Management of viral hepatitis in the HIV coinfected
|
|
|
- Isabel Bryant
- 5 years ago
- Views:
Transcription
1 Management of viral hepatitis in the HIV coinfected patient Sanjay Bhagani BSc MB ChB FRCP Royal Free Hospital/University College London

2
3 Rate per 1,000 person years D:A:D: Liver-related death is a frequent cause of non-aids death in HIV-infected patients Analysis of 2,482 deaths in 180,176 person-years among 33,308 individuals AIDS remains the primary cause of death amongst HIV-positive individuals Rate of death according to calendar year and specific cause of death Adapted from D:A:D Study Group. AIDS. 2010;24:
4 Prevalence of HBV: Global Estimates HBsAg Prevalence High ( 8%) Intermediate (2% to 8%) Low (<2%) HBsAg +ve, (%) Taiwan Vietnam China Africa Philippines Thailand Japan Indonesia 4.0 South Korea India Russia US Mast EE, et al. MMWR Recomm Rep. 2006;55:1 33 Custer B, et al. J Clin Gastroenterol. 2004;38(10 suppl):s158-s168
5 Global HIV/HBV Thio, C. Hepatology 2009; 49(5): s138
6 Liver-related Mortality Rate (per 1000 person-years) HIV/HBV Co-infection: Increased risk of ESLD due to HBV P< P<0.001 P= HIV-/HBsAg- HIV+ HBsAg+ HIV+/HBsAg+ Thio CL, et al. Lancet. 2002:360:
7 Immune activation and liver disease Cirrhosis HCV/HBV Alcohol Hepatic fibrosis HSC activation Altered portal vein circulation HIV -> GIT CD4+ T-cell depletion IL-1 TNF-a IFN-a IL-12 Microbial translocation LPS macrophage Immune activation DCs Mathurin et al., Hepatology 2000; 32: ; Paik et al., Hepatology 2003; 37: ; Balagopal et al., Gastroenterology 2008; 135: Slide courtesy of S. Lewin
8 Does HBV effect HIV? Chun, et al, JID 2012
9 Natural history of HBV infection where does co-infection fit in? Early childhood > 95% Immune tolerance < 5% Adulthood HIV/HBV Higher viral loads HBeAg Chronic Hepatitis B HBV DNA + HCC Inactive carrier HBeAg+ Chronic Hepatitis B HIV/HBV Increased likelihood HIV/HBV: Increased viral loads Lower ALT Increased fibrosis HBs+ HBe- HBV DNA low HIV/HBV Reduced seroconversion Adapted from: Chen DS, et al. J Gastroenterol Hepatol 1993;8:470 5; Seeff L, et al. N Engl J Med 1987;316:965 70; Thio CL, et al. Lancet 2002;360:1921 6; Gilson RJ, et al. AIDS 1997;11: ; Colin JF, et al. Hepatology 1999;29:
10 Treating HBV Prevent progression to end-stage liver disease Prevent HCC
11 Potency Anti-HBV drugs PegIFN TBV ETV* TDF* LAM* FTC* ADV Nucleosides Nucleotides *Anti-HIV activity Genetic barrier

12 EACS Guidelines 2012
 0.74 0.50 (0.14,1.87) 0.30 Male gender 1.52 (0.50,4.51) 0.40 1.18 (0.35,3.92) 0.79 HBV DNA >3.3 log IU/mL 1,2 6.5 (1.99, 22.97) 0.0003 6.09 (1.96,18.91) 0.")
 0.66 - - BMI >25 0.44 (0.10-1.57) 0.17 0.52 (0.14,1.82) 0.29 CD4 <200 1.72 (0.53,5.30) 0.30 1.26 (0.37,4.29) 0.71 HIV VL >400,000 1.16 (0.18, 5.35) 0.83 - - Platelets <150 2.18 (0.")
13 Agbaji et al, (CROI, 2013) HBV in the resource-poor setting; how useful is FibroScan? HBV/HIV co-infected Univariate Multivariate OR, 95% CI p value OR, 95% CI p value Age 30 yrs 0.83 (0.26,3.03) (0.14,1.87) 0.30 Male gender 1.52 (0.50,4.51) (0.35,3.92) 0.79 HBV DNA >3.3 log IU/mL 1,2 6.5 (1.99, 22.97) (1.96,18.91) HBeAg reactive 2.50 (0.69, 8.41) HIV mono-infected Married Current alcohol use 1.1 (0.37, 3.46) 2.62 (0.81, 8.19) (0.74,7.60) 0.15 ALT (0.27, 2.46) BMI > ( ) (0.14,1.82) 0.29 CD4 < (0.53,5.30) (0.37,4.29) 0.71 HIV VL >400, (0.18, 5.35) Platelets < (0.45, 9.76)
14 Pertinent issues in HIV/HBV coinfection management TDF +/- 3TC/FTC works What options for patients NOT needing HAART PegIFN What about hepatic flares with anti-hbv therapy? What about slow responders to TDF? For patients needing HAART What to do with patients developing Tenofovir toxicity? Global implications of lamivudine resistance
15 Pertinent issues in HIV/HBV coinfection management TDF +/- 3TC/FTC works What options for patients NOT needing HAART PegIFN What about hepatic flares with anti-hbv therapy? What about slow responders to TDF? For patients needing HAART What to do with patients developing Tenofovir toxicity? Global implications of lamivudine resistance
16 High rates of HBeAg seroconversion following HBV active HAART HBeAg loss by pre-haart ALT Months ALT normal ALT abnormal Longitudinal Thai cohort (n=47); HBeAg-positive (n=30); median follow up = 27 month HBeAg loss = 46%; HBsAg loss = 13% Avahingson et al., 5 th IAS Conference, Capetown 2009, Poster # WEPEB226

17 TDF and HCC risk
18 TDF and HCC risk
19 TDF and HCC risk
20 Patients (%) MORTAVIC: Causes of death in HIVinfected adults in France in 2010 Patients (%) Patients (%) Cause of death Number of documented deaths= Non AIDS-defining and non hepatitisrelated cancers AIDS Liver Cardiovascular Created from Rosenthal E, et al. EASL Barcelona Spain. Oral presentation Liver-related cause of death 0 Cirrhosis 71 Hepatocellular carcinoma Cholangiocarcinoma No details except HCV 18 HCV HCV + HBV 4 7 Cause of underlying cirrhosis HBV Other
21 Pertinent issues in HIV/HBV coinfection management TDF +/- 3TC/FTC works What options for patients NOT needing HAART PegIFN What about hepatic flares with anti-hbv therapy? What about slow responders to TDF? For patients needing HAART What to do with patients developing Tenofovir toxicity? Global implications of lamivudine resistance
22 PegIFN and HIV/HBV Very little data in HIV/HBV co-infected patients Ingiliz P et al. (combination with adefovir) No e-seroconversion after 48 weeks HBV DNA levels not maintained post-rx Predictors of response in mono-infected patients Genotype A/B High ALT (>3 ULN) Low HBV DNA (< IU/L) Risk of de-compensation/complications in cirrhotic CP-B/C patients EASL Practice Guidelines. J Hepatol 2009;50:227 42; Ingiliz P, et al. Antivir Ther 2008;13:

23 Can pegifn intensification help clear HBeAg in TDF treated HBV/HIV co-infection?. CROI 2013: Anders Boyd et al. Case control from larger French HIV/HBV prospective cohort CROI 2013: Patrick Miailhes et al. The ANRS HB01 EMVIPEG Study N=51, no control group Median 39/12 TDF based cart already Kaplan-Meier of cummulative loss of HBeAg pegifn 7/12 controls HBV DNA Undetectable? peginf 1/10 (10%) Ctrl 2/30 (7%) 37 months TDF + 3TC/FTC on pegifn pegifn 12 24/52 post pegifn HBeAg loss 12/51 (24%) 8/51 (16%) HBeAb seroconversion 6 (12%) 4 (8%) HBsAg loss 2 (4%) 2 (4%) 6 Matched qhbeag at baseline /12 12/12 36/12 24/12 addition of pegifn did not allow to increase the rate of HBe seroconversion in HBeAg + HIV co-infected patients Peg-IFN-INTS during TDF-treatment was associated with accelerated HBeAg-loss But no effect on qhbeag/qhbsag decline or longterm serological outcomes. Adding peg-ifn to a TDF-containing regimen may not be a beneficial option in co-infection
24 Pertinent issues in HIV/HBV coinfection management TDF +/- 3TC/FTC works What options for patients NOT needing HAART PegIFN What about hepatic flares with anti-hbv therapy? What about slow responders to TDF? For patients needing HAART What to do with patients developing Tenofovir toxicity? Global implications of lamivudine resistance
25 Hepatic flares post-starting TDFbased cart in co-infected patients Avihingasanon, et al AIDS Research Therapy 2012

