Clinical Infectious Diseases Advance Access published July 23, 2014
|
|
|
- Joleen Stanley
- 5 years ago
- Views:
Transcription
1 Clinical Infectious Diseases Advance Access published July 23, The Effect of Therapeutic Lumbar Punctures on Acute Mortality from Cryptococcal Meningitis Melissa A. Rolfes 1, Kathy Huppler Hullsiek 2, Joshua Rhein 1,3, Henry W. Nabeta 3, Kabanda Taseera 4, Charlotte Schutz 5, Abdu Musubire 3, Radha Rajasingham 1,3, Darlisha A. Williams 1,3, Friedrich Thienemann 5, Conrad Muzoora 4, Graeme Meintjes 5,6, David B. Meya 1,3,7, David R. Boulware 1 1 Department of Medicine, Medical School, University of Minnesota, Minneapolis, MN, USA 2 Division of Biostatistics, School of Public Health, University of Minnesota, Minneapolis, MN, USA 3 Infectious Diseases Institute, Makerere University, Kampala, Uganda 4 Internal Medicine, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda 5 Institute of Infectious Disease and Molecular Medicine and Department of Medicine, University of Cape Town, Cape Town, South Africa 6 Department of Medicine, Imperial College London, London, UK 7 School of Medicine, College of Health Sciences, Makerere University, Kampala, Uganda Corresponding author contract info: Melissa A Rolfes, riede056@umn.edu, th St. SE, MTRF Rm 3-500, University of Minnesota, Minneapolis, MN, USA Alt corresponding author: David R Boulware, boulw001@umn.edu, th St. SE, MTRF Rm 3-222, Minneapolis, MN 55455, USA 40-word summary: Intracranial pressure management with repeat lumbar puncture (LP) was investigated in patients with cryptococcal meningitis in sub-saharan Africa. Conducting at least one additional LP soon after cryptococcal diagnosis was related to decreased risk of acute mortality regardless of initial pressure. The Author Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please journals.permissions@oup.com.
2 2 Abstract Introduction: Cryptococcal meningitis is the most common cause of adult meningitis in sub-saharan Africa. Raised intracranial pressure (ICP) is common in cryptococcosis. Prior studies suggest elevated ICP is associated with mortality, and guidelines recommend frequent lumbar punctures (LPs) to control ICP. However, the magnitude of the impact of LPs on cryptococcal-related mortality is unknown. Methods: 248 individuals with HIV-associated cryptococcal meningitis, screened for the Cryptococcal Optimal ART Timing (COAT) trial in Uganda and South Africa, were observed. Individuals received an LP to diagnose meningitis and subsequent therapeutic LPs were recommended for elevated ICP (>250 mmh 2 O) or new symptoms. We compared survival, through 11 days, between individuals receiving at least one therapeutic LP with individuals not receiving therapeutic LPs. The COAT trial randomized subjects at 7-11 days, thus follow-up stopped at time of death, randomization, or 11 days. Results: 75 (30%) individuals had at least one therapeutic LP. Individuals receiving therapeutic LPs had higher cerebrospinal fluid (CSF) opening pressures, higher CSF fungal burdens, and were more likely to have altered mental status at baseline than those with no therapeutic LPs. 31 deaths (18%) occurred among 173 individuals without a therapeutic LP and 5 deaths (7%) among 75 with at least one therapeutic LP. The adjusted relative risk of mortality was 0.31 (95% confidence interval: ). The association was observed regardless of opening pressure at baseline. Conclusions: Therapeutic LPs were associated with a 69% relative improvement in survival, regardless of initial intracranial pressure. The role of therapeutic LPs should be re-evaluated.
3 3 Introduction Despite recognition of the burden and advancements in treatment, acute mortality from HIVassociated cryptococcal meningitis in resource-limited settings remains high with 17-50% mortality within two weeks of diagnosis among individuals in sub-saharan Africa [1 9]. One complication of cryptococcal meningitis is elevated intracranial pressure (ICP), defined as a CSF opening pressure greater than 250 mmh 2 O, and prior literature suggests there is higher mortality among cryptococcal patients with raised ICP [10 12]. Raised ICP is common at the time of diagnosis and frequently leads to changes in mental status, headache, loss of vision and hearing, or death. Aggressive management of ICP is therefore suggested in treatment guidelines for cryptococcal meningitis, including daily therapeutic lumbar punctures (LPs) until pressures and symptoms have normalized [13,14]. With these recommendations, elevated ICP typically resolves over the first two weeks of antifungal therapy. Prior studies have not found an association between baseline opening pressure and 2-week mortality attributed, in part, to aggressive control of ICP with therapeutic LPs [4,15,16]. A recent comparison to historical data also suggested that following a strict schedule of therapeutic LPs may have led to lower 30-day mortality in a hospital in Tanzania [17]. We aimed to add to the current body of literature and estimate the direct effect of therapeutic LPs on acute mortality in a prospective cohort of HIV-infected individuals with cryptococcal meningitis in Uganda and South Africa. Methods Study Population Data from the Cryptococcal Optimal ART Timing (COAT) trial, conducted from November 2010 to April 2012, and an observational cohort of patients with cryptococcal meningitis, from April 2012 through December 2012, were used in this analysis. Ethical approval was granted from the Uganda National Council of Science and Technology, South African Medicines Control Council, and the
4 4 Institutional Review Boards at the University of Minnesota, Makerere University, University of Cape Town, and Mbarara University of Science and Technology. The COAT trial was a randomized clinical strategy trial of early ART initiation (one week after cryptococcal meningitis diagnosis) compared to deferred ART initiation (five weeks after cryptococcal meningitis diagnosis; NCT ). Individuals with suspected meningitis were recruited from three sites: Mulago National Referral Hospital in Kampala, Uganda; Mbarara National Referral Hospital in Mbarara, Uganda; and GF Jooste Hospital in Cape Town, South Africa. Individuals participating in COAT were randomized within 7-11 days of cryptococcal treatment initiation. Observational cohort recruitment occurred at Mulago Hospital after enrollment in the COAT trial ended. Individuals in the observational cohort received identical care to COAT participants, but with deferred ART initiation. HIV-infected, ART-naive individuals were eligible for enrollment into the trial or cohort if they were at least 18 years old, provided written informed consent, had cryptococcal meningitis documented by CSF culture or cryptococcal antigen test, and were receiving amphotericin-based treatment. Individuals on antifungal therapy for more than one week or with a prior episode of cryptococcal meningitis were excluded. Antifungal induction treatment included two weeks of amphotericin B deoxycholate ( mg/kg/day) plus fluconazole (800 mg/day). Baseline clinical and laboratory features were collected at the time of cryptococcal meningitis diagnosis. For this analysis, follow-up time began the day after diagnosis of cryptococcal meningitis in order to allow individuals the opportunity for a therapeutic LP. For individuals screened for the COAT trial, observation ended at the time of death or at randomization (7-11 days after starting treatment for cryptococcal meningitis) because the COAT protocol indicated a scheduled LP be performed at randomization and at 14 days. The median time of COAT randomization was 8 days from the start of antifungal therapy. For individuals in the observational cohort, observation ended at the time of death or after 11 days of follow-up.
5 5 Lumbar Punctures and CSF Parameters Therapeutic LPs after the diagnostic LP were recommended for those with baseline CSF opening pressure greater than 250 mmh 2 O or symptoms of raised pressure [14]. Participants could receive multiple therapeutic LPs at the discretion of the attending clinician; however, in this analysis, exposure was defined as receiving at least one therapeutic LP. Written informed consent was provided for the initial diagnostic LP, and verbal consent was required before all subsequent therapeutic LPs. Participants or their surrogate had the right to refuse therapeutic LPs. The amount of CSF removed during an LP was recorded, and CSF opening and closing pressures were measured whenever the study team performed the LP. Statistical Analysis Because exposure status was not known at the start of observation, receipt of therapeutic LPs was included as a time-varying exposure in analysis. Individuals contributed person-time to the no therapeutic LP group after their diagnostic LP and until they received a therapeutic LP, died, or were censored (at COAT trial randomization or a maximum of 11 days of follow-up). Once a therapeutic LP was performed, individuals contributed person-time to the therapeutic LP group. Crude mortality rates were calculated for person-time before a therapeutic LP as well as for person-time after the first therapeutic LP. Differences in baseline factors by eventual LP and vital status were compared using Chisquare and Wilcoxon rank-sum tests. The outcome of interest was all-cause mortality within 11 days of follow-up. Time to death was modeled with a pooled Poisson regression model. Inverse probability weights were used to control for confounding (see Appendix). The relative risk of mortality was estimated, comparing the therapeutic LP group with the no therapeutic LP group [18,19]. Possible confounders were considered among baseline characteristics associated with exposure, known to be related to acute mortality, and that changed the estimated relative risk by more than 10% after adjustment. Linear, non-linear, and categorical forms of continuous variables were considered.
