Mycobacteriology William H. Benjamin, Jr.
|
|
|
- Loraine Scott
- 5 years ago
- Views:
Transcription
 Mycolic acids (C78-91) Waxes Obligate aerobes Slow growing days to weeks to form colonies 18 hour doubling time")
1 Mycobacteriology William H. Benjamin, Jr. William H. Benjamin, PhD Department of Pathology UAB 1 Mycobacteria sp. Acid Fast Bacilli (AFB) Mycolic acids (C78-91) Waxes Obligate aerobes Slow growing days to weeks to form colonies 18 hour doubling time for M. tuberculosis 2 1

2 Identification of Acid Fast Bacilli Mycobacterium sp. - are identified by the acid fast stain Mycobacteria predate animal life 100 named Mycobacterial species More than 40 have infected humans AIDS other immunocompromised 3 4 2
3 Obligate Pathogenic Mycobacteria Mycobacterium tuberculosis First bacteria shown to cause disease 1882 Koch s postulates M. leprae causes Hansen s disease or leprosy 5 Mycobacterium tuberculosis Humans are the only natural host 1/3 of the world population is infected 9.2 million cases of tuberculosis/year disease 1.7 million deaths caused by tuberculosis/year 6 3
4 Prehistory of Tuberculosis 17,000 BPE (before present era) bison in Wyoming USA IS6110 and Spoligotype confirmed M. tuberculosis 10,000 BPE in Germany skeletal evidence BPE Egypt Potts disease PCR positive for Mtb sequence 1300 BPE 8 year old Inca boy Pott s disease, AFB smear positive, IS6110 PCR positive 7 8 4
5 Tuberculosis in the United States 30,000 Cases Deaths 25,000 20,000 15,000 13,299 10,000 5, U. S. Tuberculosis Cases 20,000 18,000 16,000 14,000 12,000 10,000 8,000 6,000 4,000 2,000 0 U. S. Born Foreign Born

6 Alabama Tuberculosis Cases

7 Examples of high prevalence countries Namibia Zambia US Population (million) Tuberculosis cases 16,156 78,000 13,676 Tuberculosis rate/100, Tuberculosis death rate 61? Transmission of Tuberculosis Transmission is by infectious droplet droplet diameter 1-5 µm droplet contains 1-3 bacilli droplets settle 9 mm/min in still air infectious dose is infectious droplets average patient exhales 1.25 infectious droplets/hour some cases produce infectious droplets/hour 7
8 Exposure close contact No infection >50% Infection 50% Primary active TB 5% Latent TB 95% Never reactivate 90% Reactivation TB 5% lifetime HIV+ 5-10% per year 15 Tuberculosis Risk Factors AIDS - CD 4 < 400 Iatrogenic immunosuppression - corticosteroids Age young old Alcoholism/malnourishment Diabetes Genetics 8
9 Mantoux skin test mm of induration 17 Significant Induration on Mantoux 15 mm Always indicates infection 10 mm population at risk low income, minority races, IV drug users foreign born - from high prevalence countries Institution populations - prisons, nursing homes, mental institutions silicosis, diabetes mellitus, malignancies, immunosuppressive agents 5 mm Early, immunosuppressed HIV positive or HIV risk factors HIV status unknown Chest film consistent with old nonreactive tuberculosis Recent close contact with infectious tuberculosis case 18 9

 Miliary tuberculosis Cold abscess")
 Types of Disease caused")
10 Types of Tuberculous disease Childhood tuberculosis Adult or reactivation disease Acute tuberculous pneumonia (AIDS) Miliary tuberculosis Cold abscess Addison s disease (Adrenal insufficiency) Types of Disease caused by M. tuberculosis 20 10
11 M. tuberculosis infection without disease Inhalation of infectious droplet Hilar and peribronchiolar lymph nodes 4-6 weeks Lymphohematogenous dissemination 6-8 weeks Tubercle formation Granulomatous inflammation: caseous necrosis Dystrophic calcification (Ghon complex) Diagnosis of Tuberculosis AFB smear Tuberculin skin test (Mantoux test) Chest radiograph AFB culture 11
 Causes positive skin test Used in much of the world, except US M.")
12 Tuberculosis prevention Environmental - decrease exposure Avoid crowded conditions Air changes UV irradiation Chemoprophylaxis after positive skin test INH - after Tuberculin skin test conversion 6 months of daily oral INH BCG vaccine (Bacille-Calmette-Guerin) Causes positive skin test Used in much of the world, except US M. tuberculosis direct smear 24 12
13 Environmental Resistance of M. tuberculosis Survives drying Susceptible to UV irradiation (2 hours in sunlight) Resistant to many disinfectants susceptible to chlorine and phenols Pasteurization kills (62 o C 30 min or 71.7 o C 15 sec) HEPA filters 25 Germicidal Ultraviolet Light UV light at 254 nm is effective in killing infectious agents In air ducts In upper room irradiation Also used in biological safety cabinets Demonstration of effectiveness of killing M. tuberculosis on Middlebrook 7H11 plate 26 13
 1990 2848 126 (4.4%) 24 (0.8%) 1991 2931 120 (4.1%) 23 (0.8%) 1992 3226 145 (4.5%) 35 (1.1%) 1993 3418 177 (5.2%) 39 (1.1%) 1994 4330 259 (5.9%) 89 (2.")
