Patogenesi e terapia della Neuropatia Motoria Multifocale
|
|
|
- Hester Chandler
- 6 years ago
- Views:
Transcription


1 26 Settembre 2014 Patogenesi e terapia della Neuropatia Motoria Multifocale Francesca Gallia Neurologia 2, Ist. Clin. Humanitas Rozzano, Milano
2 Multifocal Motor Neuropathy Rare disorder characterized by: progressive, predominantly distal, multineuropathic limb weakness, usually more pronounced in the arms; minimal or no sensory loss; multifocal persistent partial motor conduction block. Frequent (30-50%) association with anti-gm1 IgM antibodies Frequent (80%) response to IVIg


3
4 Prevalence of MMN Prevalence was estimated to be 1-2 per 100,000 inhabitants (Nobile-Orazio et al, 2005) and was 0.6 per 100,000 inhabitants in the Dutch study (Cats et al. 2010) MMN is more frequent in men than women (Nobile- Orazio et al, 2.6:1; Cats et al, 2010: 2.7:1) Age at onset is 41 y.o. with 80% of reported patients between 20 and 50 y.o. (Nobile-Orazio et al, 2005). MMN affects men earlier than women (38 vs 45 y.o.) (Cats et al, 2010).
5 CLINICAL FEATURES OF MMM Total reported patients until Men/women (ratio) 200/76 (2.6:1) Mean age of onset (range) 41.0 (15-72) Progression: chronic progressive 82% step-wise/rel.-rem. 14%/4% Limb weakness: 100% Asymmetric 94% Distal > proximal 87% Upper > lower limbs 79% Muscle atrophy (often mild) 86% Fasciculations 58% Cramps 55% Deep tendon reflexes: Reduced or absent 72% Normal or Brisk 28% Sensory impairment (minor) 20%
6 Distinguishing features in CIDP, LSS, MMN, MND Features CIDP LSS MMN LMND Distribution Symmetric Multineuropathic Multineuropathic Asymm or Symm Arms >legs no yes (40-70%) yes (80%) sometimes Distal>prox. no yes yes often Sensory loss yes yes no no Gen.Areflexia yes no no no Cranial/bulbar yes no no yes Motor CB yes yes yes no Reduced CV yes no no no ReducedSNAP yes yes no no CSF proteins yes rare (1/3) rare (1/3) no GM1 IgM no no yes (30-40%) rare (5-10%) Sural biopsy demyelin. demyelin. normal normal Steroid response yes (2/3) yes (2/3) no (1/10) no IVIg effective yes (2/3) yes (1/2) yes (4/5) no
7 2010 EFNS/PNS Criteria for MMN A) Core criteria (both must be present) 1. Asymmetric limb weakness, or motor involvement having a nerve distribution in > 2 nerves, slowly progressive or stepwise progressive, for > 1 month 2. No objective sensory abnormalities except for minor vibration sense abnormalities in the lower limbs. B) Supportive clinical criteria 3. Predominant upper limb involvement 4. Decreased or absent tendon reflexes in the affected limb 5. Absence of cranial nerve involvement 6. Cramps and fasciculations in the affected limb 7. Response to immune therapy C) Exclusion criteria 8. Upper motor neuron signs 9. Marked bulbar involvement 10. Sensory impairment beside minor vibration loss in the legs 11. Diffuse symmetric weakness during the initial weeks JPNS 2010
8 2010 EFNS/PNS NCS Criteria for MMN 1. Definite motor CB: prox. vs distal neg. CMAP area reduction > 50% whatever the nerve segment length. Negative distal CMAP amp. must be >20% of lower NL & > 1 mv & increase of proximal CMAP duration (temporal dispersion: TD) 30%. 2. Probable motor CB: negative CMAP area reduction of > 30% over a long segment of an UL nerve with TD 30%; OR negative CMAP area reduction of > 50% with TD > 30%. 3. Normal sensory nerve conduction in upper limb segments with CB and normal SNAP amplitudes.
9 Neurology 2002;58: /6 patients improved with IVIg
10 Neurology 2006: 67: 592-6) 14/20 (70%) with CB vs.7/13 (54%) without CB (including 7 without any demyelinating features) improved with IVIg
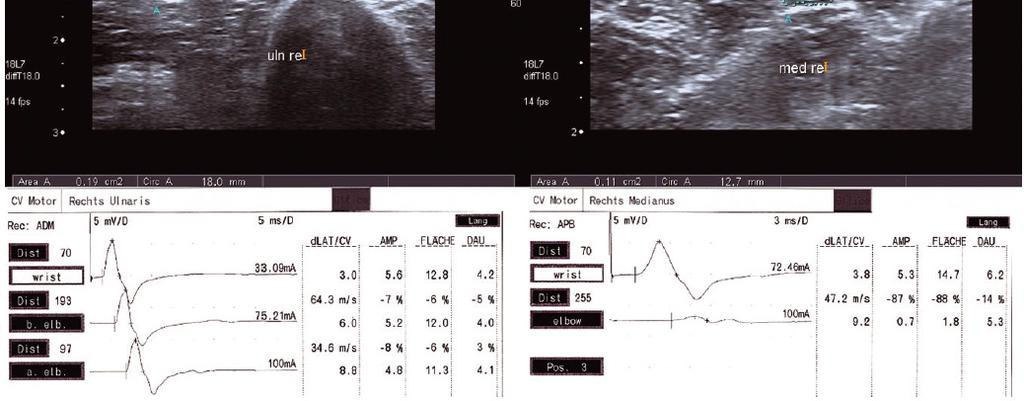
11 Case Report: 26 y.o. woman History: 1 yr progressive left hand weakness in the muscles of ulnar nerve, extending 6 mos later to muscles of median nerve; N.E: Severe weakness (1-2) & atrophy in left ulnar nerve; mild weakness (4) & atrophy in left median nerve. Normal sensation. DTR slightly reduced distally in left arm.