6 6 Linear terms were chosen for all variables except Glasgow Coma Scale (GCS) scores, which were dichotomized as less than 15 (indicating altered mental status) or 15 for all models. P values less than 0.05 were considered statistically significant. All data analyses were conducted in SAS version 9.3 (SAS Institute, Cary, NC). Missing Data Multiple imputation was conducted to better estimate the effect of therapeutic LPs accounting for missing baseline characteristics (see Appendix). The most common missing characteristic was weight (34% missing), due to the inability of critically ill individuals to stand for measurement. Other common missing factors were CSF opening pressure (16% missing) and serum potassium (12% missing). All other variables were missing in less than 10% of the data. Reasons for missing data stemmed from insufficient supplies or specimen volumes and were, thus, assumed to be missing at random [20]; with the exception of weight, which could be related to severity of illness and short-term mortality. Sensitivity analyses considered models with an indicator variable for missing weight but were found not to change the overall conclusions. Results Study Population Four hundred seventy-four individuals were screened, and 257 were found to have cryptococcal meningitis and were considered for inclusion in this analysis. Nine individuals died or had a therapeutic LP on the same day as diagnosis and were excluded from further analysis, leaving 248 individuals for analysis (Figure 1). Included individuals were all HIV-infected and observed for a total of 1,698 persondays (median follow-up 7 days, [IQR: 6-8 days]). The median age of the cohort was 36 years, median duration of headache was 2 weeks before diagnosis, 55% were male, and 29% had altered mental status (GCS <15). Seventy-five (30%) subjects received at least one therapeutic LP after diagnosis. The median baseline ICP at diagnosis was 269 mmh 2 O (IQR: mmh 2 O) and was significantly higher among
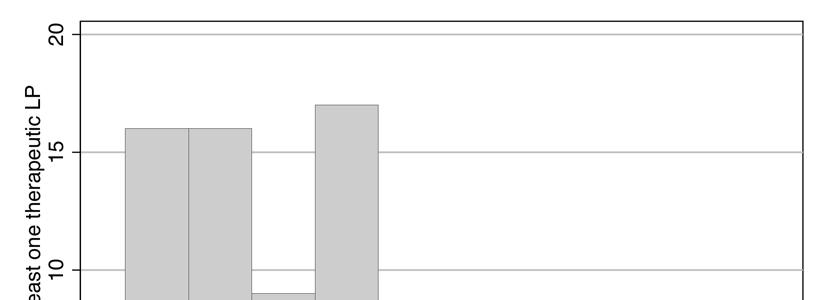
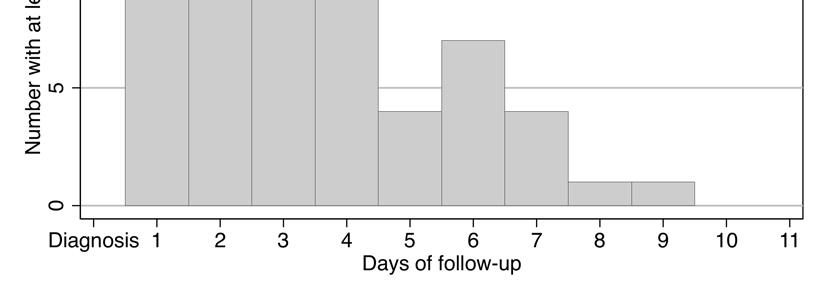
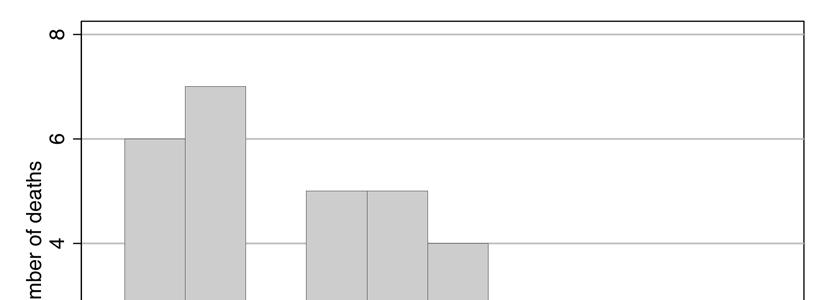
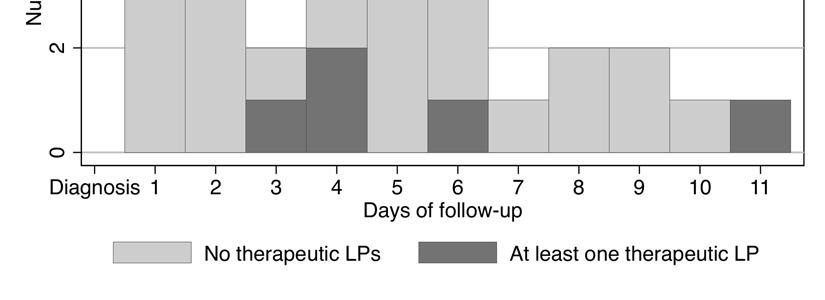
7 7 individuals who later received a therapeutic LP (Table 1). The majority of individuals (80%) receiving a therapeutic LP underwent only one LP during follow-up, although 15 individuals had 2 or more LPs including two individuals who received 7 LPs and one individual who received 8 LPs during the observation period. The median time to first therapeutic LP was 3 days after diagnosis (IQR: 2-4 days; Figure 2). At the first therapeutic LP, the median opening pressure was 270 mmh 2 O (IQR: mmh 2 O) overall, being higher than 250 mmh 2 O in 58% of persons. At the first therapeutic LP, ICP was higher among those with initially elevated ICP at diagnosis; median opening pressure was 329 mmh 2 O (IQR: mmh 2 O) among those with opening pressure greater than 250 mmh 2 O at diagnosis, and 255 mmh 2 O (IQR: mmh 2 O) among those with opening pressure less than 250 mmh 2 O at diagnosis. The occurrence of therapeutic LPs was slightly different by study site, with LPs occurring more frequently in Kampala and Cape Town (Table 1). Those receiving additional LPs had higher CSF fungal burden, higher CSF opening and closing pressures, and more CSF volume was removed during the first diagnostic LP. Other clinical and demographic characteristics were generally similar between the groups. Acute Mortality Thirty-six deaths occurred during observation for an overall mortality rate of 2.1 per 100 person-days (95% CI: per 100 person-days). The median time to death was 4 days (IQR: 2-6 days). Acute mortality was associated with lower weight, missing weight at baseline, lower GCS, greater heart rate, faster respiratory rate, and higher CSF fungal burden at cryptococcal meningitis diagnosis (Table 2). The CSF opening pressure, amount of CSF removed, and CSF white blood cell counts at the diagnostic LP were similar between those who died and those surviving through follow-up. Deaths in the group who received a therapeutic LP occurred later during observation than the deaths among those who did not receive additional LPs (Figure 3). Prior to receiving a therapeutic LP, the mortality rate was 2.4 per 100 person-days (95% CI: per 100 person-days) compared to 1.3 per 100 person-days (95% CI: per 100 person-days) after receiving a therapeutic LP. Of those who
8 8 received a therapeutic LP and died, all 5 individuals underwent only one additional LP during observation. Multivariable Association The crude, unweighted relative risk (RR) of mortality was 0.5 (95% CI: 0.2, 1.4), comparing those with at least one compared to those with no therapeutic LP (Table 3). Adjustment for heart rate, CSF fungal burden, and an indicator for low GCS into the weighted model resulted in more extreme relative risks (adjusted models 1-3). After adjusting for heart rate, CSF fungal burden, and GCS (adjusted model 3), the average effect of therapeutic LPs was to reduce the risk of mortality by 69% (95% CI: 18-88%). Additional adjustment for CSF opening pressure did not result in measureable changes in the relative risk (0.31; 95% CI: ). Adjustment for baseline CSF closing pressure and weight did not alter the estimated effect. Opening Pressure Subgroups Exploratory analysis was conducted to assess whether the effect of therapeutic LPs differed by baseline CSF opening pressure. The frequency of therapeutic LPs was higher in the subgroup with high baseline pressures than in those with lower pressures (Table 4); however, there was little evidence of heterogeneity of the relative risk estimates, suggesting that the effect of therapeutic LPs on acute mortality did not differ by baseline opening pressure. Forty individuals did not have CSF opening pressure measured at the time of diagnosis, primarily because non-study staff conducted the initial LP without the use of a manometer. Baseline characteristics were similar among those who did and did not have opening pressure measured (results not shown), except that a greater amount of CSF was removed during the diagnostic LP in those with measured opening pressure (median 8 ml removed in those without manometer measurement [IQR: 5-15 ml] versus 16 ml in those with measurements [IQR: ml], P<.001). Of those with missing opening pressure data, 15% of individuals received therapeutic LPs during follow-up. Overall, mortality was highest among those without pressure measurements (23%) compared to individuals with measured
9 9 pressures (13%). The sample size was too small to draw definitive conclusions on the effect of therapeutic LPs on mortality in those without measured CSF opening pressure. Discussion In this study, 30% of patients with HIV-associated cryptococcal meningitis received at least one therapeutic LP, and, overall, 15% died within 11 days of follow-up. The majority of those who died (85%) did not have a therapeutic LP during observation. After adjustment for potential confounding, a 69% relative survival benefit was observed after receiving a therapeutic LP. Raised intracranial pressure is common in cryptococcal meningitis, occurring in over 60% of patients in sub-saharan Africa [5,15,17], thus these findings may have a large impact on recovery from cryptococcal meningitis. Prior data suggest ICP can build up over time and any rise may initially be asymptomatic [11,15]. Therefore, reducing CSF volume before ICP has increased to symptomatic or detrimental levels may provide one possible explanation for improved survival after a therapeutic LP. In AIDS-related cryptococcosis, increased pressure primarily results from blockage of CSF drainage in the arachnoid villi and granulations by masses of cryptococcal cells or shed polysaccharide, inflammation, or a combination of these factors [11,21 23]. Several studies detail a possible link between raised ICP and short-term mortality after cryptococcosis [11,12,15,21]; however, no prior direct estimates exist of the effect of ICP management with therapeutic LPs on mortality. The evidence from this analysis provides a direct estimate of a survival benefit with therapeutic LPs and strongly supports the current treatment guidelines, which stress the importance of ICP management in cryptococcal meningitis. The effect of therapeutic LPs did not appear to be relegated to only those with high baseline opening pressures, suggesting that all cryptococcal patients regardless of initial opening pressure may benefit from therapeutic LPs. However, as this subgroup analysis was small and likely underpowered, further studies of therapeutic LPs are needed to understand whether all patients would experience a survival benefit with therapeutic LPs during antifungal treatment.
10 10 Another important finding was that less CSF volume was removed during LPs in which the opening pressure was not measured. Additionally, patients in whom the opening pressure was not measured during the diagnostic LP were less likely to receive therapeutic LPs in follow-up. Among other differences that may exist for those without measured pressure, it is possible that the initial volume removed was insufficient to normalize pressure, partly explaining the increased mortality rate in this subgroup. Unfortunately, most patients throughout the world do not have the baseline CSF pressure measured because of limited awareness of the importance of measuring CSF opening pressure [24] or lack of access to manometers for accurate measurement [15,25]. There is good evidence that intravenous tubing sets assembled to spinal needles coupled with a meter measuring stick are an accurate alternative to manometers to measure CSF opening pressure [17]; however, in the absence of a manometer or pressure measurement, the optimal timing and volume of CSF removed during repeat LPs is unclear. Recommendations are to initially remove 20 ml of CSF during the diagnostic LP and repeat therapeutic LPs daily, if needed based on symptoms [26]. One problem with this recommendation is that typically the Cryptococcus diagnosis is made after the initial diagnostic LP is complete and the opportunity is missed to quickly remove greater volumes of CSF and reduce ICP. Our group in Uganda routinely pre-screens HIV-infected patients with subacute/chronic meningitis with the cryptococcal antigen lateral flow assay (Immy, Inc. Norman, Oklahoma) using fingerstick specimens or whole blood/plasma specimens at the bedside during the informed consent process prior to the lumbar puncture. For patients with a positive cryptococcal antigen, a manometer can be prioritized for use and ICP can be normalized during the first LP a patient receives. Furthermore, an inability to control ICP may be unavoidable using a strategy based on reported symptoms, which, when compounded by the time demands of repeat LPs, make repeat therapeutic LPs inconsistent and infrequent, as our data suggest. A limitation to our analysis is the potential for unmeasured confounding, as data on the daily clinical status of patients was unavailable for analysis, particularly prior to COAT trial randomization. Characteristics such as worsening headache or declines in mental status may have occurred more among individuals who died quickly. If these symptoms were also more common among those who did not
11 11 receive an LP perhaps because the patient or his/her attendant declined an LP, then uncontrolled confounding may be present. Although it is unknown whether such confounding exists, it is reasonable to assume that LPs were uniformly considered and recommended, because the same clinician attended to patients within a site. This uniformity reduces the potential for confounding. One approach to assess for residual confounding was to evaluate the effect of therapeutic LPs stratified by baseline opening pressure, a strong indicator for undergoing additional LPs. The mortality trend was similar by baseline pressure strata providing some reassurance against residual confounding. Further investigation of therapeutic LPs during cryptococcal meningitis therapy is warranted to see if the beneficial effect is uniformly experienced in different settings and to better understand the role of multiple therapeutic LPs. In our cohort therapeutic LPs were considered based on baseline CSF opening pressure and symptoms of raised ICP while other studies have used a systematic approach when conducting scheduled therapeutic LPs for phase II trials to document the early fungicidal activity. These studies with scheduled LPs have failed to find associations between raised baseline ICP and increased mortality [4,15]. Future trials should examine whether survival differs between a strategy to perform therapeutic LPs based on CSF opening pressures greater than 250 mmh 2 O versus a strategy using a predefined schedule of lumbar punctures (e.g. on days 1, 3, 7, and 14) for all patients. In conclusion, our analysis supports the call for continued vigilance on ICP management during the window of high mortality shortly after diagnosis with HIV-associated cryptococcal meningitis, including improved access to manometers to monitor CSF pressures and the use of therapeutic LPs to reduce CSF pressure during antifungal therapy. Words = 2922 Acknowledgements: We thank Drs. Claudia Munoz-Zanzi, Alan Lifson, and James Neaton for their comments. We thank support from Drs. Trinh Ly, Chris Lambros, Karen Reese, and Neal Wetherall. We thank institutional support from Drs. Paul Bohjanen, Andrew Kambugu, Alex Coutinho, and Aaron
12 12 Friedman, and the IDI DataFax team of Mariam Namawejje and Mark Ssennono for data management with support from the NIAID Office of Cyberinfrastructure and Computational Biology (OCICB), Kevin Newell, and Dr. Steven Reynolds. Funding Financial support for this research was provided by the National Institute of Allergy and Infectious Diseases (U01AI089244; R21NS065713; K23AI073192; T32AI055433) and Wellcome Trust (081667, to GM). Disclosures The authors have no other reported conflicts of interest References 1. Brouwer AE, Rajanuwong A, Chierakul W, et al. Combination antifungal therapies for HIV-associated cryptococcal meningitis: a randomised trial. Lancet 2004; 363: Heyderman RS, Gangaidzo IT, Hakim JG, et al. Cryptococcal meningitis in human immunodeficiency virusinfected patients in Harare, Zimbabwe. Clin. Infect. Dis. 1998; 26: Jarvis JN, Meintjes G, Williams Z, Rebe K, Harrison TS. Symptomatic relapse of HIV-associated cryptococcal meningitis in South Africa: the role of inadequate secondary prophylaxis. South African Med. J. 2010; 100: Jarvis JN, Bicanic T, Loyse A, et al. Determinants of Mortality in a Combined Cohort of 501 Patients With HIV-Associated Cryptococcal Meningitis: Implications for Improving Outcomes. Clin. Infect. Dis. 2013; : Kambugu A, Meya DB, Rhein J, et al. Outcomes of cryptococcal meningitis in Uganda before and after the availability of highly active antiretroviral therapy. Clin. Infect. Dis. 2008; 46: Kisenge PR, Hawkins AT, Maro VP, et al. Low CD4 count plus coma predicts cryptococcal meningitis in Tanzania. BMC Infect. Dis. 2007; 7: Loyse A, Wilson D, Meintjes G, et al. Comparison of the early fungicidal activity of high-dose fluconazole, voriconazole, and flucytosine as second-line drugs given in combination with amphotericin B for the treatment of HIV-associated cryptococcal meningitis. Clin. Infect. Dis. 2012; 54: McCarthy KM, Morgan J, Wannemuehler KA, et al. Population-based surveillance for cryptococcosis in an antiretroviral-naive South African province with a high HIV seroprevalence. AIDS 2006; 20: Mwaba P, Mwansa J, Chintu C, et al. Clinical presentation, natural history, and cumulative death rates of 230 adults with primary cryptococcal meningitis in Zambian AIDS patients treated under local conditions. Postgrad. Med. J. 2001; 77: Van Der Horst C, Saag M, Cloud G, et al. Treatment of Cryptococcal Meningitis Associated with the Acquired Immunodeficiency Syndrome. N. Engl. J. Med. 1997; 337:15 21.
