Differential Diagnosis of Polyarthritis/Polyarthralgia
|
|
|
- Andrew Ferguson
- 5 years ago
- Views:
Transcription
1 Differential Diagnosis of Polyarthritis/Polyarthralgia Robert P. Friday, M.D., Ph.D. Newton-Wellesley Hospital Rheumatology Mass General Hospital Rheumatology
2 None. Disclosures
3 Polyarthritis Outline 1. DDx: includes primary arthritides and systemic disease History narrows the field Physical exam confirms suspicion Labs and X-rays can be misleading in the absence of a good history and exam. 2. Common arthritides a few key points. 3. Summary.
4 Rheumatology Consult for Joint Pain: Common Chief Complaints Doc, my body is full of arthritis. My bones hurt! My joints hurt, but my arthritis test was negative. I have pain all over and tested positive for lupus. I don t know why I m here.
5 Joints (or not ) Osteoarthritis Erosive Osteoarthritis Rheumatoid arthritis Gout CPPD arthropathy Psoriatic arthritis Ankylosing spondylitis Reactive arthritis Palindromic rheumatism Undifferentiated polyarthritis Polymyalgia rheumatica Fibromyalgia Poly-bursitis Peripheral neuropathy Joints PLUS SLE Sjögren s syndrome Systemic sclerosis Inflammatory myopathy Adult-onset Still s disease Sarcoidosis Relapsing polychondritis Behçet s disease Systemic vasculitis Parvovirus B19 infection Hepatitis C > B Acute rheumatic fever Early Lyme disease Chikungunya virus Zika virus
6 A more basic view of the DDx for polyarticular pain 1. Osteoarthritis 2. Inflammatory arthritis (has its own DDx) 3. Arthralgia (pain without joint abnormality) 4. Bursitis or Tendinitis 5. Myofascial pain / Fibromyalgia When it is early in the course of symptoms, differentiating among these causes is often difficult for anyone. Embrace the challenge!
7 Diagnostic Evaluation of Joint Pain 1. A thorough HISTORY and EXAM are critical for differentiating causes of joint pain. Is pain localized to joints vs. more diffuse MSK pain? Radiographs may yield specific diagnostic clues. Lab tests support the clinical impression and may provide prognostic information. 2. Joint pain is like any other clinical problem. Just like a heart murmur, the significance of joint pain is determined by the company it keeps. Interpret a joint exam just like an EKG pattern recognition may point you to the diagnosis.
8 Normal Joint Homunculus
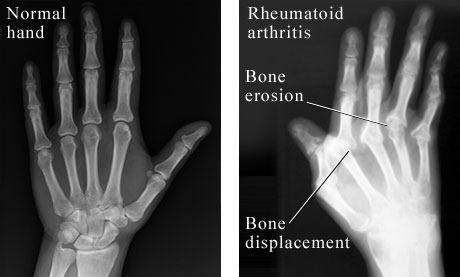
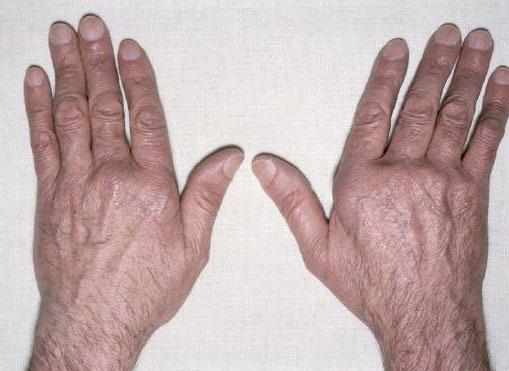
9 Rheumatoid Arthritis
10 Case 1 Slam dunk 18yF w/ 1 year of joint pain, previously healthy. Progressively: hands (MCPs and PIPs), elbows, shoulders, ankles, feet, jaw. Knees swollen more recently. Pain 8-9/10, with naproxen 5-6/10. In college, going to the gym regularly. +Fatigued. AM stiffness lasts 4 hours. Can t walk up stairs easily. No rashes, no fevers, no weight loss, no alopecia. Saw PCP (after a year), ESR 11 25, CRP 11.7 mg/l, RF positive (x2), ANA neg, TSH normal, vit D low (17 ng/ml). Tearful in office swollen joints = 34, tender joints = 36 MEDS: naproxen, vitamin D. LABS: ESR 70, CRP 65 mg/l, RF 565, CCP 261, ANA 1:40.
11 Osteoarthritis

12 RA, PsA, SLE, other CTD, CPPD, Gout
13 Historical Clues Duration - when did it start? Location - which joints? (if joints at all ) Character - pain, swelling, stiffness? Onset - acute or insidious? Timing - AM? eve? night? w/rest or activity? Treatment - what have you tried? Other - symptoms of systemic disease? Fam Hx - Gout, OA, RA, psoriasis or PsA.
14 Duration of Polyarticular Complaints Acute (days) Typically inflammatory Infectious Viral Bacterial (usu. monoarth) Early Lyme disease Crystal-induced Often have est. diagnosis of Gout or CPPD Reactive arthritis Early chronic cause Chronic (wks to yrs) Is it inflammatory or not? Rheumatoid Psoriatic Crystal Connective tissue dz Vasculitis Myositis Adult Still s disease Osteoarthritis Fibromyalgia
15 Inflammatory vs. Non-inflammatory Features of Joint Pain Inflammatory Non-inflammatory Pain ++ / / ++ Stiffness ++ / / ++ Swelling / - Nighttime Pain Morning stiffness ++ + / - > 60 min < 30 min
16 Useful questions to ask Morning Stiffness: How long until you feel the best you are going to feel for the day? Stiffness has various meanings for patients. Activity Limitations / Disruptions: Do you have difficulty with ADLs? (offer examples) Any pleasurable activities you can no longer do? How well do you sleep? Does pain wake you?
17 Physical Exam Look for signs of CTD, psoriasis, vasculitis: Skin rash Sun exposed (SLE, Dermatomyositis, other CTD) Extensor surfaces, umbilicus, gluteal cleft, scalp (Psoriasis) Palpable purpura (Vasculitis) Skin thickening or morphea (Systemic sclerosis) Hair loss thinning, patchy alopecia (SLE) Nails pitting/onycholysis (Psoriasis), abnormal nailfold capillaries (CTD) HEENT dry eye and dry mouth (Sjogren s) oral ulcers/lesions (SLE, Behçet s) ocular inflammation (Spondyloarthritis, RA, Behçet s) abnormal temporal arteries (GCA/PMR) nasal crusts or blood; nose or ear cartilage inflammation (ANCA vasculitis, Relapsing polychondritis)