 2000 4932 278 (5.6%) 99 (2.0%) 2001 5609 271 (4.8%) 69 (1.2%) 2002 5228 223 (4.2%) 50 (1%) 2003 4626 275 (5.9%) 57 (1.2%) 2004 4025 252 (6.2%) 29 (0.7%) 2005 3972 230 5.")
14 UV Exposed Culture Plate 0 min 1 min 27 AFB Cultures at UAB total Positive Positive cultures cultures for Mtb (3.0%) 42 (1.6%) (2.8%) 23 (0.9%) (4.4%) 24 (0.8%) (4.1%) 23 (0.8%) (4.5%) 35 (1.1%) (5.2%) 39 (1.1%) (5.9%) 89 (2.1%) (5.3%) 98 (2.4%) (5.6%) 82 (2.1%) (7.0%) 114 (2.7%) (5.6%) 77 (1.5%) (5.1%) 73 (1.5%) (5.6%) 99 (2.0%) (4.8%) 69 (1.2%) (4.2%) 50 (1%) (5.9%) 57 (1.2%) (6.2%) 29 (0.7%) %) 31 (0.8% (5.2%) 38 (0.8%) 28 14
15 Diagnostic M. tuberculosis Cultures Patients Days to growth Days to Identification AFB positive Respiratory Positive AFB M. tuberculosis /28 60% 17/35 48% 20/28 71% 20/31 65% 14/20 70% 14/34 41% 12/15 80% 12/28 43% 7/12 58% 7/29 24% 5/7 71% 5/22 23% 6/11 55% 6/18 33% 29 Number of Patients Each Species of Mycobacteria Were Isolated from at UAB 1990 to 2007 M. avium cx M. tuberculosis M. fortuitum M. kansasii M. abscessus Rapid pigmented M. xenopi M. lentiflavum M. marinum M. scrofulaceum M. mucogenicum M. szulgai M. gastri M. brumae M. triplex M. austroafricanum M. smegmatis M. flavescens M. haemophilum M. thermoresistable M. peregrinum M. simiae

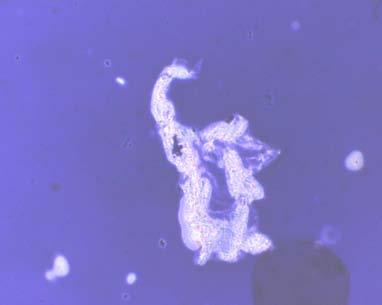
16 M. tuberculosis concentrated smear 31 Microbiological Diagnosis of Tuberculosis Digestion - mucolytic agents Decontamination Concentration Acid fast Stain Cultivation of Mycobacteria solid media liquid culture Anti-Mycobacterial susceptibilities 32 16
 2% NaOH 1% oxalic acid Centrifuge 3000 x g for 30 min.")
17 33 Decontamination and Concentration of AFB Cultures Mucolytic agent (N-acetyl-L-cysteine) 2% NaOH 1% oxalic acid Centrifuge 3000 x g for 30 min
 Liquid media - 8 to 14 days to detection BACTEC 460 ( 14 CO 2 release")
 35 Colony Morphology of M. gordonae and M.")
18 Mycobacteria Culture Media Solid media days to detection Loewenstein-Jensen (egg based) Middlebrook 7H11 (agar based) Liquid media - 8 to 14 days to detection BACTEC 460 ( 14 CO 2 release from 14 C palmitic acid) MB/BacT (CO 2 production) ESP (O 2 utilization - pressure change) MIDGIT (O 2 utilization - quenching of fluorescence) 35 Colony Morphology of M. gordonae and M. tuberculosis 36 18





19 Liquid Culture Systems VersaTREK Mycobacteria MGIT BD MB/BacT 37 Growth in Liquid Medium: M. tuberculosis and M. fortuitum 38 19


20 M. tuberculosis cords in liquid culture 39 Mycobacterium abscessus direct sputum smear 40 20



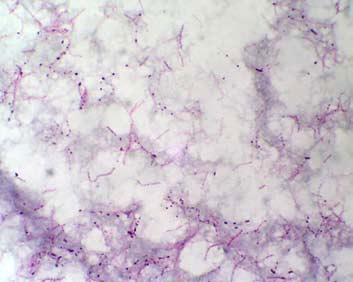
21 Gram Stain of M. tuberculosis cords 41 M. Kansasii concentrated smear 42 21
22 Identification of Mycobacteria Biochemical tests 2 to 3 weeks GenProbe - DNA - RNA hybridization 2 hours HPLC - high performance liquid chromatography 1 hour 43 Hybridization Protection Assay (GenProbe) Denatured (heat) Acridinium-labeled probe Alkaline hydrolysis Inactivated probe Substrate light 44 22
23 Mycobacterium avium complex (MAC) found in soil and water - tap water transmission through either respiratory or GI tract pulmonary disease like tuberculosis disseminated disease in AIDS patients 50% of autopsies resistant to many anti-mycobacterial drugs slow growing non-pigmented colonies Other Important MOTT M. kansasii - Photochromogen Tuberculosis like disease M. marinum - Photochromogen Found in water - fish tanks and surface water 30 to 33 o C optimum temperature M. scrofulaceum - granulomatous cervical lymphadenitis in children M. fortuitum - M. chelonei complex Rapid growers - colonies in less than 7 days Skin infections, pulmonary disease 23



24 M. marinum lymphocutaneous 47 M. marinum Fresh or salt water or no water exposure Photochromogen 1-2 patients/year at UAB 9 finger patients 30 o C optimum temperature colonies form in days 48 24
25 Mycobacterium leprae Hansen s disease humans and armadillos are the only natural hosts 12 million cases worldwide 6,000 registered cases in US, cases/year transmitted by inhalation or skin contact with contaminated respiratory secretions of lepromatous patients incubation period is 3 months to 3 years 50 25