12 2010 EFNS/PNS Supportive Criteria for MMN Elevated IgM anti-gm1 antibodies Increased CSF proteins but < 100 mg/dl MRI Gadolinium enhancement/ hypertrophy of the brachial plexuses (or high resolution sonography) Clinical improvement after IVIg therapy
13 Diagnostic Categories in MMN A) Definite MMN - Core criteria and exclusion criteria AND definite CB with normal sensory NCS in > 1 nerve B) Probable MMN - Core criteria and exclusion criteria AND probable CB with normal sensory NCS in > 2 nerve or - Core criteria and exclusion criteria AND probable CB with normal sensory NCS in 1 nerve AND > 1 supportive criteria: C) Possible MMN - Core criteria and exclusion criteria AND normal sensory NCS and response to IVIg or - Core criteria 1 in 1 nerve and clinical involvement of 1 nerve, no sensory loss, exclusion criteria AND definite or probable CB with normal NCS in 1 nerve

14 LOCALIZATION OF GM1 & Gal(β1-3)GalNAc PNS Motor nerve terminals at NMJ Compact myelin Outer myelin Paranodal myelin Nodes of Ranvier Schwann cells Illa et al, Ann Neurol, 1995 CNS Gray > white matter Isolated spinal motor neuron Axon network & gray matter
15 ANTI-GM1 IgM ANTIBODIES BY ELISA IN MOTOR NEURON SYNDROMES

16 JNNP 2013 IgM antibody Frequency versus controls Sensitivity Specificity Positive Predictive value GM1 p< % 93% 65.5% GM1 >1/2560 p< % 99.3% 91.2% GM2 n.s. 7.5% 98.1% 50% NS6S n.s. 22.5% 91.4% 39.1% Galactocerebroside p< % 70.4% 37.5% GM1-Gal p< % 85.2% 58.8% GM1-Gal >1/2560 p< % 92.2% 66.6% GM1-Gal >1/5120 p< % 98.6% 88.9%

17
18 EVIDENCES FOR IMMUNE PATHOGENESIS IN MMN IgM antibodies to GM1 or other gangliosides are present in 30-50% of MMN patients (but may be also found in other PN and MND) and often decrease during clinical improvement; Deposits of IgM were found at the nodes of Ranvier of sural nerve in a patient with CB (and MND); CB can be induced in vitro & vivo by serum from MMN patients with and without anti-gm1 IgM; Most patients with MMN respond to immune therapies (IVIg). Illa et al
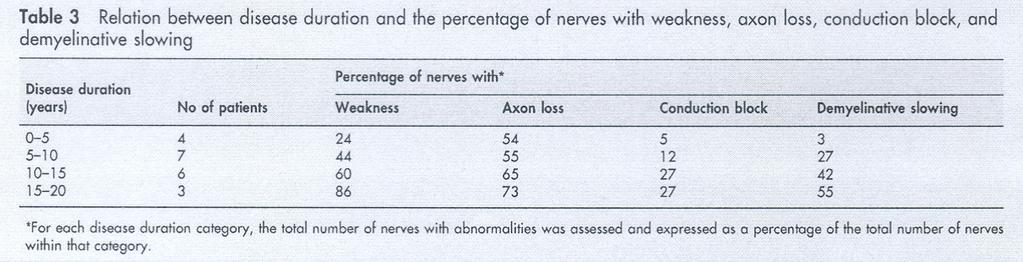
19 Disability progression in MMN Years of neuropathy N pts N pts Rankin 2 score > % disable patients % 33% 17.5% 9.5% Years from onset neuropathy
20 IMMUNE THERAPIES IN MMN No. No. (%) No. (%) Therapy treated improved worsened Steroids (alone) 64 (62) 7 (11%) 14(22%) Plasmaexch.(alone) 21 (20) 4 (20%) 2 (10%) IVIg: 383 impairment: 303/373 (81%) disability: 91/123 (74%)
21 IVIg for Multifocal Motor Neuropathy Van Schaik I, van den Berg L, de Haan R, Vermeulen M Cochrane Database of Systematic Review, 2005, April 18 Reviewers summary and conclusion: Four RCT assessing the effect of IVIg in MMN have been performed including a total of 34 patients. Strength improved in 78% pts treated with IVIg vs 4% with placebo; disability improved in 39% treated and 11% untreated patients IVIg has beneficial effect on strength in MMN and provide a non-significant trends toward improvement in disability More research is needed to discover whether IVIg improves disability and is cost-effective.
22 PATIENTS : 44 subjects; 41 completed the study. DESIGNS: double-blind, cross-over IGIV 10% versus placebo. RESULTS: Greater decline from baseline (61% vs 34%) in grip strength after placebo (p=0.005). A greater proportion of subjects deteriorated under placebo (36% vs 12%; p=0.021) CONCLUSIONS: IGIV,10% safe, tolerated & effective in MMN
23 LONG-TERM IVIg THERAPY IN MMN Azulay et al., J Neurol Neurosurg Psychiatry /12 (66%) responding pts required repeated Ig x 9-48 mos, uneffective in 3 after 3 mos; 2 (11%) in remission after 1 yr. Van den Berg et al., Brain /7 (86%) responding pts required weekly Ig (0.4g/kg/wk) x 2-4 yrs (follow-up); 3 (43%) had some deterioration. Periodic IVIg are necessary in most MMN patients
24 Neurology MMN patients responding to IVIg treated with periodic IVIg infusions for 5-12 yrs (mean 8.2) Summed dcmap Mean MRC Summed pcmap
25
26 JNNP 2011; 82: 87-91)
27 Are IVIg similarly effective in the maintenance treatment of MMN? MRC sum score MMN patients treated for 5 years Flebogamma IgVena Gammagard Kiovig Flebogamma IgV Gammagard Kioving Average initial MRC Average final MRC
28 Disability progression in MMN Years of neuropathy Treated patients Rankin > (14%) 1 (25%) Untreated patients Rankin > 3 2 (12%) 3 (25%) 3 (60%) 2 (66%) 100 % disable patients (Rankin > 3) p< 0.01 p< 0.01 Treated Not treated Years from onset neuropathy
29 SHOULD WE CONSIDER OTHER IMMUNE THERAPIES IN MMN? To treat patients not responsive to IVIg To treat patients progressively less responsive or unresponsive to IVIg To reduce the cost of IVIg use To reduce patients dependency from IVIg and Hospital admission
 were equally effective for 3 courses J Periph Nerv Syst 2009; 14: 93-100 a) 5/5 deteriorated or did not tolerate 50% reduced SCIg b) 4/5 maintained for 6")
30 Eur J Neurol 2009; 16: a) 9 patients in a single blinded cross-over study of IVIg vs SCIg b) IVIg (+4.3%) & SCIg (+3.6%) were equally effective for 3 courses J Periph Nerv Syst 2009; 14: a) 5/5 deteriorated or did not tolerate 50% reduced SCIg b) 4/5 maintained for 6 mos improvement with equal dose of SCIg
31
32 OTHER IMMUNE THERAPIES IN MMN No. No. (%) Therapy treated improved Cyclophoshamide i.v (75%) oral 6 3 (50%) Interferon-β1a 15 8 (53%) Azathioprine, (alone) 10 (4) 5 (2) (50%) Rituximab (61%) Eculizumab 13 7 (54%) Mycophenolate 1 0 Cyclosporine 2 2
33 28 pts randomized 1 pt with MMF IVIg by 50%. No signif. of IVIg after 12 mo. Pts did not have drug toxicity. No signif. progression after 12 mo Muscle strength, FS unchanged after 3 months & GMI-IgM after 12 months. Adjunctive MMF was safe but did not alter MMN course or allow IVIg reduction
34

35 Immunosuppressant & Immunomodulatory treatments for MMN Umapathi T, Hughes RAC, Nobile-Orazio E, Leger JM Cochrane Database of Systematic Reviews 2012 Reviewers conclusion: In the only RCT, mycophenolate mofetil did not significantly improve strength or function or reduce the need for IVIg The use of corticosteroids, and occasionally plasma exchange, has been associated with deterioration. There are some reports of benefit but also of serious adverse events from cyclophosphamide either as a primary agent or for patients who do not respond or lose their response to IVIg or require frequent infusions There is still little or no evidence about azathioprine, β interferon, rituximab or ciclosporin, Trials of IS should be undertaken but non-randomised studies do not suggest a particular favourite candidate.