13 Graybill JR, Sobel J, Saag M, et al. Diagnosis and management of increased intracranial pressure in patients with AIDS and cryptococcal meningitis. The NIAID Mycoses Study Group and AIDS Cooperative Treatment Groups. Clin. Infect. Dis. 2000; 30: Fessler R, Sobel J, Guyot L, et al. Management of Elevated Intracranial Pressure in Patients with Cryptococcal Meningitis. J. Acquir. Immune Defic. Syndr. 1998; 17: World Health Organization. Rapid advice: Diagnosis, Prevention and Management of Cryptococcal disease in HIV-infected adult, adolescents and children. Geneva: Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2010; 50: Bicanic T, Brouwer AE, Meintjes G, et al. Relationship of cerebrospinal fluid pressure, fungal burden and outcome in patients with cryptococcal meningitis undergoing serial lumbar punctures. AIDS 2009; 23: Schaars CF, Meintjes GA, Morroni C, Post FA, Maartens G. Outcome of AIDS-associated cryptococcal meningitis initially treated with 200 mg/day or 400 mg/day of fluconazole. BMC Infect. Dis. 2006; 6: Meda J, Kalluvya S, Downs JA, et al. Cryptococcal Meningitis Management in Tanzania with Strict Schedule of Serial Lumber Punctures using Intravenous Tubing Sets: an Operational Research Study. J. Acquir. Immune Defic. Syndr. Hum. Retrovirology 2014; :Publish Ahead of Print. 18. Zou G. A Modified Poisson Regression Approach to Prospective Studies with Binary Data. Am. J. Epidemiol. 2004; 159: Spiegelman D, Hertzmark E. Easy SAS calculations for risk or prevalence ratios and differences. Am. J. Epidemiol. 2005; 162: Rothman KJ, Greenland S, Lash TL. Modern Epidemiology. 3rd ed. Wolters Kluwer Health/Lippincott Williams & Wilkins, Denning D, Armstrong R, Lewis B, Stevens D. Elevated Cerebrospinal Fluid Pressures in Patients with Cryptococcal Meningitis and Acquired Immunodeficiency Syndrome. Am. J. Med. 1991; 91: Loyse A, Wainwright H, Jarvis JN, et al. Histopathology of the arachnoid granulations and brain in HIVassociated cryptococcal meningitis: correlation with cerebrospinal fluid pressure. AIDS 2010; 24: Lee SC, Dickson DW, Casadevall A. Pathology of cryptococcal meningoencephalitis: analysis of 27 patients with pathogenetic implications. Hum. Pathol. 1996; 27: Shoham S, Cover C, Donegan N, Fulnecky E, Kumar P. Cryptococcus neoformans meningitis at 2 hospitals in Washington, D.C.: adherence of health care providers to published practice guidelines for the management of cryptococcal disease. Clin. Infect. Dis. 2005; 40: Harrison TS. The burden of HIV-associated cryptococcal disease. AIDS 2009; 23: Govender N, Meintjes GA, Bicanic T, et al. Guideline for the prevention, diagnosis and management of cryptococcal meningitis among HIV-infected persons: 2013 update. SAJHIVMED 2013; 14:76 86.
14 14 Table 1: Baseline characteristics and mortality by therapeutic lumbar punctures among HIV-infected individuals with cryptococcal meningitis in South Africa and Uganda. At least one therapeutic LP No therapeutic LP N with data Median [IQR] Median [IQR] N with data or N (%) a or N (%) a N per group 75 (30%) 173 (70%) Follow-up time (days) 7 [6, 9] 7 [6, 8] P-value Site c Kampala 61 (34%) 120 (66%) Mbarara 4 (11%) 34 (89%) Cape Town 10 (35%) 19 (65%) Age (years) [29, 40] [30, 42] 0.15 Males (59%) (53%) 0.38 Weight (kg) [46, 62] [45, 57] 0.08 Missing weight (43%) (30%) 0.05 Headache duration < 7 days 8 (11%) 18 (11%) 7-13 days 27 (38%) 50 (30%) days 16 (22%) 35 (21%) 21 days 21 (29%) 66 (39%) Papilledema 71 0 (0%) (5%) 0.06 Karnofsky Score [40, 50] [40, 60] 0.16 Glasgow Coma Scale < (35%) (26%) 0.15 Heart rate (per minute) [66, 90] [72, 97] 0.01 Respiratory rate (per minute) [20, 24] [20, 24] 0.4 Temperature > 37.5 o C, axillary 74 9 (12%) (23%) 0.04 Clinical Laboratory Values Hemoglobin (g/dl) [9.4, 13.0] [8.9, 13.0] 0.41 Creatinine (mg/dl) [0.5, 0.8] [0.6, 0.9] 0.03 CSF Parameters Opening pressure (mmh 2 O) [220, 440] [150, 338] <0.001 Opening pressure >250 mmh 2 O (70%) (50%) Closing pressure (mmh 2 O) [80, 137] [60, 120] 0.04 Amount of CSF removed (ml) [12, 27] [8, 20] <0.001 b
15 15 Quantitative cryptococcal CSF culture (log 10 CFU/mL) [4.4, 5.6] [3.9, 5.5] 0.03 White blood cells (/μl of CSF) d [36, 310] [25, 135] 0.08 White blood cells < 5 cells/μl (46%) (42%) 0.55 Outcome Died 75 5 (7%) (18%) Mortality rate (per 100 persondays) e (95% CI: ) (95% CI: ) a Median and interquartile range (IQR). Frequency and percentages are column percentages. b P values from chi-square test for frequencies and Wilcoxon rank-sum test for medians. c Row percentages are presented. d Among those with detectable CSF white blood cell count ( 5 cells/μl). e All individuals contributed person-time to the no therapeutic LP group until he/she received a therapeutic LP, at which point the individual contributed person-time to the therapeutic LP group. Total follow-up time was 395 person-days after individuals received their first therapeutic LP and 1,314 persondays prior to the first therapeutic LP. Confidence intervals (CI) are exact CIs and P value from a crude, unweighted Poisson regression model.
16 16 Table 2: Baseline characteristics by vital status among HIV-infected individuals with cryptococcal meningitis in South Africa and Uganda. Died N with data Median [IQR] or N (%) a Survived Observation N with data Median [IQR] or N (%) a P-value b N per group 36 (15%) 212 (85%) Follow-up time (days) 4 [2, 6] 7 [6,8] Site c Kampala 31 (17%) 150 (82%) Mbarara 3 (8%) 35 (92%) Cape Town 2 (7%) 27 (93%) Age (years) [30, 44] [29, 40] 0.10 Males, N (%) (56%) (54%) 0.88 Weight (kg) [40.0, 54.0] [46.0, 59.7] Missing weight (58%) (30%) Karnofsky Score [40, 50] [40, 60] 0.02 Glasgow Coma Scale < (44%) (26%) 0.03 Heart rate (per minute) [76, 106] [70, 90] Respiratory rate (per minute) [20, 26] [20, 24] 0.03 CSF Parameters Opening Pressure (mmh 2 O) [150, 392] [180, 370] 0.92 Opening pressure >250 mmh 2 O (59%) (56%) 0.74 Closing pressure (mmh 2 O) (54, 110) (70, 130) 0.08 Amount of CSF removed (ml) (10,23) (10, 23) 0.47 Quantitative cryptococcal CSF culture (log 10 CFU/mL) [4.6, 5.8] [4.0, 5.5] 0.04 White blood cells (/μl of CSF) d [25, 135] [30, 180] 0.35 White blood cells < 5 cells/μl (55%) (41%) 0.15 a Median and interquartile range (IQR). Frequency and percentages are column percentages. b P values from chi-square test for frequencies and Wilcoxon rank-sum test for medians. c Row percentages are presented. d Among those with detectable CSF white blood cell count ( 5 cells/μl).
17 17 Table 3: Estimated relative risk of acute mortality after receiving a therapeutic lumbar puncture in HIVinfected individuals with cryptococcal meningitis in South Africa and Uganda. Relative Risk 95% CI Mean sw i (sd) a Crude, unweighted model 0.53 (0.20, 1.37) -- Marginal Structural Model Pooled Poisson Regression b Adjusted model (0.19, 1.32) 1.01 (0.22) Adjusted model (0.14, 1.07) 1.01 (0.29) Adjusted model (0.12, 0.82) 1.02 (0.52) Confidence interval (CI); Glasgow Coma Score (GCS); stabilized weight (sw i ); standard deviation (sd). a Stabilized weights (sw i ) are the product of the stabilized exposure and stabilized censoring weights. b Adjusted model 1 is adjusted for heart rate. Adjusted model 2 is adjusted model 1 additionally adjusted for CSF fungal burden. Adjusted model 3 is adjusted model 2 additionally adjusted with an indicator for GCS <15.