26 Clinical Types of Leprosy Tuberculoid leprosy intact cell mediated response to M. leprae organisms rare in tissue organisms grow in nerves in cooler parts of the body cutaneous loss of sensation - nerve damage due to cell mediated immunity diagnosis Leprosy does not grow on artificial media will grow in nude mice or armadillo AFB stain of nasal secretions lepromin test - skin test treatment dapsone and rifampicin - at least 1 year prevention isolation of acute lepromatous cases vaccines under development 26



27 Lepromatous Leprosy depressed CMI response specific for M. leprae bacteremia with localization in nerves and skin high numbers of organisms in macrophages less loss of nerve function leonine facies other organs involved - testes, spleen and liver Lepromatous leprosy 54 27



28 Tuberculoid leprosy Non-progressive disease intact cell mediated response organisms rare in tissue macular lesions predominate organisms invade nerves and form granulomas cutaneous loss of sensation - nerve damage due to CMI 55 Tuberculous leprosy 56 28
Medical Bacteriology- Lecture 10. Mycobacterium. Actinomycetes. Nocardia
 Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- Lecture 10 Mycobacterium Actinomycetes Nocardia 1 Mycobacterium Characteristics - Large, very weakly gram positive rods - Obligate aerobes, related to Actinomycetes - Catalase positive
Medical Bacteriology- lecture 13. Mycobacterium Actinomycetes
 Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
Medical Bacteriology- lecture 13 Mycobacterium Actinomycetes Mycobacterium tuberculosis Large, very weakly gram positive rods, Obligate aerobes, related to Actinomycetes, non spore forming, non motile
MYCOBACTERIA. Pulmonary T.B. (infect bird)
") MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
MYCOBACTERIA SPP. Reservoir Clinical Manifestation Mycobacterium tuberculosis Human Pulmonary and dissem. T.B. M. lepra Human Leprosy M. bovis Human & cattle T.B. like infection M. avium Soil, water, birds,
Characteristics of Mycobacterium
 Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
Mycobacterium Characteristics of Mycobacterium Very thin, rod shape. Culture: Aerobic, need high levels of oxygen to grow. Very slow in grow compared to other bacteria (colonies may be visible in up to
AFB Identification Texas Approach
 AFB Identification Texas Approach Ken Jost Texas Department of State Health Services 6th National Conference on Laboratory Aspects of TB June 21, 2010 DSHS-Austin TB Lab Customers & Samples Year 2009 175
AFB Identification Texas Approach Ken Jost Texas Department of State Health Services 6th National Conference on Laboratory Aspects of TB June 21, 2010 DSHS-Austin TB Lab Customers & Samples Year 2009 175
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE
 Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
Mycobacteria & Tuberculosis PROF.HANAN HABIB & PROF ALI SOMILY DEPRTMENT OF PATHOLOGY, MICROBIOLOGY UNIT COLLEGE OF MEDICINE Objectives l Recognize that tuberculosis as a chronic disease mainly affecting
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
number Done by Corrected by Doctor Hamid Al Zoubi
 number 15 Done by أبو عجمي ة مها Corrected by Waseem Abu Obeida Doctor Hamid Al Zoubi In case you don t know - (Bacillus = rod) and (bacilli = rods) - hypersensitivity tests can be either immediate (within
number 15 Done by أبو عجمي ة مها Corrected by Waseem Abu Obeida Doctor Hamid Al Zoubi In case you don t know - (Bacillus = rod) and (bacilli = rods) - hypersensitivity tests can be either immediate (within
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual Definitions Page 1 2.0 DEFINITIONS Many of the definitions that follow are taken from
MYCOBACTERIOLOGY SERVICE MANUAL
 MYCOBACTERIOLOGY SERVICE MANUAL The Office of Laboratory Services (OLS) provides primary isolation and identification of Mycobacterium species in human diagnostic specimens. Reference specimens of AFB
MYCOBACTERIOLOGY SERVICE MANUAL The Office of Laboratory Services (OLS) provides primary isolation and identification of Mycobacterium species in human diagnostic specimens. Reference specimens of AFB
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
MYCOBACTERIUM. Mycobacterium Tuberculosis (Mtb) nontuberculous mycobacteria (NTM) Mycobacterium lepray
 nontuberculous mycobacteria (NTM) Mycobacterium lepray") MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