26 Co-relates of hepatic flares Avihingasanon, et al AIDS Research Therapy 2012
27 Hepatic flares in HBV/HIV Usually in the first 12 weeks post-cart Associated with high HBV DNA levels and high baseline ALTs Restoration of innate and adaptive anti- HBV response in the presence of high HBV DNA De-compensation rare BUT caution with cirrhosis
28 Pertinent issues in HIV/HBV coinfection management TDF +/- 3TC/FTC works What options for patients NOT needing HAART PegIFN What about hepatic flares with anti-hbv therapy? What about slow responders to TDF? For patients needing HAART What to do with patients developing Tenofovir toxicity? Global implications of lamivudine resistance

29 Patterns of persistent viraemia
30 Delayed response with TDF How long is delayed? In this small study almost all delayed responders suppressed by a median of 49 months. No TDF associated mutations X1 new lam-associated polymormphism Childs, et al AIDS 2013
31 Pertinent issues in HIV/HBV coinfection management TDF +/- 3TC/FTC works What options for patients NOT needing HAART PegIFN What about hepatic flares with anti-hbv therapy? What about slow responders to TDF? For patients needing HAART What to do with patients developing Tenofovir toxicity? Global implications of lamivudine resistance
32 Renal impairment with TDF watch this space. 240 patients with a 3yeartime follow-up, normal egfr at baseline1 >400 HIV+ patients receiving TDF Duration of treatment (months) NRTI-based therapy with TDF without TDF Figure 1: MDRD clearance over time Pune: RFH: Pujari, et al, CROI 2013
33 What about tenofovir toxicity or HIV resistance to tenofovir or 3TC/FTC? BHIVA Guidelines 2010; HIV Medicine 2010

34 Management options for HIV/HBV co-infection
35 Pertinent issues in HIV/HBV coinfection management TDF +/- 3TC/FTC works What options for patients NOT needing HAART PegIFN What about hepatic flares with anti-hbv therapy? What about slow responders to TDF? For patients needing HAART What to do with patients developing Tenofovir toxicity? Global implications of lamivudine resistance
36 Incidence of Resistance Incidence of HBV Resistance in Patients Treated with LAM in HBV infection vs. HIV/HBV co-infection 100% 80% LAM 1 (YMDD ) Triple HBV mutation twice as common in HIV/HBV 3 LAM 2 (YMDD in HIV/HBV) 70% 90% 60% 40% 20% 24% 42% 47% 53% 0% year 1 year 2 year 3 year 4 1. Lai C.L., et al., Clinical Infectious Diseases (2003) 36: Benhamou Y et al. Hepatology 1999; 30: Matthews GV, et al. AIDS 2006;20(6):
37 Disease Progression, % Impact of lamivudine resistance on progression of liver disease Patients with severe fibrosis or cirrhosis Placebo (n = 215) YMDDm (n = 209) (49%) Wild-Type (n = 221) Placebo 21% 15 YMDDm 13% 10 5 WT 5% Time after Randomization (months) Liaw, N Engl J Med. 2004
38 More than just drug resistance Overlapping Pol and S Mutations in Pol changes in S ADASMs Antiviral Drug- Associated S mutations ADAPVEMS Antiviral Drug Associated Potentially Vaccine (and detection) Escape Mutations Associated with L- nucleosides and Entacavir, possibly with adefovir
39 Envelope/Polymerase Mutations and the Antigen/Antibody Binding Capacity in Genotype A and D HBV/HIV Co-infected Subjects (n=9) with LAM Resistance Envelope changes Polymerase changes Ag Ab binding [IC 50 (μg/ml)] Wild type Wild type 1.09 HBIG escape sg145r Anti-viral drug resistant se164d sw196s si195m sm198i se164d/i195m rtw153g rtv173l rtm204i rtm204v rtv207i rtv173/rtl180/rtm204v > Cooley L et al. AIDS 2003;17:
40 ARV Rollout AZT/d4T+LAM+NNRTI?Global Impact
41 Liver related mortality rate/100 py HIV/HBV co-infection: mortality in the resource rich setting HBV < HAART HBV-active (95%) Thio et al Lancet 2002 Hoffman et al., AIDS 2009

42

43
44 HIV/HCV co-infection Pertinent management issues 2013
45 WHO: Global HIV and HCV Global HIV infection 1 (% adult prevalence) infection Global chronic HCV infection 2 (% adult prevalence) North America up to 3.1% Europe up to 1.2% Asia Pacific up to 1.3% North America up to 2.49% Europe up to 2.49% Asia Pacific up to and over 10% Latin America up to 2.3% Africa and Middle East up to 25.9% Latin America up to and over 10% Africa and Middle East up to and over 10% Estimated total HIV infections worldwide: 33.3 million WHO=World Health Organisation Estimated total chronic HCV infections worldwide: 170 million HCV genotypes 1 3 have a worldwide distribution Genotypes 1a and 1b are most common and account for 60% of global infections 1. Adapted from UNAIDS Global View of HIV infection Available at _2010_HIV_Prevalence_Map_em.pdf. Accessed September 2012; 2. Adapted from WHO Hepatitis C Guide Available at Accessed September 2012

46 EuroSIDA: Prevalence of HIV/HCV co-infection and distribution of HCV genotypes North 60% 40% 20% 0% Genotype North: 18.3% Central: 15.0% East: 31.3% Central 60% 40% 20% 0% Genotype 60% South South: 35.5% 60% East 40% 40% 20% 20% 0% Genotype 0% Genotype Map shows prevalence of HIV/HCV coinfection by region in N=5,957 HIV-infected patients with an HCV antibody test available 1 Bar charts shows prevalence of HCV genotype in n=1,940 HIV/HCV-coinfected patients by region 2 Created from: 1. Rockstroh J, et al. J Infect Dis. 2005;192: ; 2. Soriano V, et al. J Infect Dis. 2008;198:
 HCV incidence in IDU: Decreased from 13.9 to 2.")
47 Swiss HIV Cohort Study: Changing patterns of HCV incidence Incidence rate (per 100 py) HCV incidence in MSM: Reached 4.1 cases per 100 PY in 2011 (18 fold increase since 1998) HCV incidence in IDU: Decreased from 13.9 to 2.2 cases per 100 PY HCV incidence in heterosexuals Remained <1 per 100 PY throughout the study period Swiss HIV Cohort Study: HCV yearly incidence rate by transmission group* HET IDU MSM Predictors of HCV seroconversion in MSM 1,2 : History of UAI, multiple partners, use of sex-toys and fisting STIs, especially syphilis and LGV PY=patient years; IDU=intravenous drug users; UAI=unprotected anal intercourse; Calendar year *Shaded: 95% confidence intervals 1. STIs=sexually Adapted from transmitted Wandeler infections; G, et al. LGV=lymphogranuloma CROI Seattle venereum; USA. Poster Q106; 2. Van de HET=heterosexual Laar T, al. JID 2007;196:230 8.


