BIOLOGIC THERAPY : A NEW OPTION FOR TREATMENT JUVENILE IDIOPATHIC ARTHRITIS DR TON THAT HOANG
|
|
|
- Kory Little
- 5 years ago
- Views:
Transcription

1 BIOLOGIC THERAPY : A NEW OPTION FOR TREATMENT JUVENILE IDIOPATHIC ARTHRITIS DR TON THAT HOANG
2 INTRODUCTION JIA is the most common chronic rheumatic inflammatory disease of childhood. If not successfully treated, it can lead to severe disability. Juvenile idiopathic arthritis (JIA) is a collective term for arthritides that are diagnosed before the age of 16 years.diagnosis requires disease duration of at least 6 weeks and the exclusion of other causes of arthritis.
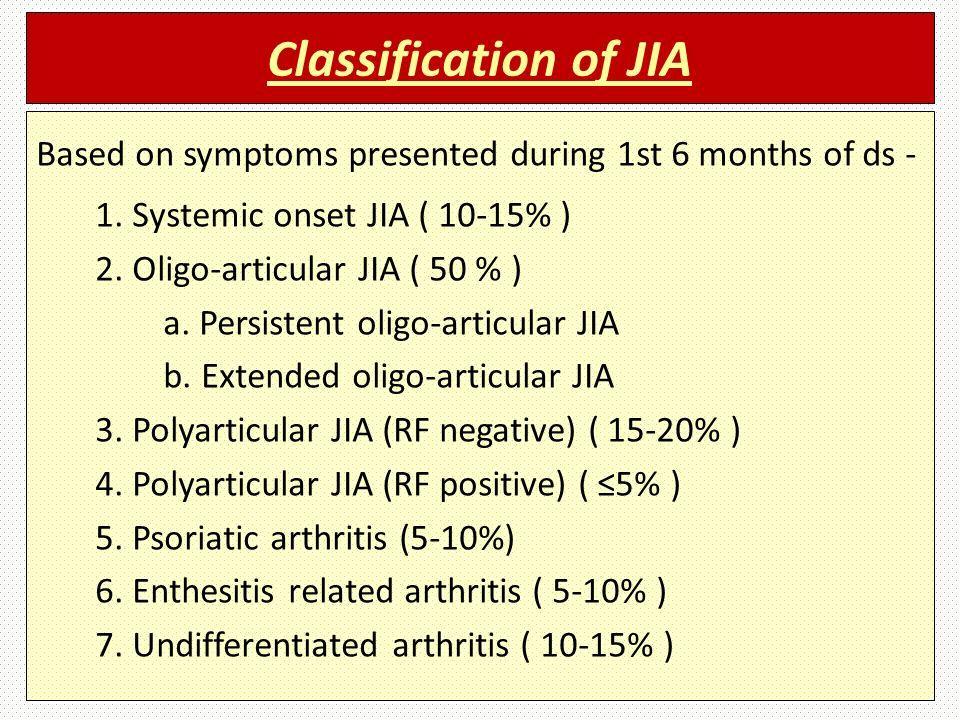
3 CLASSIFICATION
4 Principles of management Two major trends : Window of opportunity : literature suggests that treating inflammatory disease early and aggressively to switch off the immune process leads to better longterm. Treat to target : This concept has arisen in the era of biological agents, when treatment goals have become more ambitious and patient outcomes vastly improved.
5 Principles of management (cont ) The first treatment : Anti-inflammatory drugs : NSAIDs, Steroids Classical DMARDs : Methotrexate, Sulfasalazine, Hydroxycloroquin But : 30% patients reponse to NSAIDs. 50% patients nonresponse to Methotrexate (*) (*) Silverman E, Mouy R, Spiegel L et al. Leflunomide in juvenile rheumatoid arthritis (JRA) investigator group. Leflunomide or methotrexate for juvenile rheumatoid arthritis. N. Engl. J. Med. 352, (2005).

6 Side effects of Corticosteroids
7 Biologic therapies Biologic therapies : are treatments which utilise either monocloral antibodies or soluble cytokine receptors, to specifically target individual components of the immune system(*) Biologics should not be used unless a patient is intolerant to, or has failed optimised treatment with MTX; this is defined as 15mg/m2 given subcutaneously once-weekly for at least 3 months; higher doses have no evidence to suggest increased efficacy (**) (*) Ungar W, et al. Sem Arth Rheum 2013;42: The use of biologic response modifiers in polyarticular course juvenile idiopathic arthriits: a systematic review. (**)Dueckers G, Guellac N, Arbogast M, Dannecker G, Foeldvari I, Frosch M, et al. Evidence and consensus based treatment guidelines 2010 for juvenile idiopathic arthritis by the German Society of Paediatric Rheumatology. Klin Padiatr. 2011;223: doi: /s
8 History of biologic agents Biologic agents: bench to bedside medicine. Biologic agents are approved by FDA for treatment JIA Anti TNF-α : Etanercept (1999), Adalimumab (2008) Anti IL-1 : Anakinra Anti IL-6 : Tocilizumab (2011) Rituximab Abatacept
9 Comparison of treatment response, remission rate and drug adherence in polyarticular juvenile idiopathic arthritis patients treated with etanercept, adalimumab or tocilizumab Background : Treatment response, remission rates and compliance in patients with polyarticular juvenile idiopathic arthritis (polyjia) treated with adalimumab, etanercept, or tocilizumab were analyzed in clinical practice. Methods: Honeff et al, Arthritis & Therapy (2016) 18:272 Treatment response, remission rates and compliance in patients with polyarticular juvenile idiopathic arthritis (polyjia) treated with adalimumab, etanercept, or tocilizumab were analyzed in clinical practice. 236 patients started adalimumab, 419 etanercept and 74 tocilizumab, with differences in baseline patient characteristics 9
10 Improvement in patients using etanercept, adalimumab or tocilizumab according to the ACRpedi30 10
11 Improvement in patients following etanercept, adalimumab or tocilizumab treatment according to Juvenile Disease Activity Score 10 at baseline compared with the last observation 11
12 Rates of Juvenile Disease Activity Score (JADAS)10 remission and minimal disease activity in patients taking etanercept, adalimumab or tocilizumab 12
13 SAFE 13
14 Conclusions Adalimumab/etanercept/tocilizumab showed comparable efficacy toward polyjia. Tolerance was acceptable. 14
15 15
Overview of Paediatric Investigation Plan (PIP) in Paediatric Rheumatology
 in Paediatric Rheumatology") Overview of Paediatric Investigation Plan (PIP) in Paediatric Rheumatology Paediatric Rheumatology Expert Meeting, London 4 th December 29 Dr. Richard Veselý, Dr. Emma Sala Soriano Paediatric Investigation
Overview of Paediatric Investigation Plan (PIP) in Paediatric Rheumatology Paediatric Rheumatology Expert Meeting, London 4 th December 29 Dr. Richard Veselý, Dr. Emma Sala Soriano Paediatric Investigation
RHEUMATOID ARTHRITIS DRUGS
 Rheumatology Biologics Criteria from the Exceptional Access Program RHEUMATOID ARTHRITIS DRUGS DRUG NAME BRS REIMBURSED DOSAGE FORM/ STRENGTH Adalimumab Humira 40 mg/0.8 syringe and 40mg/0.8 pen for Anakinra
Rheumatology Biologics Criteria from the Exceptional Access Program RHEUMATOID ARTHRITIS DRUGS DRUG NAME BRS REIMBURSED DOSAGE FORM/ STRENGTH Adalimumab Humira 40 mg/0.8 syringe and 40mg/0.8 pen for Anakinra
ETANERCEPT Generic Brand HICL GCN Exception/Other ETANERCEPT ENBREL GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW)
") Generic Brand HICL GCN Exception/Other ETANERCEPT ENBREL 18830 GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Does the patient have a diagnosis of moderate to severe rheumatoid
Generic Brand HICL GCN Exception/Other ETANERCEPT ENBREL 18830 GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Does the patient have a diagnosis of moderate to severe rheumatoid