MYCOBACTERIUM nontuberculous mycobacteria (NTM) Mycobacterium Tuberculosis (Mtb) Mycobacterium lepray 1-tubercle bacilli are thin 2- straight rods 3- obligate aerobes 4- derive energy from the oxidation
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
ACCME/Disclosures. Two Patients and a Caveat 4/13/2016. Patient #1: 13 y/o boy with IPEX syndrome; s/p BMT
 Two Patients and a Caveat The Use and Misuse of Molecular Methods in Mycobacterial Infections Gary W. Procop, MD Director, Molecular Microbiology Infectious Disease Pathologist Cleveland Clinic ACCME/Disclosures
Two Patients and a Caveat The Use and Misuse of Molecular Methods in Mycobacterial Infections Gary W. Procop, MD Director, Molecular Microbiology Infectious Disease Pathologist Cleveland Clinic ACCME/Disclosures
MO TASEM AJ Nader Alaridah
 22 MO TASEM AJ...... Nader Alaridah Mycobacterium ** Mycobacterium is a class of Actinobacteria, which are non-spore forming, non-motile and acid-fast bacilli ( they remain stained with the red dye carbofuchsin
22 MO TASEM AJ...... Nader Alaridah Mycobacterium ** Mycobacterium is a class of Actinobacteria, which are non-spore forming, non-motile and acid-fast bacilli ( they remain stained with the red dye carbofuchsin
Mycobacterium tuberculosis. Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology
 Dr.Baha, AL-Amiedi Ph. D.Microbiology") Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
Mycobacterium tuberculosis Lecture (14) Dr.Baha, AL-Amiedi Ph. D.Microbiology Robert Koch 1843-1910 German physician Became famous for isolating the anthrax bacillus (1877), tuberculosis bacillus (1882)
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Order: Actinomycetales. Family: Mycobactericeae. Some are parasitic to cold blooded animal, others are saprophytic in nature.
 Order: Actinomycetales Family: Mycobactericeae They are widely distributed in nature. Few no is pathogenic for man & animal. Some are parasitic to cold blooded animal, others are saprophytic in nature.
Order: Actinomycetales Family: Mycobactericeae They are widely distributed in nature. Few no is pathogenic for man & animal. Some are parasitic to cold blooded animal, others are saprophytic in nature.
Respiratory System الفريق الطبي االكاديمي
 Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Respiratory System الفريق الطبي االكاديمي Pathology sheet 5 Tuberculosis Done by: Ahmad Al-Sahele Introduction: as we know TB is caused by mycobacterium tubercolosis; now keep in your mind another microorganism
Mycobacterial cell wall. Cell Cycle Lengths. Outline of Laboratory Methods. Laboratory Methods
 Laboratory Methods Cell Cycle Lengths Generation time (hrs) Days needed for 26 generations (colony) E. coli 0.33 0.36 Nancy Connell, PhD Professor, nfectious Disease Department of Medicine Center for Emerging
Laboratory Methods Cell Cycle Lengths Generation time (hrs) Days needed for 26 generations (colony) E. coli 0.33 0.36 Nancy Connell, PhD Professor, nfectious Disease Department of Medicine Center for Emerging
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
NTM Plus Case Studies
 NTM Plus Case Studies Youngmi Kim, Sr. Microbiologist MS, M(ASCP) Case 1 Referred Culture for ID & appropriate susceptibility Case 1 7/7/15: MGIT broth received DOC: 5-30-15 Source: FNA Mesenteric Mass,
NTM Plus Case Studies Youngmi Kim, Sr. Microbiologist MS, M(ASCP) Case 1 Referred Culture for ID & appropriate susceptibility Case 1 7/7/15: MGIT broth received DOC: 5-30-15 Source: FNA Mesenteric Mass,
Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis
 Annals of Clinical & Laboratory Science, vol. 33, no. 2, 2003 179 Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis complex,
Annals of Clinical & Laboratory Science, vol. 33, no. 2, 2003 179 Microscopic Morphology in Smears Prepared from MGIT Broth Medium for Rapid Presumptive Identification of Mycobacterium tuberculosis complex,
Nontuberculous Mycobacteria (NTM)
") Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
Nontuberculous Mycobacteria (NTM) Bacteria, like plants and animals, have been classified into similar groups. The groups are called "families." One such family of bacteria is known as the Mycobacteriaceae.