18 Photodistribution of SLE Rashes

19 Distribution of Psoriasis

20 Palpable purpura

21 DIP-limited Psoriatic Arthiritis
22 Physical Exam Joint exam synovitis (soft tissue swelling +/- effusion) is the hallmark of inflammatory arthritis: Inspection, Palpation, ROM, Strength, DTRs. Erythema, warmth, tender, effusion EASIER to detect Soft tissue swelling (may be subtle) HARDER to detect Neuro exam goes along with MSK exam. If only one or a few joints hurt, examine every joint.
23 Articular (Joint) Disease Periarticular/Soft Tissue Joint Exam Elements OA Inflammatory Arthralgia Bursitis or Tendinitis Myofascial Inspection Swelling varies yes no yes no Erythema no varies no yes no Palpation Warmth no yes no yes no Tenderness along joint line varies varies periarticular yes Movement ROM limited limited full or limited full, pain often limits full Pain w/active or passive both both usually both active > passive usually both
24 Some Non-inflammatory / Non-arthritic causes of musculoskeletal pain Thyroid disease Fibromyalgia syndrome Medications (temporally associated with use) Cholesterol-lowering agents; SERMs & aromatase inhibitors; antithyroid drugs (methimazole, PTU) Primary sleep disorders Obstructive sleep apnea Restless legs syndrome Joint hypermobility / hyperextensibility Ehlers-Danlos syndrome Malignancy
25 Laboratory Testing Diagnostically Helpful: Creatinine and liver enzymes assess for renal and hepatic dysfunction as signs of systemic illness; baseline for therapy. CBC anemia due to chronic inflammation, cytopenias in SLE/CTD, heme malignancy(rare). Urinalysis Renal disease is often asymptomatic in SLE and vasculitis. ESR and CRP non-specific, often helpful, but often normal in patients with active inflammatory disease. NOTE: a high normal CRP of 7-8 mg/l may be elevated for a given patient.
26 Laboratory Testing Not usually helpful diagnostically: Uric Acid this is not a diagnostic test for gouty arthritis. Hyperuricemia is a risk factor for gout, so when gout is a possible cause of joint pain it is appropriate to assess the level (i.e., typically NOT in a 30yo woman!). Lyme serology only helpful if early Lyme disease is suspected to be the cause of polyarthralgia. Lyme arthritis is NOT polyarticular it is a late manifestation of infection with B. burgdorferi presenting with inflammatory monoarticular (or oligoarticular) joint disease.
27 Serological Testing Serologies support the clinical impression they are not diagnostic as isolated positive test results. Anti-CCP Ab (CCP = cyclic citrullinated peptide) Highly specific for RA (low titers seen in other dz), a/w extra-articular manifestations and high risk for joint damage. Rheumatoid factor (RF) A reliable marker of RA only in a patient with polyarticular synovitis, otherwise it is non-specific. Anti-nuclear antibody (ANA) Not specific for SLE positive in other CTDs, RA, autoimmune liver and thyroid disease, healthy individuals.
28 Additional Testing HLA-B27 only helpful if suspecting axial spondyloarthritis, which is not typically polyarticular (usually inflammatory back pain +/- mono- or oligoarticular peripheral arthritis). Calcium axis evaluation if CPPD arthropathy confirmed or suspected, assess Ca, Mg, Phos, PTH and 25-OHD. Additional studies to assess for hemochromatosis may also be appropriate if otherwise suspected clinically. Serum Ferritin if considering Adult Onset Still s Disease or CPPD arthropathy related to hemochromatosis.
29 Case 2 Not So Crystal Clear 65yM w/ CAD s/p stenting 4 years ago p/w bilateral shoulder pain and stiffness and bilateral knee pain and swelling x3 weeks. Feels his symptoms are muscle and joint related. Cramping sensation behind both knees. Difficulty getting up from low seats (e.g., toilet). Nocturnal pain, hard to sleep, AM stiffness lasts hours. Advil 400mg 5x/day and Aleve 440mg BID only slight relief. Stopped rosuvastatin for 3 days, no improvement in symptoms. Avid golfer, no tick bites but worried about Lyme. No FH of arthritis or autoimmune disease. ROS: No rash, headache, eye/vision symptoms, jaw claudication, fever, chills, sweats, unexplained weight loss.
30 Case 2 (continued) MEDS: ASA, lisinopril, rosuvastatin, metoprolol, clopidogrel. EXAM: Looks well, discomfort when moving (shoulders and knees). No ocular inflammation. No lymphadenopathy. Lungs clear. Heart regular, no murmur. No peripheral edema. No rash. No neuro deficits, but strength exam limited by pain. Unable to abduct right shoulder beyond 90 degrees, pain on the left with better ROM. Bilateral knee effusions L > R, with warmth, tenderness and pain upon flexion. Hip ROM is stiff with only mild discomfort. No abnormalities of hands, wrists, ankles or feet. LABS: Mild anemia, CMP normal. ESR 54, CRP 91 mg/l, ANA negative, RF negative, anti-ccp negative, uric acid 5.4 mg/dl, CPK 35, parvovirus negative, Lyme negative.
31 Case 2 (continued) IMAGING: None obtained. PROCEDURE: Bilateral knee arthrocentesis 10mL from L knee and 35mL from R knee, yellow fluid with moderate turbidity. Both joints injected with depomedrol. Fluid WBC counts: L knee = 4084, R knee = Crystal analysis: L knee = no crystals, R knee = +CPPD crystals inside WBCs. DDx: Rx: Polymyalgia rheumatica (no sx of temporal arteritis) Rheumatoid arthritis, seronegative Polyarticular CPPD arthropathy ( pseudogout ) Other inflammatory arthritis Prednisone 15mg daily (cures all ills at least initially!)
32 Radiographs (usually normal at first) RA = soft tissue swelling, periarticular osteopenia, joint space narrowing, marginal erosions. OA = osteophytes, narrowing, central erosion, subchondral sclerosis and subchondral cysts. Gout = calcified tophi, overhanging edges ( rat bite erosions). CPPD = chondrocalcinosis (wrist, knee, hips/pelvis). PsA = periostitis, erosion, narrowing, fusion, pencil-in-cup deformity. SLE = non-erosive, reducible ulnar deviation. SSc = calcinosis (in soft tissue), distal tuft resorption.
33 Osteoarthritis Epidemiology Rare <35yo, incidence and prevalence increase with age (>80% of population >55yo in some form). Numerous risk factors, both environmental and genetic. Diagnostic considerations Joints most affected: hand IP joints, feet, knees, hips, spine. Distinguishing between Inflammatory vs. Non-inflammatory OA may affect therapy. May be associated with CPPD crystal deposition (with evident chondrocalcinosis on radiographs). Typical radiographic changes develop over years.


34 Osteoarthritis (and osteopenia)


35 Erosive osteoarthritis



36 CPPD Arthropathy
37 Rheumatoid Arthritis Epidemiology 1% of Caucasian population, up to 5% of women >65yo. Women affected 2-3x > Men. Occurs at any age, peak incidence 50-75yo. Genetics and smoking identified as risk factors. Diagnostic considerations Constitutional symptoms: fatigue, weight loss, occ. fever. Numerous extra-articular organs can be involved (40% of pts over lifetime): skin, bone, muscle, eye, heart, lung, CNS, PNS. Recent guidelines devised to promote EARLY diagnosis. Radiographs normal in early disease, and we like to keep them that way! RA and fibromyalgia are often co-morbid, sometimes leading to diagnostic confusion or a delay in the diagnosis of seronegative RA.
38


39 Rheumatoid arthritis (early)
40 Case 3 A Cautionary Tale 68yoM with alcohol use disorder (sober 2 years), h/o Lyme arthritis (knee), polyarticular synovitis with effusions and bursitis. Labs: ESR 54 mm/hr CRP 68.9 mg/l HCT 34.5 % Plts 633,000 RF 537 Anti-CCP 237


41 This is NOT Lyme arthritis!!!

42 2/2010

43 9/2014
44 2/2010 9/2014
 -")
45 Epidemiology Male:Female equally affected Age of onset 30s and 40s Psoriasis - up to 30% have arthritis 20-40% involves spine or SI joints Arthritis may precede skin disease Psoriatic Arthritis Extra-articular Features Psoriatic skin lesions - typically thick scale on erythematous base, but some variability Fingernails: pitting, onycholysis, transverse depressions Eye inflammation (30%) - conjunctivitis, iritis Dactylitis, tendinitis 5 subtypes: Spondyloarthritis, Mono/oligoarthritis, Polyarthritis, DIP-limited arthritis, Arthritis mutilans.