1 P a g e. Systemic Juvenile Idiopathic Arthritis (SJIA) (1.3) Patients 2 years of age and older with active systemic juvenile idiopathic arthritis.
 (1.3) Patients 2 years of age and older with active systemic juvenile idiopathic arthritis.") LENGTH OF AUTHORIZATION: Initial: 3 months for Crohn s or Ulcerative Colitis; 1 year for all other indications. Renewal: 1 year dependent upon medical records supporting response to therapy and review
LENGTH OF AUTHORIZATION: Initial: 3 months for Crohn s or Ulcerative Colitis; 1 year for all other indications. Renewal: 1 year dependent upon medical records supporting response to therapy and review
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: abatacept_orencia 4/2008 2/2018 2/2019 2/2018 Description of Procedure or Service Abatacept (Orencia ), a
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: abatacept_orencia 4/2008 2/2018 2/2019 2/2018 Description of Procedure or Service Abatacept (Orencia ), a
APPLICATION FOR SPECIAL AUTHORITY. Subsidy for Tocilizumab
 APPLICATION FOR SPECIAL AUTHORITY Fm SA1781 Subsidy f Tocilizumab Application Categy Page Cytokine release syndrome - Initial application... 2 Previous use - Initial application... 2 Rheumatoid Arthritis
APPLICATION FOR SPECIAL AUTHORITY Fm SA1781 Subsidy f Tocilizumab Application Categy Page Cytokine release syndrome - Initial application... 2 Previous use - Initial application... 2 Rheumatoid Arthritis
Orencia (abatacept) for Rheumatoid Arthritis. Media backgrounder
 for Rheumatoid Arthritis. Media backgrounder") Orencia (abatacept) for Rheumatoid Arthritis Media backgrounder What is Orencia (abatacept)? Orencia (abatacept) is the first biologic agent to be available in both an intravenous (IV) and a self-injectable,
Orencia (abatacept) for Rheumatoid Arthritis Media backgrounder What is Orencia (abatacept)? Orencia (abatacept) is the first biologic agent to be available in both an intravenous (IV) and a self-injectable,
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 9 Last Review Date: March 16, 2018 Simponi / Simponi
The Hospital for Sick Children Technology Assessment at SickKids (TASK)
") The Hospital for Sick Children Technology Assessment at SickKids (TASK) THE USE OF BIOLOGIC RESPONSE MODIFIERS IN POLYARTICULAR-COURSE JUVENILE IDIOPATHIC ARTHRITIS Report No. 2010-01 Date: January 11,
The Hospital for Sick Children Technology Assessment at SickKids (TASK) THE USE OF BIOLOGIC RESPONSE MODIFIERS IN POLYARTICULAR-COURSE JUVENILE IDIOPATHIC ARTHRITIS Report No. 2010-01 Date: January 11,
Erelzi (etanercept) Frequently Asked Questions
 Frequently Asked Questions") Erelzi (etanercept) Frequently Asked Questions 1. What is the funding status of Erelzi (etanercept)? Effective December 21, 2017, Erelzi (etanercept) will be added to the Ontario Drug Benefit (ODB) Formulary
Erelzi (etanercept) Frequently Asked Questions 1. What is the funding status of Erelzi (etanercept)? Effective December 21, 2017, Erelzi (etanercept) will be added to the Ontario Drug Benefit (ODB) Formulary
Regulatory Status FDA- approved indication: Simponi and Simponi ARIA are tumor necrosis factor (TNF) blockers indicated for the treatment of:
 blockers indicated for the treatment of:") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 8 Last Review Date: March 17, 2017 Simponi / Simponi
ADALIMUMAB Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW)
") Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Does the patient have a diagnosis of moderate to severe rheumatoid
Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Does the patient have a diagnosis of moderate to severe rheumatoid
Regulatory Status FDA-approved indication: Orencia is a selective T cell costimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 8 Last Review Date: March 16, 2018 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 8 Last Review Date: March 16, 2018 Orencia Description Orencia (abatacept)
Coverage Criteria: Express Scripts, Inc. monograph dated 12/15/ months or as otherwise noted by indication
 BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
BENEFIT DESCRIPTION AND LIMITATIONS OF COVERAGE ITEM: PRODUCT LINES: COVERED UNDER: DESCRIPTION: CPT/HCPCS Code: Company Supplying: Setting: Kineret (anakinra subcutaneous injection) Commercial HMO/PPO/CDHP
Abatacept (Orencia) for active rheumatoid arthritis. August 2009
 for active rheumatoid arthritis. August 2009") Abatacept (Orencia) for active rheumatoid arthritis August 2009 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Abatacept (Orencia) for active rheumatoid arthritis August 2009 This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES HUMIRA PEDIATRIC
 Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 HUMIRA PEDIATRIC GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the patient currently taking Humira? If
Generic Brand HICL GCN Exception/Other ADALIMUMAB HUMIRA 24800 HUMIRA PEDIATRIC GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the patient currently taking Humira? If
Effective Health Care Program
 Comparative Effectiveness Review Number 28 Effective Health Care Program Disease-Modifying Antirheumatic Drugs (DMARDs) in Children With Juvenile Idiopathic Arthritis (JIA) Executive Summary Background
Comparative Effectiveness Review Number 28 Effective Health Care Program Disease-Modifying Antirheumatic Drugs (DMARDs) in Children With Juvenile Idiopathic Arthritis (JIA) Executive Summary Background
Horizon Scanning Technology Summary. Adalimumab (Humira) for juvenile idiopathic arthritis. National Horizon Scanning Centre.