Laboratory Diagnostic Techniques. Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust
 Laboratory Diagnostic Techniques Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust Learning Objectives 1) When to consider a diagnosis of TB 2) When to consider a referral
Laboratory Diagnostic Techniques Hugo Donaldson Consultant Microbiologist Imperial College Healthcare NHS Trust Learning Objectives 1) When to consider a diagnosis of TB 2) When to consider a referral
TUBERCULOSIS. Famous victims in their intellectual prime: Chopin, Paganini, Thoreau, Keats, Elizabeth Browning, Brontës
 TUBERCULOSIS GENERAL Tuberculosis (TB) kills 1,700,000 annually worldwide. "The Captain of all the men of death that came to take him away was the consumption, for it was that which brought him down to
TUBERCULOSIS GENERAL Tuberculosis (TB) kills 1,700,000 annually worldwide. "The Captain of all the men of death that came to take him away was the consumption, for it was that which brought him down to
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing
 Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing 1. Essentials for the Mycobacteriology Laboratory: Promoting Quality Practices 1.1 Overview: Mycobacterial Culture, Identification,
Overview of Mycobacterial Culture, Identification, and Drug Susceptibility Testing 1. Essentials for the Mycobacteriology Laboratory: Promoting Quality Practices 1.1 Overview: Mycobacterial Culture, Identification,
Tuberculosis. Impact of TB. Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH)
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 20 Tuberculosis Learning Objectives 1. Describe the biologic characteristics of the agent 2. Determine the epidemiologic characteristics
MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit
 MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit Topics to be covered What is Tuberculosis? TB bacteria and what is unique about it. How is TB different from HIV? How is TB
MODULE ONE" TB Basic Science" Treatment Action Group TB/HIV Advocacy Toolkit Topics to be covered What is Tuberculosis? TB bacteria and what is unique about it. How is TB different from HIV? How is TB
Stacy White, PhD May 12, TB for Community Providers. Phoenix, Arizona
 Role of the Laboratory in TB Diagnosis Stacy White, PhD May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Stacy White, PhD has the following disclosures
Role of the Laboratory in TB Diagnosis Stacy White, PhD May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Stacy White, PhD has the following disclosures
Tuberculosis Elimination: The Role of the Infection Preventionist
 Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
Tuberculosis Elimination: The Role of the Infection Preventionist Preface: What Happens when Health Care Professionals are not familiar with TB? A 15 year old student was diagnosed with highly infectious
TB Laboratory for Nurses
 TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
TB Laboratory for Nurses Shea Rabley, RN, MN Consultant Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures None 2014 MFMER slide-2 Objectives Participants will be able to: 1. Name 2 safety
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Transmission and Pathogenesis of Tuberculosis. Transmission and Pathogenesis of Tuberculosis. Mycobacteria. Introduction to the pathogen Transmission
 Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Assistant Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Assistant Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Transmission and Pathogenesis of Tuberculosis
 Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Associate Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Transmission and Pathogenesis of Tuberculosis Adithya Cattamanchi MD, MAS Associate Professor of Medicine University of California San Francisco Slides adapted from James Watts, Phil Hopewell Transmission
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lisa Armitige, MD, PhD August 13, 2014 Lisa Armitige,
NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW.
 INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW.") NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW. K. Clay 1, K. Bhatt 1, D. Burns 1, J. Evans 2, S. Gardiner 2, EG. Smith 2, P. Hawkey 2,
NON-TUBERCULOUS MYCOBACTERIAL (NTM) INFECTIONS ISOLATED FROM BIRMINGHAM HEARTLANDS HOSPITAL: A CASE NOTES REVIEW. K. Clay 1, K. Bhatt 1, D. Burns 1, J. Evans 2, S. Gardiner 2, EG. Smith 2, P. Hawkey 2,
Leprosy. Dr Rodney Itaki Lecturer Anatomical Pathology Discipline
 Leprosy Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Leprosy - Overview Slow progressive infection
Leprosy Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea Division of Pathology School of Medicine & Health Sciences Leprosy - Overview Slow progressive infection
TB Updates for the Physician Rochester, Minnesota June 19, 2009
 TB Updates for the Physician Rochester, Minnesota June 19, 2009 Mycobacterial Laboratory Science Update Nancy L. Wengenack, Ph.D. Associate Professor of Laboratory Medicine and Pathology Division of Clinical
TB Updates for the Physician Rochester, Minnesota June 19, 2009 Mycobacterial Laboratory Science Update Nancy L. Wengenack, Ph.D. Associate Professor of Laboratory Medicine and Pathology Division of Clinical
What is it? Sherlock knows! Mycobacteria Identification System
 What is it? Sherlock knows! Mycobacteria Identification System Sherlock Mycobacteria Identification System Tuberculosis ID 15 Minutes... $5.00 Is it accurate? Established technology with over five years