18 18 Table 4: Association of therapeutic lumbar puncture and acute mortality in HIV-infected individuals with cryptococcal meningitis by baseline CSF opening pressure. Baseline CSF opening pressure < 250 mmh 2 O At least one therapeutic LP No therapeutic LP Overall Number of individuals (% of overall) 21 (23%) 70 (77%) 91 Deaths, N (%) 0 (0%) 11 (16%) 11 (12%) Person-days of observation Mortality rate (per 100 person-days) Unadjusted relative risk (95% CI) Baseline CSF opening pressure 250 mmh 2 O 0.00 [0.00, 2.25] a Number of individuals (% of overall) 48 (41%) 69 (59%) 117 Deaths, N (%) 4 (8%) 12 (17%) 16 (14%) Person-days of observation Mortality rate (per 100 person-days) Unadjusted relative risk (95% CI) 0.65 [0.15, 2.14] Baseline CSF opening pressure not available Number of individuals (% of overall) 6 (15%) 34 (85%) 40 Deaths, N (%) 1 (17%) 8 (24%) 9 (23%) Person-days of observation Mortality rate (per 100 person-days) Unadjusted relative risk (95% CI) 1.13 [0.03, 8.42] Lumbar puncture (LP); confidence interval (CI). a A value of 0.5 was added to both the numerator and denominator for the group with at least one therapeutic LP in order to estimate the rate and confidence intervals.
19 19 Figure Legends: Figure 1: Selection of cohort participants among HIV-infected individuals in South Africa and Uganda screened for cryptococcal meningitis. Figure 2: Time of the first therapeutic lumbar puncture (LP) in days from diagnosis of cryptococcal meningitis, among 75 HIV-infected individuals in South Africa and Uganda who received at least one LP after an initial diagnostic LP. The median time after diagnosis until the first therapeutic LP was 3 days. Figure 3: The distribution of time to death among those with and without at least one therapeutic lumbar puncture (LP) among HIV-infected individuals with cryptococcal meningitis in South Africa and Uganda. A total of 36 deaths occurred within 11 days after diagnosis with cryptococcal meningitis. The overall median time to death was 4 days after diagnosis.
20 20
21 21
22 22
Treatment of Cryptococcal Meningitis. Graeme Meintjes University of Cape Town GF Jooste Hospital Imperial College London
 Treatment of Cryptococcal Meningitis Graeme Meintjes University of Cape Town GF Jooste Hospital Imperial College London Cryptococcal meningitis Predominantly in HIV infected patients with CD4 < 200 Studies
Treatment of Cryptococcal Meningitis Graeme Meintjes University of Cape Town GF Jooste Hospital Imperial College London Cryptococcal meningitis Predominantly in HIV infected patients with CD4 < 200 Studies
Reproducibility of CSF quantitative culture methods for estimating rate of clearance in cryptococcal meningitis
 Medical Mycology, 2016, 54, 361 369 doi: 10.1093/mmy/myv104 Advance Access Publication Date: 14 January 2016 Original Article Original Article Reproducibility of CSF quantitative culture methods for estimating
Medical Mycology, 2016, 54, 361 369 doi: 10.1093/mmy/myv104 Advance Access Publication Date: 14 January 2016 Original Article Original Article Reproducibility of CSF quantitative culture methods for estimating
HIV-associated Cryptococcal Meningitis in sub-saharan Africa: Factors affecting short and long-term survival
 HIV-associated Cryptococcal Meningitis in sub-saharan Africa: Factors affecting short and long-term survival A DISSERTATION SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY OF MINNESOTA
HIV-associated Cryptococcal Meningitis in sub-saharan Africa: Factors affecting short and long-term survival A DISSERTATION SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY OF MINNESOTA
Dr. Andrew D Kambugu The Infectious Diseases Institute, Makerere University College of Health Sciences
 The Future of Antiretroviral Therapy in Africa: Perspectives from Uganda Dr. Andrew D Kambugu The Infectious Diseases Institute, Makerere University College of Health Sciences Discussion Outline A. Characteristics
The Future of Antiretroviral Therapy in Africa: Perspectives from Uganda Dr. Andrew D Kambugu The Infectious Diseases Institute, Makerere University College of Health Sciences Discussion Outline A. Characteristics
Timing of Antiretroviral Therapy after Diagnosis of Cryptococcal Meningitis
 The new england journal of medicine original article Timing of Antiretroviral Therapy after Diagnosis of Cryptococcal Meningitis David R. Boulware, M.D., M.P.H., David B. Meya, M.Med., Conrad Muzoora,
The new england journal of medicine original article Timing of Antiretroviral Therapy after Diagnosis of Cryptococcal Meningitis David R. Boulware, M.D., M.P.H., David B. Meya, M.Med., Conrad Muzoora,
Cryptococcal Antigen Screening: Perspectives from Uganda. Dr. David Meya, MMed Dr. David Boulware, MD MPH ASLM, Capetown 2012
 Cryptococcal Antigen Screening: Perspectives from Uganda Dr. David Meya, MMed Dr. David Boulware, MD MPH ASLM, Capetown 2012 Introduction Globally, an estimated 957,900 cases of cryptococcal meningitis
Cryptococcal Antigen Screening: Perspectives from Uganda Dr. David Meya, MMed Dr. David Boulware, MD MPH ASLM, Capetown 2012 Introduction Globally, an estimated 957,900 cases of cryptococcal meningitis
Timing of ART in patients with opportunistic infections
 Timing of ART in patients with opportunistic infections Graeme Meintjes University of Cape Town Imperial College London HIV Congress 2014, Taj Lands End Hotel, Mumbai, 22 March 2014 OUTLINE Yesterday Prof
Timing of ART in patients with opportunistic infections Graeme Meintjes University of Cape Town Imperial College London HIV Congress 2014, Taj Lands End Hotel, Mumbai, 22 March 2014 OUTLINE Yesterday Prof
MAJOR ARTICLE. amphotericin; cryptococcal meningitis; HIV/AIDS; potassium; side effect. Keywords.
 MAJOR ARTICLE Standardized Electrolyte Supplementation and Fluid Management Improves Survival During Amphotericin Therapy for Cryptococcal Meningitis in Resource-Limited Settings Nathan C. Bahr, 1,2,3
MAJOR ARTICLE Standardized Electrolyte Supplementation and Fluid Management Improves Survival During Amphotericin Therapy for Cryptococcal Meningitis in Resource-Limited Settings Nathan C. Bahr, 1,2,3
Downloaded from:
 Jarvis, JN; Meintjes, G; Williams, Z; Rebe, K; Harrison, TS (2010) Symptomatic relapse of HIV-associated cryptococcal meningitis in South Africa: the role of inadequate secondary prophylaxis. South African
Jarvis, JN; Meintjes, G; Williams, Z; Rebe, K; Harrison, TS (2010) Symptomatic relapse of HIV-associated cryptococcal meningitis in South Africa: the role of inadequate secondary prophylaxis. South African
High-Dose Amphotericin B with Flucytosine for the Treatment of Cryptococcal Meningitis in HIV-Infected Patients: A Randomized Trial
 MAJOR ARTICLE HIV/AIDS High-Dose Amphotericin B with Flucytosine for the Treatment of Cryptococcal Meningitis in HIV-Infected Patients: A Randomized Trial Tihana Bicanic, 1,4 Robin Wood, 1 Graeme Meintjes,
MAJOR ARTICLE HIV/AIDS High-Dose Amphotericin B with Flucytosine for the Treatment of Cryptococcal Meningitis in HIV-Infected Patients: A Randomized Trial Tihana Bicanic, 1,4 Robin Wood, 1 Graeme Meintjes,
Determinants of Mortality in a Combined Cohort of 501 Patients With HIV-Associated Cryptococcal Meningitis: Implications for Improving Outcomes
 Clinical Infectious Diseases Advance Access published December 26, 2013 MAJOR ARTICLE HIV/AIDS Determinants of Mortality in a Combined Cohort of 501 Patients With HIV-Associated Cryptococcal Meningitis:
Clinical Infectious Diseases Advance Access published December 26, 2013 MAJOR ARTICLE HIV/AIDS Determinants of Mortality in a Combined Cohort of 501 Patients With HIV-Associated Cryptococcal Meningitis:
Challenges in diagnosis and management of Cryptococcal immune reconstitution inflammatory syndrome (IRIS) in resource limited settings
 in resource limited settings") Challenges in diagnosis and management of Cryptococcal immune reconstitution inflammatory syndrome (IRIS) in resource limited settings Musubire AK 1, Meya BD 1,2,3, Mayanja-Kizza H 3, Lukande R 4, Wiesner
Challenges in diagnosis and management of Cryptococcal immune reconstitution inflammatory syndrome (IRIS) in resource limited settings Musubire AK 1, Meya BD 1,2,3, Mayanja-Kizza H 3, Lukande R 4, Wiesner
THE PREVALENCE, CLINICAL FEATURES, RISK FACTORS AND OUTCOME ASSOCIATED WITH CRYPTOCOCCAL MENINGITIS IN HIV POSITIVE PATIENTS IN KENYA
 December 2010 Ea s t Af r i c a n Me d i c a l Jo u r n a l 481 East African Medical Journal Vol. 87 No. 12 December 2010 THE PREVALENCE, CLINICAL FEATURES, RISK FACTORS AND OUTCOME ASSOCIATED WITH CRYPTOCOCCAL
December 2010 Ea s t Af r i c a n Me d i c a l Jo u r n a l 481 East African Medical Journal Vol. 87 No. 12 December 2010 THE PREVALENCE, CLINICAL FEATURES, RISK FACTORS AND OUTCOME ASSOCIATED WITH CRYPTOCOCCAL
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Boulware DR, Meya DB, Muzoora C, et al. Timing of antiretroviral
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Boulware DR, Meya DB, Muzoora C, et al. Timing of antiretroviral
Title: Evaluation of a Point-of-Care Immunoassay Test Kit StrongStep for Cryptococcal Antigen Detection
 Title: Evaluation of a Point-of-Care Immunoassay Test Kit StrongStep for Cryptococcal Antigen Detection Edward Mpoza 1, Liliane Mukaremera 1,3, Lillian Tugume 1, Reuben Kiggundu 1, Didas Atwebembere Kundura
Title: Evaluation of a Point-of-Care Immunoassay Test Kit StrongStep for Cryptococcal Antigen Detection Edward Mpoza 1, Liliane Mukaremera 1,3, Lillian Tugume 1, Reuben Kiggundu 1, Didas Atwebembere Kundura
MDS Mentorship Experience
 MDS Mentorship Experience MENTOR: CARRIE KOVARIK, MD UNIVERSITY OF PENNSYLVANIA MENTEE: MONICA RANI, MD UNIVERSITY OF MINNESOTA NORTHWESTERN UNIVERSITY From Philadelphia ------ > Kampala, Uganda COAT
MDS Mentorship Experience MENTOR: CARRIE KOVARIK, MD UNIVERSITY OF PENNSYLVANIA MENTEE: MONICA RANI, MD UNIVERSITY OF MINNESOTA NORTHWESTERN UNIVERSITY From Philadelphia ------ > Kampala, Uganda COAT
Clinical Infectious Diseases Advance Access published December 6, 2013
 Clinical Infectious Diseases Advance Access published December 6, 2013 1 Determinants of Mortality in a Combined Cohort of 501 Patients with HIVassociated Cryptococcal Meningitis: Implications for Improving
Clinical Infectious Diseases Advance Access published December 6, 2013 1 Determinants of Mortality in a Combined Cohort of 501 Patients with HIVassociated Cryptococcal Meningitis: Implications for Improving
Management of Cryptococcal Meningitis in HIV-infected children in National Pediatric Hospital
 Management of Cryptococcal Meningitis in HIV-infected children in National Pediatric Hospital Olivier Marcy 1,2, Sam Sophan 2, Ung Vibol 2, Chan Bunthy 2, Pok Moroun 2, Chy Kam Hoy 2, Ban Thy 2, Chhour
Management of Cryptococcal Meningitis in HIV-infected children in National Pediatric Hospital Olivier Marcy 1,2, Sam Sophan 2, Ung Vibol 2, Chan Bunthy 2, Pok Moroun 2, Chy Kam Hoy 2, Ban Thy 2, Chhour
Original Article. Noparat Oniem, M.D., Somnuek Sungkanuparph, M.D.