 for juvenile idiopathic arthritis. National Horizon Scanning Centre.") Horizon Scanning Technology Summary National Horizon Scanning Centre Adalimumab (Humira) for juvenile idiopathic arthritis June 2007 This technology summary is based on information available at the time
Horizon Scanning Technology Summary National Horizon Scanning Centre Adalimumab (Humira) for juvenile idiopathic arthritis June 2007 This technology summary is based on information available at the time
National Institute for Health and Clinical Excellence Level 1A, City Tower Piccadilly Plaza Manchester M1 4BD
 xxxxx xxxxxx xxxxxx xxxxxxx - xxxxxxxxx x National Institute for Health and Clinical Excellence Level 1A, City Tower Piccadilly Plaza Manchester M1 4BD Dear xxxxx, 1st September 2011 Comments on the August
xxxxx xxxxxx xxxxxx xxxxxxx - xxxxxxxxx x National Institute for Health and Clinical Excellence Level 1A, City Tower Piccadilly Plaza Manchester M1 4BD Dear xxxxx, 1st September 2011 Comments on the August
Juvenile idiopathic arthritis managed in the new millennium: one year outcomes of an inception cohort of Australian children
 Tiller et al. Pediatric Rheumatology (2018) 16:69 https://doi.org/10.1186/s12969-018-0288-z RESEARCH ARTICLE Open Access Juvenile idiopathic arthritis managed in the new millennium: one year outcomes of
Tiller et al. Pediatric Rheumatology (2018) 16:69 https://doi.org/10.1186/s12969-018-0288-z RESEARCH ARTICLE Open Access Juvenile idiopathic arthritis managed in the new millennium: one year outcomes of
ACTEMRA (tocilizumab)
") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 1. Active Polyarticular Juvenile Idiopathic Arthritis (PJIA) b. Patient has an intolerance or has experienced
Regulatory Status FDA-approved indication: Orencia is a selective T cell co-stimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Orencia Page: 1 of 9 Last Review Date: September 20, 2018 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Orencia Page: 1 of 9 Last Review Date: September 20, 2018 Orencia Description Orencia (abatacept)
Orencia (abatacept) DRUG.00040
 DRUG.00040") Market DC Orencia (abatacept) DRUG.00040 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Comments Quantity Limit Orencia (abatacept) - AGP, VA MCD only 4 vials per 28
Market DC Orencia (abatacept) DRUG.00040 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Comments Quantity Limit Orencia (abatacept) - AGP, VA MCD only 4 vials per 28
Clinical Policy: Etanercept (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid
 Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid") Clinical Policy: (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Enbrel ) is tumor necrosis
Clinical Policy: (Enbrel) Reference Number: PA.CP.PHAR.250 Effective Date: 01/18 Last Review Date: 08/17 Line of Business: Medicaid Coding Implications Revision Log Description (Enbrel ) is tumor necrosis
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 Program Number 2017 P 3041-8 Program Step Therapy Medications UnitedHealthcare Pharmacy Clinical Pharmacy Programs *Orencia (abatacept) *This step criteria refers to the subcutaneous formulation of abatacept
Program Number 2017 P 3041-8 Program Step Therapy Medications UnitedHealthcare Pharmacy Clinical Pharmacy Programs *Orencia (abatacept) *This step criteria refers to the subcutaneous formulation of abatacept
2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients
 2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients Dr Alberta Hoi Rheumatologist MBBS, FRACP, PhD NEW ERA IN MUSCULOSKELETAL MEDICINE New drugs - Biologics,
2017 PERIOPERATIVE MEDICINE SYMPOSIUM Peri-operative use of immunosuppression in rheumatology patients Dr Alberta Hoi Rheumatologist MBBS, FRACP, PhD NEW ERA IN MUSCULOSKELETAL MEDICINE New drugs - Biologics,
3. Has the patient shown improvement in signs and symptoms of the disease? Y N
 Pharmacy Prior Authorization MERC CARE (MEDICAID) Orencia (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax signed
Pharmacy Prior Authorization MERC CARE (MEDICAID) Orencia (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign and date. Fax signed
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Update on the Treatment of Rheumatoid Arthritis Sabrina Fallavollita MDCM McGill University Canadian Society of Internal Medicine
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Update on the Treatment of Rheumatoid Arthritis Sabrina Fallavollita MDCM McGill University Canadian Society of Internal Medicine
Rheumatology journal club October 20, 2017 Presented by: Matthew Stoll MD,PhD,PSCS
 Efficacy and safety of abatacept, a T-cell modulator, in a randomised, double-blind, placebo-controlled, phase III study in psoriatic arthritis (Mease et al., 2017) Rheumatology journal club October 20,
Efficacy and safety of abatacept, a T-cell modulator, in a randomised, double-blind, placebo-controlled, phase III study in psoriatic arthritis (Mease et al., 2017) Rheumatology journal club October 20,
Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65
 CG-DRUG-64, CG-DRUG-65") Market DC Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Cyltezo (adalimumab-adbm) 40 mg/0.8 ml prefilled syringe #* ^ Approval Duration 1 year
Market DC Cyltezo (adalimumab-adbm) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Cyltezo (adalimumab-adbm) 40 mg/0.8 ml prefilled syringe #* ^ Approval Duration 1 year