What is it? Sherlock knows! Mycobacteria Identification System Sherlock Mycobacteria Identification System Tuberculosis ID 15 Minutes... $5.00 Is it accurate? Established technology with over five years
Appendix C. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix C Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix C Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
Variety of Names. Great White Plague
 Tuberculosis...Where youth grows pale, and spectre-thin, and dies;... You must not look at me in my dying gasp, nor breathe my passing breath... That drop of blood is my death warrant. I must die. --John
Tuberculosis...Where youth grows pale, and spectre-thin, and dies;... You must not look at me in my dying gasp, nor breathe my passing breath... That drop of blood is my death warrant. I must die. --John
Mycobacterial Infections in HIV. H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine
 Mycobacterial Infections in HIV H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine Learning Objectives List the most common mycobacterial infections
Mycobacterial Infections in HIV H. Gene Stringer, Jr., MD Infectious Diseases Section Department of Medicine Morehouse School of Medicine Learning Objectives List the most common mycobacterial infections
General Infectious Diseases
 Contents General Infectious Diseases Atibordee Meesing, MD Division of infectious disease Department of Medicine Khon kaen University Tuberculosis (TB) Overview of Nontuberculous Mycobacterial (NTM) Infections
Contents General Infectious Diseases Atibordee Meesing, MD Division of infectious disease Department of Medicine Khon kaen University Tuberculosis (TB) Overview of Nontuberculous Mycobacterial (NTM) Infections
Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014
 TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas April 1 3, 2014 Diagnosis of TB: Laboratory Ken Jost Tuesday April 1, 2014 Ken Jost, BA has the following disclosures to make: No conflict of interests No relevant
HIDDEN IN PLAIN SITE:
 HIDDEN IN PLAIN SITE: MYCOBACTERIUM ON THE ROUTINE BENCH Christina Partington MT(ASCP) ACL Laboratory 1 Introduction The importance of the possibility of AFB appearing in a routine culture. How to recognize
HIDDEN IN PLAIN SITE: MYCOBACTERIUM ON THE ROUTINE BENCH Christina Partington MT(ASCP) ACL Laboratory 1 Introduction The importance of the possibility of AFB appearing in a routine culture. How to recognize
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Tuberculosis: The Essentials
 Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Tuberculosis: The Essentials Kendra L. Fisher, MD, PhD THORACIC TUBERCULOSIS: THE BARE ESSENTIALS Kendra Fisher MD, FRCP (C) Department of Radiology Loma Linda University Medical Center TUBERCULOSIS ()
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Tuberculosis Pathophysiology and Transmission
 Tuberculosis Pathophysiology and Transmission Paul K. Drain, MD, MPH, FACP Assistant Professor Depts. of Global Health, Medicine (Infectious Diseases), Epidemiology University of Washington June 16, 2018
Tuberculosis Pathophysiology and Transmission Paul K. Drain, MD, MPH, FACP Assistant Professor Depts. of Global Health, Medicine (Infectious Diseases), Epidemiology University of Washington June 16, 2018
Standardized Case Definition for Extrapulmonary Nontuberculous Mycobacteria Infections
 Operational Guidance for Position Statement 17 ID 07: Standardized Case Definition for Extrapulmonary Nontuberculous Mycobacteria Infections Submission Date: April 28, 2017 Committee: Infectious Disease
Operational Guidance for Position Statement 17 ID 07: Standardized Case Definition for Extrapulmonary Nontuberculous Mycobacteria Infections Submission Date: April 28, 2017 Committee: Infectious Disease
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
SWABCHA Fact Sheet: Tuberculosis (TB)
") SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
SWABCHA (TB) Text sourced from the SWABCHA Change Agent Training Guide - 2012 Introduction to TB Microscopic bacteria called Mycobacterium tuberculosis causes TB Only TB of the lungs or throat may be infectious.
2018 Vindico Medical Education. Non-tuberculous Mycobacteria: Circumventing Difficulties in Diagnosis and Treatment
 Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
Activity presentations are considered intellectual property. These slides may not be published or posted online without permission from Vindico Medical Education (cme@vindicocme.com). Please be respectful
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
Tuberculosis Part 1. Some useful truths
 Tuberculosis Part 1 Some useful truths Tuberculosis will be dealt with in detail in chapter 9 in a few week s time when we deal with the air borne bacterial diseases and the diseases of the lower respiratory
Tuberculosis Part 1 Some useful truths Tuberculosis will be dealt with in detail in chapter 9 in a few week s time when we deal with the air borne bacterial diseases and the diseases of the lower respiratory
TB 101 Disease, Clinical Assessment and Lab Testing
 TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
TB 101 Disease, Clinical Assessment and Lab Testing Pacific Islands Tuberculosis Controllers Association Conference (PITCA) Clinical Laboratory Breakout None Disclosure Objectives Be able to list and explain
9 month old with stridor, cough, low-grade fever, mild hypoxia
 9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
9 month old with stridor, cough, low-grade fever, mild hypoxia 3 months of age CXR normal Scenarios: Pregnant woman with + PPD Next steps? CXR negative, asymptomatic: treat for LTBI after delivery (INH