36 TREATMENT OF MMN 2010 EFNS/PNS RECOMMENDATIONS 1. IVIg (2 g/kg over 2 to 5 days) should be considered as first line treatment (Level A recommendation) when disability is sufficiently severe to warrant treatment. 2. Steroids are not recommended (Good Practice Point). 3. If IVIg is initially effective, repeated IVIg should be considered (Level C) and its frequency guided by the response (Good Practice Point). Typical treatment regimens are 1 g/kg every 2 to 4 weeks, or 2 g/kg every 1 to 2 months (Good Practice Point). 4. Only if IVIg is not sufficiently effective immunosuppression may be considered. Cyclophosphamide, interferon β1a, cyclosporin, azathioprine are possible agents (GPP). 5. Toxicity makes cyclophosphamide less desirable (GPP)
Answers to Self Assessment Questions
 Answers to Self Assessment Questions 1. Which of the following findings is supportive of the diagnosis of multifocal motor neuropathy (MMN): A. Absence of conduction block (CB) on nerve conduction studies
Answers to Self Assessment Questions 1. Which of the following findings is supportive of the diagnosis of multifocal motor neuropathy (MMN): A. Absence of conduction block (CB) on nerve conduction studies
Treatment of multifocal motor neuropathy with interferon-β1a
 Treatment of multifocal motor neuropathy with interferon-β1a 12 MMN RM Van den Berg-Vos, LH Van den Berg, H Franssen, PA Van Doorn, ISJ Martina, JHJ Wokke Adapted from Neurology 2000; 54: 1518-1521. Chapter
Treatment of multifocal motor neuropathy with interferon-β1a 12 MMN RM Van den Berg-Vos, LH Van den Berg, H Franssen, PA Van Doorn, ISJ Martina, JHJ Wokke Adapted from Neurology 2000; 54: 1518-1521. Chapter
Multifocal motor neuropathy: long-term clinical and electrophysiological assessment of intravenous immunoglobulin maintenance treatment
 Multifocal motor neuropathy: long-term clinical and electrophysiological assessment of intravenous immunoglobulin maintenance treatment 11 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, LH Van den Berg
Multifocal motor neuropathy: long-term clinical and electrophysiological assessment of intravenous immunoglobulin maintenance treatment 11 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, LH Van den Berg
Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment
 Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment 7 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, HW Van Es, LH Van den Berg Annals of Neurology 2000;
Multifocal motor neuropathy: diagnostic criteria that predict the response to immunoglobulin treatment 7 MMN RM Van den Berg-Vos, H Franssen, JHJ Wokke, HW Van Es, LH Van den Berg Annals of Neurology 2000;
CIDP + MMN - how to diagnose and treat. Dr Hadi Manji
 CIDP + MMN - how to diagnose and treat Dr Hadi Manji Outline Introduction CIDP Diagnosis Clinical features MRI Nerve conduction tests Lumbar puncture Nerve biopsy Treatment IV Ig Steroids Plasma Exchnage
CIDP + MMN - how to diagnose and treat Dr Hadi Manji Outline Introduction CIDP Diagnosis Clinical features MRI Nerve conduction tests Lumbar puncture Nerve biopsy Treatment IV Ig Steroids Plasma Exchnage
Clinical Commissioning Policy Proposition:
 Clinical Commissioning Policy Proposition: Rituximab for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), multifocal motor neuropathy (MMN), vasculitis of the peripheral nervous system
Clinical Commissioning Policy Proposition: Rituximab for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), multifocal motor neuropathy (MMN), vasculitis of the peripheral nervous system
Introduction and aims of the study
 Introduction and aims of the study 1 Chapter 1 Motor neuron diseases include the most incapacitating and life-threatening illnesses but also rather benign disorders with only mild symptoms and slow progression.
Introduction and aims of the study 1 Chapter 1 Motor neuron diseases include the most incapacitating and life-threatening illnesses but also rather benign disorders with only mild symptoms and slow progression.
Severe Chronic Inflammatory Demyelinating Polyneuropathy Ameliorated following High-dose (3 g/kg) Intravenous Immunoglobulin Therapy
 Intravenous Immunoglobulin Therapy") doi: 10.2169/internalmedicine.1723-18 http://internmed.jp CASE REPORT Severe Chronic Inflammatory Demyelinating Polyneuropathy Ameliorated following High-dose (3 g/kg) Intravenous Immunoglobulin Therapy
doi: 10.2169/internalmedicine.1723-18 http://internmed.jp CASE REPORT Severe Chronic Inflammatory Demyelinating Polyneuropathy Ameliorated following High-dose (3 g/kg) Intravenous Immunoglobulin Therapy
A Tale of Five Demyelinating Neuropathies
 Objectives A Tale of Five Demyelinating Neuropathies Tahseen Mozaffar, MD FAAN Professor and Vice Chair of Neurology Director, UC Irvine-MDA ALS and Neuromuscular Center Director, Neurology Residency Training
Objectives A Tale of Five Demyelinating Neuropathies Tahseen Mozaffar, MD FAAN Professor and Vice Chair of Neurology Director, UC Irvine-MDA ALS and Neuromuscular Center Director, Neurology Residency Training
Immune Mediated Neuropathies
 Immune Mediated Neuropathies Hernan Gatuslao, M.D. Assistant Professor Department of Neurology Virginia Commonwealth University School of Medicine AIDP and CIDP Acute inflammatory demyelinating polyneuropathy
Immune Mediated Neuropathies Hernan Gatuslao, M.D. Assistant Professor Department of Neurology Virginia Commonwealth University School of Medicine AIDP and CIDP Acute inflammatory demyelinating polyneuropathy
NHS England Reference: /P
 Clinical Commissioning Policy: Rituximab for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), multifocus motor neuropathy (MMN), vasculitis of the peripheral nervous system & IgM paraprotein-associated
Clinical Commissioning Policy: Rituximab for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), multifocus motor neuropathy (MMN), vasculitis of the peripheral nervous system & IgM paraprotein-associated
Jonathan Katz, MD CPMC
 Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC First, a bit of background Classic CIDP--TREATABLE MADSAM/Asymmetric Neuropathy Chronic Length Dependent Neuropathy-
Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC Jonathan Katz, MD CPMC First, a bit of background Classic CIDP--TREATABLE MADSAM/Asymmetric Neuropathy Chronic Length Dependent Neuropathy-
ORIGINAL COMMUNICATION. IVIg dose increase
 J Neurol (2009) 256:608 614 DOI 10.1007/s00415-009-0130-0 ORIGINAL COMMUNICATION Andreas Baumann Christian W. Hess Matthias Sturzenegger IVIg dose increase in multifocal motor neuropathy A prospective
J Neurol (2009) 256:608 614 DOI 10.1007/s00415-009-0130-0 ORIGINAL COMMUNICATION Andreas Baumann Christian W. Hess Matthias Sturzenegger IVIg dose increase in multifocal motor neuropathy A prospective
The clinical spectrum of Malaysian patients with. Chronic inflammatory demyelinating polyneuropathy
 Neurology Asia 2004; 9 : 39 45 The clinical spectrum of Malaysian patients with chronic inflammatory demyelinating polyneuropathy Khean Jin GOH, Wai Keong NG, Nee Kong CHEW, Chong Tin TAN Division of Neurology,
Neurology Asia 2004; 9 : 39 45 The clinical spectrum of Malaysian patients with chronic inflammatory demyelinating polyneuropathy Khean Jin GOH, Wai Keong NG, Nee Kong CHEW, Chong Tin TAN Division of Neurology,
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists
 & electromyography (EMG) for non-neurologists") Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Guide to the use of nerve conduction studies (NCS) & electromyography (EMG) for non-neurologists What is NCS/EMG? NCS examines the conduction properties of sensory and motor peripheral nerves. For both
Peripheral Neuropathies
 Peripheral Neuropathies ELBA Y. GERENA MALDONADO, MD ACTING ASSISTANT PROFESSOR UNIVERSITY OF WASHINGTON MEDICAL CENTER Objectives Definition Neurophysiology Evaluation of polyneuropathies Cases Summary