46 Dactylitis sausage digits Psoriatic Arthiritis, Mutilans type



47 Psoriatic arthritis AND Osteoarthritis
48 SLE Arthropathy Joint pain and fatigue are the most common presenting symptoms of SLE. Up to 95% of SLE patients have arthritis. Symmetrical, polyarticular usu. involves knees, wrists, PIP joints. Non-erosive, migratory, may resolve in a given joint in <24h. Lax joint capsules, tendons, ligaments = reducible deformity. Often pain >> physical findings.
49 Lupus arthropathy


50 Diffuse osteopenia. Joint space loss in wrists. Ulnar deviation. Thumb IP joints subluxed. NO joint erosions.
51 Case 75yF with recent onset of headache, proximal MSK aching (neck/shoulders > hips), decline in vision and elevated inflammatory markers. 2mo proximal pains ("all her bones hurt"), assoc with: temporal headaches and scalp tenderness. decline in vision starting after 3 weeks of symptoms. appetite off, has lost ~15-20 lbs. Feels "numbness" along the left side of her face and jaw, as well as a feeling of swelling in this area and over the forehead. Notes from recent EW visit, "She describes her jaw pain as "an electric shock" which is worse with chewing. ESR 91 and CRP 126 mg/l. ANA, RF, anti-ccp negative. ANY THOUGHTS ON A DIAGNOSIS?
52 Case (cont d) Started on prednisone 80mg daily (worrisome story). Temporal artery biopsy (performed 3 days later). Ophthalmology evaluation. RESULTS: TA biopsy = negative for arteritis. Eye exam = cataracts. Feels much better on prednisone. Tapered dose to 20mg/day since TA biopsy negative.
53 Case (cont d) 1 month later: Proximal aching has recurred on 20mg/day, just as severe. Vision stable, some headaches, not as bad. She reports increasing her prednisone to 80mg/day (on her own) to control symptoms, now at 40mg/day, a little better. ESR 83 and CRP 125 mg/l. NOW WHAT?!? Advised to continue prednisone 40mg/day? Biopsy neg GCA Time to think Presents to EW the following week with temp 103, left sided neck swelling and pain. CT with 1.3cm hypodensity in the left neck with surrounding inflammation.? Abscess,? Lymph node.