Summary of Key Points WHO Position Paper on BCG Vaccine, February 2018
 Summary of Key Points WHO Position Paper on BCG Vaccine, February 2018 1 Introduction This position paper replaces the 2004 WHO position paper on Bacille Calmette-Guérin (BCG) vaccine and the 2007 WHO
Summary of Key Points WHO Position Paper on BCG Vaccine, February 2018 1 Introduction This position paper replaces the 2004 WHO position paper on Bacille Calmette-Guérin (BCG) vaccine and the 2007 WHO
Diagnostic Value of Elisa Serological Tests in Childhood Tuberculosis
 Diagnostic Value of Elisa Serological Tests in Childhood Tuberculosis by R. Dayal, a G. Sirohi, a M. K. Singh, a P. P. Mathur, a B. M. Agarwal, a V. M. Katoch, b B. Joshi, b P. Singh, b and H. B. Singh
Diagnostic Value of Elisa Serological Tests in Childhood Tuberculosis by R. Dayal, a G. Sirohi, a M. K. Singh, a P. P. Mathur, a B. M. Agarwal, a V. M. Katoch, b B. Joshi, b P. Singh, b and H. B. Singh
7. BCG Vaccination HSE/HPSC. Guidelines on the Prevention and Control of Tuberculosis in Ireland IUATLD criteria
 7. BCG Vaccination The Bacillus Calmette-Guerin (BCG) vaccine was derived by in-vitro attenuation of the bovine tubercle bacillus between the years 1908 and 1918 in France. WHO encouraged widespread use
7. BCG Vaccination The Bacillus Calmette-Guerin (BCG) vaccine was derived by in-vitro attenuation of the bovine tubercle bacillus between the years 1908 and 1918 in France. WHO encouraged widespread use
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
2/18/19. Case 1. Question
 Case 1 Which of the following can present with granulomatous inflammation? A. Sarcoidosis B. Necrobiotic xanthogranulma C. Atypical mycobacterial infection D. Foreign Body Reaction E. All of the above
Case 1 Which of the following can present with granulomatous inflammation? A. Sarcoidosis B. Necrobiotic xanthogranulma C. Atypical mycobacterial infection D. Foreign Body Reaction E. All of the above
DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI Page 1 Page 2 nontuberculous mycobacteria ntm nontuberculous mycobacteria ntm pdf nontuberculous mycobacteria ntm patients and those
DOWNLOAD OR READ : NONTUBERCULOUS MYCOBACTERIA NTM PDF EBOOK EPUB MOBI Page 1 Page 2 nontuberculous mycobacteria ntm nontuberculous mycobacteria ntm pdf nontuberculous mycobacteria ntm patients and those
Transmission of Mycobacterium tuberculosis
 Transmission of Mycobacterium tuberculosis Charles Daley, MD National Jewish Health Disclosures Advisory Board Horizon, Johnson and Johnson, Otsuka and Spero Investigator Insmed Objectives After attending
Transmission of Mycobacterium tuberculosis Charles Daley, MD National Jewish Health Disclosures Advisory Board Horizon, Johnson and Johnson, Otsuka and Spero Investigator Insmed Objectives After attending
Nontuberculous Mycobacterial Lung Disease
 Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
Non-TB Mycobacterial Disease Jeffrey P. Kanne, MD Nontuberculous Mycobacterial Lung Disease Jeffrey P. Kanne, M.D. Consultant Disclosures Perceptive Informatics Royalties (book author) Amirsys, Inc. Wolters
At the end of this session, participants will be able to:
 Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Advanced Concepts in Pediatric Tuberculosis: Infection Control, Source Case and Contact Investigation Ana M. Alvarez, M.D. Associate Professor Division of Pediatric Infectious Diseases and Immunology University
Frances Morgan, PhD October 21, Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS
 The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
The Laboratory s Role in Caring for Patients Diagnosed with TB Frances Morgan, PhD October 21, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
TB/HIV 2 sides of the same coin. Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai
 TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
TB/HIV 2 sides of the same coin Dr. Shamma Shetye, MD Microbiology Metropolis Healthcare, Mumbai Global- Tb new cases Diagnosis-Microscopy ZN,Flourescent microscopy(fm) Rapid, inexpensive test Specificity>95%
TB Intensive Houston, Texas October 15-17, 2013
 TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis Pathogenesis and Treatment f Latent TB Infection Lynn Horvath, MD October 15, 2013 Lynn Horvath, MD has the following disclosures to make: No
TB Intensive Houston, Texas October 15-17, 2013 Tuberculosis Pathogenesis and Treatment f Latent TB Infection Lynn Horvath, MD October 15, 2013 Lynn Horvath, MD has the following disclosures to make: No
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Antimycobacterial drugs. Dr.Naza M.Ali lec Dec 2018
 Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
Antimycobacterial drugs Dr.Naza M.Ali lec 14-15 6 Dec 2018 About one-third of the world s population is infected with M. tuberculosis With 30 million people having active disease. Worldwide, 9 million
The Air We Share: Principles and Practices of TB Infection Control
 The Air We Share: Principles and Practices of TB Infection Control Session Four of a Four-Part Webinar Series Presented in Partnership with the BC Lung Association January 10, 2014 Facilitators: Nash Dhalla,
The Air We Share: Principles and Practices of TB Infection Control Session Four of a Four-Part Webinar Series Presented in Partnership with the BC Lung Association January 10, 2014 Facilitators: Nash Dhalla,
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
Objectives. TB Laboratory Methods