 Original Article Vol. 29 No. 1 Primary prophylaxis for cryptococcosis with fluconazole:- Oniem N & Sungkanuparph S. 5 Primary prophylaxis for cryptococcosis with fluconazole among HIV-infected patients
Original Article Vol. 29 No. 1 Primary prophylaxis for cryptococcosis with fluconazole:- Oniem N & Sungkanuparph S. 5 Primary prophylaxis for cryptococcosis with fluconazole among HIV-infected patients
Early versus Delayed Initiation of Antiretroviral Therapy for Concurrent HIV Infection and Cryptococcal Meningitis in Sub-Saharan Africa
 HIV/AIDS MAJOR ARTICLE Early versus Delayed Initiation of Antiretroviral Therapy for Concurrent HIV Infection and Cryptococcal Meningitis in Sub-Saharan Africa Azure T. Makadzange, 1,3 Chiratidzo E. Ndhlovu,
HIV/AIDS MAJOR ARTICLE Early versus Delayed Initiation of Antiretroviral Therapy for Concurrent HIV Infection and Cryptococcal Meningitis in Sub-Saharan Africa Azure T. Makadzange, 1,3 Chiratidzo E. Ndhlovu,
Opportunities for improvement
 Are there opportunities to manage cryptococcal meningitis better? Signals High-quality evidence Nelesh Govender National Institute for Communicable Diseases Inclusion in guidelines Translation into clinical
Are there opportunities to manage cryptococcal meningitis better? Signals High-quality evidence Nelesh Govender National Institute for Communicable Diseases Inclusion in guidelines Translation into clinical
Downloaded from:
 Patel, Raju KK; Leeme, Tshepo; Azzo, Caitlin; Tlhako, Nametso; Tsholo, Katlego; Tawanana, Ephraim O; Molefi, Mooketsi; Mosepele, Mosepele; Lawrence, David S; Mokomane, Margaret; Tenforde, Mark W; Jarvis,
Patel, Raju KK; Leeme, Tshepo; Azzo, Caitlin; Tlhako, Nametso; Tsholo, Katlego; Tawanana, Ephraim O; Molefi, Mooketsi; Mosepele, Mosepele; Lawrence, David S; Mokomane, Margaret; Tenforde, Mark W; Jarvis,
A Case of Cryptococcal Meningitis
 A Case of Cryptococcal Meningitis DOUGLAS FISH ALBANY MEDICAL COLLEGE JUNE 4, 2013 History Patient transferred from Columbia Memorial Hospital with lethargy, shortness of breath, chest pains and failure
A Case of Cryptococcal Meningitis DOUGLAS FISH ALBANY MEDICAL COLLEGE JUNE 4, 2013 History Patient transferred from Columbia Memorial Hospital with lethargy, shortness of breath, chest pains and failure
GAFFI Fact Sheet. Cryptococcal meningitis. Introduction
 GAFFI Fact Sheet Cryptococcal meningitis ION NS ACT ALOR ECTIO B GLOND F L INF FU NGA FU Introduction DARKER AREAS AND TEXT FIT WITHIN CIRCLE Cryptococcal meningitis is caused by one of the two closely
GAFFI Fact Sheet Cryptococcal meningitis ION NS ACT ALOR ECTIO B GLOND F L INF FU NGA FU Introduction DARKER AREAS AND TEXT FIT WITHIN CIRCLE Cryptococcal meningitis is caused by one of the two closely
and the Working Group from the EMBO-AIDS Related Mycoses Workshop Institute of Infectious Disease and Molecular Medicine, University of Cape Town,
 1 AIDS-related mycoses: the way forward Gordon D. Brown 1,2*, Graeme Meintjes 1, Jay K. Kolls 3, Clive Gray 1, William Horsnell 1 and the Working Group from the EMBO-AIDS Related Mycoses Workshop 1 Institute
1 AIDS-related mycoses: the way forward Gordon D. Brown 1,2*, Graeme Meintjes 1, Jay K. Kolls 3, Clive Gray 1, William Horsnell 1 and the Working Group from the EMBO-AIDS Related Mycoses Workshop 1 Institute
Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease
 Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease Assist Prof. Somnuek Sungkanuparph Division of Infectious Diseases Faculty of Medicine Ramathibodi Hospital Mahidol
Cryptococcosis of the Central Nervous System: Classical and Immune-Reconstitution Disease Assist Prof. Somnuek Sungkanuparph Division of Infectious Diseases Faculty of Medicine Ramathibodi Hospital Mahidol
Challenges in Management of Cryptococcal Meningitis. Yunus Moosa Department of ID NRMSM Durban
 Challenges in Management of Cryptococcal Meningitis Yunus Moosa Department of ID NRMSM Durban Overview Epidemiology Pathogenesis Clinical presentation Diagnosis Prognostic factors Antifungal Treatment
Challenges in Management of Cryptococcal Meningitis Yunus Moosa Department of ID NRMSM Durban Overview Epidemiology Pathogenesis Clinical presentation Diagnosis Prognostic factors Antifungal Treatment
Cryptococcal antigen prevalence in HIV-infected Tanzanians: a cross-sectional study and evaluation of a point-of-care lateral flow assay
 Tropical Medicine and International Health doi:10.1111/tmi.12157 volume 18 no 9 pp 1075 1079 september 2013 Short Communication Cryptococcal antigen prevalence in HIV-infected Tanzanians: a cross-sectional
Tropical Medicine and International Health doi:10.1111/tmi.12157 volume 18 no 9 pp 1075 1079 september 2013 Short Communication Cryptococcal antigen prevalence in HIV-infected Tanzanians: a cross-sectional
Human Immune Response Varies by the Degree of Relative Cryptococcal Antigen Shedding
 Open Forum Infectious Diseases MAJOR ARTICLE Human Immune Response Varies by the Degree of Relative Cryptococcal Antigen Shedding David R. Boulware, 1,2,a Maximilian von Hohenberg, 1,a Melissa A. Rolfes,
Open Forum Infectious Diseases MAJOR ARTICLE Human Immune Response Varies by the Degree of Relative Cryptococcal Antigen Shedding David R. Boulware, 1,2,a Maximilian von Hohenberg, 1,a Melissa A. Rolfes,
Comparison of Clinical Features and Survival between Cryptococcosis in Human Immunodeficiency Virus (HIV)-Positive and HIV-Negative Patients
-Positive and HIV-Negative Patients") Jpn. J. Infect. Dis., 61, 111-115, 2008 Original Article Comparison of Clinical Features and Survival between Cryptococcosis in Human Immunodeficiency Virus (HIV)-Positive and HIV-Negative Patients Ubonvan
Jpn. J. Infect. Dis., 61, 111-115, 2008 Original Article Comparison of Clinical Features and Survival between Cryptococcosis in Human Immunodeficiency Virus (HIV)-Positive and HIV-Negative Patients Ubonvan
Seroprevalence of histoplasmosis in Kampala, Uganda
 Medical Mycology, 2016, 54, 295 300 doi: 10.1093/mmy/myv081 Advance Access Publication Date: 2 November 2015 Original Article Original Article Seroprevalence of histoplasmosis in Kampala, Uganda Nathan
Medical Mycology, 2016, 54, 295 300 doi: 10.1093/mmy/myv081 Advance Access Publication Date: 2 November 2015 Original Article Original Article Seroprevalence of histoplasmosis in Kampala, Uganda Nathan
CRYPTOCOCCAL MENINGITIS IN HIV-INFECTED PATIENTS AT CHIANG MAI UNIVERSITY HOSPITAL: A RETROSPECTIVE STUDY
 CRYPTOCOCCAL MENINGITIS IN HIV-INFECTED PATIENTS AT CHIANG MAI UNIVERSITY HOSPITAL: A RETROSPECTIVE STUDY Romanee Chaiwarith 1, Surachet Vongsanim 1 and Khuanchai Supparatpinyo 1, 2 1 Department of Medicine,
CRYPTOCOCCAL MENINGITIS IN HIV-INFECTED PATIENTS AT CHIANG MAI UNIVERSITY HOSPITAL: A RETROSPECTIVE STUDY Romanee Chaiwarith 1, Surachet Vongsanim 1 and Khuanchai Supparatpinyo 1, 2 1 Department of Medicine,
Downloaded from:
 Lightowler, JV; Cooke, GS; Mutevedzi, P; Lessells, RJ; Newell, ML; Dedicoat, M (2010) Treatment of cryptococcal meningitis in KwaZulu- Natal, South Africa. PLoS One, 5 (1). e8630. ISSN 1932-6203 DOI: 10.1371/journal.pone.0008630
Lightowler, JV; Cooke, GS; Mutevedzi, P; Lessells, RJ; Newell, ML; Dedicoat, M (2010) Treatment of cryptococcal meningitis in KwaZulu- Natal, South Africa. PLoS One, 5 (1). e8630. ISSN 1932-6203 DOI: 10.1371/journal.pone.0008630
Six-month outcomes of HIV-infected patients given short-course fluconazole therapy for asymptomatic cryptococcal antigenemia
 CONCISE COMMUNICATION Six-month outcomes of HIV-infected patients given short-course fluconazole therapy for asymptomatic cryptococcal antigenemia Shikha W. Kapoor a, Kinanga A. Magambo a, Samuel E. Kalluvya
CONCISE COMMUNICATION Six-month outcomes of HIV-infected patients given short-course fluconazole therapy for asymptomatic cryptococcal antigenemia Shikha W. Kapoor a, Kinanga A. Magambo a, Samuel E. Kalluvya
Cryptococcal Meningitis: Diagnosis and Management Update
 Curr Trop Med Rep (2015) 2:90 99 DOI 10.1007/s40475-015-0046-y TROPICAL MYCOSIS (D BOULWARE, SECTION EDITOR) Cryptococcal Meningitis: Diagnosis and Management Update Mahsa Abassi 1,2 & David R. Boulware
Curr Trop Med Rep (2015) 2:90 99 DOI 10.1007/s40475-015-0046-y TROPICAL MYCOSIS (D BOULWARE, SECTION EDITOR) Cryptococcal Meningitis: Diagnosis and Management Update Mahsa Abassi 1,2 & David R. Boulware
Cryptococcal Meningitis in Patients with or without Human Immunodeficiency Virus: Experience in a Tertiary Hospital
 Original Article DOI 10.3349/ymj.2011.52.3.482 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 52(3):482-487, 2011 Cryptococcal Meningitis in Patients with or without Human Immunodeficiency Virus: Experience
Original Article DOI 10.3349/ymj.2011.52.3.482 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 52(3):482-487, 2011 Cryptococcal Meningitis in Patients with or without Human Immunodeficiency Virus: Experience
Management of cryptococcal meningitis in HIVinfected patients: Experience from western India
 Original Article Management of cryptococcal meningitis in HIVinfected patients: Experience from western India Atul K. Patel, Ketan K. Patel, Rajiv Ranjan, Shalin Shah 2, Jagdish K. Patel 1 Infectious Diseases
Original Article Management of cryptococcal meningitis in HIVinfected patients: Experience from western India Atul K. Patel, Ketan K. Patel, Rajiv Ranjan, Shalin Shah 2, Jagdish K. Patel 1 Infectious Diseases
Te-Yu Lin, Kuo-Ming Yeh, Jung-Chung Lin, Ning-Chi Wang, Ming-Yieh Peng, Feng-Yee Chang
 J Microbiol Immunol Infect. 9;:-6 Cryptococcal disease in patients with or without human immunodeficiency virus: clinical presentation and monitoring of serum cryptococcal antigen titers Te-Yu Lin, Kuo-Ming