Peripheral Neuropathies ELBA Y. GERENA MALDONADO, MD ACTING ASSISTANT PROFESSOR UNIVERSITY OF WASHINGTON MEDICAL CENTER Objectives Definition Neurophysiology Evaluation of polyneuropathies Cases Summary
Making sense of Nerve conduction & EMG
 Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
Making sense of Nerve conduction & EMG Drs R Arunachalam Consultant Clinical Neurophysiologist Wessex Neurological Centre Southampton University Hospital EMG/NCS EMG machine For the assessment of patients
LE SYNDROME DE GUILLAIN-BARRE
 FORMATION UNIVERSITAIRE SPECIFIQUE (FUS) Enseignement interuniversitaire MASTER DE SPECIALISATION EN MEDECINE INTERNE Samedi 19 dećembre 2015 Institute of Neurosciences LE SYNDROME DE GUILLAIN-BARRE Peter
FORMATION UNIVERSITAIRE SPECIFIQUE (FUS) Enseignement interuniversitaire MASTER DE SPECIALISATION EN MEDECINE INTERNE Samedi 19 dećembre 2015 Institute of Neurosciences LE SYNDROME DE GUILLAIN-BARRE Peter
Multifocal motor neuropathy and progressive muscular atrophy
 Multifocal motor neuropathy and progressive muscular atrophy Pathophysiological similarities and differences Lotte Vlam Cover image Meindert Vlam Layout Renate Siebes, Proefschrift.nu Printed by Ridderprint,
Multifocal motor neuropathy and progressive muscular atrophy Pathophysiological similarities and differences Lotte Vlam Cover image Meindert Vlam Layout Renate Siebes, Proefschrift.nu Printed by Ridderprint,
PhD. Authors/faculty
 Multifocal Motor Neuropathy Eduardo Nobile-Orazio, MD, PhD,Alberto Cappellari, MD,and Alberto Priori, MD, PhD No one involved in the planning of this CME activity has any y relevant financial relationships
Multifocal Motor Neuropathy Eduardo Nobile-Orazio, MD, PhD,Alberto Cappellari, MD,and Alberto Priori, MD, PhD No one involved in the planning of this CME activity has any y relevant financial relationships
Evaluation of Peripheral Neuropathy. Evaluation of Peripheral Neuropathy - Introduction
 Evaluation of Peripheral Neuropathy Chris Edwards, MD Ochsner Neurology, Main Campus Evaluation of Peripheral Neuropathy - Introduction A very common complaint in the clinic Presentation is variable Multiple
Evaluation of Peripheral Neuropathy Chris Edwards, MD Ochsner Neurology, Main Campus Evaluation of Peripheral Neuropathy - Introduction A very common complaint in the clinic Presentation is variable Multiple
Comparison of diabetes patients with demyelinating diabetic sensorimotor polyneuropathy to those diagnosed with CIDP
 Comparison of diabetes patients with demyelinating diabetic sensorimotor polyneuropathy to those diagnosed with CIDP Samantha K. Dunnigan 1, Hamid Ebadi 1, Ari Breiner 1, Hans D. Katzberg 1, Leif E. Lovblom
Comparison of diabetes patients with demyelinating diabetic sensorimotor polyneuropathy to those diagnosed with CIDP Samantha K. Dunnigan 1, Hamid Ebadi 1, Ari Breiner 1, Hans D. Katzberg 1, Leif E. Lovblom
Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM. Andrzej Sladkowski
 Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM Andrzej Sladkowski Potential causes of weakness in the ICU-1 Muscle disease Critical illness myopathy Inflammatory myopathy Hypokalemic
Critical Illness Polyneuropathy CIP and Critical Illness Myopathy CIM Andrzej Sladkowski Potential causes of weakness in the ICU-1 Muscle disease Critical illness myopathy Inflammatory myopathy Hypokalemic
Dosing schedules for IVIG: The use of an algorithm as a suggestion for personalized dosing
 Dosing schedules for IVIG: The use of an algorithm as a suggestion for personalized dosing 1 Disclosure The presentation contains information outside the labelled indication for intravenous immunoglobulin
Dosing schedules for IVIG: The use of an algorithm as a suggestion for personalized dosing 1 Disclosure The presentation contains information outside the labelled indication for intravenous immunoglobulin
1/22/2019. Nerve conduction studies. Learning objectives: Jeffrey Allen MD University of Minnesota Minneapolis, MN
 Jeffrey Allen MD University of Minnesota Minneapolis, MN February 9, 2019 Learning objectives: Describe electrophysiologic features of peripheral nerve demyelination Identify electrophysiology findings
Jeffrey Allen MD University of Minnesota Minneapolis, MN February 9, 2019 Learning objectives: Describe electrophysiologic features of peripheral nerve demyelination Identify electrophysiology findings
Corticosteroids in chronic inflammatory demyelinating polyneuropathy
 https://doi.org/10.1007/s00415-018-8948-y ORIGINAL COMMUNICATION Corticosteroids in chronic inflammatory demyelinating polyneuropathy A retrospective, multicentre study, comparing efficacy and safety of
https://doi.org/10.1007/s00415-018-8948-y ORIGINAL COMMUNICATION Corticosteroids in chronic inflammatory demyelinating polyneuropathy A retrospective, multicentre study, comparing efficacy and safety of
Clinical background of the multifocal motor neuropathy: the Lausanne experience
 Clinical background of the multifocal motor neuropathy: the Lausanne experience n T. Kuntzer, A. J. Radziwill, S. A. Botez Original article Nerve-Muscle Unit, Neurology Service, Lausanne University Hospital
Clinical background of the multifocal motor neuropathy: the Lausanne experience n T. Kuntzer, A. J. Radziwill, S. A. Botez Original article Nerve-Muscle Unit, Neurology Service, Lausanne University Hospital
Deterioration after corticosteroids in CIDP may be associated with pure focal demyelination pattern
 Eftimov et al. BMC Neurology 2014, 14:72 RESEARCH ARTICLE Open Access Deterioration after corticosteroids in CIDP may be associated with pure focal demyelination pattern Filip Eftimov *, Marinus H Liesdek,
Eftimov et al. BMC Neurology 2014, 14:72 RESEARCH ARTICLE Open Access Deterioration after corticosteroids in CIDP may be associated with pure focal demyelination pattern Filip Eftimov *, Marinus H Liesdek,
Authors' objectives To evaluate the efficacy of intravenous immunoglobulin (IVIG) for neurologic conditions.
 for neurologic conditions.") Use of intravenous immunoglobulin for treatment of neurologic conditions: a systematic review Fergusson D, Hutton B, Sharma M, Tinmouth A, Wilson K, Cameron D W, Hebert P C CRD summary This review assessed
Use of intravenous immunoglobulin for treatment of neurologic conditions: a systematic review Fergusson D, Hutton B, Sharma M, Tinmouth A, Wilson K, Cameron D W, Hebert P C CRD summary This review assessed
C hronic inflammatory demyelinating polyneuropathy
 PAPER Intractable chronic inflammatory demyelinating polyneuropathy treated successfully with ciclosporin M Odaka, M Tatsumoto, K Susuki, K Hirata, N Yuki... See end of article for authors affiliations...
PAPER Intractable chronic inflammatory demyelinating polyneuropathy treated successfully with ciclosporin M Odaka, M Tatsumoto, K Susuki, K Hirata, N Yuki... See end of article for authors affiliations...
Distal chronic spinal muscular atrophy involving the hands
 Journal ofneurology, Neurosurgery, and Psychiatry, 1978, 41, 653-658 Distal chronic spinal muscular atrophy involving the hands D. J. O'SULLIVAN AND J. G. McLEOD From St Vincent's Hospital, and Department
Journal ofneurology, Neurosurgery, and Psychiatry, 1978, 41, 653-658 Distal chronic spinal muscular atrophy involving the hands D. J. O'SULLIVAN AND J. G. McLEOD From St Vincent's Hospital, and Department
ORIGINAL CONTRIBUTION. Efficacy of Intravenous Immunoglobulin in Patients With IgG Monoclonal Gammopathy and Polyneuropathy
 ORIGINAL CONTRIBUTION Efficacy of Intravenous Immunoglobulin in Patients With IgG Monoclonal Gammopathy and Polyneuropathy Kenneth C. Gorson, MD; Allan H. Ropper, MD; David H. Weinberg, MD; Robert Weinstein,
ORIGINAL CONTRIBUTION Efficacy of Intravenous Immunoglobulin in Patients With IgG Monoclonal Gammopathy and Polyneuropathy Kenneth C. Gorson, MD; Allan H. Ropper, MD; David H. Weinberg, MD; Robert Weinstein,
Symptomatic pain treatments (carbamazepine and gabapentin) were tried and had only a transient and incomplete effect on the severe pain syndrome.
