burgdorferi sense stricto, Borrelia garinii and
ELSEVIER FEMS Immunology and Medical Microbiology 14 (1996) 159-166 /f~d~blf~ogy MICROBIOLOGY AND Abstract IgM and IgG significant reactivity to Borrelia burgdorferi sense stricto, Borrelia garinii and
Infectious Diseases (S.K. Morris), and Division of Microbiology (S.E.Richardson),
, and Division of Microbiology (S.E.Richardson),") JCM Accepts, published online ahead of print on 10 November 2010 J. Clin. Microbiol. doi:10.1128/jcm.01584-10 Copyright 2010, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 10 November 2010 J. Clin. Microbiol. doi:10.1128/jcm.01584-10 Copyright 2010, American Society for Microbiology and/or the Listed Authors/Institutions. All
Lyme Disease Surveillance in Wisconsin Christopher Steward Division of Public Health Wisconsin Department of Health Services 04/10/2014
 Lyme Disease Surveillance in Wisconsin Christopher Steward Division of Public Health Wisconsin Department of Health Services 04/10/2014 Protecting and promoting the health and safety of the people of Wisconsin
Lyme Disease Surveillance in Wisconsin Christopher Steward Division of Public Health Wisconsin Department of Health Services 04/10/2014 Protecting and promoting the health and safety of the people of Wisconsin
A Study of the Technique of Western Blot for Diagnosis of Lyme Disease caused by Borrelia afzelii in China *
 190 Biomed Environ Sci, 2013; 26(3): 190 200 Original Article A Study of the Technique of Western Blot for Diagnosis of Lyme Disease caused by Borrelia afzelii in China * LIU Zhi Yun 1,2,3,+, HAO Qin 1,+,
190 Biomed Environ Sci, 2013; 26(3): 190 200 Original Article A Study of the Technique of Western Blot for Diagnosis of Lyme Disease caused by Borrelia afzelii in China * LIU Zhi Yun 1,2,3,+, HAO Qin 1,+,
TERO HEIKKILÄ. Pediatric Graduate School, Hospital for Children and Adolescents, University of Helsinki, Helsinki, Finland. and
 1(:$17,*(16 )257+(6(52/2*
1(:$17,*(16 )257+(6(52/2*
Diagnostic and Biological Significance of Anti-p41 IgM Antibodies against Borrelia burgdorferi
 Scand. J. Immunol. 53, 416±421, 2001 Diagnostic and Biological Significance of Anti-p41 IgM Antibodies against Borrelia burgdorferi E. ULVESTAD,* A. KANESTRéM,* L. J. SéNSTEBY,* R. JUREEN,* T. OMLAND,*
Scand. J. Immunol. 53, 416±421, 2001 Diagnostic and Biological Significance of Anti-p41 IgM Antibodies against Borrelia burgdorferi E. ULVESTAD,* A. KANESTRéM,* L. J. SéNSTEBY,* R. JUREEN,* T. OMLAND,*
Lyme disease stakeholder scoping workshop
 1.1 Who is the focus: Groups that will be covered: Adults and children with a suspected or confirmed diagnosis of Lyme disease 1.2. Settings All setting where NHS care The group suggested that the following
1.1 Who is the focus: Groups that will be covered: Adults and children with a suspected or confirmed diagnosis of Lyme disease 1.2. Settings All setting where NHS care The group suggested that the following
There is no Lyme Disease in Ireland?