48 HIV/HCV coinfection may result in multisystemic disorders Global cognitive impairment Cognitive-motor impairment Dementia Peripheral neuropathy Neurologic disease Cerebrovascular disease Acute myocardial infarction Opportunistic infections Wasting syndrome Proteinuria Acute renal failure Chronic kidney disease Cardiovascular HIV disease progression Kidney disease Immune activation HIV/HCV Immune dysfunction Metabolic disorders Liver disease GI tract Diabetes mellitus Insulin resistance Steatosis Fibrosis Cirrhosis End-stage liver disease Liver-related death Microbial translocation Osteonecrosis Osteoporosis Bone fracture Bone disorders CD4 apoptosis Abnormal T-cell responses and cytokine production Cytotoxic T-cell accumulation in liver Impaired CD4 recovery post-haart Severe immunodeficiency Adapted from Operskalski EA and Kovacs A. Curr HIV/AIDS Rep. 2011;8:12 22.
49 Cumulative probability of mortality Impact of chronic HCV in patients with AIDS in the cart era Chronic HCV infection is independently associated with a 50% increase in mortality among patients with an AIDS diagnosis 0.50 w/o HCV markers Cleared HCV Chronic HCV Years of follow up Number at risk w/o HCV markers Cleared Chronic Adapted from Branch A, et al. Clin Infect Dis 2012;55:
50 Cumulative Survival Cumulative Survival HAART reduces mortality in HIV/HCV-coinfected patients Bonn cohort ( ) 285 HIV/HCV-coinfected patients Liver-related mortality rates per 100 PY: HAART: 0.45 ART: 0.69 No therapy: 1.70 Predictors of liver-related mortality: No HAART Low CD4 cell count Increasing age *p<0.001 Overall Mortality *p=0.018 Days Days HAART* Liver-Related Mortality HAART* ART No therapy ART No therapy Adapted from Qurishi N, et al. Lancet. 2003:362:
51 Effective treatment of HIV infection reduces fibrosis risk in HIV/HCV-coinfected patients Age, years Predictive factors of fibrosis progression ( 1 stage) (multivariate analysis) HAART during the follow-up Undetectable HIV viraemia* CD4 cell counts change Genotype 3 Baseline ALT, IU/mL Baseline necroinflammatory activity Time between liver biopsies Response to anti-hcv treatment ( 37 vs <37) (Yes vs No) (Yes vs No) (Per 25 cell increase) (Yes vs No) ( 66 vs <66) (L2 4 vs L0 1) (Per 1 year increase) (ETR vs no ETR) RR (95% CI)=relative risk (95% confidence interval); ETR=end-of-treatment response; HAART=highly active antiretroviral therapy; *Undetectable HIV RNA in 70% determinations during the follow up. Created from Macias J, et al. Hepatology 2009;50: Relative risk (95% CI) p multivariate Data collected from 135 coinfected patients with 2 liver biopsies >1 year apart. Specimens were centrally read and scored blindly by 2 independent pathologists using the Scheuer classification.
52 SVR (%) HCV/HIV treatment outcomes with pegifn and Ribavirin 100 Genotype 1 SVR 14 38% Genotype 3 SVR 44 73% Monoinfection APRICOT ACTG RIBAVIC Laguno et al. PRESCO 0 G1 G2/3 Genotype Fried et al, NEJM 2002, 347: , Torriani et al, NEJM 2004; 351: , Chung R, et al, NEJM 2004: 351; 451-9, Carrat F, et al, JAMA 2004: 292: , Laguno et al, AIDS 2004; 18: F27-F36, Nunez et al, JAIDS 2007: 45:

53 Rallón et al, CROI 2010, J Hepatology 2012
54 HCV Life Cycle and DAA Targets essential knowledge Receptor binding and endocytosis Fusion and uncoating Transport and release (+) RNA LD ER lumen LD Virion assembly Translation NS3/4 and polyprotein protease processing inhibitors ER lumen Membranous web LD NS5B polymerase RNA inhibitors replication Nucleoside/nucleotide Nonnucleoside NS5A* inhibitors *Role in HCV life cycle not well defined Adapted from Manns MP, et al. Nat Rev Drug Discov. 2007;6:

55 More essential knowledge
56
57 Telaprevir (TVR) in combination with pegylated interferonα-2a (P) + ribavirin (R) in HCV/HIV-coinfected patients Part A: No ART T/PR 1:1 PR48 (control) TVR+PR Pbo+PR PR PR SVR 12 follow up SVR 12 follow up SVR SVR Part B: ART (EFV/TDF/FTC or ATV/r + TDF + FTC or 3TC) T/PR 1:1 PR48 (control) TVR+PR Pbo+PR PR PR SVR 12 follow up SVR 12 follow up SVR SVR Weeks Telaprevir dose was 1,125 mg every 8 hours when the ART regimen included EFV Part A, patients had no concurrent ART Part B, patients were on stable, predefined ART with either an EFV- or an ATV/rbased regimen Adapted from Dieterich D, et al CROI Seattle USA. Oral Presentation 46.
58 Boceprevir (BOC) + pegylated interferon-α-2b + ribavirin for the treatment of HCV/HIV-coinfected patients Weeks Arm 1 PEG2b+ RBV 4wk Placebo + PEG2b + RBV 44wk Follow up SVR-24wk Arm 2 PEG2b+ RBV 4wk Bocepravir + PEG2b + RBV 44wk Follow up SVR-24wk Futility rules Two-arm study, double blinded for BOC, open-label for PEG2b/RBV 2:1 randomisation (experimental: control) BOC dose 800 mg TID 4-week lead-in with PEG2b/RBV for all patients PEG-2b 1.5µg/kg QW; RBV 600 1,400 mg/day divided BID Adapted from Sulkowski M, et al CROI Seattle USA. Oral Presentation 47.

 0% TVR + PR (n=38) 8% DC due to AEs PR (n=34) 9% BOC + PR (n=64) 20% Primary endpoint=svr at 12 weeks; interim analysis presented; TVR=telaprevir *Pegylated")
59 Patients with SVR12 (%) Patients with SVR12 (%) SVR12 with TVR or BOC + pegylated interferon and ribavirin (PR) vs PR alone in HIV/HCV coinfection SVR12: TVR + PR vs PR 1* SVR12: BOC + PR vs PR 2** 100 No ART EFV-based ART 69 ATV-based ART Total /7 11/ 16 TVR + PR 12/ 28/ /6 4/8 4/8 10/ 22 Placebo + PR Rebound in HIV-1 RNA not observed in any patient /61 9/34 BOC + PR Placebo + PR HIV-1 RNA breakthrough observed in 7 patients DC due to AEs PR (n=22) 0% TVR + PR (n=38) 8% DC due to AEs PR (n=34) 9% BOC + PR (n=64) 20% Primary endpoint=svr at 12 weeks; interim analysis presented; TVR=telaprevir *Pegylated interferon-α-2a; **Pegylated interferon-α-2b. Adapted from: 1. Dieterich DT, et al. CROI Seattle USA. Oral Presentation 46; 2. Sulkowski MS, et al. CROI Seattle USA. Oral Presentation 47. Primary endpoint=svr at 44 weeks; interim analysis presented