 TB Laboratory Methods Beverly Metchock, Dr.P.H., D(ABMM) Team Leader, Reference Laboratory, Mycobacteriology Laboratory Branch February 2011 Objectives General overview of mycobacteriology (TB) lab practices
TB Laboratory Methods Beverly Metchock, Dr.P.H., D(ABMM) Team Leader, Reference Laboratory, Mycobacteriology Laboratory Branch February 2011 Objectives General overview of mycobacteriology (TB) lab practices
BCG in Tower Hamlets. Luise Dawson Public Health Nurse
 BCG in Tower Hamlets Luise Dawson Public Health Nurse Coverage levels of BCG for infants under 1 year 100% 90.9% 95.5% 95.0% 98.7% 90% 81% 82% 80% 70% 60% 50% 40% 30% 20% 10% 0% March 0708 March 0809 March
BCG in Tower Hamlets Luise Dawson Public Health Nurse Coverage levels of BCG for infants under 1 year 100% 90.9% 95.5% 95.0% 98.7% 90% 81% 82% 80% 70% 60% 50% 40% 30% 20% 10% 0% March 0708 March 0809 March
(A) Consumption of contaminated food (B) Direct contact with fomite (C) Arthropod vector (D) Respiratory route (E) Sexual contact
 Consumption of contaminated food (B) Direct contact with fomite (C) Arthropod vector (D) Respiratory route (E) Sexual contact") A 33-year-old man presents to the emergency department with a fever of 102.5 F, facial palsy, headache, and malaise. A circular maculopapular rash was identified on the patients left shoulder; the patient
A 33-year-old man presents to the emergency department with a fever of 102.5 F, facial palsy, headache, and malaise. A circular maculopapular rash was identified on the patients left shoulder; the patient
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Ken Jost, BA, has the following disclosures to make:
 Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Diagnosis of TB Disease: Laboratory Ken Jost, BA May 10, 2017 TB Intensive May 9-12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Ken Jost, BA, has the following disclosures to make: No conflict
Role of the Laboratory in TB Diagnosis and Management
 Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
Role of the Laboratory in TB Diagnosis and Management Michael Pentella, Ph.D., D(ABMM), CIC Associate Director University Hygienic Lab Clinical Associate Professor, College of Public Health, University
Nontuberculous mycobacteria isolated from pulmonary specimens between 2004 and 2009: causative agent or not?
 NEW MICROBIOLOGICA, 33, 399-403, 2010 Nontuberculous mycobacteria isolated from pulmonary specimens between 2004 and 2009: causative agent or not? Can Bicmen 1, Meral Coskun 1, Ayriz T. Gunduz 1, Gunes
NEW MICROBIOLOGICA, 33, 399-403, 2010 Nontuberculous mycobacteria isolated from pulmonary specimens between 2004 and 2009: causative agent or not? Can Bicmen 1, Meral Coskun 1, Ayriz T. Gunduz 1, Gunes
General Session IV - Dale Schwab April 20, 2017
 The Culture of Clinical Commercial Labs Presented by: Dale Schwab PhD, Senior Scientific Director, Infectious Disease April 20, 2017 Objectives Challenges for the reference laboratory in MTB diagnosis/opportunities
The Culture of Clinical Commercial Labs Presented by: Dale Schwab PhD, Senior Scientific Director, Infectious Disease April 20, 2017 Objectives Challenges for the reference laboratory in MTB diagnosis/opportunities
TB Intensive San Antonio, Texas November 11 14, 2014
 TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
TB Intensive San Antonio, Texas November 11 14, 2014 Tuberculosis Pathogenesis and Treatment of Latent TB Infection Lynn Horvath, MD November 11, 2014 Lynn Horvath, MD has the following disclosures to
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Self-Study Modules on Tuberculosis
 Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Self-Study Modules on Tuberculosis Transmission and Pathogenesis of Tube rc ulos is U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Disease Control and Prevention National Center for HIV/AIDS,
Research Methods for TB Diagnostics. Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012
 Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Research Methods for TB Diagnostics Kathy DeRiemer, PhD, MPH University of California, Davis Shanghai, China: May 8, 2012 Overview Why do we need good TB diagnostics? What works? What doesn t work? How
Molecular diagnosis of MDR-TB using GenoType MTBDRplus 96 assay in Ibadan, Nigeria
 Niger. J. Physiol. Sci. 28(December 2013) 187 191 www.njps.com.ng Molecular diagnosis of MDR-TB using GenoType MTBDRplus 96 assay in Ibadan, Nigeria * 1 Kehinde A.O. and 2 Adebiyi, E.O. Department of Medical
Niger. J. Physiol. Sci. 28(December 2013) 187 191 www.njps.com.ng Molecular diagnosis of MDR-TB using GenoType MTBDRplus 96 assay in Ibadan, Nigeria * 1 Kehinde A.O. and 2 Adebiyi, E.O. Department of Medical
56% of these were in south east Asia and west pacific region.
 Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Tuberc ulosis Dr. ASAAD FARHAN ASSIST. PROF.PEDS. Learning objectives epidemiology Tuberculosis remains worlds deadliest communicable disease. TB is present in all regions of the world. WHO estimates that
Appendix B. Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997)
") Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
Appendix B Recommendations for Counting Reported Tuberculosis Cases (Revised July 1997) Since publication of the Recommendations for Counting Reported Tuberculosis Cases 1 in January 1977, numerous changes
TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks
 1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On
1 TB facts & figures Microbiology of TB Transmission of TB Infection control in health care settings Special cases Resistant TB Masks 2 Page 1 4 NHS Lothian Infection Prevention and Control Study Day On