54 Lymphoma, not PMR/GCA
55 Key Points 1. History and physical examination are critical to identifying the etiology of joint complaints. 2. Distinguish inflammatory from non-inflammatory joint pain. 3. Non-articular symptoms suggest systemic inflammatory disease. 4. Inflammatory joint disease can cause rapid damage, so early diagnosis and treatment are critical. Next Best Steps Focus on dissecting the history of patients with joint complaints to improve diagnostic acumen. Pursue rational testing (lab studies and imaging) in the evaluation of joint pain rather than a screening or shotgun approach.
Differential Diagnosis of Polyarthritis/Polyarthralgia
 Differential Diagnosis of Polyarthritis/Polyarthralgia Robert P. Friday, M.D., Ph.D. Newton-Wellesley Hospital Rheumatology Mass General Hospital Rheumatology None. Disclosures Polyarthritis Outline 1.
Differential Diagnosis of Polyarthritis/Polyarthralgia Robert P. Friday, M.D., Ph.D. Newton-Wellesley Hospital Rheumatology Mass General Hospital Rheumatology None. Disclosures Polyarthritis Outline 1.
Objectives. Joint Pain. Case 1. Rheumatology for the Primary MD (Not just your grandmother s disease) 12/4/2010
 12/4/2010") Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
Objectives Rheumatology for the Primary MD (Not just your grandmother s disease) Identify when it is appropriate to refer for rheumatologic evaluation Autoimmune/ Inflammatory v. noninflammatory disease
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
Mary Derlacki, FNP. No financial relationships to disclose. Office Rheumatology for the Nurse Practitioner. Rheumatoid Arthritis
 Office Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Drs. Cassell and Boren Eugene, OR 541-687-0816 mderlacki@comcast.net No financial relationships to disclose Rheumatoid Arthritis 1% of
Office Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Drs. Cassell and Boren Eugene, OR 541-687-0816 mderlacki@comcast.net No financial relationships to disclose Rheumatoid Arthritis 1% of
RHEUMATOLOGY OVERVIEW. Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center
 RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
RHEUMATOLOGY OVERVIEW Carmelita J. Colbert, MD Assistant Professor of Medicine Division of Rheumatology Loyola University Medical Center What is Rheumatology? Medical science devoted to the rheumatic diseases
Patient #1. Rheumatoid Arthritis. Rheumatoid Arthritis. 45 y/o female Morning stiffness in her joints >1 hour
 Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
Patient #1 Rheumatoid Arthritis Essentials For The Family Medicine Physician 45 y/o female Morning stiffness in her joints >1 hour Hands, Wrists, Knees, Ankles, Feet Polyarticular, symmetrical swelling
When is it Rheumatoid Arthritis When to Refer
 When is it Rheumatoid Arthritis When to Refer Nancy A. Brown, DO Spring 2015 When is it Rheumatoid Arthritis When to Refer Learning objectives To review the definition and epidemiology of Rheumatoid Arthritis
When is it Rheumatoid Arthritis When to Refer Nancy A. Brown, DO Spring 2015 When is it Rheumatoid Arthritis When to Refer Learning objectives To review the definition and epidemiology of Rheumatoid Arthritis
Jeopardy. What s the rash? $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400
 Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Jeopardy Antibodies & more antibodies Aching joints What s the rash? Potpourri Image Challenge $100 $100 $100 $100 $100 $200 $200 $200 $200 $200 $300 $300 $300 $300 $300 $400 $400 $400 $400 $400 $500 $500
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis
 Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
How do polyarthritis, polyarthralgias, and diffuse aches and pains differ?
 Approach to the patient with polyarthritis How do polyarthritis, polyarthralgias, and diffuse aches and pains differ? Polyarthritis is definite inflammation (swelling, tenderness, warmth) of more than
Approach to the patient with polyarthritis How do polyarthritis, polyarthralgias, and diffuse aches and pains differ? Polyarthritis is definite inflammation (swelling, tenderness, warmth) of more than
A CRP B FBC C LFT D blood culture E uric acid
 1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
1 A 39 year old lady with rheumatoid arthritis is admitted to hospital with a hot, swollen and painful right knee. Which is the most important blood test? A CRP B FBC C LFT D blood culture E uric acid
Juvenile Idiopathic Arthritis (JIA)
") Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
Juvenile Idiopathic Arthritis (JIA) Kaveh Ardalan, MD, MS Division of Rheumatology Ann & Robert H. Lurie Children s Hospital of Chicago Assistant Professor, Pediatrics and Medical Social Sciences Northwestern
Articular disease of the hand - the target joint approach
 Articular disease of the hand - the target joint approach Poster No.: C-1817 Congress: ECR 2016 Type: Educational Exhibit Authors: R. R. Domingues Madaleno 1, A. P. Pissarra 1, I. Abreu 2, A. Canelas 1,
Articular disease of the hand - the target joint approach Poster No.: C-1817 Congress: ECR 2016 Type: Educational Exhibit Authors: R. R. Domingues Madaleno 1, A. P. Pissarra 1, I. Abreu 2, A. Canelas 1,
Rheumatoid Arthritis. Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011
 Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
Rheumatoid Arthritis Marge Beckman FALU, FLMI Vice President RGA Underwriting Quarterly Underwriting Meeting March 24, 2011 The security of experience. The power of innovation. www.rgare.com Case Study
2/23/18. Disclosures. Rheumatic Diseases of Childhood. Making Room for Rheumatology. I have nothing to disclose. James J.
 Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
Making Room for Rheumatology James J. Nocton, MD Disclosures I have nothing to disclose Rheumatic Diseases of Childhood Juvenile Idiopathic Arthritis (JIA) Systemic Lupus Erythematosus (SLE) Juvenile Dermatomyositis
First Presentation of Joint Pain
 First Presentation of Joint Pain Andrew Harrison Rheumatologist Wellington Regional Rheumatology Unit, HVDHB Bowen Centre, Crofton Downs, Wellington Assoc. Prof. in Medicine, University of Otago Wellington
First Presentation of Joint Pain Andrew Harrison Rheumatologist Wellington Regional Rheumatology Unit, HVDHB Bowen Centre, Crofton Downs, Wellington Assoc. Prof. in Medicine, University of Otago Wellington
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care. Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018
 Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018 No Disclosures Objectives Recognize early signs of RA/PsA what to
Rheumatoid arthritis and Psoriatic arthritis: a guide for Primary Care Nina Flavin, MD Rheumatology Confluence Health April 13 th, 2018 No Disclosures Objectives Recognize early signs of RA/PsA what to
Department of Paediatrics Clinical Guideline
 Department of Paediatrics Clinical Guideline The child and young person with possible arthritis (joint swelling and/or pain, loss of function for >4 weeks) Definition: Juvenile Idiopathic Arthritis (JIA)
Department of Paediatrics Clinical Guideline The child and young person with possible arthritis (joint swelling and/or pain, loss of function for >4 weeks) Definition: Juvenile Idiopathic Arthritis (JIA)
Rheumatology for the Nurse Practitioner. Mary Derlacki, FNP Eugene Rheumatology
 Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Eugene Rheumatology Financial Relationships Amgen Genentech AbbVie IS THIS LUPUS? S.T. is a 45 y/o woman with 9 months of joint pain, fatigue,
Rheumatology for the Nurse Practitioner Mary Derlacki, FNP Eugene Rheumatology Financial Relationships Amgen Genentech AbbVie IS THIS LUPUS? S.T. is a 45 y/o woman with 9 months of joint pain, fatigue,
Juvenile Chronic Arthritis
 Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK) Childhood Arthritis JCA/JIA/JRA Remember Acute rheumatic
Juvenile Chronic Arthritis Dr. Christa Visser MBChB MMed (Med Phys) Diploma Musculoskeletal Medicine (UK), Member Society of Orthopaedic Medicine (UK) Childhood Arthritis JCA/JIA/JRA Remember Acute rheumatic
Bones? Did someone say bones? 12/31/2012. W.R Reinus, MD MBA FACR
 William R. Reinus, MD MBA FACR Temple University Medical Center Aug 2012 (55) 1 Bones? Did someone say bones? 2 ABC S OF ARTHRITIS Arthritis: By definition, any disease that is jointcentered: Both sides