J Microbiol Immunol Infect. 9;:-6 Cryptococcal disease in patients with or without human immunodeficiency virus: clinical presentation and monitoring of serum cryptococcal antigen titers Te-Yu Lin, Kuo-Ming
Diagnostic and therapeutic strategies in cryptococcosis: impact on outcome
 REVIEW Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 113(7): e180050, 2018 1 6 Diagnostic and therapeutic strategies in cryptococcosis: impact on outcome Timothée Boyer Chammard 1, Elvis Temfack 2, Olivier
REVIEW Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 113(7): e180050, 2018 1 6 Diagnostic and therapeutic strategies in cryptococcosis: impact on outcome Timothée Boyer Chammard 1, Elvis Temfack 2, Olivier
Fungal Meningitis. Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse Bern
 Fungal Meningitis Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse 51 3010 Bern Death due to infectious diseases in sub-saharan Africa Park BJ. Et al AIDS 2009;23:525
Fungal Meningitis Stefan Zimmerli Institute for infectious diseases University of Bern Friedbühlstrasse 51 3010 Bern Death due to infectious diseases in sub-saharan Africa Park BJ. Et al AIDS 2009;23:525
ISPUB.COM. Cryptococcal Meningitis in AIDS. O Busari, A Adeyemi, S Agboola INTRODUCTION BIOLOGY AND PATHOGENESIS CLINICAL FEATURES
 ISPUB.COM The Internet Journal of Infectious Diseases Volume 7 Number 1 O Busari, A Adeyemi, S Agboola Citation O Busari, A Adeyemi, S Agboola.. The Internet Journal of Infectious Diseases. 2008 Volume
ISPUB.COM The Internet Journal of Infectious Diseases Volume 7 Number 1 O Busari, A Adeyemi, S Agboola Citation O Busari, A Adeyemi, S Agboola.. The Internet Journal of Infectious Diseases. 2008 Volume
HIV-Associated Cryptococcal Meningitis: Bridging the Gap Between Developed and Resource-Limited Settings
 Curr Clin Micro Rpt (2016) 3:92 102 DOI 10.1007/s40588-016-0035-5 MYCOLOGY (J PERFECT, SECTION EDITOR) HIV-Associated Cryptococcal Meningitis: Bridging the Gap Between Developed and Resource-Limited Settings
Curr Clin Micro Rpt (2016) 3:92 102 DOI 10.1007/s40588-016-0035-5 MYCOLOGY (J PERFECT, SECTION EDITOR) HIV-Associated Cryptococcal Meningitis: Bridging the Gap Between Developed and Resource-Limited Settings
Cryptococcal meningitis in HIV infected: Experience from a North Indian tertiary center
 Original Article Cryptococcal meningitis in HIV infected: Experience from a North Indian tertiary center Susheel Kumar, Ajay Wanchu, Arunaloke Chakrabarti 1, Aman Sharma, Pradeep Bambery, Surjit Singh
Original Article Cryptococcal meningitis in HIV infected: Experience from a North Indian tertiary center Susheel Kumar, Ajay Wanchu, Arunaloke Chakrabarti 1, Aman Sharma, Pradeep Bambery, Surjit Singh
Cost-effectiveness of CRAG-LFA screening for cryptococcal meningitis among people living with HIV in Uganda
 Ramachandran et al. BMC Infectious Diseases (2017) 17:225 DOI 10.1186/s12879-017-2325-9 RESEARCH ARTICLE Open Access Cost-effectiveness of CRAG-LFA screening for cryptococcal meningitis among people living
Ramachandran et al. BMC Infectious Diseases (2017) 17:225 DOI 10.1186/s12879-017-2325-9 RESEARCH ARTICLE Open Access Cost-effectiveness of CRAG-LFA screening for cryptococcal meningitis among people living
KAP conference 19 th March 2008: Dr Mohamed Hussein Jin.
 SENSITIVITY PATTERNS, SEROTYPES OF CRYPTOCOCCUS NEOFORMANS AND DIAGNOSTIC VALUE OF INDIA INK IN PATIENTS WITH CRYPTOCOCCAL MENINGITIS AT KENYATTA NATIONAL HOSPITAL. KAP conference 19 th March 2008: Dr
SENSITIVITY PATTERNS, SEROTYPES OF CRYPTOCOCCUS NEOFORMANS AND DIAGNOSTIC VALUE OF INDIA INK IN PATIENTS WITH CRYPTOCOCCAL MENINGITIS AT KENYATTA NATIONAL HOSPITAL. KAP conference 19 th March 2008: Dr
Cryptococcal Meningitis
 Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
Cryptococcal Meningitis Dr N Thumbiran Infectious Diseases Department UKZN Index patient 27 year old female Presented to King Edward Hospital on 17/07/2005 with: Severe headaches Vomiting Photophobia X
Copyright 2013 The Authors. Deposited on: 03 February 2014
 Robertson, E.J., Najjuka, G., Rolfes, M.A., Akampurira, A., Jain, N., Anantharanjit, J., von Hohenburg, M., Tassieri, M., Carlsson, A., Meya, D.B., Harrison, T.S., Fries, B., Boulware, D.R., and Bicanic,
Robertson, E.J., Najjuka, G., Rolfes, M.A., Akampurira, A., Jain, N., Anantharanjit, J., von Hohenburg, M., Tassieri, M., Carlsson, A., Meya, D.B., Harrison, T.S., Fries, B., Boulware, D.R., and Bicanic,
A retrospective review of paediatric. cryptococcosis in three academic. hospitals in Johannesburg,
 A retrospective review of paediatric cryptococcosis in three academic hospitals in Johannesburg, 2002-2011. Fikile Cynthia Mabena A dissertation submitted to the Faculty of Health Sciences, University
A retrospective review of paediatric cryptococcosis in three academic hospitals in Johannesburg, 2002-2011. Fikile Cynthia Mabena A dissertation submitted to the Faculty of Health Sciences, University
CRYPTOCOCCUS MENINGITIS IN A COHORT OF HIV POSITIVE KENYAN PATIENTS: OUTCOME AFTER TWO WEEKS OF THERAPY
 December 2013 (Supplement) Ea s t Af r i c a n Me d i c a l Jo u r n a l S33 East African Medical Journal Vol. 90 No. 12 (Supplement) December 2013 CRYPTOCOCCUS MENINGITIS IN A COHORT OF HIV POSITIVE KENYAN
December 2013 (Supplement) Ea s t Af r i c a n Me d i c a l Jo u r n a l S33 East African Medical Journal Vol. 90 No. 12 (Supplement) December 2013 CRYPTOCOCCUS MENINGITIS IN A COHORT OF HIV POSITIVE KENYAN
PREGNANCY OUTCOMES AMONG HIV-INFECTED WOMEN IN UGANDA AND ZIMBABWE
 PREGNANCY OUTCOMES AMONG HIV-INFECTED WOMEN IN UGANDA AND ZIMBABWE Kathryn Lancaster, MPH 3rd International Workshop on HIV & Women January 15, 2013 HIV among women of reproductive age Women of reproductive
PREGNANCY OUTCOMES AMONG HIV-INFECTED WOMEN IN UGANDA AND ZIMBABWE Kathryn Lancaster, MPH 3rd International Workshop on HIV & Women January 15, 2013 HIV among women of reproductive age Women of reproductive
CRYPTOCOCCOSIS IN HIV-INFECTED CHILDREN
 CRYPTOCOCCOSIS IN HIV-INFECTED CHILDREN Surachai Likasitwattanakul, Boonsom Poneprasert and Virat Sirisanthana Department of Pediatrics, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
CRYPTOCOCCOSIS IN HIV-INFECTED CHILDREN Surachai Likasitwattanakul, Boonsom Poneprasert and Virat Sirisanthana Department of Pediatrics, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand
Combination Antifungal Therapy for Cryptococcal Meningitis
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Combination Antifungal Therapy for Cryptococcal Meningitis Jeremy N. Day, M.D., Ph.D., Tran T.H. Chau, M.D., Ph.D., Marcel Wolbers,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article Combination Antifungal Therapy for Cryptococcal Meningitis Jeremy N. Day, M.D., Ph.D., Tran T.H. Chau, M.D., Ph.D., Marcel Wolbers,
Preventing HIV morbidity & mortality: fast-tracking infants on to ART
 Preventing HIV morbidity & mortality: fast-tracking infants on to ART Brian Eley Paediatric Infectious Diseases Unit Red Cross War Memorial Children s Hospital Department of Paediatrics & Child Health
Preventing HIV morbidity & mortality: fast-tracking infants on to ART Brian Eley Paediatric Infectious Diseases Unit Red Cross War Memorial Children s Hospital Department of Paediatrics & Child Health
Development of cryptococcal immune reconstitution inflammatory syndrome 41 months after the initiation of antiretroviral therapy in an AIDS patient
 DOI 10.1186/s12981-015-0075-6 CASE REPORT Open Access Development of cryptococcal immune reconstitution inflammatory syndrome 41 months after the initiation of antiretroviral therapy in an AIDS patient
DOI 10.1186/s12981-015-0075-6 CASE REPORT Open Access Development of cryptococcal immune reconstitution inflammatory syndrome 41 months after the initiation of antiretroviral therapy in an AIDS patient
Antifungal Combinations for Treatment of Cryptococcal Meningitis in Africa
 The new england journal of medicine Original Article Antifungal Combinations for Treatment of Cryptococcal Meningitis in Africa S.F. Molloy, C. Kanyama, R.S. Heyderman, A. Loyse, C. Kouanfack, D. Chanda,
The new england journal of medicine Original Article Antifungal Combinations for Treatment of Cryptococcal Meningitis in Africa S.F. Molloy, C. Kanyama, R.S. Heyderman, A. Loyse, C. Kouanfack, D. Chanda,
Matobogolo M. Boaz, 1 Samuel Kalluvya, 2,3 Jennifer A. Downs, 2,4 Bonaventura C. T. Mpondo, 1 and Stephen E. Mshana 5. 1.
 Tropical Medicine Volume 2016, Article ID 6573672, 7 pages http://dx.doi.org/10.1155/2016/6573672 Research Article Pattern, Clinical Characteristics, and Outcome of Meningitis among HIV-Infected Adults
Tropical Medicine Volume 2016, Article ID 6573672, 7 pages http://dx.doi.org/10.1155/2016/6573672 Research Article Pattern, Clinical Characteristics, and Outcome of Meningitis among HIV-Infected Adults
Point-of-Care Testing for Cryptococcal Disease among Hospitalized Human Immunodeficiency virus Infected Adults in Ethiopia
 Point-of-Care Testing for Cryptococcal Disease among Hospitalized Human Immunodeficiency virus Infected Adults in Ethiopia Admasu Tenna Mamuye, Addis Ababa University Ethan Bornstein, Emory University
Point-of-Care Testing for Cryptococcal Disease among Hospitalized Human Immunodeficiency virus Infected Adults in Ethiopia Admasu Tenna Mamuye, Addis Ababa University Ethan Bornstein, Emory University
Clinical Features and Serum Biomarkers in HIV Immune Reconstitution Inflammatory Syndrome after Cryptococcal Meningitis: A Prospective Cohort Study
 Clinical Features and Serum Biomarkers in HIV Immune Reconstitution Inflammatory Syndrome after Cryptococcal Meningitis: A Prospective Cohort Study David R. Boulware 1,2 *, David B. Meya 1,3, Tracy L.