INFLIXIMAB Remicade (infliximab), Inflectra (infliximab-dyyb), Ixifi* (infliximabqbtx), Renflexis (infliximab-abda)
, Inflectra (infliximab-dyyb), Ixifi* (infliximabqbtx), Renflexis (infliximab-abda)") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 6 years of age or older 1. Moderate to severe Crohn s disease (CD) a. Patient has fistulizing disease
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following: 6 years of age or older 1. Moderate to severe Crohn s disease (CD) a. Patient has fistulizing disease
6 ADRs, 2 LOE. 2 ADRs, 4 LOE. Ineffectiveness 24 ADRs 7, 1 pt for convenience. 48% had antibodies against Infliximab at baseline
 Summary of Published Switch data Table 1. Information Patients Switch from (n) Reason for switch Switch to: (n) Results Numbers Presse Med. 2002 (1) 14 Infliximab (8) (6) 6 ADRs, 2 LOE 2 ADRs, 4 LOE (8)
Summary of Published Switch data Table 1. Information Patients Switch from (n) Reason for switch Switch to: (n) Results Numbers Presse Med. 2002 (1) 14 Infliximab (8) (6) 6 ADRs, 2 LOE 2 ADRs, 4 LOE (8)
Treatment of Rheumatoid Arthritis: The Past, the Present and the Future
 Treatment of Rheumatoid Arthritis: The Past, the Present and the Future Lai-Ling Winchow FCP(SA) Cert Rheum(SA) Chris Hani Baragwanath Academic Hospital University of the Witwatersrand Outline of presentation
Treatment of Rheumatoid Arthritis: The Past, the Present and the Future Lai-Ling Winchow FCP(SA) Cert Rheum(SA) Chris Hani Baragwanath Academic Hospital University of the Witwatersrand Outline of presentation
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 21 July 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 21 July 2010 Examination of the dossier of medicinal products included on the reimbursement list for a period of 5
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 21 July 2010 Examination of the dossier of medicinal products included on the reimbursement list for a period of 5
Horizon Scanning Technology Summary. Abatacept (Orencia) for juvenile idiopathic arthritis. National Horizon Scanning Centre.
 for juvenile idiopathic arthritis. National Horizon Scanning Centre.") Horizon Scanning Technology Summary National Horizon Scanning Centre Abatacept (Orencia) for juvenile idiopathic arthritis June 2007 This technology summary is based on information available at the time
Horizon Scanning Technology Summary National Horizon Scanning Centre Abatacept (Orencia) for juvenile idiopathic arthritis June 2007 This technology summary is based on information available at the time
2017 Blue Cross and Blue Shield of Louisiana
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Regulatory Status FDA-approved indication: Enbrel and Erelzi are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.27 Subject: Enbrel Page: 1 of 8 Last Review Date: March 16, 2018 Enbrel Description Enbrel (etanercept),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.27 Subject: Enbrel Page: 1 of 8 Last Review Date: March 16, 2018 Enbrel Description Enbrel (etanercept),
Infections and Biologics
 Overview Infections and Biologics James Galloway What is the risk of infection with biologics? Are some patients at greater risk? Are some drugs safer? Case scenario You recently commenced Judith, a 54
Overview Infections and Biologics James Galloway What is the risk of infection with biologics? Are some patients at greater risk? Are some drugs safer? Case scenario You recently commenced Judith, a 54
Technology Assessment Report commissioned by the NIHR HTA Programme on behalf of the National Institute for Health and Care Excellence.
 Technology Assessment Report commissioned by the NIHR HTA Programme on behalf of the National Institute for Health and Care Excellence December 2014 Protocol 1. Title of the project Abatacept, adalimumab,
Technology Assessment Report commissioned by the NIHR HTA Programme on behalf of the National Institute for Health and Care Excellence December 2014 Protocol 1. Title of the project Abatacept, adalimumab,
Rheumatoid Arthritis. Improving Outcomes in RA: Three Pillars. RA: Chronic Joint Destruction and Disability What We Try to Prevent
 Rheumatoid Arthritis Modern Management of Common Problems in Rheumatology: Rheumatoid Arthritis Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid
Rheumatoid Arthritis Modern Management of Common Problems in Rheumatology: Rheumatoid Arthritis Jonathan Graf, M.D. Associate Professor of Medicine, UCSF Division of Rheumatology, SFGH Director, UCSF Rheumatoid
Amjevita (adalimumab-atto)
") *- Florida Healthy Kids Amjevita (adalimumab-atto) Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2 #* ^ prefilled
*- Florida Healthy Kids Amjevita (adalimumab-atto) Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2 #* ^ prefilled
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC)
") DERBYSHIRE JOINT AREA PRERIBING COMMITTEE (JAPC) Derbyshire commissioning guidance on biologic drugs f the treatment of Rheumatoid arthritis with methotrexate This algithm is a tool to aid the implementation
DERBYSHIRE JOINT AREA PRERIBING COMMITTEE (JAPC) Derbyshire commissioning guidance on biologic drugs f the treatment of Rheumatoid arthritis with methotrexate This algithm is a tool to aid the implementation