60 Tolerability and safety signals from the pilot studies

61 NB: HCV PIs, cyp450 metabolised, so important DDIs
62 Kinetic Guided Rx length TVR W4 W8 W12 W24 W48 Rx Naïve/ Relapsers PIFN + R + TVR ervr+ P + R P + R ervr- Partial Responders/ Non-Responders/ Cirrhotics?HIV PIFN + R + TVR P + R Stopping Rules Week 4 or week 12 HCV RNA >1000 U/l
63 BOV- kinetic guided Rx length W4 W8 W12 W28 W36 W48 ervr+ PIFN + R + BOV Rx Naïve P + R ervr- PIFN + R + BOV P + R Partial Responders/ Relapsers PIFN + R + BOV P + R P + R Cirrhotics(and?HIV+) PIFN + R + BOV Stopping Rules week 12 >100 U/l
64 Stopping Rules for BOC and TVR Established as futility rule in PegIFN/Rib Reduce exposure to potentially toxic drugs Cost-benefit In DAAs, also helpful to stop emergence of further Resistance Associated Variants Boceprevir Week 12 HCV RNA >100 IU/l Week 12 detectable HCV RNA Telaprevir Week 4 HCV RNA >1000 IU/l Week 8 HCV RNA >1000 IU/l Week 12 detectable HCV RNA
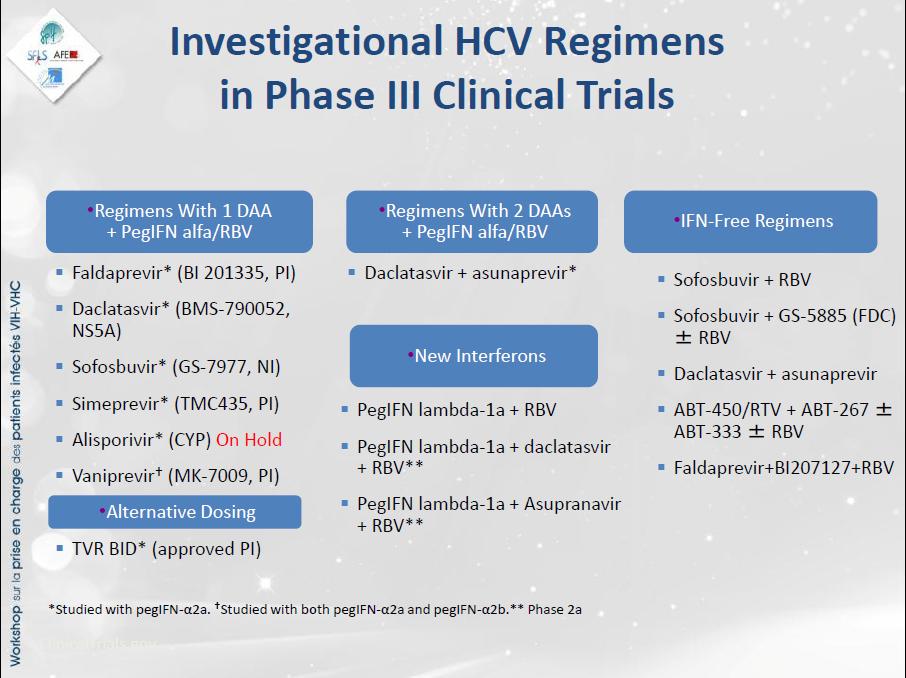
65 So what s on the horizon? New once daily new generation PIs with pifn and Ribavirin PegIFN-lamda in combination with NS5a inhibitor and ribavirin IFN-free therapies
66 Management of newly diagnosed HIV-HCV coinfected Management of genotype-1 HIV/HCV Co-infected patients Genotype 1 Patients Newly diagnosed chronic HCV GT 1 infection Perform transient elastography and/or serum marker and/or liver biopsy F0F1 a F2F3 a F4 a In general, treatment can be deferred. Consider treatment with Peg/RBV and an HCV protease inhibitor or Peg/RBV alone if low HCV viral load, IL28B CC genotype, absence of insulin resistance and high CD4+ cell count. Treatment with Peg/RBV and an HCV protease inhibitor. Treatment with Peg/RBV and an HCV protease inhibitor if compensated disease. Treatment should be undergone in specialised centres. a Metavir fibrosis score: F0=no fibrosis; F1= portal fibrosis, no septae; F2= portal fibrosis, few septae, F3=bridging fibrosis, F4=cirrhosis. EACS Heptitis/HIV Guidelines 2012

67 BOC in F4 disease in HCV monoinfection

")
68 French EAP TVR/BOC in patients with advanced fibrosis and previous non-response (CUPIC) Hezode, et al EASL 2012

69 Is IFN-free therapy a reality?


70 Combining DAAs Nuc + NS5a (Electron study)


71 Aviator study combining Nuc+NS5a +/- Non-nuc +/- R
72 HCV Rx landscape the future? pifn + R + PI for urgent Need pifn + R (g3/g2 + acute HCV) Monitor frequently Early cart Clinical Trials IFN-alpha Historical therapy! Use of IL28B? P/R lead-in phase? Response guided therapy First line 1 or 2 DAA + R 2 or 3 DAAs 2 nd Line 2DAAs + P+R 2 or 3 DAAs
73 Challenges for 2013 Global testing/access for HBV/HCV and anti-hbv/hcv treatment HCV/HIV Rx now or wait? What do with PegIFN/R null-reponders and triple therapy failures?