 were tried and had only a transient and incomplete effect on the severe pain syndrome.") Laurencin 1 Appendix e-1 Supplementary Material: Clinical observations Patient 1 (48-year-old man) This patient, who was without a notable medical history, presented with thoracic pain and cough, which
Laurencin 1 Appendix e-1 Supplementary Material: Clinical observations Patient 1 (48-year-old man) This patient, who was without a notable medical history, presented with thoracic pain and cough, which
Comparison of electrophysiological findings in axonal and demyelinating Guillain-Barre syndrome
 Iranian Journal of Neurology Original Paper Iran J Neurol 2014; 13(3): 138-143 Comparison of electrophysiological findings in axonal and demyelinating Guillain-Barre syndrome Received: 9 Mar 2014 Accepted:
Iranian Journal of Neurology Original Paper Iran J Neurol 2014; 13(3): 138-143 Comparison of electrophysiological findings in axonal and demyelinating Guillain-Barre syndrome Received: 9 Mar 2014 Accepted:
Case Report Central Nervous System Demyelination in a Charcot-Marie-Tooth Type 1A Patient
 Case Reports in Neurological Medicine Volume 2013, Article ID 243652, 4 pages http://dx.doi.org/10.1155/2013/243652 Case Report Central Nervous System Demyelination in a Charcot-Marie-Tooth Type 1A Patient
Case Reports in Neurological Medicine Volume 2013, Article ID 243652, 4 pages http://dx.doi.org/10.1155/2013/243652 Case Report Central Nervous System Demyelination in a Charcot-Marie-Tooth Type 1A Patient
This is a repository copy of Anti-MAG negative distal acquired demyelinating symmetric neuropathy in association with a neuroendocrine tumor..
 This is a repository copy of Anti-MAG negative distal acquired demyelinating symmetric neuropathy in association with a neuroendocrine tumor.. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk//
This is a repository copy of Anti-MAG negative distal acquired demyelinating symmetric neuropathy in association with a neuroendocrine tumor.. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk//
Nerve Conduction Studies and EMG
 Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Intravenous immunoglobulin response treatment-naïve chronic inflammatory demyelinating polyradiculoneuropathy
 Predicting IVIg response in CIDP 1 http://hdl.handle.net/1765/105969 Intravenous immunoglobulin response in Chapter treatment-naïve 3.3 chronic inflammatory demyelinating polyradiculoneuropathy Intravenous
Predicting IVIg response in CIDP 1 http://hdl.handle.net/1765/105969 Intravenous immunoglobulin response in Chapter treatment-naïve 3.3 chronic inflammatory demyelinating polyradiculoneuropathy Intravenous
Peripheral neuropathy (PN)
") Peripheral neuropathy (PN) damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic:
Peripheral neuropathy (PN) damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic:
Differential Diagnosis of Neuropathies and Compression. Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre
 Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Differential Diagnosis of Neuropathies and Compression Dr Ashwin Pinto Consultant Neurologist Wessex Neurological Centre Outline of talk Mononeuropathies median and anterior interosseous nerve ulnar nerve
Study population The study population comprised adult patients fulfilling the following inclusion criteria:
 Cost-utility analysis of intravenous immunoglobulin and prednisolone for chronic inflammatory demyelinating polyradiculoneuropathy McCrone P, Chisholm D, Knapp M, Hughes R, Comi G, Dalakas M C, Illa I,
Cost-utility analysis of intravenous immunoglobulin and prednisolone for chronic inflammatory demyelinating polyradiculoneuropathy McCrone P, Chisholm D, Knapp M, Hughes R, Comi G, Dalakas M C, Illa I,
For convenience values outside the normal range are bolded. Normal values for the specified patient are stated below the tables.
 Case tudy 8 or convenience values outside the normal range are bolded. Normal values for the specified patient are stated below the tables. History: 60 year-ol man with a history of left hand weakness
Case tudy 8 or convenience values outside the normal range are bolded. Normal values for the specified patient are stated below the tables. History: 60 year-ol man with a history of left hand weakness
sensory nerves, motor nerves, autonomic nerves
 damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: long term, begins subtly
damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: long term, begins subtly
Infection-Associated Neurological Syndromes
 Infection-Associated Neurological Syndromes Anand P, MD PhD Medical Director, BloodCenter of Wisconsin Assistant Professor, Medical College of Wisconsin ASFA Annual Meeting San Antonio, TX, May 8th, 2015
Infection-Associated Neurological Syndromes Anand P, MD PhD Medical Director, BloodCenter of Wisconsin Assistant Professor, Medical College of Wisconsin ASFA Annual Meeting San Antonio, TX, May 8th, 2015
A/Professor Arun Aggarwal Balmain Hospital
 A/Professor Arun Aggarwal Balmain Hospital Nerve Conduction Studies Test to evaluate the function of motor / sensory nerves Evaluate Paraesthesia (numbness, tingling, burning) Weakness of arms and legs
A/Professor Arun Aggarwal Balmain Hospital Nerve Conduction Studies Test to evaluate the function of motor / sensory nerves Evaluate Paraesthesia (numbness, tingling, burning) Weakness of arms and legs
Motor and sensory nerve conduction studies
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Hands-on Course 2 Assessment of peripheral nerves function and structure in suspected peripheral neuropathies
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Hands-on Course 2 Assessment of peripheral nerves function and structure in suspected peripheral neuropathies
Drug Class Prior Authorization Criteria Immune Globulins
 Drug Class Prior Authorization Criteria Immune Globulins Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy has been developed through review of
Drug Class Prior Authorization Criteria Immune Globulins Line of Business: Medicaid P & T Approval Date: August 16, 2017 Effective Date: August 16, 2017 This policy has been developed through review of
Pharmacoeconomics of Intravenous Immunoglobulin in various Neurological Disorders
 303 Pharmacoeconomics of Intravenous Immunoglobulin in various Neurological Disorders Ching-Piao Tsai Acta Neurol Taiwan 2010;19:304-309 INTRODUCTION Intravenous immunoglobulin (IVIG) has multiple actions
303 Pharmacoeconomics of Intravenous Immunoglobulin in various Neurological Disorders Ching-Piao Tsai Acta Neurol Taiwan 2010;19:304-309 INTRODUCTION Intravenous immunoglobulin (IVIG) has multiple actions
DATE: 13 Mar 2015 CONTEXT AND POLICY ISSUES
 TITLE: Immunomodulatory Drugs and Intravenous Immunoglobulin (IVIg) for Patients with Chronic Demyelinating Polyneuropathy Who Are in Remission: A Review of Clinical and Cost-effectiveness and Guidelines
TITLE: Immunomodulatory Drugs and Intravenous Immunoglobulin (IVIg) for Patients with Chronic Demyelinating Polyneuropathy Who Are in Remission: A Review of Clinical and Cost-effectiveness and Guidelines
Multifocal motor neuropathy
 Multifocal motor neuropathy Jan-Thies H Van Asseldonk, Hessel Franssen, Renske M Van den Berg-Vos, John H J Wokke, Leonard H Van den Berg Multifocal motor neuropathy (MMN) is an immune-mediated disorder
Multifocal motor neuropathy Jan-Thies H Van Asseldonk, Hessel Franssen, Renske M Van den Berg-Vos, John H J Wokke, Leonard H Van den Berg Multifocal motor neuropathy (MMN) is an immune-mediated disorder
High resolution ultrasound in peripheral neuropathies
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 5 Advanced neurosonology - Level 3 High resolution ultrasound in peripheral neuropathies
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 5 Advanced neurosonology - Level 3 High resolution ultrasound in peripheral neuropathies
Electrodiagnostics for Back & Neck Pain. Steven Andersen, MD Providence Physiatry Clinic
 Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
Multifocal motor neuropathy with conduction
 3838ournal of Neurology, Neurosurgery, and Psychiatry 1995;59:38-44 Hopital de la Salpetriere, Paris, France P Bouche J-M Uger Hopital de Bicetre, le Kremlin-Bicetre, Paris, France A Moulonguet D Adams
3838ournal of Neurology, Neurosurgery, and Psychiatry 1995;59:38-44 Hopital de la Salpetriere, Paris, France P Bouche J-M Uger Hopital de Bicetre, le Kremlin-Bicetre, Paris, France A Moulonguet D Adams
S everal antibodies against gangliosides have been detected
 568 PAPER Central motor conduction in patients with anti-ganglioside antibody associated neuropathy syndromes and hyperreflexia Y Oshima, T Mitsui, H Yoshino, I Endo, M Kunishige, A Asano, T Matsumoto...