C. Assess clinical response after the first three months of treatment.
 Government Health Plan (GHP) of Puerto Rico Authorization Criteria Tumor Necrosis Factor Alpha (TNFα) Adalimumab (Humira ) Managed by MCO Section I. Prior Authorization Criteria A. Physician must submit
Government Health Plan (GHP) of Puerto Rico Authorization Criteria Tumor Necrosis Factor Alpha (TNFα) Adalimumab (Humira ) Managed by MCO Section I. Prior Authorization Criteria A. Physician must submit
Perioperative Medicine:
 Perioperative Medicine: Management of rheumatologic agents Divya Gollapudi, MD May 2016 Medical Operative Consult Clinic Harborview Medical Center Your patient Ms. L is a 55 year-old F w/ h/o RA who presents
Perioperative Medicine: Management of rheumatologic agents Divya Gollapudi, MD May 2016 Medical Operative Consult Clinic Harborview Medical Center Your patient Ms. L is a 55 year-old F w/ h/o RA who presents
Actemra. Actemra (tocilizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.12 Subject: Actemra Page: 1 of 13 Last Review Date: September 20, 2018 Actemra Description Actemra
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.12 Subject: Actemra Page: 1 of 13 Last Review Date: September 20, 2018 Actemra Description Actemra
Clinical Policy: Tocilizumab (Actemra) Reference Number: CP.PHAR.263 Effective Date: Last Review Date: Line of Business: HIM, Medicaid
 Reference Number: CP.PHAR.263 Effective Date: Last Review Date: Line of Business: HIM, Medicaid") Clinical Policy: (Actemra) Reference Number: CP.PHAR.263 Effective Date: 07.01.16 Last Review Date: 11.18 Line of Business: HIM, Medicaid Coding Implications Revision Log See Important Reminder at the
Clinical Policy: (Actemra) Reference Number: CP.PHAR.263 Effective Date: 07.01.16 Last Review Date: 11.18 Line of Business: HIM, Medicaid Coding Implications Revision Log See Important Reminder at the
Regulatory Status FDA-approved indication: Enbrel is a tumor necrosis factor (TNF) blocker indicated for the treatment of:
 blocker indicated for the treatment of:") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Section: Prescription Drugs Effective Date: Oct 1, 2016 Subject: Enbrel Page: 1 of 7 Last Review Date:
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Section: Prescription Drugs Effective Date: Oct 1, 2016 Subject: Enbrel Page: 1 of 7 Last Review Date:
3. Is the prescribed dose within the Food and Drug Administration (FDA)- approved dosing for giant cell arteritis?
- approved dosing for giant cell arteritis?") Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Actemra (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH PESLVAIA & AETA BETTER HEALTH KIDS Actemra (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Clinical Policy: Tocilizumab (Actemra) Reference Number: ERX.SPMN.44
 Reference Number: ERX.SPMN.44") Clinical Policy: (Actemra) Reference Number: ERX.SPMN.44 Effective Date: 10/16 Last Review Date: 09/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: (Actemra) Reference Number: ERX.SPMN.44 Effective Date: 10/16 Last Review Date: 09/16 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases
 Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy
Drug Class Prior Authorization Criteria Therapeutic Agents in Rheumatic and Inflammatory Diseases Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy
2. Does the patient have a diagnosis of giant cell arteritis (GCA)? Y N
? Y N") Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Actemra (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Actemra (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information, sign
Regulatory Status FDA-approved indication: Enbrel and Erelzi are tumor necrosis factor (TNF) blockers indicated for the treatment of: (2-3)
 blockers indicated for the treatment of: (2-3)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.27 Subject: Enbrel Page: 1 of 10 Last Review Date: June 22, 2018 Enbrel Description Enbrel (etanercept),
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.27 Subject: Enbrel Page: 1 of 10 Last Review Date: June 22, 2018 Enbrel Description Enbrel (etanercept),
Rheumatoid arthritis 2010: Treatment and monitoring
 October 12, 2010 By Yusuf Yazici, MD [1] The significant changes in the way rheumatoid arthritis has been managed include earlier, more aggressive treatment with combination therapy. Significant changes
October 12, 2010 By Yusuf Yazici, MD [1] The significant changes in the way rheumatoid arthritis has been managed include earlier, more aggressive treatment with combination therapy. Significant changes
Rheumatoid arthritis
 Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Rheumatoid arthritis 1 Definition Rheumatoid arthritis is one of the most common inflammatory disorders affecting the population worldwide. It is a systemic inflammatory disease which affects not only
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: golimumab_simponi 8/2013 2/2018 2/2019 3/2018 Description of Procedure or Service Golimumab (Simponi and
Regulatory Status FDA-approved indication: Orencia is a selective T cell costimulation modulator indicated for: (1)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 6 Last Review Date: December 8, 2017 Orencia Description Orencia (abatacept)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.18 Subject: Orencia Page: 1 of 6 Last Review Date: December 8, 2017 Orencia Description Orencia (abatacept)
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Comparative Effectiveness Studies of Biologics Learning Objectives Understand the motivation for comparative effectiveness research
Annual Rheumatology & Therapeutics Review for Organizations & Societies Comparative Effectiveness Studies of Biologics Learning Objectives Understand the motivation for comparative effectiveness research
(minutes for web publishing)
") Rheumatology Subcommittee of the Pharmacology and Therapeutics Advisory Committee (PTAC) Meeting held on 17 October 2017 (minutes for web publishing) Rheumatology Subcommittee minutes are published in