William R. Reinus, MD MBA FACR Temple University Medical Center Aug 2012 (55) 1 Bones? Did someone say bones? 2 ABC S OF ARTHRITIS Arthritis: By definition, any disease that is jointcentered: Both sides
What organ system is involved? What is the pathology? What is the possible etiology?
 Johan van Rensburg What organ system is involved? What is the pathology? What is the possible etiology? Genetic Environmental What are the possible complications? How is the patient s functioning impaired?
Johan van Rensburg What organ system is involved? What is the pathology? What is the possible etiology? Genetic Environmental What are the possible complications? How is the patient s functioning impaired?
Department of Paediatrics Clinical Guideline. Guideline for the child with possible arthritis (joint swelling/pain, loss of function)
") Department of Paediatrics Clinical Guideline Guideline for the child with possible arthritis (joint swelling/pain, loss of function) Definition: Juvenile Idiopathic Arthritis (JIA) is defined as arthritis
Department of Paediatrics Clinical Guideline Guideline for the child with possible arthritis (joint swelling/pain, loss of function) Definition: Juvenile Idiopathic Arthritis (JIA) is defined as arthritis
Mr. OA: Case Presentation
 CLINICAL CASES Case 1: Mr. OA OA Mr. OA: Case Presentation 62-year-old lawyer Mild left knee pain for 3 month, but became worse 1 week ago No swelling 1 week earlier: 2-hour walk in the countryside 2 days
CLINICAL CASES Case 1: Mr. OA OA Mr. OA: Case Presentation 62-year-old lawyer Mild left knee pain for 3 month, but became worse 1 week ago No swelling 1 week earlier: 2-hour walk in the countryside 2 days
CME for Family Medicine Specialists. Evelyn Sutton, MD, FRCPC, FACP November 17, 2018
 CME for Family Medicine Specialists Evelyn Sutton, MD, FRCPC, FACP November 17, 2018 Disclosures Received $ from Advisory Board Consultant: Amgen, Abvie, Pfizer, Actelion, Lilly, Grants: Arthritis Society,
CME for Family Medicine Specialists Evelyn Sutton, MD, FRCPC, FACP November 17, 2018 Disclosures Received $ from Advisory Board Consultant: Amgen, Abvie, Pfizer, Actelion, Lilly, Grants: Arthritis Society,
EARLY INFLAMMATORY ARTHRITIS. Cristina Tacu Consultant Rheumatologist Brighton and Sussex University Hospital
 EARLY INFLAMMATORY ARTHRITIS Cristina Tacu Consultant Rheumatologist Brighton and Sussex University Hospital EIA: Introduction National priority Preventable cause of disability Very common condition High
EARLY INFLAMMATORY ARTHRITIS Cristina Tacu Consultant Rheumatologist Brighton and Sussex University Hospital EIA: Introduction National priority Preventable cause of disability Very common condition High
Rheumatology Review Update in Internal Medicine COPYRIGHT. Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center.
 Rheumatology Review Update in Internal Medicine Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston MA Case #1 True statement(s) regarding etanercept and leflunomide, for the treatment
Rheumatology Review Update in Internal Medicine Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston MA Case #1 True statement(s) regarding etanercept and leflunomide, for the treatment
Rheumatologic Emergencies It s not just swollen joints. Joanne Homik Rheumatologist University of Alberta
 Rheumatologic Emergencies It s not just swollen joints Joanne Homik Rheumatologist University of Alberta Or is it? Disclosures No relevant conflicts of interest regarding the content of this presentation
Rheumatologic Emergencies It s not just swollen joints Joanne Homik Rheumatologist University of Alberta Or is it? Disclosures No relevant conflicts of interest regarding the content of this presentation
REFERRAL GUIDELINES: RHEUMATOLOGY
 Outpatient Page 1 1 REFERRAL GUIDELINES: RHEUMATOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential Referral Content Referring
Outpatient Page 1 1 REFERRAL GUIDELINES: RHEUMATOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential Referral Content Referring
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition
 Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
Kelley's Textbook of Rheumatology. 2 Volume Set. Text with Internet Access Code for Premium Consult Edition Firestein, G ISBN-13: 9781437717389 Table of Contents VOLUME I STRUCTURE AND FUNCTION OF BONE,
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Understanding Rheumatoid Arthritis
 Understanding Rheumatoid Arthritis Understanding Rheumatoid Arthritis What Is Rheumatoid Arthritis? 1,2 Rheumatoid arthritis (RA) is a chronic autoimmune disease. It causes joints to swell and can result
Understanding Rheumatoid Arthritis Understanding Rheumatoid Arthritis What Is Rheumatoid Arthritis? 1,2 Rheumatoid arthritis (RA) is a chronic autoimmune disease. It causes joints to swell and can result
SLE-key Case Studies
 SLE-key Case Studies Ellen M. Field, M.D. Lehigh Valley Health Network, Bethlehem, PA Donald E. Thomas, Jr., M.D., FACP, FACR, RhMSUS, CCD Arthritis and Pain Assoc. of PG County, Greenbelt, MD Case Study
SLE-key Case Studies Ellen M. Field, M.D. Lehigh Valley Health Network, Bethlehem, PA Donald E. Thomas, Jr., M.D., FACP, FACR, RhMSUS, CCD Arthritis and Pain Assoc. of PG County, Greenbelt, MD Case Study
Osteoarthritis. Rheumatology Update. Gout 1/17/2013
 Osteoarthritis Rheumatology Update Richard Zweig, MD January, 2013 Degeneration of cartilage over time accompanied by increase in bone density and bone formation around the joint Risks include: aging,
Osteoarthritis Rheumatology Update Richard Zweig, MD January, 2013 Degeneration of cartilage over time accompanied by increase in bone density and bone formation around the joint Risks include: aging,
Rheumatology Pearls 1) A detailed history is much more useful in the work up of patients with inflammatory peripheral arthritis than any lab tests.
 A detailed history is much more useful in the work up of patients with inflammatory peripheral arthritis than any lab tests.") Rheumatology Pearls 1) A detailed history is much more useful in the work up of patients with inflammatory peripheral arthritis than any lab tests. Features suggestive of an inflammatory arthritis that
Rheumatology Pearls 1) A detailed history is much more useful in the work up of patients with inflammatory peripheral arthritis than any lab tests. Features suggestive of an inflammatory arthritis that
How to interpret and order rheumatology tests
 How to interpret and order rheumatology tests Kam Shojania, MD, FRCPC Clinical Professor and Head, UBC Division of Rheumatology Faculty/Presenter Disclosure Faculty: Kam Shojania Relationships with financial
How to interpret and order rheumatology tests Kam Shojania, MD, FRCPC Clinical Professor and Head, UBC Division of Rheumatology Faculty/Presenter Disclosure Faculty: Kam Shojania Relationships with financial
2018 ReachMD Page 1 of 10
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Physical examination of the musculosceletal- and nervous system. Pánczél Pál dr.
 Physical examination of the musculosceletal- and nervous system in the practice of internal medicine. Pánczél Pál dr. Bursae = sacks of the synovial membrane fulfilled with synovium. Localised between
Physical examination of the musculosceletal- and nervous system in the practice of internal medicine. Pánczél Pál dr. Bursae = sacks of the synovial membrane fulfilled with synovium. Localised between
Rhematologic serum testing is: Before request serologic tests, ANCA associated antigens c-anca: most commonly against the proteinase 3 (PR-3)
") thorough P/E. Rhematologic serum testing is: Useful to confirm a clinical impression or sort out a differential diagnosis Not useful as a screening test A positive test may or may not be associated with
thorough P/E. Rhematologic serum testing is: Useful to confirm a clinical impression or sort out a differential diagnosis Not useful as a screening test A positive test may or may not be associated with
Systemic forms of stiffness
 Systemic forms of stiffness ANNA LITWIC CONSULTANT RHEUMATOLOGIST SALISBURY DISTRICT HOSPITAL CLINICAL RESEARCH FELLOW MRC LIFECOURSE EPIDEMIOLOGY UNIT Overview Rheumatoid arthritis Know it when you see
Systemic forms of stiffness ANNA LITWIC CONSULTANT RHEUMATOLOGIST SALISBURY DISTRICT HOSPITAL CLINICAL RESEARCH FELLOW MRC LIFECOURSE EPIDEMIOLOGY UNIT Overview Rheumatoid arthritis Know it when you see