 Dear Sirs, Registered Charity: 19588 "Encouraging awareness, prevention & treatment of Lyme Disease (Borreliosis) in Ireland." There is no Lyme Disease in Ireland? I am writing to you with sincere concerns
Dear Sirs, Registered Charity: 19588 "Encouraging awareness, prevention & treatment of Lyme Disease (Borreliosis) in Ireland." There is no Lyme Disease in Ireland? I am writing to you with sincere concerns
Diagnosis of Lyme Borreliosis
 CLINICAL MICROBIOLOGY REVIEWS, July 2005, p. 484 509 Vol. 18, No. 3 0893-8512/05/$08.00 0 doi:10.1128/cmr.18.3.484 509.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved. Diagnosis
CLINICAL MICROBIOLOGY REVIEWS, July 2005, p. 484 509 Vol. 18, No. 3 0893-8512/05/$08.00 0 doi:10.1128/cmr.18.3.484 509.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved. Diagnosis
Public health impact of strain specific immunity to Borrelia burgdorferi
 Khatchikian et al. BMC Infectious Diseases (2015) 15:472 DOI 10.1186/s12879-015-1190-7 RESEARCH ARTICLE Public health impact of strain specific immunity to Borrelia burgdorferi Camilo E. Khatchikian 1*,
Khatchikian et al. BMC Infectious Diseases (2015) 15:472 DOI 10.1186/s12879-015-1190-7 RESEARCH ARTICLE Public health impact of strain specific immunity to Borrelia burgdorferi Camilo E. Khatchikian 1*,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Intravenous Antibiotic Therapy and Associated Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Intravenous Antibiotic Therapy and Associated Professional
Intravenous Antibiotic Therapy and Associated Page 1 of 18 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Intravenous Antibiotic Therapy and Associated Professional
Treponemal-Specific Tests for the Serodiagnosis of Syphilis: A Comparative Evaluation of Seven Assays
 JCM Accepts, published online ahead of print on 23 February 2011 J. Clin. Microbiol. doi:10.1128/jcm.02555-10 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
JCM Accepts, published online ahead of print on 23 February 2011 J. Clin. Microbiol. doi:10.1128/jcm.02555-10 Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All
Supporting Information Table of Contents
 Supporting Information Table of Contents Supporting Information Figure 1 Page 2 Supporting Information Figure 2 Page 4 Supporting Information Figure 3 Page 5 Supporting Information Figure 4 Page 6 Supporting
Supporting Information Table of Contents Supporting Information Figure 1 Page 2 Supporting Information Figure 2 Page 4 Supporting Information Figure 3 Page 5 Supporting Information Figure 4 Page 6 Supporting
High sensitivity and specificity of the C6-peptide ELISA on cerebrospinal fluid in Lyme neuroborreliosis patients
 ORIGINAL ARTICLE BACTERIOLOGY High sensitivity and specificity of the C6-peptide ELISA on cerebrospinal fluid in Lyme neuroborreliosis patients N. D. van Burgel 1, A. Brandenburg 2, H. J. Gerritsen 1,
ORIGINAL ARTICLE BACTERIOLOGY High sensitivity and specificity of the C6-peptide ELISA on cerebrospinal fluid in Lyme neuroborreliosis patients N. D. van Burgel 1, A. Brandenburg 2, H. J. Gerritsen 1,
Two Standards of Care
 Two Standards of Care ILADS and IDSA guidelines reflect deeply divided opinions about treatment approaches, clinical judgment and patient preferences By Lorraine Johnson, JD, MBA Medically recognized standards
Two Standards of Care ILADS and IDSA guidelines reflect deeply divided opinions about treatment approaches, clinical judgment and patient preferences By Lorraine Johnson, JD, MBA Medically recognized standards
Received 26 January 1995/Returned for modification 10 May 1995/Accepted 8 June 1995
 JOURNAL OF CLINICAL MICROBIOLOGY, Sept. 1995, p. 2260 2264 Vol. 33, No. 9 0095-1137/95/$04.00 0 Copyright 1995, American Society for Microbiology Antibodies against Whole Sonicated Borrelia burgdorferi
JOURNAL OF CLINICAL MICROBIOLOGY, Sept. 1995, p. 2260 2264 Vol. 33, No. 9 0095-1137/95/$04.00 0 Copyright 1995, American Society for Microbiology Antibodies against Whole Sonicated Borrelia burgdorferi
Antibodies to Borrelia burgdorferi OspA, OspC, OspF and C6 antigens as markers for early