Clinical Features and Serum Biomarkers in HIV Immune Reconstitution Inflammatory Syndrome after Cryptococcal Meningitis: A Prospective Cohort Study David R. Boulware 1,2 *, David B. Meya 1,3, Tracy L.
ORIGINAL ARTICLE STUDY OF CRYPTOCOCCAL MENINGITIS IN HIV POSITIVE PATIENTS
 STUDY OF CRYPTOCOCCAL MENINGITIS IN HIV POSITIVE PATIENTS Sunil Kumar 1, Madhu Jumla. 1. Assistant Professor, Department of Medicine, Vijayanagara Institute of Medical Sciences, Bellary, Karnataka.. Assistant
STUDY OF CRYPTOCOCCAL MENINGITIS IN HIV POSITIVE PATIENTS Sunil Kumar 1, Madhu Jumla. 1. Assistant Professor, Department of Medicine, Vijayanagara Institute of Medical Sciences, Bellary, Karnataka.. Assistant
Randomized Placebo-controlled Trial of Prednisone for the TB-Immune Reconstitution Inflammatory Syndrome
 Randomized Placebo-controlled Trial of Prednisone for the TB-Immune Reconstitution Inflammatory Syndrome Graeme Meintjes 1,2, Robert J Wilkinson 1,2,3,4, Chelsea Morroni 1, Dominique Pepper 1,2, Kevin
Randomized Placebo-controlled Trial of Prednisone for the TB-Immune Reconstitution Inflammatory Syndrome Graeme Meintjes 1,2, Robert J Wilkinson 1,2,3,4, Chelsea Morroni 1, Dominique Pepper 1,2, Kevin
Cryptococcal meningitis in HIV-infected patients: a longitudinal study in Cambodia
 Tropical Medicine and International Health doi:10.1111/j.1365-3156.2010.02622.x volume 15 no 11 pp 1375 1381 november 2010 Cryptococcal meningitis in HIV-infected patients: a longitudinal study in Cambodia
Tropical Medicine and International Health doi:10.1111/j.1365-3156.2010.02622.x volume 15 no 11 pp 1375 1381 november 2010 Cryptococcal meningitis in HIV-infected patients: a longitudinal study in Cambodia
Case : A 39-Year-Old Zimbabwean Man with a Severe Headache
 Founded by Richard C. Cabot Eric S. Rosenberg, M.D., Nancy Lee Harris, M.D., Editors Virginia M. Pierce, M.D., David M. Dudzinski, M.D., Meridale V. Baggett, M.D., Dennis C. Sgroi, M.D., Jo Anne O. Shepard,
Founded by Richard C. Cabot Eric S. Rosenberg, M.D., Nancy Lee Harris, M.D., Editors Virginia M. Pierce, M.D., David M. Dudzinski, M.D., Meridale V. Baggett, M.D., Dennis C. Sgroi, M.D., Jo Anne O. Shepard,
Case Report Diagnosis of Cryptococcosis and Prevention of Cryptococcal Meningitis Using a Novel Point-of-Care Lateral Flow Assay
 Case Reports in Medicine Volume 2013, Article ID 640216, 4 pages http://dx.doi.org/10.1155/2013/640216 Case Report Diagnosis of Cryptococcosis and Prevention of Cryptococcal Meningitis Using a Novel Point-of-Care
Case Reports in Medicine Volume 2013, Article ID 640216, 4 pages http://dx.doi.org/10.1155/2013/640216 Case Report Diagnosis of Cryptococcosis and Prevention of Cryptococcal Meningitis Using a Novel Point-of-Care
NIH Public Access Author Manuscript Clin Infect Dis. Author manuscript; available in PMC 2009 October 1.
 NIH Public Access Author Manuscript Published in final edited form as: Clin Infect Dis. 2008 October 1; 47(7): 893 899. doi:10.1086/591534. Normalization of Serum Rapid Plasma Reagin Titer Predicts Normalization
NIH Public Access Author Manuscript Published in final edited form as: Clin Infect Dis. 2008 October 1; 47(7): 893 899. doi:10.1086/591534. Normalization of Serum Rapid Plasma Reagin Titer Predicts Normalization
Downloaded from:
 Molefi, M; Chofle, AA; Molloy, SF; Kalluvya, S; Changalucha, JM; Cainelli, F; Leeme, T; Lekwape, N; Goldberg, DW; Haverkamp, M; Bisson, GP; Perfect, JR; Letang, E; Fenner, L; Meintjes, G; Burton, R; Makadzange,
Molefi, M; Chofle, AA; Molloy, SF; Kalluvya, S; Changalucha, JM; Cainelli, F; Leeme, T; Lekwape, N; Goldberg, DW; Haverkamp, M; Bisson, GP; Perfect, JR; Letang, E; Fenner, L; Meintjes, G; Burton, R; Makadzange,
Shunting in cryptococcal meningitis
 clinical article J Neurosurg 125:177 186, 2016 ing in cryptococcal meningitis Jacob Cherian, MD, 1 Robert L. Atmar, MD, 2 and Shankar P. Gopinath, MD 1 Departments of 1 Neurosurgery and 2 Medicine, Section
clinical article J Neurosurg 125:177 186, 2016 ing in cryptococcal meningitis Jacob Cherian, MD, 1 Robert L. Atmar, MD, 2 and Shankar P. Gopinath, MD 1 Departments of 1 Neurosurgery and 2 Medicine, Section
Meningi&s in HIV NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Meningi&s in HIV Christina M. Marra, MD Neurology and Medicine University of Washington School of Medicine Susceptibility to CNS Opportunistic Infections CD4+
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Meningi&s in HIV Christina M. Marra, MD Neurology and Medicine University of Washington School of Medicine Susceptibility to CNS Opportunistic Infections CD4+
Toxicity of Amphotericin B deoxycholate-based induction therapy. in patients with HIV-associated cryptococcal meningitis
 AAC Accepted Manuscript Posted Online 8 September 2015 Antimicrob. Agents Chemother. doi:10.1128/aac.01698-15 Copyright 2015, American Society for Microbiology. All Rights Reserved. 1 1 2 Toxicity of Amphotericin
AAC Accepted Manuscript Posted Online 8 September 2015 Antimicrob. Agents Chemother. doi:10.1128/aac.01698-15 Copyright 2015, American Society for Microbiology. All Rights Reserved. 1 1 2 Toxicity of Amphotericin
Technical appendix to How should access to antiretroviral treatment be measured? Published in the Bulletin of the World Health Organization
 Technical appendix to How should access to antiretroviral treatment be measured? Published in the Bulletin of the World Health Organization Leigh F. Johnson Andrew Boulle Centre for Infectious Disease
Technical appendix to How should access to antiretroviral treatment be measured? Published in the Bulletin of the World Health Organization Leigh F. Johnson Andrew Boulle Centre for Infectious Disease
GUIDELINE FOR THE MANAGEMENT OF CRYPTOCOCCAL MENINGITIS
 GUIDELINE FOR THE MANAGEMENT OF CRYPTOCOCCAL MENINGITIS Full title of guideline Guideline for the management of cryptococcal meningitis Author Dr P Venkatesan (ID consultant) Division and specialty Medicine,
GUIDELINE FOR THE MANAGEMENT OF CRYPTOCOCCAL MENINGITIS Full title of guideline Guideline for the management of cryptococcal meningitis Author Dr P Venkatesan (ID consultant) Division and specialty Medicine,
Cryptococcal meningoencephalitis in HIV/AIDS: when to start antiretroviral therapy?
 Franco Paredes et al. Ann Clin Microbiol Antimicrob (2017) 16:9 DOI 10.1186/s12941-017-0184-2 Annals of Clinical Microbiology and Antimicrobials EDITORIAL Cryptococcal meningoencephalitis in HIV/AIDS:
Franco Paredes et al. Ann Clin Microbiol Antimicrob (2017) 16:9 DOI 10.1186/s12941-017-0184-2 Annals of Clinical Microbiology and Antimicrobials EDITORIAL Cryptococcal meningoencephalitis in HIV/AIDS:
ORIGINAL ARTICLE /j x
 ORIGINAL ARTICLE 10.1111/j.1469-0691.2006.01367.x Endemic fungal infections caused by Cryptococcus neoformans and Penicillium marneffei in patients infected with human immunodeficiency virus and treated
ORIGINAL ARTICLE 10.1111/j.1469-0691.2006.01367.x Endemic fungal infections caused by Cryptococcus neoformans and Penicillium marneffei in patients infected with human immunodeficiency virus and treated
By: Kokeb T. January, 2016.