 www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
Hths 2231 Laboratory 13 Alterations in Musculoskeletal
 Watch Movie: Osteoporosis Answer the movie questions on the worksheet. Complete activities 1-4. Activity #1: Click on the website link in activity 1 to review the structure and function of bone. Activity
Watch Movie: Osteoporosis Answer the movie questions on the worksheet. Complete activities 1-4. Activity #1: Click on the website link in activity 1 to review the structure and function of bone. Activity
Manifestations and Presentations of Collagen Vascular Diseases. Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL
 Manifestations and Presentations of Collagen Vascular Diseases Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL June 29, 2018 Disclosures Joseph LaConti, M.D., Ph.D., has
Manifestations and Presentations of Collagen Vascular Diseases Joseph LaConti, M.D., Ph.D. Center for Arthritis and Rheumatic Diseases Miami, FL June 29, 2018 Disclosures Joseph LaConti, M.D., Ph.D., has
Rheumatology Red Flags and Emergencies :Workshop DR. MICHAEL STARR DIVISION OF RHEUMATOLOGY MUHC
 Rheumatology Red Flags and Emergencies :Workshop DR. MICHAEL STARR DIVISION OF RHEUMATOLOGY MUHC Family Medicine Review Course, November 28th, 2018 Disclosures Amgen Janssen Roche BMS Pfizer UCB Novartis
Rheumatology Red Flags and Emergencies :Workshop DR. MICHAEL STARR DIVISION OF RHEUMATOLOGY MUHC Family Medicine Review Course, November 28th, 2018 Disclosures Amgen Janssen Roche BMS Pfizer UCB Novartis
Undifferentiated Connective Tissue Disease and Overlap Syndromes. Mark S. Box, MD
 Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Undifferentiated Connective Tissue Disease and Overlap Syndromes Mark S. Box, MD Overlap Syndromes As many as 25% of patients with rheumatic diseases with systemic symptoms cannot be definitely diagnosed
Update - Imaging of the Spondyloarthropathies. Spondyloarthropathies. Spondyloarthropathies
 Update - Imaging of the Spondyloarthropathies Donald J. Flemming, M.D. Dept of Radiology Penn State Hershey Medical Center Spondyloarthropathies Family of inflammatory arthritides of synovium and entheses
Update - Imaging of the Spondyloarthropathies Donald J. Flemming, M.D. Dept of Radiology Penn State Hershey Medical Center Spondyloarthropathies Family of inflammatory arthritides of synovium and entheses
1 Eileen Ginsburg, DNP, FNP-BC, ARNP 10/10/2018
 Rheumatology labs: Which to order and what do I do with the results? 1 Eileen Ginsburg, DNP, FNP-BC, ARNP 2 OBJECTIVES: By the end of the lecture you will 1. be able to decide which labs you want to order
Rheumatology labs: Which to order and what do I do with the results? 1 Eileen Ginsburg, DNP, FNP-BC, ARNP 2 OBJECTIVES: By the end of the lecture you will 1. be able to decide which labs you want to order
Rheumatoid Arthritis
 Rheumatoid Arthritis What is rheumatoid arthritis? Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. Rheumatoid arthritis can also cause inflammation of
Rheumatoid Arthritis What is rheumatoid arthritis? Rheumatoid arthritis (RA) is an autoimmune disease that causes chronic inflammation of the joints. Rheumatoid arthritis can also cause inflammation of
History Taking and the Musculoskeletal Examination
 History Taking and the Musculoskeletal Examination Introduction A thorough rheumatologic assessment is performed within the context of a good general evaluation of the patient. The patient should be undressed
History Taking and the Musculoskeletal Examination Introduction A thorough rheumatologic assessment is performed within the context of a good general evaluation of the patient. The patient should be undressed
DISCUSSION BY: Dr M. R. Shakeebi, MD, Rheumatologist
 Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Case presentations Related to some Rheumatic Diseases Lab & Clinic i Programs, Tuesday, April 24, 2012 COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD, Immunologist COORDINATOR: Dr M. Mahdi Mohammadi, LMD,PhD,
Review Article. Appraoch to Patients with Polyarticular Symptoms. Introduction. Raymond WS Wong
 Review Article Appraoch to Patients with Polyarticular Symptoms Raymond WS Wong Abstract: Keywords: Polyarticular symptoms represent the most common symptom complex resulting in referral to a rheumatologist
Review Article Appraoch to Patients with Polyarticular Symptoms Raymond WS Wong Abstract: Keywords: Polyarticular symptoms represent the most common symptom complex resulting in referral to a rheumatologist
INFLAMMATORY/ AUTOIMMUNE AND DEGENERATIVE JOINT DISEASES. Wahinuddin Sulaiman Faculty of Medicine, UniKL Royal College of Medicine Perak
 INFLAMMATORY/ AUTOIMMUNE AND DEGENERATIVE JOINT DISEASES Wahinuddin Sulaiman Faculty of Medicine, UniKL Royal College of Medicine Perak Outline Introduction Assessment / evaluation OA vs RA Treatment JOINT
INFLAMMATORY/ AUTOIMMUNE AND DEGENERATIVE JOINT DISEASES Wahinuddin Sulaiman Faculty of Medicine, UniKL Royal College of Medicine Perak Outline Introduction Assessment / evaluation OA vs RA Treatment JOINT
AOS 3: Rheumatoid Arthritis
 AOS 3: Rheumatoid Arthritis Arthritis (General) = inflamed joint - NOT a single disease: covers >100 types - Involves disability + decreased quality of life o Can also occur in young people (not just the
AOS 3: Rheumatoid Arthritis Arthritis (General) = inflamed joint - NOT a single disease: covers >100 types - Involves disability + decreased quality of life o Can also occur in young people (not just the
The Johns Hopkins Hospital
 The Johns Hopkins Hospital 19901006 2016/03/21-04/20 (rheumatology) (emergecny medicine) (rheumatology consult team) attending Dr. Haque, R2 Dr. Michailidou, fellow Dr. Adler "She is a so interesting case.
The Johns Hopkins Hospital 19901006 2016/03/21-04/20 (rheumatology) (emergecny medicine) (rheumatology consult team) attending Dr. Haque, R2 Dr. Michailidou, fellow Dr. Adler "She is a so interesting case.
Rheumatology Cases for the Internist
 Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
Rheumatology Cases for the Internist Marc C. Hochberg, MD, MPH Professor of Medicine Head, Division of Rheumatology and Clinical Immunology Vice Chair, Department of Medicine University of Maryland School
The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy
 The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy Learning Objectives When to use an acute rheumatology service Appropriate use of steroids by condition Injection or Oral or Intramuscular
The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy Learning Objectives When to use an acute rheumatology service Appropriate use of steroids by condition Injection or Oral or Intramuscular
8/29/2012. Outline Juvenile idiopathic arthritis. 1. Classification-ILAR. 1. Classification-clinical diagnosis. 1. JIA classification
 Outline Juvenile idiopathic arthritis 1. Classification and symptoms (ILAR-International league of Associations for Rheumatology) 2. Imaging J. Herman Kan, M.D. Section chief, musculoskeletal imaging Edward
Outline Juvenile idiopathic arthritis 1. Classification and symptoms (ILAR-International league of Associations for Rheumatology) 2. Imaging J. Herman Kan, M.D. Section chief, musculoskeletal imaging Edward
Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa
 Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa Basic Concepts ANA DsDNA Sm RNP SSA SSB RF/CCP ESR/CRP ANCA Cases Summary Rheumatology Tests Lie and Mislead! Rheumatology Rally
Scott Vogelgesang, MD Division of Rheumatology/Immunology University of Iowa Basic Concepts ANA DsDNA Sm RNP SSA SSB RF/CCP ESR/CRP ANCA Cases Summary Rheumatology Tests Lie and Mislead! Rheumatology Rally
1. To review the diagnosis of gout and its differential. 2. To understand the four stages of gout
 Objectives 1. To review the diagnosis of gout and its differential GOUT 2. To understand the four stages of gout 3. To develop an approach for the acute treatment of gout Anthony Lim 9/13/12 Cycle 3 4.
Objectives 1. To review the diagnosis of gout and its differential GOUT 2. To understand the four stages of gout 3. To develop an approach for the acute treatment of gout Anthony Lim 9/13/12 Cycle 3 4.
Artropathies: what can be seen in hands?