Rheumatology Subcommittee of the Pharmacology and Therapeutics Advisory Committee (PTAC) Meeting held on 17 October 2017 (minutes for web publishing) Rheumatology Subcommittee minutes are published in
Efficacy and Safety of Tocilizumab in the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis
 New Evidence reports on presentations given at EULAR 2010 Efficacy and Safety of Tocilizumab in the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis Report on EULAR 2010 presentations
New Evidence reports on presentations given at EULAR 2010 Efficacy and Safety of Tocilizumab in the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis Report on EULAR 2010 presentations
Actemra (tocilizumab) CG-DRUG-81
 CG-DRUG-81") Market DC Actemra (tocilizumab) CG-DRUG-81 Override(s) Prior Authorization Approval Duration 1 year Medications Line of Business Quantity Limit Actemra (tocilizumab) vials VA MCD and All L-AGP May be subject
Market DC Actemra (tocilizumab) CG-DRUG-81 Override(s) Prior Authorization Approval Duration 1 year Medications Line of Business Quantity Limit Actemra (tocilizumab) vials VA MCD and All L-AGP May be subject
ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") UnitedHealthcare Community Plan Medical Benefit Drug Policy ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION Policy Number: CS2018D0039J Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
UnitedHealthcare Community Plan Medical Benefit Drug Policy ORENCIA (ABATACEPT) INJECTION FOR INTRAVENOUS INFUSION Policy Number: CS2018D0039J Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
New Evidence reports on presentations given at EULAR Tocilizumab for the Treatment of Rheumatoid Arthritis
 New Evidence reports on presentations given at EULAR 2012 Tocilizumab for the Treatment of Rheumatoid Arthritis Report on EULAR 2012 presentations Tocilizumab monotherapy is superior to adalimumab monotherapy
New Evidence reports on presentations given at EULAR 2012 Tocilizumab for the Treatment of Rheumatoid Arthritis Report on EULAR 2012 presentations Tocilizumab monotherapy is superior to adalimumab monotherapy
ORENCIA (abatacept) Demonstrates Comparable Efficacy to Humira ( adalimumab
 Demonstrates Comparable Efficacy to Humira ( adalimumab") ORENCIA (abatacept) Demonstrates Comparable Efficacy to Humira (adalimumab) in Patients with Moderate to Severe Rheumatoid Arthritis in First Head-to-Head Study of These Agents ORENCIA demonstrated comparable
ORENCIA (abatacept) Demonstrates Comparable Efficacy to Humira (adalimumab) in Patients with Moderate to Severe Rheumatoid Arthritis in First Head-to-Head Study of These Agents ORENCIA demonstrated comparable
New Evidence reports on presentations given at EULAR Tocilizumab for the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis
 New Evidence reports on presentations given at EULAR 2011 Tocilizumab for the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis Report on EULAR 2011 presentations Benefit of continuing
New Evidence reports on presentations given at EULAR 2011 Tocilizumab for the Treatment of Rheumatoid Arthritis and Juvenile Idiopathic Arthritis Report on EULAR 2011 presentations Benefit of continuing
ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Oxford Clinical Policy Policy Number: PHARMACY 284.9 T2 Effective Date: June 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Oxford Clinical Policy Policy Number: PHARMACY 284.9 T2 Effective Date: June 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION
 INJECTION FOR INTRAVENOUS INFUSION") ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2018D0043I Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
ACTEMRA (TOCILIZUMAB) INJECTION FOR INTRAVENOUS INFUSION UnitedHealthcare Commercial Medical Benefit Drug Policy Policy Number: 2018D0043I Effective Date: March 1, 2018 Table of Contents Page INSTRUCTIONS
Early synovitis clinics
 Early synovitis clinics Jeremy Jones MD FRACP FAFRM Consultant Rheumatologist, Llandudno General Hospital Honorary Research Fellow School of Sport, Health and Exercise Sciences Bangor University RA medication
Early synovitis clinics Jeremy Jones MD FRACP FAFRM Consultant Rheumatologist, Llandudno General Hospital Honorary Research Fellow School of Sport, Health and Exercise Sciences Bangor University RA medication
Drugs and Applicable Coding: J-code: Enbrel-J1438; Humira-J0135; Remicade-J1745; Inflectra-Q5102; Cimzia-J0718; Simponi-J1602 Renflexis - pending
 Policy Subject: Anti-TNF Agents Policy Number: SHS PBD16 Category: Rheumatology & Autoimmune Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS Individual
Policy Subject: Anti-TNF Agents Policy Number: SHS PBD16 Category: Rheumatology & Autoimmune Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS Individual
Immune Modulating Drugs Prior Authorization Request Form
 Patient: HPHC member ID #: Requesting provider: Phone: Servicing provider: Diagnosis: Contact for questions (name and phone #): Projected start and end date for requested Requesting provider NPI: Fax:
Patient: HPHC member ID #: Requesting provider: Phone: Servicing provider: Diagnosis: Contact for questions (name and phone #): Projected start and end date for requested Requesting provider NPI: Fax:
EXTENDED REPORT. Paediatric rheumatology
 To cite: Sengler C, Klotsche J, Niewerth M, et al. The majority of newly diagnosed patients with juvenile idiopathic arthritis reach an inactive disease state within the first year of specialised care:
To cite: Sengler C, Klotsche J, Niewerth M, et al. The majority of newly diagnosed patients with juvenile idiopathic arthritis reach an inactive disease state within the first year of specialised care:
2017 Blue Cross and Blue Shield of Louisiana
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Title: Predictive factors of relapse, in patients with JIA in remission, after discontinuation of synthetic disease-modifying antirheumatic drugs.