74 HIV/Hepatitis - unequal Burden?
HIV/HBV co-infection Les Liasions Dangereuses
 HIV/HBV co-infection Les Liasions Dangereuses Sanjay Bhagani Infectious Diseases/HIV Medicine Royal Free Hospital Sanjay Bhagani, Royal Free Hospital, London Reena Shah, AKUH, Nairobi Liver Related Mortality
HIV/HBV co-infection Les Liasions Dangereuses Sanjay Bhagani Infectious Diseases/HIV Medicine Royal Free Hospital Sanjay Bhagani, Royal Free Hospital, London Reena Shah, AKUH, Nairobi Liver Related Mortality
HIV/HCV co-infected patients should be prioritised for HCV treatment. Sanjay Bhagani Royal Free Hospital/UCL London
 HIV/HCV co-infected patients should be prioritised for HCV treatment Sanjay Bhagani Royal Free Hospital/UCL London Also requires other resources What should a prioritisation process Life-saving at this
HIV/HCV co-infected patients should be prioritised for HCV treatment Sanjay Bhagani Royal Free Hospital/UCL London Also requires other resources What should a prioritisation process Life-saving at this
Treatment of chronic hepatitis C in HIV co-infected patients
 Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
Treatment of chronic hepatitis C in HIV co-infected patients Vicente Soriano Department of Infectious Diseases Hospital Carlos III, Madrid, Spain The most prevalent chronic viral infections in humans HBV
HIV/hepatitis co-infection. Christoph Boesecke Department of Medicine I University Hospital Bonn Germany
 HIV/hepatitis co-infection Christoph Boesecke Department of Medicine I University Hospital Bonn Germany Clinical Management and Treatment of HBV and HCV Co-infection in HIVpositive Persons Hepatitis B
HIV/hepatitis co-infection Christoph Boesecke Department of Medicine I University Hospital Bonn Germany Clinical Management and Treatment of HBV and HCV Co-infection in HIVpositive Persons Hepatitis B
Acute Hepatitis B Virus Infection with Recovery
 Hepatitis B: Clear as Mud Melissa Osborn, MD, MSCR Assistant Professor Emory University School of Medicine Atlanta, GA 1 Objectives 1. Distinguish the various stages in the natural history of chronic hepatitis
Hepatitis B: Clear as Mud Melissa Osborn, MD, MSCR Assistant Professor Emory University School of Medicine Atlanta, GA 1 Objectives 1. Distinguish the various stages in the natural history of chronic hepatitis
COMPETING INTEREST OF FINANCIAL VALUE
 Sixth Annual BHIVA Conference for the Management of HIV/Hepatitis Co-Infection in collaboration with BASL and BVHG Dr Ed Wilkins North Manchester General Hospital COMPETING INTEREST OF FINANCIAL VALUE
Sixth Annual BHIVA Conference for the Management of HIV/Hepatitis Co-Infection in collaboration with BASL and BVHG Dr Ed Wilkins North Manchester General Hospital COMPETING INTEREST OF FINANCIAL VALUE
Professor Vincent Soriano
 Five Nations Conference on HIV and Hepatitis in partnership with Professor Vincent Soriano Hospital Carlos III, Madrid, Spain Professor Vincent Soriano in partnership with Hospital Carlos III, Madrid,
Five Nations Conference on HIV and Hepatitis in partnership with Professor Vincent Soriano Hospital Carlos III, Madrid, Spain Professor Vincent Soriano in partnership with Hospital Carlos III, Madrid,
Access to care and response to HCV treatment in Europe. Sanjay Bhagani Royal Free Hospital/UCL London
 Access to care and response to HCV treatment in Europe Sanjay Bhagani Royal Free Hospital/UCL London Access to care and response to HCV treatment in Europe Overview HCV/HIV co-infection in Europe Current
Access to care and response to HCV treatment in Europe Sanjay Bhagani Royal Free Hospital/UCL London Access to care and response to HCV treatment in Europe Overview HCV/HIV co-infection in Europe Current
HBV in HIV Forgotten but not Gone
 Activity Code FA376 HBV in HIV Forgotten but not Gone Richard K. Sterling, MD, MSc VCU Hepatology Professor of Medicine Chief, Section of Hepatology Virginia Commonwealth University Learning Objectives
Activity Code FA376 HBV in HIV Forgotten but not Gone Richard K. Sterling, MD, MSc VCU Hepatology Professor of Medicine Chief, Section of Hepatology Virginia Commonwealth University Learning Objectives
Predictors of Response to Hepatitis C Therapy in the DAA Era. Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid
 Predictors of Response to Hepatitis C Therapy in the DAA Era Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid Why Predicting HCV Response? Select candidates for therapy Prioritizing
Predictors of Response to Hepatitis C Therapy in the DAA Era Pablo Barreiro Servicio de Enfermedades Infecciosas Hospital Carlos III, Madrid Why Predicting HCV Response? Select candidates for therapy Prioritizing
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Viral Hepatitis and HIV. Norah Terrault, MD, MPH Professor of Medicine Director, Viral Hepatitis Center University of California San Francisco
 Viral Hepatitis and HIV Norah Terrault, MD, MPH Professor of Medicine Director, Viral Hepatitis Center University of California San Francisco Faculty Disclosures Grant support - Vertex, Roche, Novartis,
Viral Hepatitis and HIV Norah Terrault, MD, MPH Professor of Medicine Director, Viral Hepatitis Center University of California San Francisco Faculty Disclosures Grant support - Vertex, Roche, Novartis,
Hepatitis B Virus therapy. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Case #1. Case #1. Case #1: Audience vote VS. The Great Debate: When to Treat HCV in our HIV coinfected patients
 Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
Case #1 The Great Debate: When to Treat HCV in our HIV coinfected patients Medical Management of AIDS December, 2012 Moderated by George Beatty,MD 35 year old African American man, CD4 + 450, HIV RNA
Treatment of Hepatitis C in HIV-Coinfected Patients. Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain
 Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Treatment of Hepatitis C in HIV-Coinfected Patients Vincent Soriano Department of Infectious Diseases Hospital Carlos III Madrid, Spain Estimated no. of persons infected with HIV and hepatitis viruses
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy?
 Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
Management of CHC G1 patients who are relapsers or non-responders to Peg IFN and RBV therapy: Wait or Triple Therapy? Prof. Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors
 Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Treatment of Chronic Hepatitis C in HIV infection
 Treatment of Chronic Hepatitis C in HIV infection June 25, 211 Andrew Talal, MD, MPH Associate Professor of Medicine Associate Medical Director Center for the Study of Hepatitis C Weill Cornell Medical
Treatment of Chronic Hepatitis C in HIV infection June 25, 211 Andrew Talal, MD, MPH Associate Professor of Medicine Associate Medical Director Center for the Study of Hepatitis C Weill Cornell Medical
Hepatitis C & HIV Coinfection and Brief Advances on Hepatitis B & HIV: The Evidence and New Proposals
 Hepatitis C & HIV Coinfection and Brief Advances on Hepatitis B & HIV: The Evidence and New Proposals Douglas G. Fish, MD Albany Medical College April 3, 2009 Cali Colombia Objectives HCV Epidemiology
Hepatitis C & HIV Coinfection and Brief Advances on Hepatitis B & HIV: The Evidence and New Proposals Douglas G. Fish, MD Albany Medical College April 3, 2009 Cali Colombia Objectives HCV Epidemiology
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
Viral Hepatitis The Preventive Potential of Antiviral Therapy. Thomas Berg
 Viral Hepatitis The Preventive Potential of Antiviral Therapy Thomas Berg Therapeutic and preventive strategies in patients with hepatitis virus infection Treatment of acute infection Treatment of chronic
Viral Hepatitis The Preventive Potential of Antiviral Therapy Thomas Berg Therapeutic and preventive strategies in patients with hepatitis virus infection Treatment of acute infection Treatment of chronic
Viral hepatitis in patients living with HIV: can we still speak of special population?
 Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
Viral hepatitis in patients living with HIV: can we still speak of special population? Maurizio Bonacini, M.D., A.G.A.F. Mission Gastroenterology and Hepatology San Francisco, CA YES for HBV Excluded by
Hepatitis B Virus therapy. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Hepatitis B Virus therapy Maria Buti Hospital Universitario Valle Hebron Barcelona Spain Disclosures Advisor: AbbVie, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen, Merck Sharp &
Protease inhibitor based triple therapy in treatment experienced patients
 Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Management of Chronic Hepatitis B in Asian Americans
 Management of Chronic Hepatitis B in Asian Americans Myron J Tong; UCLA, CA Calvin Q. Pan; Mount Sinai, NY Hie-Won Hann; Thomas Jefferson, PA Kris V. Kowdley; Virginia Mason, WA Steven Huy B Han; UCLA,
Management of Chronic Hepatitis B in Asian Americans Myron J Tong; UCLA, CA Calvin Q. Pan; Mount Sinai, NY Hie-Won Hann; Thomas Jefferson, PA Kris V. Kowdley; Virginia Mason, WA Steven Huy B Han; UCLA,
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy
 How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
Hepatitis Delta. Vicente Soriano Infectious Diseases Unit La Paz University Hospital & IdiPAZ Madrid, Spain
 Hepatitis Delta Vicente Soriano Infectious Diseases Unit La Paz University Hospital & IdiPAZ Madrid, Spain Disclosures Member of speaker bureau and advisory board for: Roche, Boehringer, Gilead, Viiv,
Hepatitis Delta Vicente Soriano Infectious Diseases Unit La Paz University Hospital & IdiPAZ Madrid, Spain Disclosures Member of speaker bureau and advisory board for: Roche, Boehringer, Gilead, Viiv,
Cornerstones of Hepatitis B: Past, Present and Future
 Cornerstones of Hepatitis B: Past, Present and Future Professor Man-Fung Yuen Queen Mary Hospital The University of Hong Kong Hong Kong 1 Outline Past Natural history studies Development of HBV-related
Cornerstones of Hepatitis B: Past, Present and Future Professor Man-Fung Yuen Queen Mary Hospital The University of Hong Kong Hong Kong 1 Outline Past Natural history studies Development of HBV-related
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
A tale of two patients
 15 th Annual Resistance and Antiviral Therapy Meeting Dr Sanjay Bhagani Royal Free Hospital, London Thursday 29 September 2011, Royal College of Physicians, London A tale of two patients Sanjay Bhagani
15 th Annual Resistance and Antiviral Therapy Meeting Dr Sanjay Bhagani Royal Free Hospital, London Thursday 29 September 2011, Royal College of Physicians, London A tale of two patients Sanjay Bhagani
HIV and Hepatitis C: Advances in Treatment
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and Hepatitis C: Advances in Treatment John Scott, MD, MSc Asst Professor University of Washington Presentation prepared & presented by: John Scott, MD,
Chronic Hepatitis B: management update.
 Chronic Hepatitis B: management update. E.O.Ogutu Department of clinical medicine & therapeutics, University of Nairobi. Physicians meeting,kisumu 2011. Background epidemiology Chronic hepatitis B (CHB)
Chronic Hepatitis B: management update. E.O.Ogutu Department of clinical medicine & therapeutics, University of Nairobi. Physicians meeting,kisumu 2011. Background epidemiology Chronic hepatitis B (CHB)
Treatment of chronic hepatitis B 2013 update
 22 February 213 Treatment of chronic hepatitis B 213 update Pietro Lampertico 1st Gastroenterology Unit Fondazione IRCCS Cà Granda - Ospedale Maggiore Policlinico Università di Milano EASL 212 Clinical
22 February 213 Treatment of chronic hepatitis B 213 update Pietro Lampertico 1st Gastroenterology Unit Fondazione IRCCS Cà Granda - Ospedale Maggiore Policlinico Università di Milano EASL 212 Clinical
The Impact of HBV Therapy on Fibrosis and Cirrhosis
 The Impact of HBV Therapy on Fibrosis and Cirrhosis Jordan J. Feld, MD, MPH Associate Professor of Medicine University of Toronto Hepatologist Toronto Centre for Liver Disease Sandra Rotman Centre for
The Impact of HBV Therapy on Fibrosis and Cirrhosis Jordan J. Feld, MD, MPH Associate Professor of Medicine University of Toronto Hepatologist Toronto Centre for Liver Disease Sandra Rotman Centre for
HIV coinfection and HCC
 HIV coinfection and HCC 3 rd APASL STC on HCC 21 st -23 rd Nov 2013 Cebu, Phillippines George KK Lau MBBS (HK), MRCP(UK), FHKCP, FHKAM (GI), MD(HK), FRCP (Edin, Lond) Consultant, Humanity and Health GI
HIV coinfection and HCC 3 rd APASL STC on HCC 21 st -23 rd Nov 2013 Cebu, Phillippines George KK Lau MBBS (HK), MRCP(UK), FHKCP, FHKAM (GI), MD(HK), FRCP (Edin, Lond) Consultant, Humanity and Health GI
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Hepatitis C: a treatment revolution
 Sunday, 10th July 2016 Michaelmas Cay 2 Room Concurrent 11 Health Innovation Hepatitis C: a treatment revolution Dr. Heather McNamee Hepatitis C a treatment revolution Dr Heather McNamee Medical Director
Sunday, 10th July 2016 Michaelmas Cay 2 Room Concurrent 11 Health Innovation Hepatitis C: a treatment revolution Dr. Heather McNamee Hepatitis C a treatment revolution Dr Heather McNamee Medical Director
Dr David Rowbotham NHS. The Leeds Teaching Hospitals. NHS Trust
 Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Nurses Update June 2010 Chronic Hepatitis HBV / HCV David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Nurses Update June 2010 Chronic Hepatitis HBV / HCV David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
NUCs for Chronic Hepatitis B. Rafael Esteban Hospital Universitario Valle Hebron and Ciberehd del Instituto Carlos III. Barcelona.
 NUCs for Chronic Hepatitis B Rafael Esteban Hospital Universitario Valle Hebron and Ciberehd del Instituto Carlos III. Barcelona. Spain Disclosures Advisory board of, and/or, received speaker fee from
NUCs for Chronic Hepatitis B Rafael Esteban Hospital Universitario Valle Hebron and Ciberehd del Instituto Carlos III. Barcelona. Spain Disclosures Advisory board of, and/or, received speaker fee from
Hepatitis C Management and Treatment
 Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
Hepatitis C Management and Treatment Kaya Süer Near East University Faculty of Medicine Infectious Diseases and Clinical Microbiology 1 Discovery of Hepatitis C Key facts Hepatitis C: the virus can cause
Clinical cases: HIV/HCV coinfection
 Clinical cases: HIV/HCV coinfection José Vicente Fernández-Montero Hospital Carlos III, Madrid Case #1 General considerations about antiviral therapy CASE # 1 43 year-old, male patient Former IDU No prior
Clinical cases: HIV/HCV coinfection José Vicente Fernández-Montero Hospital Carlos III, Madrid Case #1 General considerations about antiviral therapy CASE # 1 43 year-old, male patient Former IDU No prior
Clinical Cases Hepatitis C Naïve Patients. Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona.
 Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Clinical Cases Hepatitis C Naïve Patients Rafael Esteban Liver Unit. Hospital General Universitari Vall Hebron. Barcelona. Case study 1 27 year old woman, Diagnosed with Chronic Hepatitis C 3 years ago
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Should Elderly CHC Patients (>70 years old) be Treated?
 be Treated?") Should Elderly CHC Patients (>70 years old) be Treated? Deepak Amarapurkar Consultant Gastroenterologist & Hepatologist Bombay Hospital & Medical Research Center, Mumbai & Jagjivanram Western Railway Hospital,
Should Elderly CHC Patients (>70 years old) be Treated? Deepak Amarapurkar Consultant Gastroenterologist & Hepatologist Bombay Hospital & Medical Research Center, Mumbai & Jagjivanram Western Railway Hospital,
Hepatitis B. Epidemiology and Natural History and Implications for Treatment
 Hepatitis B Epidemiology and Natural History and Implications for Treatment Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco
Hepatitis B Epidemiology and Natural History and Implications for Treatment Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco
Basics of hepatitis B diagnostics. Dr Emma Page MRCP MD(Res) Locum Consultant Sexual Health & Virology
 Locum Consultant Sexual Health & Virology") Basics of hepatitis B diagnostics Dr Emma Page MRCP MD(Res) Locum Consultant Sexual Health & Virology Basics of hepatitis B diagnostics Background Epidemiology Morphology Life-cycle Diagnostic markers
Basics of hepatitis B diagnostics Dr Emma Page MRCP MD(Res) Locum Consultant Sexual Health & Virology Basics of hepatitis B diagnostics Background Epidemiology Morphology Life-cycle Diagnostic markers
HBV/HCV COINFECTIONS IN PATIENTS WITH HIV. Dr Reena Harania MBBS, MRCP, MSc Infectious Disease
 HBV/HCV COINFECTIONS IN PATIENTS WITH HIV Dr Reena Harania MBBS, MRCP, MSc Infectious Disease Adults and children estimated to be living with HIV as of end 2005 North America 1.2 million [650 000 1.8 million]
HBV/HCV COINFECTIONS IN PATIENTS WITH HIV Dr Reena Harania MBBS, MRCP, MSc Infectious Disease Adults and children estimated to be living with HIV as of end 2005 North America 1.2 million [650 000 1.8 million]
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors
 Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Management of Decompensated Chronic Hepatitis B
 Management of Decompensated Chronic Hepatitis B Dr James YY Fung, FRACP, MD Department of Medicine The University of Hong Kong Liver Transplant Center Queen Mary Hospital State Key Laboratory for Liver
Management of Decompensated Chronic Hepatitis B Dr James YY Fung, FRACP, MD Department of Medicine The University of Hong Kong Liver Transplant Center Queen Mary Hospital State Key Laboratory for Liver
Viral hepatitis in reproductive health. Pierre Jean Malè. Training in Reproductive Health Research - Geneva 2006
 Viral hepatitis in reproductive health Pierre Jean Malè Training in Reproductive Health Research - Geneva 2006 15.03.2006 HBV and HCV treatment Pierre-Jean Malè MD 15.03.2006 Global Impact of Hepatitis
Viral hepatitis in reproductive health Pierre Jean Malè Training in Reproductive Health Research - Geneva 2006 15.03.2006 HBV and HCV treatment Pierre-Jean Malè MD 15.03.2006 Global Impact of Hepatitis
Viral hepatitis and Hepatocellular Carcinoma