568 PAPER Central motor conduction in patients with anti-ganglioside antibody associated neuropathy syndromes and hyperreflexia Y Oshima, T Mitsui, H Yoshino, I Endo, M Kunishige, A Asano, T Matsumoto...
Myasthenia Gravis. Mike Gilchrist 10/30/06
 Myasthenia Gravis Mike Gilchrist 10/30/06 Overview Background Pathogenesis Clinical Manifestations Diagnosis Treatment Associated Conditions Background Severe muscle disease Most common disorder of neuromuscular
Myasthenia Gravis Mike Gilchrist 10/30/06 Overview Background Pathogenesis Clinical Manifestations Diagnosis Treatment Associated Conditions Background Severe muscle disease Most common disorder of neuromuscular
Clinical and electrophysiologic features of childhood Guillain-Barré syndrome in Northeast China
 Journal of the Formosan Medical Association (2014) 113, 634e639 Available online at www.sciencedirect.com journal homepage: www.jfma-online.com ORIGINAL ARTICLE Clinical and electrophysiologic features
Journal of the Formosan Medical Association (2014) 113, 634e639 Available online at www.sciencedirect.com journal homepage: www.jfma-online.com ORIGINAL ARTICLE Clinical and electrophysiologic features
NEUROLOGY NEUROSURGERY
 J7ournal of Neurology, Neurosurgery, and Psychiatry 1996;60:599-603 599 Multifocal motor neuropathy In 1982 Lewis et all reported five patients with a chronic, asymmetric, motor and sensory neuropathy
J7ournal of Neurology, Neurosurgery, and Psychiatry 1996;60:599-603 599 Multifocal motor neuropathy In 1982 Lewis et all reported five patients with a chronic, asymmetric, motor and sensory neuropathy
A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017
 A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017 Disclosures Research support from Cytokinetics, Inc Catalyst, Inc Editorial fees from UptoDate. Objectives Describe
A Practical Approach to Polyneuropathy SLOCUM DICKSON ANNUAL TEACHING DAY NOVEMBER 4, 2017 Disclosures Research support from Cytokinetics, Inc Catalyst, Inc Editorial fees from UptoDate. Objectives Describe
Update on Neurologic Complications in Persons With HIV Infection: 2017
 Update on Neurologic Complications in Persons With HIV Infection: 2017 FORMATTED: MM/DD/YY Chicago, Illinois: May 10, 2017 Dennis Kolson, MD, PhD Professor of Neurology University of Pennsylvania Philadelphia,
Update on Neurologic Complications in Persons With HIV Infection: 2017 FORMATTED: MM/DD/YY Chicago, Illinois: May 10, 2017 Dennis Kolson, MD, PhD Professor of Neurology University of Pennsylvania Philadelphia,
Paraparetic Guillain-Barré syndrome
 Paraparetic Guillain-Barré syndrome Bianca van den Berg, MD Christiaan Fokke, MD Judith Drenthen, MD Pieter A. van Doorn, MD, PhD Bart C. Jacobs, MD, PhD Correspondence to Dr. Jacobs: b.jacobs@erasmusmc.nl
Paraparetic Guillain-Barré syndrome Bianca van den Berg, MD Christiaan Fokke, MD Judith Drenthen, MD Pieter A. van Doorn, MD, PhD Bart C. Jacobs, MD, PhD Correspondence to Dr. Jacobs: b.jacobs@erasmusmc.nl
Miller Fisher Syndrome A variant of Guillan Barré Syndrome. Sarah I. Sheikh, BM BCh, MRCP
 Miller Fisher Syndrome A variant of Guillan Barré Syndrome Sarah I. Sheikh, BM BCh, MRCP History of GBS 1859 Jean Baptiste Octave Landry de Thézillat (1826-1865) published his observation on ascending
Miller Fisher Syndrome A variant of Guillan Barré Syndrome Sarah I. Sheikh, BM BCh, MRCP History of GBS 1859 Jean Baptiste Octave Landry de Thézillat (1826-1865) published his observation on ascending
Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype Five Years after Initial Diagnosis
 Case Reports in Neurological Medicine Volume 2013, Article ID 356157, 4 pages http://dx.doi.org/10.1155/2013/356157 Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype
Case Reports in Neurological Medicine Volume 2013, Article ID 356157, 4 pages http://dx.doi.org/10.1155/2013/356157 Case Report An Unusual Case of Recurrent Guillain-Barre Syndrome of a Different Subtype
MOTOR NEURONE DISEASE
 MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
MOTOR NEURONE DISEASE Dr Arun Aggarwal Department of Rehabilitation Medicine, RPAH Department of Neurology, Concord Hospital. Motor Neurone Disease Umbrella term in UK and Australia (ALS in USA) Neurodegenerative
Pathogenesis and treatment of immune-mediated neuropathies
 Therapeutic Advances in Neurological Disorders Review Pathogenesis and treatment of immune-mediated neuropathies Helmar C. Lehmann, Gerd Meyer zu Horste, Bernd C. Kieseier and Hans-Peter Hartung Ther Adv
Therapeutic Advances in Neurological Disorders Review Pathogenesis and treatment of immune-mediated neuropathies Helmar C. Lehmann, Gerd Meyer zu Horste, Bernd C. Kieseier and Hans-Peter Hartung Ther Adv
Prediction of Functional Outcome in Axonal Guillain-Barre Syndrome Eun Jung Sung, MD, Dae Yul Kim, MD, Min Cheol Chang, MD, Eun Jae Ko, MD
 Original Article Ann Rehabil Med 2016;40(3):481-488 pissn: 2234-0645 eissn: 2234-0653 http://dx.doi.org/10.5535/arm.2016.40.3.481 Annals of Rehabilitation Medicine Prediction of Functional Outcome in Axonal
Original Article Ann Rehabil Med 2016;40(3):481-488 pissn: 2234-0645 eissn: 2234-0653 http://dx.doi.org/10.5535/arm.2016.40.3.481 Annals of Rehabilitation Medicine Prediction of Functional Outcome in Axonal
IVIG (intravenous immunoglobulin) Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen
 Bivigam, Carimune NF, Flebogamma, Gammagard, Gammagard S/D, Gammaked, Gammaplex, Gamunex-C, Octagam, Privigen") Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Pre - PA Allowance None Prior-Approval Requirements Diagnoses Patient must have ONE of the following documented indications: 1. Primary Immunodeficiency Disease (PID) with ONE of the a. Hypogammaglobulinemia,
Compound Action Potential, CAP
 Stimulus Strength UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY INTRODUCTION TO NEUROPHYSIOLOGY Spring, 2013 Textbook of Medical Physiology by: Guyton & Hall, 12 th edition
Stimulus Strength UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PHYSIOLOGY & BIOCHEMISTRY INTRODUCTION TO NEUROPHYSIOLOGY Spring, 2013 Textbook of Medical Physiology by: Guyton & Hall, 12 th edition
Supplementary Online Content
 Supplementary Online Content Stevens O, Claeys KG, Poesen K, Veroniek S, Van Damme P. Diagnostic challenges and clinical characteristics of hepatitis E virus associated Guillain- Barré syndrome. JAMA Neurol.
Supplementary Online Content Stevens O, Claeys KG, Poesen K, Veroniek S, Van Damme P. Diagnostic challenges and clinical characteristics of hepatitis E virus associated Guillain- Barré syndrome. JAMA Neurol.