 Title: Predictive factors of relapse, in patients with JIA in remission, after discontinuation of synthetic disease-modifying antirheumatic drugs. Background Juvenile idiopathic arthritis (JIA) is not
Title: Predictive factors of relapse, in patients with JIA in remission, after discontinuation of synthetic disease-modifying antirheumatic drugs. Background Juvenile idiopathic arthritis (JIA) is not
Cimzia. Cimzia (certolizumab pegol) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Section: Prescription Drugs Effective Date: April 1, 2018 Subject: Cimzia Page: 1 of 5 Last Review
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.50.11 Section: Prescription Drugs Effective Date: April 1, 2018 Subject: Cimzia Page: 1 of 5 Last Review
Scottish Medicines Consortium
 Scottish Medicines Consortium abatacept, 250mg powder for concentrate for solution (Orencia ) No. (400/07) Bristol Myers Squibb Pharmaceuticals Ltd 10 August 2007 The Scottish Medicines Consortium has
Scottish Medicines Consortium abatacept, 250mg powder for concentrate for solution (Orencia ) No. (400/07) Bristol Myers Squibb Pharmaceuticals Ltd 10 August 2007 The Scottish Medicines Consortium has
Clinical Policy: Abatacept (Orencia) Reference Number: ERX.SPA.123 Effective Date:
 Reference Number: ERX.SPA.123 Effective Date:") Clinical Policy: (Orencia) Reference Number: ERX.SPA.123 Effective Date: 10.01.16 Last Review Date: 05.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Orencia) Reference Number: ERX.SPA.123 Effective Date: 10.01.16 Last Review Date: 05.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form Submit request via: Fax
 Website Form Submit request via: Fax") Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Enbrel (etanercept) require a prior
Prior Authorization Conditions for Approval of Enbrel (etanercept) Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 All requests for Enbrel (etanercept) require a prior
Dr Daniel Ching. Rheumatology Therapeutic Clinical Trials Centre Timaru
 Dr Daniel Ching Rheumatology Therapeutic Clinical Trials Centre Timaru Therapeutic Advances in Rheumatology GP CME Meeting, Dunedin, 18.08.2013 Dr Daniel Ching, MB FRCP FRACP Consultant Rheumatologist,
Dr Daniel Ching Rheumatology Therapeutic Clinical Trials Centre Timaru Therapeutic Advances in Rheumatology GP CME Meeting, Dunedin, 18.08.2013 Dr Daniel Ching, MB FRCP FRACP Consultant Rheumatologist,
Technology appraisal guidance Published: 16 December 2015 nice.org.uk/guidance/ta373
 Abatacept, adalimumab, etanercept and tocilizumab for treating juvenile idiopathic arthritis Technology appraisal guidance Published: 16 December 2015 nice.org.uk/guidance/ta373 NICE 2017. All rights reserved.
Abatacept, adalimumab, etanercept and tocilizumab for treating juvenile idiopathic arthritis Technology appraisal guidance Published: 16 December 2015 nice.org.uk/guidance/ta373 NICE 2017. All rights reserved.
Certolizumab pegol (Cimzia) for psoriatic arthritis second line
 for psoriatic arthritis second line") Certolizumab pegol (Cimzia) for psoriatic arthritis second line This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Certolizumab pegol (Cimzia) for psoriatic arthritis second line This technology summary is based on information available at the time of research and a limited literature search. It is not intended to
Center for Evidence-based Policy
 P&T Committee Brief Targeted Immune Modulators: Comparative Drug Class Review Alison Little, MD Center for Evidence-based Policy Oregon Health & Science University 3455 SW US Veterans Hospital Road, SN-4N
P&T Committee Brief Targeted Immune Modulators: Comparative Drug Class Review Alison Little, MD Center for Evidence-based Policy Oregon Health & Science University 3455 SW US Veterans Hospital Road, SN-4N
Proposal relating to the funding of TNF inhibitors (Humira and Enbrel) and gabapentin (Neurontin)
 and gabapentin (Neurontin)") 14 July 2015 Proposal relating to the funding of TNF inhibitors (Humira and Enbrel) and gabapentin (Neurontin) PHARMAC is seeking feedback on a proposal relating to the funding of the TNF-inhibitor medicines
14 July 2015 Proposal relating to the funding of TNF inhibitors (Humira and Enbrel) and gabapentin (Neurontin) PHARMAC is seeking feedback on a proposal relating to the funding of the TNF-inhibitor medicines
(tofacitinib) are met.
 are met.") Xeljanz (tofacitinib) Policy Number: 5.01. 560 Origination: 3/2014 Last Review: 3/2014 Next Review: 3/2015 Policy BCBSKC will provide coverage for Xeljanz (tofacitinib) when it is determined to be medically
Xeljanz (tofacitinib) Policy Number: 5.01. 560 Origination: 3/2014 Last Review: 3/2014 Next Review: 3/2015 Policy BCBSKC will provide coverage for Xeljanz (tofacitinib) when it is determined to be medically
University of Bristol - Explore Bristol Research. Peer reviewed version. Link to published version (if available): / X.