 Viral hepatitis and Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Viral hepatitis and Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Learning Objectives. Disclosures (Activity w/i 12 months) WHY DISCUSS HCV/HIV COINFECTION? HCV/HIV Effect on Health Utilization in A5001
 WHY DISCUSS HCV/HIV COINFECTION? HCV/HIV Effect on Health Utilization in A5001") Learning Objectives HCV/HIV COINFECTION Soup to Nuts Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine At the
Learning Objectives HCV/HIV COINFECTION Soup to Nuts Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine At the
Primary Care for Hepatitis B and C:
 Primary Care for Hepatitis B and C: Clinical Tools for Efficient Management Estimated 17 Million Persons With HCV Infection Worldwide 3-4 million newly infected each yr worldwide Advances in Internal Medicine
Primary Care for Hepatitis B and C: Clinical Tools for Efficient Management Estimated 17 Million Persons With HCV Infection Worldwide 3-4 million newly infected each yr worldwide Advances in Internal Medicine
Update on HIV-HCV Epidemiology and Natural History
 Update on HIV-HCV Epidemiology and Natural History Jennifer Price, MD Assistant Clinical Professor of Medicine University of California, San Francisco Learning Objectives Upon completion of this presentation,
Update on HIV-HCV Epidemiology and Natural History Jennifer Price, MD Assistant Clinical Professor of Medicine University of California, San Francisco Learning Objectives Upon completion of this presentation,
Meet the Professor: HIV/HCV Coinfection
 Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Meet the Professor: HIV/HCV Coinfection Vincent Lo Re, MD, MSCE Assistant Professor of Medicine and Epidemiology Division of Infectious Diseases Center for Clinical Epidemiology and Biostatistics University
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Hepatitis C in HIV Patients: The Speeding Sidecar. Andrew Desruisseau, MD,MSCI Assistant Professor Meharry Medical College
 Hepatitis C in HIV Patients: The Speeding Sidecar Andrew Desruisseau, MD,MSCI Assistant Professor Meharry Medical College Patient: Mr. DW 40 year old AAM admitted with fever, nonproductive cough and hypoxemia
Hepatitis C in HIV Patients: The Speeding Sidecar Andrew Desruisseau, MD,MSCI Assistant Professor Meharry Medical College Patient: Mr. DW 40 year old AAM admitted with fever, nonproductive cough and hypoxemia
Don t interfere My first choice is always nucs!
 Don t interfere My first choice is always nucs! Robert G Gish MD Professor Consultant Stanford University Medical Director, Hepatitis B Foundation Singapore Viral Hepatitis Meeting 2014 1 Disclosures Dr
Don t interfere My first choice is always nucs! Robert G Gish MD Professor Consultant Stanford University Medical Director, Hepatitis B Foundation Singapore Viral Hepatitis Meeting 2014 1 Disclosures Dr
Novedades en el tratamiento de la hepatitis B: noticias desde la EASL. Maria Buti Hospital Universitario Valle Hebrón Barcelona
 Novedades en el tratamiento de la hepatitis B: noticias desde la EASL Maria Buti Hospital Universitario Valle Hebrón Barcelona Milestones in CHB treatment Conventional IFN 1991 Lamivudine (LAM) 1998 Adefovir
Novedades en el tratamiento de la hepatitis B: noticias desde la EASL Maria Buti Hospital Universitario Valle Hebrón Barcelona Milestones in CHB treatment Conventional IFN 1991 Lamivudine (LAM) 1998 Adefovir
HCV Case Study. Treat Now or Wait for New Therapies
 HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
HIV HCV Co Infection Case: The Agnostic Radiologist
 HIV HCV Co Infection Case: The Agnostic Radiologist Douglas T. Dieterich, M.D Professor of Medicine Division of Liver Diseases, Gastroenterology and Infectious Diseases Department of Medicine Mount Sinai
HIV HCV Co Infection Case: The Agnostic Radiologist Douglas T. Dieterich, M.D Professor of Medicine Division of Liver Diseases, Gastroenterology and Infectious Diseases Department of Medicine Mount Sinai
Over the past decade, the introduction of
 MANAGEMENT OF CHRONIC HEPATITIS C IN HIV-INFECTED PATIENTS: CLINICAL EXPERIENCE WITH PEGYLATED INTERFERON α PLUS RIBAVIRIN Raymond T. Chung, MD* ABSTRACT Coinfection with hepatitis C virus (HCV) is common
MANAGEMENT OF CHRONIC HEPATITIS C IN HIV-INFECTED PATIENTS: CLINICAL EXPERIENCE WITH PEGYLATED INTERFERON α PLUS RIBAVIRIN Raymond T. Chung, MD* ABSTRACT Coinfection with hepatitis C virus (HCV) is common
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Oral combination therapy: future hepatitis C virus treatment? "Lancet Oct 30;376(9751): Oral combination therapy with a nucleoside
: Oral combination therapy with a nucleoside") Author manuscript, published in "Journal of Hepatology 2011;55(4):933-5" DOI : 10.1016/j.jhep.2011.04.018 Oral combination therapy: future hepatitis C virus treatment? Commentary article on the following
Author manuscript, published in "Journal of Hepatology 2011;55(4):933-5" DOI : 10.1016/j.jhep.2011.04.018 Oral combination therapy: future hepatitis C virus treatment? Commentary article on the following
Current State of Treatment for HCV. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 Activity Code FA376 Current State of Treatment for HCV Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives Upon completion of this presentation, learners should be
Activity Code FA376 Current State of Treatment for HCV Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives Upon completion of this presentation, learners should be
Clinical Management of Hepatitis B WAN-CHENG CHOW DEPARTMENT OF GASTROENTEROLOGY & HEPATOLOGY SINGAPORE GENERAL HOSPITAL
 Clinical Management of Hepatitis B WAN-CHENG CHOW DEPARTMENT OF GASTROENTEROLOGY & HEPATOLOGY SINGAPORE GENERAL HOSPITAL The World Health Organisation recent initiatives on HBV infection Launching of the
Clinical Management of Hepatitis B WAN-CHENG CHOW DEPARTMENT OF GASTROENTEROLOGY & HEPATOLOGY SINGAPORE GENERAL HOSPITAL The World Health Organisation recent initiatives on HBV infection Launching of the
Clinical dilemmas in HBeAg-negative CHB
 Clinical dilemmas in HBeAg-negative CHB George V. Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National & Kapodistrian University of Athens Director of Academic Department
Clinical dilemmas in HBeAg-negative CHB George V. Papatheodoridis Professor in Medicine & Gastroenterology Medical School of National & Kapodistrian University of Athens Director of Academic Department
Hepatitis B. ECHO November 29, Joseph Ahn, MD, MS Associate Professor of Medicine Director of Hepatology Oregon Health & Science University
 Hepatitis B ECHO November 29, 2017 Joseph Ahn, MD, MS Associate Professor of Medicine Director of Hepatology Oregon Health & Science University Disclosures Advisory board Gilead Comments The speaker Joseph
Hepatitis B ECHO November 29, 2017 Joseph Ahn, MD, MS Associate Professor of Medicine Director of Hepatology Oregon Health & Science University Disclosures Advisory board Gilead Comments The speaker Joseph
Treatment of chronic hepatitis C in drug-naïve patients
 Treatment of chronic hepatitis C in drug-naïve patients 8th International Workshop on HIV & Hepatitis Co-infection Madrid, 31. May 2012 Christoph Sarrazin J. W. Goethe-University Hospital Medizinische
Treatment of chronic hepatitis C in drug-naïve patients 8th International Workshop on HIV & Hepatitis Co-infection Madrid, 31. May 2012 Christoph Sarrazin J. W. Goethe-University Hospital Medizinische
HBV Diagnosis and Treatment
 HBV Diagnosis and Treatment Anna S. F. Lok, MD Alice Lohrman Andrews Professor in Hepatology Director of Clinical Hepatology Assistant Dean for Clinical Research University of Michigan Ann Arbor, MI, USA
HBV Diagnosis and Treatment Anna S. F. Lok, MD Alice Lohrman Andrews Professor in Hepatology Director of Clinical Hepatology Assistant Dean for Clinical Research University of Michigan Ann Arbor, MI, USA
Introduction. The ELECTRON Trial
 63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
Hepatocellular Carcinoma: Can We Slow the Rising Incidence?
 Hepatocellular Carcinoma: Can We Slow the Rising Incidence? K.Rajender Reddy M.D. Professor of Medicine Director of Hepatology Medical Director of Liver Transplantation University of Pennsylvania Outline
Hepatocellular Carcinoma: Can We Slow the Rising Incidence? K.Rajender Reddy M.D. Professor of Medicine Director of Hepatology Medical Director of Liver Transplantation University of Pennsylvania Outline
HBV Therapy in Special Populations: Liver Cirrhosis
 HBV Therapy in Special Populations: Liver Cirrhosis Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
HBV Therapy in Special Populations: Liver Cirrhosis Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
HIV-HBV coinfection: Issues with treatment in 2018
 HIV-HBV coinfection: Issues with treatment in 2018 Pr Karine Lacombe, INSERM UMR-S1136, IPLESP Infectious Diseases Dpt, St Antoine, AP-HP Sorbonne Université, Paris, France Global epidemiology Same routes
HIV-HBV coinfection: Issues with treatment in 2018 Pr Karine Lacombe, INSERM UMR-S1136, IPLESP Infectious Diseases Dpt, St Antoine, AP-HP Sorbonne Université, Paris, France Global epidemiology Same routes
SHOULD EVERYONE WITH HCV/HIV COINFECTION BE TREATED NOW?