 CVI Accepts, published online ahead of print on 15 February 2012 Clin. Vaccine Immunol. doi:10.1128/cvi.05653-11 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Antibodies to
CVI Accepts, published online ahead of print on 15 February 2012 Clin. Vaccine Immunol. doi:10.1128/cvi.05653-11 Copyright 2012, American Society for Microbiology. All Rights Reserved. 1 2 Antibodies to
PE1662/E Lyme Disease Action submission of 27 October 2017
 PE1662/E Lyme Disease Action submission of 27 October 2017 We support the petitioners calls for action to improve the position with regard to awareness, diagnosis and treatment of Lyme disease. We would
PE1662/E Lyme Disease Action submission of 27 October 2017 We support the petitioners calls for action to improve the position with regard to awareness, diagnosis and treatment of Lyme disease. We would
Bordetella pertussis igg-pt elisa Kit
 Bordetella pertussis IgG-PT ELISA Kit Application Bordetella pertussis IgG-PT ELISA Kit is a quantitative test for the detection of IgG antibodies against pertussis toxin in human serum samples. Background
Bordetella pertussis IgG-PT ELISA Kit Application Bordetella pertussis IgG-PT ELISA Kit is a quantitative test for the detection of IgG antibodies against pertussis toxin in human serum samples. Background
Mouse Anti-OVA IgM Antibody Assay Kit
 Mouse Anti-OVA IgM Antibody Assay Kit Catalog # 3017 For Research Use Only - Not Human or Therapeutic Use INTRODUCTION Ovalbumin (OVA) is a widely used antigen for inducing allergic reactions in experimental
Mouse Anti-OVA IgM Antibody Assay Kit Catalog # 3017 For Research Use Only - Not Human or Therapeutic Use INTRODUCTION Ovalbumin (OVA) is a widely used antigen for inducing allergic reactions in experimental
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Feder HM Jr, Johnson BJB, O Connell S, et al. A critical appraisal
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Feder HM Jr, Johnson BJB, O Connell S, et al. A critical appraisal
SUPPLEMENTARY MATERIALS
 SUPPLEMENTARY MATERIALS Supplementary Table 1. Demographic and clinical characteristics of the primary Sjögren's syndrome patient cohort Number % Females/males 73/5 93.6/6.4 Age, median (range) years 65
SUPPLEMENTARY MATERIALS Supplementary Table 1. Demographic and clinical characteristics of the primary Sjögren's syndrome patient cohort Number % Females/males 73/5 93.6/6.4 Age, median (range) years 65
Treponema pallidum IgM ELISA Kit
 Treponema pallidum IgM ELISA Kit Catalog Number KA0969 96 assays Version: 03 Intended for research use only www.abnova.com Table of Contents Introduction... 3 Intended Use... 3 Background... 3 Principle
Treponema pallidum IgM ELISA Kit Catalog Number KA0969 96 assays Version: 03 Intended for research use only www.abnova.com Table of Contents Introduction... 3 Intended Use... 3 Background... 3 Principle
disease, laboratory confirmation is required to avoid both under- and overdiagnosis.
 Accuracy of Clinician Suspicion of Lyme Disease in the Emergency Department Lise E. Nigrovic, MD, MPH, a Jonathan E. Bennett, MD, b Fran Balamuth, MD, PhD, c Michael N. Levas, MD, d Rachel L. Chenard,
Accuracy of Clinician Suspicion of Lyme Disease in the Emergency Department Lise E. Nigrovic, MD, MPH, a Jonathan E. Bennett, MD, b Fran Balamuth, MD, PhD, c Michael N. Levas, MD, d Rachel L. Chenard,
Lyme Disease IgM Cat # Z For in vitro diagnostic use
 DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
See external label 96 tests HSV 2 IgA. Cat #
 DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite D/E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite D/E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
The Borrelial Fibronectin-Binding Protein RevA Is an Early Antigen of Human Lyme Disease
 CLINICAL AND VACCINE IMMUNOLOGY, Feb. 2010, p. 274 280 Vol. 17, No. 2 1556-6811/10/$12.00 doi:10.1128/cvi.00437-09 Copyright 2010, American Society for Microbiology. All Rights Reserved. The Borrelial
CLINICAL AND VACCINE IMMUNOLOGY, Feb. 2010, p. 274 280 Vol. 17, No. 2 1556-6811/10/$12.00 doi:10.1128/cvi.00437-09 Copyright 2010, American Society for Microbiology. All Rights Reserved. The Borrelial