Muscle Wasting & Weakness in Critical Illness
 Muscle Wasting & Weakness in Critical Illness Clin A/Prof Michael O Leary Intensive Care Service Royal Prince Alfred Hospital, Sydney Sydney Medical School, The University of Sydney Disclosures I have
Muscle Wasting & Weakness in Critical Illness Clin A/Prof Michael O Leary Intensive Care Service Royal Prince Alfred Hospital, Sydney Sydney Medical School, The University of Sydney Disclosures I have
Hyperreflexia in Guillain-Barré syndrome: relation with acute motor axonal neuropathy and anti-gm1 antibody
 18 Department of Neurology, Chiba University School of Medicine, Chiba, Japan S Kuwabara K Ogawara M Mori T Hattori Department of Neurology, Dokkyo University School of Medicine, Tochigi, Japan M Koga
18 Department of Neurology, Chiba University School of Medicine, Chiba, Japan S Kuwabara K Ogawara M Mori T Hattori Department of Neurology, Dokkyo University School of Medicine, Tochigi, Japan M Koga
Traumatic Nerve Injuries. Nerve Injuries and Repair as Seen Through Electrodiagnostic Medicine
 Nerve Injuries and Repair as Seen Through Electrodiagnostic Medicine Ultra EMG February 2013 William S. Pease, M.D. Traumatic Nerve Injuries An orderly sequence of degeneration and regeneration follows
Nerve Injuries and Repair as Seen Through Electrodiagnostic Medicine Ultra EMG February 2013 William S. Pease, M.D. Traumatic Nerve Injuries An orderly sequence of degeneration and regeneration follows
EDUCATIONAL COMMENTARY NEUROLOGIC AUTOIMMUNE DISEASES
 EDUCATIONAL COMMENTARY NEUROLOGIC AUTOIMMUNE DISEASES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits,
EDUCATIONAL COMMENTARY NEUROLOGIC AUTOIMMUNE DISEASES Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits,
Disclosure. Entrapment Neuropathies - Overview. Common mononeuropathy sites. Definitions. Common mononeuropathy sites. Common mononeuropathy sites
 Disclosure Entrapment Neuropathies - Overview I receive compensation from Wiley- Blackwell publishers for my work as Editor-in-Chief of Muscle & Nerve Lawrence H. Phillips, II, MD Definitions Mononeuropathy:
Disclosure Entrapment Neuropathies - Overview I receive compensation from Wiley- Blackwell publishers for my work as Editor-in-Chief of Muscle & Nerve Lawrence H. Phillips, II, MD Definitions Mononeuropathy:
DIAGNOSIS OF DIABETIC NEUROPATHY
 DIAGNOSIS OF DIABETIC NEUROPATHY Dept of PM&R, College of Medicine, Korea University Dong Hwee Kim Electrodiagnosis ANS Clinical Measures QST DIAGRAM OF CASUAL PATHWAYS TO FOOT ULCERATION Rathur & Boulton.
DIAGNOSIS OF DIABETIC NEUROPATHY Dept of PM&R, College of Medicine, Korea University Dong Hwee Kim Electrodiagnosis ANS Clinical Measures QST DIAGRAM OF CASUAL PATHWAYS TO FOOT ULCERATION Rathur & Boulton.
IMMUNE GLOBULIN (IVIG AND SCIG) Brand Name Generic Name Length of Authorization Bivigam IVIG Per Medical Guidelines Carimune IVIG Per Medical
 Brand Name Generic Name Length of Authorization Bivigam IVIG Per Medical Guidelines Carimune IVIG Per Medical") Brand Name Generic Name Length of Authorization Bivigam IVIG Per Medical Guidelines Carimune IVIG Per Medical Guidelines Flebogamma IVIG Per Medical Guidelines Gammagard IVIG/SCIG Per Medical Guidelines
Brand Name Generic Name Length of Authorization Bivigam IVIG Per Medical Guidelines Carimune IVIG Per Medical Guidelines Flebogamma IVIG Per Medical Guidelines Gammagard IVIG/SCIG Per Medical Guidelines
The New Entity of Paranodopathies: A Target Structure with Therapeutic Consequences
 The New Entity of Paranodopathies: A Target Structure with Therapeutic Consequences Abstract Authors Kathrin Doppler, Claudia Sommer Affiliation Neurological Clinic, University Hospital Würzburg Key words
The New Entity of Paranodopathies: A Target Structure with Therapeutic Consequences Abstract Authors Kathrin Doppler, Claudia Sommer Affiliation Neurological Clinic, University Hospital Würzburg Key words
Inflammatory neuropathies are uncommon but important to diagnose because they are treatable.
 MANAGEMENT OF INFLAMMATORY NEUROPATHIES See end of article for authors affiliations c GUILLAIN-BARRÉ Correspondence to: Dr Robert Hadden, West London Neurosciences Centre, Charing Cross Hospital, Fulham
MANAGEMENT OF INFLAMMATORY NEUROPATHIES See end of article for authors affiliations c GUILLAIN-BARRÉ Correspondence to: Dr Robert Hadden, West London Neurosciences Centre, Charing Cross Hospital, Fulham
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Guillain-Barré syndrome and related disorders
 Guillain-Barré syndrome and related disorders Dr Benjamin Wakerley Department of Neurology Gloucestershire Royal Hospital Disclosures Novartis - educational grant Guillain-Barré syndrome and related disorders
Guillain-Barré syndrome and related disorders Dr Benjamin Wakerley Department of Neurology Gloucestershire Royal Hospital Disclosures Novartis - educational grant Guillain-Barré syndrome and related disorders
Rituximab in patients with CIDP: A report of 13 cases and review of the literature
 Rituximab in patients with CIDP: A report of 13 cases and review of the literature Luana Benedetti, Chiara Briani, Diego Franciotta, Raffaella Fazio, Ilaria Paolasso, Cristoforo Comi, Marco Luigetti, Mario
Rituximab in patients with CIDP: A report of 13 cases and review of the literature Luana Benedetti, Chiara Briani, Diego Franciotta, Raffaella Fazio, Ilaria Paolasso, Cristoforo Comi, Marco Luigetti, Mario
Intravenous immunoglobulin how to use it
 DECEMBER 2001 93 THERAPEUTIC INTERVENTION Intravenous immunoglobulin how to use it Jane Pritchard and Richard A.C. Hughes Department of Neuroimmunology, Guy s, King s and St Thomas School of Medicine,
DECEMBER 2001 93 THERAPEUTIC INTERVENTION Intravenous immunoglobulin how to use it Jane Pritchard and Richard A.C. Hughes Department of Neuroimmunology, Guy s, King s and St Thomas School of Medicine,
A Case of Acute Sensory Neuropathy Associated with Contrast Enhancement of the Cauda Equina on Magnetic Resonance Imaging
 61 Case Report St. Marianna Med. J. Vol. 33, pp. 61 66, 2005 A Case of Acute Sensory Neuropathy Associated with Contrast Enhancement of the Cauda Equina on Magnetic Resonance Imaging Toshinari Kobayashi
61 Case Report St. Marianna Med. J. Vol. 33, pp. 61 66, 2005 A Case of Acute Sensory Neuropathy Associated with Contrast Enhancement of the Cauda Equina on Magnetic Resonance Imaging Toshinari Kobayashi
Intravenous immunoglobulin (IVIG) in the treatment of chronic demyelinating polyradiculoneuropathy
 in the treatment of chronic demyelinating polyradiculoneuropathy") Acta neurol. belg., 2001, 101, 147-151 Editorial Intravenous immunoglobulin (IVIG) in the treatment of chronic demyelinating polyradiculoneuropathy P. Y. K. VAN DEN BERGH Service de Neurologie, Centre
Acta neurol. belg., 2001, 101, 147-151 Editorial Intravenous immunoglobulin (IVIG) in the treatment of chronic demyelinating polyradiculoneuropathy P. Y. K. VAN DEN BERGH Service de Neurologie, Centre
Wingerchuk et al, Neurol, 2006
 Current Understanding of Neuromyelitis Optica Jacqueline A. Leavitt, M.D. Mayo Clinic Rochester, MN I have no financial disclosures 46 y/o F Pain in R temple worse with head movements, resolved in days
Current Understanding of Neuromyelitis Optica Jacqueline A. Leavitt, M.D. Mayo Clinic Rochester, MN I have no financial disclosures 46 y/o F Pain in R temple worse with head movements, resolved in days
UvA-DARE (Digital Academic Repository) Treatment of chronic inflammatory neuropathies Eftimov, F. Link to publication
 Treatment of chronic inflammatory neuropathies Eftimov, F. Link to publication") UvA-DARE (Digital Academic Repository) Treatment of chronic inflammatory neuropathies Eftimov, F. Link to publication Citation for published version (APA): Eftimov, F. (2015). Treatment of chronic inflammatory
UvA-DARE (Digital Academic Repository) Treatment of chronic inflammatory neuropathies Eftimov, F. Link to publication Citation for published version (APA): Eftimov, F. (2015). Treatment of chronic inflammatory