 SHOULD EVERYONE WITH HCV/HIV COINFECTION BE TREATED NOW? Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Disclosures
SHOULD EVERYONE WITH HCV/HIV COINFECTION BE TREATED NOW? Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Disclosures
New Therapies on the Horizon in Hepatitis C Patients Paul Y. Kwo, MD
 Viral Targets for HCV New Therapies on the Horizon in Hepatitis C Patients Paul Y. Kwo, MD Sites for development of inhibitors Metalloproteinase Serine protease (trans) Core E E2 NS2 NS3 NS4a/NS4b NS5a/NS5b
Viral Targets for HCV New Therapies on the Horizon in Hepatitis C Patients Paul Y. Kwo, MD Sites for development of inhibitors Metalloproteinase Serine protease (trans) Core E E2 NS2 NS3 NS4a/NS4b NS5a/NS5b
Treatment as a form of liver cancer prevention The clinical efficacy and cost effectiveness of treatment across Asia
 Treatment as a form of liver cancer prevention The clinical efficacy and cost effectiveness of treatment across Asia Prof. Henry LY Chan Head, Division of Gastroenterology and Hepatology Director, Institute
Treatment as a form of liver cancer prevention The clinical efficacy and cost effectiveness of treatment across Asia Prof. Henry LY Chan Head, Division of Gastroenterology and Hepatology Director, Institute
Optimized HBV Treatment Through Baseline and on-treatment Predictor Oral Antiviral Therapy. Watcharasak Chotiyaputta
 Optimized HBV Treatment Through Baseline and on-treatment Predictor Oral Antiviral Therapy Watcharasak Chotiyaputta Progression of Liver Disease Goal of HBV Treatment: prevention the development of cirrhosis
Optimized HBV Treatment Through Baseline and on-treatment Predictor Oral Antiviral Therapy Watcharasak Chotiyaputta Progression of Liver Disease Goal of HBV Treatment: prevention the development of cirrhosis
British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2
 British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2 Systematic literature search 2.1 Questions and PICO criteria Data bases: Medline,
British HIV Association Guidelines for the Management of Hepatitis Viruses in Adults Infected with HIV 2013 Appendix 2 Systematic literature search 2.1 Questions and PICO criteria Data bases: Medline,
An Update HBV Treatment
 An Update HBV Treatment Epidemiology Natural history Treatment Daryl T.-Y. Lau, MD, MPH Associate Professor of Medicine Director of Translational Liver Research Division of Gastroenterology BIDMC, Harvard
An Update HBV Treatment Epidemiology Natural history Treatment Daryl T.-Y. Lau, MD, MPH Associate Professor of Medicine Director of Translational Liver Research Division of Gastroenterology BIDMC, Harvard
Management of chronic hepatitis B : recent advance in the treatment of antiviral resistance
 anagement of chronic hepatitis B : recent advance in the treatment of antiviral resistance / 김강모 연수강좌 anagement of chronic hepatitis B : recent advance in the treatment of antiviral resistance 김강모 울산대학교의과대학서울아산병원소화기내과
anagement of chronic hepatitis B : recent advance in the treatment of antiviral resistance / 김강모 연수강좌 anagement of chronic hepatitis B : recent advance in the treatment of antiviral resistance 김강모 울산대학교의과대학서울아산병원소화기내과
How to use pegylated Interferon for Chronic Hepatitis B in 2015
 How to use pegylated Interferon for Chronic Hepatitis B in 215 Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of Songkla University, Thailand ASIAN-PACIFIC CLINICAL PRACTICE
How to use pegylated Interferon for Chronic Hepatitis B in 215 Teerha Piratvisuth NKC Institute of Gastroenterology and Hepatology Prince of Songkla University, Thailand ASIAN-PACIFIC CLINICAL PRACTICE
Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona
 Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona rrent HCV Therapy 8% % sustained response 6% 4% 2% % 54-61% 41% 34% 25% 16% 6% IFN 24w IFN 48w Peg
Tratamiento de la Hepatitis C Rafael Esteban Hospital General Universitario Valle de Hebrón Barcelona rrent HCV Therapy 8% % sustained response 6% 4% 2% % 54-61% 41% 34% 25% 16% 6% IFN 24w IFN 48w Peg
Update on HBV Treatment
 Update on HBV Treatment Calvin Q. Pan MD, FAASLD, FACG, MACP Professor of Medicine Division of Gastroenterology and Hepatology Department of Medicine, NYU Langone Health New York University School of Medicine,
Update on HBV Treatment Calvin Q. Pan MD, FAASLD, FACG, MACP Professor of Medicine Division of Gastroenterology and Hepatology Department of Medicine, NYU Langone Health New York University School of Medicine,
Influence of Baseline HCV Genotype upon Treatment Outcome of Acute HCV Infection in HIV Co-Infected Individuals
 Influence of Baseline HCV Genotype upon Treatment Outcome of Acute HCV Infection in HIV Co-Infected Individuals Christoph Boesecke, Hans-Jürgen Stellbrink, Stefan Mauss, Emma Page, Mark Nelson, Sanjay
Influence of Baseline HCV Genotype upon Treatment Outcome of Acute HCV Infection in HIV Co-Infected Individuals Christoph Boesecke, Hans-Jürgen Stellbrink, Stefan Mauss, Emma Page, Mark Nelson, Sanjay
Considerations for Antiretroviral Use in Patients with Hepatitis B Virus & Human Immunodeficiency Syndrome Coinfection
 Considerations for Antiretroviral Use in Patients with Hepatitis B Virus & Human Immunodeficiency Syndrome Coinfection Mahnaz Arian, MD Assistant Professor in infectious Disease Mashhad university of Medical
Considerations for Antiretroviral Use in Patients with Hepatitis B Virus & Human Immunodeficiency Syndrome Coinfection Mahnaz Arian, MD Assistant Professor in infectious Disease Mashhad university of Medical
Is there a need for combination therapy? No. Maria Buti Hospital General Universitario Valle Hebron Barcelona. Spain
 Is there a need for combination therapy? No Maria Buti Hospital General Universitario Valle Hebron Barcelona. Spain No, No and No EASL Update HBV Guidelines 2012 The most potent drugs with the optimal
Is there a need for combination therapy? No Maria Buti Hospital General Universitario Valle Hebron Barcelona. Spain No, No and No EASL Update HBV Guidelines 2012 The most potent drugs with the optimal
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
Areas of Interest. HCV Epidemiology, Natural History HCV Treatment. HBV Epidemiology and Prevention. Monoinfected Coinfected
 CROI 2011 UPDATE Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases Univ. of Cincinnati College of Medicine Areas of Interest HCV Epidemiology, Natural History
CROI 2011 UPDATE Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases Univ. of Cincinnati College of Medicine Areas of Interest HCV Epidemiology, Natural History
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
The role of triple therapy with protease inhibitors in hepatitis C virus genotype 1na «ve patients
 The role of triple therapy with protease inhibitors in hepatitis C virus genotype 1na «ve patients David R. Nelson Clinical and Translational Science Institute, University of Florida, FL, USA Liver International
The role of triple therapy with protease inhibitors in hepatitis C virus genotype 1na «ve patients David R. Nelson Clinical and Translational Science Institute, University of Florida, FL, USA Liver International
Interferon-based and interferon-free new treatment options
 Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Glecaprevir-Pibrentasvir in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2)
") Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
HIV-HCV Co-Infection. George Mason University Falls Church, Virginia. Overview. Prevalence of HCV co-infection Incidence and Recent Trends
 HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova
HIV-HCV Co-Infection Zobair Younossi MD, MPH, FACG, AGAF, FAASLD Chairman, Department of Medicine, Inova Fairfax Hospital Vice President for Research, Inova Health System Professor of Medicine, VCU-Inova
Is there a need for combination treatment? Yes!
 18.0.2012 C Hep Meeting Berlin Is there a need for combination treatment? Yes! Florian van Bömmel University Hospital Leipzig Hepatology Section Germany Most patients respond to monotherapy with entecavir
18.0.2012 C Hep Meeting Berlin Is there a need for combination treatment? Yes! Florian van Bömmel University Hospital Leipzig Hepatology Section Germany Most patients respond to monotherapy with entecavir
The medical management of hepatitis C
 CLINICAL EXPERIENCE WITH PEGYLATED INTERFERON α-2a PLUS RIBAVIRIN FOR CHRONIC HEPATITIS C VIRUS INFECTION IN PATIENTS INFECTED WITH HIV: THE APRICOT STUDY Douglas T. Dieterich, MD* ABSTRACT Currently,
CLINICAL EXPERIENCE WITH PEGYLATED INTERFERON α-2a PLUS RIBAVIRIN FOR CHRONIC HEPATITIS C VIRUS INFECTION IN PATIENTS INFECTED WITH HIV: THE APRICOT STUDY Douglas T. Dieterich, MD* ABSTRACT Currently,
Who to Treat? Consider biopsy Treat. > 2 ULN Treat Treat Treat Treat CIRRHOTIC PATIENTS Compensated Treat HBV DNA detectable treat
 Who to Treat? Parameter AASLD US Algorithm EASL APASL HBV DNA CRITERIA HBeAg+ >, IU/mL > 2, IU/mL > 2, IU/mL >, IU/mL HBeAg- > 2, IU/mL > 2, IU/mL > 2, IU/mL > 2, IU/mL ALT CRITERIA PNALT 1-2 ULN Monitor
Who to Treat? Parameter AASLD US Algorithm EASL APASL HBV DNA CRITERIA HBeAg+ >, IU/mL > 2, IU/mL > 2, IU/mL >, IU/mL HBeAg- > 2, IU/mL > 2, IU/mL > 2, IU/mL > 2, IU/mL ALT CRITERIA PNALT 1-2 ULN Monitor