 Pre-ART nutritional status and its association with mortality in adult patients enrolled on ART at Fiche Hospital in North Shoa, Oromia Region, Ethiopia: retrospective cohort study. By: Kokeb T. January,
Pre-ART nutritional status and its association with mortality in adult patients enrolled on ART at Fiche Hospital in North Shoa, Oromia Region, Ethiopia: retrospective cohort study. By: Kokeb T. January,
Opportunistic Infections BHIVA Guidelines
 Opportunistic Infections BHIVA Guidelines Mark Nelson David Dockrell Simon Edwards I have.. 1. Read all of the BHIVA guidelines 12% 2. Read some of the BHIVA guidelines in their entirety 3. Browsed some
Opportunistic Infections BHIVA Guidelines Mark Nelson David Dockrell Simon Edwards I have.. 1. Read all of the BHIVA guidelines 12% 2. Read some of the BHIVA guidelines in their entirety 3. Browsed some
Tuberculosis Immune Reconstitution Inflammatory Syndrome (TB- IRIS)
") Tuberculosis Immune Reconstitution Inflammatory Syndrome (TB- IRIS) Graeme Meintjes Institute of Infectious Disease and Molecular Medicine (IDM) Wellcome Centre for Infectious Diseases Research in Africa
Tuberculosis Immune Reconstitution Inflammatory Syndrome (TB- IRIS) Graeme Meintjes Institute of Infectious Disease and Molecular Medicine (IDM) Wellcome Centre for Infectious Diseases Research in Africa
Clinical use of a TB Diagnostic using LAM Detection in Urine. Robin Wood, IDM, University of Cape Town
 Clinical use of a TB Diagnostic using LAM Detection in Urine Robin Wood, IDM, University of Cape Town Declaration of Interests Statement Robin Wood, FCP (SA), D.Sc.(Med), FRS (SA). Emeritus Professor of
Clinical use of a TB Diagnostic using LAM Detection in Urine Robin Wood, IDM, University of Cape Town Declaration of Interests Statement Robin Wood, FCP (SA), D.Sc.(Med), FRS (SA). Emeritus Professor of
High Prevalence of Cryptococcal Antigenemia among HIV-infected Patients Receiving Antiretroviral Therapy in Ethiopia
 High Prevalence of Cryptococcal Antigenemia among HIV-infected Patients Receiving Antiretroviral Therapy in Ethiopia Abere Shiferaw Alemu 1 *, Russell R. Kempker 2 *, Admasu Tenna 3, Christopher Smitson
High Prevalence of Cryptococcal Antigenemia among HIV-infected Patients Receiving Antiretroviral Therapy in Ethiopia Abere Shiferaw Alemu 1 *, Russell R. Kempker 2 *, Admasu Tenna 3, Christopher Smitson
Research Article Challenges in Assessing Outcomes among Infants of Pregnant HIV-Positive Women Receiving ART in Uganda
 Hindawi AIDS Research and Treatment Volume 2017, Article ID 3202737, 4 pages https://doi.org/10.1155/2017/3202737 Research Article Challenges in Assessing Outcomes among Infants of Pregnant HIV-Positive
Hindawi AIDS Research and Treatment Volume 2017, Article ID 3202737, 4 pages https://doi.org/10.1155/2017/3202737 Research Article Challenges in Assessing Outcomes among Infants of Pregnant HIV-Positive
Journal of Infectious Diseases Advance Access published August 25, 2014
 Journal of Infectious Diseases Advance Access published August 25, 2014 1 Reply to Decker et al. Ruth Koepke 1,2, Jens C. Eickhoff 3, Roman A. Ayele 1,2, Ashley B. Petit 1,2, Stephanie L. Schauer 1, Daniel
Journal of Infectious Diseases Advance Access published August 25, 2014 1 Reply to Decker et al. Ruth Koepke 1,2, Jens C. Eickhoff 3, Roman A. Ayele 1,2, Ashley B. Petit 1,2, Stephanie L. Schauer 1, Daniel
Recurrent cryptococcal immune reconstitution inflammatory syndrome in an HIV-infected patient after anti-retroviral therapy: a case report
 Hu et al. Annals of Clinical Microbiology and Antimicrobials 2013, 12:40 CASE REPORT Open Access Recurrent cryptococcal immune reconstitution inflammatory syndrome in an HIV-infected patient after anti-retroviral
Hu et al. Annals of Clinical Microbiology and Antimicrobials 2013, 12:40 CASE REPORT Open Access Recurrent cryptococcal immune reconstitution inflammatory syndrome in an HIV-infected patient after anti-retroviral
Chronic Lung Disease in vertically HIV infected children. Dr B O Hare Senior Lecturer in Paediatrics and Child Health, COM, Blantyre
 Chronic Lung Disease in vertically HIV infected children Dr B O Hare Senior Lecturer in Paediatrics and Child Health, COM, Blantyre Natural history of HIV in vertically infected children without and with
Chronic Lung Disease in vertically HIV infected children Dr B O Hare Senior Lecturer in Paediatrics and Child Health, COM, Blantyre Natural history of HIV in vertically infected children without and with
P Mwaba, J Mwansa, C Chintu, J Pobee, M Scarborough, S Portsmouth, A Zumla
 Postgrad Med J 2001;77:769 773 769 Medicine and the P Mwaba Pathology and Microbiology, University Teaching Hospital, Lusaka, Zambia J Mwansa C Chintu Medicine, University J Pobee London Hospitals Trust,
Postgrad Med J 2001;77:769 773 769 Medicine and the P Mwaba Pathology and Microbiology, University Teaching Hospital, Lusaka, Zambia J Mwansa C Chintu Medicine, University J Pobee London Hospitals Trust,
Aetiology of meningitis at the Moi Teaching and Referral Hospital, Eldoret, Kenya. D. K. Lagat, MBChB, Mmed(Moi)
") Aetiology of meningitis at the Moi Teaching and Referral Hospital, Eldoret, Kenya D. K. Lagat, MBChB, Mmed(Moi) Introduction Meningitis is common and important Syndromes of meningitis: Acute bacterial
Aetiology of meningitis at the Moi Teaching and Referral Hospital, Eldoret, Kenya D. K. Lagat, MBChB, Mmed(Moi) Introduction Meningitis is common and important Syndromes of meningitis: Acute bacterial
1 Fungal Pathogens Laboratory, National Heart and Lung Institute, Imperial College London, SW7 2AY UK
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 AIDS-Related Mycoses: Current progress in
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 AIDS-Related Mycoses: Current progress in
Trends in HIV prevalence and incidence sex ratios in ALPHA demographic surveillance sites,
 Trends in HIV prevalence and incidence sex ratios in ALPHA demographic surveillance sites, 1990 2010 Zaba B 1, Calvert C 1, Marston M 1, Isingo R 2, Nakiyingi Miiro J 3, Lutalo T 4, Crampin A 1,5, Nyamukapa
Trends in HIV prevalence and incidence sex ratios in ALPHA demographic surveillance sites, 1990 2010 Zaba B 1, Calvert C 1, Marston M 1, Isingo R 2, Nakiyingi Miiro J 3, Lutalo T 4, Crampin A 1,5, Nyamukapa
Monitoring and impact of fluconazole serum and cerebrospinal fluid concentration in HIV-associated cryptococcal meningitis-infected patients
 DOI: 10.1111/j.1468-1293.2009.00778.x HIV Medicine (2010), 11, 276 281 ORIGINAL RESEARCH r 2009 British HIV Association Monitoring and impact of fluconazole serum and cerebrospinal fluid concentration
DOI: 10.1111/j.1468-1293.2009.00778.x HIV Medicine (2010), 11, 276 281 ORIGINAL RESEARCH r 2009 British HIV Association Monitoring and impact of fluconazole serum and cerebrospinal fluid concentration
Statistical Analysis Plan (SAP)
") Statistical Analysis Plan (SAP) Comparison of artemether-lumefantrine and chloroquine with and without primaquine for the treatment of Plasmodium vivax in Ethiopia: a randomized controlled trial Contents
Statistical Analysis Plan (SAP) Comparison of artemether-lumefantrine and chloroquine with and without primaquine for the treatment of Plasmodium vivax in Ethiopia: a randomized controlled trial Contents
Articles. Funding European and Developing Countries Clinical Trials Partnership.
 Cryptococcal meningitis screening and community-based early adherence support in people with advanced HIV infection starting antiretroviral therapy in Tanzania and Zambia: an open-label, randomised controlled
Cryptococcal meningitis screening and community-based early adherence support in people with advanced HIV infection starting antiretroviral therapy in Tanzania and Zambia: an open-label, randomised controlled
mycoses Antifungal susceptibilities of Cryptococcus neoformans cerebrospinal fluid isolates from AIDS patients in Kenya Summary Introduction
 mycoses Diagnosis,Therapy and Prophylaxis of Fungal Diseases Original article Antifungal susceptibilities of Cryptococcus neoformans cerebrospinal fluid isolates from AIDS patients in Kenya Rennatus Mdodo,
mycoses Diagnosis,Therapy and Prophylaxis of Fungal Diseases Original article Antifungal susceptibilities of Cryptococcus neoformans cerebrospinal fluid isolates from AIDS patients in Kenya Rennatus Mdodo,
Antiretroviral treatment outcomes after the introduction of tenofovir in the public-sector in South Africa
 Antiretroviral treatment outcomes after the introduction of tenofovir in the public-sector in South Africa Alana T Brennan, Kate Shearer, Mhairi Maskew, Prudence Ive, Ian Sanne, Matthew P Fox Health Economics
Antiretroviral treatment outcomes after the introduction of tenofovir in the public-sector in South Africa Alana T Brennan, Kate Shearer, Mhairi Maskew, Prudence Ive, Ian Sanne, Matthew P Fox Health Economics
Changes in viral suppression status among US HIV-infected patients receiving care
 CONCISE COMMUNICATION Changes in viral suppression status among US HIV-infected patients receiving care Nicole Crepaz a, Tian Tang b, Gary Marks a and H. Irene Hall a Objective: To examine changes in viral
CONCISE COMMUNICATION Changes in viral suppression status among US HIV-infected patients receiving care Nicole Crepaz a, Tian Tang b, Gary Marks a and H. Irene Hall a Objective: To examine changes in viral
The availability and cost are obstacles to using pvl in monitoring HIV treatment outcomes in resource-constrained settings
 Impact of the frequency of plasma viral load monitoring on treatment outcome among perinatally HIVinfected Asian children stable on first-line NNRTI-based cart T Sudjaritruk, DC Boettiger, NV Lam, KAM
Impact of the frequency of plasma viral load monitoring on treatment outcome among perinatally HIVinfected Asian children stable on first-line NNRTI-based cart T Sudjaritruk, DC Boettiger, NV Lam, KAM
Monitoring Recent HIV Infection in Ireland, 2017
 Monitoring Recent HIV Infection in Ireland, 2017 January 2019 Key Facts 1 13% of HIV diagnoses in 2017 (of those tested) were likely to be recent infections (within 4 months), using the Recent Infection
Monitoring Recent HIV Infection in Ireland, 2017 January 2019 Key Facts 1 13% of HIV diagnoses in 2017 (of those tested) were likely to be recent infections (within 4 months), using the Recent Infection
Diagnostic accuracy of Xpert MTB/RIF Ultra for tuberculous meningitis in HIV-infected adults: a prospective cohort study
 Diagnostic accuracy of Xpert MTB/RIF Ultra for tuberculous meningitis in HIV-infected adults: a prospective cohort study Nathan C Bahr, Edwin Nuwagira, Emily E Evans, Fiona V Cresswell, Philip V Bystrom,
Diagnostic accuracy of Xpert MTB/RIF Ultra for tuberculous meningitis in HIV-infected adults: a prospective cohort study Nathan C Bahr, Edwin Nuwagira, Emily E Evans, Fiona V Cresswell, Philip V Bystrom,
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Molloy SF, Kanyama C, Heyderman RS, et al. Antifungal combinations
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Molloy SF, Kanyama C, Heyderman RS, et al. Antifungal combinations
Ventriculoperitoneal shunts in non-hiv cryptococcal meningitis
 Liu et al. BMC Neurology (2018) 18:58 https://doi.org/10.1186/s12883-018-1053-0 RESEARCH ARTICLE Open Access Ventriculoperitoneal shunts in non-hiv cryptococcal meningitis Jia Liu 1, Zhuo-lin Chen 1, Min
Liu et al. BMC Neurology (2018) 18:58 https://doi.org/10.1186/s12883-018-1053-0 RESEARCH ARTICLE Open Access Ventriculoperitoneal shunts in non-hiv cryptococcal meningitis Jia Liu 1, Zhuo-lin Chen 1, Min
Pitfalls associated with the use of molecular diagnostic panels in the diagnosis of cryptococcal meningitis
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2017 Pitfalls associated with the use of molecular diagnostic panels in the diagnosis of cryptococcal meningitis
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2017 Pitfalls associated with the use of molecular diagnostic panels in the diagnosis of cryptococcal meningitis
The war on cryptococcosis: A Review of the antifungal arsenal
 REVIEW Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 113(7): e170391, 2018 1 7 The war on cryptococcosis: A Review of the antifungal arsenal Ahmad Mourad, John R Perfect/ + Duke University Medical Center,
REVIEW Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 113(7): e170391, 2018 1 7 The war on cryptococcosis: A Review of the antifungal arsenal Ahmad Mourad, John R Perfect/ + Duke University Medical Center,
Epidemiology of Cryptococcosis and Cryptococcal Meningitis in a large retrospective cohort of patients after solid organ transplantation
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2017 Epidemiology of Cryptococcosis and Cryptococcal Meningitis in a large retrospective cohort of patients after
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2017 Epidemiology of Cryptococcosis and Cryptococcal Meningitis in a large retrospective cohort of patients after
Clinical Practice Guidelines for the Management of Cryptococcal Disease: 2010 Update by the Infectious Diseases Society of America
 IDSA GUIDELINES Clinical Practice Guidelines for the Management of Cryptococcal Disease: 2010 Update by the Infectious Diseases Society of America John R. Perfect, 1 William E. Dismukes, 2 Francoise Dromer,
IDSA GUIDELINES Clinical Practice Guidelines for the Management of Cryptococcal Disease: 2010 Update by the Infectious Diseases Society of America John R. Perfect, 1 William E. Dismukes, 2 Francoise Dromer,