5.1 Alex.
 5.1 Alex http://tinyurl.com/neuromakessense Alex is a 20-year-old full-time national serviceman. His only past medical history is asthma, presents to A&E with a 4-day history of bilateral finger weakness
5.1 Alex http://tinyurl.com/neuromakessense Alex is a 20-year-old full-time national serviceman. His only past medical history is asthma, presents to A&E with a 4-day history of bilateral finger weakness
Chapter 17 Nervous System
 Chapter 17 Nervous System 1 The Nervous System Two Anatomical Divisions Central Nervous System (CNS) Brain and Spinal Cord Peripheral Nervous System (PNS) Two Types of Cells Neurons Transmit nerve impulses
Chapter 17 Nervous System 1 The Nervous System Two Anatomical Divisions Central Nervous System (CNS) Brain and Spinal Cord Peripheral Nervous System (PNS) Two Types of Cells Neurons Transmit nerve impulses
Dendrites Receive impulse from the axon of other neurons through synaptic connection. Conduct impulse towards the cell body Axon
 Dendrites Receive impulse from the axon of other neurons through synaptic connection. Conduct impulse towards the cell body Axon Page 22 of 237 Conduct impulses away from cell body Impulses arise from
Dendrites Receive impulse from the axon of other neurons through synaptic connection. Conduct impulse towards the cell body Axon Page 22 of 237 Conduct impulses away from cell body Impulses arise from
Current treatment in Guillain-Barré Syndrome and myasthenia gravis
 4 rd Congress of the European Academy of Neurology Lisbon, Portugal, June 16-19, 2018 Teaching Course 10 Current treatments in neurology Level 1 Current treatment in Guillain-Barré Syndrome and myasthenia
4 rd Congress of the European Academy of Neurology Lisbon, Portugal, June 16-19, 2018 Teaching Course 10 Current treatments in neurology Level 1 Current treatment in Guillain-Barré Syndrome and myasthenia
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
Guillain-Barré Syndrome
 Guillain-Barré Syndrome Ouch! www.philippelefevre.com Guillain-Barré Syndrome Acute post-infective polyneuropathy Heterogeneous condition with several variant forms Lipid A Neuronal Ganglioside Pathogenesis
Guillain-Barré Syndrome Ouch! www.philippelefevre.com Guillain-Barré Syndrome Acute post-infective polyneuropathy Heterogeneous condition with several variant forms Lipid A Neuronal Ganglioside Pathogenesis
High-dose intravenous. multifocal motor neuropathy. immunoglobulin therapy in
 High-dose intravenous immunoglobulin therapy in multifocal motor neuropathy E. Nobile-Orazio, MD, PhD; N. Meucci, MD; S. Barbieri, MD, PhD; M. Carpo, MD; and G. Scarlato, MD Article abstract-we treated
High-dose intravenous immunoglobulin therapy in multifocal motor neuropathy E. Nobile-Orazio, MD, PhD; N. Meucci, MD; S. Barbieri, MD, PhD; M. Carpo, MD; and G. Scarlato, MD Article abstract-we treated
A family study of Charcot-Marie-Tooth disease
 Joturnal of Medical Genetics, 1982, 19, 88-93 A family study of Charcot-Marie-Tooth disease A P BROOKS* AND A E H EMERY From the University Department of Human Genetics, Western General Hospital, Edinburgh
Joturnal of Medical Genetics, 1982, 19, 88-93 A family study of Charcot-Marie-Tooth disease A P BROOKS* AND A E H EMERY From the University Department of Human Genetics, Western General Hospital, Edinburgh
Multifocal motor neuropathy presenting as a post-infectious complication of dengue: a CASE report
 Higgoda et al. BMC Infectious Diseases (2018) 18:415 https://doi.org/10.1186/s12879-018-3334-z CASE REPORT Open Access Multifocal motor neuropathy presenting as a post-infectious complication of dengue:
Higgoda et al. BMC Infectious Diseases (2018) 18:415 https://doi.org/10.1186/s12879-018-3334-z CASE REPORT Open Access Multifocal motor neuropathy presenting as a post-infectious complication of dengue:
Primary Diagnosis: Diagnosis Code(s) (if known): Individual s Weight (lbs) (kg)
 (if known): Individual s Weight (lbs) (kg)") Request Date: Initial Request Buy and Bill Individual s Name: Insurance Identification Number: Subsequent request Date of Birth: Individual s Phone Number: Primary Diagnosis: Diagnosis Code(s) (if known):
Request Date: Initial Request Buy and Bill Individual s Name: Insurance Identification Number: Subsequent request Date of Birth: Individual s Phone Number: Primary Diagnosis: Diagnosis Code(s) (if known):
Diagnosis and Management of Immune-mediated Neuropathies
 Continuing Medical Education 39 Diagnosis and Management of Immune-mediated Neuropathies Sung-Tsang Hsieh Abstract- Immune-mediate neuropathies, or inflammatory neuropathies are neuropathies due to the
Continuing Medical Education 39 Diagnosis and Management of Immune-mediated Neuropathies Sung-Tsang Hsieh Abstract- Immune-mediate neuropathies, or inflammatory neuropathies are neuropathies due to the
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases
 Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Peripheral neuropathies, neuromuscular junction disorders, & CNS myelin diseases Peripheral neuropathies according to which part affected Axonal Demyelinating with axonal sparing Many times: mixed features
Immune Globulin. Prior Authorization
 MB9423 Covered Service: Yes when meets criteria below Prior Authorization Required: Additional Information: Yes as shown below Requires prior authorization through Navitus and is considered medically appropriate
MB9423 Covered Service: Yes when meets criteria below Prior Authorization Required: Additional Information: Yes as shown below Requires prior authorization through Navitus and is considered medically appropriate
CLINICAL AND LABORATORY FEATURES OF NEUROPATHIES WITH SERUM IgM BINDING TO TS-HDS
 CLINICAL AND LABORATORY FEATURES OF NEUROPATHIES WITH SERUM IgM BINDING TO TS-HDS ALAN PESTRONK, MD, 1,2 ROBERT E. SCHMIDT, MD, PhD, 2 RATI M. CHOKSI, MS, 1 R. BRIAN SOMMERVILLE, MD, 1 and MUHAMMAD T.
CLINICAL AND LABORATORY FEATURES OF NEUROPATHIES WITH SERUM IgM BINDING TO TS-HDS ALAN PESTRONK, MD, 1,2 ROBERT E. SCHMIDT, MD, PhD, 2 RATI M. CHOKSI, MS, 1 R. BRIAN SOMMERVILLE, MD, 1 and MUHAMMAD T.
Acute respiratory failure in the setting of Chronic In lammatory Demyelinating Polyneuropathy
 Open Journal of Clinical & Medical Case Reports Volume 3 (2017) Issue 20 ISSN 2379-1039 Acute respiratory failure in the setting of Chronic In lammatory Demyelinating Polyneuropathy Joseph Burns*; Michael
Open Journal of Clinical & Medical Case Reports Volume 3 (2017) Issue 20 ISSN 2379-1039 Acute respiratory failure in the setting of Chronic In lammatory Demyelinating Polyneuropathy Joseph Burns*; Michael