: / X.") Sen, E. S., & Ramanan, A. V. (2016). Biologic drugs in pediatric rheumatology. International Journal of Rheumatic Diseases, 19(6), 533-535. https://doi.org/10.1111/1756-185x.12924 Peer reviewed version
Sen, E. S., & Ramanan, A. V. (2016). Biologic drugs in pediatric rheumatology. International Journal of Rheumatic Diseases, 19(6), 533-535. https://doi.org/10.1111/1756-185x.12924 Peer reviewed version
First Name. Specialty: Fax. First Name DOB: Duration:
 Prescriber Information Last ame: First ame DEA/PI: Specialty: Phone - - Fax - - Member Information Last ame: First ame Member ID umber DOB: - - Medication Information: Drug ame and Strength: Diagnosis:
Prescriber Information Last ame: First ame DEA/PI: Specialty: Phone - - Fax - - Member Information Last ame: First ame Member ID umber DOB: - - Medication Information: Drug ame and Strength: Diagnosis:
Medication Policy Manual. Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013
 Medication Policy Manual Policy No: dru289 Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1,
Medication Policy Manual Policy No: dru289 Topic: Xeljanz, tofacitinib Date of Origin: January 21, 2013 Committee Approval Date: January 19, 2015 Next Review Date: January 2016 Effective Date: April 1,
Tuberculosis and Biologic Therapies: Risk and Prevention
 Tuberculosis and Biologic Therapies: Risk and Prevention Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health & Science
Tuberculosis and Biologic Therapies: Risk and Prevention Kevin L. Winthrop, MD, MPH Associate Professor, Divisions of Infectious Diseases, Public Health and Preventive Medicine Oregon Health & Science
Technology appraisal guidance Published: 14 December 2011 nice.org.uk/guidance/ta238
 Tocilizumab for the treatment of systemic juvenile idiopathic arthritis Technology appraisal guidance Published: 14 December 2011 nice.org.uk/guidance/ta238 NICE 2018. All rights reserved. Subject to Notice
Tocilizumab for the treatment of systemic juvenile idiopathic arthritis Technology appraisal guidance Published: 14 December 2011 nice.org.uk/guidance/ta238 NICE 2018. All rights reserved. Subject to Notice
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES
 Generic Brand HICL GCN Exception/Other GOLIMUMAB SIMPONI 22533, 22536, 34697, 35001 ROUTE = SUBCUTANE. GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the request for a
Generic Brand HICL GCN Exception/Other GOLIMUMAB SIMPONI 22533, 22536, 34697, 35001 ROUTE = SUBCUTANE. GUIDELINES FOR USE INITIAL CRITERIA (NOTE: FOR RENEWAL CRITERIA SEE BELOW) 1. Is the request for a
Although this presentation includes information regarding pharmaceuticals (including products under development), the information is not intended as
, the information is not intended as") Although this presentation includes information regarding pharmaceuticals (including products under development), the information is not intended as any advertisement and/or medical advice. Forward-Looking
Although this presentation includes information regarding pharmaceuticals (including products under development), the information is not intended as any advertisement and/or medical advice. Forward-Looking
RECOMMENDATIONS FOR THE USE OF BIOLOGICAL AGENTS FOR THE TREATMENT OF RHEUMATIC DISEASES*
 RECOMMENDATIONS FOR THE USE OF BIOLOGICAL AGENTS FOR THE TREATMENT OF RHEUMATIC DISEASES* * DISCLAIMER These recommendations are written to assist Australian rheumatologists prescribing biological agents
RECOMMENDATIONS FOR THE USE OF BIOLOGICAL AGENTS FOR THE TREATMENT OF RHEUMATIC DISEASES* * DISCLAIMER These recommendations are written to assist Australian rheumatologists prescribing biological agents
APPLICATION FOR SUBSIDY BY SPECIAL AUTHORITY
 APPLICANT (stamp sticker acceptable) Page 1 Fm SA1620 Etanercept INITIAL APPLICATION - juvenile idiopathic arthritis Applications only from a named specialist rheumatologist. Approvals valid f 6 months.
APPLICANT (stamp sticker acceptable) Page 1 Fm SA1620 Etanercept INITIAL APPLICATION - juvenile idiopathic arthritis Applications only from a named specialist rheumatologist. Approvals valid f 6 months.
1 Executive summary. Background
 1 Executive summary Background Rheumatoid Arthritis (RA) is the most common inflammatory polyarthropathy in the UK affecting between.5% and 1% of the population. The mainstay of RA treatment interventions
1 Executive summary Background Rheumatoid Arthritis (RA) is the most common inflammatory polyarthropathy in the UK affecting between.5% and 1% of the population. The mainstay of RA treatment interventions
Antirheumatic drugs. Rheumatic Arthritis (RA)
") Antirheumatic drugs Rheumatic Arthritis (RA) Disease Modifying Antirheumatic drugs (DMARDs) DMARDs are used in the treatment of rheumatic arthritis RA and have been shown to slow the course of the disease,
Antirheumatic drugs Rheumatic Arthritis (RA) Disease Modifying Antirheumatic drugs (DMARDs) DMARDs are used in the treatment of rheumatic arthritis RA and have been shown to slow the course of the disease,
Effective Health Care Program
 Comparative Effectiveness Review Number 55 Effective Health Care Program Drug Therapy for Rheumatoid Arthritis in Adults: An Update Executive Summary Background Rheumatoid arthritis (RA), which affects
Comparative Effectiveness Review Number 55 Effective Health Care Program Drug Therapy for Rheumatoid Arthritis in Adults: An Update Executive Summary Background Rheumatoid arthritis (RA), which affects
Proposed Retirement for HEDIS : Disease-Modifying Anti-Rheumatic Drug Therapy for Rheumatoid Arthritis (ART)
") Proposed Retirement for HEDIS 1 2020 2 : Disease-Modifying Anti-Rheumatic Drug Therapy for Rheumatoid Arthritis (ART) NCQA seeks public comment on the proposed retirement of the Disease-Modifying Anti-Rheumatic
Proposed Retirement for HEDIS 1 2020 2 : Disease-Modifying Anti-Rheumatic Drug Therapy for Rheumatoid Arthritis (ART) NCQA seeks public comment on the proposed retirement of the Disease-Modifying Anti-Rheumatic
Humira (adalimumab) DRUG.00002
 DRUG.00002") Humira (adalimumab) DRUG.00002 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Humira 10 mg/0.2 ml syringe Humira pediatric Crohn s Disease starter pack 40 mg/0.8 ml
Humira (adalimumab) DRUG.00002 Override(s) Prior Authorization Quantity Limit Approval Duration 1 year Medications Humira 10 mg/0.2 ml syringe Humira pediatric Crohn s Disease starter pack 40 mg/0.8 ml
Simponi / Simponi ARIA (golimumab)
") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 6 Last Review Date: September 15, 2016 Simponi / Simponi
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.51 Subject: Simponi / Simponi ARIA Page: 1 of 6 Last Review Date: September 15, 2016 Simponi / Simponi
Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65
 CG-DRUG-64, CG-DRUG-65") Market DC Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2
Market DC Amjevita (adalimumab-atto) CG-DRUG-64, CG-DRUG-65 Override(s) Prior Authorization Quantity Limit Medications Amjevita 20 mg/0.4 ml prefilled syringe Amjevita (adalimumab-atto) 40 mg/0.8 ml 2