 Artropathies: what can be seen in hands? Poster No.: C-2452 Congress: ECR 2015 Type: Educational Exhibit Authors: B. M. Torres Rodrigues, J. C. Ruivo Rodrigues, C. Albuquerque, D. Silva; Viseu/PT Keywords:
Artropathies: what can be seen in hands? Poster No.: C-2452 Congress: ECR 2015 Type: Educational Exhibit Authors: B. M. Torres Rodrigues, J. C. Ruivo Rodrigues, C. Albuquerque, D. Silva; Viseu/PT Keywords:
Rheumatology Potpourri. Dr. Philip A. Baer Seacourses Asia CME December 2017
 Rheumatology Potpourri Dr. Philip A. Baer Seacourses Asia CME December 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Rheumatology Potpourri Dr. Philip A. Baer Seacourses Asia CME December 2017 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Joint Injuries and Disorders
 Joint Injuries and Disorders Introduction A joint is where two or more bones come together. Your joints include the knees, hips, elbows and shoulders. There are many types of joint disorders, including
Joint Injuries and Disorders Introduction A joint is where two or more bones come together. Your joints include the knees, hips, elbows and shoulders. There are many types of joint disorders, including
Rheumatology Educational Goals & Objectives
 Rheumatology Educational Goals & Objectives Musculoskeletal complaints are very common in the practice of primary care. They may reflect overuse or trauma, or be a manifestation of a broad range of musculoskeletal
Rheumatology Educational Goals & Objectives Musculoskeletal complaints are very common in the practice of primary care. They may reflect overuse or trauma, or be a manifestation of a broad range of musculoskeletal
JuvenileIdiopathicArthritis. Dr Johan Siebert
 JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
JuvenileIdiopathicArthritis Dr Johan Siebert 1 NORMAL DIARTHRODIAL JOINT Synovial is a thin membrane enclosing the joint space The joint space contains fluid that bathes the joint and reduces friction
Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital
 Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital 1. Soft Tissue Rheumatism 2. Myofascial Pain 3. Neurovascular compression Syndromes 4. Complex Regional Pain Syndromes Tendinitis, tenosynovitis
Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital 1. Soft Tissue Rheumatism 2. Myofascial Pain 3. Neurovascular compression Syndromes 4. Complex Regional Pain Syndromes Tendinitis, tenosynovitis
Aches and Pains in Rheumatology: Is it Fibromyalgia, Osteoarthritis, or Rheumatoid Disease?
 Aches and Pains in Rheumatology: Is it Fibromyalgia, Osteoarthritis, or Rheumatoid Disease? SCOTT T ANDERSON, MD, PHD, FACR, CCHP-P CLINICAL PROFESSOR Menu(rotating) DIVISION OF RHEUMATOLOGY, ALLERGY,
Aches and Pains in Rheumatology: Is it Fibromyalgia, Osteoarthritis, or Rheumatoid Disease? SCOTT T ANDERSON, MD, PHD, FACR, CCHP-P CLINICAL PROFESSOR Menu(rotating) DIVISION OF RHEUMATOLOGY, ALLERGY,
RHEUMATOLOGY PATIENT HISTORY FORM
 !! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
!! RAMOS RHEUMATOLOGY, PC RHEUMATOLOGY PATIENT HISTORY FORM Date: / / NAME: Birthdate: / / Last First M. I. Age: Sex: F M Marital status: Never married Married Divorced Separated Widowed Partnered/significant
Rheumatoid Arthritis. Rheumatoid Arthritis. RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling. Rheumatic Diseases
 RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases The prevalence of rheumatoid arthritis in most Caucasian populations approaches 1% among adults 18 and over and
RCS 6080 Medical and Psychosocial Aspects of Rehabilitation Counseling Rheumatic Diseases The prevalence of rheumatoid arthritis in most Caucasian populations approaches 1% among adults 18 and over and
Gout. Crystal deposition disease: Imaging perspectives. Crystal associated arthropathies. Clinical Stages of Gout 07/06/60
 Crystal associated arthropathies Crystal deposition disease: Imaging perspectives Warapat Virayavanich, MD Ramathibodi hospital, Mahidol University Commonly seen arthropathy MSU (gout) CPPD HADD Uncommon
Crystal associated arthropathies Crystal deposition disease: Imaging perspectives Warapat Virayavanich, MD Ramathibodi hospital, Mahidol University Commonly seen arthropathy MSU (gout) CPPD HADD Uncommon
Inflammatory rheumatic diseases
 Learning objectives Inflammatory rheumatic diseases Bruce Kidd Barts & The London, Queen Mary, University of London To understand: 1. prevalence and range of the rheumatological s 2. clinical features
Learning objectives Inflammatory rheumatic diseases Bruce Kidd Barts & The London, Queen Mary, University of London To understand: 1. prevalence and range of the rheumatological s 2. clinical features
Rheumatologic Manifestations of Gastrointestinal Diseases
 Rheumatologic Manifestations of Gastrointestinal Diseases NATASHA DEHGHAN, MD, FRCPC CLINICAL ASSISTANT PROFESSOR VASCULITIS CLINIC, MARY PACK ARTHRITIS CENTRE Objectives To discuss a few common rheumatologic
Rheumatologic Manifestations of Gastrointestinal Diseases NATASHA DEHGHAN, MD, FRCPC CLINICAL ASSISTANT PROFESSOR VASCULITIS CLINIC, MARY PACK ARTHRITIS CENTRE Objectives To discuss a few common rheumatologic
Ultrasound in Rheumatology
 Arthritis Research UK Primary Care Centre Winner of a Queen s Anniversary Prize For Higher and Further Education 2009 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer/Research Fellow Primary
Arthritis Research UK Primary Care Centre Winner of a Queen s Anniversary Prize For Higher and Further Education 2009 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer/Research Fellow Primary
Musculoskeletal Infection and Inflammation
 F.A. Davis: Advantage Musculoskeletal Infection and Inflammation(10.6.15) Page 1 Musculoskeletal Infection and Inflammation The musculoskeletal system is affected by infections and inflammatory conditions.
F.A. Davis: Advantage Musculoskeletal Infection and Inflammation(10.6.15) Page 1 Musculoskeletal Infection and Inflammation The musculoskeletal system is affected by infections and inflammatory conditions.
Physical diagnosis of musculoskeletal system. Dr. Szathmári Miklós Semmelweis University First Department of Medicine 1. Dec
 Physical diagnosis of musculoskeletal system Dr. Szathmári Miklós Semmelweis University First Department of Medicine 1. Dec. 2015. Evaluation of patients with musculoskeletal complaints Anatomic localization
Physical diagnosis of musculoskeletal system Dr. Szathmári Miklós Semmelweis University First Department of Medicine 1. Dec. 2015. Evaluation of patients with musculoskeletal complaints Anatomic localization
Types of osteoarthritis
 ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
Differential diagnostics in Rheumatology
 Differential diagnostics in Rheumatology number of affected joints lengths of duration Acute monoarthritis Chronic monoarthritis Acute polyarthritis Chronic polyarthritis Acute monoarthritis Infective
Differential diagnostics in Rheumatology number of affected joints lengths of duration Acute monoarthritis Chronic monoarthritis Acute polyarthritis Chronic polyarthritis Acute monoarthritis Infective
Seronegative Arthritis. Dr Mary Gayed 25 th April 2018
 Seronegative Arthritis Dr Mary Gayed 25 th April 2018 Overview Description of the conditions Discussion of symptoms & investigations that may be required Discussion of management and treatment Questions
Seronegative Arthritis Dr Mary Gayed 25 th April 2018 Overview Description of the conditions Discussion of symptoms & investigations that may be required Discussion of management and treatment Questions
Joint Disorders. Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10. Overview Disorders of the Muscular System Disorders of the Skeletal System
 Module 7 -Chapter 10. Overview Disorders of the Muscular System Disorders of the Skeletal System") Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10 Overview Disorders of the Muscular System Disorders of the Skeletal System Susie Turner, MD 1/9/13 Joint Disorders Arthritis Inflammation of Joint
Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10 Overview Disorders of the Muscular System Disorders of the Skeletal System Susie Turner, MD 1/9/13 Joint Disorders Arthritis Inflammation of Joint
Crystal induced arthropathies. Dr. Amitesh Aggarwal
 Crystal induced arthropathies Dr. Amitesh Aggarwal 1 Crystal induced Arthropathies Gout Pseudogout Debilitating illnesses; Recurrent episodes of pain and joint inflammation; Formation and deposition of
Crystal induced arthropathies Dr. Amitesh Aggarwal 1 Crystal induced Arthropathies Gout Pseudogout Debilitating illnesses; Recurrent episodes of pain and joint inflammation; Formation and deposition of
ELENI ANDIPA General Hospital of Athens G. Gennimatas
 ELENI ANDIPA General Hospital of Athens G. Gennimatas Technological advances over the last years have caused a dramatic improvement in ultrasound quality and resolution An established imaging modality
ELENI ANDIPA General Hospital of Athens G. Gennimatas Technological advances over the last years have caused a dramatic improvement in ultrasound quality and resolution An established imaging modality
Presenter Disclosure Information
 4:15 5:45 pm Diagnostic Challenges of Rheumatologic Disease SPEAKER Peng Thim Fan, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Peng Thim Fan,
4:15 5:45 pm Diagnostic Challenges of Rheumatologic Disease SPEAKER Peng Thim Fan, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Peng Thim Fan,
A Patient s Guide to Psoriatic Arthritis
 A Patient s Guide to Psoriatic Arthritis Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Psoriatic Arthritis Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled from a variety
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? COPYRIGHT
 Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
Ultrasound in Rheumatology
 Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer Research Institute for Primary Care & Health Sciences, Keele University Department of Rheumatology, Cannock Hospital, Royal Wolverhampton
Ultrasound in Rheumatology Alison Hall Consultant MSK Sonographer Research Institute for Primary Care & Health Sciences, Keele University Department of Rheumatology, Cannock Hospital, Royal Wolverhampton
EXAMINING THE CRUCIAL COALITION BETWEEN DERMATOLOGY AND RHEUMATOLOGY IN PSORIATIC ARTHRITIS
 EXAMINING THE CRUCIAL COALITION BETWEEN DERMATOLOGY AND RHEUMATOLOGY IN PSORIATIC ARTHRITIS ACTIVITY 1: EARLY COLLABORATION IN THE TREATMENT OF PSA Key Slides COMMON COMORBIDITIES OF PSORIATIC DISEASE
EXAMINING THE CRUCIAL COALITION BETWEEN DERMATOLOGY AND RHEUMATOLOGY IN PSORIATIC ARTHRITIS ACTIVITY 1: EARLY COLLABORATION IN THE TREATMENT OF PSA Key Slides COMMON COMORBIDITIES OF PSORIATIC DISEASE
Case Based Rheumatology STEVE S LEE, DO FACR SCPMG FONTANA
 Case Based Rheumatology STEVE S LEE, DO FACR SCPMG FONTANA Disclosure Clinical Investigator: EMD Serono Amgen Roche 1 Learning Objectives Crystalline arthropathy GCA/PMR Infectious arthritis Connective
Case Based Rheumatology STEVE S LEE, DO FACR SCPMG FONTANA Disclosure Clinical Investigator: EMD Serono Amgen Roche 1 Learning Objectives Crystalline arthropathy GCA/PMR Infectious arthritis Connective
Approach to Arthritis
 Approach to Arthritis Dr. V. Krishnamurthy M. D., D. M. (Rheumatology) Rheumatologist, Chennai Meenakshi Multispecialty Hospital Rheumatologist, Meenakshi Academy of Higher Education (MAHER), Apollo Specialty
Approach to Arthritis Dr. V. Krishnamurthy M. D., D. M. (Rheumatology) Rheumatologist, Chennai Meenakshi Multispecialty Hospital Rheumatologist, Meenakshi Academy of Higher Education (MAHER), Apollo Specialty
Diseases. Siriporn Juthong, M.D. Division of Rheumatology 23/11/58
 Common Connective tissue Diseases Siriporn Juthong, M.D. Division of Rheumatology Songklanagarind Hospital 23/11/58 What are the diseases in connective tissue disorder? Sign and symptoms of CTD? Nonspecific
Common Connective tissue Diseases Siriporn Juthong, M.D. Division of Rheumatology Songklanagarind Hospital 23/11/58 What are the diseases in connective tissue disorder? Sign and symptoms of CTD? Nonspecific
Polymyalgia, Temporal Arteritis and pineapples
 Polymyalgia, Temporal Arteritis and pineapples Rod Hughes Consultant Rheumatologist Ashford St Peter s Hospital Trust Chertsey Wed 11 th May 2011 Meeting aims Pineapples their significance in disease Defining
Polymyalgia, Temporal Arteritis and pineapples Rod Hughes Consultant Rheumatologist Ashford St Peter s Hospital Trust Chertsey Wed 11 th May 2011 Meeting aims Pineapples their significance in disease Defining
Rheumatology 101 A Pediatrician s Guide
 Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
Rheumatology 101 A Pediatrician s Guide Pediatric Staff and Alumni Day 2016 Dawn M. Wahezi, Yonit Sterba, Tamar Rubinstein Disclosures None Pick a Group Group 1 A child with a limp Group 2 ANA To test
LIST ALL CURRENT MEDICATIONS BELOW INCLUDING INJECTIONS/INFUSION MEDICINES MEDS) Name of Medication Dose How often taken
 Name of Medication Dose How often taken") Please take a moment to fill out the following forms front and back: Pharmacy Information: (Include the Name, Address and Phone Number of the Pharmacy) Preferred Local: Preferred Mail Order/Specialty:
Please take a moment to fill out the following forms front and back: Pharmacy Information: (Include the Name, Address and Phone Number of the Pharmacy) Preferred Local: Preferred Mail Order/Specialty:
The Painful Elbow, Wrist, and Hand. Jennifer R Marks, MD
 The Painful Elbow, Wrist, and Hand Jennifer R Marks, MD The Painful Elbow A 44 yo M presents to clinic complaining of a sore elbow What further questions do you have for this patient? What is on your differential
The Painful Elbow, Wrist, and Hand Jennifer R Marks, MD The Painful Elbow A 44 yo M presents to clinic complaining of a sore elbow What further questions do you have for this patient? What is on your differential
Assessment of Inflammatory Back Pain: New Concepts in Diagnosis
 Assessment of Inflammatory Back Pain: New Concepts in Diagnosis March 2 nd, 2018 Spine Therapy Network Interprofessional Synposium Sheraton Toronto Airport Hotel, Toronto, CANADA Laura Passalent PT, BScPT,
Assessment of Inflammatory Back Pain: New Concepts in Diagnosis March 2 nd, 2018 Spine Therapy Network Interprofessional Synposium Sheraton Toronto Airport Hotel, Toronto, CANADA Laura Passalent PT, BScPT,
The Rheumatoid Hand Deformities & Management. Dr. Anirudh Sharma Resident Department of Orthopedics
 + The Rheumatoid Hand Deformities & Management Dr. Anirudh Sharma Resident Department of Orthopedics + Why is Rheumatoid Arthritis important? + RA is a very debilitating disease median life expectancy
+ The Rheumatoid Hand Deformities & Management Dr. Anirudh Sharma Resident Department of Orthopedics + Why is Rheumatoid Arthritis important? + RA is a very debilitating disease median life expectancy
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R
 The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
Seronegative spondyloarthropathies : A Pictorial Review
 Seronegative spondyloarthropathies : A Pictorial Review Poster No.: P-0008 Congress: ESSR 2012 Type: Scientific Exhibit Authors: J. Acosta Batlle, B. Palomino Aguado, M. D. Lopez Parra, S. 1 2 3 2 4 1
Seronegative spondyloarthropathies : A Pictorial Review Poster No.: P-0008 Congress: ESSR 2012 Type: Scientific Exhibit Authors: J. Acosta Batlle, B. Palomino Aguado, M. D. Lopez Parra, S. 1 2 3 2 4 1
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Definition and Risk Factors Idiopathic vs. Secondary OA Clinical Features Diagnosis Radiologic Features ACR OA
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Definition and Risk Factors Idiopathic vs. Secondary OA Clinical Features Diagnosis Radiologic Features ACR OA
Arthritis. that affects the joints.
 Arthritis that affects the joints. The word arthritis literally means inflammation of the joints. Though joint inflammation is often a symptom, rather than a specific diagnosis itself, the term arthritis
Arthritis that affects the joints. The word arthritis literally means inflammation of the joints. Though joint inflammation is often a symptom, rather than a specific diagnosis itself, the term arthritis
Psoriasis and Psoriatic Arthritis Combined Clinic Electronic Medical Records Form
 Psoriasis and Psoriatic Arthritis Combined Clinic Electronic Medical Records Form NAME: AGE: SEX: CHIEF COMPLAINT: HISTORY OF PRESENT ILLNESS: The patient presents for the initial evaluation of [psoriasis
Psoriasis and Psoriatic Arthritis Combined Clinic Electronic Medical Records Form NAME: AGE: SEX: CHIEF COMPLAINT: HISTORY OF PRESENT ILLNESS: The patient presents for the initial evaluation of [psoriasis